 Vincy Chan
Vincy Chan Maria Jennifer Estrella
Maria Jennifer Estrella Jessica Babineau
Jessica Babineau Angela Colantonio
Angela Colantonio
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Med. , 22 July 2022
Sec. Regulatory Science
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.815660
Background: When used optimally, clinical practice guidelines (CPGs) can reduce inappropriate variations in practice, improve application of research to practice, and enhance the quality of healthcare. However, a common criticism, despite its potential, is the lack of consideration for equity and disadvantaged populations.
Objectives: This protocol is for a systematic review of CPGs for traumatic brain injury (TBI) and homelessness that aims to assess (1) the extent to which evidence regarding TBI and homelessness is integrated in CPGs for homelessness and TBI, respectively, and (2) equity considerations in CPGs for TBI and homelessness.
Methods and analysis: The methodology for this review is guided by the PRISMA-P, validated search filters for CPGs, and methodological guides to searching systematic reviews and gray literature. CPGs will be identified from (a) databases for peer-reviewed literature (MEDLINE, Embase, CINAHL, and PsycInfo), (b) targeted websites and Google Search for gray literature, and (c) reference lists of peer-reviewed and gray literature that meet the eligibility criteria. Searching for gray literature, including from guideline-specific resources, is a critical component of this review and is considered an efficient approach to identifying CPGs, given the low precision of searching peer-reviewed databases. Two independent reviewers will screen all articles based on pre-determined eligibility criteria. A narrative synthesis will be conducted to identify the proportion of CPGs that integrate evidence about TBI and homelessness and how TBI and homelessness is or is not integrated in CPGs. Quality appraisal will take the form of an equity assessment of CPGs and will be completed independently by two reviewers.
Conclusion: This protocol outlines the methodology for a systematic review of CPGs for TBI and homelessness. The resulting systematic review from this protocol will form an evidence-based foundation to advance CPGs for individuals with lived experience of TBI and homelessness.
Systematic review registration: identifier: CRD42021287696.
Traumatic brain injury (TBI) research has gained momentum in recent years, owing to the condition being a growing public health concern (1–3). Defined as “an alteration in brain function or other evidence of brain pathology caused by an external force,” (4) TBI remains a leading cause of death and disability among all trauma-related injuries, across all ages and in all countries (5, 6). The consequences of TBI, regardless of severity, are long-lasting, leaving survivors of TBI with significant physical, emotional, and cognitive disabilities (7, 8) and costing the international economy an estimated US$400 billion annually (9). The immense global challenge caused by TBI has led to research efforts to increase understanding about TBI, reduce its burden, and improve the quality of life of, and healthcare for, survivors of TBI (9).
The development and dissemination of clinical practice guidelines (CPGs) is a known method of translating research findings to practice, including in the field of TBI (10–12). CPGs are “statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options” (13). When used optimally, CPGs can reduce inappropriate variations in practice, improve application of research to practice, and enhance quality and safety of healthcare (13); however, CPGs are often criticized for focusing on effectiveness and cost-effectiveness of treatment (14). Another criticism is the lack of consideration for equity (14–16) [i.e., the fair distribution and access to resources and opportunities (17)] and health inequities or “differences in health that are not only unnecessary and avoidable, but in addition, are considered unfair and unjust” (18). In effect, CPG interventions and recommendations may not always be available, cost-effective, or beneficial for all population groups, specifically disadvantaged groups who experience substantial health inequities (15). We acknowledge the possible stigma that accompanies the term disadvantaged, marginalized, or underserved (19). This paper will use the term “disadvantaged group” to capture the lack of fair opportunities that put these individuals in a disadvantaged position (18) and to remain consistent with the language used by the GRADE Working Group (14, 19).
One such disadvantaged group is individuals with lived experience of homelessness (20, 21), where TBI has been found to be disproportionately prevalent (22). Individuals experiencing homelessness suffer significant health inequities that are exacerbated by social determinants of health (e.g., poverty, adverse experiences and trauma, lack of education, unemployment, domestic violence, and social disconnection) (20, 21). Such health inequities include poorer mental and physical health, higher morbidity and mortality, greater use of acute hospital services, and reduced likelihood of accessing primary and preventive health services (21). The latter subsequently leads to delayed diagnoses, poor control of health conditions, and hospitalization for preventable conditions (21). These health inequities speak to the need to view homelessness as both a medical and a social issue (21), and for CPGs to integrate evidence regarding homelessness into recommendations to not only manage adverse outcomes associated with TBI but also take into account the differences in injury experience and needs of individuals experiencing homelessness. Failure to integrate research findings that may illuminate the inequities experienced by this disadvantaged group could lead to lack of prioritization for their needs and misallocation of resources, overestimation or underestimation of treatment effectiveness, lack of consideration for specific outcomes that are perceived valuable, and continued barriers to accessing care (14).
In recognizing the role of guidelines in promoting health equity, the GRADE Working Group published the GRADE Equity Guidelines Series to guide efforts to incorporate considerations regarding health equity in developing and evaluating CPGs (19, 23–25). Unfortunately, most studies included in CPGs for TBI are population-based and fail to consider the diversity in patient characteristics, thereby promoting a one-size-fits-all approach to care (9).
This protocol outlines the methodology for a systematic review of CPGs for TBI and homelessness. Through conducting a preliminary search, we found that clinical guidelines for homelessness have also been developed to provide recommendations for all individuals experiencing homelessness. As such, the primary objective is to assess the extent to which evidence about homelessness is integrated in CPGs for TBI and the extent to which evidence about TBI is integrated in CPGs for homelessness. The secondary objective of the systematic review is to assess equity considerations in CPGs for TBI and homelessness. Findings from the systematic review will provide an evidence-based foundation to advance CPGs for individuals with lived experience of TBI and homelessness.
This protocol is guided by the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Protocols (PRISMA-P) (26) and a methodological guide to systematic review of CPGs (27). The reporting of the systematic review search strategy will follow the PRISMA extension for searching (PRISMA-S) (28) and the reporting of the systematic review will follow the PRISMA Equity Extension (29). This protocol is registered on PROSPERO (CRD42021287696).
We will search the following for CPGs: (a) databases for peer-reviewed literature, (b) targeted websites and Google Search for gray literature, and (c) reference lists of peer-reviewed and gray literature that meet the inclusion criteria.
The development of the search strategy for databases was informed by (a) a validated search for retrieving CPGs from MD Anderson Cancer Centre Library (MDACCL) (30) and (b) search strategies of scoping or systematic reviews of CPGs, TBI, and/or homelessness (11, 12, 31–33). Three concepts, (A) CPG, (B) TBI, and (C) homelessness, were developed to form the final search structure, (A+B) OR (A+C), that will be used to search each database. No date or language limits will be placed on the search strategies, however, where possible, we will exclude animal studies and conference abstracts. Supplementary Material 1 presents the search strategy that was developed for the MEDLINE® ALL (in Ovid, including Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE® Daily) database, which will be translated to Embase and Embase Classic (Ovid), CINAHL (EBSCO), and APA PsycInfo (Ovid). This search strategy was developed with an Information Specialist (JB) and team members with research and subject-matter expertise relevant to TBI and homelessness (VC, MJE, AC).
The search strategy for gray literature was informed by Goldin et al.'s methodology on applying systematic review search methods to gray literature (34). Gray literature for this systematic review is defined as CPGs that are identified outside of the peer-reviewed literature. They will be identified by searching targeted websites and Google Search.
Targeted websites include those from guideline development organizations and CPG databases/repositories, health technology assessment agencies, medical or allied health professional associations, and brain injury and housing organizations. Gray Matters: A Practical Tool for Searching Health-Related Gray Literature developed by the Canadian Agency for Drugs and Technologies in Health (CADTH; hereafter referred to as “Gray Matters”) (35) will be used to identify targeted websites. Additional websites not captured by Gray Matters will be identified by the research team (VC, MJE, JB, AC) and through consultation with stakeholders of the systematic review, which include front-line staff and service providers in the housing and brain injury sectors; health professionals who provide care for individuals with TBI and/or lived experience of homelessness; and researchers who conduct research and develop guidelines on TBI and homelessness. Google Search will also be used to identify additional relevant websites and gray literature.
The targeted websites will be searched by entering keywords for concept (A) CPGs, (B) TBI, and (C) homelessness in the search bar. Websites without a search bar will be manually reviewed for relevant gray literature. Supplementary Material 2 presents the keywords that will be used to develop the search strategies for each targeted website and Google Search, applying the search functionalities of the websites. The search structure for peer-reviewed literature will also be applied to the gray literature search: (A+B) OR (A+C). Supplementary Material 3 presents targeted websites identified by the research team that are not captured by Gray Matters and will be expanded upon consultation with stakeholders.
Reference lists of scoping and systematic reviews and CPGs identified from the databases and the gray literature search will be manually reviewed.
Only CPGs for TBI or CPGs for homelessness will be included and they must meet the eligibility criteria outlined in the PICAR Statement (27) presented in Table 1. The PICAR Statement for systematic review of CPGs is adapted from the PICO statement for systematic review of interventions (27).
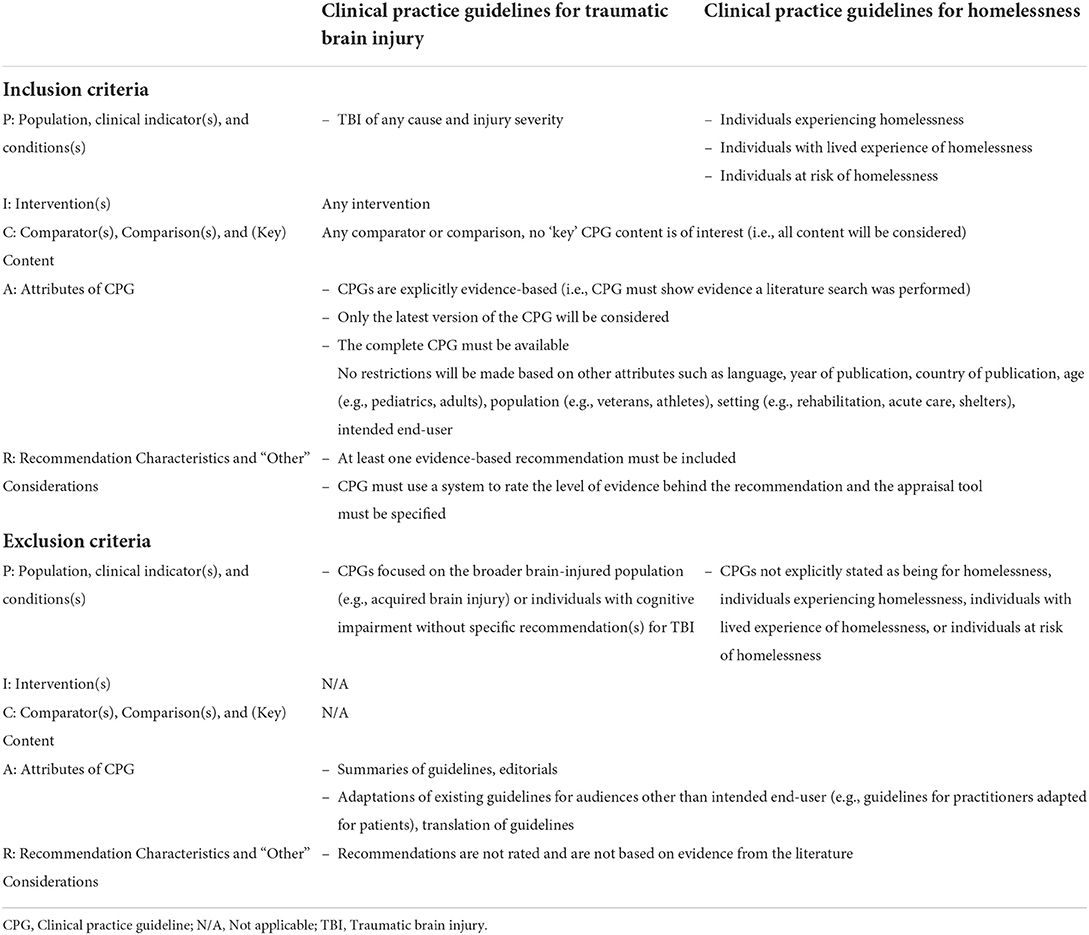
Table 1. PICAR statement for eligibility criteria.
EndNote X8 (36) will be used for reference management and Covidence (37) will be used for de-duplication and study selection. Two independent reviewers will screen all articles retrieved from the search strategy based on the above eligibility criteria. At the title and abstract screen, articles that focus on (a) the broader brain-injured population without specific mention of TBI or (b) housing without specific mention of homelessness will also be considered for full-text review to confirm that the guidelines focus on the TBI population or on homelessness. Scoping and systematic reviews of CPGs for TBI or homelessness will also be included in the title and abstract screen and their reference lists will be manually searched to identify additional CPGs not retrieved using the above search strategy. Any additional guidelines retrieved will be subject to the above inclusion and exclusion criteria.
Prior to formal title and abstract screening, a pilot screen of 20 articles will be conducted until a minimum of 80% agreement using the kappa statistic is achieved between the two reviewers. Similarly, prior to formal full-text screening, a pilot of 10% of full-text articles will be conducted until a minimum 80% agreement is achieved between the two reviewers. Non-English language abstracts will be assessed using the English full-text translation, DeepL Translate, Google Translate, or reviewers with knowledge of the language. Any discrepancies will be resolved by consensus or consultation with a third reviewer. The PRISMA flow chart (38) will be completed to illustrate the study selection process, including the number of English and non-English articles retrieved and included in the review.
Two independent reviewers will review the Gray Matters checklist and the first ten pages of Google Search results to identify potentially relevant websites using the title and/or short text underneath the title. The reviewers will then document the name and link to each website/organization and the date the website/organization was identified in an Excel file to develop a list of unique targeted websites for searching. These websites will be searched by two independent reviewers for potentially relevant CPGs using the search strategy outlined in Supplementary Material 2. The date on which each website was searched and the authors, titles, and links of the potentially relevant CPGs will be documented in the Excel file to generate a list of unique articles to review. This list will be compared to CPGs identified through the search for peer-reviewed literature and duplicates will be removed prior to screening.
Two independent reviewers will screen all articles retrieved from the targeted websites based on the eligibility criteria outlined in Table 1. At the title and abstract screen, the executive summaries and/or table of contents will be reviewed if an abstract is not available. Similar to the study selection of peer-reviewed literature, CPGs that focus on (a) the broader brain-injured population without specific mention of TBI or (b) housing without specific mention of homelessness will also be considered for full-text review to confirm that the guidelines focus on the TBI population or on homelessness. All decisions will be documented in an Excel file and a numeric code will be assigned to each article: 1 = include or maybe (i.e., it is unclear whether it meets eligibility criteria) and 0 = exclude. The screening of full-text articles will also be documented in an Excel file using the numeric code of 1 = include and 0 = exclude. The reason for excluding any full-text articles will also be documented in the Excel file. Supplementary Material 4 presents the Excel file that will be used to document the study selection process for gray literature; this file may be adapted during the systematic review.
As with the study selection process for peer-reviewed literature, a pilot screen of 20 CPGs will be conducted at the title and abstract screen and 10% of full-texts will be conducted until a minimum 80% agreement is achieved between the two reviewers. Any discrepancies will be resolved by consensus or consultation with a third reviewer. Similar to the selection process for peer-reviewed literature, non-English language reports will be assessed using any available English translations, DeepL Translate, Google Translate, or reviewers with knowledge of the language. The study selection process for gray literature will be added to the PRISMA flow chart that will be generated for peer-reviewed literature (38), including the number of English and non-English reports identified and included in the review. References will be added to EndNote X8 (36) for reference management.
The data extraction and synthesis plan presented in this protocol was adapted from Tannenbaum et al. (39), who examined sex and gender considerations in Canadian CPGs. First, the text and reference lists of the CPGs will be searched for (a) keywords describing TBI and homelessness that are consistent with the search strategy for peer-reviewed literature and gray literature and (b) content consistent with the definitions of TBI and homelessness, both displayed in Table 2. This will enable us to categorize the guidelines into (a) text-positive or (b) text-negative.
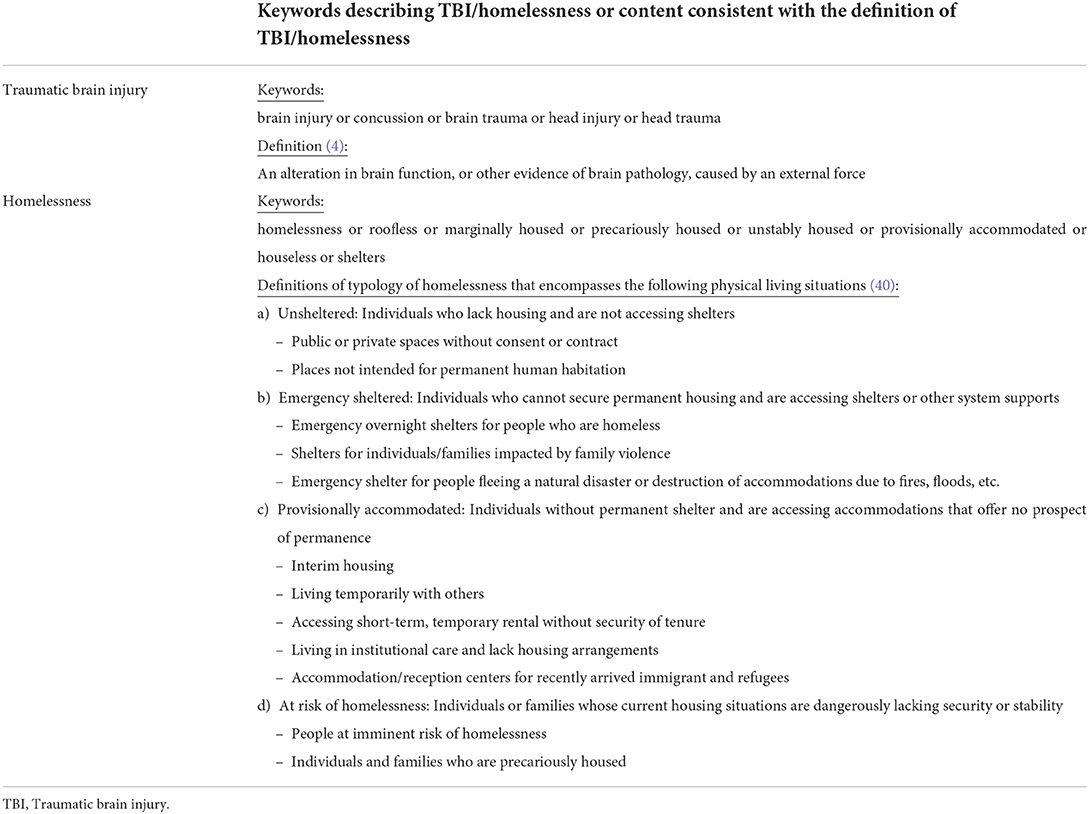
Table 2. Keywords and definitions for traumatic brain injury and homelessness.
Text-positive CPGs for TBI are those that contain at least one of the keywords for or content consistent with homelessness in the text (i.e., body) of the guidelines. Similarly, text-positive CPGs for homelessness are those that contain at least one of the keywords for or content consistent with TBI in text of the guidelines. Text-negative CPGs for TBI are those that do not include any of the keywords for or content consistent with homelessness in the body of the guidelines, while text-negative CPGs for homelessness are those that do not include any of the keywords for or content consistent with TBI in the body of the guidelines.
Text-positive and text-negative guidelines will be synthesized separately. Text-positive TBI CPGs will be categorized into one of the following categories: (1) guideline specifically recommends evidence-based diagnostic, management, or treatment approaches for individuals experiencing homelessness or with lived experience of homelessness; (2) guideline acknowledges or makes reference to data (e.g., epidemiologic, risk factors, outcome) regarding individuals experiencing homelessness or with lived experience of homelessness only, without recommendations; or (3) guideline mentions individuals experiencing homelessness or with lived experience of homelessness without context related to the literature or recommendations. Text-positive CPGs for homelessness will be categorized into one of the following categories: (1) guideline specifically recommends evidence-based diagnostic, management, or treatment approaches for individuals with TBI; (2) guideline acknowledges or makes reference to data (e.g., epidemiologic, risk factors, outcome) regarding individuals with TBI only, without recommendations; or (3) guideline mentions individuals with TBI without context related to the literature or recommendations. Data (i.e., quotes) that are used to categorize the guidelines will be extracted.
Text-negative TBI CPGs will be categorized into one of two categories: (1) reference lists contain articles that include keywords for homelessness but the text of the guideline does not contain any keywords for or content consistent with the definition of homelessness or (2) no article in the reference list includes keywords for homelessness. Text-negative CPGs for homelessness will be categorized into one of two categories: (1) reference lists contain articles that include keywords for TBI but the text of the guideline did not contain any keywords for or content consistent with the definition of TBI or (2) no article in the reference list includes keywords for TBI. Data (i.e., the reference) that are used to categorize the guideline into category one will be extracted.
Two independent reviewers will complete the data extraction and synthesis. Similar to the study selection process, a pilot extraction and synthesis of 10% of guidelines will be conducted until a minimum 80% agreement using the kappa statistic is achieved between the two reviewers. Discrepancies will be resolved through consensus or consultation with a third reviewer.
A narrative synthesis will be conducted, informed by tools and techniques in the Guidance on the Conduct of Narrative Synthesis in Systematic Reviews (41):
1. Groupings and clusters: In addition to categorizing the text-positive and text-negative guidelines into the groups above, the guidelines will also be grouped by other characteristics, with the number and types of groupings to be refined during data synthesis. Some groupings that will be explored include (a) the type of guideline—TBI vs. homelessness, (b) country the guideline was developed, (c) year of publication, (d) focus of the guideline—e.g., early management, rehabilitation, etc., (e) population the guideline was developed for—e.g., pediatrics vs. adults, (f) target audience (e.g., clinicians, allied health professionals, schools).
2. Tabulation: The number of guidelines in each of the groups will be identified, with the primary outcomes of interest being the proportion of text-positive guidelines for TBI (i.e., the number guidelines for TBI that were text-positive divided by the total number of guidelines for TBI included in the review) and homelessness (i.e., the number guidelines for homelessness that were text-positive divided by the total number of guidelines for homelessness included in the review).
3. Qualitative analysis: Content analysis of text-positive and text-negative guidelines (42) will be conducted to address a secondary outcome of this review, which is to understand how homelessness is or is not integrated in CPGs for TBI, and how TBI is or is not integrated in CPGs for homelessness. This analytical method is appropriate, as it allows both quantification and categorization of data (41).
Quality appraisal will take the form of an equity assessment of CPGs. The equity lens from Dans et al. (14) and the equity extension from the GRADE working group will be used to assess equity in the CPGs identified in the systematic review (19, 23–25). Table 3 presents the five criteria proposed by Dans et al. to evaluate how well CPGs address equity (14) and the considerations for equity in the GRADE methodology for developing clinical, public health, and health system guidelines (hereafter referred to as the “GRADE Equity Guideline”) from the GRADE working group (23). Any technical, methodological, or supporting documents associated with the CPGs included in the review will be retrieved to better inform the quality appraisal process (27). Quality appraisal will be completed by two independent reviewers, with a pilot assessment of 10% of guidelines until a minimum 80% agreement using the kappa statistic is achieved between the two reviewers. Discrepancies will be resolved through consensus or consultation with a third reviewer.
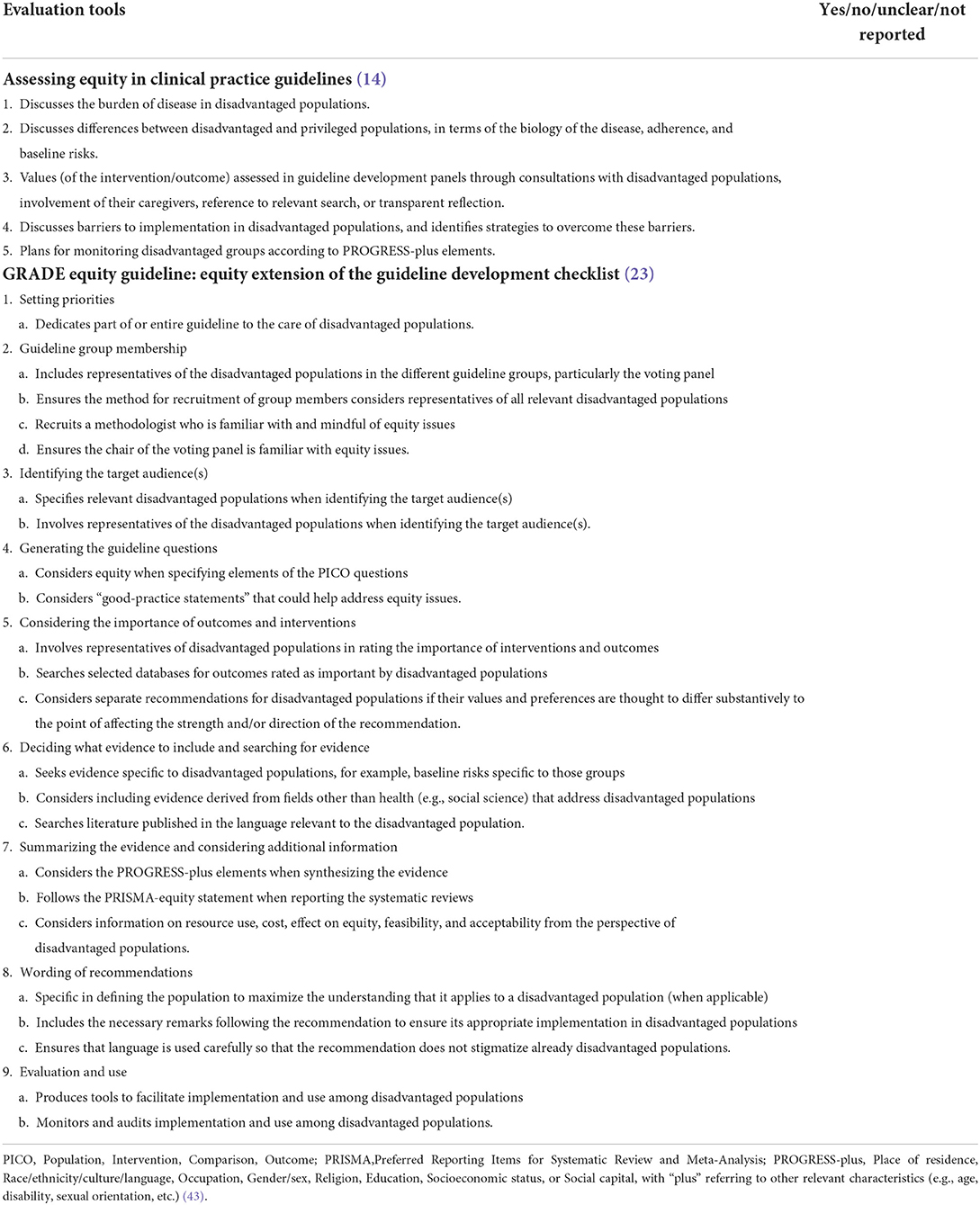
Table 3. Quality appraisal checklist to assess equity in clinical practice guidelines.
Results of the quality appraisal will complement findings from the review and will be integrated in the analysis. As such, no CPG will be excluded from this review based on the quality appraisal. We believe this is an appropriate quality appraisal compared to more traditional assessments tools for CPGs, such as the Appraisal of Guidelines for Research and Evaluation (AGREE) Instrument, as the focus of the systematic review is to assess the extent to which evidence regarding homelessness is integrated in TBI CPGs and the extent to which TBI is integrated in CPGs for homelessness. It also directly addresses the secondary aim of assessing equity considerations in CPGs.
This protocol outlines the methodology for a systematic review of CPGs for TBI and homelessness. It is guided by the PRISMA-P (26), validated search filters for CPGs (30), and methodological guides to systematic reviews (27) and gray literature searching (34). In particular, this protocol outlines a transparent, rigorous, and systematic search strategy to identify gray literature to increase replicability. Searching for gray literature, including from guideline-specific resources, is a critical component of this review and is considered an efficient approach to identifying CPGs, given the low precision of searching databases for peer-reviewed CPGs (30).
However, we acknowledge limitations of this protocol. First, this systematic review will determine if and how CPGs for TBI and homelessness consider homelessness and TBI, respectively; it will not systematically search for and review available research evidence on TBI and homelessness. As such, a separate systematic review of evidence on homelessness and TBI is encouraged to identify missed opportunities to integrate evidence regarding homelessness into CPGs for TBI and evidence regarding TBI into CPGs for homelessness. Furthermore, we recognize the risk of publication bias, as only publicly available CPGs will be included in the review. It is plausible that organizations may develop evidence-based CPGs that are not publicly available and these will be missed, unless identified through the gray literature search. Furthermore, while we will not place any restrictions on the language, year, and country of the CPGs, we recognize that non-English language CPGs may still be missed in this review. Finally, we acknowledge that the quality appraisal tool selected for the systematic review will not assess the methodological rigor of the CPGs. However, we believe the quality appraisal selected for this study is appropriate as it directly addresses the aims of this review.
Despite these limitations, the systematic review that will be produced from this protocol is a critical first step to addressing care for individuals with lived experience of homelessness and TBI. Assessing the extent to which evidence about homelessness is integrated in CPGs for TBI and the extent to which evidence about TBI is integrated in CPGs for homelessness, along with equity considerations in CPGs for TBI and homelessness, will form an evidence-based foundation to advance CPGs for individuals with lived experience of TBI and homelessness.
Research Ethics Board approvals are not required for the systematic review as only publicly available data will be analyzed. Findings will be disseminated in the form of a peer-reviewed publication and presentations at scientific conferences and to stakeholders of this research.
VC and AC conceptualized the study. VC, MJE, and JB developed the search strategy. VC formulated the design. VC and MJE drafted the manuscript. All authors critically reviewed the manuscript and approved the final manuscript.
This work has been supported in part by the Canada Research Chairs Program (Fund Number N/A) and the Ontario Ministry of Health and Long-Term Care, Ministry Grant #725A.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The views expressed in the publication are the views of the authors and do not necessarily reflect those of the Ministry of Health and Long-Term Care.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.815660/full#supplementary-material
1. Sandsmark DK, Diaz-Arrastia R. Advances in traumatic brain injury research in 2020. Lancet Neurol. (2021) 20:5–7. doi: 10.1016/S1474-4422(20)30455-5
2. Tabish SA, Syed N. Recent advances and future trends in traumatic brain injury. J Emerg Med. (2014) 4:1–22. doi: 10.4172/2165-7548.1000229
3. Khellaf A, Khan DZ, Helmy A. Recent advances in traumatic brain injury. J Neurol. (2019) 266:2878–89. doi: 10.1007/s00415-019-09541-4
4. Menon DK, Schwab K, Wright DW, Maas AI. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. (2010) 91:1637–40. doi: 10.1016/j.apmr.2010.05.017
5. Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC, Punchak M, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. (2018) 130:1080–97. doi: 10.3171/2017.10.jns17352
6. Rubiano AM, Carney N, Chesnut R, Puyana JC. Global neurotrauma research challenges and opportunities. Nature. (2015) 527:S193–7. doi: 10.1038/nature16035
7. Bramlett HM, Dietrich WD. Long-term consequences of traumatic brain injury: current status of potential mechanisms of injury and neurological outcomes. J Neurotrauma. (2015) 32:1834–48. doi: 10.1089/neu.2014.3352
8. Konrad C, Geburek AJ, Rist F, Blumenroth H, Fischer B, Husstedt I, et al. Long-term cognitive and emotional consequences of mild traumatic brain injury. Psychol Med. (2011) 41:1197–211. doi: 10.1017/S0033291710001728
9. Maas AIR, Menon DK, Adelson PD, Andelic N, Bell MJ, Belli A, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. (2017) 16:987–1048. doi: 10.1016/S1474-4422(17)30371-X
10. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients' care. Lancet. (2003) 362:1225–30. doi: 10.1016/S0140-6736(03)14546-1
11. Di B-s, Wei M, Ma W-j, Zhang Q, Lu A-q, Wang H, et al. A critical review to traumatic brain injury clinical practice guidelines. Medicine. (2019) 98:e14592. doi: 10.1097/MD.0000000000014592
12. Patel A, Vieira MM, Abraham J, Reid N, Tran T, Tomecsek K, et al. Quality of the development of traumatic brain injury clinical practice guidelines: a systematic review. PLoS ONE. (2016) 11:e0161554. doi: 10.1371/journal.pone.0161554
13. Institute of Medicine. Clinical Practice Guidelines We Can Trust. Washington, DC: National Academies Press (2011).
14. Dans AM, Dans L, Oxman AD, Robinson V, Acuin J, Tugwell P, et al. Assessing equity in clinical practice guidelines. J Clin Epidemiol. (2007) 60:540–6. doi: 10.1016/j.jclinepi.2006.10.008
15. Eslava-Schmalbach J, Mosquera P, Alzate JP, Pottie K, Welch V, Akl EA, et al. Considering health equity when moving from evidence-based guideline recommendations to implementation: a case study from an upper-middle income country on the GRADE approach. Health Policy Plan. (2017) 32:1484–90. doi: 10.1093/heapol/czx126
16. Mizen LAM, Macfie ML, Findlay L, Cooper S-A, Melville CA. Clinical guidelines contribute to the health inequities experienced by individuals with intellectual disabilities. Implement Sci. (2012) 7:42. doi: 10.1186/1748-5908-7-42
17. National Collaborating Centre for Determinants of Health. Let's Talk: Health Equity. Antigonish, NS: National Collaborating Centre for Determinants of Health, St. Francis Xavier University (2013).
18. Whitehead M. The concepts and principles of equity and health. Int J Health Serv. (1992) 22:429–45. doi: 10.2190/986L-LHQ6-2VTE-YRRN
19. Welch VA, Akl EA, Guyatt G, Pottie K, Eslava-Schmalbach J, Ansari MT, et al. GRADE equity guidelines 1: considering health equity in GRADE guideline development: introduction and rationale. J Clin Epidemiol. (2017) 90:59–67. doi: 10.1016/j.jclinepi.2017.01.014
20. Bowen E, Savino R, Irish A. Homelessness and health disparities: a health equity lens. In: Larkin H, Aykanian A, Streeter CL, editors. Homelessness Prevention and Intervention in Social Work: Policies, Programs, and Practices. Cham: Springer International Publishing (2019). p. 57–83.
21. Stafford A, Wood L. Tackling health disparities for people who are homeless? Start with social determinants. Int J Environ Res Public Health. (2017) 14:1535. doi: 10.3390/ijerph14121535
22. Stubbs JL, Thornton AE, Sevick JM, Silverberg ND, Barr AM, Honer WG, et al. Traumatic brain injury in homeless and marginally housed individuals: a systematic review and meta-analysis. Lancet Public Health. (2020) 5:e19–32. doi: 10.1016/S2468-2667(19)30188-4
23. Akl EA, Welch V, Pottie K, Eslava-Schmalbach J, Darzi A, Sola I, et al. GRADE equity guidelines 2: considering health equity in GRADE guideline development: equity extension of the guideline development checklist. J Clin Epidemiol. (2017) 90:68–75. doi: 10.1016/j.jclinepi.2017.01.017
24. Welch VA, Akl EA, Pottie K, Ansari MT, Briel M, Christensen R, et al. GRADE equity guidelines 3: considering health equity in GRADE guideline development: rating the certainty of synthesized evidence. J Clin Epidemiol. (2017) 90:76–83. doi: 10.1016/j.jclinepi.2017.01.015
25. Pottie K, Welch V, Morton R, Akl EA, Eslava-Schmalbach JH, Katikireddi V, et al. GRADE equity guidelines 4: considering health equity in GRADE guideline development: evidence to decision process. J Clin Epidemiol. (2017) 90:84–91. doi: 10.1016/j.jclinepi.2017.08.001
26. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
27. Johnston A, Kelly SE, Hsieh SC, Skidmore B, Wells GA. Systematic reviews of clinical practice guidelines: a methodological guide. J Clin Epidemiol. (2019) 108:64–76. doi: 10.1016/j.jclinepi.2018.11.030
28. Rethlefsen ML, Kirtley S, Waffenschmidt S, Ayala AP, Moher D, Page MJ, et al. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst Rev. (2021) 10:39. doi: 10.1186/s13643-020-01542-z
29. Welch V, Petticrew M, Petkovic J, Moher D, Waters E, White H, et al. Extending the PRISMA statement to equity-focused systematic reviews (PRISMA-E 2012): explanation and elaboration. Int J Equity Health. (2015) 14:92. doi: 10.1186/s12939-015-0219-2
30. Lunny C, Salzwedel DM, Liu T, Ramasubbu C, Gerrish S, Puil L, et al. Validation of five search filters for retrieval of clinical practice guidelines produced low precision. J Clin Epidemiol. (2020) 117:109–16. doi: 10.1016/j.jclinepi.2019.09.022
31. Pottie K, Kendall CE, Aubry T, Magwood O, Andermann A, Salvalaggio G, et al. Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. Can Med Assoc J. (2020) 192:E240. doi: 10.1503/cmaj.190777
32. Chan V, Estrella MJ, Babineau J, Colantonio A. Protocol for a scoping review on rehabilitation among individuals who experience homelessness and traumatic brain injury. BMJ Open. (2021) 11:e052942. doi: 10.1136/bmjopen-2021-052942
33. Jolliffe L, Lannin NA, Cadilhac DA, Hoffmann T. Systematic review of clinical practice guidelines to identify recommendations for rehabilitation after stroke and other acquired brain injuries. BMJ Open. (2018) 8:e018791. doi: 10.1136/bmjopen-2017-018791
34. Godin K, Stapleton J, Kirkpatrick SI, Hanning RM, Leatherdale ST. Applying systematic review search methods to the grey literature: a case study examining guidelines for school-based breakfast programs in Canada. Syst Rev. (2015) 4:138. doi: 10.1186/s13643-015-0125-0
35. The Canadian Agency for Drugs Technologies in Health (CADTH). Grey Matters: A Practical Tool for Searching Health-Related Grey Literature. Ottawa: CADTH (2018). Available online at: https://www.cadth.ca/grey-matters-practical-tool-searching-health-related-grey-literature-0 (accessed October 20, 2021).
38. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
39. Tannenbaum C, Clow B, Haworth-Brockman M, Voss P. Sex and gender considerations in Canadian clinical practice guidelines: a systematic review. CMAJ Open. (2017) 5:E66–73. doi: 10.9778/cmajo.20160051
40. Gaetz S, Barr C, Friesen A, Harris B, Hill C, Kovacs-Burns K, et al. Canadian Definition of Homelessness. Toronto: Canadian Observatory on Homelessness Press (2012).
41. Popay J, Roberts HM, Sowden AJ, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. In: A Product from the ESRC Methods Programme. Version 12006.
42. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15:1277–88. doi: 10.1177/1049732305276687
43. Cochrane, Methods Equity. PROGRESS-Plus 2021. Available online at: https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus (accessed October 12, 2021).
Keywords: clinical practice guideline, traumatic brain injury, concussion, homeless, health inequity, evidence-based practice, knowledge synthesis, disadvantaged populations
Citation: Chan V, Estrella MJ, Babineau J and Colantonio A (2022) A systematic review protocol for assessing equity in clinical practice guidelines for traumatic brain injury and homelessness. Front. Med. 9:815660. doi: 10.3389/fmed.2022.815660
Received: 16 November 2021; Accepted: 29 June 2022;
Published: 22 July 2022.
Edited by:
Hengli Tian, Shanghai Jiao Tong University School of Medicine, ChinaReviewed by:
Donna Ouchterlony, Setting Priorities for Retirement Years Foundation, United StatesCopyright © 2022 Chan, Estrella, Babineau and Colantonio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vincy Chan, dmluY3kuY2hhbkB1aG4uY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.