
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 12 December 2022
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1056374
 David Martínez-López1
David Martínez-López1 Ivan Ferraz-Amaro2Diana Prieto-Peña1Lara Sánchez-Bilbao1Alba Herrero-Morant1Carmen Álvarez-Reguera1Fabricio Benavides-Villanueva1Cristina Corrales-Selaya1Martín Trigueros-Vázquez1
Ivan Ferraz-Amaro2Diana Prieto-Peña1Lara Sánchez-Bilbao1Alba Herrero-Morant1Carmen Álvarez-Reguera1Fabricio Benavides-Villanueva1Cristina Corrales-Selaya1Martín Trigueros-Vázquez1 Miguel Ángel González-Gay1
Miguel Ángel González-Gay1 Ricardo Blanco1*
Ricardo Blanco1*Background: COVID-19 may present different degrees of severity. Viral infections in patients with rheumatic inflammatory diseases (R-IMID) trend to present more severe disease. However, data comparing the severity of the disease between R-IMID and the general population are scarce.
Objectives: To compare predisposing factors, clinical, serological features, and severity of COVID-19 infection in patients with and without R-IMID.
Methods: Case-control study in a single University Hospital. We included all consecutive patients with a diagnosis of an R-IMID and COVID-19 infection up to March 31st, 2021. This cohort was compared to patients without R-IMID and not receiving immunosuppressive therapy, matched for sex and age (±5 years). Confirmed infection was defined if a patient had a positive nasopharyngeal swab for SARS-CoV-2. Severity was divided into mild, moderate, severe and critical according to the United States National Institute of Health (NIH) guidelines.
Results: We included 274 R-IMID patients (185 women/89 men), mean age 59.1 ± 18 years. More frequent R-IMID were: Rheumatoid arthritis (28.8%), Psoriatic Arthritis (20.1%), axial Spondyloarthritis (12.4%), Polymyalgia Rheumatica (8%) and Systemic Lupus Erythematosus (8%). Hypertension and dyslipidemia were more frequent in patients with R-IMID. Although most of the cases were mild, critical cases and deaths were more frequent in R-IMID. When adjusted by comorbidities, no statistical differences were observed.
Conclusion: R-IMID have a very similar clinical presentation when compared to the general population. There is a trend to an increased severity of the disease in patients with R-IMID.
It is not clearly established whether patients with R-IMID are at risk of a more severe COVID-19. Regarding the treatments received, it is known that Rituximab is associated with a worse prognosis. This is unclear for other treatments used in R-IMID. Risk factors specific to patients with R-IMID have not been established.
Patients with R-IMID present a trend to an increased severity of COVID-19 infection, not reaching statistical significance when adjusted by comorbidities. Receiving Rituximab is associated with worse outcomes in patients with COVID-19 and R-IMID. We identified various severity factors for severe disease in patients with COVID-19 and R-IMID. Of these factors, the one with higher odds ratio was receiving Rituximab.
These findings might be useful for a better risk stratification for patients with COVID-19 and R-IMID. This stratification can be useful to decide which patients might benefit from treatments for COVID-19 at the onset of the disease.
Since the first cases described in Wuhan (China) in December 2019, coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic (1, 2).
According to the World Health Organization (WHO), there have been more than four hundred million cases of COVID-19, including almost four million deaths (2).
The severity of COVID-19 ranges from asymptomatic or mild cases to a life-threatening disease that can result in fatal outcomes. Several poor prognostic factors have been identified, including advanced age, obesity, smoking history, diabetes mellitus, and immunosuppression (3).
Patients with rheumatic immune-mediated inflammatory diseases (R-IMID) may have a global increased risk of infections due to the disease itself, comorbidities and/or immunosuppressive therapy (4–6).
However, data regarding the severity of COVID-19 in patients with R-IMID and immunosuppressive therapy have been controversial. Some studies have found an increased risk of COVID-19 severity in patients with R-IMID (7–10).
By contrast, other studies have not confirmed these results, and conclude that there is no increased risk of severity in patients with R-IMID (11–14).
However, most of the evidence mentioned relies on small case series of patients and seldom compares the results in these patients with the general population.
A recent systematic review and meta-analysis by Xu et al. (15) including 31 articles and 1,138 patients concluded that patients with R-IMID have substantial rates of severe outcomes. However, this study shows important geographical variations in these outcomes and most of the studies included do not establish a comparison with the general population.
Regarding immunosuppressive therapy received by R-IMID patients, the available evidence points to an increased severity of COVID-19 in patients in treatment with rituximab (RTX) (9, 16, 17).
However, data regarding other immunosuppressive therapies, such as glucocorticoids, cDMARDs or other biologic or synthetic DMARDs remain unclear (10, 14, 18, 19).
In the previous studies carried out in populations with COVID-19 and R-IMID, some comorbidities have been reported to be related with worse outcomes. This is the case of older age at presentation, hypertension, diabetes mellitus, obesity and previous heart disease (8, 19–22).
Lymphopenia has also been identified as a risk factor for severe COVID-19 in the general population. However, this has not been assessed in the population with R-IMID. High levels of CRP, D-dimer, LDH, ferritin, IL-6, and elevated liver enzymes and creatinine have also been proposed as increased severity factors (22).
To our knowledge, the difference between the clinical presentation of COVID-19 and the laboratory findings between patients with R-IMID and the general population have not been analyzed. In the general population, the presence of dyspnea and gastrointestinal symptoms have been associated with increased severity of the disease (22).
To sum up, most of the evidence published points toward an increased severity of COVID-19 in patients with R-IMID, but the evidence behind this statement is still weak Therefore, further research is needed on this topic. The purpose of our study was to compare predisposing factors, clinical, serological features, severity and mortality of COVID-19 infection in patients with and without R-IMID.
We carried out a retrospective case-control study in a single University Hospital. We included all consecutive patients with a diagnosis of a R-IMID and a positive test for COVID-19 up to March 31st, 2021.
Rheumatic immune-mediated inflammatory disease was diagnosed by expert rheumatologists from our center according to current classification criteria for each R-IMID. Confirmed COVID-19 was defined if the patient had a positive polymerase chain reaction (PCR) test in nasopharyngeal swab for SARS-CoV-2.
A total of 274 patients with R-IMID and COVID-19 infection were identified. Therefore, 274 controls were selected, and matched by sex and age (±5 years). Controls were defined as patients with a positive PCR in nasopharyngeal swab for SARS-CoV-2, but without any R-IMID diagnosis and not receiving immunosuppressive therapy.
A total of 70 patients of each group (25.5%) required hospitalization due to the severity of COVID-19. The rest of the patients of this study (74.5%) were not admitted to the hospital.
Many classifications have been used to classify the different severity grades of the disease. We used the United States National Institute of Health (NIH) guidelines since they are one of the most trusted. This guideline divides COVID-19 case severity into mild, moderate, severe or critical disease according to various clinical and radiological parameters (23).
The main outcome variables for this study were: (a) Severity of COVID-19 in patients with R-IMID and controls according to NIH guidelines and (b) Mortality of COVID-19 in both groups.
Data were obtained from the patients’ clinical records after the patient was considered cured from the disease or suffered a mortal outcome. Patients were considered to be cured from COVID-19 when the symptoms disappeared and a negative PCR test in nasopharyngeal swab for SARS-CoV 2 was obtained.
For all patients with COVID-19, we obtained the following data from their medical records: Sex, age, presence of comorbidities and cardiovascular risk factors, previous diagnosis of R-IMID, treatment for R-IMID at the onset of the symptoms, previous therapies for R-IMID, COVID-19 symptoms, analytical data, including CRP, creatinine, leukocytes, lymphocytes (at the onset of COVID-19 and previous), hemoglobin, platelets, ferritin, LDH, D-Dimer…), therapies for COVID-19 and severity of the disease according to NIH guidelines and mortality.
Results were expressed as mean ± standard deviation (SD) for variables with a normal distribution, or as median and interquartile range (IQR) for those not normally distributed. Percentages were shown for categorical variables Student’s t-test or Mann-Whitney U-test were used to compare continuous variables as appropriate. The chi-square test or the Fisher exact test were used to assess differences between categorical variables. Multivariable logistic regression analysis, adjusting for confounders, was assessed to analyze the association between COVID-19 infection severity and mortality. Confounding variables were selected from demographics and traditional CV risk factors if they had a p-value lower than 0.20. A p-value <0.05 was considered statistically significant in all the calculations. Data management and analysis were performed using SPSS for Windows version 25 (SPSS Inc, Chicago, IL, USA).
We carried out a review of the literature in search of previous case-control studies performed in patients with COVID-19 and R-IMID.
The search was performed in the month of December 2021. The objective of this review was clarifying if patients with R-IMID have a more severe course of COVID-19.
We searched articles in the bases of PubMed, Scielo, and Cochrane Library.
We used the terms COVID-19 + SARS-CoV2 + R-IMID + rheumatic inflammatory disease + rheumatoid arthritis + connective tissue disease + case-control in different combinations. The inclusion criteria were: (1) the study included both patients with R-IMID and COVID-19, and (2) the study was a case-control study.
We included 274 patients with R-IMID patients and COVID-19 infection. Table 1 summarizes the underlying diseases and immunosuppressive therapy. The most frequent R-IMID was rheumatoid arthritis (n = 79, 28.8%), followed by psoriatic arthritis (n = 55, 20.1%) and spondyloarthritis (n = 34, 12.4%). At the onset of COVID-19 infection, 27% of the patients (n = 75) were receiving treatment with at least one conventional DMARD. The most frequently used cDMARD was methotrexate (n = 62, 23%) followed by hydroxychloroquine (n = 50, 18%). Biological DMARDs were used in 60 patients (21.9%), being the most frequently used TNF inhibitors (n = 41, 15%). Also, a considerable number of patients (n = 77, 28%) were receiving treatment with oral glucocorticoids.
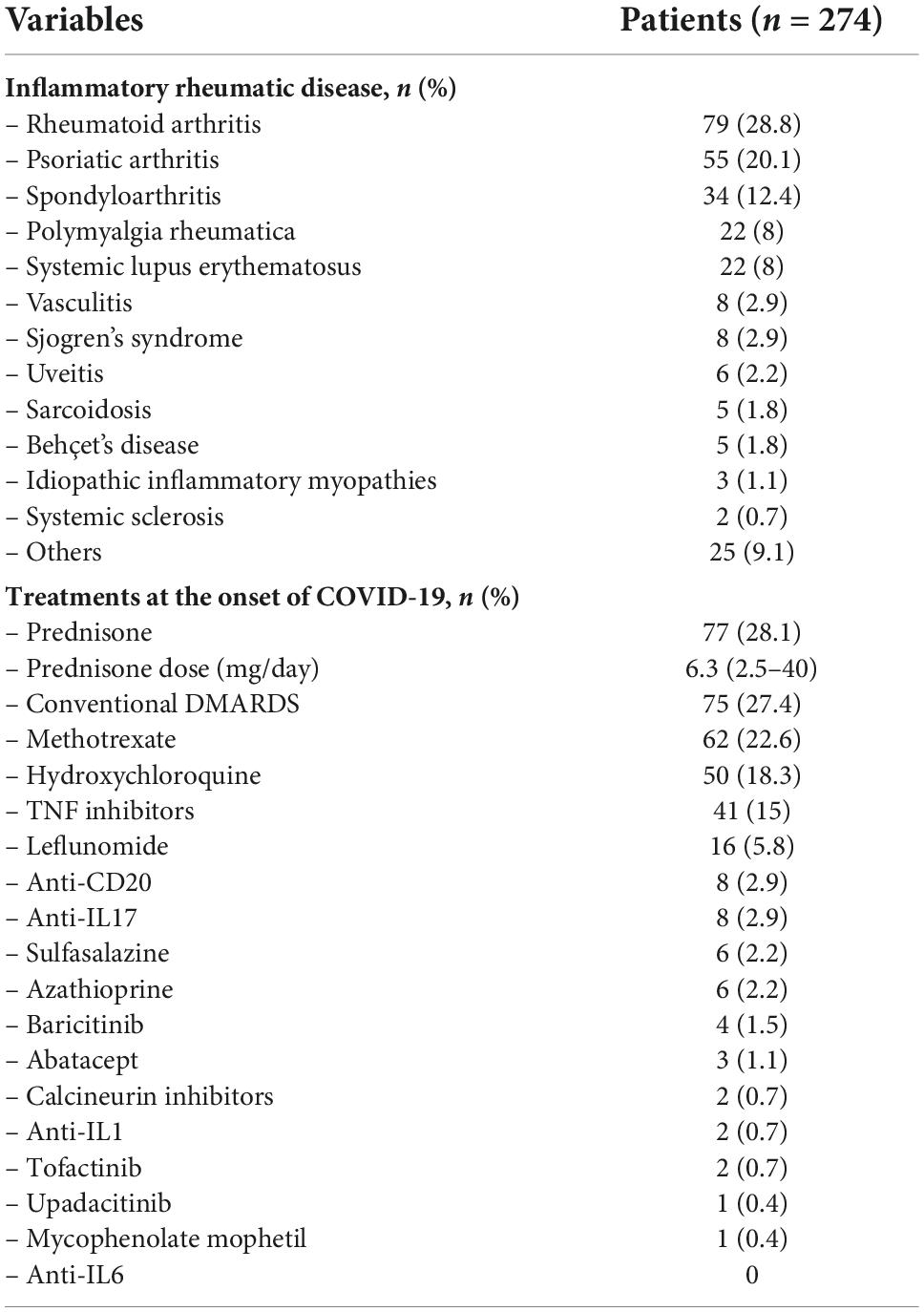
Table 1. Underlying diseases and immunosuppressive therapy in 274 patients with inflammatory rheumatology diseases complicated with coronavirus disease 2019 (COVID-19).
We also included 274 COVID-19 matched-controls without R-IMID or immunosuppressive therapy. The main characteristics of both groups are shown in Table 2.
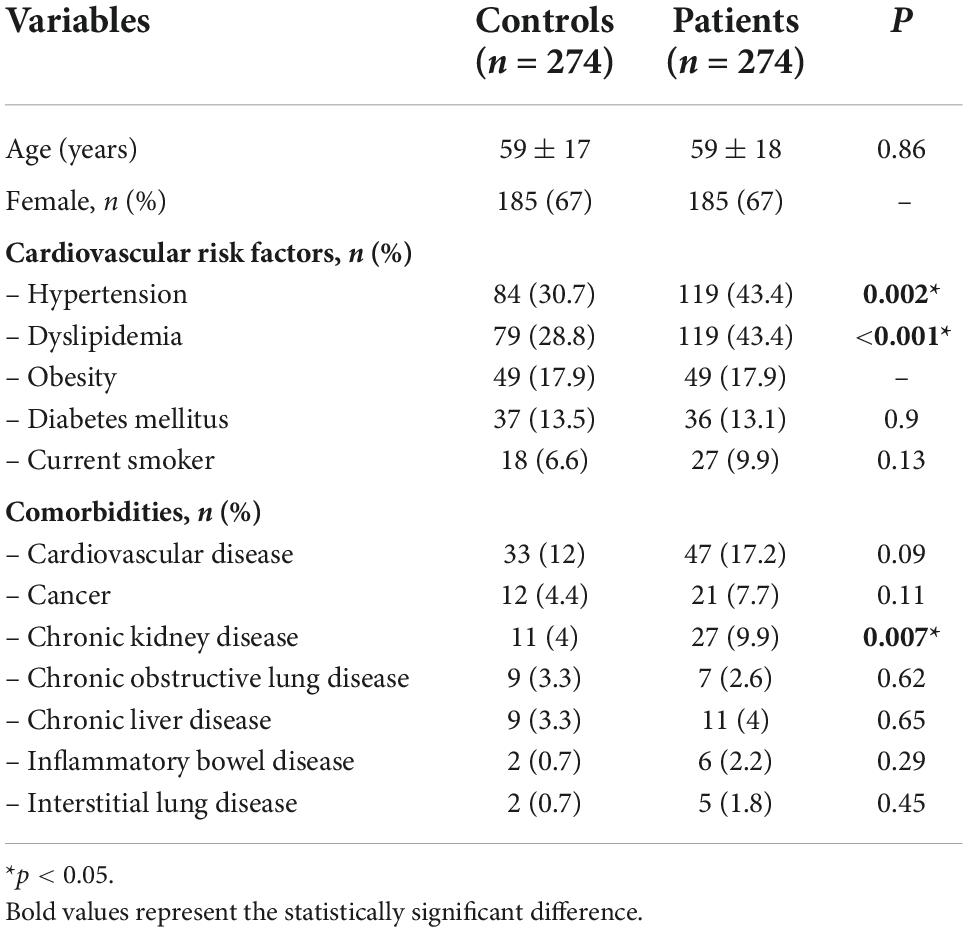
Table 2. Demographics, cardiovascular risk factors and comorbidities in coronavirus disease (COVID) patients with inflammatory rheumatology diseases versus controls.
In both groups most patients were female (67%) with a mean age of 59 ± 18 years.
Hypertension, dyslipidemia and chronic kidney disease were significantly more frequent in patients with R-IMID when compared to controls. No other significant differences were found in the remaining comorbidities analyzed.
In the whole group, most of the patients (n = 383, 69.9%) showed symptoms related to COVID-19, while the remaining were asymptomatic (Table 3).
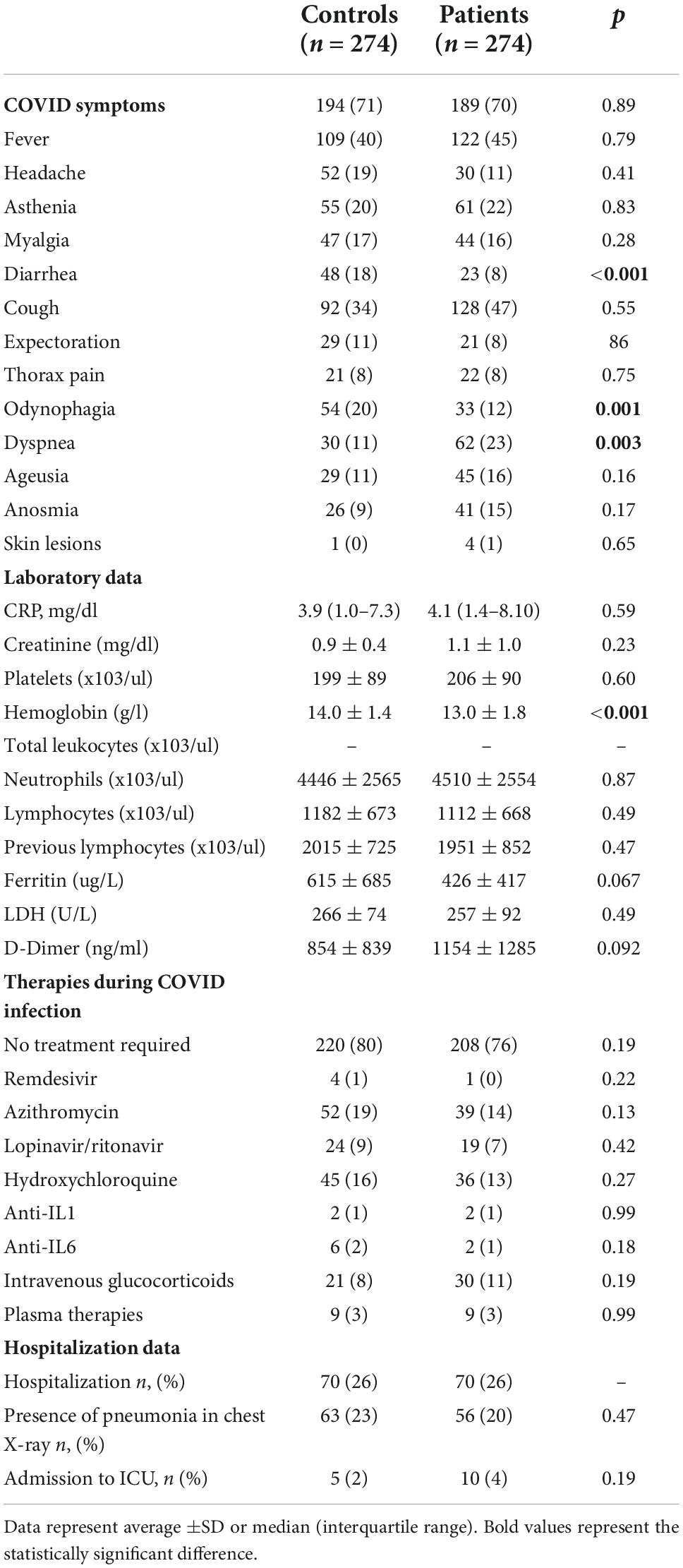
Table 3. Main clinical, analytical and therapy of coronavirus (COVID) disease in patients with rheumatic immune-mediated diseases (IMIDs) and case controls.
The most frequent symptoms were: fever (n = 231, 42.2%), cough (n = 220, 40.1%) and asthenia (n = 116, 21.2%). Dyspnea was more frequent in the R-IMID group, while diarrhea and odynophagia were more frequent in the control group. No other statistically significant differences were found in the rest of the symptoms between both groups.
When analyzing laboratory parameters (Table 3) no differences were found between both groups in the values of C-reactive protein, platelets, leukocytes, lymphocytes, ferritin or D-Dimer. Hemoglobin values were significantly lower in the R-IMID group.
Therapies used for COVID-19 in both groups are shown in Table 3.
Other data regarding the severity of the disease are shown in Table 3. As mentioned previously, 70 patients (25.5%) in each group were admitted to the hospital. Therefore, there were no differences regarding the hospitalization rate between both groups. Presence of pneumonia in plain chest X-ray was found in 63 patients (23%) in the control group, and in 56 patients (20%) in the R-IMID group. No statistical differences were found between both groups.
A total of five patients (2%) in the control group were admitted to the intensive care unit (ICU), while 10 patients (4%) in the R-IMID were admitted to the ICU. However, these differences did not reach statistical significance.
Statistical analysis of severity of patients with R-IMID compared to controls is shown in Table 4. In the crude analysis the results indicate that there is a significant difference between both groups with an increased severity in patients with R-IMID.
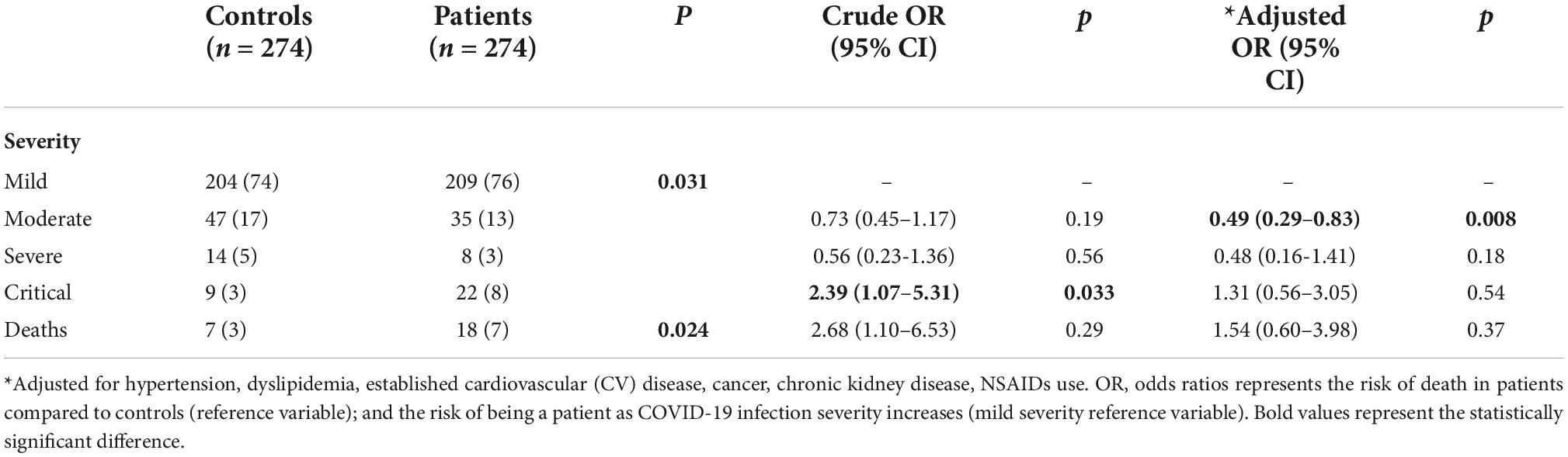
Table 4. Coronavirus disease 2019 (COVID-19) severity and deaths in patients and controls.
However, when these results are adjusted by comorbidities, there were no statistical significant difference between both groups.
When analyzing thrombotic events, three patients in the R-IMID group suffered thrombotic events (deep vein thrombosis in one case and pulmonary embolism in two cases) while only one patients in the control group suffered a thrombotic event (deep vein thrombosis). There were no statistically significant differences between both groups.
Regarding mortality, there were 18 deaths (7%) in the R-IMID group, with only seven deaths (3%) in the control group, with a crude odds ratio of 2.68. However, in the adjusted analysis, there were no statistically significant differences between both groups.
In Table 5, we compared the main characteristics of R-IMID patients who had mild COVID-19 infection with those who developed severe COVID-19 infection. In this analysis, we identified risk factors for severe COVID-19 infection in R-IMID patients: age higher than 65 years old, hypertension, dyslipidemia and the presence of cardiovascular, kidney or pulmonary diseases. Regarding analytical findings, the presence of increased levels of creatinine and lymphopenia were also associated with worse outcomes. Rituximab was the only treatment associated with severe disease.
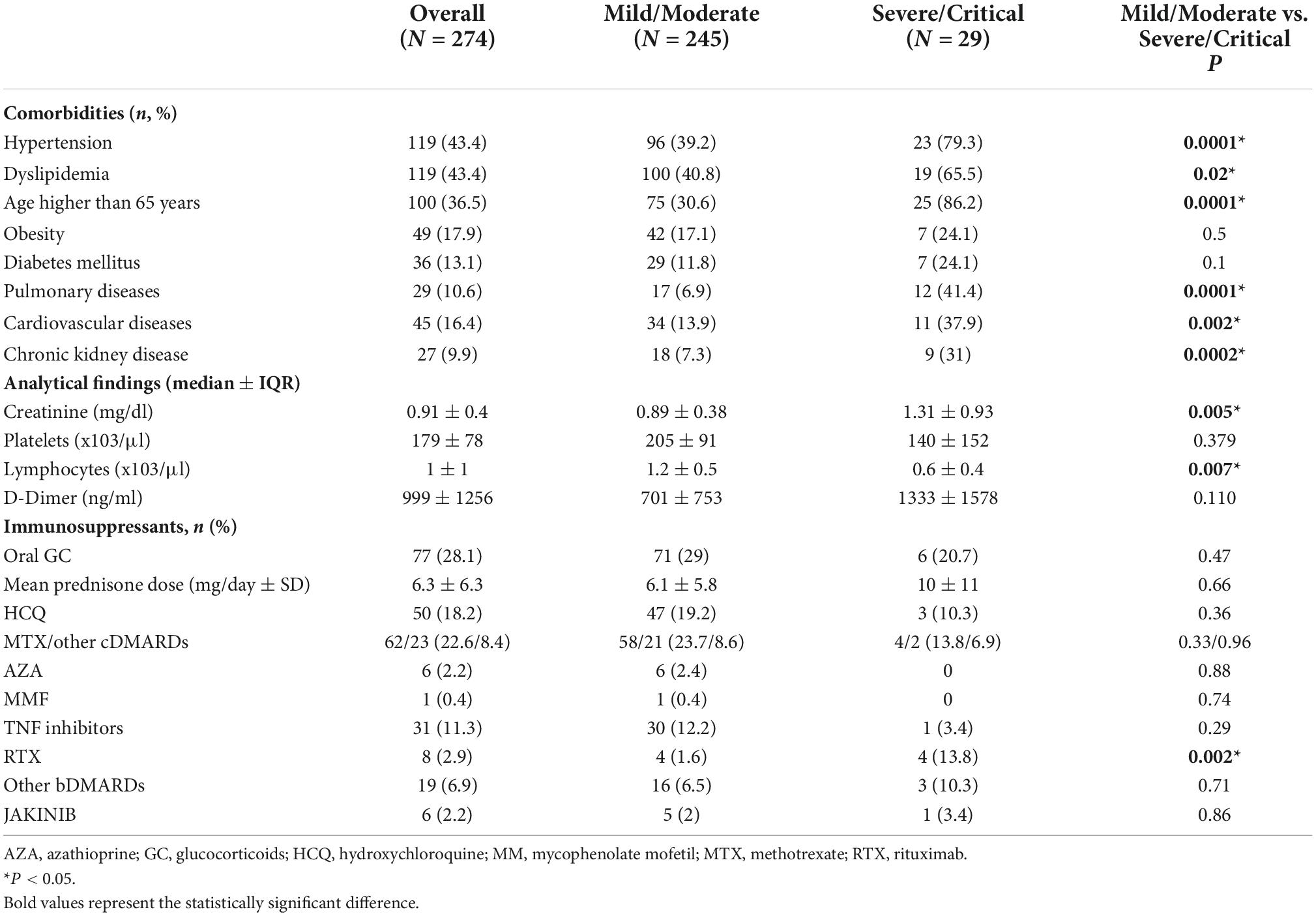
Table 5. Clinical severity of 274 with rheumatic immune-mediated diseases (R-IMID) diagnosed with coronavirus disease 2019 (COVID-19) [analytical findings and Immunosuppressants are at coronavirus (COVID) diagnosis].
These severity factors are also analyzed in Figure 1, in which the odds ratio for each factor has been calculated. Although the confidence intervals are wide due to the small sample, the largest OR were found in: treatment with anti-CD20 agents [OR = 7.8 (1.73–35.2)], the presence of hypertension [OR = 6.7 (2.2–20.5)] and previous cancer history [OR = 5.93 (2–17.3)].
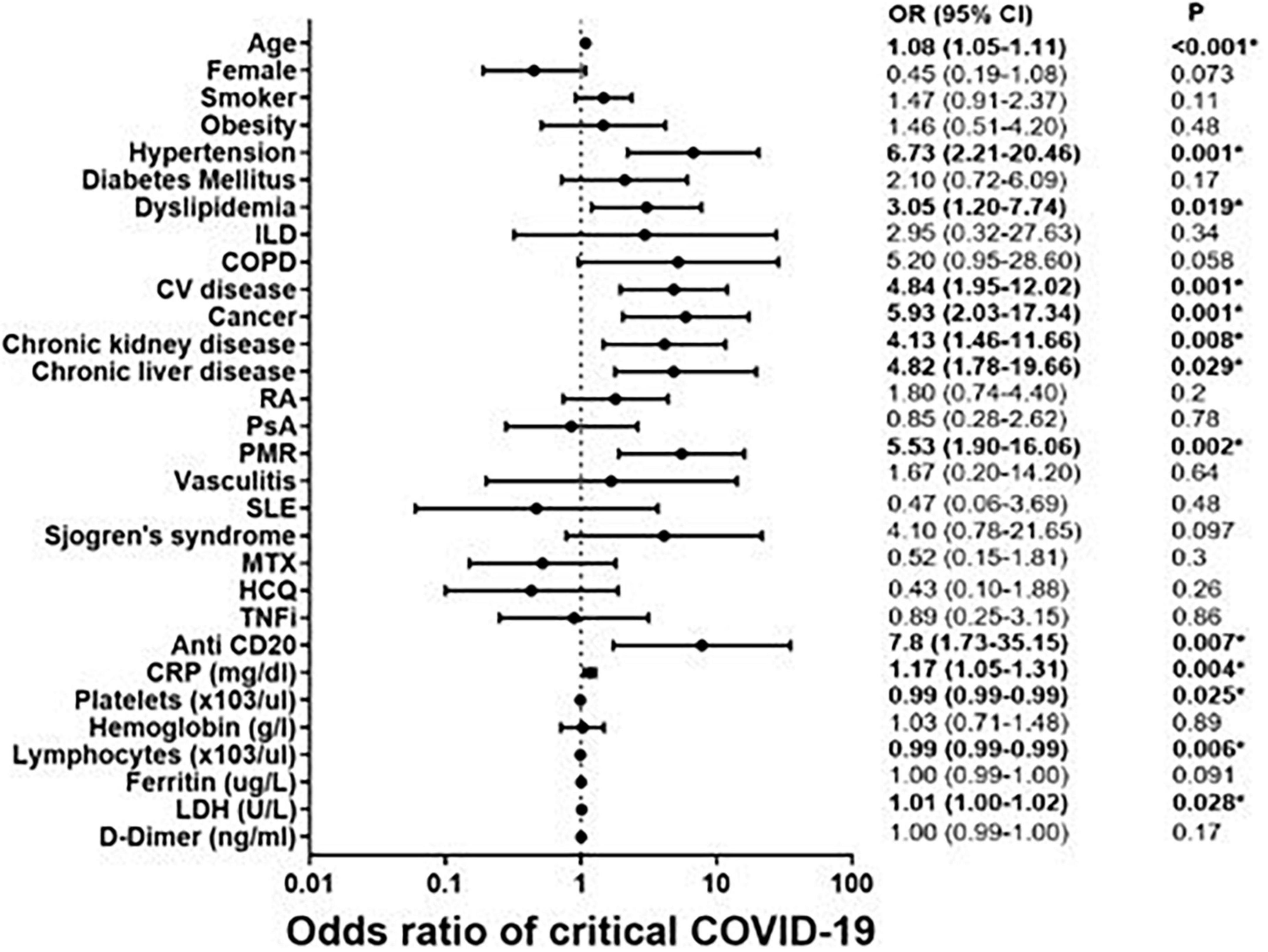
Figure 1. Predictive severity coronavirus disease 2019 (COVID-19) factors in 274 patients with rheumatic immune-mediated diseases (R-IMID).
In the search for literature review we only obtained 3 case-control studies that met both the inclusion, shown in Table 6. The details of these studies are shown in discussion.
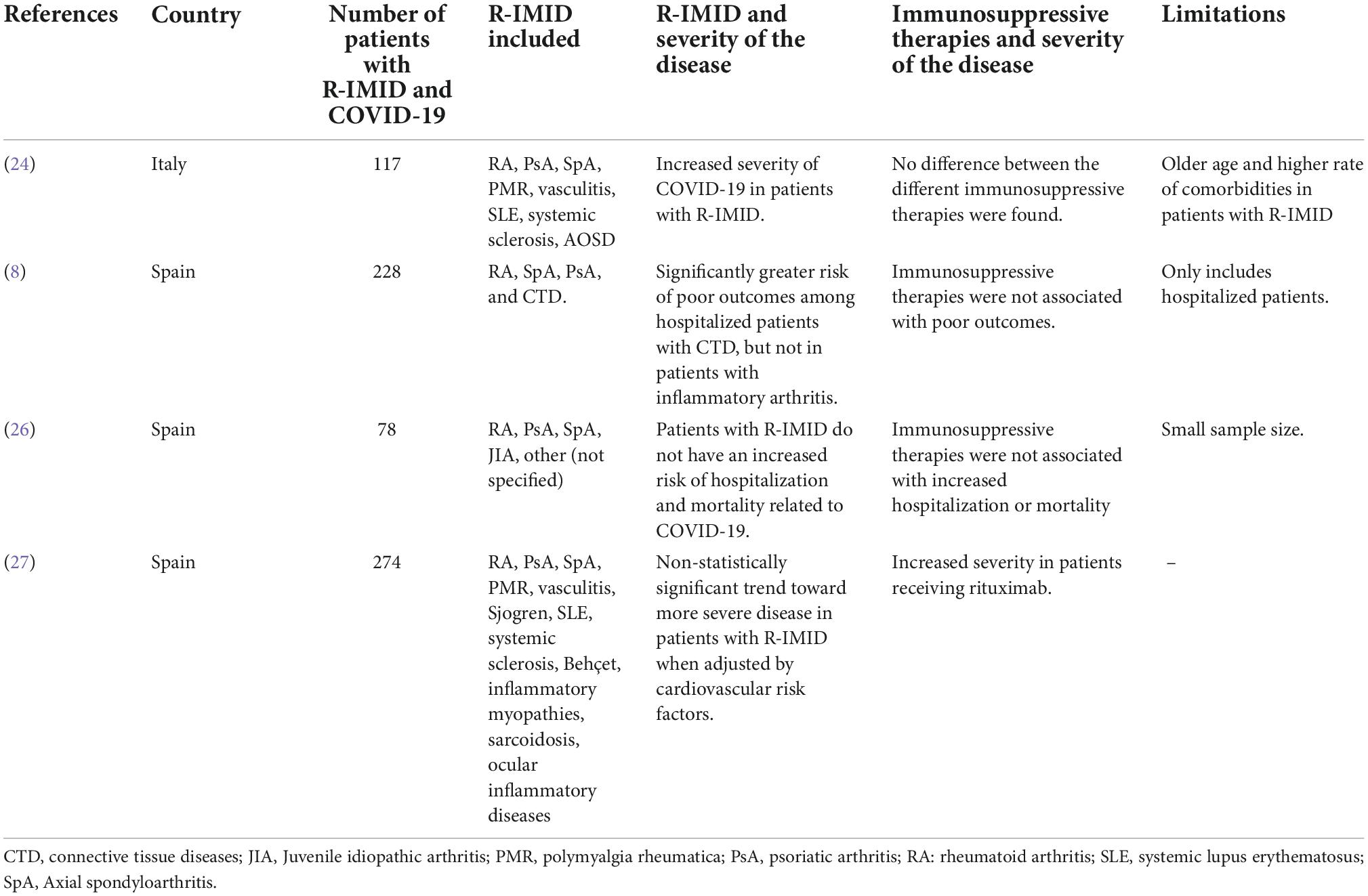
Table 6. Literature review of previous case-control studies in patients with rheumatic immune-mediated diseases (R-IMID) and coronavirus disease 2019 (COVID-19).
Although many studies with patients with R-IMID and COVID-19 have been published, most of these studies were only case series and did not establish a comparison with the general population. We report the largest case-control study including 274 patients with R-IMID with COVID-19 infection. These data were compared with 274 controls matched by age and sex, with no diagnosis of R-IMID.
When analyzing these results and comparing patients with R-IMID to the patients in the control group, we found that there is greater severity in patients with R-IMID with COVID-19 according to the NIH scale of severity. However, when we adjust these results according to comorbidities, there are no significant differences, leaving only a slight trend toward greater severity. Therefore, greater severity of COVID-19 in our group of patients with R-IMID was probably due to the high number of comorbidities, and not an increased risk due to the disease itself. Regardless, it must also be taken into account that these comorbidities are more frequent in patients with some of these R-IMID. This has been clearly established, for example, in rheumatoid arthritis (24). RTX was identified as the only immunosuppressive therapy related to an increased severity of COVID-19 infection.
To our knowledge, only three previous case-control studies have been published (Table 6). The first case-control study involving patients with R-IMID and COVID-19 was published by Fredi et al. (1, 25). This study included 117 patients and 117 matched controls. This study concludes that there was an increased severity of COVID-19 in patients with R-IMID. However, patients with R-IMID were significantly older and with more comorbidities when compared to controls (25).
The second case-control study was performed by Pablos et al. (8). This multicenter study included only hospitalized patients. This study also concluded that there was an increased risk of poor outcomes in patients with connective tissue diseases. However, these poor outcomes were not observed in patients with inflammatory arthritis.
In contrast with the two previous studies, the study published by Mena et al. (26), found no increased severity (measured by risk of hospitalization and death) in patients with R-IMID. This study has a smaller sample size when compared to the previous (n = 78).
Our study includes the largest sample size when compared to the previous case-control studies published. In the previous studies, with the exception of Mena’s study (26), the higher prevalence of comorbidities and older age in patients with R-IMID might influence the results. In order to avoid potential confusion factors, we adjusted our results by age, sex, and comorbidities. Furthermore, in our study the severity was measured in a standardized and internationally accepted scale (NIH severity classification). The previous studies have used various methods to measure severity (necessity of hospitalization, mechanical ventilation, mortality…). However, measuring the outcomes makes it difficult to compare different studies and increases the variability of the results between centers.
In addition, we assessed for the first time the possible differences in the clinical presentation and laboratory parameters between R-IMID patients and controls. Our study shows that the clinical presentation in patients with R-IMID and the general population is very similar. With the exception of diarrhea and odynophagia which were more frequent in the controls, and dyspnea and cough, that were more frequent in the patients with R-IMID. Hemoglobin values were significantly lower in the R-IMID group. No other significant differences were found in laboratory parameters between the two groups.
Regarding the use of immunosuppressive therapy, none of the previous studies found correlation between any therapy and worse outcomes.
However, our study shows an increased severity of the disease in patients receiving rituximab, in line with the previous evidence obtained from other studies. (9, 16, 17).
Regarding treatments received for COVID-19, both groups received similar treatments, as shown in Table 3. However, treatment was constantly changing as scientific knowledge on COVID-19 evolved, so it’s difficult to assess the impact of these treatments in outcomes of our patients. In any case, most patients had mild disease and did not require any treatment.
Regardless, our study had some limitations and results must be carefully interpreted.
First, we would like to highlight that this study has some limitations due to its retrospective nature.
A second limitation, is that these cases were collected over a long period of time. During this time period, there was a rapid development of scientific knowledge around COVID-19. This translated into changes in treatment and better outcomes in these patients as time passed.
The last limitation is due to the heterogeneity of the diseases included. This limits the extrapolation of results to patients with a specific diagnosis.
In conclusion, patients with R-IMID have a very similar clinical presentation when compared to the general population. Although there is a trend to an increased severity of the disease in patients with R-IMID, this trend did not reach statistical significance. Although our study shows some advantages over the previous ones, there are also some limitations due to its retrospective nature. Therefore, more research is needed to characterize the clinical features, risk factors and severity of COVID-19 infection in R-IMID infection.
Patients were first involved in this research at the start of the COVID-19 pandemic. Many patients consulted us with doubts about the new virus, how their disease could affect their prognosis, and if they were at a greater risk of presenting a worse outcome due to the medications they needed to treat their rheumatological disease. By then, no answers could be provided due to the lack of evidence. Therefore, we decided to launch this project to help the scientific community provide these answers. Therefore, for the design of this study we first took into account the concerns of our patients, paying special attention to the mortality caused by the disease. We have contact with various patient’s associations that will help us disseminate the results of this research. Also, some preliminary results have been announced in local newspapers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study protocol was approved by the Clinical Research Ethics Committee of the Hospital Marqués de Valdecilla (Santander, Spain) (Protocol number: 2020.151). Written informed consent from the patients/participants or patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
DM-L collected patient data by reviewed medical records, statistical analysis, and drafted the manuscript including tables and figures. IF-A performed advanced statistical analysis, elaboration of tables and figures, and reviewed the manuscript. DP-P prepared the patient database and reviewed the article. LS-B, AH-M, CÁ-R, FB-V, CC-S, and MT-V collected patient data by reviewed medical records. MG-G reviewed the article and elaborated the cover letter. RB provided the original idea, reviewed the article, and elaborated tables and figures. All authors contributed to the article and approved the submitted version.
We thank all the staff, physicians, nurses, and assistants of Rheumatology Unit of University Hospital Marqués de Valdecilla for their interest and collaboration during all these years.
Disclosures that might be interpreted as constituting of possible conflict(s) of interest for the study: IF-A received grants/research supports from AbbVie, MSD, Janssen, and Roche and received consultation fees from company-sponsored speaker’s bureau associated with AbbVie, Pfizer, Roche, Sanofi, Sobi, Amgen, Celgene, and MSD and received support for attending meetings and/or travel from AbbVie, Pfizer, Roche, Sanofi, Sobi, Amgen, Celgene, and MSD. DP-P received research support from UCB Pharma, Roche, AbbVie, and Lilly outside the submitted work. MG-G had received grants/research supports from AbbVie, MSD, Janssen, and Roche and had consultation fees/participation in company-sponsored speaker’s bureau from AbbVie, Pfizer, Roche, Sanofi, Lilly, Celgene, and MSD and received support for attending meetings and/or travel from AbbVie, Pfizer, Roche, Sanofi, Lilly, Celgene, and MSD. RB received grants/research supports from AbbVie, MSD, and Roche, and had consultation fees/participation in company-sponsored speaker’s bureau from AbbVie, Pfizer, Roche, Bristol-Myers, Lilly, Janssen, and MSD and received support for attending meetings and/or travel from AbbVie, Pfizer, Roche, Bristol-Myers, Lilly, Janssen, and MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AZA, Azathioprine; COVID-19, coronavirus disease 2019; CRP, C-reactive protein; CTD, connective tissue diseases; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; GC, glucocorticoids; DMARD, disease-modifying antirheumatic drugs; cDMARD, conventional disease-modifying antirheumatic drugs; HCQ, hydroxychloroquine; ILD, interstitial lung disease; IQR, interquartile range; JIA, juvenile idiopathic arthritis; LDH, lactate dehydrogenase; MMF, mycophenolate mofetil; MTX, methotrexate; NIH, National Institute of Health; PCR, polymerase chain reaction; PMR, polymyalgia rheumatic; PsA, psoriatic arthritis; RA, rheumatoid arthritis; RTX, rituximab; R-IMID, rheumatic immune-mediated diseases; SLE, systemic lupus erythematosus; SpA, axial spondyloarthritis; TNF, tumor necrosis factor; TNFi, tumor necrosis factor inhibitors; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SD, standard deviation; WHO, World Health Organization.
1. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
2. World Health Organization [WHO]. WHO coronavirus (COVID19) dashboard. (2021). Available online at: https://covid19.who.int/ (accessed September 1, 2021).
3. Wang L, He W, Yu X, Hu D, Bao M, Liu H, et al. Coronavirus disease 2019 in elderly patients: characteristics and prognostic factors based on 4week followup. J Infect. (2020) 80:639–45. doi: 10.1016/j.jinf.2020.03.019
4. Vince A, Dusek D. [Immunosupression and viral infections in rheumatic diseases]. Reumatizam. (2007) 54:5862.
5. Youssef J, Novosad S, Winthrop K. Infection risk and safety of corticosteroid use. Rheum Dis Clin North Am. (2016) 42:157176. doi: 10.1016/j.rdc.2015.08.004
6. Bryant P, Baddley J. Opportunistic infections in biological therapy, risk and prevention. Rheum Dis Clin North Am. (2017) 43:2741. doi: 10.1016/j.rdc.2016.09.005
7. BritoZerón P, SisóAlmirall A, FloresChavez A, Retamozo S, RamosCasals M. SARSCoV2 infection in patients with systemic autoimmune diseases. Clin Exp Rheumatol. (2021) 39:676687. doi: 10.55563/clinexprheumatol/lekp1y
8. Pablos J, Galindo M, Carmona L, Lledó A, Retuerto M, Blanco R, et al. Clinical outcomes of hospitalised patients with COVID19 and chronic inflammatory and autoimmune rheumatic diseases: a multicentric matched cohort study. Ann Rheum Dis. (2020) 79:15441549. doi: 10.1136/annrheumdis2020218296
9. BachillerCorral J, Boteanu A, GarciaVillanueva M, de la Puente C, Revenga M, DiazMiguel M, et al. Risk of severe COVID19 infection in patients with inflammatory rheumatic diseases. J Rheumatol. (2021) 15:jrheum.200755. doi: 10.3899/jrheum.200755
10. Sharmeen S, Elghawy A, Zarlasht F, Yao Q. COVID19 in rheumatic disease patients on immunosuppressive agents. Semin Arthritis Rheum. (2020) 50:680686. doi: 10.1016/j.semarthrit.2020.05.010
11. Haberman R, Axelrad J, Chen A, Castillo R, Yan D, Izmirly P, et al. Covid19 in immunemediated inflammatory diseases—case series from New York. N Engl J Med. (2020) 383:85–8. doi: 10.1056/NEJMc2009567
12. Costantino F, Bahier L, Tarancón L, Leboime A, Vidal F, Bessalah L, et al. COVID19 in French patients with chronic inflammatory rheumatic diseases: clinical features, risk factors and treatment adherence. Joint Bone Spine. (2021) 88:105095. doi: 10.1016/j.jbspin.2020.105095
13. So H, Mak J, So J, Lui G, Lun F, Lee J, et al. Incidence and clinical course of COVID19 in patients with rheumatologic diseases: a populationbased study. Semin Arthritis Rheum. (2020) 50:885889. doi: 10.1016/j.semarthrit.2020.07.012
14. Nuño L, Novella Navarro M, Bonilla G, FrancoGómez K, Aguado P, Peiteado D, et al. Clinical course, severity and mortality in a cohort of patients with COVID19 with rheumatic diseases. Ann Rheum Dis. (2020) 79:16591661. doi: 10.1136/annrheumdis2020218054
15. Xu C, Yi Z, Cai R, Chen R, Thong B, Mu R. Clinical outcomes of COVID19 in patients with rheumatic diseases: a systematic review and metaanalysis of global data. Autoimmun Rev. (2021) 20:102778. doi: 10.1016/j.autrev.2021.102778
16. Jones J, Faruqi A, Sullivan J, Calabrese C, Calabrese L. COVID19 outcomes in patients undergoing B cell depletion therapy and those with humoral immunodeficiency states: a scoping review. Pathog Immun. (2021) 6:76103. doi: 10.20411/pai.v6i1.435
17. LoarceMartos J, GarcíaFernández A, LópezGutiérrez F, GarcíaGarcía V, CalvoSanz L, Del BosqueGranero I, et al. High rates of severe disease and death due to SARSCoV2 infection in rheumatic disease patients treated with rituximab: a descriptive study. Rheumatol Int. (2020) 40:20152021. doi: 10.1007/s0029602004699x
18. Montero F, MartínezBarrio J, SerranoBenavente B, González T, Rivera J, Molina Collada J, et al. Coronavirus disease 2019 (COVID19) in autoimmune and inflammatory conditions: clinical characteristics of poor outcomes. Rheumatol Int. (2020) 40:15931598. doi: 10.1007/s00296020046764
19. Gianfrancesco M, Hyrich K, AlAdely S, Carmona L, Danila M, Gossec L, et al. Characteristics associated with hospitalization for COVID19 in people with rheumatic disease: data from the COVID19 global rheumatology alliance physicianreported registry. Ann Rheum Dis. (2020) 79:859–66. doi: 10.1136/annrheumdis2020217871
20. Hyrich K, Machado P. Rheumatic disease and COVID19: epidemiology and outcomes. Nat Rev Rheumatol. (2021) 17:7172. doi: 10.1038/s41584020005622
21. Grainger R, Machado P, Robinson P. Novel coronavirus disease2019 (COVID19) in people with rheumatic disease: epidemiology and outcomes. Best Pract Res Clin Rheumatol. (2021) 35:101657. doi: 10.1016/j.berh.2020.101657
22. Gao Y, Ding M, Dong X, Zhang J, Kursat Azkur A, Azkur D, et al. Risk factors for severe and critically ill COVID19 patients: a review. Allergy. (2021) 76:428455. doi: 10.1111/all.14657
23. COVID19 Treatment Guidelines Panel. Coronavirus disease 2019 (COVID19) treatment guidelines. National Institutes of Health (2019). Available online at: https://www.covid19treatmentguidelines.nih.gov (accessed June 18, 2021).
24. Dougados M, Soubrier M, Antunez A, Balint P, Balsa A, Buch M, et al. Prevalence of comorbidities in rheumatoid arthritis and evaluation of their monitoring: results of an international, crosssectional study (COMORA). Ann Rheumat Dis. (2014) 73:6268. doi: 10.1136/annrheumdis-2013-204223
25. Fredi M, Cavazzana I, Moschetti L, Andreoli L, Franceschini F, Brescia Rheumatology COVID19 Study Group. COVID19 in patients with rheumatic diseases in northern Italy: a singlecentre observational and casecontrol study. Lancet Rheumatol. (2020) 2:e549e556. doi: 10.1016/S26659913301697
26. MenaVázquez N, Manrique AS, RojasGiménez M, RayaÁlvarez E, VellosoFeijoó M, LópezMedina C, et al. Hospitalization and mortality from COVID19 of patients with rheumatic inflammatory diseases in Andalusia. Reumatol Clin. (2021). [Epub ahead of print].
Keywords: COVID-19, autoimmune diseases, antirheumatic agents, rituximab, biologic agents
Citation: Martínez-López D, Ferraz-Amaro I, Prieto-Peña D, Sánchez-Bilbao L, Herrero-Morant A, Álvarez-Reguera C, Benavides-Villanueva F, Corrales-Selaya C, Trigueros-Vázquez M, González-Gay MÁ and Blanco R (2022) Coronavirus disease 2019 in patients with rheumatic immune-mediated diseases in a single University Hospital, matched case-control study and literature review. Front. Med. 9:1056374. doi: 10.3389/fmed.2022.1056374
Received: 28 September 2022; Accepted: 23 November 2022;
Published: 12 December 2022.
Edited by:
Coziana Ciurtin, University College London, United KingdomReviewed by:
Ivan Castellví, Hospital Universitari de la Santa Creu i Sant Pau, SpainCopyright © 2022 Martínez-López, Ferraz-Amaro, Prieto-Peña, Sánchez-Bilbao, Herrero-Morant, Álvarez-Reguera, Benavides-Villanueva, Corrales-Selaya, Trigueros-Vázquez, González-Gay and Blanco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardo Blanco, cmJsYW5jb3ZlbGFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.