
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 25 April 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.854970
This article is part of the Research TopicPrevention and Control of Human T Lymphotropic Viruses 1 and 2 (HTLV-1/2)View all 32 articles
 Cintia Yolette Urbano Pauxis Aben-Athar1,2,3
Cintia Yolette Urbano Pauxis Aben-Athar1,2,3 Edilson Coelho Sampaio1,2,3
Edilson Coelho Sampaio1,2,3 Denise Silva Pinto4
Denise Silva Pinto4 Antonio Carlos Rosário Vallinoto2,3*
Antonio Carlos Rosário Vallinoto2,3* Izaura Maria Vieira Cayres Vallinoto2,3*
Izaura Maria Vieira Cayres Vallinoto2,3*Introduction: The absence of nursing care plans aimed at people living with HTLV-1 (PLHTLV) led us to develop and test a proposed nursing care plan based on the evaluation of 55 PLHTLV to outline interventions according to the clinical stage.
Methods: After interviews with symptomatic patients, nursing diagnoses were made using the NANDA International Nursing Diagnoses (The International Nursing Knowledge Association). Subsequently, interventions were selected through the Classification of Nursing Interventions (NIC), and expected results were selected through the Classification of Nursing Outcomes (NOC).
Results: The actual diagnoses included (ii) chronic pain, (iii) impaired urinary elimination, and (iv) sexual dysfunction; the health promotion diagnosis was (i) risk-prone health behavior; and the risk diagnoses were (i) risk of feeling powerless and (ii) risk of falls in adults. Nursing care must prevent the lack of adherence to monitoring, establish goals and promote family involvement. A safe home environment requires intervention for fall prevention. Full support in understanding pharmacological and non-pharmacological therapies for chronic pain is needed. Interventions allow patients with impaired urinary function to be reintroduced to society. For sexual dysfunction, it is necessary to discuss safe sex and behavioral changes. Regarding risk behaviors, it is necessary to guide the patient/family, adapt language to the education level of these individuals, and help them better accept the condition, among other guidelines.
Conclusion: The development of a nursing care plan for PLHTLV is essential for preventing the rapid progression of disease and the improvement of the quality of life of PLHTLV and should be included in the multidisciplinary approach to the secondary level of prevention of HTLV-1.
Human T-lymphotropic virus 1 (HTLV-1) was the first human retrovirus to be isolated from lymphocytes from a person with T-cell lymphoma (1). Studies carried out in the Caribbean and Japan made it possible to detect anti-HTLV-1 antibodies in people who had a neurological picture of spastic paresis, with the lower limbs being the most affected (2–4). The first clinical findings showed that HTLV-1 was a neurotropic agent and that, somehow, it was associated with the pathogenesis of the disease (2), currently called HTLV-1-associated myelopathy (HAM) (5).
Even 40 years after its isolation, HTLV-1 infection continues to be neglected (6), with no efficient drug treatment (7, 8) that promotes healing. Currently, treatment has been administered in the clinical practice of many health professionals, with the application of palliative care associated with the use of some drugs aimed at improving the health status of people living with HTLV-1 (PLHTLV) and, consequently, their quality of life (9, 10).
In Brazil, the follow-up of less complex cases of HTLV-1 can be performed in primary health care (PHC), while more complex cases, in which there is a need for the diagnosis of diseases associated with infection or the elaboration of the clinical management of these patients, should be aimed at secondary or tertiary levels of health care (11). Assistance for PLHTLV takes place through multidisciplinary teams, and nursing deserves to be highlighted since, especially in Brazil, it is one of the professions with the highest number of professionals and the closest proximity to users of the Unified Health System (SUS). For this professional class, the nursing process represents a great achievement because it allows the organization, energization, improvement and individualization of the care process. In addition, it allows for humanized care that is complementary to the assistance of other health professionals (12).
However, in Brazil, there is a lack of information among health professionals (13), especially among nurses (14), which makes it difficult to assist and monitor PLHTLV, as nurses must be able to identify diagnoses and plan interventions that are appropriate to improve the quality of care provided to the patient (14, 15). Associated with this, HTLV infection remains a public health problem in Brazil, with the absence of effective public policies that allow the reduction of transmission and the use of therapeutic measures (11). In this sense, the importance of building effective care plans is highlighted based on validation studies of tests and the creation of protocols (11), which provide an improvement in quality of life (15) and reduce vulnerability among PLHTLV (13).
The care plan must provide parameters to monitor the clinical status of patients, assist in the education process regarding prevention measures, and encourage the promotion of care for both PLWHA and their families to improve quality of care and quality of life, reduce stigma and discrimination, direct care, and increase the visibility of the topic (13). Thus, the present study aimed to develop a nursing care plan based on the evaluation of 55 PLHTLV and to design interventions according to the clinical picture.
This was an observational, descriptive and cross-sectional study. The research was carried out from August 2016 to December 2018 at the Laboratory of Clinical and Epidemiology of Endemic Diseases of the Nucleus of Tropical Medicine (NMT) and at the Laboratory of Studies in Functional Rehabilitation (LAERF) of the Federal University of Pará (UFPA).
The present study was based on a spontaneous demand for care from patients diagnosed with HTLV who sought the service for periodic evaluation. Fifty-five PLHTLV were evaluated (34 asymptomatic and 21 symptomatic for HAM), over 18 years of age and who agreed to participate in the research, by signing the Free and Informed Consent Form (TLCE). The research was approved by the Research Ethics Committee of the Institute of Health Sciences (ICS) of the Federal University of Pará (UFPA) (CAAE: 55699316.6.0000.0018).
As described previously (16), data collection took place through the clinical assessment of PLHTLV using a semistructured interview questionnaire, including the following questions: (i) identification; (ii) socio-economic data (marital status, profession/occupation, family income and education); (iii) epidemiological data (blood transfusion, injecting drug use, information on sexual relations, number of partners, use of contraceptive methods, history of STI, history of breastfeeding, family history of HTLV or HTLV-associated disease); and (iv) clinical data (time of HTLV infection, how the diagnosis was made, and questions about HAM symptoms). The following instruments were used: the SALSA Scale, a social participation scale, the Brazilian version of the SF-36 Quality of Life Questionnaire and the Summarized Pain Inventory.
After the evaluation of the patients, the following steps were performed: (a) identification of diagnoses; (b) formulation of nursing results; (c) initial proposal of nursing interventions; and (d) elaboration of a care plan.
After the patients were interviewed, the identification of nursing diagnoses was carried out through the use of the Nursing Diagnoses of NANDA International (The International Nursing Knowledge Association) definitions and classification 2021–2023 (17).
The Nursing Outcomes Classification (NOC) (18) was used to select the expected outcomes for each proposed intervention. Subsequently, the selection of nursing interventions was made using the Classification of Nursing Interventions (NIC) (19). The intervention consisted of a therapy that could be directed to both the patient and his or her family (19).
The evaluation of 55 PLHTLV allowed the construction of a nursing care plan to be used in clinical practice in an outpatient setting. This plan was organized according to specific nursing methodologies based on the NANDA-I taxonomy (2021–2023) (17).
The diagnoses are listed in Table 1 by domain to facilitate the identification of the main affected areas in the patients. Of the 13 domains established in the NANDA-I taxonomy (17), the patients in this research had seven affected areas and needed special attention from nurses during the consultation.
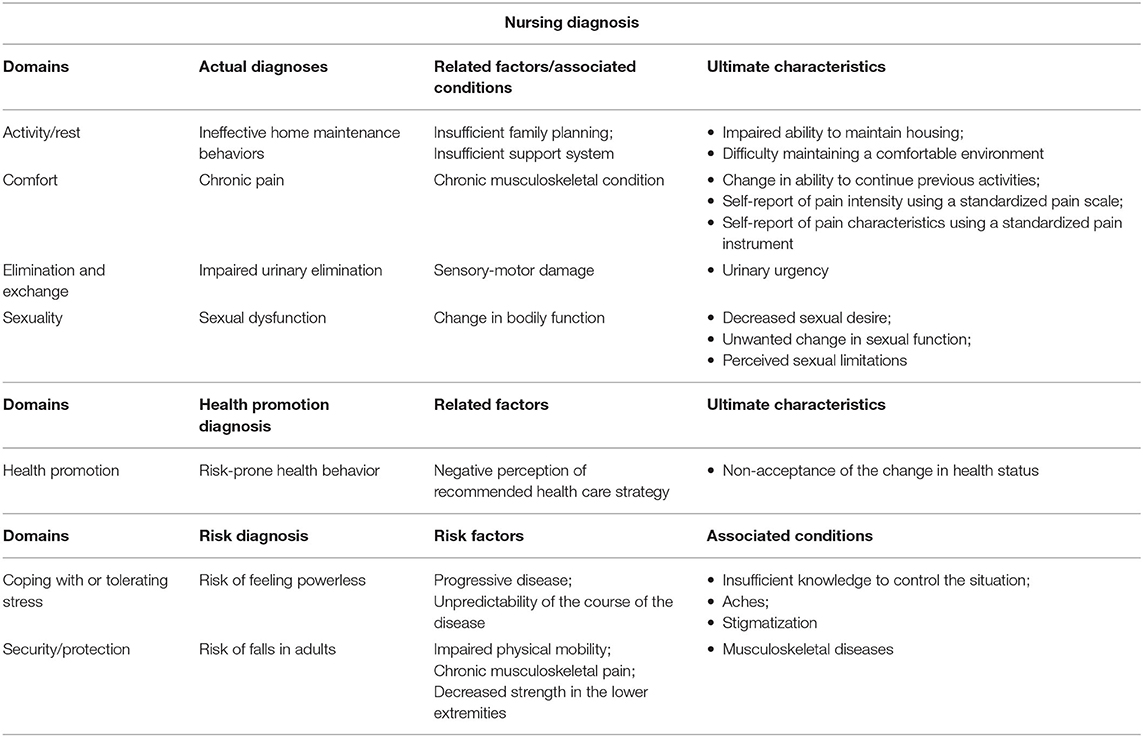
Table 1. NANDA-I nursing diagnoses of patients with HTLV-1.
The domains identified were (i) activity/rest, (ii) comfort, (iii) elimination and exchange, (iv) sexuality, (v) health promotion, (vi) coping/stress tolerance and (vii) safety/protection.
Thus, in Table 1, the following real nursing diagnoses are presented: (i) lack of adherence, (ii) impaired home maintenance, (iii) chronic pain, (iv) impaired urinary elimination and (v) sexual dysfunction. In addition, the health promotion diagnosis was risk-prone health behavior, and the following risk diagnoses were identified: risk of feeling helpless and risk of falls.
The identification of diagnoses allows the nurse to draw up a care plan that must be followed for the proposed interventions and, later, must be evaluated to see if the expected results were achieved.
Table 2 presents the care plan established for the assessment and monitoring of PLHTLV. Notably, such a plan should be used as a guide for nurses' conduct during care for PLHTLV since such diagnoses were common to the patients evaluated. It is relevant to highlight that each patient must be individually and critically evaluated so that the nurse can implement care directed to the real needs of PLHTLV.
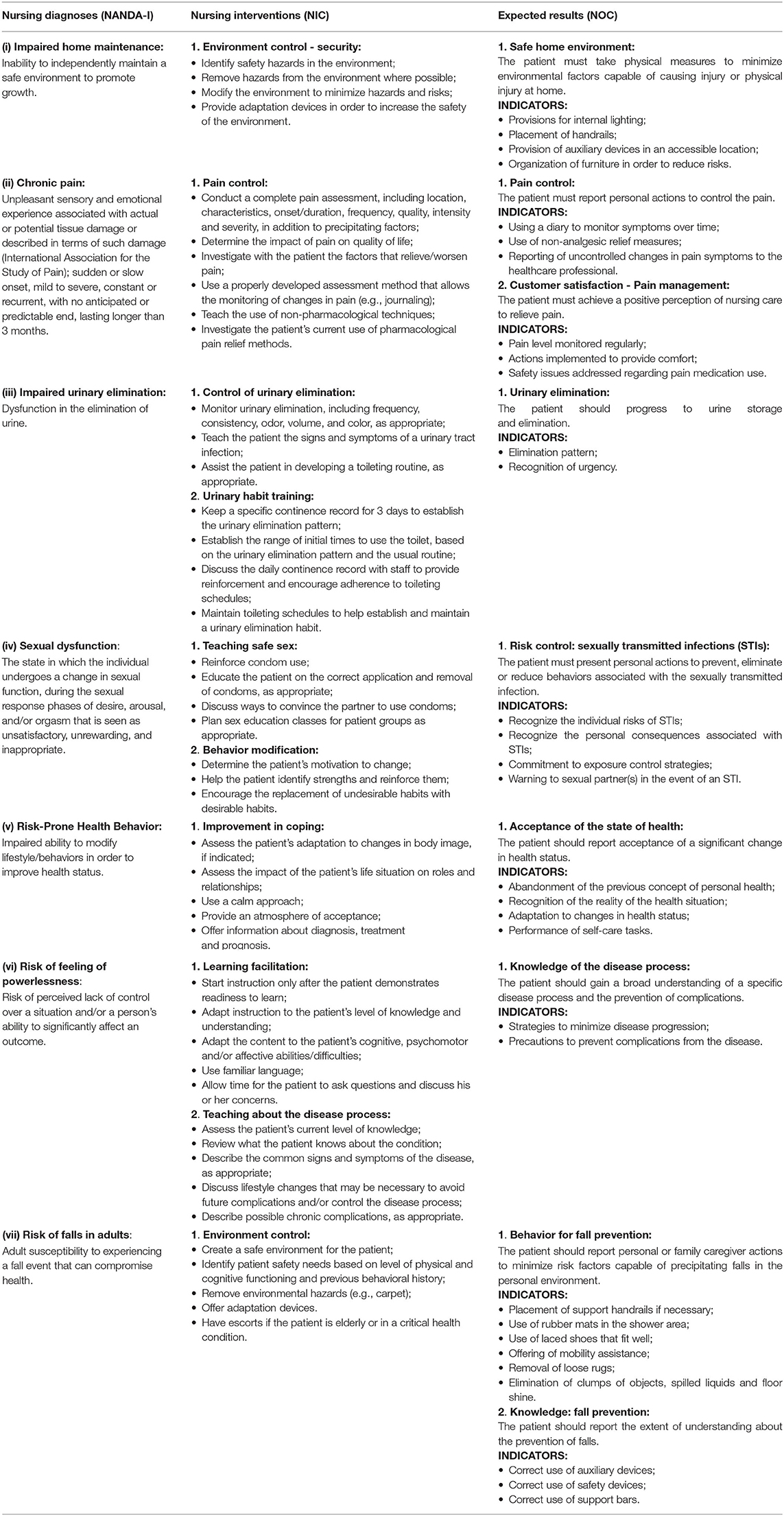
Table 2. Nursing care plans for HTLV-1-infected patients.
The nurse must, at each consultation, reassess the patient and identify the diagnoses to establish new behaviors to be followed based on the care plan produced in this research. The routine periodic consultations allow the clinical follow-up of the patient, targeted care aimed at improving the quality of life, and sex education with the purpose of interrupting the chain of transmission of the virus.
Nursing consultations for PLHTLV are intended to promote self-care actions, institute care for recovery, and provide guidance for adaptation to the consequences imposed by diseases associated with the virus (20). In this sense, the care plan deserves to be highlighted, as it can be used as a tool to promote holistic care (21), but it requires planning and must be created based on nursing diagnoses, as these allow the identification of what achievements are desired and what interventions are needed (22).
Nursing must act based on two main aspects: the establishment of mutual goals and the promotion of family involvement. It is entirely relevant that professionals be trained to promote the correct orientation to patients (23). Family members, in turn, should be encouraged so that a support network can be established (24). In this way, a favorable environment is created to promote adherence to rehabilitation, as well as to enable the improvement of trust and, consequently, the improvement of the nurse/patient interpersonal relationship (25). It becomes possible for the patient to redefine many issues, such as their plans and dreams, which are often left aside after the diagnosis (23).
The diagnosis of ineffective home maintenance behaviors refers to the impossibility of independently leaving the safe environment. Environmental control has been instituted as an intervention to achieve a safe home environment (17–19). It is common for patients with HTLV-1 to report falls and even fear of falls (26); therefore, some changes in the environment in which the patient lives are necessary.
Pain causes not only physical discomfort but also functional limitations and limitations in carrying out activities (24); in addition, pain treatment is often tiring and does not always achieve positive results (27). Therefore, the teaching of pain control and/or monitoring becomes indispensable. Thus, pharmacological and non-pharmacological therapies must be maintained so that pain is controlled (28), and nursing must remain attentive to eliminate patients' possible doubts and to help them understand the therapies chosen by health team.
Another nursing diagnosis verified in the patients in this study was impaired urinary elimination, so the interventions suggested in the care plan included elimination control and urinary habit training, which aim, above all, for efficient urinary elimination (17–19). The neurological sequelae are painful, and many patients develop urinary disorders, which often make it impossible to carry out their usual activities. In this sense, the instructions and the promotion of bladder reestablishment allow the patient's reintroduction to society, with the accomplishment of their tasks and with the strengthening of ties (29).
Disabilities that occur as a result of the neurodegenerative process often cause the patient to lose privacy, as he or she becomes dependent on other people to perform self-care activities such as going to the bathroom (23). Furthermore, the increase in urinary frequency causes not only emotional damage but also social damage due to inherent isolation (23). As a result, the quality of life is affected, and as there is no treatment that totally improves this urinary issue, rehabilitation must be offered (30).
Sexual issues must be addressed during patient education practices, as diagnosis with HTLV-1 causes changes in the sexual life of PLHTLV (29). The condition of the person living with the virus, increased urinary frequency and sexual dysfunction change the routine of couples and, as a consequence, change the ability to experience pleasure and sometimes cause the separation of couples who previously had sexual and affective relationships (20). The diagnosis of sexual dysfunction was evident in this research, and due to its consequences, the following intervention was established: teaching safe sex and behavior modification (17–19).
Teaching and counseling actions are very important health promotion activities and therefore require professionals to know the implications of HTLV-1 infection, as there is a lack of knowledge among health professionals (31). Counseling should include questions about sexuality and the use of prevention measures and should also address pregnancy, prenatal care, childbirth and the postpartum period, in particular issues related to avoiding breastfeeding and using formulas to replace breastmilk (29).
The health promotion and risk diagnoses identified from the assessment of PLHTLV demand the following interventions: improving coping, facilitating learning and/or teaching the disease process and controlling the environment (17, 19).
HTLV-1 is associated with a chronic disease that promotes mobility impairment, which becomes an important factor in the risk of falls. To prevent and/or reduce this risk, the patient should be instructed to use mobility aids. However, even with the risk of falling, patients prefer to derive support from objects rather than use an aid (24). The importance of guidance is evident so that such risk is avoided.
Guidance can also be provided to help the patient and/or family member better accept the health condition, preventing risk-prone health behavior. Understanding allows for better acceptance and encourages the continuity of participation and engagement in activities in society, thus enabling the acquisition of a new attitude toward the disease (24).
The risk of feeling helpless was evidenced among the patients in this research, and for this situation to be avoided, it is necessary for nurses to teach the health and disease process, always clarifying the doubts of the patient and family members. Such instruction must be performed orally and/or in writing, with the language always being adapted according to the level of education of patients and their families (32), as has already occurred in other care centers for PLHTLV (20).
Within this context of health promotion, it is essential to carry out activities through nursing, either based on the guidelines, the care taught or the possibility of identifying risks and the use of timely interventions. This enables the patient to provide care not only for the treatment of the consequences of the pathology but also for himself or herself as a human being, thus providing more comprehensive care (20, 23).
Nursing is a profession that stands out in the context of health care for PLHTLV, given the possibility for nurses to work in different care contexts, from primary to tertiary health care, and to always seek to develop promotion activities and the protection and recovery of health according to the guidelines of the SUS. The care activity of nurses takes place through the nursing process, which consists of a scientific work methodology that directs care based on clinical findings. Thus, it is understood that the elaboration of a care plan for PLHTLV constitutes an advance for care to become more directed to the clinical characteristics of this specific public. Additionally, it enables the redefinition of the nurse's role in this context.
The clinical evaluation of the patients in this research allowed the identification of nursing diagnoses that enabled the construction of a care plan, which aims to improve care for PLHTLV. The findings of this research confirm the importance of nurses being able to assess and identify diagnoses to enable the creation of more comprehensive care. Finally, the development of a nursing care plan allowed the planning of feasible actions that aim to improve and complement the multidisciplinary care offered to PLHTLV and their families, seeking to increase the perseverance, comfort and quality of life of patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Health Sciences Institute of the Federal University of Pará (CAAE: 55699316.6.0000.0018). The patients/participants provided their written informed consent to participate in this study.
CA-A, DP, and AV conceived and designed the study. CA-A, DP, and ES assisted in patient recruitment and health care. CA-A, AV, and ICV wrote the manuscript. All authors read and approved the final manuscript.
This study was supported by the National Council for Scientific and Technological Development (CNPq; # 301869/2017-0; and 442522/2019-3), Pan-American Health Organization (#SCON2021-00310), and the Federal University of Pará (PAPQ-2022).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all patients who agreed to participate in the study.
1. Poiesz BJ, Ruscetti FW, Gazdar AF, Bunn PA, Minna JD, Gallo RC. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc Natl Acad Sci USA. (1980) 77:7415. doi: 10.1073/pnas.77.12.7415
2. Gessain A, Vernant JC, Maurs L, Barin F, Gout O, Calender A, et al. Antibodies to human t-lymphotropic virus type-1 in patients with tropical spastic paraparesis. Lancet. (1985) 8452:407–10. doi: 10.1016/S0140-6736(85)92734-5
3. Osame M, Usuku K, Izumo S, Ijichi N, Amitani H, Igata A, et al. HTLV-I associated myelopathy: a new clinical entity. Lancet. (1986) 327:1031–2. doi: 10.1016/S0140-6736(86)91298-5
4. Araujo AQC, Wedemann D. HTLV-1 associated neurological complex. What is hidden below the water? AIDS Rev. (2019) 21:4. doi: 10.24875/AIDSRev.19000108
5. Iijima N, Yamauchi J, Yagishita N, Araya N, Aratani S, Tanabe K, et al. Clinical course of neurogenic bladder dysfunction in human T-cell leukemia virus type-1-associated myelopathy/tropical spastic paraparesis: a nationwide registry study in Japan. Orphanet J Rare Dis. (2021) 16:355. doi: 10.1186/s13023-021-01990-3
6. Martin F, Tagaya Y, Gallo R. Time to eradicate HTLV-1: an open letter to WHO. Lancet. (2018) 391:1893–4. doi: 10.1016/S0140-6736(18)30974-7
7. Futsch N, Mahieux R, Dutartre H. HTLV-1, the other pathogenic yet neglected human retrovirus: from transmission to therapeutic treatment. Viruses. (2018) 10:1. doi: 10.3390/v10010001
8. Rosadas C, Assone T, Yamashita M, Adonis A, Puccioni-Sohler M, Santos M, et al. Health state utility values in people living with htlv-1 and in patients with HAM/TSP: The impact of a neglected disease on the quality of life. PLoS Negl Trop Dis. (2020) 14:e0008761. doi: 10.1371/journal.pntd.0008761
9. de Paula JJ, Romanelli LC, de Faria RCV, Proietti AB, Malloy-Diniz LF, Romano-Silva MA, et al. Cognitive impairment in the HTLV-1 infection: a comparative study associated with functional performance. J Neurovirol. (2021) 27:849–56. doi: 10.1007/s13365-020-00905-5
10. World Health Organization. Human T-Lymphotropic Virus Type 1: Technical Report. Geneva (2021). Available online at: https://apps.who.int/iris/bitstream/handle/10665/339773/9789240020221-eng.pdf?sequence=1 (accessed March 14, 2022).
11. Rosadas C, Brites C, Arakaki-Sanchez D, Casseb J, Ishak R. Brazilian protocol for sexually transmitted infections 2020: human T-cell lymphotropic virus (HTLV) infection. Rev Soc Bras Med Trop. (2021) 54:2020605. doi: 10.1590/0037-8682-605-2020
12. Dos Santos WN. Sistematização da assistência de enfermagem: o contexto histórico, o processo e obstáculos da implantação. J Manag Prim Health Care. (2014) 5:153–8. doi: 10.14295/jmphc.v5i2.210
13. Garcia IFS, Hennington EA. HTLV: uma infecção estigmatizante? Cad Saúde Pública. (2019) 35:e00005419. doi: 10.1590/0102-311x00005419
14. Soares DJ, Santos ACC, Rivemales MCC. Conhecimento da enfermeira do Programa de Saúde da Família sobre o vírus linfotrópico de células T humanas. Enferm Brasil. (2018) 17:75–82. doi: 10.33233/eb.v17i2.1009
15. Souza LS, Sampaio DC, Rivemales MCC, Oliveira LLC, Jesus APS, Lima CFM, et al. Diagnósticos de Enfermagem em pessoas soropositivas pelo vírus linfotrópico T humano. Rev Baiana Enferm. (2020) 34:37991. doi: 10.18471/rbe.v34.37991
16. Aben-Athar CYUP, Pinto DDS, Lima SS, Vallinoto IMVC, Ishak R, Vallinoto ACR. Limitations in daily activities, risk awareness, social participation, and pain in patients with HTLV-1 using the SALSA and participation scales. Braz J Infect Dis. (2020) 24:497–504. doi: 10.1016/j.bjid.2020.08.009
17. NANDA Diagnósticos de Enfermagem da NANDA-I: Definições e Classificação 2021-2023 / [NANDA International]. In: Herdman TH, Kamitsuru S, Lopes CT, editors. Diagnósticos de Enfermagem da NANDA-I: Definições e Classificação, 12ª ed. New York, NY: Thieme Medical Publishers, Inc. (2021). 590 p.
18. Moorhead S, Johnson M, Maas Ml, Swanson E. Classificação dos resultados de enfermagem (NOC). Rio de Janeiro: Elsevier. (2010). 1409 p.
19. Bulechek GM, Butcher HK, Dochterman JM. Classificação das intervenções de enfermagem (NIC). 5ª ed. Rio de Janeiro: Elsevier (2010). 1037 p.
20. Galvão-Castro B, Grassi MFR, Galvão-Castro AVS, Nunes C, Dumas AS, Boa-Sorte NM, et al. A importância da realização de um atendimento integrado e multidisciplinar às pessoas vivendo com HTLV. In: Proietti ABFC, editor. Cadernos Hemominas. Belo Horizonte (2016). p. 437–50.
21. Ballantyne H. Developing nursing care plans. Nurs Stand. (2016) 30:51–7. doi: 10.7748/ns.30.26.51.s48
22. NANDA Diagnósticos de enfermagem da NANDA-I: definições e classificação 2018-2020 [recurso eletrônico] / [NANDA International]. tradução: Regina Machado Garcez; revisão técnica: Alba Lucia Bottura Leite de Barros [ et al.]. 11ª ed. Porto Alegre: Artmed (2018). 1187 p.
23. Dos Santos ACC, Soares DJ, Rivemales MCC. (Des)conhecimento, adoecimento e limitações impostas pelo HTLV: experiências de mulheres soropositivas. Cad. Saúde Colet. (2017) 25:45–50. doi: 10.1590/1414-462x201700010186
24. Nepomuceno APFA, Ribeiro CMLP, Maia GAG, Agnol PD, De Melo GCN, Ribas JGR. Aspectos da reabilitação no paciente com mielopatia associada ao HTLV-1. In: Proietti ABFC, editor. Cadernos Hemominas. 6ª ed. Belo Horizonte (2016). p. 304–17.
25. Kahl C, Meireles HS, Lanzoni GMM, Koerich C, Da Cunha KS. Ações e interações na prática clínica do enfermeiro na Atenção Primária à Saúde. Rev Esc Enferm USP. (2018) 52:03327. doi: 10.1590/s1980-220x2017025503327
26. Lago V, da Conceição CS, Pinto EBC, Costa JC, Sá KN. Center of gravity oscillations in HTLV-1-associated myelopathy/tropical spastic paraparesis. Fisioterapia em Movimento. (2020) 33:e003303. doi: 10.1590/1980-5918.033.ao03
27. Macêdo MC, Mota Rde S, Patrício NA, Santos AP, Mendes SM, Dias CM, et al. Quality of life and pain multidimensional aspects in individuals with HTLV-1. Braz J Infect Dis. (2016) 20:494–8. doi: 10.1016/j.bjid.2016.05.010
28. Martins JVP, Baptista AF, Araújo AQC. Quality of life in patients with HTL V-I associated myelopathy/tropical spastic paraparesis. Arq Neuropsiquiatr. (2012) 70:257–61. doi: 10.1590/S0004-282X2012005000006
29. Rivemales MCC. Representações sociais sobre a vivência da sexualidade em homens e mulheres soropositivas para o HTLV (tese / tese de doutorado/ PhD These). Salvador: Universidade Federal da Bahia (2013). 205 p.
30. Tanajura D, Castro N, Oliveira P, Neto A, Muniz A, Carvalho NB, et al. Neurological manifestations in HTLV-1 infected individuals without HAM/TSP: a longitudinal cohort study. Clin Infect Dis. (2015) 61:49–56. doi: 10.1093/cid/civ229
31. Santos VS, Rivemales MCC. Facilidades e dificuldades encontradas na realização do aconselhamento às pessoas que vivem com HTLV. Ciênc Cuid Saúde. (2012) 11:542–8. doi: 10.4025/cienccuidsaude.v11i3.20262
Keywords: HTLV-1, care plan, nursing, diagnostics, assistance
Citation: Aben-Athar CYUP, Sampaio EC, Pinto DS, Vallinoto ACR and Cayres Vallinoto IMV (2022) Providing a Nursing Care Plan as a Requirement for Secondary Prevention for People Living With HTLV-1. Front. Med. 9:854970. doi: 10.3389/fmed.2022.854970
Received: 14 January 2022; Accepted: 31 March 2022;
Published: 25 April 2022.
Edited by:
Juarez Antonio Simões Quaresma, Universidade do Estado do Pará, BrazilReviewed by:
Hamid Reza Jahantigh, University of Bari Aldo Moro, ItalyCopyright © 2022 Aben-Athar, Sampaio, Pinto, Vallinoto and Cayres Vallinoto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Carlos Rosário Vallinoto, dmFsbGlub3RvQHVmcGEuYnI=; Izaura Maria Vieira Cayres Vallinoto, aXZhbGxpbm90b0B1ZnBhLmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.