 Mai Sasaki Aanensen Fraz1,2,3*
Mai Sasaki Aanensen Fraz1,2,3* Gry Dahle4
Gry Dahle4 Kirsten Margrete Skaug1
Kirsten Margrete Skaug1 Sophie Jarraud5
Sophie Jarraud5 Stephan Frye1Jørgen Vildershøj Bjørnholt1,6
Stephan Frye1Jørgen Vildershøj Bjørnholt1,6 Ingvild Nordøy7,8
Ingvild Nordøy7,8- 1Department of Microbiology, Oslo University Hospital, Oslo, Norway
- 2Centre for Rare Disorders, Oslo University Hospital, Oslo, Norway
- 3Department of Medicine, Lovisenberg Diaconal Hospital, Oslo, Norway
- 4Department of Cardiothoracic Surgery, Oslo University Hospital, Oslo, Norway
- 5National Reference Centre for Legionella, Institute of Infectious Agents, Hospices Civils de Lyon, Lyon, France
- 6Faculty of Medicine, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 7Section for Clinical Immunology and Infectious Diseases, Oslo University Hospital, Oslo, Norway
- 8Research Institute of Internal Medicine, Oslo University Hospital, Oslo, Norway
Extrapulmonary infections with Legionella species are rare, but important to acknowledge. We report a case of infective endocarditis (IE) with Legionella bozemanae in a 66-year-old immunocompetent man with an aortic homograft. The diagnosis was made by direct 16S rRNA gene amplification from valve material, confirmed by a targeted Legionella-PCR in serum and the detection of L. bozemanae specific antibodies. To our knowledge, this is the first confirmed case of IE with L. bozemanae as causative pathogen. The infected aortic prosthesis was replaced by a homograft, and the patient was successfully treated with levofloxacin and azithromycin for 6 weeks.
Introduction
The Legionellaceae are widespread in water and soil environment, and can colonize manmade water sources. This is also true for Legionella bozemanae, which has also been found in commercial potting soils (1–4). L. bozemanae is uncommonly a pathogen, but it has been reported to be able to cause severe and necrotizing pneumonia in immunocompromised patients (5, 6). Extrapulmonary infections with L. bozemanae are even rarer, however cases of arthritis and soft tissue infections are described (7–9). There are 18 previous reports of infective endocarditis (IE) caused by Legionella species in the English literature, and in only two of these, the affected valve was native (10–20). The presentation of Legionella endocarditis tends to be subacute, with weight loss, low-grade fever and anemia, and without peripheral manifestations as embolic events or immune complex depositions (21). Exceptions from this are two reports of bacterial seeding to the central nervous system and one case of digital microembolisms (15, 19, 20). In the previous reports of Legionella endocarditis, the majority of IE patients had no preceding or concurrent airway infection, with only four of 18 cases reporting clinical or radiological findings consistent with pneumonia. In one case series, the Legionella endocarditis cases were believed to be part of hospital outbreaks of Legionella (10). Another feature of the reported Legionella IEs in the literature is that although small valvular vegetations are often visible at surgery, they are frequently undetectable by echocardiograms (10, 17). Accordingly, as the patients also often display only moderate signs of inflammation, the diagnosis of IE can be delayed.
Case description
A 66-year-old immunocompetent man with an increasingly symptomatic aortic stenosis and bicuspid aortic valve underwent aortic valve replacement in April 2021 at Oslo University Hospital, Rikshospitalet. He was otherwise healthy, besides an occasional migraine. The inserted prosthetic aortic valve was a biological 23 mm Perimount prosthesis (Edwards Lifesciences, Irvine, CA, United States), and an aorta Intergard woven graft 30 mm (Getinge, Göteborg, Sweden) was also inserted (Day 0). The surgical procedure was uneventful, and per operative echocardiogram and postoperative chest x-ray were normal. The further disease course, diagnostics and treatment in this case is illustrated in the timeline of Figure 1.
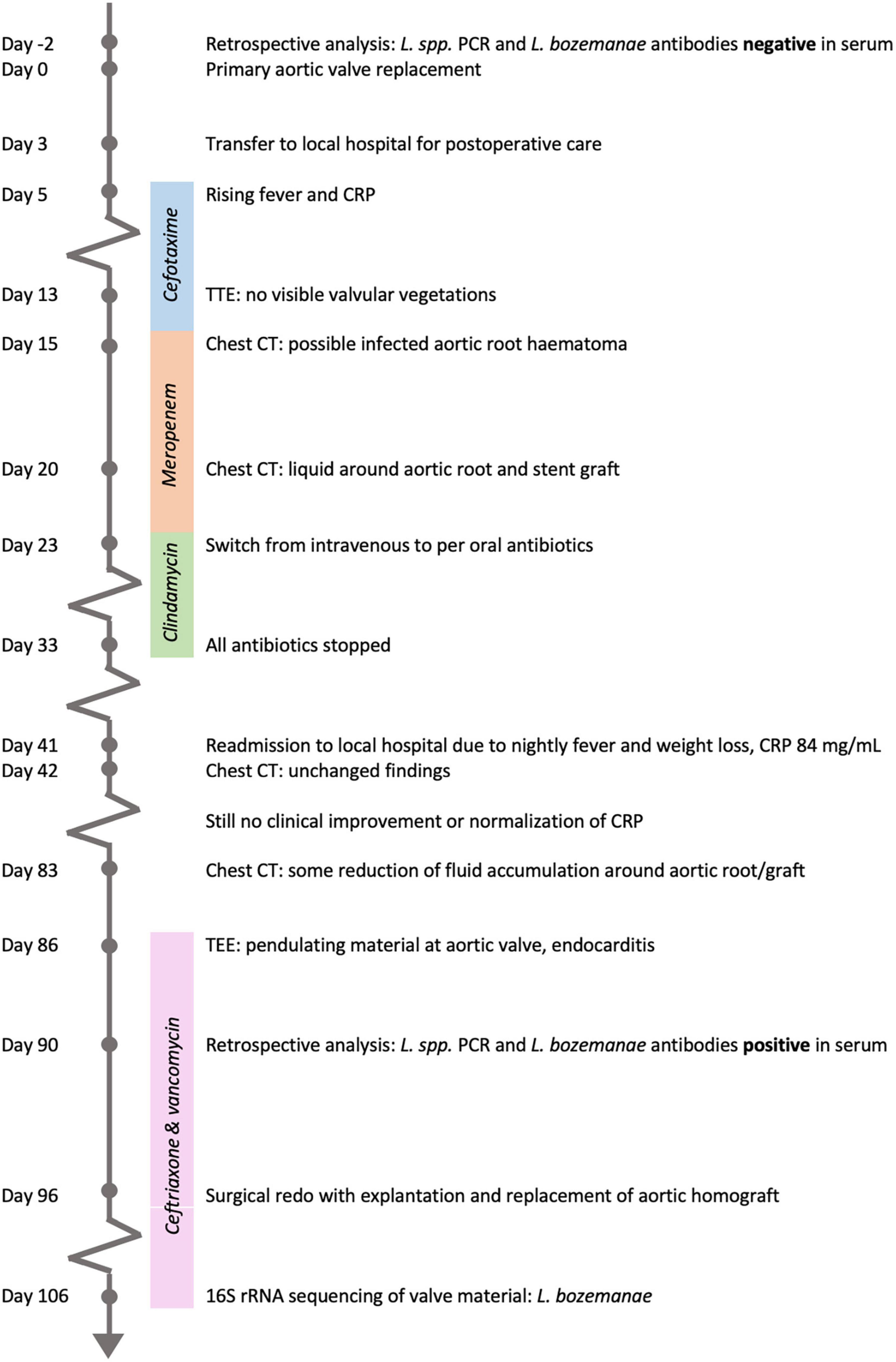
Figure 1. Timeline from admission for the primary aortic valve replacement until microbial diagnosis by 16S rRNA sequencing of valve material.
The patient was transferred to his local hospital for postoperative care on Day 3 after surgery. Physical examination at the day of transfer revealed no heart murmur or pulmonary crepitations. During the first postoperative week he developed fever and CRP increased to a maximum of 329 mg/L on Day 8. Antibiotic treatment with cefotaxime was started. There were no visible valvular vegetations by transthoracic echocardiogram on Day 14. As his condition failed to improve, a chest CT was performed on Day 15 displaying a possible infected aortic root hematoma. CT also demonstrated pleural- and pericardial fluid, but no lung parenchymal infiltrations. In this period, the patient complained of a non-productive troublesome cough. CRP levels did not fall significantly, and the antibiotic treatment was switched to meropenem. Pleural fluid was drained. Subsequently, CRP decreased to 34 mg/L and the patient’s condition somewhat improved. The patient was discharged to his home with a 10 days course of oral clindamycin.
However, he continued to have nightly fever and weight loss after the discharge. He also had a short self-limiting episode of pain, rubor and swelling in his left knee. On Day 41 he was readmitted to his local hospital with increasing fever, and CRP had increased to 84 mg/L. There were normal findings by physical examination of his knee joint. Chest CT was repeated on Day 42 with unchanged findings around the aortic root, and still no lung parenchymal infiltrations. The patient was observed without starting any antibiotic treatment, with the aim of catching a pathogen by repeated blood culturing. He stayed afebrile the following 2 days, and was again discharged without any blood culture findings. However, the patient did not improve clinically, and CRP was continuously moderately elevated. Therefore, chest CT was again repeated on Day 83, this time revealing some reduction of fluid accumulation around the aortic root and ascendens graft. Finally, transesophageal echocardiogram was performed Day 86, showing pendulating material at the ventricular side of the aortic valve cusps, consistent with endocarditis (Figure 2). The patient had at this time developed a second degree atrioventricular block, and a temporary pacemaker was inserted.
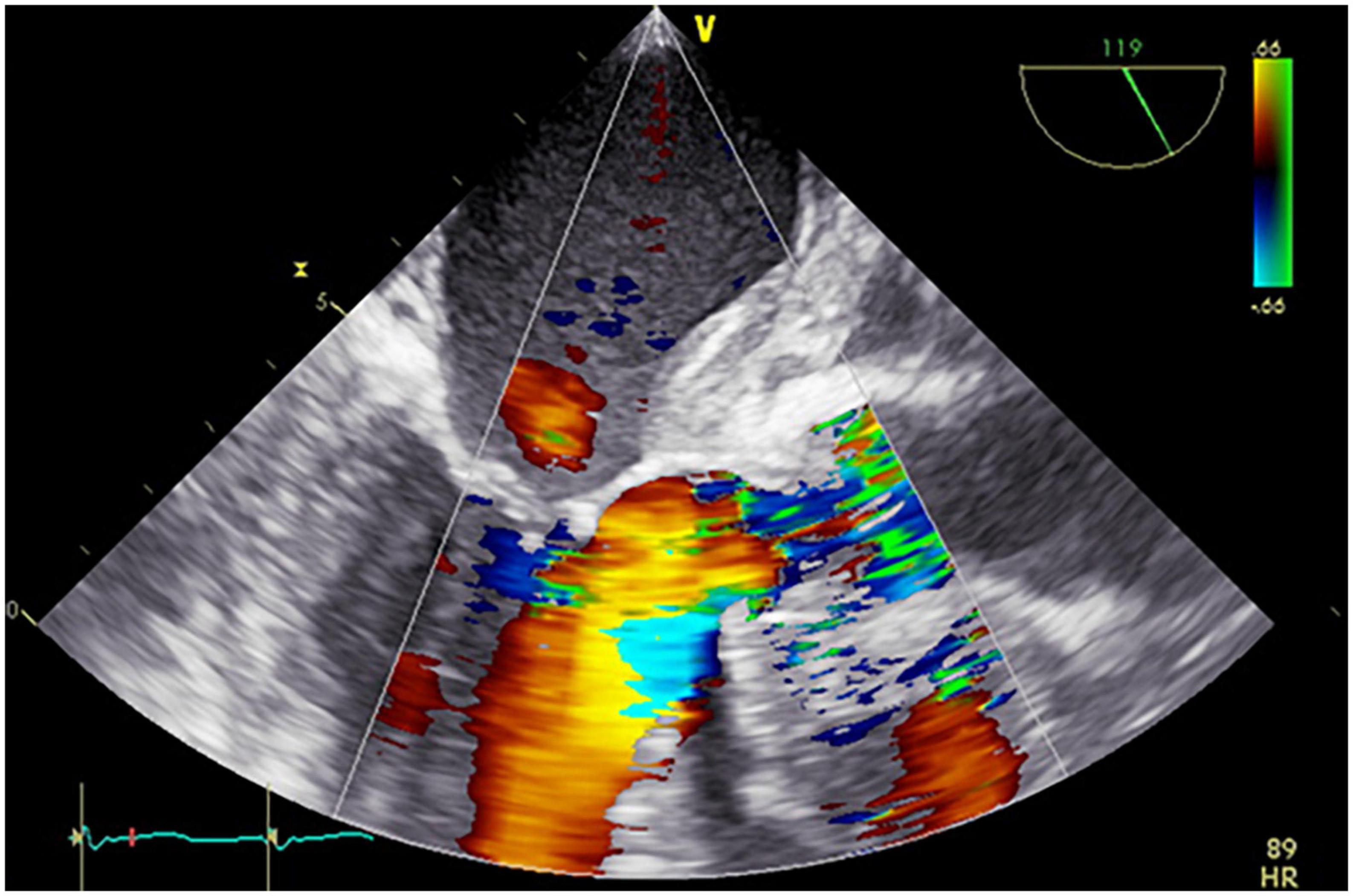
Figure 2. Pre-operative transesophageal echocardiogram. Severe aortic regurgitation and thickened aortic wall.
As blood cultures remained negative, the patient was treated empirically with ceftriaxone and vancomycin from Day 86. The patient’s condition deteriorated despite this treatment, and he was decided to undergo redo surgery. The Perimount prosthesis and the ascendens graft were excised and replaced by a Homograft 22 mm (Cell and Tissue laboratory, Sahlgrenska, Sweden) on Day 96. Microscopy of acridin stained excised valve material demonstrated scarcely distributed rods (Figure 3), but culture of the explant on standard bacterial and fungal media did not yield growth. However, direct 16S rRNA gene amplification of valve material yielded sequences of 720 base pairs matching 100% with L. bozemanae in the National Center for Biotechnology Information (NCBI) Blast database and EzBioCloud (22). The valve tissue DNA extraction and 16S rRNA gene amplification were performed twice with same result. Seeding of the explanted valve material was also done on buffered charcoal-yeast extract (BCYE) media for Legionella, but we were not able to grow L. bozemanae. The patient was finally treated with levofloxacin and azithromycin for 6 weeks. The atrioventricular block progressed to a total block after the redo, and a permanent pacemaker was implanted after 4 weeks. Transthoracal echocardiogram was performed by the end of the antibiotic treatment, displaying an aortic graft in satisfactory position, without leakage. Post treatment CT arteriography showed significant decline of fluid around the aortic root. The patient is now physically fit and is doing well, a year after completed therapy.
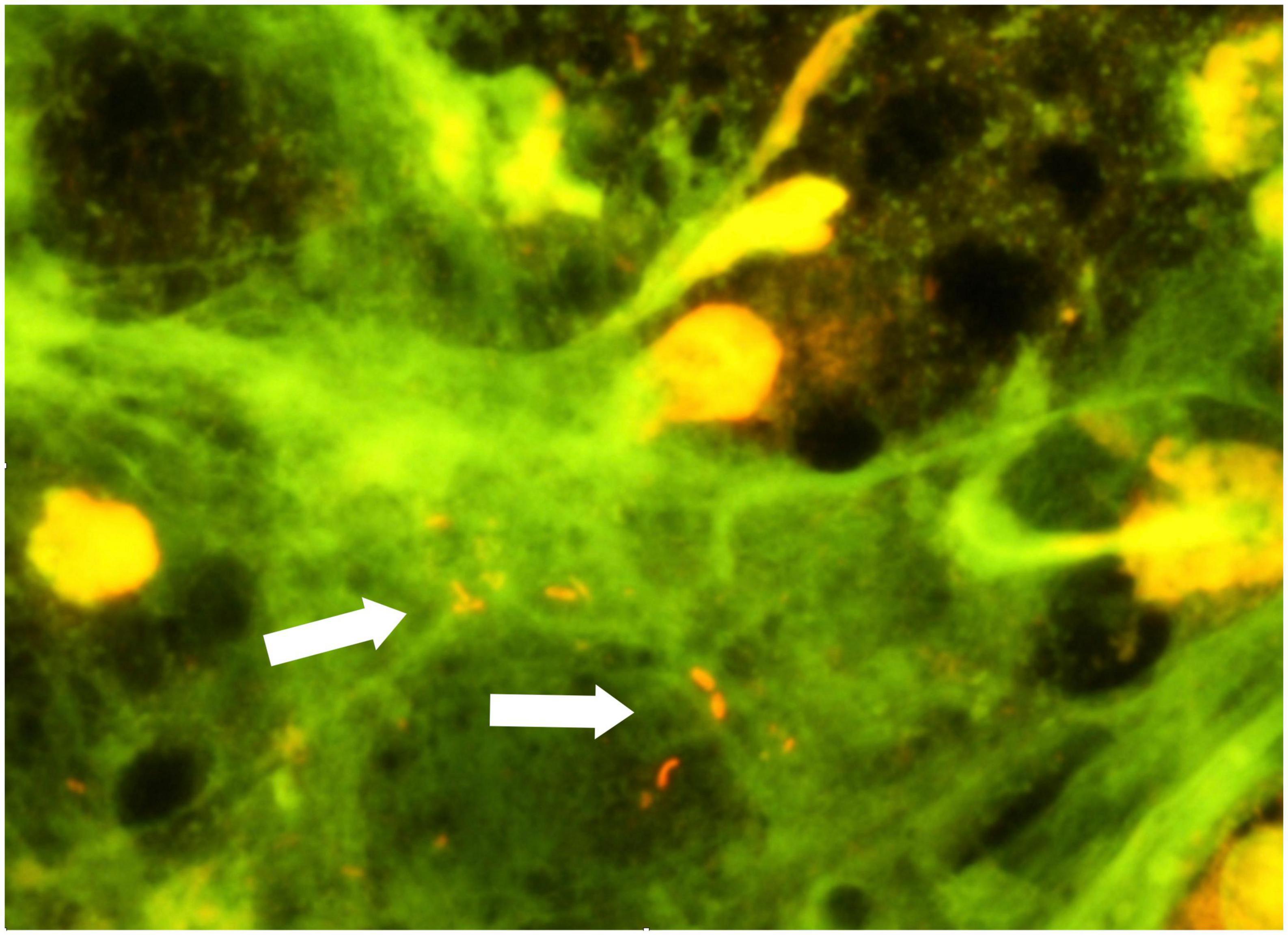
Figure 3. Excised valve material, acridin stain. Rods marked by white arrows.
An environmental search was performed to detect Legionella spp. in water sources at the local hospital, at the university hospital where the surgery was performed and at the patient’s home. L. bozemanae was not detected in any of these locations.
The diagnosis of L. bozemanae was confirmed retrospectively by a hybridization probe-based dual-color LightCycler real-time PCR with primers that amplify a 378-bp product within the 16S rRNA gene of Legionella spp. of the patient’s serum (23). The serum was sampled and stored frozen from 6 days (Day 90) before the reoperation. Subsequent melting point analysis corresponded with L. bozemanae. Additionally, an assay to detect L. bozemanae specific antibodies was performed by the French National Reference Center for Legionella (Lyon, France). Serum from 2 days before the primary operation (Day-2), was negative (<1:16) for L. bozemanae antibodies, while in serum from Day 90 the titer was positive (>1:2048).
Finally, although the diagnosis was certain, we performed 16S Nanopore sequencing on both cardiac valve material and serum from Day 90 to see if this method would detect L. bozemanae. DNA was extracted by SelectNAplus from Molzym (Bremen, Germany) and prepared for Nanopore sequencing using a 16S Barcoding Kit (SQK-RAB204, Oxford Nanopore Technologies, Oxford, UK). Sequencing was performed on a MinION flowcell (FLO-MIN106D, Oxford Nanopore Technologies, Oxford, UK) for 43 h. Sequences were filtered by size and quality using ProwlerTrimmer and blasted against the NCBI 16S rRNA refseq database, which was complemented with a full-length sequence of the 16S rRNA gene of L. bozemanae, extracted from the whole genome assembly GCF_900640135.1. While the serum sample from Day 90 yielded 36,673 reads before filtering and 10,678 after, the valve sample only gave 153 reads with 90 reads left after filtering. No Legionella specific sequences were found in the serum-derived reads. On the other hand, 89 of the 90 (98%) reads from the valve sample were identified as L. bozemanae specific.
Discussion
Infective endocarditis has a high mortality rate, and early identification of the causative microbe is important to target antibiotic therapy and improve outcome. Legionella spp. are not routinely recoverable from blood cultures and will not be covered by standard empiric antibiotic treatment for endocarditis. A subacute disease course without typical IE findings adds to making the diagnosis of this infection challenging. This case report has several take-away lessons: Most important, although Legionella spp. are infrequent causes of infectious endocarditis in general, they should be considered in culture negative cases of post-surgery prosthetic valve endocarditis (PVE) (24). This case also demonstrates that PVE caused by L. bozemanae is possible in an otherwise healthy and immunocompetent host.
Furthermore, this and most other similar cases show that the Legionella bacteria’s way of entrance to cause endocarditis often remains unknown. Although Legionella is often associated with airway infection, the literature shows that airway symptoms are often not present in Legionella PVE. Our patient experienced a protracted disease course after the primary surgery, with fluctuating fever and CRP. Repeated chest CT showed no pulmonary infiltrations, and Legionella was not detected by Legionella PCR in bronchial lavage fluid after the reoperation. The patient experienced some dry cough, but this could as well be attributed to pleural irritation by pleural fluid present. L. bozemanae was neither detected in the water systems of the operating hospital, the local hospital nor the patient’s house.
When it comes to treatment, there are no randomized trials involving legionellosis with non-pneumophila species. For long, antimicrobial susceptibility testing (AST) for Legionella has been challenging and not standardized, until the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Legionella Infections recently issued a recommendation (25). In this case, AST was impossible due to lack of a positive culture. The literature regarding antibiotic susceptibility for Legionella species other than pneumophila is scarce, but AST studies performed by broth microdilution and in a human monocyte cell line demonstrate higher activity of quinolones than erythromycin against L. bozemanae (26). However, fluoroqinolone resistance may be induced during antibiotic treatment (27). Based on this knowledge and the gravity of the infection in this case, our patient was given a combination of levofloxacin and azithromycin. However, long QT interval should always be considered and monitored when combining these drugs (28).
We identified the microbial cause of endocarditis by broad-range 16S rRNA gene amplification of the excised specimen. This is common practice in blood culture negative endocarditis (BCNE) when explanted valve material is available, and can identify a microbial cause in about two thirds of cases (29). In cases of IE where surgery has not been performed, a reliable molecular method to detect relevant microbial genetic material in blood, serum or plasma would be an ideal diagnostic tool. Unfortunately, as of today no such method has shown satisfactory performance. Metagenomic next-generation sequencing of plasma is suggested as a promising aid in systemic infections, although both false positive and false negative results, as well as the noise of polymicrobial identification can make interpretation of results challenging (30–32). Our 16S Nanopore sequencing of the patient’s serum were not able to detect any Legionella.
In this case, targeted Legionella PCR was positive in serum from 6 days before the redo. The European Society of Cardiology guidelines recommend the use of targeted PCR of EDTA-blood when IE with Bartonella spp., Tropheryma whipplei or fungi are suspected (33). The guidelines also recommend systematic serological testing for Legionella pneumophila in BCNE according to local epidemiology. However, most serological assays for Legionella only detect L. pneumophila, which leaves a diagnostic gap for other Legionella spp. that may be underdiagnosed. Serological assays for Legionella species other than pneumophila are not avaliable in Norway, and is in general not widely performed as there are no commercial tests. International laboratory collaboration partners or networks can be helpful in cases like ours. Targeted Legionella PCR is on the other hand more commonly performed, and is mostly used in airway specimens. The sensitivity of targeted Legionella PCR in sera of patients with Legionella pneumonia has previously been reported to be 30–63% depending on the target gene, and the specificity to be 100% (34–36).
In conclusion, Legionella endocarditis is difficult to diagnose due to both indistinct clinical findings and the fact that microbiological identification depends on the clinicians’ suspicion. Targeted Legionella PCR of serum should be considered in cases of culture negative PVE, and Legionella spp. as a cause of BCNE are likely underdiagnosed.
Data availability statement
The genomic sequences presented in this case report are included in the Supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MF collected the data and drafted the manuscript. KS, SF, SJ, and JB analyzed and interpreted the data. GD and IN provided clinical care for the patient. All authors reviewed, edited, and approved the final manuscript.
Acknowledgments
We acknowledge all healthcare and laboratory workers involved in the diagnosis and treatment of the patient. We especially thank Bente Cecilie Borgen and the other infection prevention workers who performed the environmental search.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1055465/full#supplementary-material
References
1. Casati S, Gioria-Martinoni A, Gaia V. Commercial potting soils as an alternative infection source of Legionella pneumophila and other Legionella species in Switzerland. Clin Microbiol Infect. (2009) 15:571–5. doi: 10.1111/j.1469-0691.2009.02742.x
2. Koide M, Arakaki N, Saito A. Distribution of Legionella longbeachae and other legionellae in Japanese potting soils. J Infect Chemother. (2001) 7:224–7. doi: 10.1007/s101560170017
3. Patterson WJ, Hay J, Seal DV, McLuckie JC. Colonization of transplant unit water supplies with Legionella and protozoa: precautions required to reduce the risk of legionellosis. J Hosp Infect. (1997) 37:7–17. doi: 10.1016/s0195-6701(97)90068-2
4. Lee HK, Shim JI, Kim HE, Yu JY, Kang YH. Distribution of Legionella species from environmental water sources of public facilities and genetic diversity of L. pneumophila serogroup 1 in South Korea. Appl Environ Microbiol. (2010) 76:6547–54. doi: 10.1128/AEM.00422-10
5. Harris A, Lally M, Albrecht M. Legionella bozemanii pneumonia in three patients with AIDS. Clin Infect Dis. (1998) 27:97–9. doi: 10.1086/514618
6. Miller ML, Hayden R, Gaur A. Legionella bozemanii pulmonary abscess in a pediatric allogeneic stem cell transplant recipient. Pediatr Infect Dis J. (2007) 26:760–2. doi: 10.1097/INF.0b013e318054e338
7. Just SA, Knudsen JB, Uldum SA, Holt HM. Detection of Legionella bozemanae, a new cause of septic arthritis, by PCR followed by specific culture. J Clin Microbiol. (2012) 50:4180–2. doi: 10.1128/JCM.01899-12
8. Ibranosyan M, Beraud L, Lemaire H, Ranc AG, Ginevra C, Jarraud S, et al. The clinical presentation of Legionella arthritis reveals the mode of infection and the bacterial species: case report and literature review. BMC Infect Dis. (2019) 19:864. doi: 10.1186/s12879-019-4488-z
9. Neiderud CJ, Vidh AL, Salaneck E. Soft tissue infection caused by Legionella bozemanii in a patient with ongoing immunosuppressive treatment. Infect Ecol Epidemiol. (2013) 3:10.3402/iee.v3i0.20739. doi: 10.3402/iee.v3i0.20739
10. Tompkins LS, Roessler BJ, Redd SC, Markowitz LE, Cohen ML. Legionella prosthetic-valve endocarditis. N Engl J Med. (1988) 318:530–5.
11. Park D, Pugliese A, Cunha BA. Legionella micdadei prosthetic valve endocarditis. Infection. (1994) 22:213–5.
12. Chen TT, Schapiro JM, Loutit J. Prosthetic valve endocarditis due to Legionella pneumophila. J Cardiovasc Surg. (1996) 37:631–3.
13. McCabe RE, Baldwin JC, McGregor CA, Miller DC, Vosti KL. Prosthetic valve endocarditis caused by Legionella pneumophila. Ann Intern Med. (1984) 100:525–7.
14. Patel MC, Levi MH, Mahadevi P, Nana M, Merav AD, Robbins N. L. micdadei PVE successfully treated with levofloxacin/valve replacement: case report and review of the literature. J Infect. (2005) 51:e265–8. doi: 10.1016/j.jinf.2005.03.011
15. Young JS, Farber BF, Pupovac SS, Graver LM. Prosthetic valve legionella endocarditis. Ann Thorac Surg. (2019) 108:e271–2.
16. Pearce MM, Theodoropoulos N, Mandel MJ, Brown E, Reed KD, Cianciotto NP. Legionella cardiaca sp. nov., isolated from a case of native valve endocarditis in a human heart. Int J Syst Evol Microbiol. (2012) 62(Pt. 12):2946–54. doi: 10.1099/ijs.0.039248-0
17. Leggieri N, Gouriet F, Thuny F, Habib G, Raoult D, Casalta JP. Legionella longbeachae and endocarditis. Emerg Infect Dis. (2012) 18:95–7.
18. Compain F, Bruneval P, Jarraud S, Perrot S, Aubert S, Napoly V, et al. Chronic endocarditis due to Legionella anisa: a first case difficult to diagnose. New Microbes New Infect. (2015) 8:113–5. doi: 10.1016/j.nmni.2015.10.003
19. Fukuta Y, Yildiz-Aktas IZ, William Pasculle A, Veldkamp PJ. Legionella micdadei prosthetic valve endocarditis complicated by brain abscess: case report and review of the literature. Scand J Infect Dis. (2012) 44:414–8. doi: 10.3109/00365548.2011.645506
20. Massey R, Kumar P, Pepper JR. Innocent victim of a localised outbreak: legionella endocarditis. Heart. (2003) 89:e16. doi: 10.1136/heart.89.5.e16
21. Brusch JL. Legionnaire’s disease: cardiac manifestations. Infect Dis Clin North Am. (2017) 31:69–80.
22. Yoon SH, Ha SM, Kwon S, Lim J, Kim Y, Seo H, et al. Introducing EzBioCloud: a taxonomically united database of 16S rRNA gene sequences and whole-genome assemblies. Int J Syst Evol Microbiol. (2017) 67:1613–7. doi: 10.1099/ijsem.0.001755
23. Reischl U, Linde HJ, Lehn N, Landt O, Barratt K, Wellinghausen N. Direct detection and differentiation of Legionella spp. and Legionella pneumophila in clinical specimens by dual-color real-time PCR and melting curve analysis. J Clin Microbiol. (2002) 40:3814–7. doi: 10.1128/JCM.40.10.3814-3817.2002
24. Brouqui P, Raoult D. Endocarditis due to rare and fastidious bacteria. Clin Microbiol Rev. (2001) 14:177–207.
25. Portal E, Descours G, Ginevra C, Mentasti M, Afshar B, Chand M, et al. Legionella antibiotic susceptibility testing: is it time for international standardization and evidence-based guidance? J Antimicrob Chemother. (2021) 76:1113–6. doi: 10.1093/jac/dkab027
26. Stout JE, Arnold B, Yu VL. Comparative activity of ciprofloxacin, ofloxacin, levofloxacin, and erythromycin against Legionella species by broth microdilution and intracellular susceptibility testing in HL-60 cells. Diagn Microbiol Infect Dis. (1998) 30:37–43. doi: 10.1016/s0732-8893(97)00174-0
27. Hennebique A, Bidart M, Jarraud S, Beraud L, Schwebel C, Maurin M, et al. Digital PCR for detection and quantification of fluoroquinolone resistance in Legionella pneumophila. Antimicrob Agents Chemother. (2017) 61:e00628–617. doi: 10.1128/AAC.00628-17
28. Wang JY, Li X, Chen JY, Tong B. Epileptic seizure after use of moxifloxacin in man with legionella longbeachae pneumonia. Emerg Infect Dis. (2020) 26:2725–7. doi: 10.3201/eid2611.191815
29. Fournier PE, Thuny F, Richet H, Lepidi H, Casalta JP, Arzouni JP, et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin Infect Dis. (2010) 51:131–40. doi: 10.1086/653675
30. Ramchandar N, Burns J, Coufal NG, Pennock A, Briggs B, Stinnett R, et al. Use of metagenomic next-generation sequencing to identify pathogens in pediatric osteoarticular infections. Open Forum Infect Dis. (2021) 8:ofab346.
31. Chan WS, Au CH, Leung HC, Ho DN, Li D, Chan TL, et al. Potential utility of metagenomic sequencing for improving etiologic diagnosis of infective endocarditis. Fut. Cardiol. (2019) 15:411–24. doi: 10.2217/fca-2018-0088
32. Lee RA, Al Dhaheri F, Pollock NR, Sharma TS. Assessment of the clinical utility of plasma metagenomic next-generation sequencing in a pediatric hospital population. J Clin Microbiol. (2020) 58:e00419–20. doi: 10.1128/JCM.00419-20
33. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC Guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European society of cardiology (ESC). Endorsed by: European association for cardio-thoracic surgery (EACTS), the European association of nuclear medicine (EANM). Eur Heart J. (2015) 36:3075–128. doi: 10.1093/eurheartj/ehv319
34. Diederen BMW, de Jong CMA, Marmouk F, Kluytmans J, Peeters MF, Van der Zee A. Evaluation of real-time PCR for the early detection of Legionella pneumophila DNA in serum samples. J Med Microbiol. (2007) 56(Pt. 1):94–101. doi: 10.1099/jmm.0.46714-0
35. Murdoch DR, Walford EJ, Jennings LC, Light GJ, Schousboe MI, Chereshsky AY, et al. Use of the polymerase chain reaction to detect Legionella DNA in urine and serum samples from patients with pneumonia. Clin Infect Dis. (1996) 23:475–80.
Keywords: endocarditis, prosthetic valve endocarditis (PVE), molecular diagnostic techniques, blood culture negative endocarditis, Legionella bozemanae, Legionella bozemanii
Citation: Fraz MSA, Dahle G, Skaug KM, Jarraud S, Frye S, Bjørnholt JV and Nordøy I (2022) Case report: A prosthetic valve endocarditis caused by Legionella bozemanae in an immunocompetent patient. Front. Med. 9:1055465. doi: 10.3389/fmed.2022.1055465
Received: 27 September 2022; Accepted: 14 October 2022;
Published: 03 November 2022.
Edited by:
Francesco Paolo Bianchi, University of Bari Aldo Moro, ItalyReviewed by:
Katarina Westling, Karolinska Institutet (KI), SwedenLurdes Santos, Centro Hospitalar Universitário de São João (CHUSJ), Portugal
Copyright © 2022 Fraz, Dahle, Skaug, Jarraud, Frye, Bjørnholt and Nordøy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mai Sasaki Aanensen Fraz, bWFpLnNhc2FraS5hYW5lbnNlbkBnbWFpbC5jb20=