
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 17 January 2023
Sec. Dermatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1059448
This article is part of the Research Topic Non-Invasive Diagnostic Tools in the Management of Skin Disorders View all 10 articles
 Glauber Voltan1,2*
Glauber Voltan1,2* Wilson Marques-Júnior3
Wilson Marques-Júnior3 Jaci Maria Santana2
Jaci Maria Santana2 Claudia Maria Lincoln Silva1,2
Claudia Maria Lincoln Silva1,2 Marcel Nani Leite1,2
Marcel Nani Leite1,2 Natália Aparecida De Paula1,2
Natália Aparecida De Paula1,2 Fred Bernardes Filho2
Fred Bernardes Filho2 Josafá Gonçalves Barreto4
Josafá Gonçalves Barreto4 Moises Batista Da Silva4
Moises Batista Da Silva4 Guilherme Conde5
Guilherme Conde5 Claudio Guedes Salgado4
Claudio Guedes Salgado4 Marco Andrey Cipriani Frade1,2*
Marco Andrey Cipriani Frade1,2*Introduction: Hansen's disease (HD) primarily infects peripheral nerves, with patients without HD being free of peripheral nerve damage. Household contacts (HHCs) of patients with HD are at a 5–10 times higher risk of HD than the general population. Neural thickening is one of the three cardinal signs that define a case of HD according to WHO guidelines, exclusively considering palpation examination that is subjective and may not detect the condition in the earliest cases even when performed by well-trained professionals. High-resolution ultrasound (HRUS) can evaluate most peripheral nerves, a validated technique with good reproducibility allowing detailed and accurate examination.
Objective: This study aimed to use the peripheral nerve HRUS test according to the HD protocol as a diagnostic method for neuropathy comparing HHCs with healthy volunteers (HVs) and patients with HD.
Methods: In municipalities from 14 different areas of Brazil we selected at random 83 HHC of MB-patients to be submitted to peripheral nerve ultrasound and compared to 49 HVs and 176 HD-patients.
Results: Household contacts assessed by HRUS showed higher median and mean absolute peripheral nerve cross-sectional area (CSA) values and greater asymmetries (ΔCSA) compared to HVs at the same points. Median and mean absolute peripheral nerve CSA values were higher in patients with HD compared to HCCs at almost all points, while ΔCSA values were equal at all points. Mean ± SD focality (ΔTpT) values for HHCs and patients with HD, respectively, were 2.7 ± 2.2/2.6 ± 2.2 for the median nerve, 2.9 ± 2.7/3.3 ± 2.9 for the common fibular nerve (p > 0.05), and 1.3 ± 1.3/2.2 ± 3.9 for the ulnar nerve (p < 0.0001).
Discussion: Considering HRUS findings for HHCs, asymmetric multiple mononeuropathy signs (thickening or asymmetry) in at least 20% of the nerves evaluated could already indicates evidence of HD neuropathy. Thus, if more nerve points are assessed in HHCs (14 instead of 10), the contacts become more like patients with HD according to nerve thickening determined by HRUS, which should be a cutting-edge tool for an early diagnosis of leprosy cases.
Hansen's disease (HD), one of the oldest chronic infectious diseases affecting humans, whose etiologic agent is Mycobacterium leprae (M. leprae) and Mycobacterium lepromatosis, an obligate intracellular pathogen with tropism for macrophages and Schwann cells, primarily infects peripheral nerves and involves the skin and other tissues (1–3). HD is a current and challenging disease still representing a public health problem in developing countries such as Brazil, which ranks second in the world in the number of new cases per year, with more than twenty thousand new cases per year (4, 5). HD has no primary prevention, which means that there is no specific vaccine against M. leprae, and diagnostic and prognostic tests are not feasible or well-established in clinical routine (3). The incubation period of HD is variable, ranging from 6 months to more than 20 years, with an average period of 2–4 years, due to its very slow growth (6).
The predominance of multibacillary (MB) cases with nerve impairment indicate a late diagnosis and underscores the ineffectiveness of epidemiological control in many countries (7). Moreover, new cases not only involving high functional impairment but also affecting children reflect the failure of early HD detection and indicate continued transmission (8). People with untreated HD are generally considered to be the main source of transmission; however, because of the complex relationships between genetic, immunological, and environmental factors, most infected contacts will not develop HD, although recent studies have reported that they may be healthy carriers and transmit M. leprae to susceptible individuals (9–13). Some authors have demonstrated the presence of viable M. leprae strains in skin smear samples from patients as well as in environmental samples obtained from around their homes, revealing that the occurrence of new cases among people without previous contact with those with untreated HD may be due to other undisclosed sources of infection such as water, soil, and animals (14–17).
Contacts of MB patients diagnosed with HD are at 5 to 10 times higher risk of HD than the general population (1, 18, 19). Contact with patients with HD is the main determinant of the incidence of HD (10, 13, 19–29), and the type of contact is not limited to family relationships (18).
There are no patients with HD without peripheral nerve damage, but the exact mechanism underlying the condition is still unknown (30). Scollard (30) suggested that neuropathy may occur partly by the invasion of Schwann cells from the outside to inside, and Graham Weddell observed that HD-related damage occurs at places where there is movement, such as the wrist, elbow, knee, and ankle. Such movements lead to micro-trauma to which the body responds by sending repair cells, including macrophages. For these cells to get into the endoneurium, where the micro-trauma is located, the endothelial cells of the blood vessels in the endoneurium will express adhesion molecules (30).
In a study assessing the neuropathy occurring in HD, Defaria (31) concluded that the condition is a mixed primary peripheral polyneuropathy involving motor and sensory fibers whose earliest neural lesion appears by asymmetric axonal neuropathy and as diffuse demyelination in the later stage. In addition, neuropathy is present in all clinical forms, including those of some contacts.
The diagnosis is essentially clinical, based on a thorough dermatoneurological examination, and in the presence of hypochromic macules, the use of Semmes-Weinstein monofilaments improves its accuracy (32). Current diagnostic tools such as ELISA, PCR, and electroneuromyography (ENMG) have proved to be effective for an early diagnosis of HD and are useful for the evaluation of the efficacy of therapy, but their use is limited in HD, which has been considered a marginalized disease. In addition, these diagnostic methods are only available at referral centers and in teaching and research services (6, 31). Furthermore, pure neural HD, accounting for 5–10% of index cases that present with asymmetric neuropathy in the absence of bacilli in skin smears, remains a diagnostic challenge, often requiring a nerve biopsy, rarely available in the “clusters” and in the areas of higher endemicity (33, 34). Santos et al. (22) demonstrated that, among contacts of patients with HD eligible for a biopsy due to a change in ENMG, 27.8% showed anatomopathological changes suggestive of HD.
In 1977, some authors detected a clearly greater gradual reduction in nerve conduction velocity in the contacts of patients with HD than in HVs, suggesting that a careful (probably improved) method of recording sensory nerve action potentials in the radial cutaneous nerve branch to the index finger could be of help by confirming a diagnosis of leprosy and by detecting the disease in contacts of patients with leprosy before any clinical or bacteriological evidence of leprosy (35).
Neural thickening is one of the three cardinal signs defining a case of HD proposed by the World Health Organization guidelines (36), although only exclusively considering the clinical findings obtained by the palpation technique. When the first signs of neural damage can be noticed, at least 30% of the nerve fibers may show damage (37, 38). HD is a neural disease that may or may not have cutaneous manifestations (2, 3, 39–44). On the contrary, cases of peripheral neuropathy accompanied by neural thickening, with or without cutaneous manifestations, should lead the clinician to suspect the diagnosis of HD (45). Physical examination based on simplified neurological assessment, including palpation of the peripheral nerves, aids in the diagnosis of neural thickening and neuritis; however, this method is subjective, and the earliest cases may not be detected even by well-trained professionals (46, 47).
High-resolution ultrasound (HRUS) can evaluate most peripheral, superficial, and deep nerves and is a validated technique with good reproducibility allowing detailed and accurate examination (48–51). A hand-held ultrasound device can readily identify nerve enlargement in individuals with leprosy, notable in areas with limited healthcare resources because of the portability and low-cost nature of such devices (51, 52).
In the case of pure or primary neural leprosy (PNL), serial scans could be valuable in monitoring treatment and reactions, particularly when it is impossible to determine whether the patient is in remission. In addition, the authors suggest the US as a likely useful tool in the diagnosis of PNH (42, 49, 51).
This study proposes to assess the HRUS of peripheral nerves with an HD protocol as a diagnostic method for asymmetric and fusiform (focal) multiple mononeuropathy by comparing the household contacts of patients with untreated HD with healthy individuals and with those diagnosed with untreated HD.
This study was approved by the Research Ethics Committee of Hospital das Clínicas, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo (protocol number 2.165.032, MH-Brazil and 92228318.1.0000.5440). Written informed consent was obtained from all participants, including the parents and guardians of each participant under 18 years of age. All procedures involving human subjects are in accordance with the ethical standards of the Declaration of Helsinki (1975/2008).
Between 2016 and 2020, municipalities from different regions of Brazil (north, northeast, and southeast) whose health professionals were trained by the National Reference Center in Health Dermatology with an emphasis on HD of HCFMRP-USP were selected. In these regions, we randomly selected 176 patients (HD) and 83 household contacts (HHC) from the MB (multibacillary) patients HD by the teams. All of them were Brazilian volunteers to be submitted to peripheral nerve ultrasound. As a comparative sample of healthy Brazilian volunteers, we used 49 healthy individuals (HVs) among the cases of our service, and as a comparative sample of patients diagnosed with HD (HD), we used cases of our service as published by Voltan et al. (53, 54).
Before being submitted to the HD protocol through the HRUS, all HHCs were clinically evaluated by specialist physicians, dermatologists, or leprologists. Exclusion criteria were all individuals with neurological symptoms such as loss of strength, paresthesia, electric shock-like pain, pain or cramps, with a body mass index ≥35.0 kg/m2, a diagnosis of metaboli [c]c disease (diabetes mellitus, hypothyroidism or hyperthyroidism) or other peripheral neuropathies, and an amputated limb.
The clinical evaluation was performed by dermatologists and HD specialists trained by the Ministry of Health program. The teams were not involved in the execution and analysis of the HRUS images.
Between 2016 and 2020, a physician from our group with a specialization in US and imaging diagnosis and with extensive experience in the neuromuscular US used portable general US devices with high-frequency linear transducers ranging from 4 to 17 MHz. Each peripheral nerve was scanned in transverse and longitudinal sections, and the cross-sectional area (CSA) of transverse sections was obtained with adjustment of the angle perpendicular to the insonated nerve surface and without pressing the structures. The neural points evaluated were selected due to their proximity to bone anatomical references, facilitating the reproducibility of the method, and because they are known sites for neural compression or more common electrophysiological evaluation, besides being already well-established in the literature. The CSA was measured at these points with a continuous trace, within the hyperechoic borders of the epineurium (Figures 1A, B). For comparison with the literature, all patients underwent echographic evaluation of 10 established neural points, namely, the median nerves in the carpal tunnel (Med CT); the ulnar nerves in the cubital tunnel (UT) and the distal third of the arm (cubital pre-tunnel: 3–5 cm above the medial epicondyle)-(UpT); the common fibular nerves in the topography of the fibular head (CFFH); and the tibial nerves in the tarsal tunnel (T), all bilaterally. Exceptionally, in addition to these, four new points were established for routine focality assessment, i.e., the common fibular nerves proximal to the fibular head (3–8 cm proximal to the head of the fibula)-(CFpFH) and median nerves in the distal third of the forearm (Med pCT) (2–5 cm proximal to the carpal tunnel). The upper limb nerves were evaluated with the patient sitting and with elbows flexed between 60 and 90°. The nerves of the lower limbs were evaluated with the patient sitting or in lateral decubitus with legs slightly flexed between 90 and 130°.
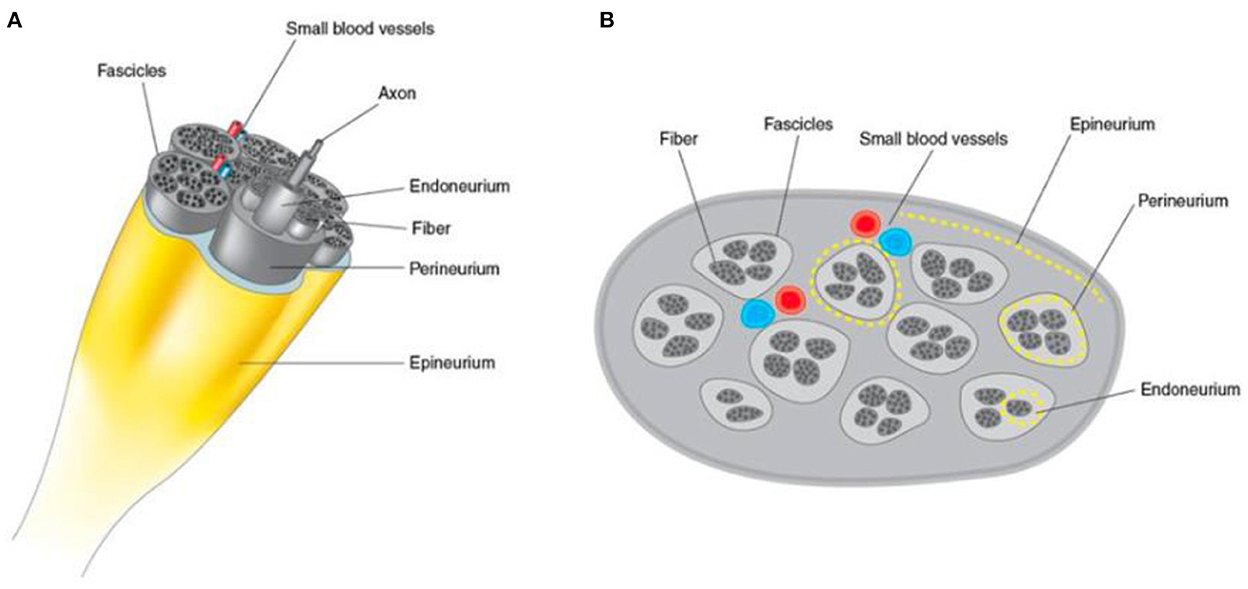
Figure 1. Schematic representation of the cross-sectional view of a normal peripheral nerve and its morphological structures obtained by HRUS. (A) 3D view and (B) with a honeycomb pattern.
Cross-sectional area values obtained from photographs of the US exams were plotted using the Excel® software and further analyzed using Prism 8 for macOS software. We calculated the means, standard deviations, and medians of absolute CSA values for each of the 14 points of the nerves evaluated (7 on the right side and 7 on the left side). The paired t-test was applied to analyze asymmetries. We calculated the indices (Δ) of the differences in absolute CSA values between the right and left sides (ΔCSAs - asymmetry) and of the differences in absolute CSA values between segments of the same nerve (ΔTpT - focality). Neural points were considered to be altered (thickened) when their absolute CSA values were greater than the reference values for normal individuals added to 2 times the standard deviation values (RV + 2 SD). Each neural point was considered to be asymmetric when ΔCSA was greater than its RV + 2 SD, and each neural point was considered to have fusiform or focal thickening when ΔTpT was greater than RV + 2 SD. We also calculated the total number of neural points with increased CSA per individual using the “cont.se” function of the Excel program, as well as the total number of points altered with respect to asymmetry (ΔCSA) and focality (ΔTpT) for each individual. The HV, HHC, and HD groups were compared by the unpaired T-test and the non-parametric Mann-Whitney test using the Prism program. To evaluate the discriminatory capacity of the US for the diagnosis of HD neuropathy, the ROC curve was applied to the numbers of altered points according to CSA, ΔCSA, and ΔTpT, which were then compared to the respective numbers obtained for healthy individuals.
The demographic characteristics, place of birth, and respective anti-PGL1 serology results of the population sample evaluated are described in Table 1.

Table 1. Distribution of the population sample of HHDs (contacts of patients with HD) by sex, age group, region of origin, and anti-PGL-I data.
For comparison of the values obtained for the patients, we considered the values established by Voltan et al. (54) as normality standards (healthy individuals—none of whom had any known contact with leprosy) for CSAs in the Brazilian population.
We have been following 11 HHCs from the southwest—Jardinópolis/SP for 3 years, 5 of whom have developed HD with neuropathy.
The 83 HHCs were evaluated by bilateral HRUS of the following peripheral nerves: Med CT, UT UpT, CFFH, and T. Based on initial observations during fieldwork, additional evaluation of new analysis points of the Med Ab and CFpFH was established as routine in the examinations. Thus, the sample number (n) varied, with measurements of 24 (29.2 %) HHCs being obtained for Med pCT and 38 (46.3 %) HHCs for CFpFH. In 21 HHCs, 14 neural points (MCT, Med pCT, UT, UpT, CFFH, CFpFH, T) were evaluated.
The means, standard deviations, and median absolute CSA values in mm2 and the values of the differences between the right and left sides (ΔCSAs/ΔAsymmetry) and between two points of the same nerve (Δ TpT/Δfocality) are listed in Table 2 according to age group.
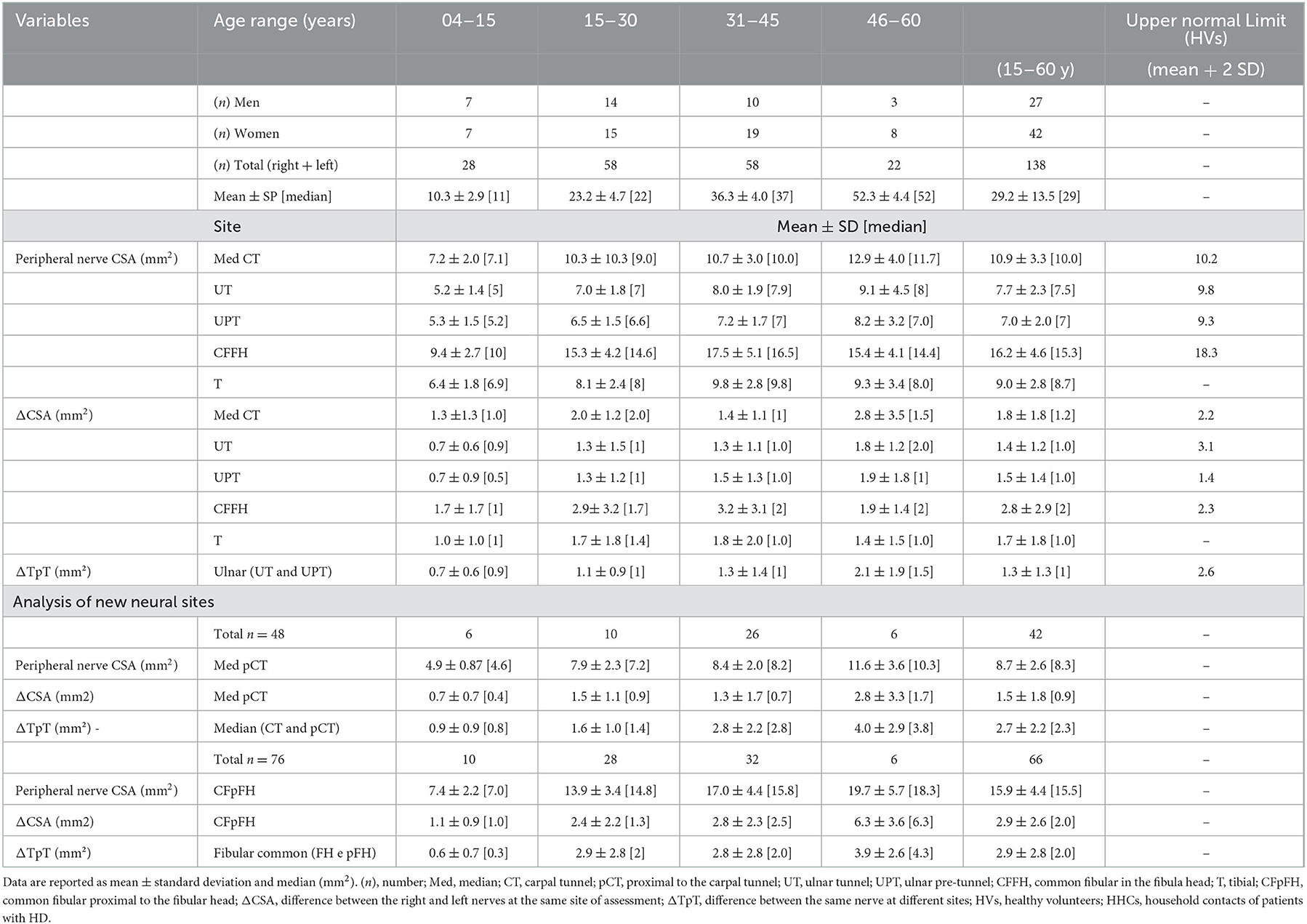
Table 2. Distribution of ultrasound measurements (CSA, ΔCSA, ΔTpT) according to age range in HHCs and upper normal limit in HVs.
We compared 49 healthy individuals (98 neural points) with 69 household contacts (HHCs) of patients diagnosed with HD (138 neural points) and with 176 patients diagnosed with HD (352 neural points) in the age range of 15–60 years.
Since the samples were unpaired and did not have parametric distribution, both the absolute values of the peripheral nerve CSAs and the values of the differences between the CSAs were compared by the non-parametric Mann-Whitney test.
Our results showed higher medians and means of the absolute values of the CSAs of peripheral nerves and greater asymmetries (ΔCSA) in the HHCs compared to the healthy volunteers at all points amenable to comparison, except for the ΔCSA of the tibial nerve, which was equal for the two groups. There was no difference in focus (ΔTpT) of the ulnar nerve between these groups although the mean ± standard deviation showed higher values for the household contacts (HHC = 1.3 ± 1.3 x HVs = 1.0 ± 0.8). The median and mean absolute values of peripheral nerve CSAs were higher in HDs than in HCCs at almost all points except for the Med Ct and UT neural points, which were equal. Asymmetry (ΔCSA) did not differ between groups at any point. The mean ± SD focality (ΔTpT) values of HCC and patients with HD were 2.7 ± 2.2/2.6 ± 2.2 for the median nerve, 2.9 ± 2.7/3.3 ± 2.9 for the common fibular nerve (p > 0.05), and 1.3 ± 1.3/2.2 ± 3.9 for the ulnar nerve (p < 0.0001), respectively, as demonstrated in Figure 2.
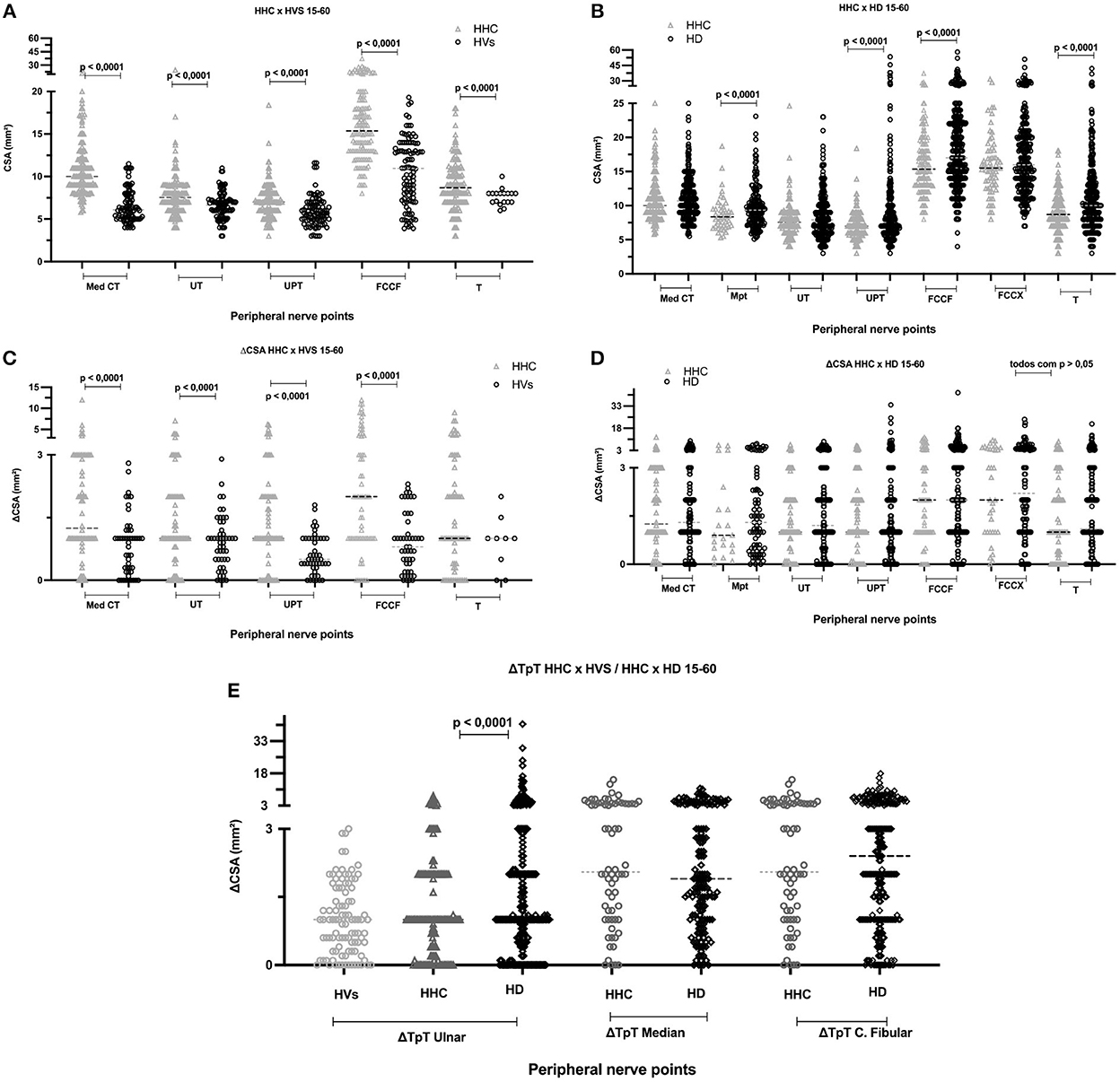
Figure 2. Absolute CSA values (mm2) of peripheral nerve sites for HVs and HHC [(A) up on the left]; absolute CSA values of peripheral nerves sites for HHC and HD [(B) up on the right]. ΔCSA (mm2) of right and left sides at the same assessment site for HVs and HHC [(C) middle on the left]; ΔCSA (mm2) of right and left sides at the same assessment site for HHC and HD [(D) middle on the right]. ΔTpT (mm2) of the different sites of the same nerve for HVs, HHC, and HD [(E) below]. (n), number; Med, median; CT, carpal tunnel; UT, ulnar tunnel; UPT, ulnar pre-tunnel; CFFH, common fibular nerve in the fibula head; T, tibial; MpT, median nerve in the proximal carpal tunnel; CFpFH, common fibular nerve proximal to the fibular head; CSA, cross-sectional area; ΔCSA, difference between the right and left nerves at the same site of assessment; ΔTpT, difference between the same nerve at different sites; HVs, healthy volunteers; HHC, household contacts of patients with HD; HD, Hansen's disease.
In 29 HHCs and 91 patients with HD, we were able to discriminate the ΔTpT (focality) of the median nerve between thickening in the carpal tunnel or proximal to the carpal tunnel, and we obtained greater nerve thickening proximal to the carpal pre-tunnel in 2 HHCs (7%) x 20 HD (22%) (Figure 3) and greater nerve enlargement on the carpal tunnel in 19 HHCs (65%) x 49 HD (53%). The chi-square value was 8.9, with p < 0.05.
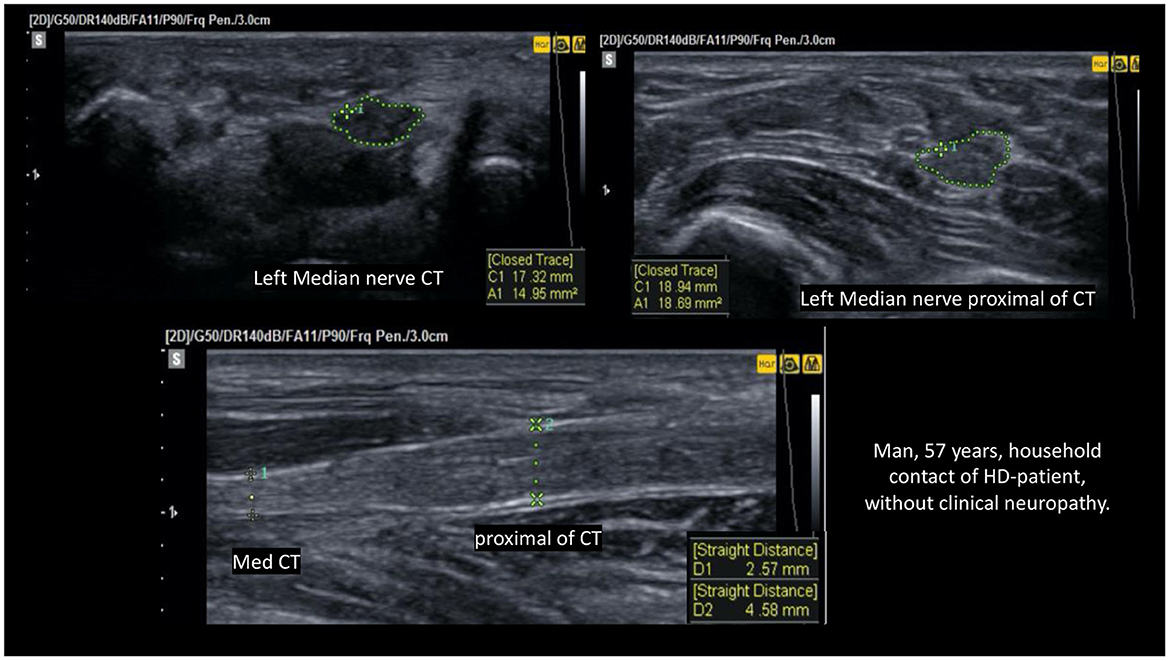
Figure 3. Fusiform thickening of the left median nerve regarding focality (ΔTpT) CSA pCT > CSA CT; ΔTpT = 18.69 −14.95 = 3.7 mm2 > ULV (upper limit value).
The nerves were considered to be enlarged when their CSA was greater than the mean ± 2 SD of the normal values established in the study by Voltan et al. (54).
To determine a possible relationship between the categorical variables, thickened nerves, neural points with asymmetry between right and left sides (ΔCSA), and nerves with the difference between segments of the same nerve (focality/ ΔTpT), we compared by the chi-square test and ROC curve household contacts of untreated patients diagnosed with HD, healthy individuals, and patients diagnosed with HD.
When we compared the mean, standard deviation, and median [Md ± SD (M)] values of the index of the number of nerves with increased CSA per individual, we detected a significant difference (p < 0.05) between all groups: healthy subjects [0.04 ± 0.09 (0)], HHC [0.27 ± 0.26 (0.2)], and HD [0.41 ± 0.29 (0.4)]. Regarding ΔCSA altered beyond normality, we detected the following differences: HVs [0.02 ± 0.08 (0)] x HHCs [0.3 ± 0.23 (0.2)] and HVs x HD [0.32 ± 0.24 (0.4)]. Also, we detected higher than normal neural focality (ΔTpT) in the HD group [0.24 ± 0.32 (0)] compared to HHCs [0.13 ± 0.27 (0)] and in the HHC group compared to HVs [0.03 ± 0.12 (0)].
When comparing healthy individuals to contacts of patients diagnosed with HD aged 15–60 years, we observed that the percentage of thickened nerves per nerve evaluated per individual was higher in contacts of patients with HD than in healthy subjects (p < 0.0001). Analysis by the ROC curve revealed that the AUC was 83.0 (95% CI: 75.4–90.5%, p < 0.0001), and when the percentage of altered nerves among those evaluated was higher than 16.5%, sensitivity reached 61.7% (CI: 49.9 to 72.4) and specificity reached 87.8% (75.8 to 94.3), with a relative risk of 5.0 (Figure 4).
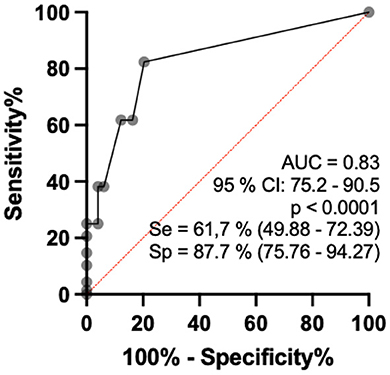
Figure 4. Analysis by the ROC curve of the percentage indices of altered nerves among the nerves evaluated per individual comparing the groups of healthy individuals and contacts of patients with HD aged 15–60 years.
Regarding the number of asymmetries between neural points (ΔCSA) per individual defined as altered (greater than the reference mean + 2DP) by the ROC curve, comparison between healthy individuals and contacts of patients diagnosed with leprosy aged 15–60 years revealed a ROC curve of 84.9 (95% CI: 0.77–0.92, p < 0.0001) and when the percentage index of neural points defined as asymmetric was >10% of the points evaluated, sensitivity was 82.3% (71.6–89.6) and specificity was 87.8% (75.76–94.27), with a relative risk of 6.72, as shown in Figure 5.
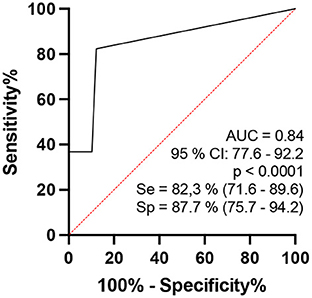
Figure 5. ROC curve analysis of the percentage indices of the number of asymmetries (ΔCSA) of the evaluated neural points considered to be altered per individual when comparing the groups of healthy persons and contacts of patients with HD (b – on the right).
In the analysis regarding the number of focalities among the points of the same nerve (ΔTpT) defined as altered (greater than the reference mean ± 2DP) per individual by the ROC curve, when comparing healthy individuals to contacts of patients diagnosed with HD aged 15–60 years, the area under the curve was 58.2 (95% CI: 0.50–0.65, p < 0.05), and when the percentage index of neural points defined as having focality was >25% of the points evaluated, sensitivity was 39.7% (32.8–47.1) and specificity was 76.4% (65.1–84.9), with a relative risk of 1.69, as shown in Figure 6.
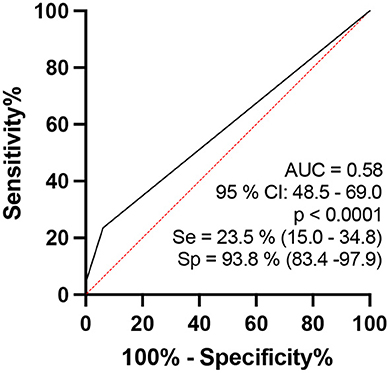
Figure 6. ROC curve analysis of the percentage indices of the number of focalities (ΔTpT) of the evaluated neural points considered to be altered per individual when comparing the groups of healthy persons and contacts of HD patients aged 15–60 years.
When we compared contacts of patients diagnosed with HD to patients aged 15–60 years, we observed that the percentage of thickened nerves per nerve evaluated per individual was higher among patients with HD than among their contacts (p = 0.0003). Considering analysis by the ROC curve, we observed that the AUC was 64.8 (95% CI: 0.57–0.72, p = 0.0003) and when the values of the percentage of altered nerves among those evaluated were higher than 55%, sensitivity reached 30.6% (CI: 24.3–37.8) and specificity reached 85.3% (75–91.8), with a relative risk of 2.0 (Figure 6). Considering the percentage index of specificity found (82.3%), for a binomial analysis, we divided our samples into individuals with up to 6 nerves altered (<6) and individuals with more than 6 nerves altered (≥6). The chi-square value with Yates' correction was 6.5 (p < 0.05), and we found that individuals with six or more thickened nerves had a relative risk of 0.48 and an odds ratio of 0.39 (Figure 7).
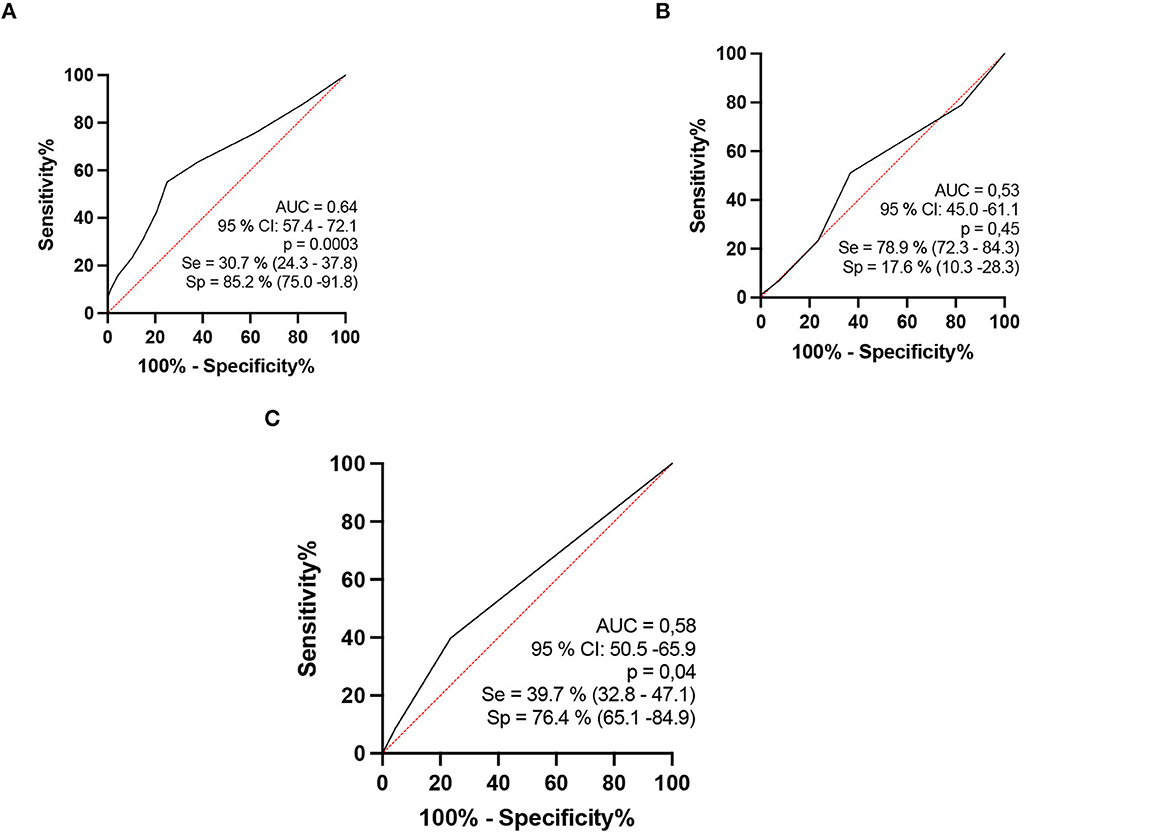
Figure 7. Analysis by the ROC curve comparing HHC and patients with HD aged 15–60 years: percentage indices of altered nerves among the nerves evaluated per individual [(A) up on the right]. The percentage indices of the number of asymmetries (ΔCSA) [(B) up on the left]. The percentage indices of the number of focalities (ΔTpT) [(C) as mentioned later].
We found only one article (55) in the literature that evaluated by the US a peripheral nerve of contacts of the patient diagnosed with HD (PubMed; keywords: leprosy + contacts + ultrasound + nerves), and three other authors suggested that the US can be used for the evaluation of HD contacts (55–57). To the best of our knowledge, our sample of the number of nerves evaluated with HRUS of peripheral nerves in HHC and patients must be the largest in the world.
When we analyze healthy individuals, contacts of patients diagnosed with HD, and patients with HD, we note neural involvement even before the individuals develop the disease. There is thickening with increased CSA in all nerves of HD contacts compared to healthy individuals although this thickening is lower compared to patients with HD. Our results support the findings of other studies by objectively demonstrating that the contact factor increases the risk of developing HD (6, 11, 13, 19, 22–24); furthermore, peripheral nerve US with an HD protocol demonstrated that the neuropathy secondary to HD is a multiple peripheral mononeuropathy, confirming the results of other authors (22, 40, 43, 44, 58–64).
Moreover, given the natural history of the disease, these data show the primary neural involvement of HD detected with objective diagnostic imaging criteria. We question whether this early peripheral nerve involvement might be a subclinical phase of the disease or a host immune response. In any case, if there is nerve involvement, it is to be expected that there was an interaction between the pathogen and host, although not all individuals do develop the disease (9–13, 16).
Regarding the morphological aspects of the behavior of the disease with respect to the involvement of peripheral nerves, when we analyze the asymmetry criteria, we can observe that the contacts of MB-patients with HD already have more asymmetrical nerves (median, ulnar and fibular), with above normal differences between the right and left sides when compared to healthy individuals, as observed by Frade et al. (40) and Lugão et al. (43) and also when healthy individuals are compared to patients. However, since asymmetry (ΔCSA) was already installed in household contacts, this criterion showed no difference between HHC and patients (Figure 8).
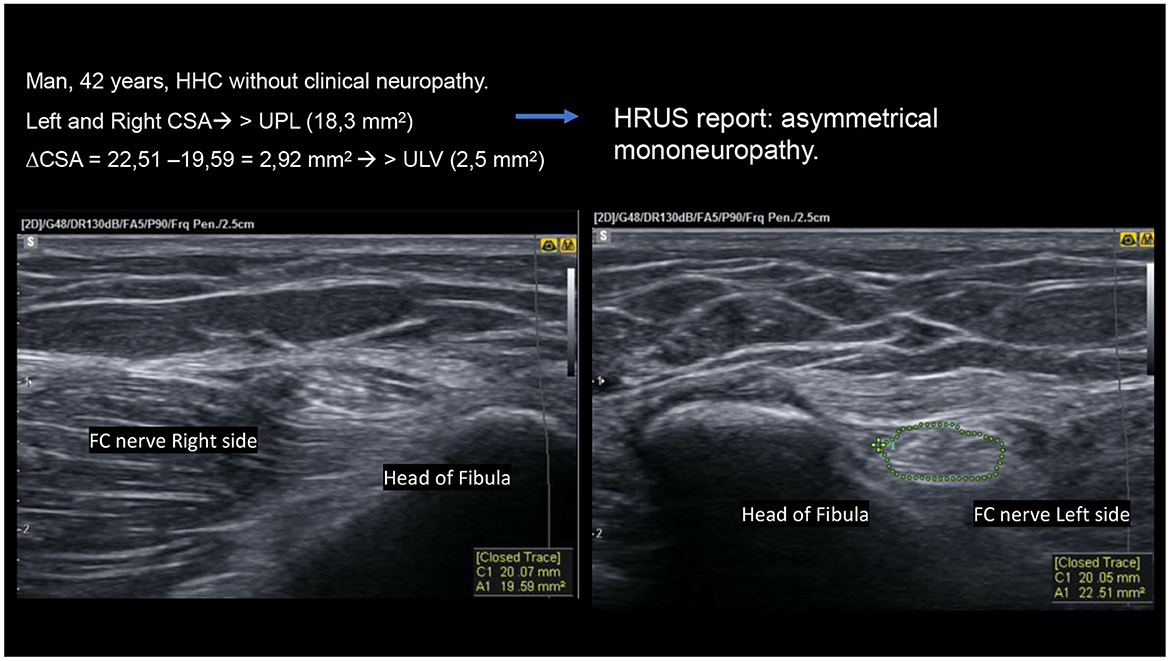
Figure 8. High-resolution ultrasound (HRUS) images of the same HHC of a patient with HD with asymmetrical mononeuropathy of the common fibular nerve on the head of the fibula.
Regarding focality within the same nerve, there was no difference between healthy subjects and contacts in the ulnar nerve; however, there was a difference between contacts and patients, demonstrating the late occurrence of this event in the natural history of the disease, as observed by Bathala et al. (59, 65) and Frade et al. (40) when comparing healthy individuals to those diagnosed with HD. The ΔTpT focality of the median nerve and the common fibular nerve was similar in HHCs and patients with HD.
Nagappa et al. (66) concluded that a median nerve enlargement of 2.0 cm proximal to the distal wrist crease distinguishes leprosy from carpal tunnel syndrome (CTS). In our study, we showed that patients with HD and their contacts had equal ΔTpT values in the median nerve, and the proportion of HHC with median nerve thickening in the carpal pre-tunnel had 4.1 OR with 90% specificity and positive predictive value compared to patients with HD. Thus, given the difference between healthy and sick subjects, we could characterize focality as a more specific marker of the disease (Figure 9). We would consider the asymmetry criteria to be more sensitive and probably of earlier detection for the characterization of peripheral nerve involvement in the evolutive phases of HD. This finding also shows that serial evaluation of leprosy contacts is a unique tool for assistance programs in public administration, being of help for an early diagnosis and thus contributing to the elimination of the disease (67).
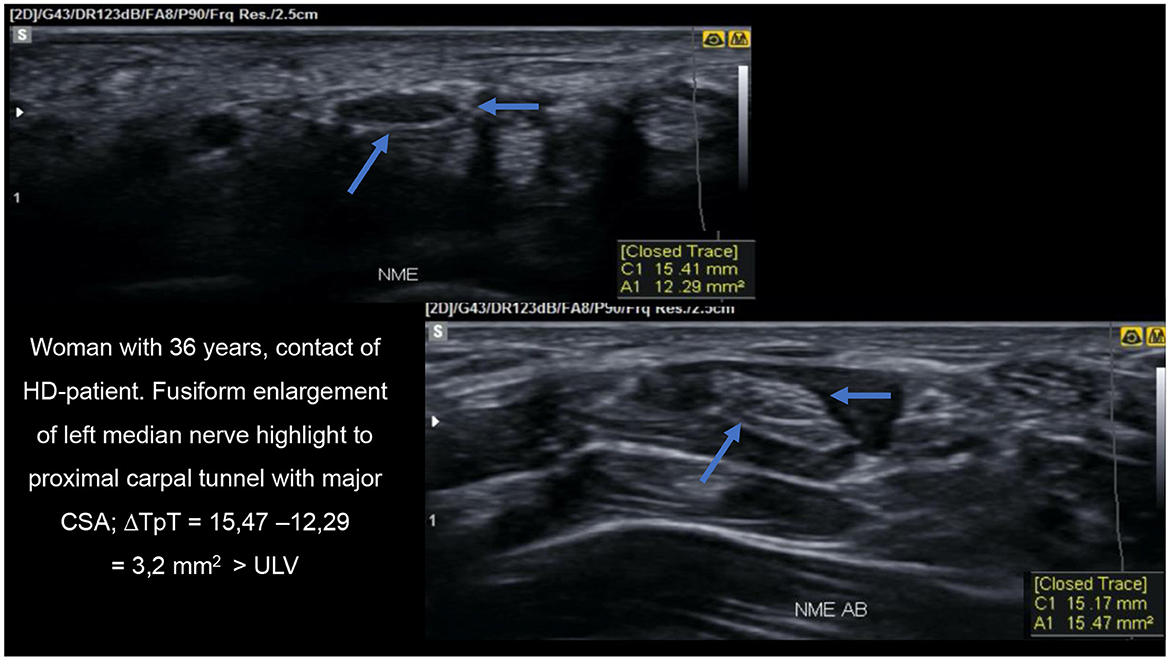
Figure 9. HRUS image demonstrating thickening of the median nerve proximal to the carpal tunnel on transverse view.
A meta-analysis of the accuracy of diagnostic tests for HD (68) that included 78 studies concluded that, although test accuracy appears reasonable, the studies suffered from heterogeneity and poor methodological quality, most of them evaluating the detection of IgM antibodies against phenolic glycolipid-I by ELISA with 63.8% sensitivity (95% CI: 55.0–71.8) and 91.0% specificity (95% CI: 86.9–93.9) in 39 of the studies while the sensitivity of qPCR (five studies) was 78.5% (95% CI: 61.9–89.2) and specificity was 89.3% (95% CI 61.4–97.8). The sensitivity of conventional PCR (17 studies) was 75.3% (95% CI 67.9–81.5) and specificity was 94.5% (95% CI: 91.4–96.5). Regarding peripheral nerve ultrasonography in the evaluation of HD neuropathy, several studies have considered it as a method with good efficacy, reproducibility, and diagnostic accuracy, besides its accessible cost and availability, even for point of care (40, 43, 47, 49, 59, 69–76).
Healthy individuals had nerves without thickening compared to contacts who had up to 20% of nerves with thickening and to patients who had up to 40% of nerves with increased CSA, results similar to those reported by Wilder-Smith et al. regarding neural dysfunction of peripheral nerves documented by ENMG, which was greater in patients with HD, followed by HHC and HVs (77). The same applies to the number of asymmetries per individual which was higher in HD compared to contacts and healthy individuals.
We also evaluated 4 new neural points in 21 contacts and 78 patients, for a total of 14 rather than 10 points. The AUC of the sum of the thickened nerves increased, thus also increasing the sensitivity and specificity of peripheral nerve US with a protocol for HD evaluation. However, increasing the number of neural points in the evaluation no longer revealed differences in asymmetry and focality between HHC and patients with HD, with the two groups being equal.
About the limitations of our study, perhaps a prospective study with an evaluation of the peripheral nerves of the contacts that show the neural thickening documented by the peripheral nerve US examination may bring more information regarding the development of the pathology. Another limitation of our study was that we did not have data on the ΔTpT (Δfocality) of the median and common fibular nerves of HVs. The data presented could also reflect on the individual's immunity acting against the nerve and promoting thickening and asymmetry, or the subclinical infection itself.
Peripheral nerve US with a protocol for HD (median, ulnar, common fibular, and tibial nerves) revealed HD as an asymmetric and/or focal peripheral multiple mononeuropathy.
Considering HRUS findings, if asymmetric multiple mononeuropathy signs (thickening or asymmetry) are detected in at least 20% of the nerves evaluated in the HHCs, these findings could already indicate evidence of HD neuropathy. Thus, if more nerve points are assessed in HHCs (14 instead of 10), these individuals become more like patients with HD according to the nerve thickening determined by HRUS, which should be a cutting-edge tool for an early diagnosis of leprosy cases.
Neural hypertrophy detected by HRUS in all peripheral nerve points seems to differentiate contacts from healthy volunteers, but the enlargement of three of seven neural points (median CT, ulnar-tunnel, and commun fibular nerve in pre-head fibula) was similar to that of patients with HD. Asymmetry of peripheral nerves was greater in the HHC group at all neural points compared to healthy volunteers, except in the tibial point, and was similar when compared to patients with HD at all points evaluated. Both findings could constitute important alerts for early and/or subclinical HD, mainly asymmetry, with 82.3% sensitivity and 87.7% specificity, respectively.
Finally, the peripheral nerve focalities of the median and common fibular nerves were similar for HHC and patients with HD, except for the ulnar nerve whose values were higher in patients with HD than in HHC. These data could also suggest important findings for the median and common fibular nerves of individuals with early and/or subclinical HD, which can be properly assessed only by HRUS, while ulnar nerve focality seems to be a late event in the natural course of the HD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
GV and MF contributed on all stage of this study, conception and design of the study, performed the statistical analysis, manuscript revision, read, and approved the submitted version. FB, ND, CMLS, ML, JS, JB, CGS, GC, and MD contributed to conception and design of the study, to data collection, obtaining, analyzing and interpreting data, and approved the submitted version. All authors contributed to the article and approved the submitted version.
This work was funded by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES) - Finance Code 001, National Council for Scientific and Technological Development (CNPq), Center of National Reference in Sanitary Dermatology and HD - Hospital of the Medical School of Ribeirão Preto, Ribeirão Preto, São Paulo, Brazil, the Brazilian Health Ministry (MS/FAEPAFMRP-USP: 749145/ 2010 and 767202/2011), Oswaldo Cruz Foundation (Fiocruz) Ribeirão Preto - TED163/2019 - Process: No. 25380.102201/2019-62/Project Fiotec: PRES-009-FIO-20, and VALE S.A. 27756/2019.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1059448/full#supplementary-material
1. Goulart IMB, Bernardes Souza DO, Marques CR, Pimenta VL, Gonçalves MA, Goulart LR. Risk and protective factors for leprosy development determined by epidemiological surveillance of household contacts. Clin Vaccine Immunol. (2008) 15:101–5. doi: 10.1128/CVI.00372-07
2. The Lancet Neurology. Leprosy as a neurological disease. Lancet Neurol. (2009) 8:217. doi: 10.1016/S1474-4422(09)70026-2
3. Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW, Williams DL. The continuing challenges of leprosy. Clin Microbiol Rev. (2006) 19:338–81. doi: 10.1128/CMR.19.2.338-381.2006
4. World Health Organization (WHO). Global leprosy (Hansen disease) update, 2020: impact of COVID-19 on global leprosy control. Wkly Epidemiol Rec. (2020) 96:421–44. Available online at: https://www.who.int/publications/i/item/who-wer9636-421-444
5. Salgado CG, Barreto JG, da Silva MB, Frade MAC, Spencer JS. What do we actually know about leprosy worldwide? Lancet Infect Dis. (2016) 16:778. doi: 10.1016/S1473-3099(16)30090-1
6. Goulart IMB, Goulart LR. Leprosy: diagnostic and control challenges for a worldwide disease. Arch Dermatol Res. (2008) 300:269–90. doi: 10.1007/s00403-008-0857-y
7. Carneiro M, Possuelo LG, Valim ARM. Neuropatia por hanseníase: atraso no diagnóstico ou um diagnóstico difícil? Cad Saude Publica. (2011) 27:2069. doi: 10.1590/S0102-311X2011001000020
8. de Oliveira MBB, Diniz LM. Leprosy among children under 15 years of age: literature review. An Bras Dermatol. (2016) 91:196–203. doi: 10.1590/abd1806-4841.20163661
9. Goulart LR, Goulart IMB. Leprosy pathogenetic background: a review and lessons from other mycobacterial diseases. Arch Dermatol Res. (2009) 301:123–37. doi: 10.1007/s00403-008-0917-3
10. Moet FJ, Meima A, Oskam L, Richardus JH. Risk factors for the development of clinical leprosy among contacts, and their relevance for targeted interventions. Lepr Rev. (2004) 75:310–26. doi: 10.47276/lr.75.4.310
11. Araujo S, Freitas LO, Goulart LR, Goulart IMB. Molecular evidence for the aerial route of infection of Mycobacterium leprae and the role of asymptomatic carriers in the persistence of leprosy. Clin Infect Dis. (2016) 63:1412–20. doi: 10.1093/cid/ciw570
12. Alter A, Grant A, Abel L, Alcaïs A, Schurr E. Leprosy as a genetic disease. Mamm Genome. (2011) 22:19–31. doi: 10.1007/s00335-010-9287-1
13. Patrocínio LG, Goulart IMB, Goulart LR, Patrocínio JA, Ferreira FR, Fleury RN. Detection of Mycobacterium leprae in nasal mucosa biopsies by the polymerase chain reaction. FEMS Immunol Med Microbiol. (2005) 44:311–6. doi: 10.1016/j.femsim.2005.01.002
14. Sharma R, Singh P, Loughry WJ, et al. Zoonotic leprosy in the southeastern United States. Emerg Infect Dis. (2015) 21:2127–34. doi: 10.3201/eid2112.150501
16. Mohanty PS, Naaz F, Katara D, et al. Viability of Mycobacterium leprae in the environment and its role in leprosy dissemination. Indian J Dermatol Venereol Leprol. (2016) 82:23–7. doi: 10.4103/0378-6323.168935
17. da Silva MB, Portela JM, Li W, et al. Evidence of zoonotic leprosy in Pará, Brazilian Amazon, and risks associated with human contact or consumption of armadillos. PLoS Negl Trop Dis. (2018) 12:6532. doi: 10.1371/journal.pntd.0006532
18. Douglas JT, Cellona RV, Fajardo TT, Abalos RM, Balagon MVF, Klatser PR. Prospective study of serological conversion as a risk factor for development of leprosy among household contacts. Clin Diagn Lab Immunol. (2004) 11:897–900. doi: 10.1128/CDLI.11.5.897-900.2004
19. Fine PEM, Sterne JAC, Pönnighaus JM, et al. Household and dwelling contact as risk factors for leprosy in northern Malawi. Am J Epidemiol. (1997) 146:91–102. doi: 10.1093/oxfordjournals.aje.a009195
20. Frade MAC, de Paula NA, Gomes CM, et al. Unexpectedly high leprosy seroprevalence detected using a random surveillance strategy in Midwestern Brazil: a comparison of ELISA and a rapid diagnostic test. PLoS Negl Trop Dis. (2017) 11:1–12. doi: 10.1371/journal.pntd.0005375
21. Lobato J, Costa MP, Reis Ede M, Gonçalves MA, Spencer JS, Brennan PJ, et al. Comparison of three immunological tests for leprosy diagnosis and detection of subclinical infection. Lepr Rev. (2011) 82:389–401.
22. Santos DF, Mendonça MR, Antunes DE, Sabino EF, Pereira RC, Goulart LR, et al. Molecular, immunological, and neurophysiological evaluations for early diagnosis of neural impairment in seropositive leprosy household contacts. PLoS Negl Trop Dis. (2018) 12:1–12. doi: 10.1371/journal.pntd.0006494
23. Gama RS, Gomides TA, Gama CF, Moreira SJ, de Neves Manta FS, de Oliveira LB, et al. High frequency of M. leprae DNA detection in asymptomatic household contacts. BMC Infect Dis. (2018) 18:1–6. doi: 10.1186/s12879-018-3056-2
24. Bazan-Furini R, Motta AC, Simão JC, Tarquínio DC, Marques W Jr, Barbosa MH, et al. Early detection of leprosy by examination of household contacts, determination of serum anti-PGL-1 antibodies and consanguinity. Mem Inst Oswaldo Cruz. (2011) 106:536–40. doi: 10.1590/S0074-02762011000500003
25. Wilder-Smith E, Wilder-Smith A, Van Brakel WH, Egger M. Vasomotor reflex testing in leprosy patients, healthy contacts and controls: a cross-sectional study in Western Nepal. Lepr Rev. (1996) 67:306–17. doi: 10.5935/0305-7518.19960031
26. Araújo S, Lobato J, Reis ÉD, Souza DO, Gonçalves MA, Costa AV, et al. Unveiling healthy carriers and subclinical infections among household contacts of leprosy patients who play potential roles in the disease chain of transmission. Mem Inst Oswaldo Cruz. (2012) 107(SUPPL.1):55–9. doi: 10.1590/S0074-02762012000900010
27. Feenstra SG, Nahar Q, Pahan D, Oskam L, Richardus JH. Social contact patterns and leprosy disease: a case-control study in Bangladesh. Epidemiol Infect. (2013) 141:573–81. doi: 10.1017/S0950268812000969
28. Vijayakumaran P, Jesudasan K, Mozhi NM, Samuel JDR. Does MDT Arrest transmission of leprosy to household contacts? Int J Lepr Other Mycobact Dis. (1998) 66:125–30.
29. Wilder-Smith E, Wilder-Smith A, Egger M. Peripheral autonomic nerve dysfunction in asymptomatic leprosy contacts. J Neurol Sci. (1997) 150:33–8. doi: 10.1016/S0022-510X(97)05363-X
30. Scollard DM. Endothelial cells and the pathogenesis of lepromatous neuritis: insights from the armadillo model. Microbes Infect. (2000) 2:1835–43. doi: 10.1016/S1286-4579(00)01335-6
31. Defaria RC, Silva MI. Electromyographic diagnosis of leprosy. Arq Neuro-psiquiatia. (1990) 48:403–13.
32. Frade MAC, Rosa DJ de F, Bernardes Filho F, Spencer JS, Foss NT. Semmes-Weinstein monofilament: A tool to quantify skin sensation in macular lesions for leprosy diagnosis. Indian J Dermatol Venereol Leprol. (2021) 87:807–15. doi: 10.25259/ijdvl_622_19
33. Kulshreshtha D, Malhotra KP, Malhotra HS, et al. Mandating nerve biopsy: a step towards personalizing therapy in pure neuritic leprosy. J Peripher Nerv Syst. (2018) 23:190–6. doi: 10.1111/jns.12283
34. Ashok Kumar SK, Reddy BSN, Ratnakar C. Correlation of skin and nerve histopathology in leprosy. Lepr Rev. (1996) 67:119–25. doi: 10.5935/0305-7518.19960012
35. V. P. SHETTY, L. N. MEHTA, N. H. ANTIA APFI. Teased fiber study of early nerve lesions in leprosy and in contacts, with electrophysiological correlates V. J of Neurol Neurosurg Psych. (1977) 40:708–11.
36. World Health Organization. Regional Office for South-East Asia. Guidelines for the diagnosis, treatment and prevention of leprosy. World Health Organization. (2018). Available online at: https://apps.who.int/iris/handle/10665/274127
37. Alemu Belachew W, Naafs B. Position statement: leprosy: diagnosis, treatment, and follow-up. J Eur Acad Dermatology Venereol. (2019) 33:1205–13. doi: 10.1111/jdv.15569
38. Chacha JJ, Peters L, Rivitti EA, Sotto MN, Lourenço S, Melnikov P. Sistema nervoso periférico e pressupostos da agressão neural na hanseníase. An Bras Dermatol. (2009) 84:495–500. doi: 10.1590/S0365-05962009000500008
39. Filho FB, De Paula NA, Leite MN, et al. Evidence of hidden leprosy in a supposedly low endemic area of Brazil. Mem Inst Oswaldo Cruz. (2017) 112:822–8. doi: 10.1590/0074-02760170173
40. Frade MA, Nogueira-Barbosa MH, Lugão HB, Furini RB, Marques Junior W, Foss NT, et al. New sonographic measures of peripheral nerves: a tool for diagnosis of peripheric nerve involvment in leprosy. Hansenol Int. (2013) 36:71. doi: 10.1590/s0074-02762013000300001
41. Garbino JA, Marques W Jr, Barreto JA, Heise CO, Rodrigues MM, Antunes SL, et al. Hanseníase neural primária: revisão sistemática. Arq Neuropsiquiatr. (2013) 71:397–404. doi: 10.1590/0004-282X20130046
42. Lugão HB, Frade MAC, Marques W Jr, Foss NT, Nogueira-Barbosa MH. Ultrasonography of leprosy neuropathy: a longitudinal prospective study. Small PLC, ed PLoS Negl Trop Dis. (2016) 10:e0005111. doi: 10.1371/journal.pntd.0005111
43. Lugão HB, Nogueira-Barbosa MH, Marques W, Foss NT, Frade MAC. Asymmetric nerve enlargement: a characteristic of leprosy neuropathy demonstrated by ultrasonography. PLoS Negl Trop Dis. (2015) 9:1–11. doi: 10.1371/journal.pntd.0004276
44. Scollard DM, Truman RW, Ebeneze GJ. Mechanisms of nerve injury in leprosy. Clin Dermatol. (2015) 33:46–54. doi: 10.1016/j.clindermatol.2014.07.008
45. El Gency HI, Ghanema M, Hussein SA, Almaghraby OS, Rashad W. Peripheral neuropathy is not the end but the beginning. Lepr Rev. (2017) 88:574–82. doi: 10.47276/lr.88.4.574
46. Van Brakel WH, Saunderson P, Shetty V, Brandsma JW, Post E, Jellema R, et al. International workshop on neuropathology in leprosy–consensus report. Lepr Rev. (2007) 78:416–33.
47. Lugão HB. Avaliação da reprodutibilidade da ultrassonografia de nervos periféricos em pacientes com hanseníase e voluntários saudáveis. (2015) 40(Suppl 1):19825161.
48. Wortsman X, Jemec GBE. Dermatologic Ultrasound with Clinical and Ultrasound Correlations. 1st ed. New York, NY: Springer (2013). doi: 10.1007/978-1-4614-7184-4
49. Martinoli C, Derchi LE, Bertolotto M. US and MR imaging of peripheral nerves in leprosy. Skeletal Radiol. (2000) 29:142–50. doi: 10.1007/s002560050584
50. Kara M, Özçakar L, De Muynck M, Tok F, Vanderstraeten G. Musculoskeletal ultrasound for peripheral nerve lesions. Eur J Phys Rehabil Med. (2012) 48:665–74.
51. Martinoli C, Bianchi S, Derchi LE. Ultrasonography of peripheral nerves. Semin Ultrasound CT MRI. (2000) 21:205–13. doi: 10.1016/S0887-2171(00)90043-X
52. Schenone A, Martinoli C. Ultrasonography of peripheral nerves. Neurol Sci. (2000) 21(4 SUPPL.):205–213.
53. Voltan G, Bernards Filho F, Leite MN, De Paula NA, Santana JM, Silva CM, et al. Point-of-care ultrasound of peripheral nerves in the diagnosis of Hansen's disease neuropathy. Front Med. (2022) 9:5252. doi: 10.3389/fmed.2022.985252
54. Voltan G, Bernardes-filho F, Nogueira-barbosa MH, Andrey M, Frade C. Ultrasound reference values for peripheral nerve cross-sectional areas and indices in a sample of healthy individuals in Brazil. Radiol Brasil. (2022) 55:337–45. doi: 10.1590/0100-3984.2022.0020
55. Neto FB de A, Neto RA, Cardoso LMC. The first report of pure neuritic leprosy with involvement of the anterior femoral cutaneous nerve. Neurol Int. (2019) 11:15–7. doi: 10.4081/ni.2019.8001
56. Nagappa M, Visser LH, Bathala L. Peripheral nerve sonography, a novel technique for improving the diagnosis of Hansen's neuropathy. Lepr Rev. (2021) 92:202–6. doi: 10.47276/LR.92.3.202
57. Elias J Jr, Nogueira-Barbosa MH, Feltrin LT, Furini RB, Foss NT, Marques W Jr, et al. Role of ulnar nerve sonography in leprosy neuropathy with electrophysiologic correlation. J Ultrasound Med. (2009) 28:1201–9. doi: 10.7863/jum.2009.28.9.1201
58. Bernardes-Filho F, Lima FR, Voltan G, de Paula NA, Frade MAC. Leprosy case series in the emergency room: a warning sign for a challenging diagnosis. Brazilian J Infect Dis. (2021) 25:1634. doi: 10.1016/j.bjid.2021.101634
59. WHO. Weekly epidemiological record. Global leprosy update, 2018: moving towards a leprosyfree world. Wkly Epidemiol Rec. (2019) 94:389–412. Available online at: https://www.who.int/publications/i/item/who-wer9435-36
60. Bathala LN, Krishnam V, Kumar HK, Neladimmanahally V, Nagaraju U, Kumar HM, et al. Extensive sonographic ulnar nerve enlargement above the medial epicondyle is a characteristic sign in Hansen's neuropathy. PLoS Negl Trop Dis. (2017) 11:1–10. doi: 10.1371/journal.pntd.0005766
61. Kumar N, Malhotra HS, Garg RK, et al. Comprehensive electrophysiology in leprous neuropathy - Is there a clinico-electrophysiological dissociation? Clin Neurophysiol. (2016) 127:2747–55. doi: 10.1016/j.clinph.2016.05.002
62. Nascimento OJM. Neuropatia da lepra: apresentações clínicas. Arq Neuropsiquiatr. (2013) 71:661–6. doi: 10.1590/0004-282X20130146
63. Jardim MR, Antunes SL, Santos AR, Nascimento OJ, Nery JA, Sales AM, et al. Criteria for diagnosis of pure neural leprosy. J Neurol. (2003) 250:806–9. doi: 10.1007/s00415-003-1081-5
64. Garbino JA, Ura S, Belone A de FF, Marciano LHSC, Fleury RN. Aspectos clínicos e diagnósticos da hanseníase primariamente neural. Hansen Int. [Internet]. 30° de novembro de 1994 [citado 30° de dezembro de 2022]. (2022) 19:124–9. Available online at: https://periodicos.saude.sp.gov.br/hansenologia/article/view/36507
65. dos Santos DF. Aspectos clínicos, moleculares, sorológicos e neurofisiológicos no diagnóstico precoce da neuropatia hansênica. Tese apresentando ao Programa Pó-graduação em Ciências da Saúde da Fac Med da Univ Fed Uberlância, como requisito para obtenção do título Doutor em Ciências da Saúde. (2017) 178.
66. Bathala L, Kumar K, Pathapati R, Jain S, Visser LH. Ulnar neuropathy in Hansen disease: clinical, high-resolution ultrasound and electrophysiologic correlations. J Clin Neurophysiol. (2012) 29:190–3. doi: 10.1097/WNP.0b013e31824d969c
67. Nagappa M, Pujar GS, Keshavan AH, Bathala L, Jain RD, Das A, et al. Sonographic pattern of median nerve enlargement in Hansen's neuropathy. Acta Neurol Scand. (2021) 144:155–60. doi: 10.1111/ane.13432
68. Bechelli LM. Prospects of global elimination of leprosy as a public health problem by the year 2000. Int J Lepr Other Mycobact Dis. (1994) 62:284–92.
69. Gurung P, Gomes CM, Vernal S, Leeflang MMG. Diagnostic accuracy of tests for leprosy: a systematic review and meta-analysis. Clin Microbiol Infect. (2019) 25:1315–27. doi: 10.1016/j.cmi.2019.05.020
70. Visser LH, Jain S, Lokesh B, Suneetha S, Subbanna J. Morphological changes of the epineurium in leprosy: a new finding detected by high-resolution sonography. Muscle and Nerve. (2012) 46:38–41. doi: 10.1002/mus.23269
71. Jain S, Visser LH, Suneetha S. Imaging techniques in leprosy clinics. Clin Dermatol. (2016) 34:70–8. doi: 10.1016/j.clindermatol.2015.10.014
72. Bignotti B, Tagliafico A, Martinoli C. Ultrasonography of peripheral nerves: anatomy and pathology. Ultrasound Clin. (2014) 9:525–36. doi: 10.1016/j.cult.2014.03.006
73. Jain S, Raju R, Visser LH. The diagnostic value of assessing nerve damage by high-resolution sonography and color Doppler in leprosy patients. In: 18th International Leprosy Congress. (2013).
74. Frijlink DW, Brekelmans GJF, Visser LH. Increased nerve vascularization detected by color Doppler sonography in patients with ulnar neuropathy at the elbow indicates axonal damage. Muscle and Nerve. (2013) 47:188–93. doi: 10.1002/mus.23505
75. Becker DM, Tafoya CA, Becker SL, Kruger GH, Tafoya MJ, Becker TK. The use of portable ultrasound devices in low- and middle-income countries: a systematic review of the literature. Trop Med Int Heal. (2016) 21:294–311. doi: 10.1111/tmi.12657
76. Wheat SW, Stryjewska B, Cartwright MS, A. Hand-held ultrasound device for the assessment of peripheral nerves in leprosy. J Neuroimaging. (2021) 31:76–8. doi: 10.1111/jon.12797
Keywords: leprosy, Hansen's disease, household contacts, neuropathy, high-resolution ultrasound, cross-sectional area (CSA), multiple mononeuropathy
Citation: Voltan G, Marques-Júnior W, Santana JM, Lincoln Silva CM, Leite MN, De Paula NA, Bernardes Filho F, Barreto JG, Da Silva MB, Conde G, Salgado CG and Frade MAC (2023) Silent peripheral neuropathy determined by high-resolution ultrasound among contacts of patients with Hansen's disease. Front. Med. 9:1059448. doi: 10.3389/fmed.2022.1059448
Received: 01 October 2022; Accepted: 21 December 2022;
Published: 17 January 2023.
Edited by:
Federica Veronese, Azienda Ospedaliero Universitaria Maggiore della Carità, ItalyReviewed by:
Bernard Naafs, Stichting Global Dermatology, NetherlandsCopyright © 2023 Voltan, Marques-Júnior, Santana, Lincoln Silva, Leite, De Paula, Bernardes Filho, Barreto, Da Silva, Conde, Salgado and Frade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Glauber Voltan,  Z3ZvbHRhbkBnbWFpbC5jb20=; ZHJnbGF1YmVyQGh1bWFuaXphcmVqdWluYS5jb20=; Marco Andrey Cipriani Frade, bWFuZHJleUBmbXJwLnVzcC5icg==
Z3ZvbHRhbkBnbWFpbC5jb20=; ZHJnbGF1YmVyQGh1bWFuaXphcmVqdWluYS5jb20=; Marco Andrey Cipriani Frade, bWFuZHJleUBmbXJwLnVzcC5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.