
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 15 December 2022
Sec. Intensive Care Medicine and Anesthesiology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1062381
This article is part of the Research Topic Assessing and Evaluating the Impact Of The Covid 19 Pandemic on Anxiety And Stress: A Global Perspective View all 16 articles
 Pasquale Buonanno*†
Pasquale Buonanno*† Annachiara Marra†
Annachiara Marra† Carmine Iacovazzo
Carmine Iacovazzo Maria VargasSerena NappiAndrea Uriel de SienaGiuseppe Servillo
Maria VargasSerena NappiAndrea Uriel de SienaGiuseppe ServilloBackground: Preoperative anxiety is a common sensation experienced by patients undergoing surgical interventions. It can influence intraoperative and postoperative management through the activation of the neuroendocrine system, leading to tachycardia, hypertension, pulmonary complications, higher consumption of anesthetic drugs, and increased postoperative pain. Our aim was to investigate the level of preoperative anxiety during the COVID-19 pandemic; we also compared it to the preoperative anxiety of a historical cohort before the outbreak.
Methods: This is a single-center observational study. We enrolled 314 patients during the pandemic from May 2021 to November 2021, and our historical cohort consisted of 122 patients enrolled from July 2015 to May 2016 in the university hospital “Federico II” of Naples. The Amsterdam Preoperative Anxiety and Information Scale (APAIS) and the State-Trait Anxiety Inventory (STAI) were used to evaluate preoperative anxiety. In particular, APAIS measures preoperative anxiety and the need for information, and STAI assesses state and trait anxiety through STAI-Y1 and STAI-Y2, respectively. We analyzed APAIS and STAI scores in our population stratified on the basis of age, gender, marital status, previous surgical experiences, and type of surgery, and we compared them to our historical cohort. Statistical analysis was performed through a t-test and ANOVA for parametric data, and the Mann–Whitney and Kruskal–Wallis tests for non-parametric data. Linear regression was used to investigate the correlation between demographic data and the scores of STAI and APAIS in both groups.
Results: Our results showed that state and preoperative anxiety remained stable, whereas trait anxiety increased in all the subgroups analyzed.
Discussion: Even if state anxiety is considered a variable characteristic of the emotional sphere and trait anxiety a stable element, our findings suggested that COVID-19 deeply influenced trait anxiety, thus altering the patients’ psychological foundations.
Anxiety is a common unpleasant sensation experienced by many patients undergoing surgical procedures all over the world (e.g., USA 20–50%, Europe 27–70%, India 31–46%, and Africa 47–70%). It is defined as a stress response to an unfocused threat, whereas fear is defined as the reaction to a specific danger (1–12). Anxiety can cause a state of exaggerated alertness, often in association with physical and psychological symptoms, such as restlessness, fatigue, muscular tension, sweating, tachycardia, increased blood pressure, intrusive thoughts, and difficulty maintaining concentration (8, 13, 14). Physical symptoms are triggered by the activation of the autonomic nervous system, which leads to the neuroendocrine response through an augmented release of many hormones, such as catecholamines, cortisol, and prolactin, thus increasing the risk of both intraoperative and postoperative complications, such as hemodynamic instability, pulmonary complications, and mental disorders, and higher consumption of anesthetic drugs (15–17). Some studies showed that gynecological elective surgical patients with a high anxiety trait need an increased dose of propofol for the induction and maintenance of anesthesia, while anxious patients undergoing cholecystectomy have a higher risk of intraoperative hemodynamic events (15, 16). Moreover, as previously reported, the correlation between preoperative anxiety and the reduction of pain threshold leads to an increased requirement for analgesic drugs (14, 18–22).
Preoperative anxiety can have a multifactorial origin as it can be influenced by gender, age, social status, and previous surgical experiences (23, 24).
Notably, anxiety can lead to an impairment of the immune system and, consequently, to a higher risk of infections (25).
Our study aimed to determine the level of preoperative anxiety during the COVID-19 pandemic; in addition, we compared it to the preoperative anxiety of a population screened in a previous study conducted in our center to investigate if there is any difference between pre-pandemic and pandemic times (26).
The present study was approved by the local ethic committee “Comitato Etico Università Federico II” (protocol number: 155/20). After explaining the purpose of our research and obtaining written informed consent, we enrolled 314 patients undergoing elective surgery between May 2021 and November 2021 at University Hospital “Federico II” of Naples; they were asked to fill out the questionnaires during the pre-surgical anesthesia assessment. The historical cohort was obtained from the database of a previous study that we conducted before the pandemic (from July 2015 to May 2016) on 122 patients to validate the Italian version of APAIS in the same hospital (27).
The inclusion criteria were as follows: patients in the age bracket of 18–75 years, with adequate language skills, and appropriate comprehension of the questionnaires.
The exclusion criteria were as follows: patients undergoing emergency surgery or obstetric procedures, patients enrolled in our previous study, patients with psychiatric diseases, and patients using psychotropic drugs.
We recorded the following data: anthropometric measures, marital status, educational level, family status, medical and clinical history, and previous surgery. We used two tests to investigate preoperative anxiety, the STAI questionnaire, which is divided into two sections each of them consisting of 20 questions (Y1 and Y2), and the APAIS, a 6-item questionnaire. STAI Y1 was used to measure state anxiety, whereas STAI-Y2 assessed trait anxiety of the patients. State anxiety is defined as a transitory emotional response, whereas trait anxiety is a stable psychological characteristic of the individual, describing the probability to feel anxious in a distressing situation (28). Furthermore, we used APAIS to evaluate not only the anxiety related to anesthesia and the surgery but also the need for information about them. The higher the scores of STAI and APAIS, the higher the level of anxiety of the patient.
We first performed a Shapiro–Wilk test to assess the normal distribution of the data. Parametric data were presented as mean and standard deviation, non-parametric data as median and interquartile range, and categorical variables as frequencies. Parametric data were analyzed through Student’s t-test and the analysis of variance (ANOVA), non-parametric data were analyzed through the Mann–Whitney and Kruskal–Wallis tests, and Pearson’s chi-square test was used to compare frequencies. Post hoc analyses were performed with Tukey’s test for parametric data and Dunn’s test for non-parametric data. We conducted a multivariate analysis through a linear model to correlate STAI-Y1, STAI-Y2, and APAIS scores to the demographic data such as age, gender, marital status, previous surgery, and type of surgery. Differences were considered statistically significant if p < 0.05. All tests were performed using R Studio (28).
We collected data from 122 patients before the pandemic and 314 patients during the pandemic. Socio-demographic characteristics are reported in Table 1. The two groups differed in gender composition, marital status, comorbidity, previous surgery, American Society of Anesthesiologists (ASA) status, and type of surgery. Table 2 reports the analysis of STAI-Y1; there was no difference in the scores reported by the two groups except for the subgroups of patients aged 30–39 years old and men, which showed an increased level of state anxiety during the pandemic.
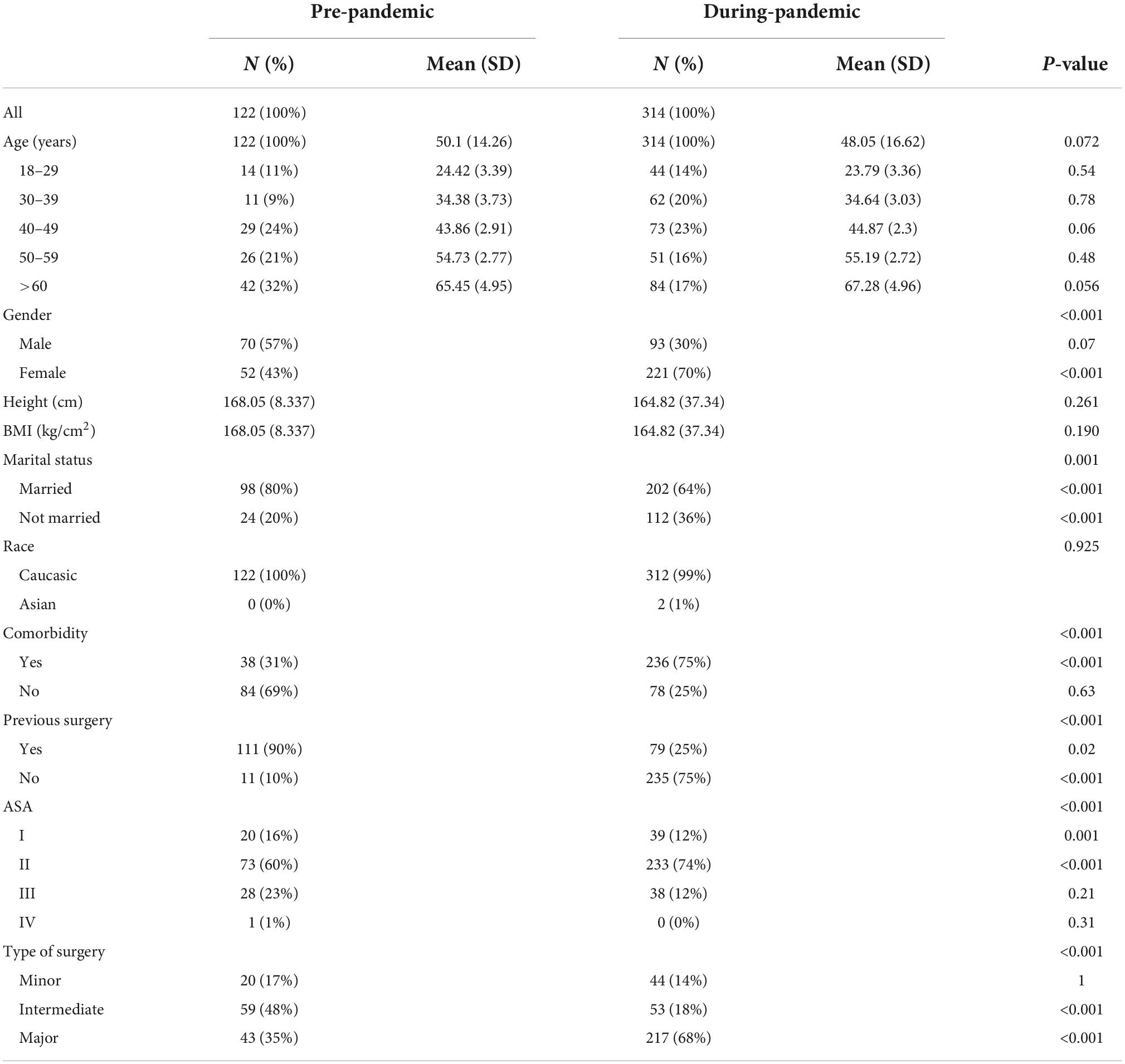
Table 1. Demographic characteristics of the study population.
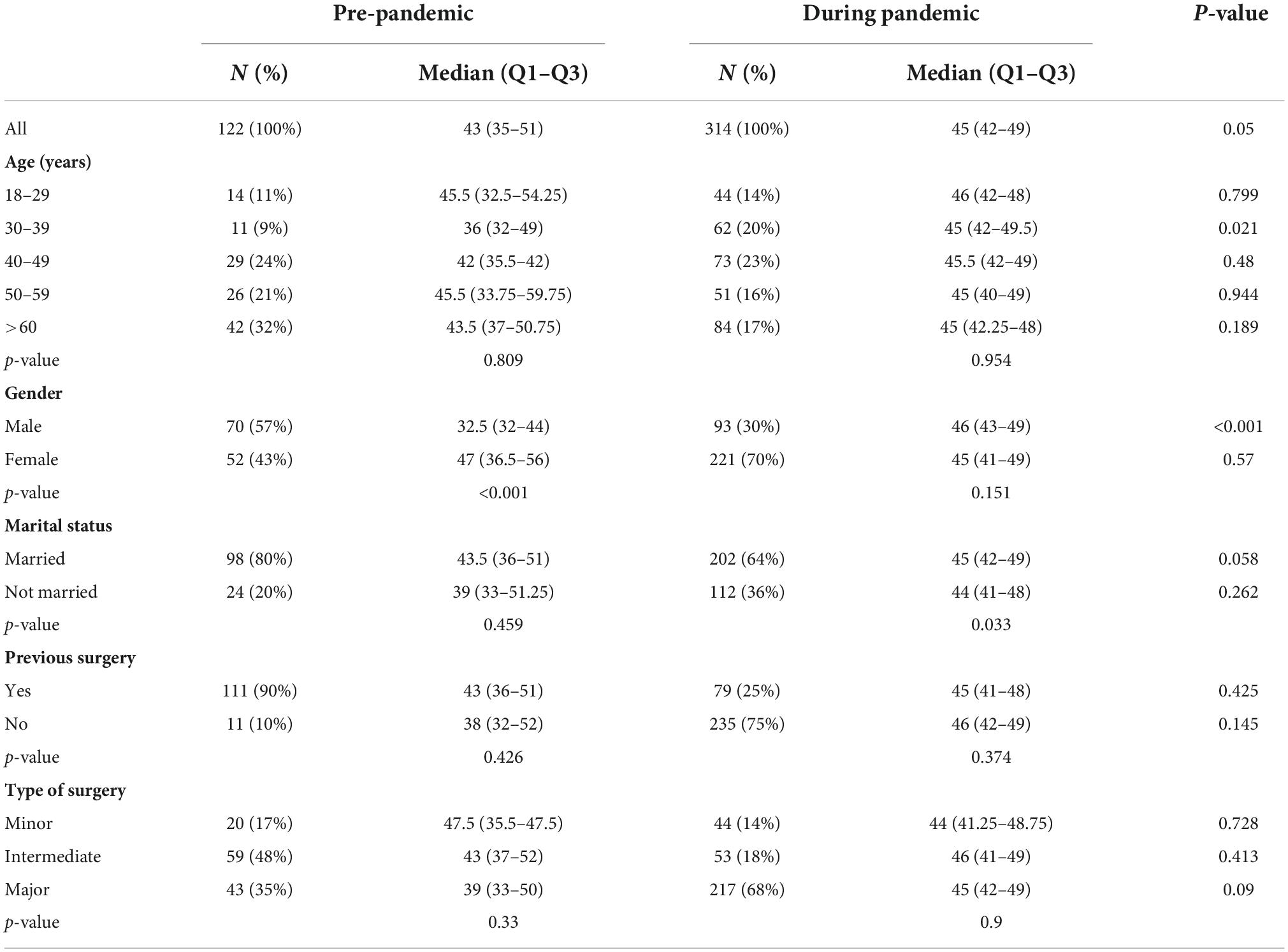
Table 2. STAY-Y1 score for pre-pandemic and during-pandemic groups.
Table 3 shows that STAI-Y2 scores were significantly higher in the during-pandemic subgroups than in pre-pandemic ones, except for the subgroups aged 50–59 years old and subjects undergoing minor surgery.
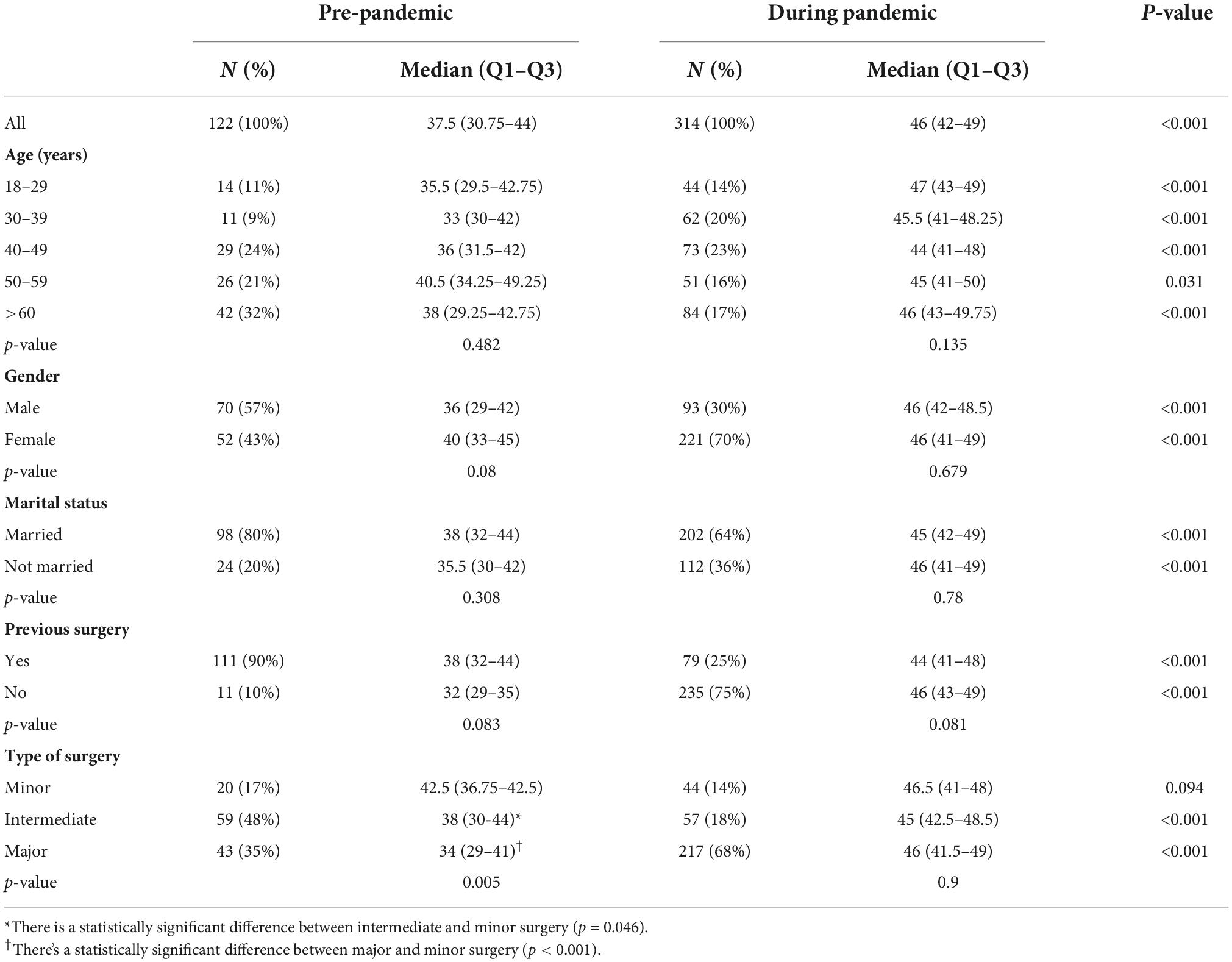
Table 3. STAY-Y2 score for pre-pandemic and during-pandemic groups.
Table 4 shows the overall APAIS score. No significant differences were detected between pre- and during-pandemic groups, except for men and patients undergoing minor surgery, which showed a lower score during the pandemic.
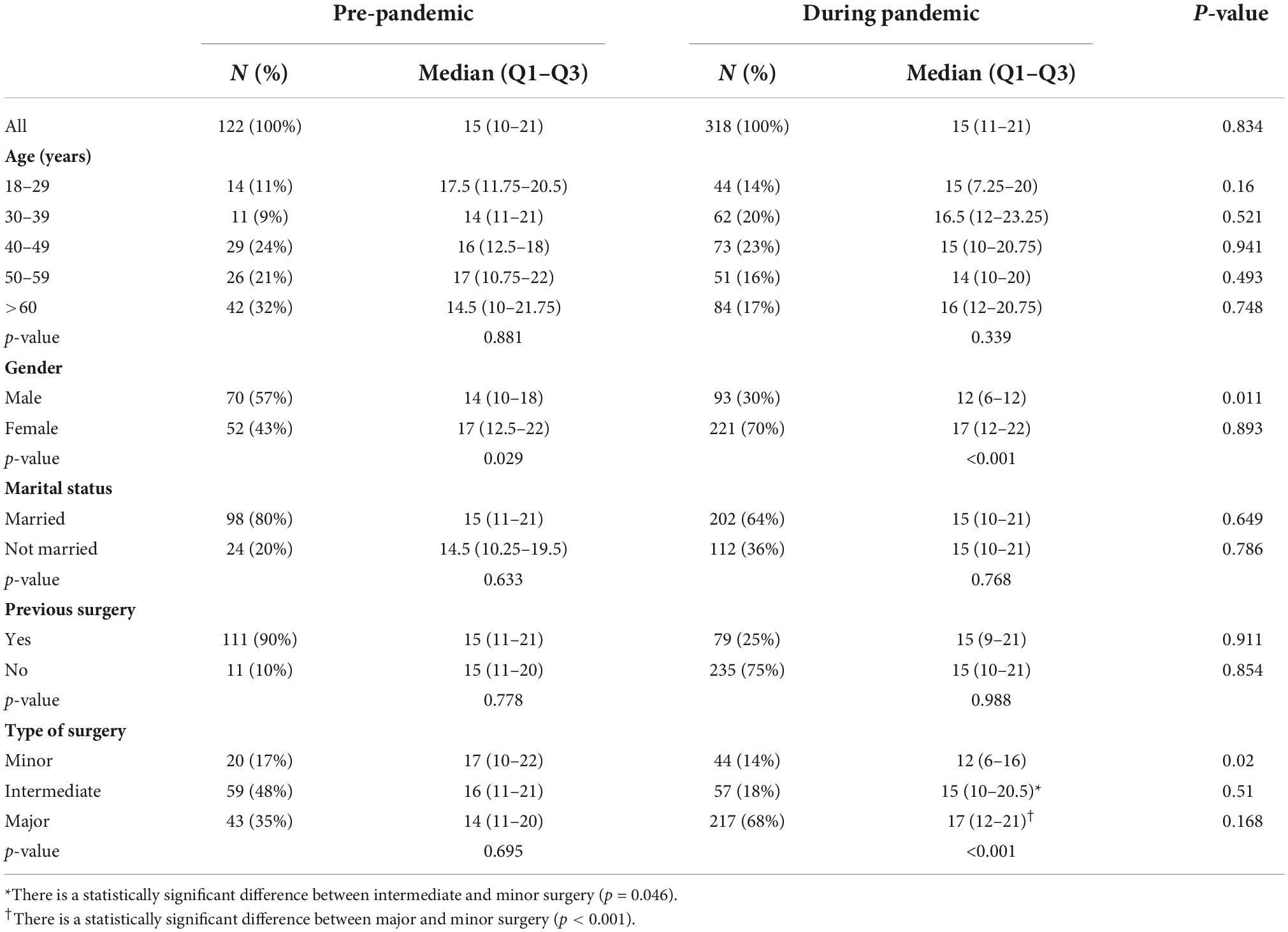
Table 4. The Amsterdam Preoperative Anxiety and Information Scale (APAIS) score for pre-pandemic and during-pandemic groups.
Supplementary Table 1 reports the score obtained from the sum of APAIS questions about the anxiety correlated to anesthesia and surgery; men experienced a lower level of anxiety during the pandemic compared to the pre-pandemic group. In both groups, it is confirmed that women are more anxious than men about anesthesia and surgery.
Supplementary Table 2 shows the score obtained from the sum of APAIS questions about the need for information about anesthesia and surgery. No significant differences were recorded between pre- and during-pandemic groups.
Multivariate analysis showed that during the pandemic, STAI-Y1 is inversely correlated to age between 30 and 39 [standardized beta coefficient −2.71, 95% confidence interval (CI): (−5.34; −0.08), p-value: 0.043], while no correlation was found between STAI-Y1 score and the other demographic data analyzed both during and before the pandemic (Supplementary Table 3). STAI-Y2 score inversely correlated only to the male gender before the pandemic (standardized beta coefficient: −3.44; 95% CI: −6.60; −0.29, p-value: 0.033; Supplementary Table 4). APAIS score inversely correlated to the male gender both before the pandemic (standardized beta coefficient: −2.54, 95% CI: −4.70; −0.37, p-value: 0.022) and during the pandemic (standardized beta coefficient: −3.94, 95% CI: −5.62; −2.25, p-value: < 0.001) and inversely correlated to age more than 60 during the pandemic (standardized beta coefficient: 3.16, 95% CI: −5.69; −0.62, p-value: 0.015; Supplementary Table 5).
Our study aimed to investigate the difference in preoperative anxiety before and during the pandemic. We found that according to STAI-Y1, there were no significant changes in state anxiety; this result was confirmed by APAIS, which did not show any modification during the pandemic for both the anxiety and the need for information subscales. Notably, all the subgroups analyzed showed increased trait anxiety during the pandemic, as recorded by STAI-Y2.
A possible explanation of this result might be the measures adopted to face the spread of the infection in the hospital; in fact, there was close monitoring of patients before admission to the hospital, checking for the virus infection through nasopharyngeal swabs. Apparently, this initial screening probably made the patient feel safe from the contagion.
Previous studies confirmed our result that age does not significantly affect preoperative anxiety, even during the COVID-19 pandemic; only older patients showed a significantly higher level of perioperative anxiety measured by APAIS during the pandemic, maybe because they felt to be a more fragile category of patients based on information conveyed by mass media (23). According to STAI-Y1, only young adults seemed to experience a higher level of anxiety during the pandemic compared to the pre-pandemic period, probably due to their greater and easier access to the internet and social media, which may have increased the exposure to misinformation; furthermore, men showed an increased level of state anxiety during the pandemic (29). This finding is in contrast with the APAIS score, which showed that during the pandemic preoperative anxiety about anesthesia and surgery in men was lower than in the pre-pandemic period; it is important to underline that APAIS questions are specifically focused on anesthesia and surgery, while STAI-Y1 questions are more generic and the patient could forget that the questionnaire refers to the procedures they will undergo (30). In addition, our data confirmed that both during and before the pandemic, the level of preoperative anxiety was lower in men than in women (23).
In accordance with other studies, previous surgical experiences, type of surgery, and marital status did not influence preoperative anxiety both during and before the pandemic (23, 31, 32).
Notably, while overall anxiety did not seem to be substantially affected by the pandemic, trait anxiety augmented in all the subgroups. These findings agree with previous studies investigating trait anxiety in different populations during the pandemic. Trait anxiety is a relatively stable characteristic of a patient’s psychology, but it can be modified by many factors such as psychological therapies; we found that the psychological burden of the pandemic was so powerful to be able to alter the hardcore of people’s emotional sphere (30, 33). The COVID-19 pandemic did impact the socio-economic, relational, and working aspects as well, and all these factors can profoundly influence the patient’s mood (34–38).
Our study has some limitations. First, pre-pandemic and during-pandemic groups are not homogenous in gender, comorbidity, previous surgery, and type of surgery. Notably, all the above-mentioned differences recorded in our groups were supposed to lead to a higher level of state anxiety during the pandemic, but we found that state anxiety was not significantly different between before and during the pandemic. Second, we investigated preoperative anxiety in our hospital; consequently, our findings must be cautiously interpreted and cannot be generalized.
In conclusion, preoperative anxiety is a fundamental issue for many patients undergoing elective surgery, and it could influence perioperative management. The COVID-19 pandemic had an important impact on the psychology of people. Our work highlighted that even if the anxiety related to surgery and anesthesia was not significantly modified during the pandemic, the COVID-19 outbreak has been able to deeply alter the emotional sphere of the patient, revealing that trait anxiety is not an unchangeable characteristic of the subject, but it can be modeled by important socio-economic changes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by “Comitato Etico Università Federico II”. The patients/participants provided their written informed consent to participate in this study.
PB conceived the study and supervised the work. AM wrote the manuscript. MV conducted statistical analyses. CI helped to supervise the project. SN collected and organized the data. AS analyzed the data and drafted the manuscript. GS critically revised the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1062381/full#supplementary-material
Supplementary Table 1 | APAIS anxiety score for pre-pandemic and during-pandemic groups.
Supplementary Table 2 | APAIS need for information score for pre-pandemic and during-pandemic groups.
Supplementary Table 3 | Standardized beta coefficients of multivariate analysis analyzing the relationship between during and pre-pandemic STAI-Y1 score and demographic data.
Supplementary Table 4 | Standardized beta coefficients of multivariate analysis analyzing the relationship between during and pre-pandemic STAI-Y2 score and demographic data.
Supplementary Table 5 | Standardized beta coefficients of multivariate analysis analyzing the relationship between during and pre-pandemic APAIS score and demographic data.
1. Abate SM, Checkol YA, Mantefardo B. Global prevalence and determinants of mortality among patients with COVID-19: a systematic review and meta-analysis. Ann Med Surg. (2021) 64:102204. doi: 10.1016/j.amsu.2021.102204
2. Ekinci M, Gölboyu BE, Dülgeroğlu O, Aksun M, Baysal PK, Çelik EC, et al. A relação entre os níveis de ansiedade no período pré-operatório e os incidentes vasovagais durante a administração de raquianestesia [The relationship between preoperative anxiety levels and vasovagal incidents during the administration of spinal anesthesia]. Rev Bras Anestesiol. (2017) 67:388–94. doi: 10.1016/j.bjan.2016.07.009
3. Hellstadius Y, Lagergren J, Zylstra J, Gossage J, Davies A, Hultman CM, et al. Prevalence and predictors of anxiety and depression among esophageal cancer patients prior to surgery. Dis Esophagus. (2016) 29:1128–34. doi: 10.1111/dote.12437
4. Bansal T, Joon A. A comparative study to assess preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section. Anaesth Pain Intens Care. (2017) 21:25–30.
5. Badner NH, Nielson WR, Munk S, Kwiatkowska C, Gelb AW. Preoperative anxiety: detection and contributing factors. Can J Anaesth. (1990) 37(4 Pt. 1):444–7. doi: 10.1007/BF03005624
6. Vadhanan P, Tripaty DK, Balakrishnan K. Pre-operative anxiety amongst patients in a tertiary care hospital in India- a prevalence study. J Soc Anesthesiol Nepal. (2017) 4:5–10. doi: 10.3126/jsan.v4i1.17377
7. Riddle DL, Wade JB, Jiranek WA. Major depression, generalized anxiety disorder, and panic disorder in patients scheduled for knee arthroplasty. J Arthroplasty. (2010) 25:581–8. doi: 10.1016/j.arth.2009.04.002
8. Bedaso A, Ayalew M. Preoperative anxiety among adult patients undergoing elective surgery: a prospective survey at a general hospital in Ethiopia. Patient Saf Surg. (2019) 13:18. doi: 10.1186/s13037-019-0198-0
9. Mulugeta H, Ayana M, Sintayehu M, Dessie G, Zewdu T. Preoperative anxiety and associated factors among adult surgical patients in Debre Markos and Felege Hiwot referral hospitals, Northwest Ethiopia. BMC Anesthesiol. (2018) 18:155. doi: 10.1186/s12871-018-0619-0
10. Nigussie S, Belachew T, Wolancho W. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC Surg. (2014) 14:67. doi: 10.1186/1471-2482-14-67
11. Moerman N, van Dam FS, Muller MJ, Oosting H. The Amsterdam preoperative anxiety and information scale (APAIS). Anesth Analg. (1996) 82:445–51. doi: 10.1097/00000539-199603000-00002
12. Ramsay MA. A survey of pre-operative fear. Anaesthesia. (1972) 27:396–402. doi: 10.1111/j.1365-2044.1972.tb08244.x
13. Sigdel S. Perioperative anxiety: a short review. Glob Anaesth Perioper Med. (2015) 1:107–8. doi: 10.15761/GAPM.1000126
14. Stamenkovic DM, Rancic NK, Latas MB, Neskovic V, Rondovic GM, Wu JD, et al. Preoperative anxiety and implications on postoperative recovery: what can we do to change our history. Minerva Anestesiol. (2018) 84:1307–17. doi: 10.23736/S0375-9393.18.12520-X
15. Maranets I, Kain ZN. Preoperative anxiety and intraoperative anesthetic requirements. Anesth Analg. (1999) 89:1346–51. doi: 10.1097/00000539-199912000-00003
16. Bayrak A, Sagiroglu G, Copuroglu E. Effects of preoperative anxiety on intraoperative hemodynamics and postoperative pain. J Coll Physicians Surg Pak. (2019) 29:868–73. doi: 10.29271/jcpsp.2019.09.868
17. Kassahun WT, Mehdorn M, Wagner TC, Babel J, Danker H, Gockel I. The effect of preoperative patient-reported anxiety on morbidity and mortality outcomes in patients undergoing major general surgery. Sci Rep. (2022) 12:6312. doi: 10.1038/s41598-022-10302-z
18. Zhang L, Hao LJ, Hou XL, Wu YL, Jing LS, Sun RN. Preoperative anxiety and postoperative pain in patients with laparoscopic hysterectomy. Front Psychol. (2021) 12:727250. doi: 10.3389/fpsyg.2021.727250
19. Tadesse M, Ahmed S, Regassa T, Girma T, Hailu S, Mohammed A, et al. Effect of preoperative anxiety on postoperative pain on patients undergoing elective surgery: prospective cohort study. Ann Med Surg. (2021) 73:103190. doi: 10.1016/j.amsu.2021.103190
20. Duivenvoorden T, Vissers MM, Verhaar JA, Busschbach JJ, Gosens T, Bloem RM, et al. Anxiety and depressive symptoms before and after total hip and knee arthroplasty: a prospective multicentre study. Osteoarthritis Cartilage. (2013) 21:1834–40. doi: 10.1016/j.joca.2013.08.022
21. Prado-Olivares J, Chover-Sierra E. Preoperatory anxiety in patients undergoing cardiac surgery. Diseases. (2019) 7:46. doi: 10.3390/diseases7020046
22. Maheshwari D, Ismail S. Preoperative anxiety in patients selecting either general or regional anesthesia for elective cesarean section. J Anaesthesiol Clin Pharmacol. (2015) 31:196–200. doi: 10.4103/0970-9185.155148
23. Mavridou P, Dimitriou V, Manataki A, Arnaoutoglou E, Papadopoulos G. Patient’s anxiety and fear of anesthesia: effect of gender, age, education, and previous experience of anesthesia. A survey of 400 patients. J Anesth. (2013) 27:104–8. doi: 10.1007/s00540-012-1460-0
24. Buonanno P, Vargas M, Marra A, Iacovazzo C, Servillo G. Preoperative anxiety: what are we really doing? Acta Biomed. (2021) 92:e2021277. doi: 10.23750/abm.v92i3.9329
25. Stein M, Keller SE, Schleifer SJ. Immune system. Relationship to anxiety disorders. Psychiatr Clin North Am. (1988) 11:349–60.
26. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory (Form Y Self-Evaluation Questionnaire). Palo Alto: Consulting Psychologist Press (1983).
27. Buonanno P, Laiola A, Palumbo C, Spinelli G, Terminiello V, Servillo G. Italian validation of the Amsterdam preoperative anxiety and information scale. Minerva Anestesiol. (2017) 83:705–11. doi: 10.23736/S0375-9393.16.11675-X
28. RStudio Team. RStudio: Integrated Development Environment for R. Boston, MA: RStudio, PBC (2022).
29. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health. (2020) 16:57. doi: 10.1186/s12992-020-00589-w
30. Voss C, Shorter P, Weatrowski G, Mueller-Coyne J, Turner K. A comparison of anxiety levels before and during the COVID-19 pandemic. Psychol Rep. (2022):332941221093250. [Epub ahead of print]. doi: 10.1177/00332941221093250
31. Nishimori M, Moerman N, Fukuhara S, van Dam FS, Muller MJ, Hanaoka K, et al. Translation and validation of the Amsterdam preoperative anxiety and information scale (APAIS) for use in Japan. Qual Life Res. (2002) 11:361–4. doi: 10.1023/a:1015561129899
32. Sirinan C, Rungreungvanich M, Vijitpavan A, Morkchareonpong C. Preanesthetic anxiety assessment: HADS versus APAIS. Thailand J Anesth. (2000) 26:155e63.
33. Jorm AF. Modifiability of trait anxiety and neuroticism: a meta-analysis of the literature. Aust N Z J Psychiatry. (1989) 23:21–9. doi: 10.3109/00048678909062588
34. Liu B, Qiao K, Lu Y. The relationship between perceived stress, state-trait anxiety, and sleep quality among university graduates in China during the COVID-19 pandemic. Front Psychol. (2021) 12:664780. doi: 10.3389/fpsyg.2021.664780
35. Fong BYF, Wong MCS, Law VTS, Lo MF, Ng TKC, Yee HHL, et al. Relationships between physical and social behavioural changes and the mental status of homebound residents in Hong Kong during the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:6653. doi: 10.3390/ijerph17186653
36. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. (2020) 15:e0231924. doi: 10.1371/journal.pone.0231924
37. Padhan R, Prabheesh KP. The economics of COVID-19 pandemic: a survey. Econ Anal Policy. (2021) 70:220–37. doi: 10.1016/j.eap.2021.02.012
Keywords: anxiety, preoperative period, test anxiety scale, psychology, COVID-19 pandemic
Citation: Buonanno P, Marra A, Iacovazzo C, Vargas M, Nappi S, de Siena AU and Servillo G (2022) Preoperative anxiety during COVID-19 pandemic: A single-center observational study and comparison with a historical cohort. Front. Med. 9:1062381. doi: 10.3389/fmed.2022.1062381
Received: 05 October 2022; Accepted: 14 November 2022;
Published: 15 December 2022.
Edited by:
Vsevolod Konstantinov, Penza State University, RussiaReviewed by:
Andrés Alexis Ramírez Coronel, Catholic University of Cuenca, EcuadorCopyright © 2022 Buonanno, Marra, Iacovazzo, Vargas, Nappi, de Siena and Servillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pasquale Buonanno, cGFzcXVhbGUuYnVvbmFubm9AdW5pbmEuaXQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.