
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 01 February 2023
Sec. Hepatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1069372
This article is part of the Research TopicThe Current Challenges Underlying Hepatitis D Virus InfectionView all 11 articles
 Licel de los Ángeles Rodríguez Lay1*
Licel de los Ángeles Rodríguez Lay1* Zexi Tan1
Zexi Tan1 Maria Caridad Montalvo Villalba1Marcia Samada Suárez2Marité Bello Corredor1
Maria Caridad Montalvo Villalba1Marcia Samada Suárez2Marité Bello Corredor1 Dayesi López Hernández1Barbara Marrero Sánchez1Lidunka Valdés Alonso1Aurélie Sausy3
Dayesi López Hernández1Barbara Marrero Sánchez1Lidunka Valdés Alonso1Aurélie Sausy3 Judith M. Hübschen3
Judith M. Hübschen3Introduction: Infection with hepatitis delta virus (HDV) is one of the most severe hepatitis B virus (HBV) complications, with a more rapid progression to cirrhosis and an increased risk of hepatic decompensation and death. Data on HDV infection in Cuba are limited. The aims of our study were to determine the HDV prevalence in HBsAg carriers and to characterize the HDV strains circulating. The data were used to assess the possibility of HDV elimination in the Cuban HBV epidemiological setting.
Methods: Five hundred and two serum samples from the same number of HBsAg carriers collected in the period 2006–2019 from all over the country were tested for anti-HDV total antibodies. If positive, the samples were analyzed for HDV-RNA using Real-Time RT-PCR targeting the ribozyme and HD antigen domains followed by genotyping based on phylogenetic analysis.
Results: Two samples were anti-HDV positive [0.39% (95% CI 0.11–1.44)]. One of them was also HDV-RNA positive. Clinically, the patient with active HDV infection had compensated liver cirrhosis. Phylogenetic analysis showed that the virus belonged to genotype 1 and thus clustered with contemporary strains from North America, Europe, Middle East, and Asia.
Discussion: This is the first HDV study, including molecular detection and virus characterization, done after the introduction of the universal childhood anti-hepatitis B vaccination. The very low prevalence of HDV infection in HBsAg carriers combined with the high HBV vaccination coverage of all newborn children, of previously identified risk groups, and of the general population currently under 40 years of age suggests that HDV elimination is feasible in Cuba if the success in HBV control is maintained.
Hepatitis delta virus (HDV) is a unique RNA virus requiring hepatitis B virus (HBV) for replication and infection of hepatocytes (1). Recent data estimated that more than 10% of people with chronic HBV infection are co-infected with HDV, yielding a global prevalence of 0.80% in the general population, and resulting in a total of 48–60 million persons presumably infected with HDV worldwide (2, 3).
The prevalence of HDV is usually assessed based on HDV antibody positivity among HBsAg carriers. Implementation of routine hepatitis B vaccination of children and other population groups in industrialized countries resulted in a considerable decrease of HDV prevalence (4). The impact of the disease in low-income countries is largely unknown due to a lack of awareness and of adequate diagnostic tools. In addition, available treatments are often suboptimal.
Hepatitis delta virus belongs to the genus Deltavirus and was recently reclassified into a new family Kolmioviridae and a new realm called Ribozyviria (5). HDV has a genome size of 1.7 kilobases (kb) and phylogenetic analyses have distinguished eight genotypes 1–8, which differ by up to 30% in their RNA sequence. Genotype 1 is present worldwide, while genotypes 2–8 were found in more specific geographical areas: HDV-2 and –4 are of Asian origin. HDV-3 is found in South America and HDV-5 to 8 were reported mainly from Africa and more recently in Brazil (1, 6–8).
Hepatitis delta virus genotype 1 has been associated with a broad spectrum of pathogenicity, while HDV genotype 2 is normally linked to milder forms of liver disease. HDV-3 has been reported in connection with a severe form of fulminant hepatitis, while HDV-4 is often related to mild liver disease although a variant of genotype 4 seems to increase the risk for progression to chronic hepatitis and cirrhosis. The more recently identified genotypes 5–8 from Africa are less well characterized (6–8).
Cuba is an HBV low prevalence country with a predominance of subgenotype A2 and HBsAg serotype adw2 (9). Three doses of hepatitis B vaccine are recommended at 2, 4, and 6 months of age and 1 dose for newborns within 24 h of birth. The high vaccination coverage of more than 95% in the study period has led to HBV control, with an incidence rate of 0.5/100.000 population in 2020 (10). In line with the WHO global strategy of hepatitis elimination by 2030, Cuba has set up a National Strategic Plan for the Prevention and Control of Sexually Transmitted Diseases including viral hepatitis (11). However, data regarding HDV infection is limited with only one serological study done 32 years ago, when the epidemiological context of HBV infection was very different from today (12). Therefore, the main aims of our study were to determine the HDV prevalence in Cuban HBsAg carriers and to characterize the HDV strains present in the country. The data were used to assess the possibility of HDV elimination in the Cuban HBV epidemiological setting. Additionally, the study provides reliable information for worldwide HDV prevalence estimates to guide international HBV and HDV control programs toward global elimination.
Five hundred and two serum samples received at the National Reference Laboratory of Viral Hepatitis at the Institute of Tropical Medicine Pedro Kouri (IPK) to confirm HBsAg positivity and/or to perform HBV molecular diagnosis between 2006 and 2019 from all over the country were included in this study. The sera had been stored at −20°C and sample information was retrieved from laboratory books or dedicated databases. Two samples had been collected in 2006, 2 in 2007, 9 in 2008, 6 in 2009, 1 in 2011, 37 in 2014, 100 in 2015, 92 in 2016, 143 in 2017, 86 in 2018, and 24 in 2019. Two hundred and ninety-one samples were received from hospitals in Havana (Tertiary Care), 76 sera were from the Eastern, 31 from the Central and 75 from the Western part of Cuba (Figure 1). Twenty-nine samples lacked data about the geographical origin of the patients. In the context of our study, the doctor in charge of a patient with detectable HDV-RNA was informed and a new serum sample for virological follow-up was requested.
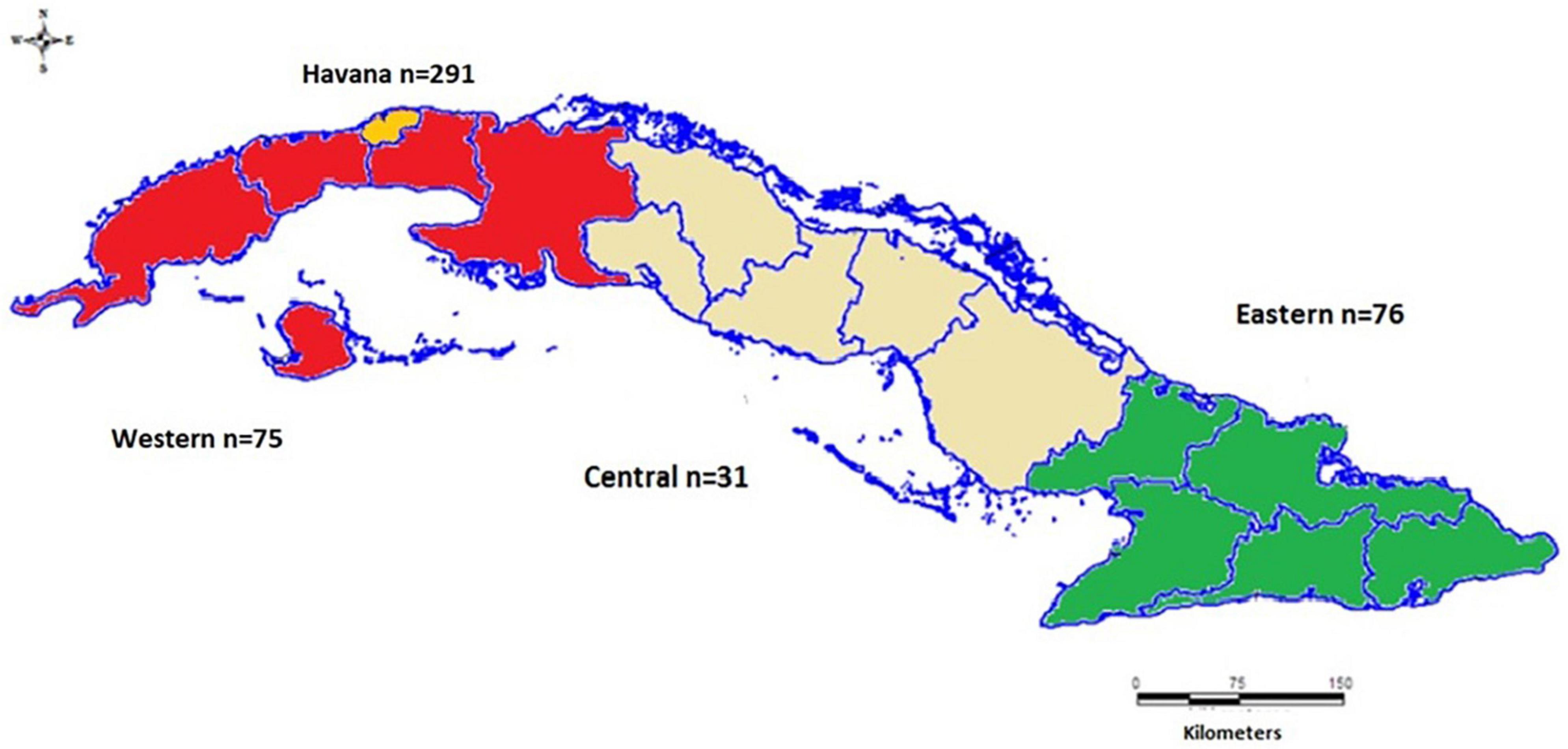
Figure 1. Map showing the main regions of Cuba and Havana as well as the number of samples originating from there.
Some demographic, epidemiological, clinical, and virological characteristics of the study population are shown in Table 1.
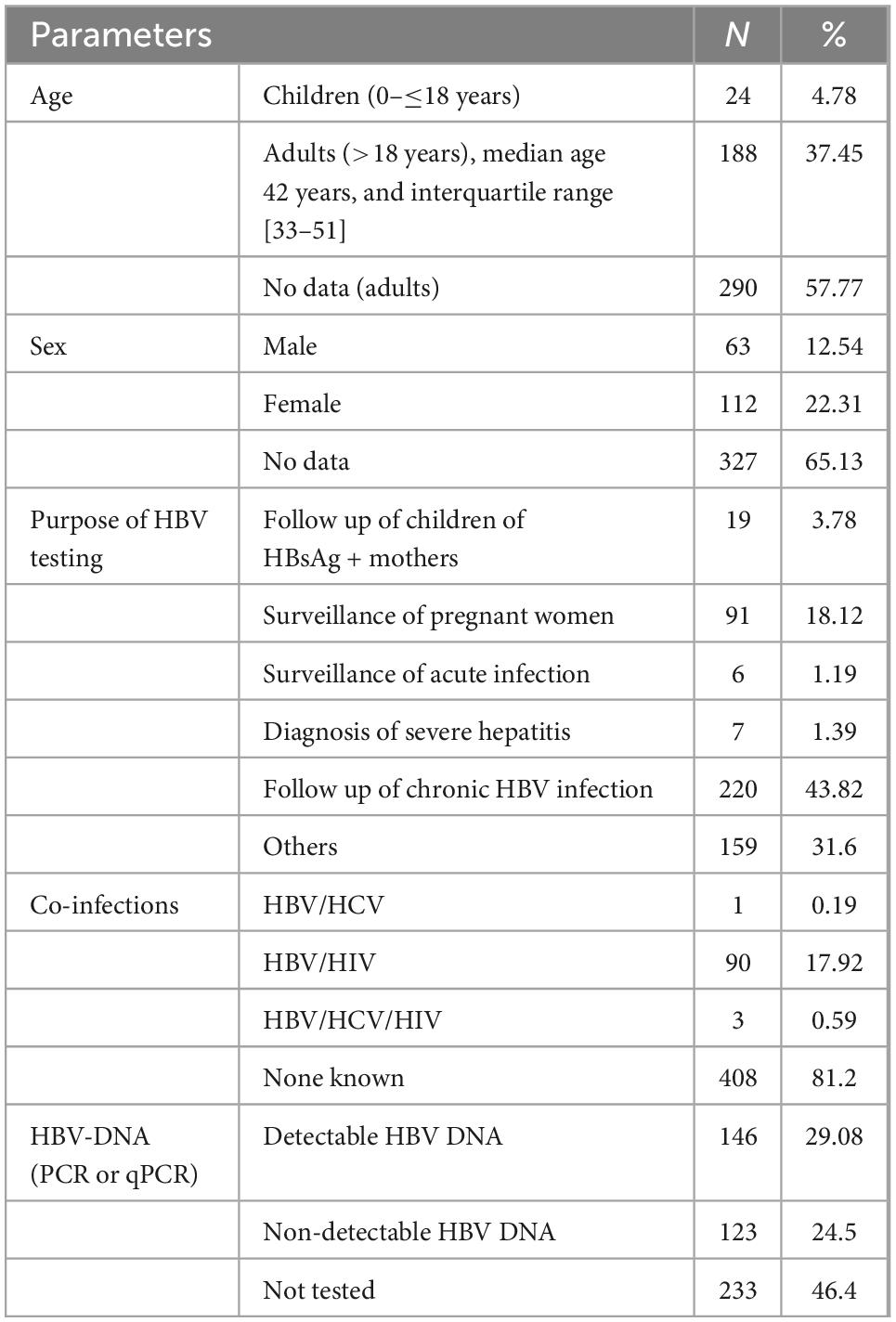
Table 1. Demographic, epidemiological, clinical, and virological characteristics of the 502 study participants, Cuba 2006–2019.
The study was conducted in compliance with the Declaration of Helsinki and using Good Laboratory Practices. The specimens tested for this research were residual samples received for HBV serological and/or molecular analysis. The research was approved by the Ethics Committee of the Institute for Tropical Medicine in Havana, Cuba (CEI-IPK 05-16). In case of positive results, the doctor in charge was informed. Written informed consent was obtained from the patient with active HDV infection (HDV-RNA positive) for reviewing the clinical history and for taking serum samples for the follow-up of the HBV and HDV infection status.
Detection and confirmation of the HBsAg was done with reagents and technology from Tecnosuma Internacional S.A. (UMELISA HBsAg PLUS and UMELISA HBsAg Confirmatory test). Total antibodies against HDV were detected with commercial enzyme linked immunosorbent assays (Dia.Pro, Italy). Both assays were performed according to the manufacturer’s instructions.
Viral RNA was extracted from 140 μL of serum using the QIAamp Viral RNA mini kit (Qiagen GmbH, Hilden, Germany). Five μL of RNA were denatured with 45 ng random primers and 10 nmol nucleotides for 5 min at 72°C. Reverse transcription (RT) was then performed for 80 min at 50°C using 200 U SuperScript III reverse transcriptase and 40 U RNaseOUT recombinant RNase inhibitor (Invitrogen, Karlsruhe, Germany) (13). RT-PCR for HDV detection was done as described previously (14). Five μL of cDNA were added to TaqMan Universal PCR Master Mix (Applied Biosystems, Foster City, CA, United States) as well as 0.5 μM primers and 2.5 μM probe.
Fragments for HDV genotyping were amplified using primers 480as, 710s, 1302das, rv900, fw900_2 and 320ds (13) as well as 1170s (5′-ctcgtcttchhcggtcaacctc-3′, Andernach et al., unpublished). cDNA synthetized as previously described was used with the Phusion High-Fidelity DNA Polymerase (New England Biolabs, Ipswich, United States). The PCR was done using 0.8 μM of primers, 0.5 mM of MgCl2 and 0.02 U/μl of the polymerase and the following amplification conditions: 98°C for 30 s, 40× (98°C for 10 s, 54°C for 30 s, 72°C for 60 s) and a final elongation at 72°C for 7 min. In addition, RNA was used with the One step RT-PCR kit (Qiagen GmbH, Hilden, Germany) and 0.5 μM of primers, 1.5 mM of MgCl2 and 1 μl of enzyme mixture per reaction. The cycling conditions were: 50°C for 30 min, 95°C for 15 min, 40× (95°C for 30 s, 54°C for 30 s, 72°C for 60 s) and a final elongation step at 72°C for 10 min.
PCR products were purified using the QIAquick gel extraction kit (Qiagen GmbH, Hilden, Germany) and sequenced using the ABI Prism Big Dye Terminator cycle sequencing reaction kit (Applied Biosystems, Foster City, CA, United States) in an ABI3130xl genetic analyzer.
Sequences were edited with SeqScape v2.5 software (Applied Biosystems) and BioEdit Sequence Alignment Editor (version 7.0.9.0, Ibis Biosciences, Carlsbad, CA, United States) and aligned with reference sequences of the 8 HDV genotypes and with similar sequences obtained by BLAST.1 Phylogenetic analyses were conducted with MEGA version 62 and phylogenetic trees were constructed using the neighbor-joining method and the Kimura 2-parameter model. The bootstrap method with 1,000 replications was used as measure of the robustness of each node.
Sequences obtained during this study were submitted to the GenBank Nucleotide Sequence Database under accession number: [MW273290].
A Microsoft Excel 2010 database was created for data analysis. The Chi-square test and the confidence interval (CI) calculations were done using GraphPad 7.0. Results were considered to be statistically significant when p < 0.05.
Two of the 502 sera were positive for HDV antibodies (0.39%, [95% CI 0.11–1.44]). One of the positive sera had been collected in 2015, the other in 2017. Both positive samples were from male patients, between 50 and 60 years old and with chronic HBV infection. None of the two patients had an HCV or HIV co-infection. Also, in both patients HBeAg was negative and HBV-DNA was undetectable. HDV-RNA was detected only in one of them.
Clinically, this patient had compensated liver cirrhosis with portal hypertension with only splenomegaly and esophageal varices grade 1. Serum alanine transaminase (ALT), aspartate transaminase (AST), and gamma-glutamyl transferase (GGT) levels were increased, while the alkaline phosphatase (ALP) and total serum bilirubin (TSB) values were in the normal range. Other hematological and biochemical parameters like creatine, albumin, platelets, and International Normalized Ratio (INR) were also in the normal range. The patient had been under Lamivudine therapy during the last 5 years. After the HDV diagnosis, he received Pegylated Interferon Alpha therapy during 1 year. At the end of the treatment the HDV-RNA and the HBV-DNA were undetectable, while the HBsAg remained positive and the enzymes ALT and AST were in the normal range [median ALT before treatment 117 vs. median post treatment 49 (p = 0.05), AST: 89 vs. 51 (p > 0.05)]. The GGT level remained high as a marker of fibrosis.
Sequence data covering nucleotide positions 1–439 and 660–1,682 of the HDV genome (according to US-2 sequence, accession number L22066.1) were obtained. Phylogenetic analysis of the combined 1,462 nucleotides showed that the sequence from Cuba belonged to genotype 1 and thus clustered with contemporary strains from North America (United States), Europe (Spain, Portugal, France, Germany, and Italy), Middle East (Iran and Turkey), and Asia (China) (Figure 2).
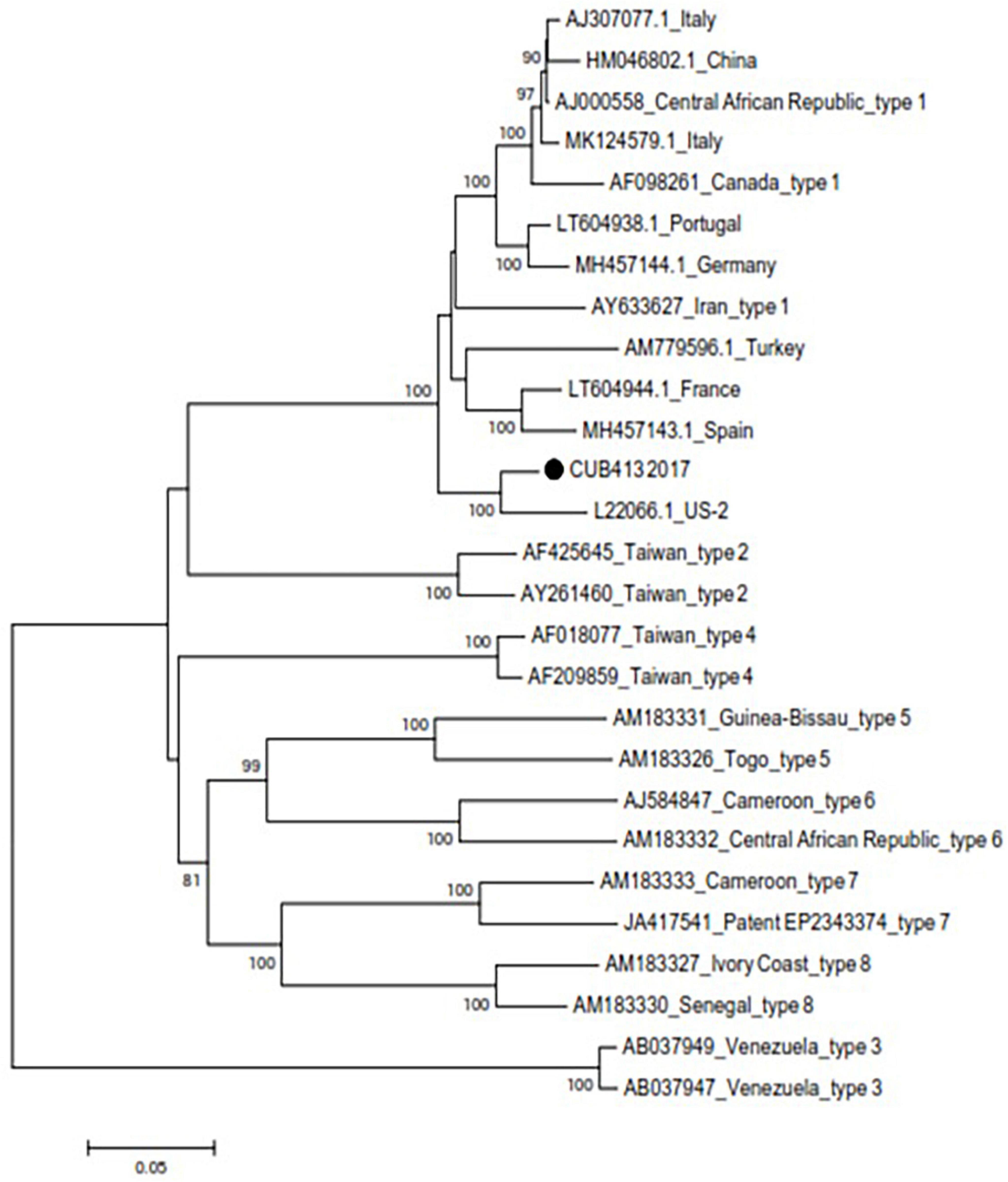
Figure 2. Phylogenetic tree based on the neighbor-joining method and the Kimura 2-parameter model using the partial genome of hepatitis delta virus (HDV). The sequence from Cuba is marked with a black dot. Each reference sequence is identified by GenBank accession number, country of origin, and genotype. Other genotype 1 sequences obtained by BLAST are identified by GenBank accession number and country of origin. Bootstrap values above 70 are shown at the nodes and genetic distance may be estimated based on the bar below the tree.
Although overlapping, the prevalence of HDV does not always coincide with that of HBV. In the past years, HBV vaccination and sexual limitations driven by the risk of AIDS have led to the control of HBV with a significant reduction of the number of HBsAg carriers in many countries. Deprived of HBV infections, the circulation of HDV has noticeably declined principally in the industrialized world (4, 15).
The anti-HDV prevalence found in the present study is very low. In the only other study done in Cuba in 1988, an anti-HDV positivity of 8.3% was detected (11). While we cannot exclude false positive results in the previous study, the ELISA kit used in the present study is expected to reliably detect HDV antibodies with reported sensitivity and specificity values of above 98% (16). The difference may be related to the success of the Cuban hepatitis B prevention and control program, since HBV vaccination is the most influential factor concerning the prevalence of both diseases (17). The vaccination strategy included in the National Immunization Program in 1992 comprised vaccination of all newborn children with the first dose provided in maternity hospitals, as well as vaccination of risk groups to prevent infection before potential exposure. In 2000, a vast vaccination campaign targeting all people less than 20 years of age was done (18). Therefore, the majority of the Cuban population currently under 40 years old is vaccinated against hepatitis B. After 28 years of nationwide vaccination, the rate of new infections has been drastically reduced (from 20.3/100.000 population in 1992 over 2.2/100.000 in 2001 to 0.5/100.000 in 2020) (10). Other measures for HBV control included the screening of all pregnant women, of blood and blood products, the surveillance of children born to HBsAg positive mothers using serological or more recently molecular techniques and education of the population. The considerable reduction of HBV cases may have influenced the HDV epidemiology and thus its currently very low prevalence rate.
Consistent global data on the prevalence of HDV are lacking because of different reasons such as lack of testing of HBsAg carriers for HDV infection or non-availability of high quality anti-HDV antibody assays and there are considerable geographical variations (3, 19, 20). Countries in Asia have reported prevalence rates between 4.4 and 60% (21–23), while in sub-Saharan Africa HDV prevalence ranged from 0 to 50% in relation to the clinical picture of the patients (12). In Europe, the situation is complex because of immigration (24–27) and also countries in the Western world with low HBV prevalence, such as the United States, report diverse HDV prevalence rates (28, 29). The Western Amazonia represents one of the places with the highest prevalence of HDV in the world (30), while other Latin American and Caribbean countries have low prevalence rates (31, 32). HDV control or elimination, however, is only possible via successful HBV immunization programs (17).
The HDV RNA positive patient was born before the introduction of routine childhood HBV vaccination in Cuba. In a recent study analyzing the characteristics of HDV patients from different regions worldwide, the authors stated that men are more frequently infected with HDV than women and that regional differences concerning disease epidemiology and management exist (33).
The interaction between HBV and HDV is complex and multiple virological and host-related factors may be involved. HDV may be temporarily or permanently the dominant virus (34) and HBV DNA levels are often low or even undetectable in patients with chronic HDV infection (33, 35). Also, in the present study both anti-HDV positive cases were HBeAg negative and HBV DNA was undetectable, although the HBV genotype may play a role in the course of chronic hepatitis D. For instance, HBV genotype C has been associated with adverse outcomes (cirrhosis, hepatocellular carcinoma, or mortality) in patients with chronic hepatitis D (36). In Cuba, HBV genotypes A and D are prevalent (9). Since these two genotypes seem to have a very different influence on HDV infectivity (37), it would be interesting to know with which HBV genotype HDV positive patients are infected to anticipate disease outcome.
For the HDV-PCR positive patient, RNA was undetectable after 1 year of Interferon treatment and the liver enzymes were normal suggesting a virological and biochemical response. Although this is the first choice of HDV treatment and decreases the HDV viral load in most patients, only 25% of the patients have undetectable levels of RNA afterward (1, 6, 38, 39). A follow up is needed to verify whether the treatment has a sustained virological response over time, even beyond 24 weeks after treatment suspension (1). Most patients with HBV/HDV coinfection have high levels of ALT, AST and TSB and maintain a stable condition for a long time before decompensation or hepatic carcinoma occur (8, 33, 40). Disease progression may be influenced by the HDV genotype, with types 1 and 3 being linked to a more severe disease than genotypes 2 and 4 (6, 35, 40).
This is the first HDV study, including molecular detection and virus characterization, done after the introduction of the universal childhood anti-hepatitis B vaccination. The very low prevalence of HDV infection in HBsAg carriers combined with the high HBV vaccination coverage of all newborn children, of previously identified risk groups, and of the general population currently under 40 years of age, suggest that HDV elimination is feasible in Cuba if the success in HBV control is maintained.
The data presented in this study are deposited in the Genbank repository (https://www.ncbi.nlm.nih.gov/genbank/), accession number: MW273290.
The study was conducted in compliance with the Declaration of Helsinki and using Good Laboratory Practices. The specimens tested for this research were residual samples received for HBV serological and/or molecular analysis. The research was approved by the Ethics Committee of the Institute for Tropical Medicine in Havana, Cuba (CEI-IPK 05-16). In case of positive results, the doctor in charge was informed. Written informed consent was obtained from the patient with active HDV infection (HDV-RNA positive) for reviewing the clinical history and for taking serum samples for the follow-up of the HBV and HDV infection status.
LÁ and JH: conceptualization, resources, supervision, and project administration. LÁ, MV, ZT, MC, DH, BS, MS, LA, and AS: methodology. LÁ, AS, and JH: software. LÁ, MV, MS, and AS: validation. LÁ, MV, MS, ZT, MC, DH, BS, AS, and JH: analysis. LÁ, MS, and ZT: investigation. LÁ, MS, and LA: data curation. LÁ: writing—original draft preparation. LÁ, MS, and JH: writing—review and editing. LÁ, MS, AS, and JH: visualization. JH: funding acquisition. All authors read and agreed to the published version of the manuscript.
We thank the Luxembourg Ministry of Foreign and European Affairs as well as the Luxembourg Institute of Health for financially supporting the work done in Luxembourg in the frame of the “Microbiology for Development” project. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We want to acknowledged all specialists in charge of the National Hepatitis Program in each province who collect and send samples to the National Reference Laboratory of Viral Hepatitis at the IPK.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Urban S, Neumann-Haefelin C, Lampertico P. Hepatitis D virus in 2021: virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut. (2021) 70:1782–94. doi: 10.1136/gutjnl-2020-323888
2. Chen H, Shen D, Ji D, Han P, Zhang W, Ma J, et al. Prevalence and burden of hepatitis D virus infection in the global population: a systematic review and meta-analysis. Gut. (2019) 68:512–21. doi: 10.1136/gutjnl-2018-316601
3. Miao Z, Zhang S, Ou X, Li S, Ma Z, Wang W, et al. Estimating the global prevalence, disease progression, and clinical outcome of hepatitis delta virus infection. J Infect Dis. (2020) 221:1677–87. doi: 10.1093/infdis/jiz633
4. Rizzetto M. Hepatitis D virus: introduction and epidemiology. Cold Spring Harb Perspect Med. (2015) 5:a021576. doi: 10.1101/cshperspect.a021576
5. International Committee on Taxonomy of Viruses (ICTV),. Deltavirus. (2020). Available online at: https://ictv.global/taxonomy/taxondetails?taxnode_id=202005347. (accessed August 18, 2022).
6. Niro G, Ferro A, Cicerchia F, Brascugli I, Durazzo M. Hepatitis delta virus: from infection to new therapeutic strategies. World J Gastroenterol. (2021) 27:3530–42. doi: 10.3748/wjg.v27.i24.3530
7. Cruz Santos M, Gomes-Gouvêa M, Costa Nunes J, Fonseca Barros L, Carrilho F, de Sousa Paiva Ferreira A, et al. The hepatitis delta genotype 8 in northeast Brazil: the north atlantic slave trade as the potential route for infection. Virus Res. (2016) 224:6–11. doi: 10.1016/j.virusres.2016.08.003
8. Tseligka ED, Clément S, Negro F. HDV pathogenesis: unravelling ariadne’s thread. Viruses. (2021) 13:778. doi: 10.3390/v13050778
9. Rodríguez L, Bello M, Montalvo M, Sariego S, Sánchez M, Valdés L, et al. Genetic diversity of the hepatitis B virus strains in cuba: absence of West-African genotypes despite the transatlantic slave trade. PLoS One. (2015) 10:e0125052. doi: 10.1371/journal.pone.0125052
10. Anuario estadístico de Salud. Electronic version ISSN. (2021). p. 1561–4433. Available online at: https://files.sld.cu/bvscuba/files/2021/08/Anuario-Estadistico-Espa%C3%B1ol-2020-Definitivo.pdf. (accessed September 9, 2022).
11. República de Cuba Ministerio de Salud Pública. Plan Estrategico Nacional Para la Prevención y Control de las ITS, el VIH y Las Hepatitis (2019–2023). Havana: República de Cuba Ministerio de Salud Pública (2019).
12. Galbán E, Rodríguez N, Toledo G, Sotto A, Castañeda C. Encuesta nacional de prevalencia de anticuerpos delta: cuba, 1988. Rev Cubana Hig Epidemiol. (1990) 28:141–52.
13. Andernach I, Leiss L, Tarnagda Z, Tahita M, Otegbayo J, Forbi J, et al. Characterization of hepatitis delta virus in sub-saharan Africa. J Clin Microbiol. (2014) 52:1629–36. doi: 10.1128/JCM.02297-13
14. Le Gal F, Gordien E, Affolabi D, Hansli T, Alloui C, Deny P, et al. Quantification of hepatitis delta virus RNA in serum by consensus real-time PCR indicates different patterns of virological response to interferon therapy in chronically infected patients. J Clin Microbiol. (2005) 43:2363–9. doi: 10.1128/JCM.43.5.2363-2369.2005
16. Noubissi-Jouegouo L, Amougou Atsama M, Tagnouokam-Ngoupo P, Gwladys Monamele C, Ngono L, Njouom R. Evolutionary trends in the prevalence of anti-HDV antibodies among patients positive for HBsAg referred to a national laboratory in cameroon from 2012 to 2017. BMC Res Notes. (2019) 12:417. doi: 10.1186/s13104-019-4460-4
17. Goyal A, Murray J. The impact of vaccination and antiviral therapy on hepatitis B and hepatitis D epidemiology. PLoS One. (2014) 9:e110143.
18. Delgado G, Galindo MA, Rodríguez L, Díaz M. Vaccination strategies against hepatitis B and their results: cuba and the united states, 2003. MEDICC Rev. (2004) 6.
19. Kamili S, Drobeniuc J, Mixson-Hayden T, Kodani M. Delta hepatitis: towards improved diagnostics. Hepatology. (2017) 66:1716–8. doi: 10.1002/hep.29564
20. Hayashi T, Takeshita Y, Hutin Y, Harmanci H, Easterbrook P, Hess S, et al. The global hepatitis delta virus (HDV) epidemic: what gaps to address in order to mount a public health response? Arch Public Health. (2021) 79:180.
21. Lin H, Lee S, Yu M, Chang T, Su C, Hu B, et al. Changing hepatitis D virus epidemiology in a hepatitis B virus endemic area with a national vaccination program. Hepatology. (2015) 61:1870–9. doi: 10.1002/hep.27742
22. Fu J, Guo D, Gao D, Huang W, Li Z, Jia B. Clinical analysis of patients suffering from chronic hepatitis B superinfected with other hepadnaviruses. J Med Virol. (2016) 28:1003–9. doi: 10.1002/jmv.24417
23. Chen X, Oidovsambuu O, Liu P, Grosely R, Elazar M, Winn V, et al. A novel quantitative microarray antibody capture assay identifies an extremely high hepatitis delta virus prevalence among hepatitis B virus-infected mongolians. Hepatology. (2017) 66:1739–49. doi: 10.1002/hep.28957
24. Wedemeyer H, Manns M. Epidemiology, pathogenesis and management of hepatitis D: update and challenges ahead. Nat Rev Gastroenterol Hepatol. (2010) 7:31–40. doi: 10.1038/nrgastro.2009.205
25. Rizzetto M, Ciancio A. Epidemiology of hepatitis D. Semin Liver Dis. (2012) 32:211–9. doi: 10.1055/s-0032-1323626
26. Brancaccio G, Giuberti T, Verucchi G, Levantesi M, Sacchini D, Fattovich G, et al. Epidemiological evolution of chronic hepatitis delta in Italy. An analysis of the master-B cohort. Dig Liv Dis. (2014) 46:e12–3. doi: 10.1016/j.dld.2014.01.030
27. Servant-Delmas A, Le Gal F, Gallian P, Gordien E, Laperche S. Increasing prevalence of HDV/HBV infection over 15 years in France. J Clin Virol. (2014) 59:126–8. doi: 10.1016/j.jcv.2013.11.016
28. Kushner T, Serper M, Kaplan D. Delta hepatitis within the veterans affairs medical system in the united states: prevalence, risk factors, and outcomes. J Hepatol. (2015) 63:586–92. doi: 10.1016/j.jhep.2015.04.025
29. Patel E, Thio C, Boon D, Thomas D, Tobian A. Prevalence of hepatitis B and hepatitis D virus infections in the united states, 2011-2016. Clin Infect Dis. (2019) 69:709–12. doi: 10.1093/cid/ciz001
30. Crispim M, Fraiji N, Campello S, Schriefer N, Stefani M, Kiesslich D. Molecular epidemiology of hepatitis B and hepatitis delta viruses circulating in the Western Amazon region, North Brazil. BMC Infect Dis. (2014) 14:94. doi: 10.1186/1471-2334-14-94
31. Alvarado-Esquivel C, Sablon E, Martinez-Garcia S, Estrada-Martinez S. Hepatitis virus and HIV infections in inmates of a state correctional facility in Mexico. Epidemiol Infect. (2005) 133:679–85. doi: 10.1017/S0950268805003961
32. Delfino C, Eirin M, Berini C, Malan R, Gentile E, Castillo A, et al. HDAg-L variants in covert hepatitis D and HBV occult infection among amerindians of argentina: new insights. J Clin Virol. (2012) 54:223–8. doi: 10.1016/j.jcv.2012.04.014
33. Wranke A, Pinheiro Borzacov L, Parana R, Lobato C, Hamid S, Ceausu E, et al. Clinical and virological heterogeneity of hepatitis delta in different regions world-wide: the hepatitis delta international network (HDIN). Liver Int. (2018) 38:842–50. doi: 10.1111/liv.13604
34. Shirvani-Dastgerdi E, Tacke F. Molecular interactions between hepatitis B virus and delta virus. World J Virol. (2015) 4:36–41. doi: 10.5501/wjv.v4.i2.36
35. Romeo R, Perbellini R. Hepatitis delta virus: making the point from virus isolation up to 2014. World J Hepatol. (2015) 7:2389-95. doi: 10.4254/wjh.v7.i22.2389
36. Sureau C, Negro F. The hepatitis delta virus: replication and pathogenesis. J Hepatol. (2016) 64:S102–16. doi: 10.1016/j.jhep.2016.02.013
37. Freitas N, Abe K, Cunha C, Menne S, Gudima S. Support of the infectivity of hepatitis delta virus particles by the envelope proteins of different genotypes of hepatitis B virus. J Virol. (2014) 88:6255–67. doi: 10.1128/JVI.00346-14
38. Farci P, Niro G. Current and future management of chronic hepatitis D. Gastroenterol Hepatol. (2018) 14:342–51.
39. Zhang Z, Urban S. Interplay between hepatitis D virus and the interferon response. Viruses. (2020) 12:1334. doi: 10.3390/v12111334
Keywords: hepatitis delta virus (HDV), hepatitis B virus, HBsAg carriers, hepatitis B vaccination, HDV elimination
Citation: de los ngeles Rodríguez Lay L, Tan Z, Villalba MCM, Suárez MS, Corredor MB, Hernández DL, Sánchez BM, Alonso LV, Sausy A and Hübschen JM (2023) Low prevalence of hepatitis delta infection in Cuban HBsAg carriers: Prospect for elimination. Front. Med. 9:1069372. doi: 10.3389/fmed.2022.1069372
Received: 13 October 2022; Accepted: 16 December 2022;
Published: 01 February 2023.
Edited by:
Ana Sandoval-Rodriguez, University of Guadalajara, MexicoReviewed by:
Laura Sanchez Orozco, University of Guadalajara, MexicoCopyright © 2023 de los Ángeles Rodríguez Lay, Tan, Villalba, Suárez, Corredor, Hernández, Sánchez, Alonso, Sausy and Hübschen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Licel de los Ángeles Rodríguez Lay,  bGljZWxAaXBrLnNsZC5jdQ==; orcid.org/0000-0002-7742-3146
bGljZWxAaXBrLnNsZC5jdQ==; orcid.org/0000-0002-7742-3146
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.