 Chi Zhang
Chi Zhang Lavanya Kodali
Lavanya Kodali Girish Mour
Girish Mour Caroline Jadlowiec
Caroline Jadlowiec Amit K. Mathur1,2*
Amit K. Mathur1,2*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 09 January 2023
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1093126
This article is part of the Research Topic Reviews on the Effect of COVID-19 on Kidney Diseases Diagnosis, Management, and Outcomes View all 8 articles
The SARS-CoV-2 virus precipitated the coronavirus 2019 (COVID-19) pandemic, which placed considerable strain on healthcare systems and necessitated immediate and rapid alterations in the delivery of healthcare. In the transplant population, COVID-19 directly impacts an inherently vulnerable population in the setting of immunosuppression and co-morbidities, but also further complicates the clinical evaluation and management of kidney transplant candidates and recipients in a strained healthcare environment being challenged by the pandemic. Many transplant centers around the world saw mortality rate spikes in organ recipients related to COVID-19, and changes in care delivery abound. This review evaluates the care of the kidney transplant patient through all phases of the process including pre-operative evaluations, perioperative care, post-transplantation considerations, and how the global pandemic has changed the way we care for our patients.
Despite nearly 100,000 patients on the US waiting list, kidney transplant (KT) remains the most optimal therapy for end-stage renal disease (ESRD), with survival, quality of life, and cost advantages over other forms of renal replacement therapy (RRT) (1, 2). Though KT has clear benefits over other RRT modalities, the rate of pre-emptive KT was only 3% in the United States in 2016 (3, 4). A critical barrier in access to transplant is a lack of timely referral to the transplant center (5). Multiple demographic and system-level characteristics, many of which are non-modifiable, have been associated with lower rates of KT referral, including older candidate age, minority race/ethnicity, lower socioeconomic status, employment status, medical literacy, and dialysis unit ownership (6–12).
Further expansion of the KT waitlist candidate pool is critical in providing equitable care to the ESRD community. While the US has the most successful deceased donation program in the entire world, there is tremendous variability in organ donation rates, kidneys recovered, and recovered kidneys utilized for transplant across the US (13). Non-utilization of kidneys recovered from deceased donors is a critical issue that varies based on organ procurement organization (OPO) performance, transplant center acceptance patterns, and the intrinsic health status of donors at the time of death (14). Greater emphasis on living donor kidney transplantation is a potential solution to these shortcomings in deceased donor system and has the potential to address the needs of the entire waitlist. Living donation had increased in the US in the years leading up to the pandemic, culminating in 6,866 living donor transplants in 2019, but only accounted for 38% of all US KTs (13). Underlying socioeconomic status may limit current donor availability and recipient access. Within the same geographic area, African American living donor candidates were less likely to progress from referral to donation and some have shown that African American donor candidates have a longer median time from screening to donation compared to other races (15). Despite near universal access to Medicare coverage for KT, African American patients and those from a lower socioeconomic class are less likely to undergo LDKT and have a lower likelihood of being listed for transplant (16–21).
The COVID-19 pandemic exacerbated an already stressed system and highlight deficiencies in all phases of care, resulting in innovation. This review focuses on the impact of COVID-19 on kidney donation and transplantation.
Pre-transplant care entails a series of interwoven processes that begins with evaluation at a transplant center, involves a myriad of diagnostic tests and clinical evaluations, and the provision of dialysis care during this time when the patient is away from their normal home institutions. The subsequent decision on whether to list the patient for transplant involves distillation of medical, surgical, and psychosocial evaluations and the input of several professionals from a multidisciplinary transplant team. The time from referral for transplant to evaluation initiation is highly variable across centers, and the entire process can extend to more than a year (22). Waitlisted candidates must wait, either to receive a kidney from their living donor or for a potential deceased donor kidney. This process can often be protracted. In the absence of a living donor, patients in the United States can wait over 7 years for a deceased donor KT, depending on their donor-specific antibody profile (23, 24).
With the onset of the pandemic, pre-transplant care delivery underwent a substantial disruption of normal processes. Due to the desire to have patients avoid excessive interactions with the hospital, care needed to be streamlined to achieve the same diagnostic accuracy to judge fitness for transplant but keep patients safe from the potential spread of the virus.
Living kidney donor evaluation is detailed and known for its rigor, which is aimed at minimizing donor risk. While there is some variability in transplant center approaches, living donor evaluations begin with screening, initial interviews with independent living donor advocates, social workers, and sometimes clinical team members. Blood and tissue typing are also essential components. If deemed suitable to proceed with an evaluation, the potential donor would proceed to subsequent testing which would include medical and surgical consultation, and diagnostic batteries that include blood pressure monitoring, blood and urine tests, cardiac function screening (EKG and echocardiogram), cross-sectional imaging, and other consultations with specialists in social services, nutrition, nursing, urology, transplant psychology and psychiatry, and pharmacy. The multidisciplinary team will approve them to move forward with donation or rule them out due to a variety of reasons, but donors may withdraw from the process at any time including right up to the time of surgery. These evaluations occur in parallel or in series with recipient evaluations. Once a living donor is approved, donors may donate directly to their intended recipient if one is designated and approved, or they may be entered into a paired kidney exchange to optimize donor-recipient matching (25). While the extensive evaluation process is rooted in safety for both the donors and for the recipient, the process can be perceived as arduous.
When there is not a living donor available, most others receive allografts from deceased donors. Brain dead donors present to the hospital antemortem and are declared braindead after a series of provocative bedside neurologic tests to suggest irreversible cessation of brainstem activity. Unlike brain death donors, donation after cardiac death donors often suffer severe injury but do not fulfill the criteria for brain death. However, if by family decision or by advance directive, they may still be able to donate once the family decides to withdraw life support. In both scenarios, the patients are referred to organ procurement organizations (OPOs) and organ donation authorization is pursued. Donor histories, diagnostic laboratory tests (including biopsy), and cross-sectional imaging are obtained, and families are counseled. Once consent is obtained and the patients are deemed medically appropriate for donation, organs are subsequently offered to transplant programs. If accepted, the procurement team arrives to the operating room and begins recovery (26). COVID-19 presented a disruption to the process as donors required testing prior to organ allocation. A positive test, depending on the transplant center, the availability of a willing recipient, and the timing within the pandemic, could obfuscate the donation process entirely. However, the universal acknowledgment of COVID-19 and the requirement to test all deceased donors in the US within the first months of the pandemic was critically important in allowing for the continuation of deceased donations as regulations on procurement loosened with time and with the greater availability of data on COVID positive donors (27).
Challenges in living donor and deceased organ donation were certainly exacerbated at the advent of the COVID-19 pandemic. Transplant centers around the world saw a decline in both deceased and living kidney donation by up to 90% in some European countries (28–34). For living donors, there was concern for contracting COVID-19 in the process of an elective procedure. Hospitals were being overrun by symptomatic COVID-19 patients requiring general and intensive care, which disincentivized time-intensive deceased donor processes including donation authorization, clinical management, and placement with transplant centers. The COVID-19 pandemic ushered in a novel and unseemly dilemma. Clinical teams felt they were choosing between two evils: Accepting waitlist mortality by post-poning transplantation or accepting potential detrimental outcomes related to post-operative recovery and immunosuppression from the virus itself or delays in care (35). Clearly, process changes were necessary and telemedicine helped bridge barriers (36).
As the pandemic evolved in the early months of 2020, it was evident that all health care including transplant and living donor care needed to evolve. The high potential of droplet transmission of the SARS-CoV-2 virus between individuals represented a threat to both patients and to providers. In order to ensure the continuation of care consultations, hospitals and clinics around the globe developed telemedicine protocols using multiple platforms (37, 38). Telemedicine included a variety of types of patient-provider interactions including telephone consultations/visits, virtual visits using video conferencing, and other schemes. The demand for remote and virtual visits with physicians, which was relatively boutique prior to the pandemic, rapidly became a daily practice (39–41).
In transplantation, telemedicine adoption filled a tremendous gap at a time of uncertainty and global paranoia. The outcomes of COVID-19 disease were still evolving, and geographic hot-spots of disease came and went, all while overwhelming healthcare facilities and providers. There was tremendous worry about the impact of COVID-19 disease on immunocompromised individuals that emerged from the very first reports of the virus. Telemedicine helped address the continued need to provide care in all phases of transplant care as needed while minimizing the risk of viral transmission to pre-transplant, peri-transplant, and post-transplant patients, as well as health care providers (42–48).
Transplant centers started the living donor evaluation process remotely, especially in patients who had limited capacity to travel. Meetings with living donor advocates, preoperative education, and informed consent could be conducted virtually, while laboratory and imaging tests be completed locally or at the transplant center using social distancing, masking, and droplet precautions. Transplant centers re-evaluated their protocols with an eye toward streamlining the entire living donor candidate care paradigm. Consultations were consolidated as multiple specialists could be seen concurrently. With the evaluation complete, only if a patient is deemed to be a suitable donor by the transplant team would the donor candidate be required to travel to the transplant center a few days prior to the scheduled kidney transplant surgery. Telemedicine and virtual donor evaluation demonstrated multiple potential benefits. For living donor candidates, virtual evaluation was financially advantageous as it required minimal travel in the evaluation phase. For the transplant center, telemedicine could also increase access to LDKT because more evaluations can be completed (36).
A similar process applied to transplant candidate evaluation. Preoperative laboratory tests could be conducted locally and shared digitally with the transplant center through the electronic medical record and diagnostic lab system inputs. Transplant evaluations were completed with one or sometimes no in-person visits, depending on the clinical history and risk. Some centers would list patients inactive on the waiting list once the evaluation was complete, and would activate them after an in-person visit and clinical exam (49).
Healthcare lags in the adoption of new technologies compared to other industries. Prior to the pandemic, large corporations and businesses conducted their work frequently using digital video-based platforms. These were not common technologies used in the daily work of transplant clinicians. However, since the advent of clinical transplantation, multidisciplinary transplant teams have met together physically to discuss the selection and listing of transplant candidates and approval of living donors. It is a near-universal activity in transplant centers. Administrative processes often required in-person meetings to resolve day-to-day operational issues prior to the pandemic. In order to minimize the risk of viral transmission and COVID-19 disease within a transplant center’s workforce, efforts to reduce in-person meetings and conferences were rapidly adopted in the early months of the pandemic. In-person selection and listing conferences were transitioned to group virtual meetings (50). While there were initial technological challenges to surmount, digital platforms for clinical and administrative meetings became commonplace. In our center, one unintended benefit of this development was that pre-existing limitations in our transplant center physical space were overcome through the use of digital platforms. Everyone on the multidisciplinary transplant team could fit in one “room” when discussing patients, including nephrologists, surgeons, nurses, social workers, dieticians, pharmacists, other medical specialists, financial coordinators, living donor advocates, and administrators. Mirroring other industries, transplant centers could provide its staff with opportunities for remote work which provided much-needed flexibility to clinical and non-clinical personnel. Digital platform adoption for virtual meetings not only revolutionized patient interactions, but also interprofessional interactions as well.
Perhaps one of the most important early breakthroughs in the pandemic was the availability of antigen testing for transplant candidates, living donors, and deceased donors. Near-universal clinical testing in early 2020 was critical in assessing real-time safety to proceed with transplant, evaluating potential viral transmission through donation and transplant, and managing resources as test results influenced utilization of personal protective equipment (PPE), anesthesia and perioperative care processes, use of respiratory isolation protocols. Positive tests in transplant candidates at the time of organ offer are frequently associated with organ decline and transplant cancelation and reactivation on the waiting list after recovery from illness or 7–10 days if the transplant candidate is asymptomatic (51). In the post-transplant setting, testing impacts in-hospital and post-operative management (52–54).
Global practices varied in the early days of the pandemic. Deceased and living donor candidates with either COVID-19 exposure or positive tests were often excluded from donation, and some centers chose to rely more on local deceased organs where the regional COVID-19 rates were known and detection rate could be better trusted (30, 34). Many transplant hospitals applied triage systems to transplant candidates, opting in the early days of the pandemic and during disease surges to place living donor transplants and combined kidney-pancreas transplants on hold, as an example. While these decisions were largely driven by the availability of local hospital resources and clinical judgment of the perceived urgency of transplant, they are not without repercussions. In England, patients who are removed from the waitlist for clinical reasons that predate the onset of COVID-19 had worse patient and graft survival, even if they were transplanted within 5 years following suspension (4). More recent studies have indicated that practice changes related to COVID-19 has been associated with an increase in waitlist hospitalizations and deaths as well as deaths in those who were never able to be evaluated for transplant candidacy (55, 56).
Transplant professionals rapidly realized the need for consolidated best practice guidance in all aspects of clinical transplantation in the early pandemic. The American Society of Transplant Surgeons (ASTS) formed a COVID-19 Strike Force to compile evidence-based guidelines. As the United States entered isolation in March 2020, the Strike Force stated that the main goals at the time were (1) Protect healthcare providers, (2) Treat patients with the virus, and (3) Prevent transmission to others. Transplants were thus only performed in acute life-threatening situations, all living donations were suspended, and local procurements were recommended to prevent transmission of the virus to procurement teams during travel. As the pandemic has continued, and as we have gained knowledge about the virus, the Strike Force recommendations evolved. While procurement team safety was still paramount, COVID-19 no longer prohibited travel nor transplantation. Other recommendations respected autonomy of transplant teams in accepting donor organs with previous COVID-19 infection and urged focus on this factor as a consideration on overall organ quality. Recommendations considered donors non-contagious 10 days after the onset of symptoms and significant recovery of organ function was expected after the initial viral inflammatory response had abated. While living donation had been active in multiple centers after the first 3 months of the pandemic, it was endorsed by the Strike Force once again by June 2020 (57). With experience and time, societies and individual transplant centers became more comfortable with using organs from COVID-19 positive donors, both from donors with asymptomatic infection and death from other causes, as well as donors who died of COVID-19 disease. Protocols for the utilization of these organ donors were developed, but COVID-19 donor transmission in non-lung solid organ transplantation continues to be rare but is considered to be unknown (58, 59).
Multiple national organizations have set forth newer guidelines, however, all recommendations come with the caveat of having insufficient long-term evidence surrounding this novel virus (60).
The National Institute of Health (NIH), American Society of Transplantation and the Organ Procurement and Transplantation Network (OPTN) published similar guidelines with a few minor differences (61–63). PCR testing within 72 h of deceased organ procurement, ideally as close to organ recovery as possible, and testing within 72 h prior to surgery for living donors was recommended. The specimens should be from respiratory sites using PCR because rapid antigen and non-respiratory testing lack sufficient evidence. It is recommended to defer transplant if either the donor or recipient tests positive for COVID-19 or if infection is strongly suspected. According to the AST, those who have had resolution of symptoms but continue to test positive within 21–90 days of disease onset are considered low risk for transmission. Both the AST and OPTN state that a positive test 21–90 days after resolved COVID-19 symptoms, a positive test 10–21 days after symptom onset, asymptomatic donors with an incidental positive test, and resolved COVID-19 with a positive test > 90 days can all be considered for non-lung organ acceptance. Though the guidelines state organ acceptability from an infectious disease standpoint, a positive test 90 days after resolution of initial COVID-19 infection could potentially represent re-infection. Additionally, the AST states that death related to COVID-19 complications can also be considered for non-lung acceptance. Though an increasing number of non-lung organs from positive donors have not shown evidence of recipient transmission, with all cases, the risk of waitlist mortality should be weighed against mortality in donor-derived infection (Table 1). A negative rapid antigen test is unacceptable if there is suspicion for infection and a confirmatory PCR test is necessary in these cases.
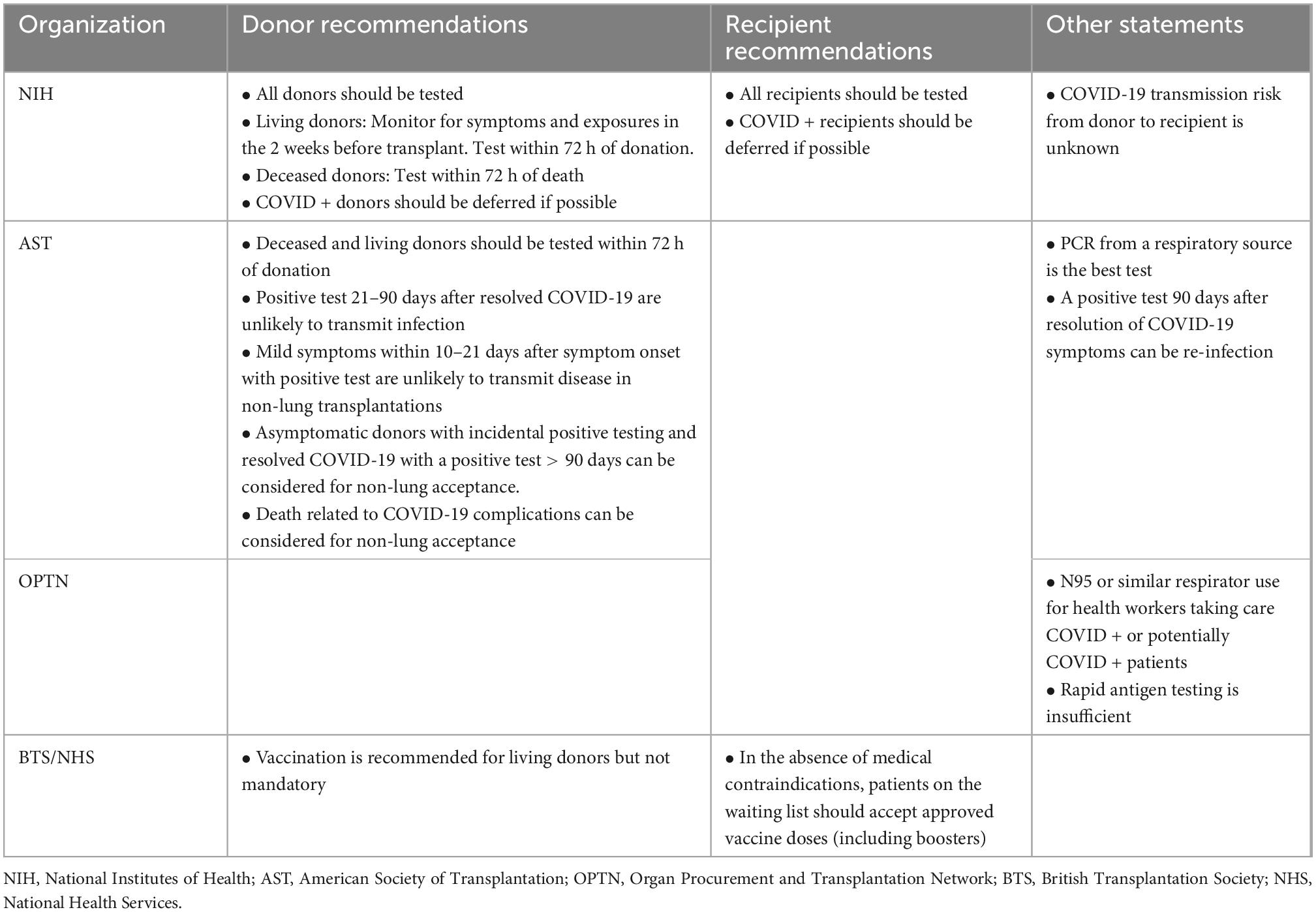
Table 1. National organization recommendations for COVID-19 testing.
When the coronavirus first emerged in Wuhan, China at the end of 2019, it was unexpectedly virulent and led to unprecedented lockdown measures in the country. Similar measures were taken when the virus arrived in the Western world, but with varying degrees of success in controlling the spread. While it became obvious that immunization would be necessary, vaccine development is also a daunting task, leading the US Department of Health and Human services to create “Operation Warp Speed” to expedite the process (64). Traditionally, vaccinations are inoculations of either deactivated or a live attenuated virus to stimulate human B lymphocytes to produce antibodies. However, time pressure and the novelty of the virus itself led to the development of messenger RNA that encode the blueprint of the SARS-CoV-2 spike protein. While the spike protein is foreign to us, it is abundant on the surface of the virus, allowing B cells in the vaccinated person to produce antibodies that can neutralize the virus (65–67). By mid-summer, the two leading companies, Moderna and Pfizer, published promising clinical trial results, showing that both vaccines induced anti-SARS-CoV2 immune responses in all participants (68, 69). A few months later, both vaccines received emergency use authorization (70).
Of course, immunology is much more complicated, and we present a simplified version of the evidence. In the aftermath of vaccination, hospitals and national studies continued to identify COVID-19 as the leading cause of death in solid organ transplant recipients after the onset of the pandemic, some within the first year of transplant but noted throughout the post-transplant course (71). In the solid organ transplant population, elevated age, use of antimetabolite medications, recent transplant, and receiving a kidney allograft are all indirectly proportional to the level of anti-spike antibody, an oft used surrogate for immunity after vaccination (72–74). The immune response of transplant patients was more muted compared to the general population. Poor post-vaccination humoral responses have led to France’s early adoption of a third vaccination injection in dialysis and in transplant patients (75). The NIH also has a clinical trial underway to study if immune responses to vaccination improve when immunosuppression medication is temporarily reduced in the days leading up to and following vaccination (76, 77). Though still unmatched to the general population, as boosters became available in the US, data shows that additional mRNA inoculations increase antibody titers for the majority of solid organ transplant patients (78, 79).
Despite our increasing molecular understanding of the virus, in the fall of 2021, a woman in Colorado with ESRD was denied kidney transplantation due to her and her living donor’s unvaccinated status, sparking national political debate and fierce media coverage (80–84). She was informed that her status on the waitlist would be inactivated if she were not to start the vaccination series within 30 days and vaccination refusal warranted removal from the kidney transplant list. She cited religious grounds and uncertainties about the vaccine itself as reasons for her hesitancy and reported feeling coerced by the hospital system. Despite the publicity, University of Colorado Health held firm on their decision, stating that patients undergoing organ transplant have higher mortality rates in unvaccinated organ recipients who contract COVID-19 and that transplant candidates are routinely subject to health requirements, including vaccinations as well as abstaining from tobacco and alcohol (85).
Though the media coverage of the Colorado case was intense, vaccine hesitancy long predates the pandemic. Vaccination discussions have historically centered around children. In recent years, parental refusal for non-medical reasons such as religion and uncertainties about the vaccine itself have become increasingly common in the general and transplant pediatric population (86–88). Some of this hesitancy can be linked to the now admittedly falsified studies linking vaccines to autism (89). The American Academy of Pediatrics and the American Society of Transplantation (AST) recommends complete appropriate vaccinations prior to solid organ transplantation, but up to 70% of children are incompletely vaccinated before surgery because most of the times, the children were either too young or too sick to be immunized at the appropriate ages (90, 91). When presented with a hypothetical situation of a parent refusing all vaccinations for non-medical reasons prior to solid organ transplant, programs responded very differently: 47% would list the patient, 22% would not, and 30% were unsure. Additionally, only 4% of pediatric transplant programs had a written policy regarding vaccine refusal (92).
Most vaccination literature exists in the pediatric population, and adult practices lacked attention until the COVID-19 pandemic. While many transplant centers have developed a vaccination policy since the Colorado case, no strict national policy exists currently. The most recent joint statement with ASTS, AST, and the International Society of Heart and Lung Transplantation in March 2022, officially recommends all eligible transplant candidates, donors, and caretakers be vaccinated, ideally 2 weeks prior to surgery with two vaccinations plus boosters, but ultimately, individual centers should make the final decision and have clear and understandable policies (93). Proponents of having universal guidelines state that vaccinations protect the recipient and the allograft from vaccine-preventable disease, protects other patients and healthcare workers in the clinical setting, and maximizes the benefits of scarce organs. The opposition argue that vaccination requirements may cause irreversible harm to patients who refuse, violate patient autonomy, and create additional barriers to marginalized groups (94).
Similar discussions occurred in Europe. While persuasive arguments could be made for and against vaccine mandates, the NHS Blood and Transplant and the British Transplant Society urged physicians to discuss the benefits and repercussions of vaccine refusal, but ultimately do not mandate vaccination for transplant candidacy in a public joint statement in 2021 (95, 96).
Individual transplant programs have struggled with the impact of COVID-19-related mortality in their post-transplant patients (97). Since the pandemic, COVID-19 has been a leading cause of post-transplant mortality, particularly in patients with prolonged immunosuppression (98). Transplant outcome public reporting emphasize graft survival and patient survival in the first 3 years after transplant, and so many programs have developed COVID-19 vaccination policies to ensure continuation of strong post-transplant outcomes. Excess graft loss or death related to COVID-19 has significant impact on transplant programs with regard to quality rankings, which ultimately could affect their standing with commercial payers. The development of these policies has been met with controversy. COVID-19 vaccine mistrust has frequently been shaped as a political statement and vaccination rates have varied geographically. Transplant programs have received feedback from referring physicians and patients expressing their lack of trust or refusing vaccines altogether. Transplant programs have also had to contend with their own vaccine requirements—how to navigate the creation of a COVID-19 vaccine mandate for transplant candidacy if other vaccines (hepatitis B, MMR, etc.) were not absolutely required for listing. The pandemic has presented many challenges to clinical transplant program policy development and will likely do so as we evaluate epidemiologic trends in disease, clinical outcomes of COVID-19 with new variants, and whether low severity infections will become the norm as SARS-CoV-2 becomes endemic.
In the US and globally, economically, and socially disadvantaged groups were disproportionally affected by COVID-19 infections (99, 100). Though African Americans represented 10% of the solid organ transplant population at one center, they made up 50% of the COVID-19 positive cohort (101). While vaccination requirements can potentially exacerbate preexisting mistrust in the healthcare system due to historical mistreatments of disadvantaged communities, interventions that attenuate the clinical impact of COVID-19 disease exist (102). For the extremely marginalized population, addressing their basic needs for survival such as access to food, shelter, and basic healthcare opens avenues for vaccination (103). Additionally, most early interventions for vaccination refusal have centered around the Information Deficit Model (104). Though correcting misinformation about vaccinations did not elicit behavioral change, a trusting relationship between patients, their caregivers, and providers that provides unbiased vaccine information increased vaccination rates in those diametrically opposed to immunization previously (105–108). In the modern era, social media has worked well to encourage the partially vaccinated to complete their series.
US Transplant programs have also developed clinical pathways to vaccinate patients for COVID-19 during the transplant evaluation phase through vaccination appointments with transplant center providers or piggybacking on other appointments to optimize patient convenience as well as obeisance to transplant center vaccination policies for candidates and living donors. Ultimately, transplant programs will need to closely monitor the progression of SARS-CoV-2 epidemiology to inform vaccine policy mandates. Furthermore, transplant programs are currently navigating the development of clinical pathways for utilization of monoclonal antibodies that serve as spike protein attachment inhibitors for the virus as pre-exposure prophylaxis (EVUSHELD™, tixagevimab co-packaged with cilgavimab) (109). The exorbitant mortality observed in 2020 and 2021 in the post-transplant population has given transplant programs the experience it needs to adapt with regard to policies and the availability of new therapeutics.
From May 2021 to Feb 2022 in the US, 455 non-lung organs were transplanted from donors with a positive COVID-19 test, with 278 transplants being kidneys (62). So far, results of donor-derived COVID-19 transmission during transplantation are rare (110). In an Italian series, 10 urgent transplant need patients received livers from deceased brain death donors who either had positive COVID-19 testing at time of transplant or had previously been infected. Of the 10 recipients, 5 had history of severe COVID-19 infection requiring hospitalization before transplant. Eight tested negative and two tested positive for COVID-19 in the immediate preoperative setting using a respiratory source sample. The 8 patients who tested negative prior to surgery continued to test negative after transplantation with a potentially infected donor organ, and none of the 10 patients experienced any COVID-19 related symptoms (59). Another study showed that two recipients who were COVID-19 negative prior to transplant remained negative post-liver transplantation with organs from incidentally positive donors without known history of COVID-19 infection. Interestingly, one of the recipients was unvaccinated (111). Despite documented successes, it is unclear how protective vaccination (or even partial vaccination) in recipients is against organs from COVID-19 positive donors. What is clear is that herd immunity applies to small communities as well. Unvaccinated caretakers have an increased chance of spreading COVID-19 to recipients, and if infected, vaccinations lessen the severity of disease if the recipient contracts COVID-19 post-transplantation (58, 112).
Toward the beginning of the pandemic, studies in the United States cited mortality rates of 13–28% in kidney transplant recipients who subsequently test positive for COVID-19. Those who were hospitalized for COVID-19 related complications had even higher mortality rates (113). Even when patients survive, they still had an 8–21% chance of requiring renal replacement therapy, a rate much higher compared to those who were not infected (114). Dauntingly high mortality rates were also seen in European transplant centers, with mortality rates ranging from 5 to 36% (115, 116). Though most early studies were single-center experiences, the TANGO International Transplant Consortium compiled data from 12 centers across the United States, Spain, and Italy of kidney transplant recipients who tested positive for COVID-19 and reported 52% AKI, 29% respiratory failure requiring mechanical ventilation, and 32% mortality (99). The need for hemodialysis as well as graft loss are thought to be sequela of acute kidney injury (AKI), a frequent COVID-19 complication affecting up to 50% of all post-renal transplant patients (117).
Additionally, while transplant patients are at high risk for severe symptomatic COVID-19 infection due to chronic immunosuppression, their other medical comorbidities also contribute to their high mortality rates (118). Elevated age, diabetes mellitus, obesity, chronic heart disease, chronic kidney disease, lung disease, and longer dialysis were all associated with higher morality (99, 101, 119–123). While the exact immunological mechanisms are unknown, age and comorbidities, not immunosuppression, may be driving the high mortality rate (124). Despite a reduced humoral response in the setting of medically induced immunosuppression, the crude mortality rate for COVID-19 positive patients on hemodialysis (30%) was higher compared to those who underwent kidney transplantation (15%) as well as the general population (14%) in one study (125).
Clearly, post-transplantation patients still require careful monitoring and care. Fortunately, technology can help ensure post-transplant continuity of care by helping mitigate similar logistical challenges surrounding geography and finances that patients experienced before surgery (126, 127). Regular appointments are important for monitoring immunosuppression and progress post-operatively. Patients have been shown to have improved adherence and reduced readmission rates after transplantation when followed virtually. Additionally, this group had better disease-specific quality of life and quicker return to employment, which is potentially attributable to increased self-care responsibility (128). Interestingly, increases in self-accountability and self-management did not change patient perception of the quality of care received compared to traditional face-to-face appointments (129). Benefits can also extend to living donors. Nearly half of the transplant centers lose contact with > 75% of donors within 2 years post-donation due to costs to donors and out of date contact information, which has limited our understanding of long-term outcomes following living donation (130, 131). Information on safety metrics could change the way we care for living donors and potentially encourage more altruistic donations. Therefore, telemedicine presents exciting future opportunities and avoids donor financial burden related to travel in the present.
Technology also has limitations. Though most patients have access to smartphones and to the internet, individuals with minimal technology experience may require assistance in navigating the visit platform. So, this will necessitate transplant centers to have troubleshooting support available. There will also need to be legislation changes. Under the state of public health emergency, CMS as well as some private payors reimburse telemedicine visits across state lines at the same rate as an in person visit. However, access may change as the world moves away from the pandemic (132–134). Continued reimbursement of virtual/telemedicine care is a critical issue in solid organ transplantation as it has facilitated access to transplant as well as improved access to post-transplant and post-donation care. Virtual interfaces also limit parts of the clinical interaction, the ability to perform physical examination, and the possibility of weight-based medication dosing (135).
As the world readjusts to the new post-pandemic normal, the transplant community should continue to embrace the ability to deliver quality care through telemedicine. While the strain on hospital access and social distancing and isolation may lessen, patients in remote areas of the country will still require access to transplant centers. These can be opportunities to explore and to develop acute hospital at home models, which have been shown to reduce readmissions and cost while improving patient experience following non-transplant surgeries (136–139).
At our high-volume transplant center, donors and recipients are tested according to national society guidelines prior to transplant, which continue to change. For living donors and all recipients, vaccination is highly encouraged and an important part of the preoperative candidacy evaluation. Our institutional practice has also changed overtime. Rather than performing routine biopsies from all COVID-19 positive donors, procurement biopsies are now being used in a case-by-case basis to add reassurance in utilizing organs from COVID + donors that have significant clinical symptoms. Post-operative biopsies are typically reserved for evidence of organ dysfunction or injury. Recipients are monitored daily for symptoms related to COVID-19 for the next 14 days but are dismissed from the hospital if clinically able. If the patients are discharged before 2 weeks, then they are encouraged to isolate and to self-monitor for symptoms. Blood samples are drawn at regular intervals (2, 7, 14, 21, and 28 days) for detection of spike protein and nucleocapsid antibodies. Routine PCR antigen tests are also performed on respiratory samples. Patients receive monoclonal antibody post-exposure prophylaxis as well as empiric antiviral treatments.
When outpatient, our institutional practice is to reduce immunosuppression for 2–4 weeks when patients who test positive for COVID-19. Those who are admitted for symptomatic infections will have discontinuation of their antiproliferative medication, trough level measurements for tacrolimus/cyclosporine, daily steroid use, and infectious disease consultation. In general, off label use of hydroxychloroquine for prophylaxis was specifically not recommended due to lack of data, shortages, and risk of QT prolongation.
At the peak of the pandemic, many hospitals, including ours, adopted a no visitation policy to prevent community transmission (140). As healthcare organizations reopened from the pandemic, our hospitals allowed limited visitors (1–2 per day) for COVID-19 patients. Visitors would be screened for symptoms prior to entering the hospital, asked about exposures, and have their temperature taken. While visiting, they are required to wear a mask and be limited to the confines of the patient’s room (141). Patients who test positive for the virus would not be able to have in-person visitors.
In conclusion, the global pandemic has been challenging for kidney transplant programs worldwide. Policy changes in the United States have helped mitigate some of the cost and access issues to healthcare. Research has prevented deaths in the form of rapid vaccine development and helped in the management of COVID-19 related complications in the transplant population. Despite the hardships, the pandemic also brought forth practice changes that can help with longstanding problems of access through more widespread use of telemedicine. As the world emerges from the shock of the pandemic, we must carry forward the lessons we have learned and the tools we have garnered.
CZ and AM: conception, design, and draft manuscript preparation. CZ: literature review. All authors reviewed and approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C, et al. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. (1996) 50:235–42. doi: 10.1038/ki.1996.307
2. Wolfe R, Ashby V, Milford E, Ojo A, Ettenger R, Agodoa L, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. (1999) 341:1725–30. doi: 10.1056/NEJM199912023412303
3. National Institutes of Health. Chapter 1: Incidence, prevalence, patient characteristics, and treatment modalities. In United States renal data system progress through research. Bethesda, MD: National Institutes of Health (2018).
4. Wallace D, Robb M, Hughes W, Johnson R, Ploeg R, Neuberger J, et al. Outcomes of patients suspended from the national kidney transplant waiting list in the united kingdom between 2000 and 2010. Transplantation. (2020) 104:1654–61. doi: 10.1097/TP.0000000000003033
5. van Dellen D, Burnapp L, Citterio F, Mamode N, Moorlock G, van Assche K, et al. Pre-emptive live donor kidney transplantation-moving barriers to opportunities: An ethical, legal and psychological aspects of organ transplantation view. World J Transplant. (2021) 11:88–98. doi: 10.5500/wjt.v11.i4.88
6. Lentine K, Pastan S, Mohan S, Reese P, Leichtman A, Delmonico F, et al. A roadmap for innovation to advance transplant access and outcomes: a position statement from the national kidney foundation. Am J Kidney Dis. (2021) 78:319–32. doi: 10.1053/j.ajkd.2021.05.007
7. Barth A, Szõllõsi G, Nemes B. Factors affecting access to the kidney transplant waiting list in eastern hungary. Transplant Proc. (2021) 53:1418–22. doi: 10.1016/j.transproceed.2021.01.044
8. Hamoda R, Patzer R, Wan W, Saunders M. 347.6: Racial-Ethnic and sex disparities in access to renal transplant waitlisting vary by age in the united states. Transplantation. (2022) 106:S357. doi: 10.1097/01.tp.0000887348.69110.f3
9. Urbanski M, Patzer R. Measuring disease and transplant knowledge among patients with advanced CKD: Tools to increase access and advance equity. Clin J Am Soc Nephrol. (2022) 17:481–3. doi: 10.2215/CJN.02140222
10. Wilk A, Cummings J, Plantinga L, Franch H, Lea J, Patzer R. Racial and ethnic disparities in kidney replacement therapies among adults with kidney failure: an observational study of variation by patient age. Am J Kidney Dis. (2022) 80:9–19. doi: 10.1053/j.ajkd.2021.12.012
11. Mathur A, Ashby V, Sands R, Wolfe R. Geographic variation in end-stage renal disease incidence and access to deceased donor kidney transplantation. Am J Transplant. (2010) 10(4 Pt 2):1069–80. doi: 10.1111/j.1600-6143.2010.03043.x
12. Reed R, Sawinski D, Shelton B, MacLennan P, Hanaway M, Kumar V, et al. Population health, ethnicity, and rate of living donor kidney transplantation. Transplantation. (2018) 102:2080–7. doi: 10.1097/TP.0000000000002286
14. Li M, King K, Husain S, Schold J, Mohan S. Deceased donor kidneys utilization and discard rates during COVID-19 pandemic in the united states. Kidney Int Rep. (2021) 6:2463–7. doi: 10.1016/j.ekir.2021.06.002
15. Kumar K, Tonascia J, Muzaale A, Purnell T, Ottmann S, Al Ammary F, et al. Racial differences in completion of the living kidney donor evaluation process. Clin Transplant. (2018) 32:e13291. doi: 10.1111/ctr.13291
16. Muzaale A, Massie A, Al Ammary F, Henderson M, Purnell T, Holscher C, et al. Donor-Recipient Relationship and Risk of ESKD in Live Kidney Donors of Varied Racial Groups. Am J Kidney Dis. (2020) 75:333–41. doi: 10.1053/j.ajkd.2019.08.020
17. Mathur A, Stewart Lewis Z, Warren P, Walters M, Gifford K, Xing J, et al. Best practices to optimize utilization of the National Living Donor Assistance Center for the financial assistance of living organ donors. Am J Transplant. (2020) 20:25–33. doi: 10.1111/ajt.15684
18. Gore J, Danovitch G, Litwin M, Pham P, Singer J. Disparities in the utilization of live donor renal transplantation. Am J Transplant. (2009) 9:1124–33. doi: 10.1111/j.1600-6143.2009.02620.x
19. Purnell T, Luo X, Cooper L, Massie A, Kucirka L, Henderson M, et al. Association of race and ethnicity with live donor kidney transplantation in the united states from 1995 to 2014. JAMA. (2018) 319:49–61. doi: 10.1001/jama.2017.19152
20. Axelrod D, Dzebisashvili N, Schnitzler M, Salvalaggio P, Segev D, Gentry S, et al. The interplay of socioeconomic status, distance to center, and interdonor service area travel on kidney transplant access and outcomes. Clin J Am Soc Nephrol. (2010) 5:2276–88. doi: 10.2215/CJN.04940610
21. Peng R, Lee H, Ke Z, Saunders M. Racial disparities in kidney transplant waitlist appearance in Chicago: Is it race or place? Clin Transplant. (2018) 32:e13195. doi: 10.1111/ctr.13195
22. Monson R, Kemerley P, Walczak D, Benedetti E, Oberholzer J, Danielson K. Disparities in completion rates of the medical prerenal transplant evaluation by race or ethnicity and gender. Transplantation. (2015) 99:236–42. doi: 10.1097/TP.0000000000000271
23. Mathur A, Xing J, Dickinson D, Warren P, Gifford K, Hong B, et al. Return on investment for financial assistance for living kidney donors in the United States. Clin Transplant. (2018) 32:e13277. doi: 10.1111/ctr.13277
24. Hart A, Lentine K, Smith J, Miller J, Skeans M, Prentice M, et al. OPTN/SRTR 2019 annual data report: Kidney. Am J Transplant. (2021) 21(Suppl 2):21–137. doi: 10.1111/ajt.16502
26. Girlanda R. Deceased organ donation for transplantation: Challenges and opportunities. World J Transplant. (2016) 6:451–9. doi: 10.5500/wjt.v6.i3.451
28. Angelico R, Trapani S, Manzia T, Lombardini L, Tisone G, Cardillo M. The COVID-19 outbreak in Italy: Initial implications for organ transplantation programs. Am J Transplant. (2020) 20:1780–4. doi: 10.1111/ajt.15904
29. Cholankeril G, Podboy A, Alshuwaykh O, Kim D, Kanwal F, Esquivel C, et al. Early Impact of COVID-19 on Solid Organ Transplantation in the United States. Transplantation. (2020) 104:2221–4. doi: 10.1097/TP.0000000000003391
30. Domínguez-Gil B, Coll E, Fernández-Ruiz M, Corral E, Del Río F, Zaragoza R, et al. COVID-19 in Spain: Transplantation in the midst of the pandemic. Am J Transplant. (2020) 20:2593–8. doi: 10.1111/ajt.15983
31. Gumber L, Gumber A. COVID-19 and ‘lockdown’ in organ transplantation in the UK. Public Health. (2020) 185:55–6. doi: 10.1016/j.puhe.2020.06.017
32. Loupy A, Aubert O, Reese P, Bastien O, Bayer F, Jacquelinet C. Organ procurement and transplantation during the COVID-19 pandemic. Lancet. (2020) 395:e95–6. doi: 10.1016/S0140-6736(20)31040-0
33. Boyarsky B, Po-Yu Chiang T, Werbel W, Durand C, Avery R, Getsin S, et al. Early impact of COVID-19 on transplant center practices and policies in the United States. Am J Transplant. (2020) 20:1809–18. doi: 10.1111/ajt.15915
34. Vistoli F, Furian L, Maggiore U, Caldara R, Cantaluppi V, Ferraresso M, et al. COVID-19 and kidney transplantation: an Italian Survey and Consensus. J Nephrol. (2020) 33:667–80. doi: 10.1007/s40620-020-00755-8
35. de Vries A, Alwayn I, Hoek R, van den Berg A, Ultee F, Vogelaar S, et al. Immediate impact of COVID-19 on transplant activity in the Netherlands. Transpl Immunol. (2020) 61:101304. doi: 10.1016/j.trim.2020.101304
36. Al Ammary F, Concepcion B, Yadav A. The scope of telemedicine in kidney transplantation: Access and outreach services. Adv Chronic Kidney Dis. (2021) 28:542–7. doi: 10.1053/j.ackd.2021.10.003
37. Zhao Y, Wei L, Liu B, Du D. Management of transplant patients outside hospital during COVID-19 epidemic: A Chinese experience. Transpl Infect Dis. (2020) 22:e13327. doi: 10.1111/tid.13327
38. Zulman D, Verghese A. Virtual care, telemedicine visits, and real connection in the era of COVID-19: Unforeseen opportunity in the face of adversity. JAMA. (2021) 325:437–8. doi: 10.1001/jama.2020.27304
39. Health Resources & Services Administration. Policy Changes During the COVID-19 Public Health Emergency. Rockville, MD: Health Resources & Services Administration (2020).
40. Centers for Medicare & Medicaid Services. Medicare telemedicine health care provider fact sheet. Baltimore, MD: Centers for Medicare & Medicaid Services (2020).
41. Congress.Gov. H.R.6074–116th Congress (2019-2020): Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020. (2020). Available online at: https://www.congress.gov/bill/116th-congress/house-bill/6074
42. Harting M, Wheeler A, Ponsky T, Nwomeh B, Snyder C, Bruns N, et al. Telemedicine in pediatric surgery. J Pediatr Surg. (2019) 54:587–94. doi: 10.1016/j.jpedsurg.2018.04.038
43. Sohn G, Wong D, Yu S. A review of the use of telemedicine in dermatologic surgery. Dermatol Surg. (2020) 46:501–7. doi: 10.1097/DSS.0000000000002230
44. Kolcun J, Ryu W, Traynelis V. Systematic review of telemedicine in spine surgery. J Neurosurg Spine. (2020) 1:1–10.
45. Morisada M, Tollefson T, Shaye D, Steele T. The digital doctor: telemedicine in facial plastic surgery. Curr Opin Otolaryngol Head Neck Surg. (2021) 29:271–6. doi: 10.1097/MOO.0000000000000722
46. Grandizio L, Foster B, Klena J. Telemedicine in Hand and Upper-Extremity Surgery. J Hand Surg Am. (2020) 45:239–42. doi: 10.1016/j.jhsa.2019.09.007
47. Jue J, Spector S, Spector S. Telemedicine broadening access to care for complex cases. J Surg Res. (2017) 220:164–70. doi: 10.1016/j.jss.2017.06.085
48. Rajasekaran K. Access to telemedicine-are we doing all that we can during the COVID-19 Pandemic? Otolaryngol Head Neck Surg. (2020) 163:104–6. doi: 10.1177/0194599820925049
49. Concepcion B, Forbes R. The role of telemedicine in kidney transplantation: Opportunities and challenges. Kidney360. (2020) 1:420. doi: 10.34067/KID.0000332020
50. Grenda T, Whang S, Evans N III. Transitioning a surgery practice to telehealth during COVID-19. Ann Surg. (2020) 272:e168–9. doi: 10.1097/SLA.0000000000004008
51. ASTS. ASTS COVID 19 Strike Force Guidance to Members on the Evolving Pandemic. Midland, TX: ASTS (2020).
52. Elhadedy M, Marie Y, Halawa A. COVID-19 in renal transplant recipients: Case series and a brief review of current evidence. Nephron. (2021) 145:192–8. doi: 10.1159/000512329
53. Elens L, Langman L, Hesselink D, Bergan S, Moes D, Molinaro M, et al. Pharmacologic treatment of transplant recipients infected with SARS-CoV-2: Considerations regarding therapeutic drug monitoring and drug-drug interactions. Ther Drug Monit. (2020) 42:360–8. doi: 10.1097/FTD.0000000000000761
54. Manitpisitkul W, McCann E, Lee S, Weir M. Drug interactions in transplant patients: what everyone should know. Curr Opin Nephrol Hypertens. (2009) 18:404–11. doi: 10.1097/MNH.0b013e32832edcb2
55. Craig-Schapiro R, Salinas T, Lubetzky M, Abel B, Sultan S, Lee J, et al. COVID-19 outcomes in patients waitlisted for kidney transplantation and kidney transplant recipients. Am J Transplant. (2021) 21:1576–85. doi: 10.1111/ajt.16351
56. Division of Nephrology, Columbia University Vagelos College of Physicians. Disaster Response to the COVID-19 Pandemic for Patients with Kidney Disease in New York City. J Am Soc Nephrol. (2020) 31:1371–9. doi: 10.1681/ASN.2020040520
58. Jayasekera C, Vikram H, Rifat Z, Wagler J, Okubo K, Braaksma B, et al. Solid Organ Transplantation From SARS-CoV-2–infected Donors to Uninfected Recipients: A Single-center Experience. Transplant Direct. (2022) 8:e1286. doi: 10.1097/TXD.0000000000001286
59. Romagnoli R, Gruttadauria S, Tisone G, Maria Ettorre G, De Carlis L, Martini S, et al. Liver transplantation from active COVID-19 donors: A lifesaving opportunity worth grasping? Am J Transplant. (2021) 21:3919–25. doi: 10.1111/ajt.16823
60. Infectious Disease Society of America. Solid Organ Transplant. Arlington, VA: Infectious Disease Society of America (2021).
61. Panel C. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Maryland: National Institutes of Health (2022).
62. Organ Procurement and Transplantation Network. Summary of Current Evidence and Information– Donor SARSCoV- 2 Testing & Organ Recovery from Donors with a History of COVID-19. Bethesda, MD: National Institutes of Health (2022).
63. American Society of Transplantation. SARS-CoV-2: Recommendations and Guidance for Organ Donor Testing and Evaluation. Mt Laurel, NJ: American Society of Transplantation (2022).
64. Lancet Commission on Covid-19 Vaccines and Therapeutics Task Force Members. Operation Warp Speed: implications for global vaccine security. Lancet Glob Health. (2021) 9:e1017–21. doi: 10.1016/S2214-109X(21)00140-6
65. Hall V, Foulkes S, Charlett A, Atti A, Monk E, Simmons R, et al. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN). Lancet. (2021) 397:1459–69.
66. Lumley S, O’Donnell D, Stoesser N, Matthews P, Howarth A, Hatch S, et al. Antibody status and incidence of SARS-CoV-2 infection in health care workers. New Engl J Med. (2021) 384:533–40. doi: 10.1056/NEJMoa2034545
67. Wei J, Matthews P, Stoesser N, Maddox T, Lorenzi L, Studley R, et al. Anti-spike antibody response to natural SARS-CoV-2 infection in the general population. Nat Commun. (2021) 12:6250. doi: 10.1101/2021.07.02.21259897
68. Jackson L, Anderson E, Rouphael N, Roberts P, Makhene M, Coler R, et al. An mRNA Vaccine against SARS-CoV-2 — Preliminary Report. New Engl J Med. (2020) 383:1920–31. doi: 10.1056/NEJMoa2022483
69. Mulligan M, Lyke K, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature. (2020) 586:589–93. doi: 10.1038/s41586-020-2639-4
70. FDA. FDA In Brief: FDA Issues Guidance on Emergency Use Authorization for COVID-19 Vaccines. Silver Spring, MD: FDA (2020).
71. Alfishawy M, Elbendary A, Mohamed M, Nassar M. COVID-19 mortality in transplant recipients. Int J Organ Transplant Med. (2020) 11:145–62.
72. Boyarsky B, Werbel W, Avery R, Tobian A, Massie A, Segev D, et al. Immunogenicity of a single dose of SARS-CoV-2 Messenger RNA vaccine in solid organ transplant recipients. JAMA. (2021) 325:1784–6. doi: 10.1001/jama.2021.4385
73. Grupper A, Rabinowich L, Schwartz D, Schwartz I, Ben-Yehoyada M, Shashar M, et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am J Transplant. (2021) 21:2719–26. doi: 10.1111/ajt.16615
75. Benotmane I, Gautier G, Perrin P, Olagne J, Cognard N, Fafi-Kremer S, et al. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA. (2021) 326:1063–5. doi: 10.1001/jama.2021.12339
76. Sakhi H, Chavarot N, Attias P, El Karoui K, Anglicheau D. [COVID-19 vaccination in dialysis and kidney transplant patients]. Nephrol Ther. (2021) 17:208–13. doi: 10.1016/j.nephro.2021.06.005
77. National Institutes of Health. COVID Protection After Transplant- Immunosuppression Reduction (CPAT-ISR). Bethesda, MD: National Institutes of Health (2021).
78. Chang A, Mitchell J, Alejo J, Chiang T, Abedon A, Kim J, et al. Immunogenicity of Ad26.COV2.S prime and two subsequent doses of mRNA SARS-CoV-2 vaccines in solid organ transplant recipients: A case series. Clin Transplant. (2022) 36:e14772. doi: 10.1111/ctr.14772
79. Geetha D, Kronbichler A, Rutter M, Bajpai D, Menez S, Weissenbacher A, et al. Impact of the COVID-19 pandemic on the kidney community: lessons learned and future directions. Nat Rev Nephrol. (2022) 18:724–37. doi: 10.1038/s41581-022-00618-4
80. Anders H. Hospital system says it will deny transplants to the unvaccinated in ‘almost all situations’. Seattle: The Washington Post (2021).
81. Chappell B. People who want organ transplants must get the COVID-19 vaccine, a hospital says. Washington, DC: NPR (2021).
82. Colorado C. UCHealth Denies Kidney Transplant To Unvaccinated Woman & Donor. New York, NY: CBS (2021).
83. Goodland M. House Republican calls out UCHealth for denying kidney transplant to unvaccinated. Denver: Colorado Politics (2021).
84. Perez P. Colorado Springs Woman’s Name ‘Inactive’ on UCHealth Kidney Transplant List Over Vaccination Status. Denver, CO: Scripps Media, Inc (2021).
85. Patty NT. Colorado Woman Who Won’t Get Vaccinated Denied Transplant. New York, NY: Associated Press (2021).
86. Salmon D, Moulton L, Omer S, DeHart M, Stokley S, Halsey N. Factors associated with refusal of childhood vaccines among parents of school-aged children: a case-control study. Arch Pediatr Adolesc Med. (2005) 159:470–6. doi: 10.1001/archpedi.159.5.470
87. Omer S, Salmon D, Orenstein W, deHart M, Halsey N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. New Engl J Med. (2009) 360:1981–8. doi: 10.1056/NEJMsa0806477
88. Gullion J, Henry L, Gullion G. Deciding to opt out of childhood vaccination mandates. Public Health Nurs. (2008) 25:401–8. doi: 10.1111/j.1525-1446.2008.00724.x
89. Davidson M. Vaccination as a cause of autism-myths and controversies. Dialogues Clin Neurosci. (2017) 19:403–7. doi: 10.31887/DCNS.2017.19.4/mdavidson
90. Burroughs M, Moscona A. Immunization of pediatric solid organ transplant candidates and recipients. Clin Infect Dis. (2000) 30:857–69. doi: 10.1086/313823
91. Verma A, Wade J. Immunization issues before and after solid organ transplantation in children. Pediatr Transplant. (2006) 10:536–48. doi: 10.1111/j.1399-3046.2006.00527.x
92. Ladd J, Karkazis K, Magnus D. Parental refusal of vaccination and transplantation listing decisions: a nationwide survey. Pediatr Transplant. (2013) 17:244–50. doi: 10.1111/petr.12046
93. ASTS. Joint Statement about COVID-19 Vaccination in Organ Transplant Candidates and Recipients. Midland, TX: ASTS (2022).
94. Kates O, Stohs E, Pergam S, Rakita R, Michaels M, Wolfe C, et al. The limits of refusal: An ethical review of solid organ transplantation and vaccine hesitancy. Am J Transplant. (2021) 21:2637–45. doi: 10.1111/ajt.16472
95. British Transplantation Society. NHS Blood And Transplant/British Transplantation Society Latest Advice On Covid-19 Vaccination I T. Bristol: United Kingdom National Health Service (2021).
96. NHS,. COVID-19 Vaccine 2022. (2022). Available online at: https://bts.org.uk/wp-content/uploads/2022/12/COVID-19-Vaccination-FAQs-for-Clinicians-and-Patients-21st-November-2022-1.pdf (accessed December 16, 2022).
97. Ziemba R, Campbell K, Yang T, Schaeffer S, Mayo K, McGann P, et al. Excess death estimates in patients with end-stage renal disease - united states, february-august 2020. MMWR Morb Mortal Wkly Rep. (2021) 70:825–9. doi: 10.15585/mmwr.mm7022e2
98. Bae S, McAdams-Demarco M, Massie A, Ahn J, Werbel W, Brennan D, et al. Early changes in kidney transplant immunosuppression regimens during the COVID-19 pandemic. Transplantation. (2021) 105:170–6. doi: 10.1097/TP.0000000000003502
99. Cravedi P, Mothi S, Azzi Y, Haverly M, Farouk S, Pérez-Sáez M, et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am J Transplant. (2020) 20:3140–8. doi: 10.1111/ajt.16185
100. Ketcham S, Adie S, Malliett A, Abdul-Aziz A, Bitar A, Grafton G, et al. Coronavirus Disease-2019 in heart transplant recipients in southeastern michigan: A case series. J Card Fail. (2020) 26:457–61. doi: 10.1016/j.cardfail.2020.05.008
101. Sharma P, Chen V, Fung C, Troost J, Patel V, Combs M, et al. COVID-19 outcomes among solid organ transplant recipients: A case-control study. Transplantation. (2021) 105:128–37. doi: 10.1097/TP.0000000000003447
102. Quinn S, Jamison A, Musa D, Hilyard K, Freimuth V. Exploring the continuum of vaccine hesitancy between african american and white adults: results of a qualitative study. PLoS Curr. (2016) 8: doi: 10.1371/currents.outbreaks.3e4a5ea39d8620494e2a2c874a3c4201
103. Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson H. Strategies for addressing vaccine hesitancy - A systematic review. Vaccine. (2015) 33:4180–90. doi: 10.1016/j.vaccine.2015.04.040
104. Simis M, Madden H, Cacciatore M, Yeo S. The lure of rationality: Why does the deficit model persist in science communication? Public Underst Sci. (2016) 25:400–14. doi: 10.1177/0963662516629749
105. Ames H, Glenton C, Lewin S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: a synthesis of qualitative evidence. Cochrane Database Syst Rev. (2017) 2:CD011787. doi: 10.1002/14651858.CD011787.pub2
106. Nyhan B, Reifler J, Richey S, Freed G. Effective messages in vaccine promotion: a randomized trial. Pediatrics. (2014) 133:e835–42. doi: 10.1542/peds.2013-2365
107. Nyhan B, Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine. (2015) 33:459–64. doi: 10.1016/j.vaccine.2014.11.017
108. Joseph N, Bernstein J, Pelton S, Belizaire M, Goff G, Horanieh N, et al. Brief client-centered motivational and behavioral intervention to promote HPV vaccination in a hard-to-reach population: A pilot randomized controlled trial. Clin Pediatr (Phila). (2016) 55:851–9. doi: 10.1177/0009922815616244
110. Georgiades F, Summers D, Butler A, Russell N, Clatworthy M, Torpey N. Renal transplantation during the SARS-CoV-2 pandemic in the UK: Experience from a large-volume center. Clin Transplant. (2021) 35:e14150. doi: 10.1111/ctr.14150
111. La Hoz R, Mufti A, Vagefi P. Short-term liver transplant outcomes from SARS-CoV-2 lower respiratory tract NAT positive donors. Transpl Infect Dis. (2022) 24:e13757. doi: 10.1111/tid.13757
112. Tsapepas D, Paget K, Mohan S, Cohen D, Husain S. Clinically Significant COVID-19 Following SARS-CoV-2 Vaccination in Kidney Transplant Recipients. Am J Kidney Dis. (2021) 78:314–7. doi: 10.1053/j.ajkd.2021.05.004
113. Lubetzky M, Aull M, Craig-Schapiro R, Lee J, Marku-Podvorica J, Salinas T, et al. Kidney allograft recipients, immunosuppression, and coronavirus disease-2019: a report of consecutive cases from a New York City transplant center. Nephrol Dial Transplant. (2020) 35:1250–61. doi: 10.1093/ndt/gfaa154
114. Akalin E, Azzi Y, Bartash R, Seethamraju H, Parides M, Hemmige V, et al. Covid-19 and Kidney Transplantation. N Engl J Med. (2020) 382:2475–7. doi: 10.1056/NEJMc2011117
115. Crespo M, Mazuecos A, Rodrigo E, Gavela E, Villanego F, Sánchez-Alvarez E, et al. Respiratory and gastrointestinal COVID-19 phenotypes in kidney transplant recipients. Transplantation. (2020) 104:2225–33. doi: 10.1097/TP.0000000000003413
116. Elias M, Pievani D, Randoux C, Louis K, Denis B, Delion A, et al. COVID-19 infection in kidney transplant recipients: Disease incidence and clinical outcomes. J Am Soc Nephrol. (2020) 31:2413–23. doi: 10.1681/ASN.2020050639
117. Nair V, Jandovitz N, Hirsch J, Nair G, Abate M, Bhaskaran M, et al. COVID-19 in kidney transplant recipients. Am J Transplant. (2020) 20:1819–25. doi: 10.1111/ajt.15967
118. Azzi Y, Bartash R, Scalea J, Loarte-Campos P, Akalin E. COVID-19 and solid organ transplantation: A review article. Transplantation. (2021) 105:37–55. doi: 10.1097/TP.0000000000003523
119. Alberici F, Delbarba E, Manenti C, Econimo L, Valerio F, Pola A, et al. A report from the Brescia Renal COVID Task Force on the clinical characteristics and short-term outcome of hemodialysis patients with SARS-CoV-2 infection. Kidney Int. (2020) 98:20–6. doi: 10.1016/j.kint.2020.04.030
120. Argenziano M, Bruce S, Slater C, Tiao J, Baldwin M, Barr R, et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: retrospective case series. BMJ. (2020) 369:m1996. doi: 10.1136/bmj.m1996
121. Cummings M, Baldwin M, Abrams D, Jacobson S, Meyer B, Balough E, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. (2020) 395:1763–70. doi: 10.1016/S0140-6736(20)31189-2
122. Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. (2020) 323:1574–81. doi: 10.1001/jama.2020.5394
123. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
124. Kates O, Haydel B, Florman S, Rana M, Chaudhry Z, Ramesh M, et al. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin Infect Dis. (2021) 73:e4090–9.
125. De Meester J, De Bacquer D, Naesens M, Meijers B, Couttenye M, De Vriese A. Incidence, characteristics, and outcome of COVID-19 in adults on kidney replacement therapy: A regionwide registry study. J Am Soc Nephrol. (2021) 32:385–96. doi: 10.1681/ASN.2020060875
126. Yadav A, Singh P. Telehealth use by living kidney donor transplant programs during the COVID-19 Pandemic and beyond: a practical approach. Curr Transplant Rep. (2021) 8:257–62. doi: 10.1007/s40472-021-00339-w
127. Abuzeineh M, Muzaale A, Crews D, Avery R, Brotman D, Brennan D, et al. Telemedicine in the Care of Kidney Transplant Recipients With Coronavirus Disease 2019: Case Reports. Transplant Proc. (2020) 52:2620–5. doi: 10.1016/j.transproceed.2020.07.009
128. Schmid A, Hils S, Kramer-Zucker A, Bogatyreva L, Hauschke D, De Geest S, et al. Telemedically supported case management of living-donor renal transplant recipients to optimize routine evidence-based aftercare: A single-center randomized controlled trial. Am J Transplant. (2017) 17:1594–605. doi: 10.1111/ajt.14138
129. Andrew N, Barraclough K, Long K, Fazio T, Holt S, Kanhutu K, et al. Telehealth model of care for routine follow up of renal transplant recipients in a tertiary centre: A case study. J Telemed Telecare. (2020) 26:232–8. doi: 10.1177/1357633X18807834
130. Waterman A, Dew M, Davis C, McCabe M, Wainright J, Forland C, et al. Living-donor follow-up attitudes and practices in US kidney and liver donor programs. Transplantation. (2013) 95:883–8. doi: 10.1097/TP.0b013e31828279fd
131. Al Ammary F, Thomas A, Massie A, Muzaale A, Shaffer A, Koons B, et al. The landscape of international living kidney donation in the United States. Am J Transplant. (2019) 19:2009–19. doi: 10.1111/ajt.15256
132. Al Ammary F, Sidoti C, Segev D, Henderson M. Health Care Policy and Regulatory Challenges for Adoption of Telemedicine in Kidney Transplantation. Am J Kidney Dis. (2021) 77:773–6. doi: 10.1053/j.ajkd.2020.09.013
135. Wang G, Fiedler A, Warth R, Bailey L, Shupe P, Gregory J. Reliability and accuracy of telemedicine-based shoulder examinations. J Shoulder Elbow Surg. (2022) 31:e369–75. doi: 10.1016/j.jse.2022.04.005
136. Foley O, Ferris T, Thompson R, Heng M, Ricciardi R, Del Carmen M, et al. Potential impact of hospital at home on postoperative readmissions. Am J Manag Care. (2021) 27:e420–5. doi: 10.37765/ajmc.2021.88797
137. Levine D, Ouchi K, Blanchfield B, Saenz A, Burke K, Paz M, et al. Hospital-Level care at home for acutely Ill adults: A randomized controlled trial. Ann Intern Med. (2020) 172:77–85. doi: 10.7326/M19-0600
138. Leong M, Lim C, Lai Y. Comparison of Hospital-at-Home models: a systematic review of reviews. BMJ Open. (2021) 11:e043285. doi: 10.1136/bmjopen-2020-043285
139. Hockley J, Essenhigh C. Implementing a hospital-at-home service to improve patient outcomes. Br J Nurs. (2021) 30:1206–7. doi: 10.12968/bjon.2021.30.20.1206
140. Siddiqi H. To suffer alone: Hospital visitation policies during COVID-19. J Hosp Med. (2020) 15:694–5. doi: 10.12788/jhm.3494
Keywords: kidney transplant, solid organ transplant, care delivery, COVID-19, telemedicine, healthcare access
Citation: Zhang C, Kodali L, Mour G, Jadlowiec C and Mathur AK (2023) The impact of COVID-19 on kidney transplant care. Front. Med. 9:1093126. doi: 10.3389/fmed.2022.1093126
Received: 08 November 2022; Accepted: 19 December 2022;
Published: 09 January 2023.
Edited by:
Nianqiao Gong, Huazhong University of Science and Technology, ChinaReviewed by:
Arzu Velioglu, Marmara University, TürkiyeCopyright © 2023 Zhang, Kodali, Mour, Jadlowiec and Mathur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amit K. Mathur,  TWF0aHVyLmFtaXRAbWF5by5lZHU=
TWF0aHVyLmFtaXRAbWF5by5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.