 Jacques Sevestre1,2†Antoine Benichou3†Vanessa Rio4Pascal Delaunay1Géraldine Gonfrier5Cécile Martaresche6Virginie Carlo4Sarah Nakam4
Jacques Sevestre1,2†Antoine Benichou3†Vanessa Rio4Pascal Delaunay1Géraldine Gonfrier5Cécile Martaresche6Virginie Carlo4Sarah Nakam4 Véronique Mondain4Michel Carles4
Véronique Mondain4Michel Carles4 Pierre Yves Jeandel3
Pierre Yves Jeandel3 Jacques Durant4*
Jacques Durant4*- 1Laboratory of Parasitology, Nice University Hospital, Nice, France
- 2IHU Méditerranée Infection, Marseille, France
- 3Department of Internal Medicine, Nice University Hospital, Nice, France
- 4Department of Infectious Diseases, Nice University Hospital, Nice, France
- 5Laboratory of Virology, Nice University Hospital, Nice, France
- 6SYNLAB Barla GmbH, Nice, France
Background: The French Riviera has been declared free of Lyme Borreliosis (LB) for years. Many patients are referred for presumed LB, sometimes with atypical clinical signs and/or doubtful serology, calling the diagnosis into question.
Methods: Patients were assessed for LB diagnosis, depending on clinical presentation, laboratory findings, and further examination by other medical professionals.
Results: Among 255 patients, 45 (18%) were classified as confirmed LB cases [including 28 ongoing LB (10%) and 17 past LB (8%)], and for 210 (82%) a Lyme borreliosis diagnosis was ruled out. Among ongoing LB, 56% had been exposed to or bitten by ticks, exclusively in rural locations of the Alpes-Maritimes. As a result of the diagnostic procedure, 132 (52%) patients had been treated. An alternative diagnosis was established for 134 (52%) patients, covering a wide range of conditions, including mainly psychological (28%) and neurological conditions (25%) or inflammatory and systemic diseases (22%).
Conclusions: Our results strongly suggest the endemicity of LB in the Alpes-Maritimes region. Confirmed LB accounted for 18% of patients while 52% were diagnosed with other conditions.
Introduction
Lyme disease, also known as Lyme Borreliosis (LB), is the most commonly reported vector-borne disease in the Northern hemisphere, and is caused by spirochaetes of the Borrelia burgdorferi genospecies complex (1–3).
Clinicians in Southern France (Alpes Maritimes), relying on historical data, usually consider the condition to be absent in this region for several reasons: reported absence of the vector (Ixodes ricinus ticks), due to unfavorable climate, and low number of suspected indigenous cases reported (4, 5).
Clinical manifestations of Lyme borreliosis are wide-ranging, but the most frequent symptom, which is also diagnostic, is a skin rash known as erythema migrans (EM). The non-specific nature of many LB clinical manifestations poses a diagnostic challenge, especially in atypical or late forms of the disease. In France and elsewhere, the definition of Lyme disease is a controversial issue, as non-characteristic presentations with symptoms such as fatigue, memory or concentration impairment, headache, arthralgia, and myalgia attributed to LB are on the rise. In this context, LB is often suspected in patients with atypical clinical presentation. Such patients should be referred to reference centers, prior to any presumptive treatment, to investigate for alternative diagnoses (6, 7), and thus avoid over-treating.
Patients and Methods
We recorded all patients referred for presumed LB to the Lyme disease competence center within the infectious diseases department of Nice University Hospital, France, between January 2016 and January 2020. Patients above 16 years of age with a diagnosis of LB, as presumed by the patient, the general practitioner or a specialist were included. We excluded patients lost during standard clinical follow-up. Variables of interest included age, gender, tick exposure, tick bite, history of EM, LB serology assay results, and past LB treatments. Prior presumed EM was only retained in case of an accurate description. Reasons for referral were classified according to the medical referral letter and patient's complaint as: EM, tick bite, positive or uncertain serology, neurological, rheumatologic (notably arthritis) or polymorphic symptoms, or other. EM was defined as a circular, non-pruriginous erythematous macule with centrifugal extension. Neurological symptoms comprised meningoradiculitis and headaches. Moreover, we defined arthritis as mono- or oligoarthritis, without fever. Personal medical history was reviewed. Signs and symptoms were recorded after thorough physical examination. Symptoms were grouped according to the main organ system involved or classified as polymorphic post-tick bite symptoms (PTBS) when patients had multiple-symptom complaints (at least three symptomatic organs involved and chronic fatigue). Results of LB serology assays, i.e., enzyme-linked immunosorbent assay (ELISA, Vidas Lyme Biomerieux IgG, and IgM), and western-blot (WB: Immunoblot-Mikrogen IgG and IgM), were collected. They were considered doubtful if not strictly negative. Two-tier serological testing was considered positive when both ELISA and western-blot testing were IgG positive, accordingly to the French guidelines (4). When patients faced a high degree of suspicion of LB, treatment was prescribed according to guidelines depending on clinical presentation. When LB suspicion was intermediate or low, patients were referred to other specialists (neurologist, rheumatologist, internal medicine specialists, psychiatrist or psychologist) in a coordinated pathway to complete investigations. If no differential diagnosis was made, LB presumptive treatment was offered regardless of potential prior treatment, in accordance with the French High Council of Public Health (Haut Conseil de la Santé Publique) guidelines (7). Unexplained, prolonged symptoms such as fatigue, impaired memory or concentration, headaches, arthralgia, and myalgia were not considered characteristic of LB but presumptive treatment was offered or if no alternative diagnosis was reached. Patients were treated with either amoxicillin (50 mg/kg/d) in case of EM, ceftriaxone (2 g/day) in case of neurological involvement, or doxycycline (200 mg/day) in other instances and in case of beta-lactam intolerance for at least 28 days (except in case of EM where the duration was 15 days). Recovery was defined as a return to the patient's previous health state before symptom appearance. No consent form was collected in this context of non-prospective, standardized patient management performed accordingly to national guidelines. Authorization for data processing was obtained. Cases were classified as either ongoing LB, past LB or non-LB. Categorical variables were compared using chi-square with Fisher's exact test. Calculation of Odds Ratio with interval confidence were calculated for all nominal categorical variables. Continuous variables were compared using the Mann-Whitney test. Differences were considered statistically significant for a p-value < 5%. Statistical analyses were performed using Statview version 5.0 (SAS institute, USA, Cary, NC, USA).
Results
Between January 2016 and January 2020, 305 patients presented at the outpatient department for presumed LB. Fifty patients were lost during follow-up. Among the 255 patients analyzed, median age was 50 years (range 18–88) with 62% women (n = 158). Patients' characteristics are detailed in Table 1. Forty percent of patients (n = 102) had already been treated for LB. The most frequently prescribed antibiotics were Doxycycline (n = 50, 49%), Amoxicillin (n = 36, 35%), Ceftriaxone (n = 5, 5%) and other antibiotics (n = 4, 4%). Seven patients had received ineffective treatments (anti-viral, anti-fungal or herbal agents). Fourteen patients had received a second-line LB treatment before the first visit in our referral clinic (6%).The ELISA test was positive in 121 patients (47%) and doubtful in 24 patients (9%). Twenty-six patients had positive ELISA associated with doubtful WB (10%). The two-tier serology (ELISA and WB) was positive in 56 patients (22%). A total of 132 patients (52%) were presumptively treated.
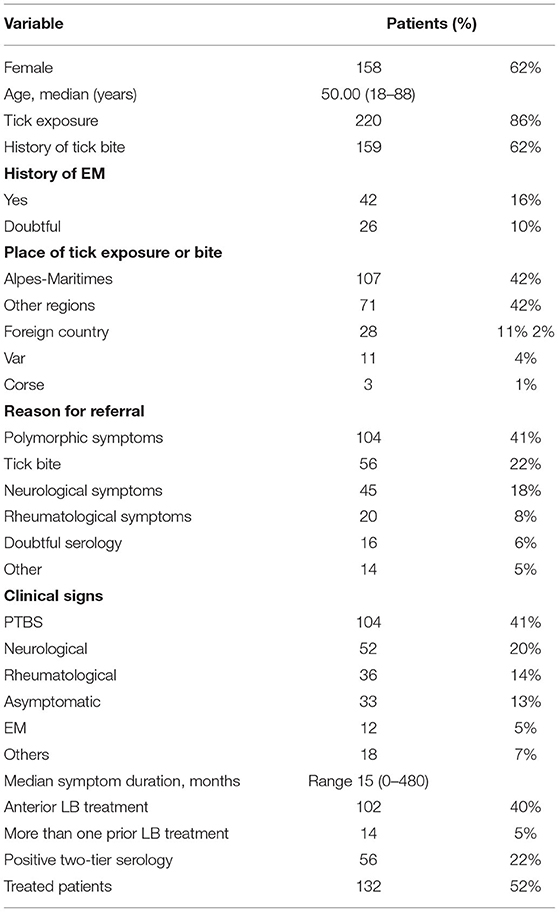
Table 1. Patients characteristics.
According to the applied criteria (Table 2), 45 patients were classified as confirmed LB cases (18%), including 28 (11%) with ongoing LB who were successfully treated (12 with EM, 10 with Neuro-Borreliosis and 6 with arthritis) and 17 (7%) with past LB (16 with EM and 1 with Neuro-Borreliosis) who had recovered after prior treatment.
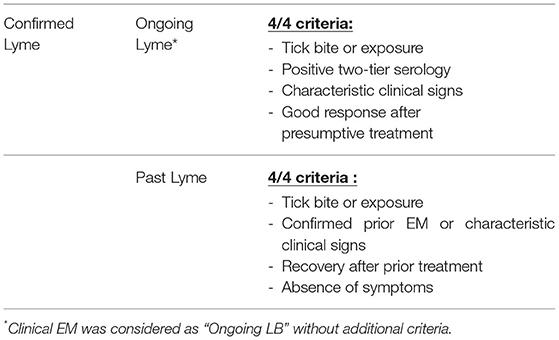
Table 2. Lyme Borreliosis diagnostic criteria.
Patients' diagnostic details are shown in Table 3 and final diagnoses detailed in Table 4. Comparison of Lyme and Non-Lyme groups appears in Table 5. Twenty-five patients supposedly contracted Lyme disease in the local rural area (indigenous cases). In 26 patients, no differential diagnosis could be ascertained despite investigations. Six patients were referred for doubtful serology with no treatment history nor EM and were asymptomatic, none were treated, they were considered as exhibiting a potential post-exposure serological scar or a false-positive serology. Among the 132 (52%) presumptively treated patients, following or concurrently with investigations, 72 achieved a significant response or recovery (54.5% of treated patients), 28 with ongoing LB and 44 with no proven LB.
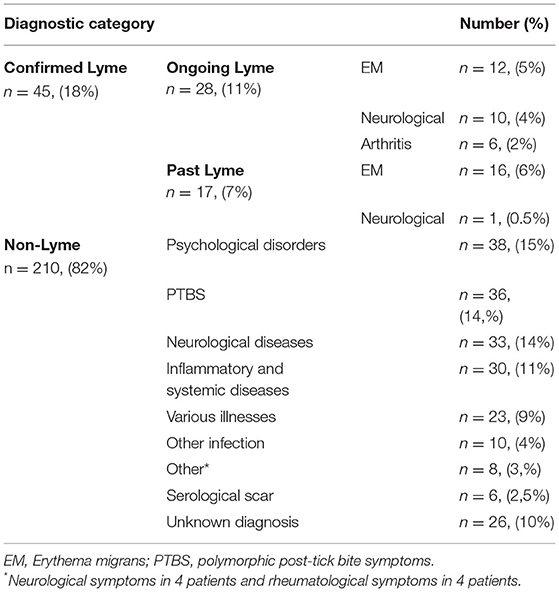
Table 3. Diagnoses among 255 subjects.
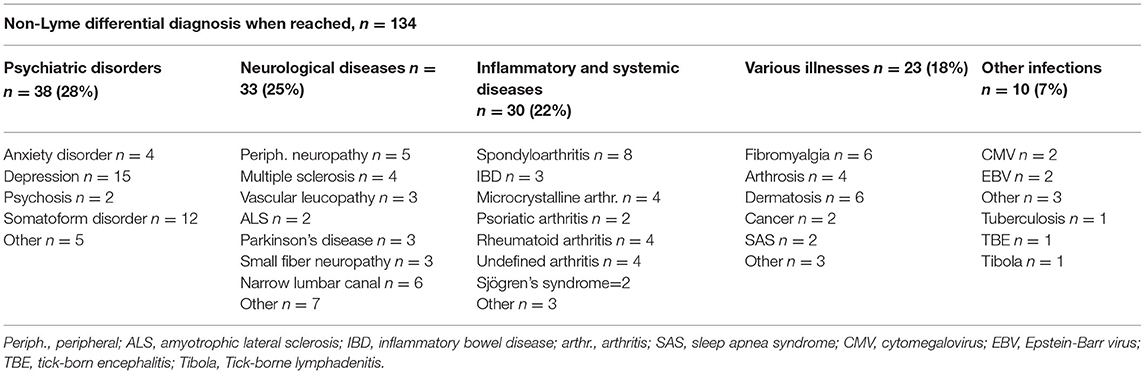
Table 4. Alternative diagnosis when achieved.
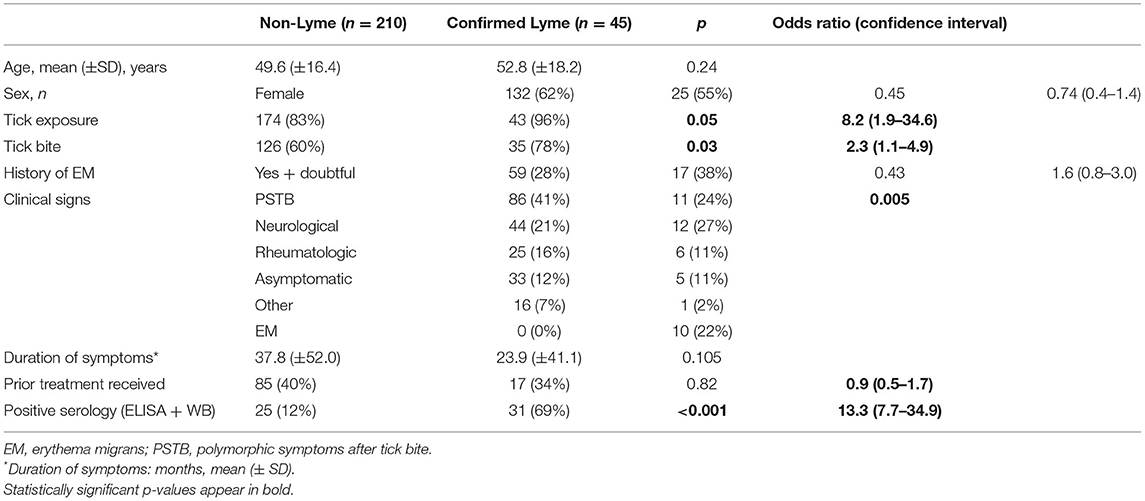
Table 5. Comparison between confirmed Lyme group and Non-Lyme group.
Discussion
These data confirm the current and potentially recent endemicity of Lyme disease in the Eastern Alpes-Maritimes, and to a lesser extent, on the French Riviera. Recently, Sevestre et al. revealed the current endemicity of Ixodes ricinus in various locations and the existence of biotopes compatible with their development and proliferation. Moreover, a significant proportion of the I. ricinus ticks collected were found to harbor Lyme group Borrelia. Excluding past confirmed cases of LB that were mostly referred for positive or uncertain serology and remained asymptomatic after EM (n = 17, 7%), ongoing confirmed LB accounted for 11% of our cohort. These results are consistent with French literature data where a final diagnosis of ongoing LB was reported in 10% of suspected cases in Paris (6), 12% in Besançon (8) and 15% in Nancy (9). A comparable rate in a low prevalence area such as the Alpes-Maritimes may be due to various factors: underestimated endemicity of the disease as mentioned above, population movements (44% of patients had been exposed or bitten by ticks in other regions or in foreign countries) and a recruitment bias. We hypothesize that in an area considered free of LB, local practitioners are less likely to suspect Lyme disease, resulting in a higher ratio of positive to suspect patients. Among our cohort, 210 patients were considered non-LB cases (82%). A differential diagnosis was made in most patients (n = 134, 81% of non-LB, i.e., 52.5% of the cohort), with a wide range of conditions, comparable to those presented by Jacquet et al., thanks to a dedicated multidisciplinary care pathway (9). Non-LB final diagnoses mainly consisted in psychological disorders (28%), neurological conditions (25%) or inflammatory and systemic diseases (22%). Some non-LB patients were presumptively treated while undergoing diagnostic investigations (n = 60, 36%) as empirical treatment of suspected LB could be considered innocuous and an alternative diagnosis was not obvious. Fourteen patients (23%) presented with moderate, unsustained improvement, potentially induced by a placebo effect (10). The remaining patients showed no improvement (n = 46, 77%). No final diagnosis could be reached in 26 patients (10%), consistently with previously cited reports (6, 8, 9).
Definition of possible LB cases remains a major subject of debate. Reports from seronegative, chronically ill patients, with proven Borreliosis and non-typical symptoms who recovered after empirical treatment challenge the conventional discourse around the disease (11). The diagnostic workup for LB traditionally involves assessing the patient's risk, objective signs and symptoms (such as EM), supported by laboratory findings when appropriate (12, 13). Formal serology results in patients presenting with potential LB symptoms may not be sufficient to definitely rule out the disease. Positive serology can be delayed in early Lyme, or remain negative in late forms of the disease, presumably due to suboptimal test sensitivity, even though this appears to be rare (14, 15). Extrinsic factors, including early antibiotic exposure, have likewise been found to influence the humoral response (16), as well as intrinsic factors such as immunodepression or inefficient host immune response (17). False negative serology have been proposed to be due to sequestration of Borrelia antibodies in immune complexes (18). Other biological diagnostic methods are under investigation, including culture and molecular biology methods (19–21). Analysis of host antigen-specific T-cell response to Borrelia is not widely adopted in clinical practice (22–24).
It is to be noted that ruling out psychological disorders in the context of such clinical presentations can be challenging as patients with “chronic Lyme disease” have been proposed to share identical characteristics of somatoform signs with fatigue, chronic pain and neurocognitive disorders such as memory or concentration impairment (25). Apart from EM, patients with disseminated infection experience signs and symptoms that depend on multiple factors such as geography (26, 27), host predisposition (28), treatment history (16–29) and infecting species. The number of genospecies belonging to the Lyme borreliosis complex continues to expand, while the pathogenicity and the variety in clinical presentations induced by many of them remains unknown (30).
This study has several limitations due to its monocentric design and to several practical difficulties. Moreover, for some patients data concerning prior treatments were obtained from patient interview, which includes a recall bias to our study. Essential work-up assessments such as psychiatric evaluation could not be performed in all patients, partly due to a lack of resources, leading to difficulties in interpreting results. Similarly, delayed investigations may have led us to over-treat certain patients. It is also to be noted that no conclusions may be drawn from empirical antibiotic treatment of suspected Lyme patients, as numerous research works have demonstrated that many improve on placebo treatments.
However, to the best of our knowledge, this work is the first to highlight the current endemicity of clinical Lyme disease. Moreover, our findings are corroborated by a recent study demonstrating the presence of both tick vectors and Lyme group Borrelia in tick vectors originating from the Alpes-Maritimes region (31). An alternative diagnosis was reached in over half of referred patients, highlighting the need for multidisciplinary management of these patients. Such a high proportion of patients diagnosed with other conditions could partly be explained by the media coverage of Lyme disease, and controversy or misleading information, resulting in patients or non-expert practitioners overly suspecting LB.
In the end, the present work establishes the occurrence of Lyme borreliosis in the Alpes-Maritimes region, as conforted by recent acarological data (31). We advocate for collaboration between infectious diseases clinicians, microbiologists and acarologists for epidemiological surveillance, and also for multidisciplinary management of patients suspect of Lyme borreliosis, to avoid misdiagnoses and improve patient care regarding this disease.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
AB, JD, VR, JS, and PJ contributed to the study design and patient clinical evaluation and wrote the manuscript. JS participated to implementation of the research. GG, PD, and CM participated to the analysis of the results. SN and VC performed psychological neurocognitive tests. VM, MC, PJ, and JD supervised the work and reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
CM was employed by company SYNLAB Barla GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nelson CA, Saha S, Kugeler KJ, Delorey MJ, Shankar MB, Hinckley AF, et al. Incidence of Clinician-Diagnosed Lyme Disease, United States, 2005–2010. Emerg Infect Dis. (2015) 21:1625–31. doi: 10.3201/eid2109.150417
2. Stanek G, Strle F. Lyme Disease, European Perspective. Infect Dis Clin North Am. (2008) 22:327–39. doi: 10.1016/j.idc.2008.01.001
3. Robert AS, Phoebe M. An estimate of Lyme borreliosis incidence in Western Europe. Journal of Public Health. (2017) 39:74–81. doi: 10.1093/pubmed/fdw017
4. Figoni J, Chirouze C, Hansmann Y, Lemogne C, Hentgen V, Saunier A, et al. Lyme borreliosis and other tick-borne diseases. Guidelines from the French Scientific Societies (I): prevention, epidemiology, diagnosis. Médecine Mal Infect. (2019) 49:318–34. doi: 10.1016/j.medmal.2019.04.381
5. Chirio D, Queyrel V, Gonfrier G, Fuzibet JG. Une maladie de Lyme azuréenne. Rev Médecine Interne. (2016) 37:A189–90. doi: 10.1016/j.revmed.2016.04.197
6. Haddad E, Chabane K, Jaureguiberry S, Monsel G, Pourcher V, Caumes E. Holistic Approach in Patients With Presumed Lyme Borreliosis Leads to Less Than 10% of Confirmation and More Than 80% of Antibiotic Failures. Clin Infect Dis. (2019) 68:2060–6. doi: 10.1093/cid/ciy799
7. Lavie E. Haute Autorité de santé - Recommandations de bonne pratique - Borréliose de Lyme et autres maladies vectorielles à tiques (MVT) (2018). Available online at: https://www.has-sante.fr/portail/jcms/c_2857558/fr/borreliose-de-lyme-et-autres-maladies-vectorielles-a-tiques (accessed February 15, 2022).
8. Bouiller K, Klopfenstein T, Chirouze C. Consultation for Presumed Lyme Borreliosis: The Need for Multidisciplinary Management. Clin Infect Dis. (2019) 68:1974. doi: 10.1093/cid/ciy994
9. Jacquet C, Goehringer F, Baux E, Conrad JA, Ganne Devonec MO, Schmutz JL, et al. Multidisciplinary management of patients presenting with Lyme disease suspicion. Médecine Mal Infect. (2019) 49:112–20. doi: 10.1016/j.medmal.2018.06.002
10. Berende A, ter Hofstede HJM, Vos FJ, van Middendorp H, Vogelaar ML, Tromp M, et al. Randomized Trial of Longer-Term Therapy for Symptoms Attributed to Lyme Disease. N Engl J Med. (2016) 374:1209–20. doi: 10.1056/NEJMoa1505425
11. Rudenko N, Golovchenko M, Vancova M, Clark K, Grubhoffer L, Oliver JH. Isolation of live Borrelia burgdorferi sensu lato spirochaetes from patients with undefined disorders and symptoms not typical for Lyme borreliosis. Clin Microbiol Infect. (2016) 22:267.e9-267.e15. doi: 10.1016/j.cmi.2015.11.009
12. Jaulhac B, Saunier A, Caumes E, Bouiller K, Gehanno JF, Rabaud C, et al. Lyme borreliosis and other tick-borne diseases. Guidelines from the French scientific societies (II). Biological diagnosis, treatment, persistent symptoms after documented or suspected Lyme borreliosis. Médecine Mal Infect. (2019) 49:335–46. doi: 10.1016/j.medmal.2019.05.001
13. Dessau RB, van Dam AP, Fingerle V, Gray J, Hovius JW, Hunfeld K-P, et al. To test or not to test? Laboratory support for the diagnosis of Lyme borreliosis: a position paper of ESGBOR, the ESCMID study group for Lyme borreliosis. Clin Microbiol Infect. (2018) 24:118–24. doi: 10.1016/j.cmi.2017.08.025
14. Leeflang MMG, Ang CW, Berkhout J, Bijlmer HA, Van Bortel W, Brandenburg AH, et al. The diagnostic accuracy of serological tests for Lyme borreliosis in Europe: a systematic review and meta-analysis. BMC Infect Dis. (2016) 16:140. doi: 10.1186/s12879-016-1468-4
15. Alby K, Capraro GA. Alternatives to serologic testing for diagnosis of Lyme disease. Clin Lab Med. (2015) 35:815–25. doi: 10.1016/j.cll.2015.07.005
16. Glatz M, Golestani M, Kerl H, Müllegger RR. Clinical relevance of different IgG and IgM serum antibody responses to Borrelia burgdorferi after antibiotic therapy for erythema migrans: long-term follow-up study of 113 patients. Arch Dermatol. (2006) 142:862–8. doi: 10.1001/archderm.142.7.862
17. Bamm VV, Ko JT, Mainprize IL, Sanderson VP, Wills MKB. Lyme disease frontiers: reconciling borrelia biology and clinical conundrums. Pathogens. (2019) 8:299. doi: 10.3390/pathogens8040299
18. Schutzer SE, Coyle PK, Belman AL, Golightly MG, Drulle J. Sequestration of antibody to Borrelia burgdorferi in immune complexes in seronegative Lyme disease. The Lancet. (1990) 335:312–5. doi: 10.1016/0140-6736(90)90606-6
19. Coulter P, Lema C, Flayhart D, Linhardt AS, Aucott JN, Auwaerter PG, et al. Two-Year Evaluation of Borrelia burgdorferi Culture and Supplemental Tests for Definitive Diagnosis of Lyme Disease. J Clin Microbiol. (2005) 43:6. doi: 10.1128/JCM.43.10.5080-5084.2005
20. Bil-Lula I, Matuszek P, Pfeiffer T, Wozniak M. Lyme Borreliosis - the Utility of Improved Real-Time PCR Assay in Detection of Borrelia burgdorferi Infections. Adv Clin Exp Med. (2015) 24:663–70. doi: 10.17219/acem/28625
21. Waddell LA, Greig J, Mascarenhas M, Harding S, Lindsay R, Ogden N. The accuracy of diagnostic tests for Lyme disease in humans, a systematic review and meta-analysis of North American research. PLoS ONE. (2016) 11:e0168613. doi: 10.1371/journal.pone.0168613
22. Jin C, Roen DR, Lehmann PV, Kellermann GH. An enhanced ELISPOT assay for sensitive detection of antigen-specific T cell responses to Borrelia burgdorferi. Cells. (2013) 2:607–20. doi: 10.3390/cells2030607
23. van Gorkom T, Sankatsing SUC, Voet W, Ismail DM, Muilwijk RH, Salomons M, et al. An enzyme-linked immunosorbent spot assay measuring Borrelia burgdorferi B31-specific interferon gamma-secreting T cells cannot discriminate active Lyme neuroborreliosis from past Lyme borreliosis: a prospective study in the Netherlands. J Clin Microbiol. (2018) 56:e01695–17. doi: 10.1128/JCM.01695-17
24. Nordberg M, Forsberg P, Nyman D, Skogman BH, Nyberg C, Ernerudh J, et al. Can ELISPOT be applied to a clinical setting as a diagnostic utility for neuroborreliosis? Cells. (2012) 1:153–67. doi: 10.3390/cells1020153
25. Zomer TP, Vermeeren YM, Landman GW, Zwerink M, van Hees BC, van Bemmel T, et al. Depressive symptoms in patients referred to a tertiary Lyme center: high prevalence in those without evidence of Lyme borreliosis. Clin Infect Dis. (2017) 65:1689–94. doi: 10.1093/cid/cix605
27. Wu X-B, Na R-H, Wei S-S, Zhu J-S, Peng H-J. Distribution of tick-borne diseases in China. Parasit Vectors. (2013) 6:119. doi: 10.1186/1756-3305-6-119
28. Iliopoulou BP, Alroy J, Huber BT. CD28 deficiency exacerbates joint inflammation upon Borrelia burgdorferi infection, resulting in the development of chronic Lyme arthritis. J Immunol. (2007) 179:8076–82. doi: 10.4049/jimmunol.179.12.8076
29. Rebman AW, Crowder LA, Kirkpatrick A, Aucott JN. Characteristics of seroconversion and implications for diagnosis of post-treatment Lyme disease syndrome: acute and convalescent serology among a prospective cohort of early Lyme disease patients. Clin Rheumatol. (2015) 34:585–9. doi: 10.1007/s10067-014-2706-z
30. Cutler SJ, Ruzic-Sabljic E, Potkonjak A. Emerging borreliae – Expanding beyond Lyme borreliosis. Mol Cell Probes. (2017) 31:22–7. doi: 10.1016/j.mcp.2016.08.003
Keywords: Lyme, Borrelia, French Riviera, borreliosis, Ixodes ricinus
Citation: Sevestre J, Benichou A, Rio V, Delaunay P, Gonfrier G, Martaresche C, Carlo V, Nakam S, Mondain V, Carles M, Jeandel PY and Durant J (2022) Emergence of Lyme Disease on the French Riviera, a Retrospective Survey. Front. Med. 9:737854. doi: 10.3389/fmed.2022.737854
Received: 07 July 2021; Accepted: 23 February 2022;
Published: 22 March 2022.
Edited by:
Monica E. Embers, Tulane University, United StatesReviewed by:
Keun Hwa Lee, Hanyang University, South KoreaRina Tilak, Armed Forces Medical College, India
Copyright © 2022 Sevestre, Benichou, Rio, Delaunay, Gonfrier, Martaresche, Carlo, Nakam, Mondain, Carles, Jeandel and Durant. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jacques Durant, ZHVyYW50LmpAY2h1LW5pY2UuZnI=
†These authors have contributed equally to this work and share first authorship