
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 27 January 2023
Sec. Dermatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1092688
 Alexander Egeberg1
Alexander Egeberg1 Joseph F. Merola2
Joseph F. Merola2 Knut Schäkel3
Knut Schäkel3 Luis Puig4Patrick D. Mahar5,6Isabella Yali Wang5Imre Pavo5
Luis Puig4Patrick D. Mahar5,6Isabella Yali Wang5Imre Pavo5 Christopher Schuster5,7Christopher E. M. Griffiths8*
Christopher Schuster5,7Christopher E. M. Griffiths8*Objective: Patients with psoriasis have an increased prevalence of type 2 diabetes when compared to the general population. Research suggests that type 2 diabetes (T2D) as well as obesity may have an impact on patients' response to treatment. This post-hoc analysis reports the efficacy of ixekizumab in treating moderate-to-severe psoriasis in patients with prediabetes or T2D.
Method and materials: UNCOVER-1, UNCOVER-2, and UNCOVER-3 were three Phase 3, multicenter, randomized, double-blind, placebo-controlled trials that evaluated the efficacy and safety of ixekizumab in adult patients with moderate-to-severe psoriasis. Patients were aged ≥18 years with chronic moderate-to-severe psoriasis (defined as ≥10% body surface area affected, static Physician Global Assessment ≥3, and Psoriasis Area and Severity Index [PASI] ≥12 at screening and baseline) who were candidates for phototherapy or systemic therapy. UNCOVER-1, UNCOVER-2, and UNCOVER-3 participants received ixekizumab as per label (that is, an initial dose of two subcutaneous injections [160 mg in total] at Week 0, followed by 80 mg every 2 weeks through Week 12 and 80 mg every 4 weeks thereafter through Week 60).
Results: The proportions of patients with prediabetes, T2D and normoglycemia that achieved PASI75, PASI90, and PASI100 at Week 60 were similar. Results suggest that patients with T2D were slower to achieve PASI100 than patients with prediabetes or those with normoglycemia. Ixekizumab had no effect on any metabolic markers in patients receiving the treatment.
Conclusions: Despite the higher rate of obesity and extreme obesity in patients with prediabetes and T2D, ixekizumab was an efficacious treatment in treating patients with psoriasis.
Plaque psoriasis is a chronic, inflammatory skin disease affecting approximately 1% of adults worldwide (1–3). Patients with psoriasis have a higher risk of developing several metabolic conditions, including type 2 diabetes (T2D), and this is thought to be a result of shared underlying pathophysiologic drivers of both diseases (4). Recent data suggest that a higher prevalence of prediabetes (precursor of T2D defined with glucose levels above normal but below diabetes diagnostic levels) in patients with psoriasis can be assumed too (5). Beyond T2D, patients with psoriasis also have increased rates of other metabolic syndrome components such as obesity, hypertension, and atherogenic dyslipidemia, such as hypertriglyceridemia and reduced high-density lipoprotein (HDL) levels (6, 7).
Recent research suggests that in patients with psoriasis, T2D reduces the response to biologic treatments, especially interleukin-17 inhibitors, after 6 months treatment (4). Additionally, obesity and hypertension may play a role in reducing responses to systemic and biologic treatments for psoriasis (4, 8). Whether this holds true for prediabetes remains unknown.
This study investigates the efficacy of ixekizumab in long-term treatment of moderate-to-severe psoriasis in patients with prediabetes or T2D (9, 10). As there is a significant correlation between psoriasis and diabetes, it is important to understand the efficacy in these patients so that clinicians can make more informed treatment decisions (11).
UNCOVER-1 (NCT01474512), UNCOVER-2 (NCT01597245), and UNCOVER-3 (NCT01646177) were Phase 3, multicenter, randomized, double-blind, placebo-controlled studies that evaluated the efficacy and safety of ixekizumab in adult patients with moderate-to-severe psoriasis (9, 10).
This post-hoc analysis included patients who received ixekizumab as per label (initial dose of two subcutaneous injections [160 mg in total] at Week 0, followed by 80 mg every 2 weeks through week (W) 12 and 80 mg every 4 weeks thereafter through W60). Patients were grouped based on the T2D diagnosis, presence of prediabetes, or normoglycemia at baseline. T2D was defined as recorded in the patient's medical history and prediabetes as a fasting glucose level ≥5.7 mmol/L (12). Patients with type 1 diabetes mellitus were excluded from the analysis.
Efficacy was assessed by the proportion of patients achieving ≥75% improvement in Psoriasis Area and Severity Index (PASI75), PASI90, and PASI100 from baseline through W60. Patients' body mass index (BMI), blood pressure, and levels of various metabolic parameters were also assessed at multiple timepoints through W60.
Data were analyzed using logistic regression analysis and mixed models with repeated measures analysis. Continuous variables were analyzed using t-tests. Non-responder imputation (NRI) was used for missing categorical data.
Among the 564 ixekizumab-treated patients with moderate-to-severe psoriasis included in this post-hoc analysis, 118 (20.9%) and 40 (7.1%) had prediabetes and T2D, respectively. In 18 (3.2%) patients with unknown T2D, fasting baseline glucose value ≥5.6 mmol/L and also ≥7.0 mmol/L and variable post-baseline values, were included in the prediabetes group. Baseline patient demographics and characteristics are summarized in Table 1. Patients with prediabetes or T2D were older and had numerically higher rates of obesity (particularly extreme obesity [BMI ≥ 40]), hypertension, hyperlipidemia, and fasting serum glucose levels at baseline compared with patients with normoglycemia. Of the patients with T2D, 77.5% had hypertension and 97.5% of patients were above normal weight. Psoriasis severity was comparable across patients with prediabetes, T2D, and normoglycemia; however, psoriasis severity and impact scores (PASI, Body Surface Area, and Dermatology Life Quality Index) were slightly higher in patients with diabetes and prediabetes.
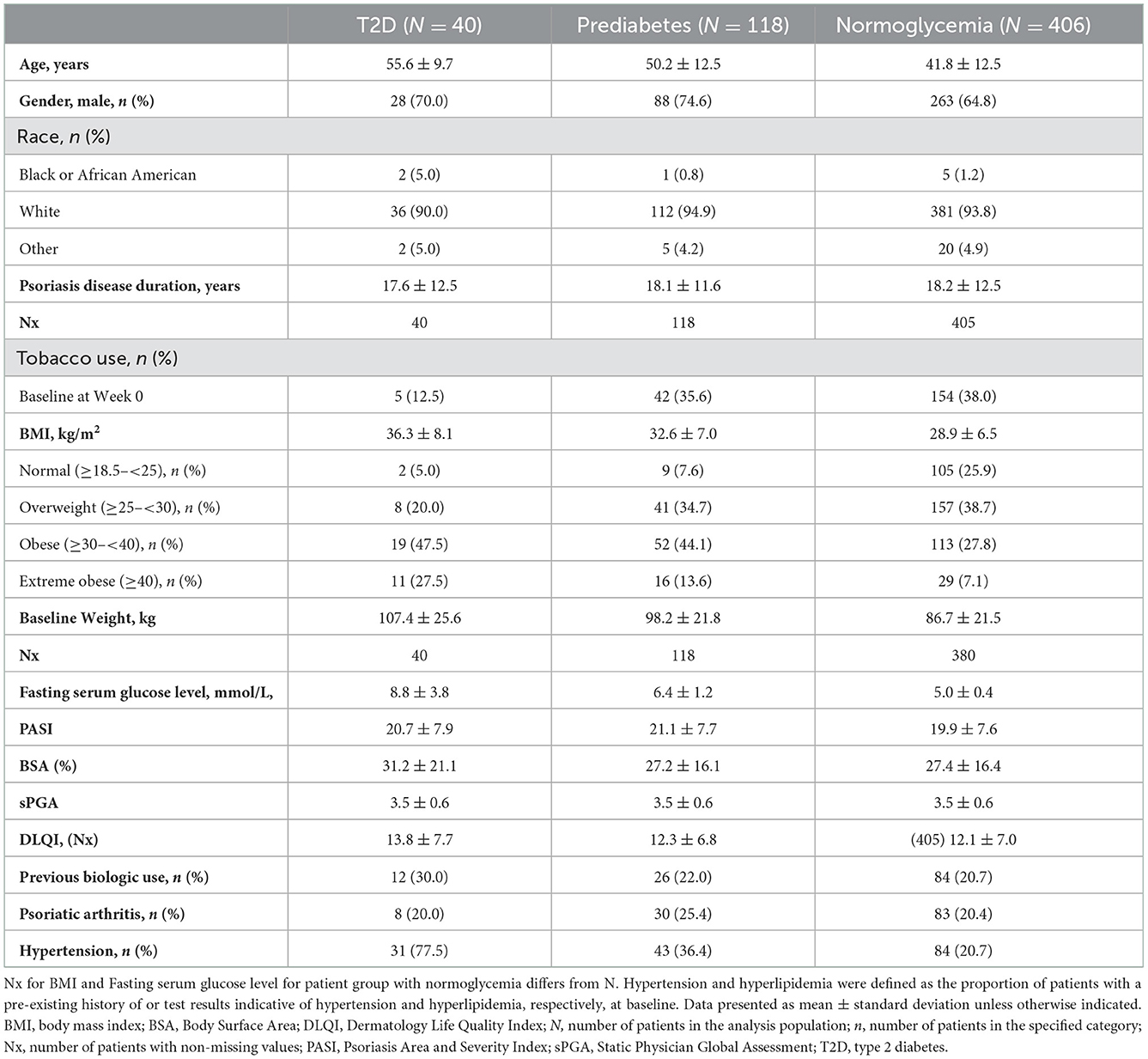
Table 1. Baseline patient demographics and characteristics in ixekizumab-treated patients included in this post-hoc analysis.
Similar proportions of patients across the three groups achieved PASI75 and PASI90 at W60, under comparable treatment duration between responses over the study period. Patients showed a rapid improvement at W1 (PASI75) and W4 (PASI90) of treatment and maintained improvements from W12 through to W60, ensuing a plateau in skin improvement (Figures 1A, B). In contrast, it appears that patients with T2D and to less extent with prediabetes had a slower onset for achieving PASI100 compared to patients with normoglycemia; however, at W60, all outcomes across the three groups were similar (Figure 1C).
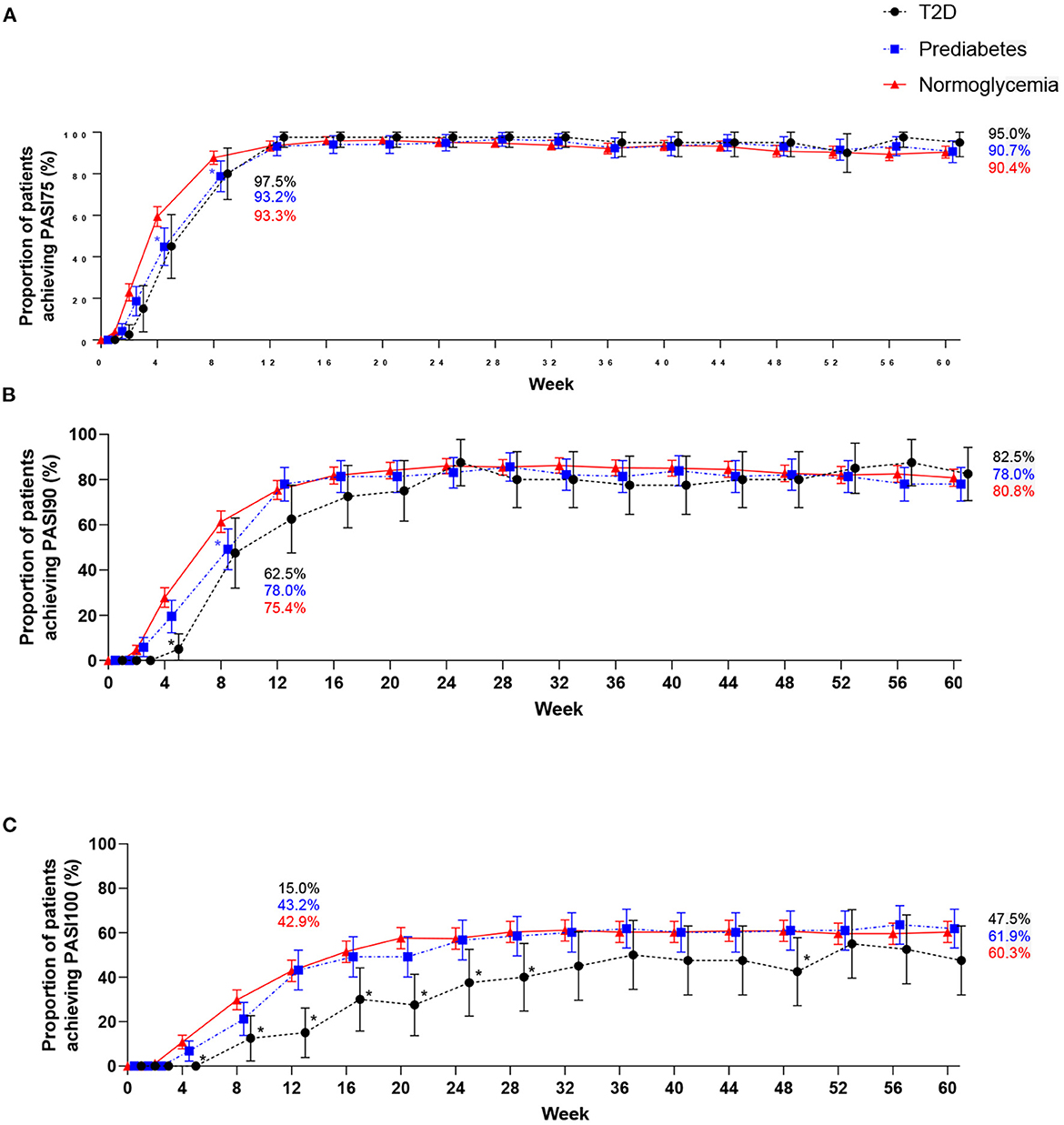
Figure 1. PASI outcomes through Week 60 (NRI). Percentage of patients with type 2 diabetes, prediabetes, and without type 2 diabetes or prediabetes (normoglycemia) achieving PASI75 (A), PASI90 (B), and PASI100 (C). n, number; PASI, Psoriasis Area and Severity Index; T2D, type 2 diabetes. Symbols in line graphs are offset horizontally to differentiate overlapping data points. 95% confidence intervals are shown. * indicates p < 0.05, T2D vs. normoglycemia, * indicates p < 0.05, prediabetes vs. normoglycemia.
At baseline, fasting serum glucose concentrations were higher in patients with prediabetes and markedly elevated T2D compared with patients with normoglycemia (Table 2). Patients with T2D had lower levels of total serum cholesterol and low-density lipoprotein cholesterol compared with patients with prediabetes and normoglycemia. It is undetermined whether the lower levels recorded were due to patients receiving concomitant medication or not. All other clinical measures and metabolic markers were similar across patients with prediabetes, T2D, and normoglycemia at baseline.
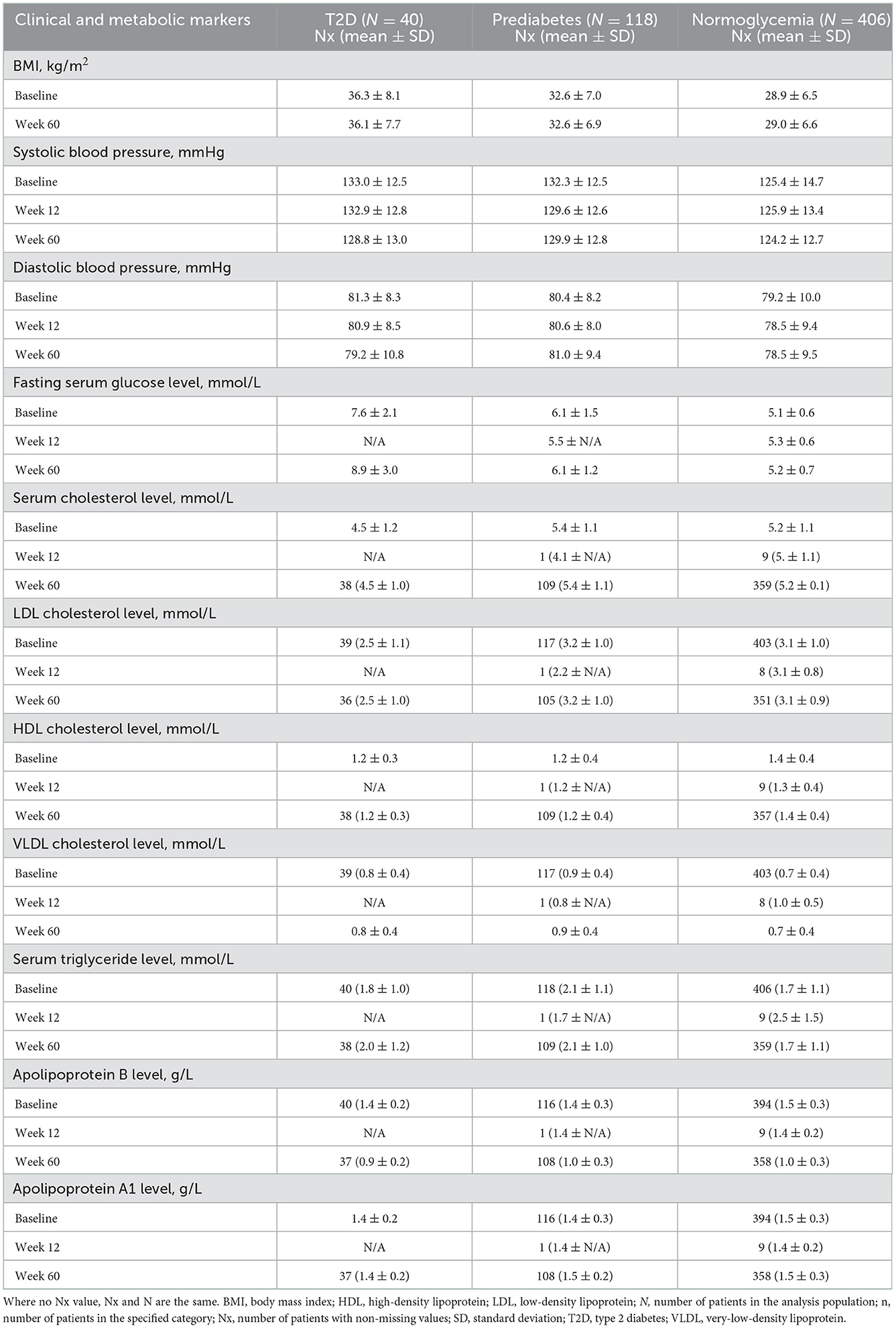
Table 2. Clinical and metabolic markers at baseline, Week 12 and Week 60.
Ixekizumab treatment had no effect on all metabolic markers mentioned in Table 2 after W12 and W60 of treatment. Importantly, clinical measures and metabolic markers did not worsen in ixekizumab-treated patients with prediabetes or T2D through to W60, despite the expected progression of glycemic impairment with time (13).
This study investigating the efficacy of ixekizumab in treating moderate-to-severe psoriasis in patients with concomitant prediabetes or T2D has revealed several important findings. Of note, comparable proportions of patients with prediabetes, T2D, and normoglycemia achieved PASI75, PASI90, and PASI100 at W60. All patients across the three groups achieved PASI75 and PASI90 at a similar response rate; however, patients with T2D achieved PASI100 more slowly than patients with prediabetes or normoglycemia. Results reported in other clinical studies indicate that the co-existence of metabolic syndrome rather than psoriasis disease severity could potentially impact the response to biological treatment (4, 8, 14). Obesity may be associated with reduced treatment responses to some biologics for psoriasis, possibly due to lower serum concentrations in obese patients where dose of the therapy is not weight-adjusted. For example, a pooled analysis of three phase 3 clinical trials evaluating the effect of bodyweight in response to ixekizumab treatment in patients with moderate-to-severe psoriasis, showed some numerical difference in PASI 90 and PASI 100 response rates between bodyweight categories (<80 kg, 80– <100 kg, and ≥100 kg) for ixekizumab and etanercept over a 12-week period (4, 15). As our patients with psoriasis and T2D had high rates of obesity and extreme obesity, which may have an effect on drug clearance, it is possible that this prevented some of them from achieving complete skin clearance and that weight reduction should also be included in the treatment plan (16). Furthermore, as T2D amplifies underlying pathophysiological inflammatory mechanisms of psoriasis, further investigation of the efficacy of ixekizumab in patients with metabolic syndrome is needed to further optimize the treatment on offer for patients with T2D.
The clinical measures and metabolic markers in ixekizumab-treated patients with prediabetes or T2D did not worsen through W60, despite the progressive nature of these diseases.
This study has some limitations. Given the post-hoc and descriptive nature of these analysis, low patient numbers potentially resulting in a low precision of the studied effect estimates, and high prevalence of other metabolic disorders in patients with prediabetes and T2D, caution should be used when interpreting these results as statistical comparisons could not be made.
In summary, this post-hoc analysis demonstrated that ixekizumab is efficacious in patients with psoriasis and prediabetes or T2D, despite high rates of obesity and extreme obesity in this group. Our results show that similar proportions of patients with prediabetes, T2D, and normoglycemia achieve PASI75, PASI90, and PASI100 at a comparable rate; however, patients with T2D may take longer to achieve PASI100. Our findings suggest that patients with psoriasis and concomitant prediabetes or T2D achieve a comparable response to treatment in the context of psoriasis compared to those with normoglycemia. This study provides clinicians with the evidence that while patients with T2D may take longer to respond, ixekizumab is effective for the treatment of patients with moderate-to-severe psoriasis who have comorbid prediabetes or T2D.
The data analyzed in this study is subject to the following licenses/restrictions: Lilly provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the US and EU and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org. Requests to access these datasets should be directed to www.vivli.org.
All patients provided written informed consent prior to enrollment. All studies were conducted with the approval of each Center's Institutional Review Board or Independent Ethics Committee and in accordance with the guiding principles of the Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
PM, CS, and IP contributed to conception and design of the study. IW performed the statistical analysis. All authors contributed to manuscript revision, read, and approved the submitted version.
This study received funding from Eli Lilly and Company. The funder had the following involvement with the study: study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication. AE has received research funding from Pfizer, Eli Lilly, the Danish National Psoriasis Foundation, and the Kgl Hofbundtmager Aage Bang Foundation. LP has received grant/research support from Abbvie, Almirall, Amgen, Boehringer Inglheim, Janssen, Leo-Pharma, Lilly, Norvartis, Pfizer, Regeneron, Roche, Sanofi and UCB.
AE has honoraria as consultant and/or speaker from AbbVie, Almirall, Bristol-Meyers Squibb, Leo Pharma, Samsung Bioepis Co., Ltd., Pfizer, Eli Lilly, Novartis, Galderma, and Janssen Pharmaceuticals. LP has received honoraria/consultation fees from Abbvie, Almirall, Amgen, Baxalta, Boehringer Inglheim, Celgene, Gebro, Janssen, Leo-Pharma, Lilly, Merck-Serono, MSD, Mylan, Norvartis, Pfizer, Regeneron, Roche, Sandoz, Samsung-Bioepis, Sanofi and UCB. LP has participated in company sponsored speaker's bureau for Celgene, Janssen, Lilly, MSD, Norvartis and Pfizer. KS is a consultant, investigator, speaker and has received grants from: AbbVie, Amgen, Almirall, Biogen, Bristol-Myers Squibb Boehringer Ingelheim, Celgene, Chugai, Galderma, Janssen-Cilag, Leo-Pharma, Lilly, Merck Sharp & Dohme Corp., Morphosys, Novartis, Pfizer, Regeneron, UCB Pharma. JM is a consultant and/or investigator for Amgen, Bristol-Myers Squibb, Abbvie, Dermavant, Eli Lilly, Novartis, Janssen, UCB, Sanofi-Regeneron, Sun Pharma, Biogen, Pfizer and Leo Pharma. CG has received honoraria or research grants from AbbVie, Almirall, Anaptysbio Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly and Company, GSK, Janssen, LEO Pharma, Pfizer, Novartis ONO Pharmaceuticals, UCB Pharma and Walgreens Boots Alliance, and is supported in part by the Manchester NIHR Biomedical Research Centre. PM has served as a consultant, investigator, speaker and/or advisor for Novartis, AstraZeneca, Abbvie, Pfizer, Bristol-Meyers Squibb, Eli Lilly and Company and Boehringer Ingelheim. PM, CS, IP, and IW are employees of Eli Lilly and Company. PM owns equity in Eli Lilly and Company. CS, IP, and IW are minor shareholders of Eli Lilly and Company.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. (2020) 369:m1590. doi: 10.1136/bmj.m1590
2. Gisondi P, Galvan A, Idolazzi L, Girolomoni G. Management of moderate to severe psoriasis in patients with metabolic comorbidities. Front Med. (2015) 2:1. doi: 10.3389/fmed.2015.00001
3. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker J. Psoriasis. Lancet. (2021) 397:1301–15. doi: 10.1016/S0140-6736(20)32549-6
4. Enos CW, Ramos VL, McLean RR, Lin T-C, Foster N, Dube B, et al. Comorbid obesity and history of diabetes are independently associated with poorer treatment response to biologics at 6 months: A prospective analysis in Corrona Psoriasis Registry. J Am Acad Dermatol. (2022) 86:68–76. doi: 10.1016/j.jaad.2021.06.883
5. Gyldenløve M, Vilsbøll T, Zachariae C, Holst JJ, Knop FK, Skov L. Impaired incretin effect is an early sign of glucose dysmetabolism in nondiabetic patients with psoriasis. J Intern Med. (2015) 278:660–70. doi: 10.1111/joim.12388
6. Ngo A, Froessl L, McWhorter JW, Perkison WB, Katta R. Diabetes detection and prevention in dermatology. Dermatol Pract Concept. (2021) 11:e2021131. doi: 10.5826/dpc.1104a131
7. Branisteanu DE, Pirvulescu RA, Spinu AE, Porumb EA, Cojocaru M, Nicolescu AC, et al. Metabolic comorbidities of psoriasis (Review). Exp Ther Med. (2022) 23:179. doi: 10.3892/etm.2021.11102
8. Pinter A, Gerdes S, Papavassilis C, Reinhardt M. Characterization of responder groups to secukinumab treatment in moderate to severe plaque psoriasis. J Dermatolog Treat. (2020) 31:769–75. doi: 10.1080/09546634.2019.1626973
9. Gordon KB, Blauvelt A, Papp KA, Langley RG, Luger T, Ohtsuki M, et al. Phase 3 trials of ixekizumab in moderate-to-severe plaque psoriasis. N Engl J Med. (2016) 375:345–56. doi: 10.1056/NEJMoa1512711
10. Griffiths CEM, Reich K, Lebwohl M, van de Kerkhof P, Paul C, Menter A, et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials. Lancet. (2015) 386:541–51. doi: 10.1016/S0140-6736(15)60125-8
11. Armstrong AW, Harskamp CT, Armstrong EJ. Psoriasis and the Risk of Diabetes Mellitus: A Systematic Review and Meta-analysis. JAMA Dermatol. (2013) 149:84–91. doi: 10.1001/2013.jamadermatol.406
12. Mirbolouk M, Derakhshan A, Charkhchi P, Guity K, Azizi F, Hadaegh F. Incidence and predictors of early adulthood pre-diabetes/type 2 diabetes, among Iranian adolescents: the Tehran Lipid and Glucose Study. Pediatr Diab. (2016) 17:608–16. doi: 10.1111/pedi.12343
13. Yigazu DM, Desse TA. Glycemic control and associated factors among type 2 diabetic patients at Shanan Gibe Hospital, Southwest Ethiopia. BMC Res Notes. (2017) 10:597. doi: 10.1186/s13104-017-2924-y
14. Merola JF, Kavanaugh A, Lebwohl MG, Gniadecki R, Wu JJ. Clinical efficacy and safety of psoriasis treatments in patients with concomitant metabolic syndrome: a narrative review. Dermatol Ther. (2022) 12:2201–16. doi: 10.1007/s13555-022-00790-2
15. Reich K, Puig L, Mallbris L, Zhang L, Osuntokun O, Leonardi C. The effect of bodyweight on the efficacy and safety of ixekizumab: results from an integrated database of three randomised, controlled Phase 3 studies of patients with moderate-to-severe plaque psoriasis. J Eur Acad Dermatol Venereol. (2017) 31:1196–207. doi: 10.1111/jdv.14252
16. Chigutsa E, Velez de Mendizabal N, Chua L, Heathman M, Friedrich S, Jackson K, et al. Exposure-response modeling to characterize the relationship between ixekizumab serum drug concentrations and efficacy responses at week 12 in patients with moderate to severe plaque psoriasis. J Clin Pharmacol. (2018) 58:1489–500. doi: 10.1002/jcph.1268
Keywords: moderate-to-severe psoriasis, type 2 diabetes, prediabetes, ixekizumab, obesity
Citation: Egeberg A, Merola JF, Schäkel K, Puig L, Mahar PD, Wang IY, Pavo I, Schuster C and Griffiths CEM (2023) Efficacy of ixekizumab in patients with moderate-to-severe plaque psoriasis and prediabetes or type 2 diabetes. Front. Med. 9:1092688. doi: 10.3389/fmed.2022.1092688
Received: 08 November 2022; Accepted: 23 December 2022;
Published: 27 January 2023.
Edited by:
Anupam Das, KPC Medical College and Hospital, IndiaReviewed by:
Savas Yayli, Koç University, TürkiyeCopyright © 2023 Egeberg, Merola, Schäkel, Puig, Mahar, Wang, Pavo, Schuster and Griffiths. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher E. M. Griffiths, Q2hyaXN0b3BoZXIuR3JpZmZpdGhzQG1hbmNoZXN0ZXIuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.