
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 15 February 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.800962
This article is part of the Research TopicOvercoming Boundaries in Public Health: Advances in International and Global HealthView all 5 articles
 Gary Ka-Ki Chung1
Gary Ka-Ki Chung1 Carol Strong2
Carol Strong2 Yat-Hang Chan1Roger Yat-Nork Chung1,3Jung-Sheng Chen4Yi-Hsuan Lin5Ru-Yi Huang6,7*
Yat-Hang Chan1Roger Yat-Nork Chung1,3Jung-Sheng Chen4Yi-Hsuan Lin5Ru-Yi Huang6,7* Chung-Ying Lin2,8,9,10*Nai-Ying Ko5
Chung-Ying Lin2,8,9,10*Nai-Ying Ko5Purpose: The novel coronavirus disease 2019 (COVID-19) caused psychological distress and changed human living styles. However, rare studies have examined the psychological distress and protective behaviors across different populations. Therefore, the present study aimed to assess psychological distress, protective behaviors, and potential predictors of psychological distress and protective behaviors across the Hong Kong general population, Taiwan healthcare workers, and Taiwan outpatients.
Methods: A cross-sectional design was used to recruit participants from Hong Kong and Taiwan. Telephone interviews were carried out for Hong Kong participants (n = 1,067; 30.2% male participants); online surveys were used for Taiwan healthcare workers (n = 500; 8.0% male participants) and Taiwan outpatients (n = 192; 32.8% male participants). All the participants completed questions on psychological distress and protective behaviors. Multiple linear regressions and multivariable logistic regressions were employed to explore the potential predictors of psychological distress and protective behaviors, respectively.
Results: Hong Kong participants had significantly lower levels of psychological distress than Taiwan participants [mean (SD) = 0.16 (0.39) vs. 0.47 (0.59) in healthcare workers and 0.46 (0.65) in outpatients; p < 0.001]. Hong Kong participants (51.7%) and Taiwan outpatients had more people showing fear of COVID-19 (52.0%) than Taiwan healthcare providers (40.8%; p < 0.001). Moreover, Hong Kong participants engaged the most in protective behaviors, followed by Taiwan healthcare providers and Taiwan outpatients (p < 0.001). Moreover, being a female, fear of COVID-19 and worry about personal savings were associated with protective behaviors in general.
Conclusions: Despite the greater COVID-19 severity and fear of COVID-19 in Hong Kong, the general population in Hong Kong experienced less psychosocial distress with higher compliance to protective behaviors than the other groups in Taiwan.
The long-lasting infection disease, novel coronavirus disease 2019 (COVID-19), has been announced as a global pandemic by the World Health Organization (WHO) (1) over one and a half years. However, the severity and infection rate of COVID-19 remains high worldwide with the emergence of several COVID-19 virus variants (2, 3). Although COVID-19 vaccines have been rapidly developed and implemented (4), concerns over vaccine uptake (5–8) and their efficacy against the emerging COVID-19 variants (9, 10) may hamper the progress toward herd immunity and recovery from COVID-19. Consequently, the psychological distress caused by the COVID-19 (11–14) is unlikely to be resolved in a short period of time. Indeed, several estimations suggest that the virus will not be under control shortly (15, 16). Therefore, the experience from the early stage of COVID-19 pandemic regarding psychological distress (i.e., unpleasant feelings and perceived discomforts, such as depression and anxiety) (17) and protective behaviors would be of great value to assist policymakers and relevant stakeholders in taking care of their citizens under the current or future COVID-19 pandemic.
Several studies have examined the psychological distress (especially in anxiety and depression) during the COVID-19 pandemic (18–29). Specifically, Ahorsu et al. (18) and Pramukti et al. (26) found that university students have issues of anxiety and suicidal ideation during the COVID-19 pandemic. Hasannia et al. (20), Patel et al. (24), and Patil et al. (25) found that healthcare workers have issues of psychological distress related to being stigmatized, burnout, and anxiety. The psychological distress issues among healthcare workers have been summarized by Olashore et al. (23) using a systematic review that the prevalence rates of anxiety (9.5–73.3%) and depression (12.5–71.9%) were high among healthcare workers in African countries. Regarding the general population, Mamun et al. (22) found that the Bangladeshi general population had a relatively high rate of suicidal ideation (5–33%), and depression is one of the key factors explaining suicidal ideation. Moreover, Alimoradi et al. (19) conducted a systematic review with meta-analysis and found that fear of COVID-19 was moderately associated with psychological distress.
We have identified three important populations across two regions (i.e., Hong Kong and Taiwan) sharing similar subcultures but with different levels of COVID-19 severity in the early stage of this pandemic to investigate the issues of psychological distress and protective behaviors. Specifically, they are Hong Kong general population, Taiwan healthcare workers, and Taiwan outpatients. The COVID-19 development in Hong Kong and Taiwan is described below. Since the first confirmed case on January 23, 2020, Hong Kong experienced several waves of the massive local outbreak in 2020 (30–32), given that the high population density and hence crowded living conditions, favor rapid COVID-19 transmission. The Center for Health Protection, which was established for effective disease prevention and control following the Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong, has taken swift actions to contain the outbreak via comprehensive contact tracing, quarantine measures, and progressively stringent social distancing policies (33). Nonetheless, despite the good compliance to personal hygiene practices and efforts by the government and community organizations in Hong Kong, 8,847 confirmed or probable infected cases and 148 deaths were identified as of the end of December 2020 (34).
On the other hand, in Taiwan, the first case who has been confirmed having COVID-19 was announced on January 21, 2020, and nearly 1 month later (i.e., on February 16, 2020), the first death caused by COVID-19 was reported. Even after the announcement of COVID-19 pandemic (i.e., mid-March 2020), Taiwan still controlled the prevalence and infection rate of COVID-19 with satisfactory performance (35, 36). Specifically, there were only 441 confirmed cases with 7 deaths at the time of 28 May 2020 (the population size in Taiwan was over 23 million). Up to the date of the data collection period in the present study (i.e., end of December 2020), there were only 799 confirmed cases with remaining 7 deaths (7, 14).
Most Hong Kong and Taiwan citizens are originated from the Han ethnicity and therefore share similar values in Confucianism, which guide them to highly appreciate harmony, social bonding, and collectivism (37–39). Apart from the Confucianism culture, both regions have experienced the SARS community outbreak, albeit in varying severity, in 2003 (40–42). During and after the SARS community outbreak, both governments have devised guidelines on infection control (40–42). However, the demographic features are somewhat different between Hong Kong and Taiwan. Specifically, Hong Kong has a much more condensed population than Taiwan (~6,804 people per km2 in Hong Kong; 1,742 people per km2 in Taiwan). Moreover, the COVID-19 severity and development were different between Hong Kong and Taiwan. Therefore, differences in psychological distress and behavioral response are expected between Hong Kong and Taiwan.
Regarding the three populations, they may have different psychological reactions and protective behaviors toward the threat of COVID-19 (17, 43, 44). However, such comparisons in psychological distress and protective behaviors are likely to be influenced by the COVID-19 severity between studied regions across populations with different features. Specifically, the general population, healthcare workers, and outpatients may have different reactions toward the COVID-19 pandemic. Subsequently, their psychological distress, fear of COVID-19, and protective behaviors may be different. Therefore, with the data from the Hong Kong general population (who have been facing a relatively more severe COVID-19 pandemic) and those from Taiwan healthcare workers and outpatients (who resided in a less severe level of COVID-19 pandemic), we can identify the potential influence of severity of COVID-19 on different populations' psychological distress, protective behaviors, and related risk factors.
The present study thus had two aims: (i) to assess the situation of and differences in psychological distress and protective behaviors across Hong Kong general population, Taiwan healthcare workers, and Taiwan outpatients; and (ii) to investigate the potential predictors for psychological distress and protective behaviors across the populations.
A cross-sectional study design was used to recruit participants from two regions (i.e., Hong Kong and Taiwan).
Data in Hong Kong were collected from a population-wide random sample of households via telephone survey from 11 September to October 12, 2020. The inclusion criteria for the study were Hong Kong Chinese residents aged 18 or above. Upon successful contact with a target household, one qualified member of the household was selected among those family members using the last-birthday random selection method. Telephone interviews were carried out by experienced interviewers between 18:00 and 22:00 on weekdays. Prior appointments were arranged for suitable respondents in other periods including weekends and public holidays. Among the 12,443 dialed telephone numbers, 10,555 were invalid cases in which 254 were non-residential lines, 4,776 were fax lines/invalid lines, 1,308 were cut off immediately, and 4,217 were non-contacts after three attempts. Among the 1,888 answered calls, 28 had mid-way termination, 59 could not establish contact with an eligible person after three attempts, and 734 were refused by the eligible persons, resulting in a final sample of 1,067 respondents with a response rate of 56.5% (i.e., 1,067 respondents divided by 1,888 answered calls). This study has been approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee in July 2020 with a registered number of 2,020.378.
Regarding the data collection in Taiwan, a convenience sampling was used and the survey period was between 24 September and 31 December 2020. Healthcare workers and outpatients in the National Cheng Kung University Hospital (NCKUH) were approached to complete the survey. Through the email dissemination, 500 healthcare workers and 192 outpatients from the NCKUH, which has about 5,000 employees and 1,500 beds, agreed to participate in this study. Specifically, the survey link contains clear information regarding the present study that was sent out via the email addresses that were stored in the NCKU Information Technology (IT) system. The first page of the online survey described the purpose and information of the study. When the participant agreed to participate, he or she should click on the agree button on this page for them to continue the online survey. The inclusion criteria for the Taiwan participants were: (i) a healthcare worker or an outpatient in the NCKUH and (ii) aged 20 years or over. The Institute Review Board (IRB) from the NCKUH approved the study with a registered number of A-ER-109-149.
Depression and anxiety were the two types of distress that were used to compose the psychological distress in the present study. The 4-item Patient Health Questionnaire (PHQ-4) for Depression and Anxiety (45), which combines the Patient Health Questionnaire-2 (PHQ-2) and the Generalized Anxiety Disorder-2 (GAD-2) scales, was adopted to assess the depression and anxiety symptoms of Hong Kong participants during COVID-19. Similar four items with slightly different wordings (given that the cultures were somewhat different between Hong Kong and Taiwan) were used for Taiwan participants. All the four items were rated on a four-point Likert scale (0 = not at all; 3 = nearly every day), and the psychological distress in the present study was a standardized summated score from the four-item scores (i.e., summed scores of the four items divided by the item number of 4 to make a scale between 0 and 3). Therefore, a higher score in psychological distress indicates a higher level of distress. The internal consistency of the four items on psychological distress was excellent (Cronbach's α = 0.88). Moreover, results of the confirmatory factor analysis using maximum likelihood estimator supported the one-factor structure of the psychological distress (p-value of the χ2 = 0.23; comparative fit index = 1.000; Tucker–Lewis index = 0.999; root-mean-square-error of approximation = 0.017; and standardized root mean square residual = 0.004).
Five types of behaviors were assessed according to the recommendations made by Hong Kong and Taiwan governments: regular handwashing, regular ventilation maintenance, regular household disinfection, substantial reduction of family gathering, and substantial reduction of friend gathering. A dichotomous score (yes and no) was used for assessing these protective behaviors. The internal consistency of the five items on protective behaviors was acceptable (Cronbach's α = 0.67).
One item (I am afraid of COVID-19) designed by the present authors was used to assess whether the participants feared of COVID-19. A dichotomous score (yes and no) was used for assessing fear of COVID-19.
Two types of worry designed by the present authors were assessed: worry on the sufficiency of personal protective equipment (PPE) and that of personal savings. A dichotomous score (yes and no) was used for assessing the two types of worry. The internal consistency of the two worry items was good (Cronbach's α = 0.73).
Age, sex, and educational level were assessed in the survey to understand the demographics of the studied samples.
Descriptive statistics, including frequency and mean, were used to summarize the features of the studied samples. The χ2-tests (for categorical-dependent variables) and the independent t-tests (for continuous-dependent variables) were then applied to examine whether the features and demographics were significantly different between Hong Kong and Taiwan participants. Multiple linear regression models were constructed to examine predictors on psychological distress with the independent variables of age, sex, group (i.e., Hong Kong participants or Taiwan participants), fear of COVID-19, reduction of family gathering, reduction of friend gathering, worry on PPE sufficiency, and worry on personal savings. Multivariable logistic regression models were employed to examine predictors on these five types of protective behaviors with the independent variables of age, sex, group (i.e., Hong Kong participants or Taiwan participants), fear of COVID-19, worry on PPE sufficiency, and worry on personal savings. Moreover, interaction of group and sex were further investigated. Specifically, similar multiple linear regression and logistic regression models were performed with the stratification of group (by Hong Kong participants, Taiwan healthcare workers, and Taiwan outpatients) or sex (by male and female participants). For multiple linear regression models, standardized coefficients were used to present the effect size; for multivariable logistic regression models, adjusted odds ratios (AORs) were used to present the effect size. Moreover, 95% CIs of the AORs were calculated. Assumptions for multiple linear regression were checked using (i) skewness <3 and kurtosis <8 (for normality), (ii) Durbin–Watson statistics between 1.5 and 2.5 (for homoscedasticity), and (iii) variance inflation factor (VIF) value <10 (for independence). Sample size in the present study was sufficient for the constructed regression models (including multiple linear regression models and multivariable logistic regression models) according to the rule of thumb in estimating required numbers in a regression model (i.e., the ratio of subjects to predictors should range between 8 and 30) (46–50). By using the ratio of 30 and the 10 predictors, the sample size at 300 is sufficient for all the regression models in the present study. All the statistical analyses were conducted using the IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA).
Table 1 presents the comparisons of the participants recruited from different areas. Specifically, the Hong Kong participants (n = 1,067; 68.3% aged above 50 years) were significantly older than the Taiwan healthcare workers (n = 500; 4.8% aged above 50 years) and Taiwan outpatients (n = 192; 8.9% aged above 50 years; p < 0.001). Regarding sex distribution, male participants were significantly more in Hong Kong participants (30.2%) and Taiwan outpatients (32.8%) than in Taiwan healthcare workers (8.0%; p < 0.001). In addition, the educational level in Hong Kong participants (21.0% had a degree/diploma or above) was lower than the Taiwan participants (96.6% in healthcare workers and 84.9% in outpatients had a degree/diploma or above; p < 0.001).
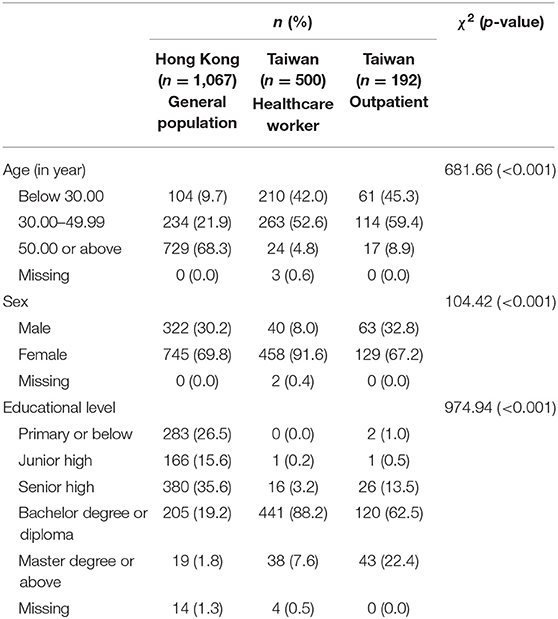
Table 1. Comparisons of participants' demographics between Hong Kong and Taiwan.
Table 2 additionally reports the psychological distress and behavior comparisons between Hong Kong and Taiwan participants. The results indicated that Hong Kong participants had significantly lower levels of psychological distress than Taiwan participants [mean (SD) = 0.16 (0.39) vs. 0.47 (0.59) in healthcare workers and 0.46 (0.65) in outpatients; p < 0.001]. Moreover, Hong Kong participants (51.7%) and Taiwan outpatients had more people showing fear of COVID-19 (48.4%) than Taiwan healthcare providers (40.8%; p < 0.001). Hong Kong participants (93.7%) and Taiwan healthcare providers (90.8%) had more people engaging in protective behavior of handwashing than did Taiwan outpatients (60.9%; p < 0.001). Hong Kong participants had more people than Taiwan participants engaging in protective behaviors of maintaining ventilation (90.5 vs. 74.0% in healthcare workers and 68.8% in outpatients; p < 0.001); disinfecting household (78.2 vs. 39.8% in healthcare workers and 42.2% in outpatients; p < 0.001); reducing family gathering (39.8 vs. 7.0% in healthcare workers and 9.4% in outpatients; p < 0.001); and reducing friend gathering (57.2 vs. 8.2% in healthcare providers and 12.0% in outpatients; p < 0.001). Moreover, Hong Kong participants had less people than Taiwan participants in worrying PPE sufficiency (3.6 vs. 97.4% in healthcare providers and 16.1% in outpatients; p < 0.001) and personal savings (31.2 vs. 91.4% in healthcare providers and 37.5% in outpatients; p < 0.001).
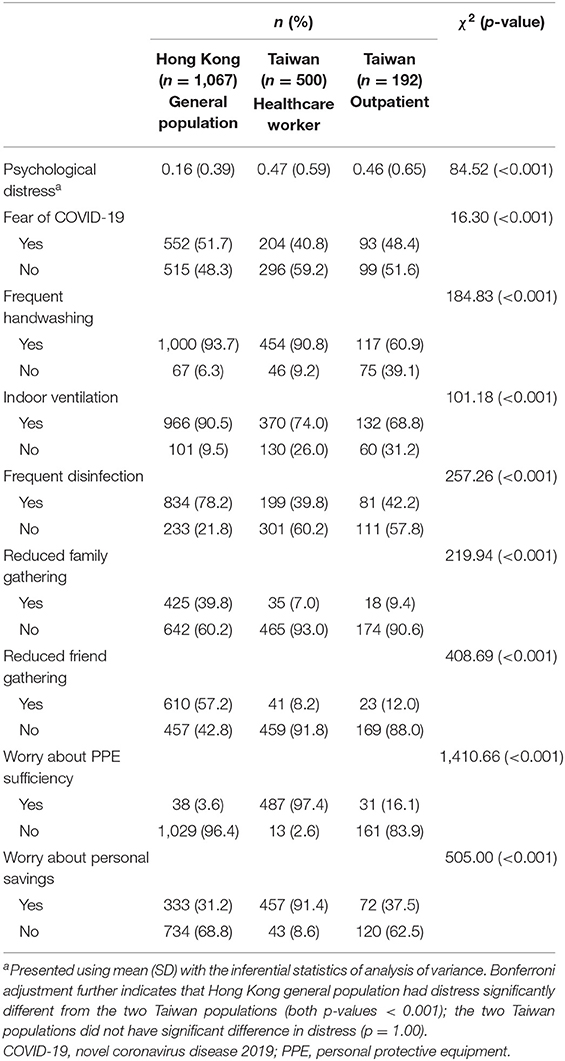
Table 2. Comparisons of participants' distress and behaviors between Hong Kong and Taiwan.
The lower levels of psychological distress in Hong Kong participants than those in Taiwan participants were confirmed by the multiple linear regression when other studied variables were controlled (i.e., all the variables listed in Table 3 were entered into the same regression model) (Table 3). The assumptions for the multiple linear regression model were satisfied: skewness = 2.21, kurtosis = 5.14, Durbin–Watson statistics = 2.03, and VIF = 1.07 to 6.45. The entire multiple linear regression model was significant (R2 = 0.115; adjusted R2 = 0.110; F-value = 22.63; p < 0.001). Moreover, reduced friend gathering [reference group: No; standardized coefficient (β) = 0.074; p = 0.034] and worry on personal savings (reference group: No; β = 0.085; p = 0.003) were significantly associated with higher levels of psychological distress. However, a significant interaction of different population was found in the association between worry on personal saving and psychological distress: the relationship was positive among Hong Kong participants (β = 0.203; p < 0.001) and among Taiwan outpatients (β = 0.179; p = 0.019), but negative among Taiwan healthcare workers (β = −0.440; p < 0.001) (Supplementary Table S1).
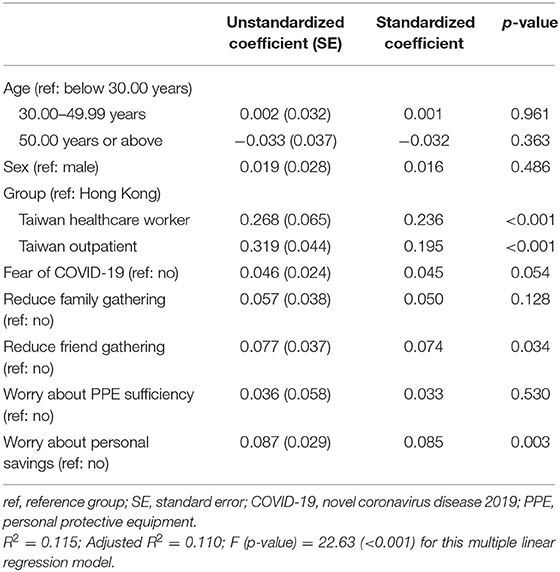
Table 3. Multiple linear regression model in explaining psychological distress.
Regarding the behaviors, multivariable logistic regressions showed that female participants as compared with male participants engaged more in handwashing (AOR = 1.68; 95% CI = 1.17, 2.41), maintaining ventilation (AOR = 1.37; 95% CI = 1.00, 1.88), and disinfecting household (AOR = 1.45; 95% CI = 1.12, 1.87). Moreover, Taiwan participants as compared with Hong Kong participants engaged less in all the protective behaviors significantly (AOR = 0.02–0.68). Fear of COVID-19 was a significant predictor in all the protective behaviors (AOR = 1.36–2.61). Additionally, participants having worry on personal savings, as compared with those without worry on savings, engaged less in handwashing (AOR = 0.47; 95% CI = 0.31, 0.70), maintaining ventilation (AOR = 0.56; 95% CI = 0.40, 0.79), and disinfecting household (AOR = 0.62; 95% CI = 0.48, 0.81), but were more likely to reduce gathering with family (AOR = 2.24; 95% CI = 1.71, 2.92) and friends (AOR = 2.18; 95% CI = 1.66, 2.87) (Table 4). Stratified analyses further showed that the associations between fear of COVID-19 and personal hygiene practices, and that between worry on personal savings and all protective behaviors, were stronger in Hong Kong participants than in Taiwan participants (Supplementary Table S2).
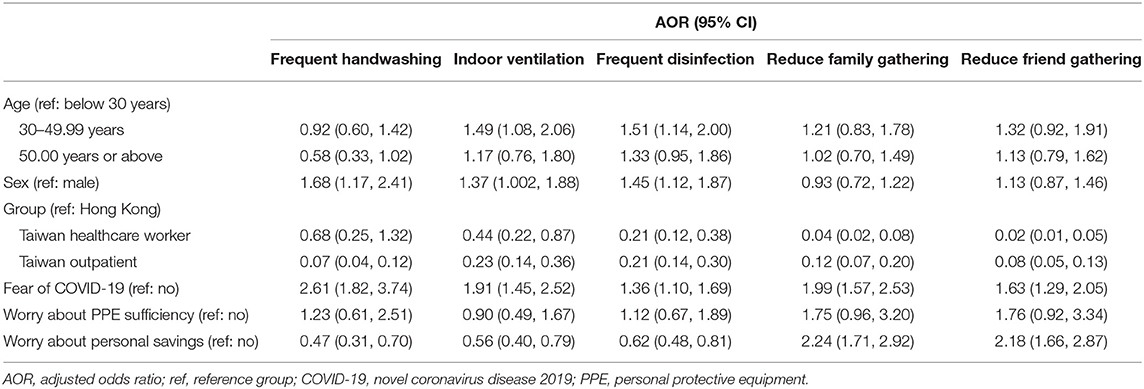
Table 4. Multivariable logistic regression models in explaining protective behaviors.
The present study showed that the general population in Hong Kong experienced less psychosocial distress than the other groups in Taiwan. Although the level of fear of COVID-19 was higher in Hong Kong than in Taiwan, people in Hong Kong were less worried about the supply of PPE and their personal savings, and engaged in more protective behaviors under the pandemic. In addition to the apparent impact of reduced friend gatherings on psychosocial distress possibly due to a strong sense of collective identity in Chinese communities, further analyses showed that the association of worry about personal savings with psychosocial distress was particularly evident in Hong Kong. Moreover, being a female, fear of COVID-19 and worry about personal savings were associated with protective behaviors in general. Specifically, fear of COVID-19 was a particularly stronger facilitator of personal hygiene practices in the general population of Hong Kong compared with the other groups in Taiwan. Worrying about personal savings also tended to be a stronger risk factor of personal hygiene practices and a stronger facilitator of reduced gatherings in Hong Kong.
One interesting observation from this study is that the greater level of fear of COVID-19 in Hong Kong was accompanied by less severe psychosocial distress compared with Taiwan. The particularly stronger fear of COVID-19 in Hong Kong could plausibly be attributable to the painful experience of SARS back in 2003. Although both Hong Kong and Taiwan experienced the SARS outbreak, Hong Kong was hit more severely both in terms of infection and economic impact. Specifically, there were 1,755 SARS cases and 299 deaths (out of 6.73 million citizens) in Hong Kong (51), compared with 664 cases and 73 deaths (out of 22.6 million citizens) in Taiwan (52). In addition, the economic crisis followed by SARS was more devastating in Hong Kong with the estimated temporary shock of 2.63% gross domestic product (GDP) loss and estimated persistent shock of 3.21% GDP loss over 10 years, whereas the corresponding figures of GDP loss in Taiwan were 0.49 and 0.53% (53). Therefore, it is reasonable that the COVID-19 pandemic evoked painful memories of the SARS outbreak and hence instigated a greater level of fear in Hong Kong than in Taiwan.
However, the SARS crisis has also been turned into an opportunity in face of the COVID-19 pandemic, which has rendered a better pandemic preparedness at government and community levels, and enhanced awareness of infection control and resilience against COVID-19 distress in the general public (54–56). This echoes with our observation on the lower levels of worries and psychosocial distress in Hong Kong even though the severity of COVID-19 pandemic was greater than in Taiwan. Apart from the lesson learned from SARS, other protective factors including efforts on infection control and risk communication by the Center for Health Protection (56), strong mobilization of resources in the community (57), and the launch of social policies on financial security and employment support (58, 59) in Hong Kong could also have buffered the general public from the psychosocial distress caused by the pandemic.
In addition to the differential levels of psychosocial distress and engagement of protective behaviors, this study also identified several distinctive determinants across groups in Hong Kong and Taiwan. For example, although the fear of COVID-19 has been consistently reported as a critical predictor of positive behavioral changes (60–62), we observed a stronger association with personal hygiene practices in Hong Kong where the local COVID-19 outbreak was more severe than in Taiwan. Consistent with the Protection Motivation Theory (63), increased perceived severity of the pandemic and perceived vulnerability to COVID-19 infections could have led to the greater level of fear in densely populated Hong Kong, and hence facilitated the adoption of personal hygiene practices via the threat appraisal. Additionally, the previous successful experience in combating SARS via good hygiene practices may also have facilitated the behavioral change via the coping appraisal. The differential impact of fear between Hong Kong and Taiwan suggests that the association between fear of COVID-19 and personal hygiene practices may need to be induced when the pandemic severity achieves a certain level. Such an observation echoes with a recent study capturing the temporal change in COVID-19 severity in Taiwan that the association between fear and protective behaviors was not significant during March and May 2020 but became significant during May and July 2021 when the largest COVID-19 outbreak in Taiwan was emerging (64).
Another distinctive determinant between Hong Kong and Taiwan was the worry about personal savings, with its associations with distress and protective behaviors consistently more apparent in Hong Kong. The stronger impact could plausibly be explained by the greater pre-existing income inequality in Hong Kong, given that the Gini Coefficient based on post-tax post-social transfer monthly household income in 2016 was high at 0.473 in Hong Kong but only 0.336 in Taiwan (65, 66). In addition, Hong Kong has been the most unaffordable city in the world in terms of the annual cost of living, compared with a ranking of 28th for Taipei, Taiwan in 2020 (67). Taken together, those who were worried about personal savings, who also tended to be of a lower socioeconomic position in Hong Kong, may have experienced a greater level of psychosocial distress under the pandemic-related economic downturn. This is also in line with the previous COVID-19 research in Hong Kong supporting a partial mediation of inequalities in mental health via people's concerns over livelihood and economic activity (68, 69). Furthermore, studies in Hong Kong also revealed that the socially deprived individuals tended to be more concerned about PPE as they had lower reserves and hence utilization (68, 70), which may help explain why to worry about personal savings acted as a risk factor of personal hygiene practices but a facilitator of reduced social gatherings in Hong Kong. Adopting personal hygiene practices may be costly and so they engaged in these behaviors less frequently; instead, reducing social gatherings can help them save money and PPE.
Several limitations of this study are worth mentioning. First, due to the cross-sectional design in the surveys in Hong Kong and Taiwan, the temporal sequence of associations could not be established. Second, the residual confounding may exist in the present study's findings due to unavailable or incomparable data on health literacy, socioeconomic position, and baseline mental health status prior to COVID-19. Third, fear of COVID-19 was measured by one single item, which may not be as reliable and accurate as other more robust measurement tools, such as the Fear of COVID-19 Scale (71–74). Fourth, some measures were assessed using a dichotomous scale (i.e., protective behaviors, fear of COVID-19, and worry). Therefore, the responses in dichotomous scale may provide insufficient psychometric information for data analysis. Fifth, the measures used in the present study (except for the measure of psychological distress) were designed by the present authors. These measures have not been tested using the content validity ratio, although the present authors who are experts in this field agree that these measures are valid. Future studies should check these measures' psychometric properties if they want to use these measures. Sixth, two methods (i.e., telephone and online survey) were used for data collection. However, we are confident that the different data collection methods used in the present study do not cause serious biases, given the empirical evidence showing that different data collection methods are equivalent in the data quality (75–77). Lastly, the findings of the comparative study are generalizable only to Hong Kong and Taiwan during the period that the COVID-19 outbreak was more severe in Hong Kong, but not to other countries being harder hit by COVID-19 or to other time periods, especially when the COVID-19 situations in Hong Kong and Taiwan reversed in mid-2021. Accordingly, a large-scale study involving different parts of the world (e.g., Eastern countries and Western countries) may provide additional insightful information for worldwide policymakers to make an appropriate decision in fighting the COVID-19 pandemic.
Despite the greater COVID-19 severity and fear of COVID-19 in Hong Kong, the general population in Hong Kong experienced less psychosocial distress with higher compliance to protective behaviors than the other groups in Taiwan. Worry about personal savings and fear of COVID-19 appeared to be distinctive determinants of psychosocial distress and protective behaviors in Hong Kong. Such distinctive determinants may be attributable to the differences in social contexts between Hong Kong and Taiwan, including pre-existing income inequalities, the severity of COVID-19 outbreaks, related responses at government and community levels, and the past experiences and legacy of SARS.
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
The study was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (registered number: 2020.378) and the Institute Review Board from the National Cheng Kung University Hospital (registered number: A-ER-109-149). The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
C-YL and GC performed material preparation, data collection, data analyses, and written the first draft of the manuscript. All authors contributed to conception and design of the study, contributed to data interpretation, critically commented on previous versions of the manuscript, and read and approved the final manuscript.
This study was supported in part by the Ministry of Science and Technology, Taiwan (Grant No. MOST109-2327-B-006-005), in part by the Taipei Municipal Wanfang Hospital Cross-Institutions Fund (Grant No. 110-swf-01), and in part by the Higher Education Sprout Project, Ministry of Education to the Headquarters of University Advancement at National Cheng Kung University (NCKU). Data collection in Hong Kong was also supported by a research project grant from the Chinese University of Hong Kong Institute of Health Equity, which was funded by the Vice-Chancellor's Discretionary Fund of the Chinese University of Hong Kong (Project Ref No.: 136604080).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the participants. GC also acknowledges the Research Grant Council of Hong Kong for its support over his Postdoctoral Fellowship (Ref. No.: PDFS2122-4H02).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.800962/full#supplementary-material
1. Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
2. Abedi V, Olulana O, Avula V, Chaudhary D, Khan A, Shahjouei S, et al. Racial, economic, and health inequality and COVID-19 infection in the United States. J Racial Ethnic Health Dispar. (2021) 8:732–42. doi: 10.1007/s40615-020-00833-4
3. Jungreis I, Sealfon R, Kellis M. SARS-CoV-2 gene content and COVID-19 mutation impact by comparing 44 Sarbecovirus genomes. Nat Commun. (2021) 12:1–20. doi: 10.1038/s41467-021-22905-7
4. Li Y, Tenchov R, Smoot J, Liu C, Watkins S, Zhou Q. A comprehensive review of the global efforts on COVID-19 vaccine development. ACS Central Sci. (2021) 7:512–33. doi: 10.1021/acscentsci.1c00120
5. Chen I-H, Ahorsu DK, Ko N-Y, Yen C-F, Lin C-Y, Griffiths MD, et al. Adapting the motors of influenza vaccination acceptance scale into the motors of COVID-19 vaccination acceptance scale: psychometric evaluation among mainland Chinese university students. Vaccine. (2021) 39:4510–5. doi: 10.1016/j.vaccine.2021.06.044
6. Fan C-W, Chen I-H, Ko N-Y, Yen C-F, Lin C-Y, Griffiths MD, et al. Extended theory of planned behavior in explaining the intention to COVID-19 vaccination uptake among mainland Chinese university students: an online survey study. Human Vaccines Immunother. (2021) 17:3413–20. doi: 10.1080/21645515.2021.1933687
7. Kukreti S, Lu M-Y, Lin Y-H, Strong C, Lin C-Y, Ko N-Y, et al. Willingness of Taiwan's healthcare workers and outpatients to vaccinate against COVID-19 during a period without community outbreaks. Vaccines. (2021) 9:246. doi: 10.3390/vaccines9030246
8. Yahaghi R, Ahmadizade S, Fotuhi R, Taherkhani E, Ranjbaran M, Buchali Z, et al. Fear of COVID-19 and perceived COVID-19 infectability supplement theory of planned behavior to explain Iranians' intention to get COVID-19 vaccinated. Vaccines. (2021) 9:684. doi: 10.3390/vaccines9070684
9. Brüssow H. COVID-19: vaccination problems. Environ Microbiol. (2021) 23:2878–90. doi: 10.1111/1462-2920.15549
10. Zeyaullah M, Alshahrani AM, Muzammil K, Ahmad I, Alam S, Khan WH, et al. COVID-19 and SARS-CoV-2 variants: current challenges and health concern. Front Genet. (2021) 12:916. doi: 10.3389/fgene.2021.693916
11. Chen C-Y, Chen I-H, Pakpour AH, Lin C-Y, Griffiths MD. Internet-related behaviors and psychological distress among schoolchildren during the COVID-19 school hiatus. Cyberpsychol Behav Soc Networking. (2021) 24:654–63. doi: 10.1089/cyber.2020.0497
12. Chen I-H, Chen C-Y, Liu C-H, Ahorsu DK, Griffiths MD, Chen Y-P, et al. Internet addiction and psychological distress among Chinese schoolchildren before and during the COVID-19 outbreak: a latent class analysis. J Behav Addict. (2021) 10:731–46. doi: 10.1556/2006.2021.00052
13. Chen I-H, Chen C-Y, Pakpour AH, Griffiths MD, Lin C-Y, Li X-D, et al. Problematic internet-related behaviors mediate the associations between levels of internet engagement and distress among schoolchildren during COVID-19 lockdown: a longitudinal structural equation modeling study. J Behav Addict. (2021) 10:135–48. doi: 10.1556/2006.2021.00006
14. Lu M-Y, Ahorsu DK, Kukreti S, Strong C, Lin Y-H, Kuo Y-J, et al. The prevalence of posttraumatic stress disorder symptoms, sleep problems, and psychological distress among COVID-19 frontline healthcare workers in Taiwan. Front Psychiatry. (2021) 12:705657. doi: 10.3389/fpsyt.2021.705657
15. Nkwayep CH, Bowong S, Tewa J, Kurths J. Short-term forecasts of the COVID-19 pandemic: a study case of Cameroon. Chaos Solitons Fractals. (2020) 140:110106. doi: 10.1016/j.chaos.2020.110106
16. Pak A, Adegboye OA, Adekunle AI, Rahman KM, Mcbryde ES, Eisen DP. Economic consequences of the COVID-19 outbreak: the need for epidemic preparedness. Front Public Health. (2020) 8:241. doi: 10.3389/fpubh.2020.00241
17. Alimoradi Z, Broström A, Tsang HW, Griffiths MD, Haghayegh S, Ohayon MM, et al. Sleep problems during COVID-19 pandemic and its' association to psychological distress: a systematic review and meta-analysis. E Clin Med. (2021) 36:100916. doi: 10.1016/j.eclinm.2021.100916
18. Ahorsu DK, Pramukti I, Strong C, Wnag H-W, Griffiths MD, Lin C-Y, et al. COVID-19-related variables and its association with anxiety and suicidal ideation: differences between international and local university students in Taiwan. Psychol Res Behav Manag. (2021) 14:1857–66. doi: 10.2147/PRBM.S333226
19. Alimoradi Z, Ohayon MM, Griffiths MD, Lin C-Y, Pakpour AH. Fear of COVID-19 and its association with mental health related factors: a systematic review and meta-analysis. BJ Psych Open. (2022).
20. Hasannia E, Mohammadzadeh F, Tavakolizadeh M, Davoudian N, Bay M. Assessment of the anxiety level and trust in information resources among iranian health-care workers during the pandemic of coronavirus disease 2019. Asian J Social Health Behav. (2021) 4:163–8. doi: 10.4103/shb.shb_68_21
21. Li Y-P, Lin C-Y, Chen Y-P, Kuo Y-J, Griffiths MD. Gender differences in the factors associated with the fear of COVID-19 among Taiwanese older people. Inquiry. (2021) 58:1–9. doi: 10.1177/00469580211055587
22. Mamun MA, Sakib N, Gozal D, Bhuiyan AI, Hossain S, Bodrud-Doza M, et al. The COVID-19 pandemic and serious psychological consequences in Bangladesh: a population-based nationwide study. J Affect Disord. (2021) 279:462–72. doi: 10.1016/j.jad.2020.10.036
23. Olashore AA, Akanni OO, Fela-Thomas AL, Khutsafalo K. The psychological impact of COVID-19 on health-care workers in African Countries: a systematic review. Asian J Soc Health Behav. (2021) 4:85–97. doi: 10.4103/shb.shb_32_21
24. Patel BR, Khanpara BG, Mehta PI, Patel KD, Marvania NP. Evaluation of perceived social stigma and burnout, among health-care workers working in covid-19 designated hospital of India: a cross-sectional study. Asian J Soc Health Behav. (2021) 4:156–62. doi: 10.4103/shb.shb_54_21
25. Patil ST, Datar MC, Shetty JV, Naphade NM. “Psychological consequences and coping strategies of patients undergoing treatment for COVID-19 at a tertiary care hospital”: a qualitative study. Asian J Soc Health Behav. (2021) 4:62–8. doi: 10.4103/shb.shb_5_21
26. Pramukti I, Strong C, Sitthimongkol Y, Setiawan A, Pandin MGR, Yen C-F, et al. Anxiety and suicidal thoughts during the COVID-19 pandemic: a cross-country comparison among Indonesian, Taiwanese, and Thai university students. J Med Internet Res. (2020) 22:e24487. doi: 10.2196/24487
27. Rajabimajd N, Alimoradi Z, Griffiths MD. Impact of COVID-19-related fear and anxiety on job attributes: a systematic review. Asian J Soc Health Behav. (2021) 4:51–5. doi: 10.4103/shb.shb_24_21
28. Sharma R, Bansal P, Chhabra M, Bansal C, Arora M. Severe acute respiratory syndrome coronavirus-2-associated perceived stress and anxiety among indian medical students: a cross-sectional study. Asian J Soc Health Behav. (2021) 4:98–104. doi: 10.4103/shb.shb_9_21
29. Yi J, Chen I-H, Lin C-Y, Li C-C, Liao XL, Wei Z-H, et al. The effect of primary and middle school teachers' problematic internet use and fear of COVID-19 on psychological need thwarting of online teaching and psychological distress. Healthcare. (2021) 9:1199. doi: 10.3390/healthcare9091199
30. Centre for Health Protection. Latest Situation of Cases of COVID-19. Hong Kong (2021). Available online at: https://www.chp.gov.hk/files/pdf/local_situation_covid19_en.pdf (accessed August 6, 2021).
31. Chung GK, Chan S-M, Chan Y-H, Yip TC-F, Ma H-M, Wong GL-H, et al. Differential impacts of multimorbidity on COVID-19 severity across the socioeconomic ladder in Hong Kong: a syndemic perspective. Int J Environ Res Public Health. (2021) 18:8168. doi: 10.3390/ijerph18158168
32. Chung GK, Chan S-M, Chan Y-H, Woo J, Wong H, Wong SY, et al. Socioeconomic patterns of COVID-19 clusters in low-incidence city, Hong Kong. Emerg Infect Dis. (2021) 27:840. doi: 10.3201/eid2711.204840
33. Legislative Council Secretariat,. Measures for the Prevention Control of Coronavirus Disease 2019 in Hong Kong. Hong Kong (2021). Available online at: https://www.legco.gov.hk/yr20-21/english/panels/hs/papers/hs20210205cb4-472-4-e.pdf (accessed August 6, 2021).
34. Kwok KO, Huang Y, Tsoi MTF, Tang A, Wong SYS, Wei WI, et al. Epidemiology, clinical spectrum, viral kinetics and impact of COVID-19 in the Asia-Pacific region. Respirology. (2021) 26:322–33. doi: 10.1111/resp.14026
35. Kuo Y-J, Chen Y-P, Wang H-W, Liu C-h, Strong C, Saffari M, et al. Community outbreak moderates the association between COVID-19-related behaviors and COVID-19 fear among older people: a one-year longitudinal study in Taiwan. Front Med. (2021) 8:756985. doi: 10.3389/fmed.2021.756985
36. Pakpour AH, Liu C-h, Hou W-L, Chen Y-P, Li Y-P, Kuo Y-J, et al. Comparing fear of COVID-19 and preventive COVID-19 infection behaviors between Iranian and Taiwanese older people: early reaction may be a key. Front Public Health. (2021) 9:740333. doi: 10.3389/fpubh.2021.740333
37. Leung H, Pakpour AH, Strong C, Lin Y-C, Tsai M-C, Griffiths MD, et al. Measurement invariance across young adults from Hong Kong and Taiwan among three internet-related addiction scales: bergen social media addiction scale (BSMAS), smartphone application-based addiction scale (SABAS), and internet gaming disorder scale-short form (IGDS-SF9) (study Part A). Addict Behav. (2020) 101:105969. doi: 10.1016/j.addbeh.2019.04.027
38. Lin C-Y, Strong C, Latner JD, Lin Y-C, Tsai M-C, Cheung P. Mediated effects of eating disturbances in the association of perceived weight stigma and emotional distress. Eat Weight Disord Stud Anorexia Bulimia Obes. (2020) 25:509–18. doi: 10.1007/s40519-019-00641-8
39. Tsai M-C, Strong C, Latner JD, Lin Y-C, Pakpour AH, Lin C-Y, et al. Attitudes toward and beliefs about obese persons across Hong Kong and Taiwan: wording effects and measurement invariance. Health Qual Life Outcomes. (2019) 17:1–11. doi: 10.1186/s12955-019-1198-6
40. Chau SW, Wong OW, Ramakrishnan R, Chan SS, Wong EK, Li PY, et al. History for some or lesson for all? A systematic review and meta-analysis on the immediate and long-term mental health impact of the 2002–2003 severe acute respiratory syndrome (SARS) outbreak. BMC Public Health. (2021) 21:1–23. doi: 10.1186/s12889-021-10701-3
41. Hsu C-Y, Wang J-T, Huang K-C, Fan AC-H, Yeh Y-P, Chen SL-S. Household transmission but without the community-acquired outbreak of COVID-19 in Taiwan. J Formosan Med Assoc. (2021) 120(Suppl. 1):S38–S45. doi: 10.1016/j.jfma.2021.04.021
42. Moallef P, Lueke NA, Gardner PJ, Patcai J. Chronic PTSD and other psychological sequelae in a group of frontline healthcare workers who contracted and survived SARS. Can J Behav Sci/Revue Can Sci Comport. (2021) 53:252. doi: 10.1037/cbs0000252
43. Al-Hanawi MK, Mwale ML, Alshareef N, Qattan AM, Angawi K, Almubark R, et al. Psychological distress amongst health workers and the general public during the COVID-19 pandemic in Saudi Arabia. Risk Manag Healthc Policy. (2020) 13:733. doi: 10.2147/RMHP.S264037
44. Simione L, Gnagnarella C. Differences between health workers and general population in risk perception, behaviors, and psychological distress related to COVID-19 spread in Italy. Front Psychol. (2020) 11:2166. doi: 10.3389/fpsyg.2020.02166
45. Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ−4. Psychosomatics. (2009) 50:613–21. doi: 10.1176/appi.psy.50.6.613
46. Green SB. How many subjects does it take to do a regression analysis? Multivariate Behav Res. (1991) 26:499–510.
47. Knapp TR, Campbell-Heider N. Numbers of observations and variables in multivariate analyses. West J Nurs Res. (1989) 11:634–41.
48. Pedhazur EJ, Schmelkin LP. Measurement, Design, and Analysis: An Integrated Approach. Hillsdale, NJ: Lawrence Erlbaum Associates (1991).
49. Sawyer R. Sample size and the accuracy of predictions made from multiple regression equations. J Educ Stat. (1982) 7:91–104.
50. Stevens J. Applied Multivariate Statistics for the Social Sciences. 4th ed. Mahwah, NJ: Lawrence Erlbaum Associates (2002).
51. Leung G, Ho, L, Lam, T, Hedley, A,. Epidemiology of SARS in the 2003 Hong Kong Epidemic. Hong Kong Medical Journal. (2009). Availeble online at: https://www.hkmj.org/system/files/hkm0912sp9p12.pdf (accessed August 3, 2021).
52. Taiwan Centers of Disease Control. Severe Acute Respiratory Syndrome (SARS). Taiwan (2014). Available online at: https://www.cdc.gov.tw/En/Category/ListContent/bg0g_VU_Ysrgkes_KRUDgQ?uaid=u1D6dRGtmP4Q5YA1GmSKIw (accessed August 3, 2021).
53. Oberholtzer K, Sivitz L, Mack A, Lemon S, Mahmoud A, Knobler S. Learning from SARS: Preparing for the Next Disease Outbreak: Workshop Summary. (2004). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK92462/pdf/Bookshelf_NBK92462.pdf (accessed August 3, 2021).
54. Kwok KO, Li KK, Chan HHH, Yi YY, Tang A, Wei WI, et al. Community responses during early phase of COVID-19 epidemic, Hong Kong. Emerg Infect Dis. (2020) 26:1575. doi: 10.3201/eid2607.200500
55. Lei M-K, Klopack ET. Social and psychological consequences of the COVID-19 outbreak: the experiences of Taiwan and Hong Kong. Psychol Trauma Theory Res Pract Policy. (2020) 12:S35. doi: 10.1037/tra0000633
56. Wong SY, Kwok KO, Chan FK. What can countries learn from Hong Kong's response to the COVID-19 pandemic? Can Med Assoc J. (2020) 192:E511–5. doi: 10.1503/cmaj.200563
57. Wan K-M, Ho LK-K, Wong NW, Chiu A. Fighting COVID-19 in Hong Kong: the effects of community and social mobilization. World Dev. (2020) 134:105055. doi: 10.1016/j.worlddev.2020.105055
58. Chan S-M, Chung GK-K, Chan Y-H, Woo J, Yeoh EK, Chung RY-N, et al. The mediating role of individual-level social capital among worries, mental health and subjective well-being among adults in Hong Kong during the COVID-19 pandemic. Curr Psychol. (2021). doi: 10.1007/s12144-021-02316-z
59. Hartley K, Jarvis DS. Policymaking in a low-trust state: legitimacy, state capacity, and responses to COVID-19 in Hong Kong. Policy Soc. (2020) 39:403–23. doi: 10.1080/14494035.2020.1783791
60. Brouard S, Vasilopoulos P, Becher M. Sociodemographic and psychological correlates of compliance with the Covid-19 public health measures in France. Can J Polit Sci/Revue Can Sci Polit. (2020) 53:253–8. doi: 10.1017/S0008423920000335
61. Harper CA, Satchell LP, Fido D, Latzman RD. Functional fear predicts public health compliance in the COVID-19 pandemic. Int J Ment Health Addict. (2021) 19:1875–88. doi: 10.1007/s11469-020-00281-5
62. Rad RE, Mohseni S, Takhti HK, Azad MH, Shahabi N, Aghamolaei T, et al. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: a cross-sectional study. BMC Public Health. (2021) 21:1–11. doi: 10.1186/s12889-021-10500-w
63. Rogers RW. A protection motivation theory of fear appeals and attitude change. J Psychol. (1975) 91:93–114. doi: 10.1080/00223980.1975.9915803
64. Chen CY, Ye JJ, Huang TS, Lee CC, Chen YT, Hsu CK, et al. Effective preventive strategies to prevent secondary transmission of COVID-19 in hemodialysis unit: the first month of community outbreak in Taiwan. Healthcare. (2021) 9:1173. doi: 10.3390/healthcare9091173
65. Directorate-General of Budget. Statistical Yearbook of the Republic of China 2019. Taiwan (2020). Available online at: https://eng.dgbas.gov.tw/public/data/dgbas03/bs2/yearbook_eng/Yearbook2019.pdf (accessed August 4, 2021).
66. Hong Kong Census Statistics Department. Thematic Report: Household Income Distribution in Hong Kong: 2016 Population By-Census. Hong Kong (2017). Available online at: https://www.bycensus2016.gov.hk/data/16BC_Income_Report.pdf (accessed August 4, 2021).
67. Irene Kew. Asia Continues to Dominate List of Most Expensive Cities in the World, Mercer's 2020 Cost of Living Survey finds: The Annual Survey Helps Employers Reassess Global Mobility Programs Amid Uncertainty from Pandemic. Hong Kong (2020). Available online at: https://www.mercer.com.hk/newsroom/mercer-2020-cost-of-living-survey-hk.html (accessed August 4, 2021).
68. Chung RY-N, Chung GK-K, Marmot M, Allen J, Chan D, Goldblatt P, et al. COVID-19 related health inequality exists even in a city where disease incidence is relatively low: a telephone survey in Hong Kong. J Epidemiol Commun Health. (2021) 75:616–23. doi: 10.1136/jech-2020-215392
69. Chung RY, Chung GK, Chan S-M, Chan Y-H, Wong H, Yeoh EK, et al. Socioeconomic inequality in mental well-being associated with COVID-19 containment measures in a low-incidence Asian globalized city. Sci Rep. (2021) 11:23161. doi: 10.1038/s41598-021-02342-8
70. Siu JYM. Health inequality experienced by the socially disadvantaged populations during the outbreak of COVID-19 in Hong Kong: an interaction with social inequality. Health Soc Care Commun. (2021) 29:1522–9. doi: 10.1111/hsc.13214
71. Ahorsu DK, Lin C-Y, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. (2020) 1–9. doi: 10.1007/s11469-020-00270-8
72. Chang K-C, Hou W-L, Pakpour AH, Lin C-Y, Griffiths MD. Psychometric testing of three COVID-19-related scales among people with mental illness. International J Mental Health Addict. (2020). doi: 10.1007/s11469-020-00361-6
73. Chen I-H, Chen C-Y, Zhao K-Y, Gamble JH, Lin C-Y, Griffiths MD, et al. Psychometric evaluation of fear of COVID-19 scale (FCV-19S) among Chinese primary and middle schoolteachers, and their students. Curr Psychol. (2021). doi: 10.1007/s12144-021-02471-3
74. Lin C-Y, Hou W-L, Mamun MA, da Silva JA, Broche-Pérez Y, Ullah I, et al. Fear of COVID-19 Scale (FCV-19S) across countries: measurement invariance issues. Nursing Open. (2021) 8:1892–908. doi: 10.1002/nop2.855
75. Deutskens E, de Ruyter K, Wetzels M. An assessment of equivalence between online and mail surveys in service research. J Serv Res. (2006) 8:346–55. doi: 10.1177/1094670506286323
76. Sarracino F, Riillo CFA, Mikucka M. Comparability of web and telephone survey modes for the measurement of subjective well-being. Surv Res Methods. (2017) 11:141–69. doi: 10.18148/srm/2017.v11i2.6740
Keywords: Asia, COVID-19, infection, psychological distress, protective behavior
Citation: Chung GK-K, Strong C, Chan Y-H, Chung RY-N, Chen J-S, Lin Y-H, Huang R-Y, Lin C-Y and Ko N-Y (2022) Psychological Distress and Protective Behaviors During the COVID-19 Pandemic Among Different Populations: Hong Kong General Population, Taiwan Healthcare Workers, and Taiwan Outpatients. Front. Med. 9:800962. doi: 10.3389/fmed.2022.800962
Received: 24 October 2021; Accepted: 03 January 2022;
Published: 15 February 2022.
Edited by:
Pietro Ferrara, University of Milano Bicocca, ItalyReviewed by:
José Manuel Reales, National University of Distance Education (UNED), SpainCopyright © 2022 Chung, Strong, Chan, Chung, Chen, Lin, Huang, Lin and Ko. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chung-Ying Lin, Y3lsaW4zNjkzM0Bncy5uY2t1LmVkdS50dw==; Ru-Yi Huang, cnV5aS5zdGFyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.