 Jiangbiao Xiong1
Jiangbiao Xiong1 Tian Xu
Tian Xu Ren Liu
Ren Liu Rui Wu
Rui Wu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 11 April 2022
Sec. Pathology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.847875
This article is part of the Research Topic Pathogenic Immune Cells in Autoimmune Diseases View all 4 articles
Objective: To explore risk factors for developing osteonecrosis in patients with systemic lupus erythematosus (SLE).
Methods: Twenty-six SLE patients with osteonecrosis from January 2018 to December 2019 were described. Fifty SLE patients without osteonecrosis were selected as controls from the SLE database (total 2,680) of our hospital during the same period. Clinical manifestations and laboratory tests were recorded and analyzed, especially antibodies. Univariate and multivariate analyses were used to evaluate possible associated risk factors.
Results: Twenty-six (3 male, 23 female) SLE patients with osteonecrosis were confirmed by X-ray and magnetic resonance imaging. The median course from SLE onset to osteonecrosis onset was 45 (range 2–302) months. Seven (27%) patients had a single joint involved and 19 (73%) patients had two or more joints involved. Besides, the incidence of femoral head osteonecrosis (FHON), knee ON, and humerus head ON were 85% (22/26), 27% (7/26), and 12%(3/26), respectively. The multivariate logistic regression analysis showed that the score of European Consensus Lupus Activity Measurement (ECLAM) at SLE onset [odds ratio (OR) 1.37; 95% confidence interval (CI) 1.07–1.75], a cumulative dose of prednisone above 10 g (OR 15.49; 95% CI 3.38–84.61), and positive of independent anti-RNP antibodies (OR 3.35; 95% CI 0.80–10.73) were significantly associated with osteonecrosis in SLE.
Conclusion: The score of ECLAM at SLE onset, a cumulative dose of prednisone above 10 g, and positive anti-RNP antibodies are associated with osteonecrosis in SLE. Herein, we reported for the first time that anti-RNP antibodies were associated with osteonecrosis in SLE patients and might be a novel predictor.
Osteonecrosis (ON) is usually induced by abnormal microvascular circulation which is believed to be the result of mechanical vascular interruption, intravascular occlusion, and extravascular compression (1). However, there are various reasons for ON in systemic lupus erythematosus (SLE) which leads to disability and affects the quality of life seriously in SLE patients. The first case of an SLE patient with ON (SLE-ON) was reported by Dubois and Cozen (2). But so far, the etiology and pathogenesis of ON in lupus remain unclear and treatment is challenged. It was initially recognized that glucocorticoids (GCs) are the main factor for lupus osteonecrosis (3). However, studies showed that other related risk factors, including gene susceptibility, lupus activity, vasculitis, Raynaud's phenomenon, hyperlipidemia, thrombophlebitis, and antiphospholipid antibodies (APL) also played a potential role in lupus osteonecrosis, although some results remained inconsistent (4–9). Early diagnosis and intervention are essential for improving the outcome of ON. It is necessary to screen out the possible risk factors for ON in SLE, which could help clinicians to identify susceptible individuals and provide prophylactic suggestions. To this point, we conducted a case-control study to analyze the clinical features and immunologic patterns of SLE patients with ON and explore the possible risk factors.
This was a cross-sectional case-control study that SLE patients with or without ON were recruited from the SLE database (total 2,680) of the First Affiliated Hospital of Nanchang University during the period from January 2018 to December 2020 who fulfilled the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus (10). Written informed consents were obtained from all patients. ON patients were confirmed by the X-ray and magnetic resonance imaging (MRI). Patients with ON were matched with patients without ON by age, sex, and body mass index(BMI) in a ratio of 1:2. Patients who overlapped with other connective tissue diseases were excluded. Disease activity was assessed according to the European Consensus Lupus Activity Measurement (ECLAM) (11). Anti-nuclear antibodies (ANA) were detected by indirect immunofluorescence (IIF). Anti-dsDNA antibodies, anticardiolipin antibodies (ACA), and anti-β2-glycoprotein I antibodies (β2GP1) were tested by ELISA while lupus anticoagulant (LAC) was tested by a dilute Russell's viper venom time with confirmatory studies. Euroline ANA profile (IgG) (EUROIMMUN Medizinische Labordiagnostika AG, Germany) was used to test 14 specific antibodies, including anti-nRNP /Sm antibodies, anti-Sm antibodies, anti-SSA antibodies, anti-SSB antibodies, anti-Ro-52 antibodies, anti-Scl-70 antibodies, anti-PM-SCL antibodies, anti-Jo-1 antibodies, anti-CENP-B antibodies, anti-PCNA antibodies, anti-ANuA antibodies, anti-Histone antibodies, anti-Rib-P antibodies, and AMA-M2 antibodies. Clinical features, laboratory indices, and treatment were collected and compared between the ON and the control group. The ethics committee of the First Affiliated Hospital of Nanchang University has confirmed that no ethical approval is required for this retrospective study.
SPSS 20.0 was used for analyses. Categorical data were analyzed by Chi-square test or Fisher exact test and numerical data by Student's t-test or Mann-Whitney test. A multivariate logistic stepwise regression was performed to identify factors associated with ON. A P < 0.05 was considered to indicate statistical significance.
Twenty-six SLE patients (23 female, 3 male) were diagnosed with ON from January 2018 to December 2020, and 50 SLE patients excluded from ON were enrolled. All the ON patients had no history of alcohol abuse, smoking, oral contraceptives, or trauma. The clinical and laboratory characteristics of patients with ON were summarized in Table 1. More than half of patients developed ON in 45 months from SLE onset (Figures 1–3). A higher score of ECLAM was shown in the SLE-ON group than the control group (P < 0.05). Age at SLE onset was significantly younger than the control group (P < 0.05). Nephritis was more common in the SLE-ON group than the control group (P < 0.05) while no significant difference was shown in terms of rash, arthritis, cutaneous vasculitis, and neuropsychiatric disorders. Thrombosis events happened in 2 patients with ON. No significant difference in comorbidities of hypertension, diabetes, and hyperlipidemia was observed between the SLE-ON group and the control group.
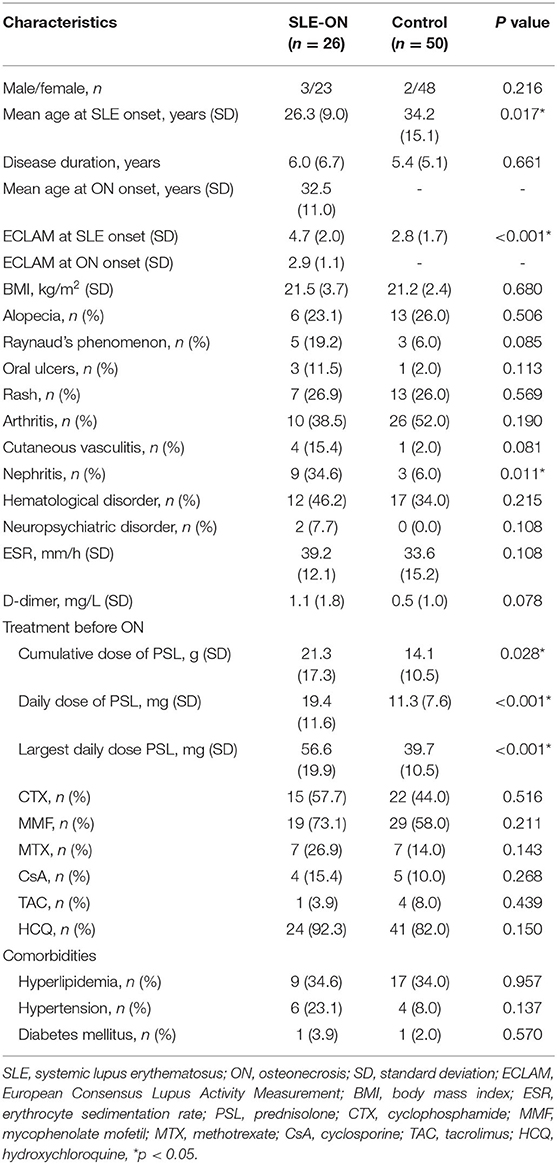
Table 1. Characteristics of patients in the SLE-ON group and control group.
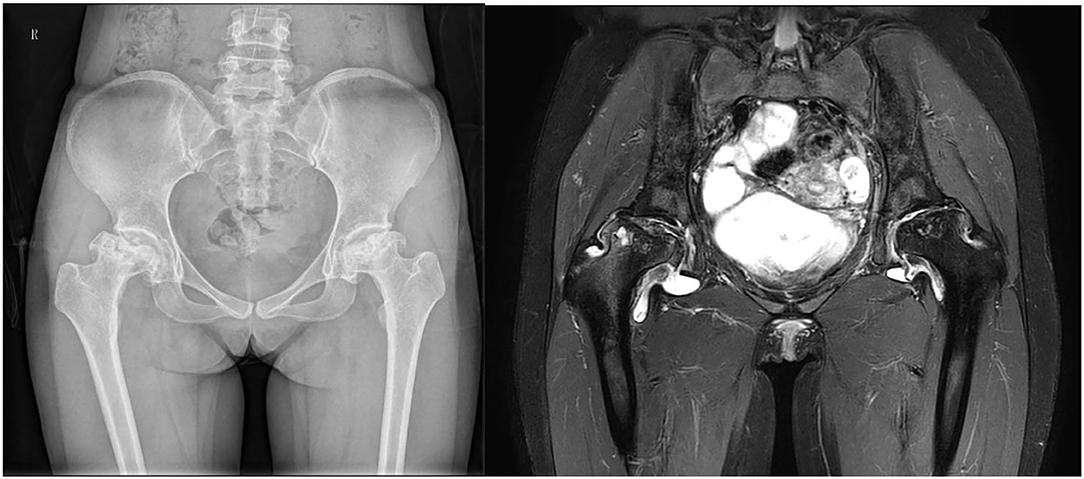
Figure 1. A 35-year-old woman with a history of SLE for 3.5 years was diagnosed with FHON.

Figure 2. A 20-year-old woman with a history of SLE for 2 years was diagnosed with humerus head ON.

Figure 3. A 48-year-old woman with a history of SLE for 7 years was diagnosed with knee ON.
A higher prednisolone dose was shown in the SLE-ON group. Seventeen (65%) patients with ON were treated with prednisolone (PSL) at a cumulative dose of more than 10 g. All the patients with ON had been treated with immunosuppressant agents (ISA), such as cyclophosphamide (CTX), methotrexate (MTX), mycophenolate mofetil (MMF), cyclosporine (CsA), tacrolimus (TAC), and hydroxychloroquine (HCQ). No significant difference in ISA administration was shown between the SLE-ON and control groups. Seven (27%) patients had a single joint involved and 19 (73%) patients had two or more joints involved. The incidence of femoral head osteonecrosis (FHON), knee ON, and humerus head ON were 85% (22/26), 27% (7/26), and 12% (3/26), respectively.
The frequency of the autoantibodies is presented in Table 2. No significant difference was found in the titer of ANA (IIF) between the SLE-ON and control group. Anti-dsDNA and other 14 specific antibodies were found insignificantly different between two groups. The frequency of independent anti-RNP antibodies (with negative anti-Sm antibodies) was significantly higher in the SLE-ON group (p = 0.014).
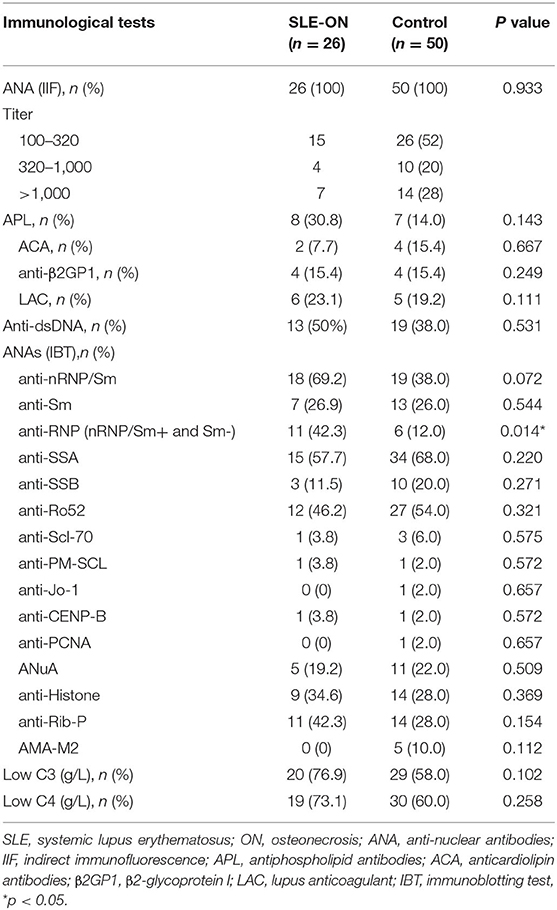
Table 2. Immunologic features in the SLE-ON group and control group.
The multivariate logistic regression analysis showed that the score of ECLAM at SLE onset [odds ratio (OR) 1.37; 95% confidence interval (CI) 1.07–1.75], a cumulative dose of PSL above 10 g (OR 15.49; 95% CI 3.38–84.61), and positive of independent anti-RNP antibodies (OR 3.35; 95% CI 0.80–10.73) had significant associations with SLE-ON (Table 3).
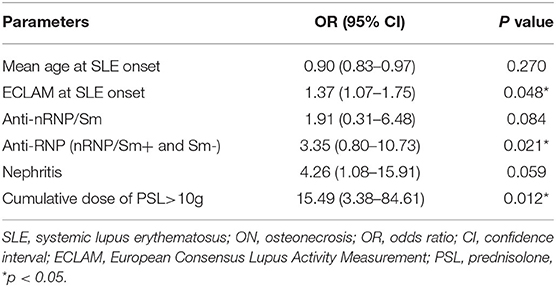
Table 3. Multivariate logistic regression analysis of parameters for ON.
Diagnosis of ON in SLE is always delayed because of insidious symptoms. Most patients show mild arthralgia without swelling and limited movement in the early stage of ON (12). In this study, the MRI of all the patients at the time of being diagnosed with ON showed they were already at or above the second stage of ON (13). Moreover, ON is more likely to occur in young patients with SLE (12, 14). As was shown in this study, the mean age of SLE onset and the mean age of ON onset of the SLE-ON group were 26.3 years and 32.5 years, respectively. Reports have estimated the prevalence of ON in SLE patients ranging from 4 to 40% (15, 16). In our two-year SLE database of 2,680 patients, only 26 (1%) patients have been diagnosed with ON, which is lower than the literature, suggesting that there may be underdiagnosis of ON in our center.
For decades, GCs have been considered as an independent predictor of ON (17–20). This study improved that point by the discovery that a cumulative dose of GCs above 10 g, an average daily dose of GCs above 20 mg, and the largest daily dose of GCs above 40 mg are risk factors for ON. In addition, the use of GCs was more likely to be correlated with FHON than other parts of ON (12). Nevertheless, studies showed that inflammation and vascular endothelial cell injuries due to SLE also contributed to the occurrence of ON (21, 22). Lupus disease activity, vasculitis, and systemic damage including nephritis have been believed to be risk factors for early ON in some reports (5, 16), which is consistent with us. APL has also been proved as a risk factor for ON in some studies (23–25). However, neither ACA nor LA showed a significant association with ON in this study, although the prevalence of positive ACA and LA were higher in the ON group.
Among autoantibodies tested in this study, only positive anti-RNP/Sm with negative anti-Sm antibodies were found significantly associated with ON, suggesting that anti-U1RNP antibodies may be an independent risk factor. The exact role of anti-RNP antibodies in the pathogenesis of autoimmune diseases remains unclear. Literature shows anti-RNP antibodies are related with manifestations of vascular disorders, for example, Raynaud's phenomenon, via affecting endothelial cells (26, 27). Therefore, the appearance of independent anti-RNP antibodies suggests that endothelial injuries play a role in the pathogenesis of ON in SLE. It is well known that the positive independent anti-RNP antibodies are strongly associated with mixed connective tissue disease (MCTD) (28). However, it is interesting to note that the incidence of ON in MCTD is not as frequent as SLE. It is reported that the IgM type of anti-U1RNP antibodies is predominantly present in SLE than MCTD (29), which reveals that the different types of anti-U1RNP antibodies may have different pathogenicities in ON.
The study has several limitations. First, the evidence is limited for the case-control design. Second, the sample size of SLE patients with ON is not large enough. In the future, a prospective study with a larger sample will be needed for the verification of these findings.
In conclusion, the score of ECLAM at SLE onset, a cumulative dose of PSL above 10 g, and positive anti-RNP antibodies are associated with ON in SLE. Herein, we reported for the first time that anti-RNP antibodies were associated with ON in SLE and might be a novel predictor.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
JX and RW: study design and drafting of manuscript. TX, RL, YW, and GW: data collection and data analysis. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank Zoe Zeng for her help with language editing.
1. Gladman DD, Chaudhry-Ahluwalia V, Ibañez D, Bogoch E, Urowitz MB. Outcomes of symptomatic osteonecrosis in 95 patients with systemic lupus erythematosus. J Rheumatol. (2001) 28:2226–9.
2. Dubois EL, Cozen L. Avascular (aseptic) bone necrosis associated with systemic lupus erythematosus. JAMA. (1960) 174:966–71. doi: 10.1001/jama.1960.03030080028005
3. Shigemura T, Nakamura J, Kishida S, Harada Y, Ohtori S, Kamikawa K, et al. Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: prospective MRI study. Rheumatology (Oxford). (2011) 50:2023–8. doi: 10.1093/rheumatology/ker277
4. Fialho SC, Bonfá E, Vitule LF, D'Amico E, Caparbo V, Gualandro S, et al. Disease activity as a major risk factor for osteonecrosis in early systemic lupus erythematosus. Lupus. (2007) 16:239–44. doi: 10.1177/0961203307076771
5. Uea-areewongsa P, Chaiamnuay S, Narongroeknawin P, Asavatanabodee P. Factors associated with osteonecrosis in Thai lupus patients: a case control study. J Clin Rheumatol. (2009) 15:345–9. doi: 10.1097/RHU.0b013e3181ba3423
6. Gladman DD, Dhillon N, Su J, Urowitz MB. Osteonecrosis in SLE: prevalence, patterns, outcomes and predictors. Lupus. (2018) 27:76–81. doi: 10.1177/0961203317711012
7. Gladman DD, Urowitz MB, Chaudhry-Ahluwalia V, Hallet DC, Cook RJ. Predictive factors for symptomatic osteonecrosis in patients with systemic lupus erythematosus. J Rheumatol. (2001) 28:761–5.
8. Sayarlioglu M, Yuzbasioglu N, Inanc M, Kamali S, Cefle A, Karaman O, et al. Risk factors for avascular bone necrosis in patients with systemic lupus erythematosus. Rheumatol Int. (2012) 32:177–82. doi: 10.1007/s00296-010-1597-9
9. Tsai HL, Chang JW, Lu JH, Liu CS. Epidemiology and risk factors for avascular necrosis in childhood systemic lupus erythematosus in a Taiwanese population. Sci Rep. (2020) 10:15563. doi: 10.1038/s41598-020-71923-w
10. Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. (2012) 64:2677–86. doi: 10.1002/art.34473
11. Vitali C, Bencivelli W, Isenberg DA, Smolen JS, Snaith ML, Sciuto M, et al. Disease activity in systemic lupus erythematosus: report of the Consensus Study Group of the European Workshop for Rheumatology Research. II Identification of the variables indicative of disease activity and their use in the development of an activity score The European Consensus Study Group for Disease Activity in SLE. Clin Exp Rheumatol. (1992) 10:541–7.
12. Gontero RP, Bedoya ME, Benavente E, Roverano SG, Paira SO. Osteonecrosis in systemic lupus erythematosus. Reumatol Clin. (2015) 11:151–5. doi: 10.1016/j.reuma.2014.05.005
13. Sugano N, Atsumi T, Ohzono K, Kubo T, Hotokebuchi T, Takaoka K. The 2001 revised criteria for diagnosis, classification, and staging of idiopathic osteonecrosis of the femoral head. J Orthop Sci. (2002) 7:601–5. doi: 10.1007/s007760200108
14. Kuroda T, Tanabe N, Wakamatsu A, Takai C, Sato H, Nakatsue T, et al. High triglyceride is a risk factor for silent osteonecrosis of the femoral head in systemic lupus erythematosus. Clin Rheumatol. (2015) 34:2071–7. doi: 10.1007/s10067-015-3075-y
15. Abu-Shakra M, Buskila Y. D, Shoenfeld Osteonecrosis in patients with SLE. Clin Rev Allergy Immunol. (2003) 25:13–24. doi: 10.1385/CRIAI:25:1:13
16. Prasad R, Ibanez D, Gladman D, Urowitz M. The role of non-corticosteroid related factors in osteonecrosis (ON) in systemic lupus erythematosus: a nested case-control study of inception patients. Lupus. (2007) 16:157–62. doi: 10.1177/0961203306075771
17. Mont MA, Pivec R, Banerjee S, Issa K, Elmallah RK, Jones LC. High-Dose Corticosteroid Use and Risk of Hip Osteonecrosis: Meta-Analysis and Systematic Literature Review. J Arthroplasty. (2015) 30:1506–12.e5. doi: 10.1016/j.arth.2015.03.036
18. Kallas R, Li J, Petri M. Predictors of osteonecrosis in systemic lupus erythematosus: A prospective cohort study. Arthritis Care Res (Hoboken). (2020). doi: 10.1002/acr.24541
19. Hussein S, Suitner M, Béland-Bonenfant S, Baril-Dionne A, Vandermeer B, Santesso N, et al. Monitoring of Osteonecrosis in Systemic Lupus Erythematosus: a systematic review and metaanalysis. J Rheumatol. (2018) 45:1462–76. doi: 10.3899/jrheum.170837
20. Zhao L, Wu X, Wu H, Su J, Zhang W, Zhao Y, et al. Symptomatic knee osteonecrosis in patients with systemic lupus erythematosus: a case-control study. Rheumatol Int. (2016) 36:1105–11. doi: 10.1007/s00296-016-3502-7
21. Zhang Q, L VJ, Jin L. Role of coagulopathy in glucocorticoid-induced osteonecrosis of the femoral head. J Int Med Res. (2018) 46:2141–8. doi: 10.1177/0300060517700299
22. Yu H, Yue J, Wang W, Liu P, Zuo W, Guo W, et al. Icariin promotes angiogenesis in glucocorticoid-induced osteonecrosis of femoral heads: In vitro and in vivo studies. J Cell Mol Med. (2019) 23:7320–30. doi: 10.1111/jcmm.14589
23. Asherson RA, Lioté F, Page B, Meyer O, Buchanan N, Khamashta MA, et al. Avascular necrosis of bone and antiphospholipid antibodies in systemic lupus erythematosus. J Rheumatol. (1993) 20:284–8.
24. Nevskaya T, Gamble MP, Pope JE. A meta-analysis of avascular necrosis in systemic lupus erythematosus: prevalence and risk factors. Clin Exp Rheumatol. (2017) 35:700–10.
25. Mok CC, Lau CS, Wong RW. Risk factors for avascular bone necrosis in systemic lupus erythematosus. Br J Rheumatol. (1998) 37:895–900. doi: 10.1093/rheumatology/37.8.895
26. Okawa-Takatsuji M, Aotsuka S, Uwatoko S, Takaono M, Iwasaki K, Kinoshita M, et al. Endothelial cell-binding activity of anti-U1-ribonucleoprotein antibodies in patients with connective tissue diseases. Clin Exp Immunol. (2001) 126:345–54. doi: 10.1046/j.1365-2249.2001.01669.x
27. Wesner N, Uruha A, Suzuki S, Mariampillai K, Granger B, Champtiaux N, et al. Anti-RNP antibodies delineate a subgroup of myositis: A systematic retrospective study on 46 patients. Autoimmun Rev. (2020) 19:102465. doi: 10.1016/j.autrev.2020.102465
28. Ahsan T, Erum U, Dahani A, Khowaja D. Clinical and immunological profile in patients with mixed connective tissue disease. J Pak Med Assoc. (2018) 68:959–62.
Keywords: systemic lupus erythematosus, osteonecrosis, risk factor, autoantibodies, anti-RNP antibody
Citation: Xiong J, Wang G, Xu T, Liu R, Yu S, Wang Y and Wu R (2022) Anti-RNP Antibody: A Potential Novel Predictor for Osteonecrosis in Systemic Lupus Erythematosus. Front. Med. 9:847875. doi: 10.3389/fmed.2022.847875
Received: 03 January 2022; Accepted: 23 March 2022;
Published: 11 April 2022.
Edited by:
Jie Zhang, Cleveland Clinic, United StatesReviewed by:
Lidan Zhao, Peking Union Medical College Hospital (CAMS), ChinaCopyright © 2022 Xiong, Wang, Xu, Liu, Yu, Wang and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rui Wu, dGNtY2xpbmljQDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.