 Lev Volkov1,2*
Lev Volkov1,2* Marion Delpuech3
Marion Delpuech3 Marie Conrad1Guilhem Courte1Aurélie Cravoisy1Lionel Nace1Cedric Baumann3
Marie Conrad1Guilhem Courte1Aurélie Cravoisy1Lionel Nace1Cedric Baumann3 Sébastien Gibot1
Sébastien Gibot1- 1Service de Réanimation Médicale, Hôpital Central, Centre Hospitalier Régional Universitaire (CHRU), Nancy, France
- 2Service de Réanimation Médico-Chirurgicale, Centre Hospitalier-Le Mans, Le Mans, France
- 3Délégation à la Recherche Clinique et à l'Innovation (DRCI), Méthodologie Promotion Investigation (MPI) Department, Methodology, Data Management, and Statistic Unit, University Hospital of Nancy, Vandœuvre-Lès-Nancy, France
Introduction: Seasonal epidemic influenza and SARS-CoV-2 are the most frequent viruses causing acute respiratory distress syndrome (ARDS). To what extent these two etiologies differ in ICU patients remains uncertain. We, therefore, aimed at comparing the severity and outcomes of influenza and SARS-CoV-2-induced ARDS in mechanically ventilated patients.
Methods: This retrospective, analytic, single-center study was conducted in the medical ICU of Nancy University Hospital in France. Adult patients hospitalized with confirmed influenza (from 2009 to 2019) or SARS-CoV-2-induced ARDS (between March 2020 and May 2021) and those under mechanical ventilation were included. Each patient with influenza was matched with two patients with COVID-19, with the same severity of ARDS. The primary endpoint was death in ICU on day 28. The secondary endpoints were the duration of vasopressors, the use of renal replacement therapy, the duration of mechanical ventilation, and the ICU length of stay.
Results: A total of 42 patients with influenza were matched with 84 patients with COVID-19. They had similar sex distribution, age, Charlson comorbidity index, and ARDS severity. On day 28, 11 (26.2%) patients in the influenza group and nine (10.7%) patients in the COVID-19 group had died (p = 0.0084, HR = 3.31, CI 95% [1.36–8.06]). In the univariate Cox model, being infected with SARS-CoV-2, SOFA and SAPS II scores, initial arterial pH, PaCO2, PaO2/FiO2, serum lactate level, platelet count, and use of renal replacement therapy were significantly associated with mortality. In the multivariate Cox model, the SOFA score at admission (p < 0.01, HR = 1.284, CI 95% [1.081; 1.525]) and the initial pH (p < 0.01, HR = 0.618, CI 95% [0.461; 0.828]) were the only predictors of mortality. The type of virus had no influence on mortality, though patients with COVID-19 underwent longer mechanical ventilation and received more neuromuscular blockers and prone positioning.
Conclusion: In mechanically ventilated patients with ARDS, 28-day mortality was higher among patients with influenza as compared to patients with COVID-19 because of a higher initial extra-pulmonary severity. However, the type of virus was not, by itself, correlated with mortality.
Introduction
The seasonal influenza virus is well known for causing winter epidemics and even unpredictable pandemics. By invading the lower respiratory tract, it can cause acute respiratory distress syndrome (ARDS) and is responsible each year for admissions to the intensive care unit (ICU) with prolonged hospitalization (1, 2). The outbreak of the coronavirus disease 2019 (COVID-19) pandemic overwhelmed hospitals with a great number of patients presenting acute respiratory failure, with many developing ARDS (3). Nowadays, influenza and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are the most frequent viruses causing ARDS (4). Their modes of transmission and clinical presentation are similar. They can cause acute respiratory disease, as well as extra-pulmonary disorders such as cardiac and kidney failure, and endotheliopathy (1, 5, 6). To understand the particularities of COVID-19 in critically ill patients, patients with influenza and COVID-19 have been compared in the literature. However, studies often compared COVID-19 with other multiple causes of ARDS, including viral and bacterial infections (7, 8). Other studies did not focus on critically ill patients (4, 9), and in those that did, not all the patients were under mechanical ventilation (10, 11). Indeed, studies dealing only with mechanically ventilated patients with ARDS are very scarce (12, 13).
This study aimed to compare the characteristics and outcomes of mechanically ventilated ICU patients suffering from influenza or SARS-CoV-2 ARDS of similar pulmonary severity to untangle the influence of the virus type by itself.
Methods
Study design and setting
We conducted a retrospective, single-center, and analytical matched cohort study in the ICU, Réanimation Médicale, Hôpital Central of the Nancy Regional and University Hospital Center in France. The study was registered on www.clinicaltrials.gov under the number NCT04941092 and was approved by the Ethics Committee of our University Hospital.
Participants
The electronic medical database of the hospital was searched for patients hospitalized in our ICU between 2009 and 2019 with the main diagnosis containing “influenza,” and between March 2020 and May 2021 with the main diagnosis containing “COVID-19” or “SARS-CoV-2.” Inclusion criteria were participants older than 18 years, a diagnosis of ARDS according to the Berlin definition criteria (14), influenza or SARS-CoV-2 infection confirmed by reverse transcription-polymerase chain reaction (RT-PCR), and the use of invasive mechanical ventilation. Exclusion criteria were pregnancy, the use of invasive mechanical ventilation for more than 48 h before admission into the ICU, or a secondary transfer to another ICU. Each patient with influenza was matched with two patients with COVID-19, based on the severity of ARDS: severe ARDS or mild to moderate ARDS.
Endpoints
The primary endpoint was mortality in the ICU within 28 days. The secondary endpoints were the duration of vasopressors, the use of renal replacement therapy, the duration of mechanical ventilation, the length of stay in the ICU, and the duration and amount of sedation.
Data collection
Data were collected from the patient's medical records and anonymized. Data included baseline demographic characteristics, such as age, sex, height, and weight, patient's past medical history, laboratory findings, and clinico-biological parameters: simplified acute physiology score (SAPS II) and sequential organ failure assessment (SOFA) score, the worst ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2), highest positive end-expiratory pressure (PEEP) level within the first 24 h of mechanical ventilation, complete blood cells count, blood chemistry, serum lactate concentration, duration of mechanical ventilation, number of prone positioning sessions, use and duration of catecholamines, renal replacement therapy, extracorporeal membrane oxygenation (ECMO), antibiotics, corticosteroids, neuromuscular blockers, and duration and quantity of midazolam, sufentanil, propofol, dexmedetomidine, and chlorpromazine.
Statistical methods
Descriptive and comparative analyses
Baseline characteristics were described as counts and percentages for categorical variables and as median and interquartile ranges for continuous variables. The distribution of the baseline parameters was compared between the two groups of infected patients using an exact chi-square test, exact Fisher test, or Wilcoxon test, according to the type of variable and statistical conditions appliance. The Fisher and chi-square tests were used for qualitative variables. The Fisher test was used in default of the chi-square test when the statistical conditions were not verified. The Wilcoxon test was used for continuous variables as they did not follow a Gaussian distribution.
Survival analysis
Patients discharged from the ICU before day 28 were censored at the time of discharge. Associations between each parameter of interest and overall survival measured during the 28 days after ICU admission were assessed by univariate Cox models on paired series. Then, correlations between variables with a p-value of <0.05 were estimated by a Pearson coefficient or a Phi coefficient, according to the type of variable. In case of high correlation (r or Phi > 0.75) between variables, a choice was made based on the clinical relevance of the variables of interest. A multivariate Cox model on paired series was then built to assess the association between virus type and mortality within 28 days of ICU admission adjusted for the selected factors. If several models were built, the selection of the final model was made based on the Akaike criterion [the best model being the one with the lowest AIC (Akaike information criterion)]. These analyses were completed by Kaplan–Meier overall survival curves compared using a log-rank test. We estimated the hazard ratios with a confidence interval of 95% and fixed the alpha's risk threshold to 5%. The analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Characteristics of the patients
Among 43 patients with influenza and 113 patients with COVID-19 who met the inclusion criteria, 42 patients with influenza were matched with 84 patients with COVID-19 (Figure 1). A total of 30 influenza patients with severe ARDS were matched with 60 COVID-19 patients with severe ARDS. Notably, 12 influenza patients with mild to moderate ARDS were matched with 24 COVID-19 patients with mild to moderate ARDS (three patients with influenza having mild ARDS were matched with one patient with COVID-19 having mild ARDS and one patient with COVID-19 having moderate ARDS, respectively, as there were not enough mild COVID-19 ARDS). No significant differences were observed for sex, age, and Charlson comorbidity index (Table 1). There were more hematologic malignancies in the influenza group (5 vs. 1). Compared to the patients with COVID-19, patients with influenza had significantly higher median SOFA and SAPS II scores, a lower initial median arterial pH, a higher initial median PaCO2, a higher median serum lactate level, a lower median platelet count, and a higher median serum creatinine level at admission (Table 1). All patients underwent mechanical ventilation.
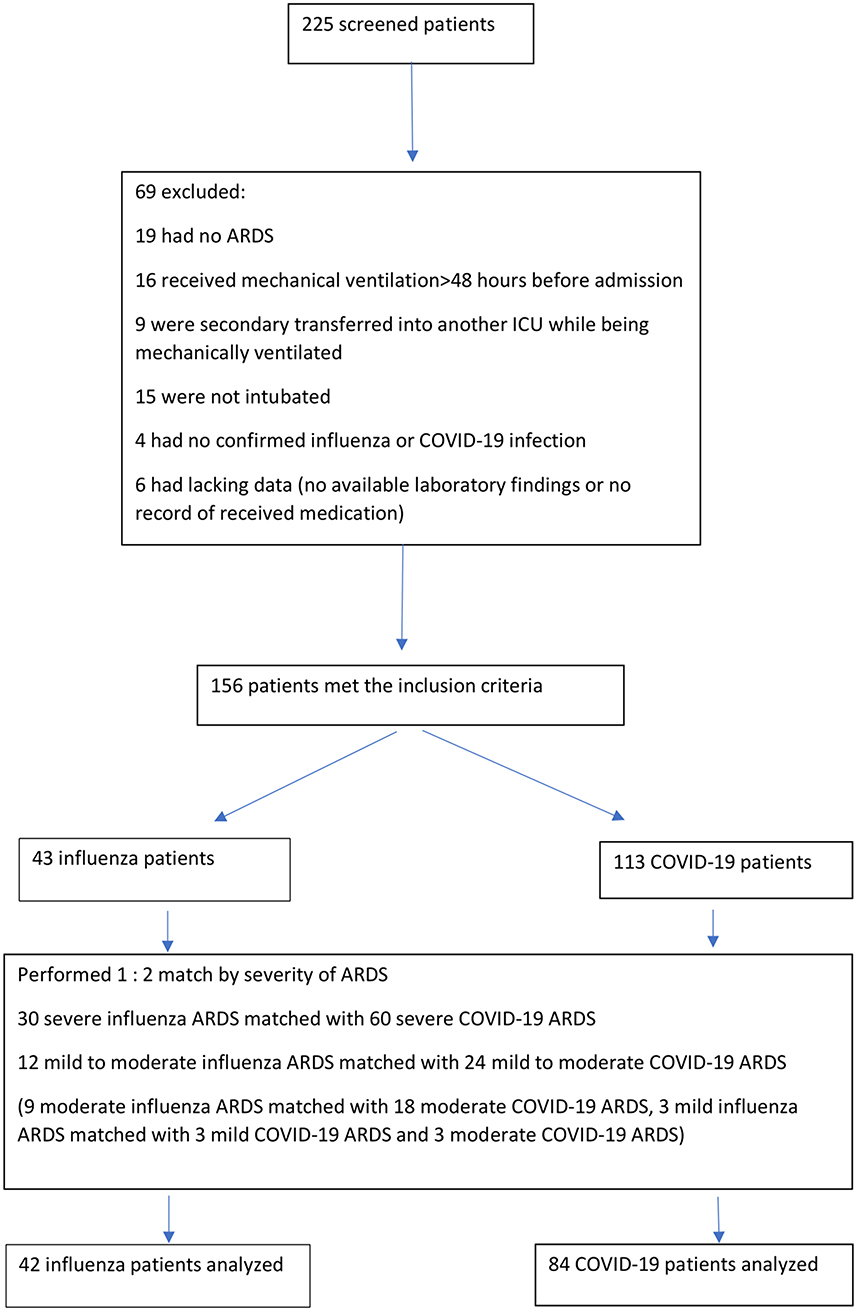
Figure 1. Flow chart.
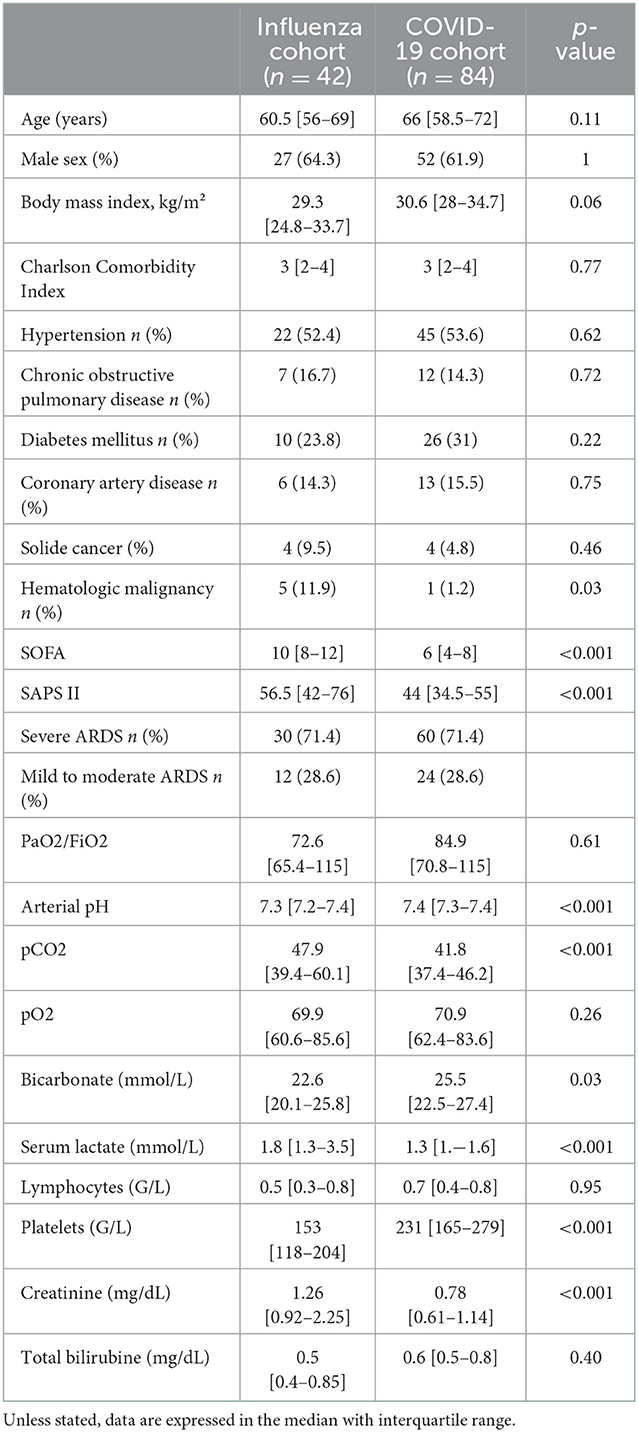
Table 1. Baseline characteristics.
ICU therapies
As shown in Table 2, patients with COVID-19 underwent significantly longer median mechanical ventilation with higher initial PEEP levels, received neuromuscular blockers more often, and underwent prone positioning more often during their ICU stay than patients with influenza. There was no statistical difference between the proportion of patients in each group receiving vasopressors, although patients with COVID-19 received vasopressors for a longer time than patients with influenza. Patients with influenza had a trend of receiving more renal replacement therapy than patients with COVID-19, without statistical significance (28.6 vs. 14.3%, p = 0.07). When comparing sedative agents, patients with COVID-19 received midazolam and sufentanil much longer, with higher doses of midazolam. Two patients with influenza were placed under ECMO, but none were in the COVID-19 group.
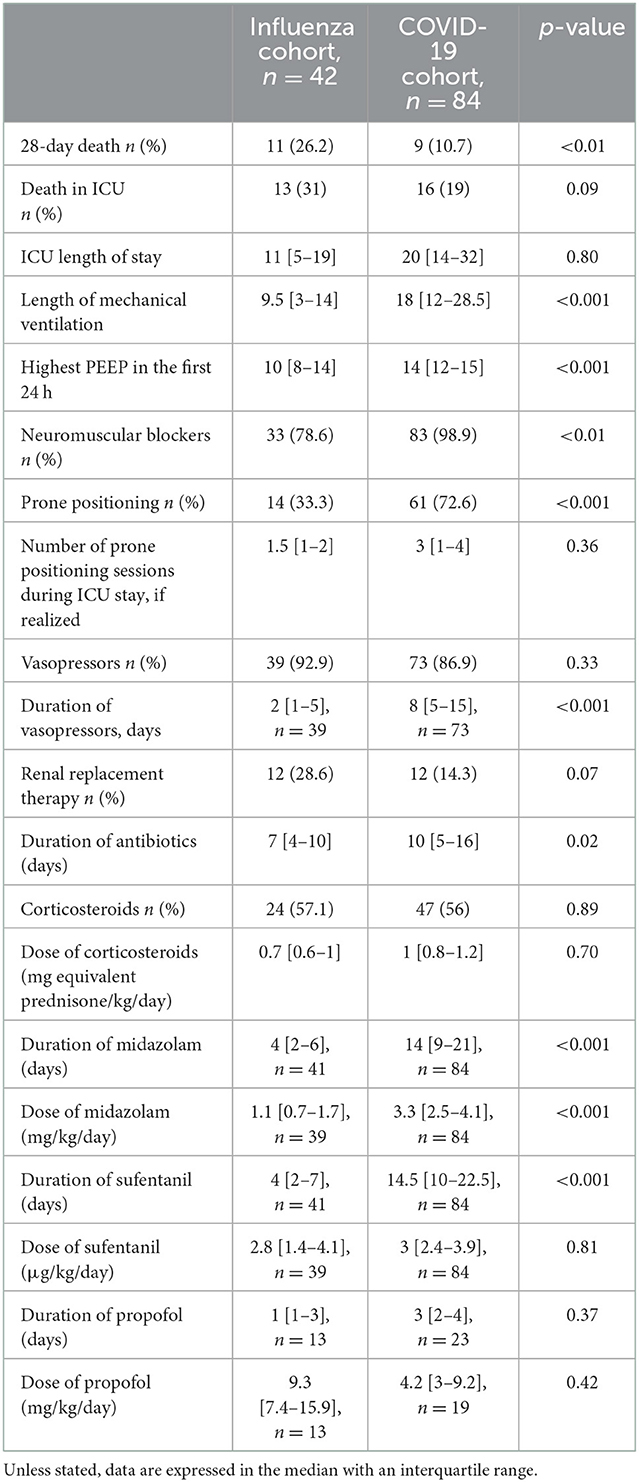
Table 2. ICU therapies and outcome.
Association between the type of virus and survival
On day 28, 11 (26.2%) patients in the influenza group and nine (10.7%) patients in the COVID-19 group had died (HR = 3.31, CI 95% [1.36–8.06], p = 0.0084). Figure 2 shows the Kaplan–Meier curve of the probability of survival from ICU admission to day 28, with a significantly higher probability of survival in the COVID-19 group (p = 0.005). Overall, death in ICU was 31% in the influenza group vs. 19% in the COVID-19 group (p = 0.09).

Figure 2. Probability of survival (Kaplan-Meyer curves).
The results of univariate Cox models are shown in Table 3. Being infected with influenza, the SOFA and SAPS II scores, initial arterial pH, PaO2/FiO2, PaCO2, serum lactate concentration, platelet count, and use of renal replacement therapy were significantly associated with mortality.
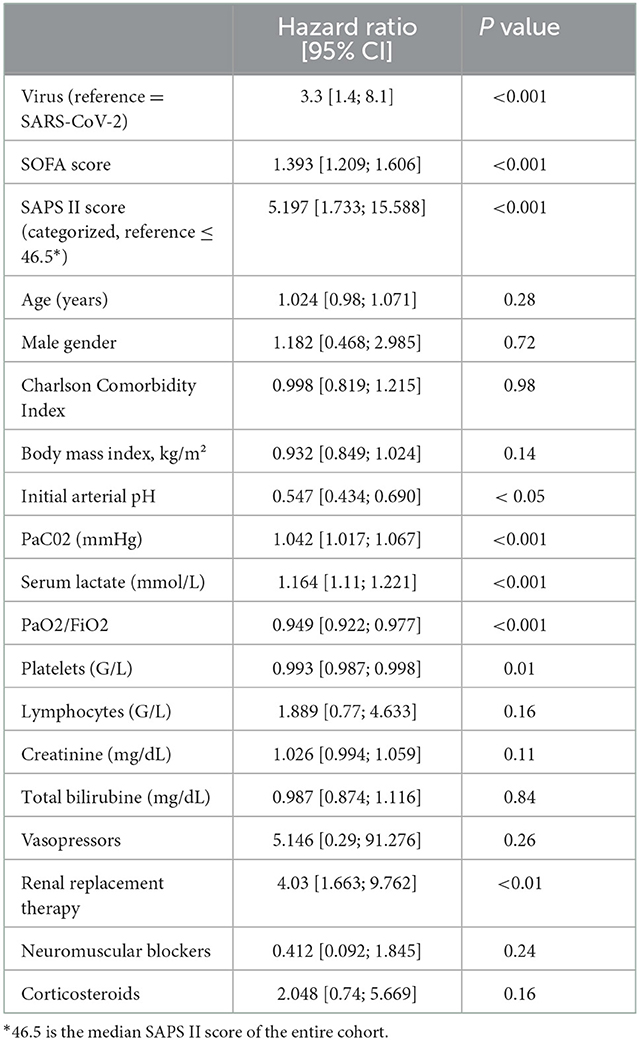
Table 3. Predictive factors of mortality (univariate Cox models results).
The analysis of correlation matrices between the variables of interest with a p-value of <0.05 in the univariate model and clinical reasoning led to the construction of two multivariate Cox models. Model 1 (Table 4) includes the type of virus, arterial pH, and SOFA score (AIC = 157.7); and model 2 (Table 5) includes the type of virus, arterial pH, and SAPS II score (AIC = 163.9). The first model including SOFA score and pH value showed to be the most parsimonious. The type of virus had no independent effect on mortality.
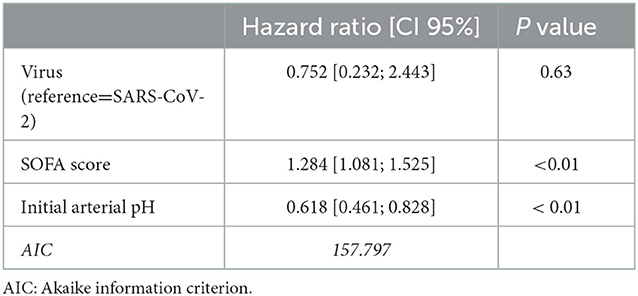
Table 4. Predictive factors of mortality (multivariate Cox model) – SOFA score considered.
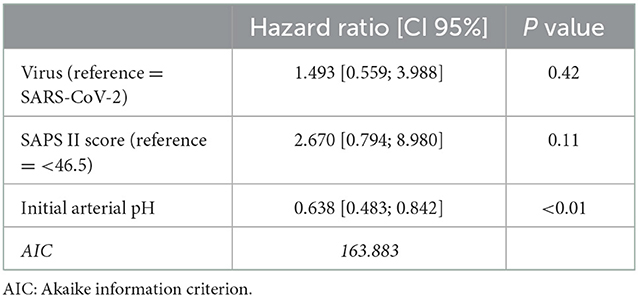
Table 5. Predictive factors of mortality (multivariate Cox model) – SAPS II score considered.
Discussion
This analytic retrospective study comparing 42 influenza and 84 COVID-19 mechanically ventilated patients, matched by the severity of ARDS, found that influenza patients had higher 28-day mortality (26.2 vs. 10.7%) (p < 0.05). However, multivariate Cox analysis revealed that the type of virus by itself did not affect mortality: SOFA score and initial arterial pH were the only independent predictors of outcome.
When not considering the early studies reporting very high mortality rates that were not confirmed afterward, the mortality of mechanically ventilated patients with COVID-19 in ICU varies between 24 and 43% (3, 15–18), with an important heterogeneity between cohorts (19, 20). The mortality of our patients with COVID-19 is lower despite similar demographics and severity than in other studies. In contrast, the 26.2% mortality rate of our patients with influenza is more consistent with the literature, as reported mortality rates in mechanically ventilated influenza patients with ARDS range between 26 and 45% (21–24). There are no arguments in the literature for a difference in the outcome, length of hospitalization, or mechanical ventilation among the different strains of influenza (25).
Studies comparing influenza and SARS-CoV-2-induced ARDS are scarce. Gjurašin et al. (12) described 42 influenza and 30 COVID-19 intubated patients in a Croatian center with mortality rates of 55 and 63%, respectively. For comparison, the overall ICU mortality in our study was 31% in patients with influenza and 19% in patients with COVID-19. Cobb et al. (10) described 74 patients with influenza and 65 patients with COVID-19 in the medical ICUs of two Washington hospitals, but less than 60% of them were intubated. Furthermore, there were more ARDS cases in their COVID-19 group than in their influenza group, which makes it difficult to compare those patients with ours. Hospital mortality in their ARDS patients was 37% in the influenza group and 46% in the COVID-19 group. Tang et al. (11) described 75 H1N1-induced ARDS from Wuhan and 73 COVID-19-induced ARDS from Beijing. In-hospital mortality was 34.7% among patients with influenza and 28.8% among patients with COVID-19. Here again, the groups had different respiratory severity (PaO2/FiO2 of 107 and 85.8% of mechanically ventilated patients in the influenza group, and 199 and 19.2% in the COVID-19 group). Cárdenas et al. (13), in a single-center study from Mexico, compared 94 influenza and 147 COVID-19 intubated patients with ARDS. Although their patients with influenza had more shock at admission, were more hypoxemic, and had a higher SOFA score, their crude ICU mortality was lower than that of the patients with COVID-19 (22 vs. 39%), which contrasted with our results. Piroth et al. (4) described the characteristics of more than 100000 hospitalized inflluenza and COVID-19 patients, using a large nationwide french database. Among them, 14% were admitted to the ICU. Their in-hospital mortality among mechanically ventilated patients was 26% in the influenza group, and 31.8% in the COVID-19 group. Finally, Ludwig et al. (9) described a German database of 6,762 patients with influenza and 2,343 patients with COVID-19, with 15% admitted to the ICU. Their mortality rate in mechanically ventilated patients was 36% in patients with influenza and 47% in patients with COVID-19. However, only 54% of ventilated patients with COVID-19 and 14% of ventilated patients with influenza had ARDS. It is, therefore, difficult to discuss and compare the mortality of these studies with ours, as they were not all focusing on critically ill patients and described patients with different respiratory severity. Of note, all these studies included patients with COVID-19 at the beginning of the pandemic, with only one study extending to October 2020 (13).
The difference in mortality between patients with influenza and COVID-19 observed in our study seems to be explained by the increased initial severity of patients with influenza, as witnessed by significantly higher SOFA and SAPS II scores at admission. As the patients were matched by the severity of ARDS, the difference in these scores is mainly due to a difference in extra-pulmonary severity. However, patients with influenza had an initial higher PaCO2 level, with lower pH, which could reflect impaired pulmonary compliance. Unfortunately, compliance could not be calculated in our study. Furthermore, significantly lower pH in the first 24 h could be explained by metabolic acidosis due to initial hemodynamic and renal failure. Botta et al. (18) showed a significant association between initial pH and 28-day mortality in their patients with COVID-19. In our study, patients with influenza had more acute kidney injury (AKI) with a higher serum creatinine level at admission, and a trend toward a more frequent use of renal replacement therapy (RRT) (28 vs. 14%) during the ICU stay, though without statistically significant difference. AKI is a well-described complication of COVID-19 (26) and influenza (27), especially in critically ill patients, and is a major risk factor for mortality. In the previously cited studies, AKI in patients with COVID-19 varies between 18 and 58%, with a need for RRT between 11 and 28% (3, 9–12, 16, 18, 19), and is associated with the highest mortality if occurring within the first 15 days (3). AKI in patients with influenza varies between 11 and 59% (9, 12, 22, 25).
In our study, patients with influenza had significantly higher lactate levels on admission and a lower platelet count, which could reflect the initial severity of the shock. By contrast, patients with COVID-19 received vasopressors significantly longer, but this was probably the consequence of a need for longer mechanical ventilation and an increased amount of sedative agents, due to secondary respiratory worsening, rather than primary hemodynamic failure.
Thus, it could be hypothesized that for an equal severity of ARDS, a greater proportion of patients with influenza has multi-organ failure at admission into the ICU. Indeed, our multivariate model shows that initial arterial pH and SOFA score are independent predictors of mortality in our patients. For example, each decrease of 0.1 points in the initial arterial pH increases the risk of mortality by 61%. In this model, there was no statistical association between the type of virus and mortality, meaning that having influenza or SARS-CoV-2 is not, by itself, a risk factor for mortality. In other words, there would be no difference in terms of mortality between patients with influenza and COVID-19, if their initial severity was similar.
Finally, patients with COVID-19 underwent longer mechanical ventilation, with higher initial PEEP levels, and received more neuromuscular blockers and prone position, which is consistent with the literature (8–10, 12). Regarding the use of sedative agents, patients with COVID-19 received midazolam longer and at a higher dose, as previously reported (28, 29). Possible explanations are that COVID-19 had a high respiratory drive and tachyphylaxis due to prolonged mechanical ventilation. Furthermore, challenges in entering patients' rooms due to isolation precautions and fear of self-extubation could lead to higher sedation (29).
Our work has several limitations. First, it is a retrospective, single-center study possibly dampening its external validity. Second, the data of patients with influenza were recorded for a period of 10 years, whereas those of patients with COVID-19 were recorded over 1 year, leading to a comparison of different periods with possible different medical practices. Third, sample sizes were small, leading to a possible misinterpretation of the results. However, to our knowledge, our study is the first to compare critically ill patients with influenza and COVID-19 matched by the severity of respiratory failure. All our patients had ARDS and underwent mechanical ventilation in the same center, making their outcomes comparable, and the results of our study pertinent.
Conclusion
This study compared mechanically ventilated patients with influenza and COVID-19 admitted to the ICU and matched by the severity of ARDS and found that the mortality was higher among patients with influenza, due to higher extra-pulmonary severity. However, the virus type, by itself, influenza or SARS-CoV-2, was not predictive of mortality.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Anonymized data are available upon request by the corresponding author. Requests to access these datasets should be directed to LV, bGV2YS52b2xrLnRvdXJzQGdtYWlsLmNvbQ==.
Ethics statement
The studies involving human participants were reviewed and approved by Comité d'éthique du CHRU de Nancy. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
LV, MC, GC, AC, LN, and SG were involved in the management of the patients. LV and SG collected data. CB and MD analyzed data. LV, SG, CB, and MD wrote the manuscript. All authors approved the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kalil AC, Thomas G. Influenza virus-related critical illness: pathophysiology and epidemiology. Crit Care. (2019) 23:258. doi: 10.1186/s13054-019-2539-x
2. Hernu R, Simon M, Baudry T, Casalegno JS, Lina B, Cour M, et al. Burden of critically ill patients with influenza in a French catchment population. Sci Rep. (2021) 11:1–7. doi: 10.1038/s41598-021-89912-y
3. COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med. (2021) 47:60–73. doi: 10.1007/s00134-020-06294-x
4. Piroth L, Cottenet J, Mariet AS, Bonniaud P, Blot M, Tubert-Bitter P, et al. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: a nationwide, population-based retrospective cohort study. Lancet Respir Med. (2021) 9:251–259. doi: 10.1016/S2213-2600(20)30527-0
5. Tan CW, Tan JY, Wong WH, Cheong MA, Ng IM, Conceicao EP, et al. Clinical and laboratory features of hypercoagulability in COVID-19 and other respiratory viral infections amongst predominantly younger adults with few comorbidities. Sci Rep. (2021) 11:1–9. doi: 10.1038/s41598-021-81166-y
6. Zaim S, Chong JH, Sankaranarayanan V, Harky A. COVID-19 and Multiorgan Response. Curr Probl Cardiol. (2020) 45:100618. doi: 10.1016/j.cpcardiol.2020.100618
7. Sjoding MW, Admon AJ, Saha AK, Kay SG, Brown CA, Co I, et al. Comparing clinical features and outcomes in mechanically ventilated patients with COVID-19 and acute respiratory distress syndrome. Ann Am Thorac Soc. (2021) 18:1876–85. doi: 10.1513/AnnalsATS.202008-1076OC
8. Bain W, Yang H, Shah FA, Suber T, Drohan C, Al-Yousif N, et al. COVID-19 versus Non-COVID ARDS: Comparison of Demographics, Physiologic Parameters, Inflammatory Biomarkers and Clinical Outcomes. Ann Am Thorac Soc Annals. (2021) 18:1202–10. doi: 10.1513/AnnalsATS.202008-1026OC
9. Ludwig M, Jacob J, Basedow F, Andersohn F, Walker J. Clinical outcomes and characteristics of patients hospitalized for Influenza or COVID-19 in Germany. Int J Infect Dis. (2021) 103:316–322. doi: 10.1016/j.ijid.2020.11.204
10. Cobb NL, Sathe NA, Duan KI, Seitz KP, Thau MR, Sung CC, et al. Comparison of clinical features and outcomes in critically ill patients hospitalized with COVID-19 versus Influenza. Ann Am Thorac Soc. (2021) 18:632–40. doi: 10.1513/AnnalsATS.202007-805OC
11. Tang X, Du RH, Wang R, Cao TZ, Guan LL, Yang CQ, et al. Comparison of Hospitalized Patients With ARDS Caused by COVID-19 and H1N1. Chest. (2020) 158:195–205. doi: 10.1016/j.chest.2020.03.032
12. Gjurašin B, Santini M, Krajinović V, Papić N, Atelj A, Kotarski V, et al. retrospective comparison between influenza and COVID-19-associated ARDS in a Croatian tertiary care center. Wien Klin Wochenschr. (2021) 133:406–11. doi: 10.1007/s00508-020-01759-x
13. Cárdenas CH, Lugo G, García DH, Pérez-Padilla R. Comparison of the clinical characteristics and mortality in ARDS due to COVID-19 versus ARDS due to Influenza, AH1N1pdm09. MedRxiv. (2021).
14. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. (2012) 307:2526–33. doi: 10.1001/jama.2012.5669
15. Ferrando C, Suarez-Sipmann F, Mellado-Artigas R, Hernández M, Gea A, Arruti E, et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. (2020) 46:2200–11. doi: 10.1007/s00134-020-06251-8
16. Oliveira E, Parikh A, Lopez-Ruiz A, Carrilo M, Goldberg J, Cearras M, et al. ICU outcomes and survival in patients with severe COVID-19 in the largest health care system in central Florida. PLoS ONE. (2021) 16:e0249038. doi: 10.1371/journal.pone.0249038
17. Quah P, Li A, Phua J. Mortality rates of patients with COVID-19 in the intensive care unit: a systematic review of the emerging literature. Crit Care. (2020) 24:285. doi: 10.1186/s13054-020-03006-1
18. Botta M, Tsonas AM, Pillay J, Boers LS, Algera AG, Bos LDJ, et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): a national, multicentre, observational cohort study. Lancet Respir Med. (2021) 9:139–48. doi: 10.1016/S2213-2600(20)30459-8
19. Chang R, Elhusseiny KM, Yeh YC, Sun WZ. COVID-19 ICU and mechanical ventilation patient characteristics and outcomes—A systematic review and meta-analysis. PLoS ONE. (2021) 16:e0246318. doi: 10.1371/journal.pone.0246318
20. Armstrong RA, Kane AD, Cook TM. Outcomes from intensive care in patients with COVID-19: a systematic review and meta-analysis of observational studies. Anaesthesia. (2020) 75:1340–9. doi: 10.1111/anae.15201
21. Bal A, Casalegno JS, Melenotte C, Daviet F, Ninove L, Edouard S, et al. Influenza-induced acute respiratory distress syndrome during the 2010-2016 seasons: bacterial co-infections and outcomes by virus type and subtype. Clin Microbiol Infect. (2020) 26:947e.1–e4. doi: 10.1016/j.cmi.2020.03.010
22. Beumer MC, Koch RM, Van Beuningen D, OudeLashof AM, Van de Veerdonk FL, Kolwijck E, et al. Influenza virus and factors that are associated with ICU admission, pulmonary co-infections and ICU mortality. J Crit Care. (2019) 50:59–65. doi: 10.1016/j.jcrc.2018.11.013
23. Martínez A, Soldevila N, Romero-Tamarit A, Torner N, Godoy P, Rius C, et al. Risk factors associated with severe outcomes in adult hospitalized patients according to influenza type and subtype. PLoS ONE. (2019) 14:e0210353. doi: 10.1371/journal.pone.0210353
24. Shah NS, Greenberg JA, McNulty MC, Gregg KS, Riddell J, Mangino JE, et al. Severe Influenza in 33 US Hospitals, 2013-2014: Complications and Risk Factors for Death in 507 Patients. Infect Control HosEpidemiol. (2015) 36:1251–60. doi: 10.1017/ice.2015.170
25. Sarda C, Palma P, Rello J. Severe influenza: overview in critically ill patients. Curr Opin Crit Care. (2019) 25:449–57. doi: 10.1097/MCC.0000000000000638
26. Gabarre P, Dumas G, Dupont T, Darmon M, Azoulay E, Zafrani L. Acute kidney injury in critically ill patients with COVID-19. Intensive Care Med. (2020) 46:1339–48. doi: 10.1007/s00134-020-06153-9
27. Watanabe T. Renal complications of seasonal and pandemic influenza A virus infections. Eur J Pediatr. (2013) 172:15–22. doi: 10.1007/s00431-012-1854-x
28. Karamchandani K, Dalal R, Patel J, Modgil P, Quintili A. Challenges in sedation management in critically ill patients with COVID-19: A brief review. Curr Anesthesiol Rep. (2021) 11:107–15. doi: 10.1007/s40140-021-00440-x
Keywords: ARDS, influenza, COVID-19, intensive care unit (ICU), mechanical ventilation
Citation: Volkov L, Delpuech M, Conrad M, Courte G, Cravoisy A, Nace L, Baumann C and Gibot S (2023) Clinical outcomes and characteristics of critically ill patients with influenza- and COVID-19-induced ARDS: A retrospective, matched cohort study. Front. Med. 9:1027984. doi: 10.3389/fmed.2022.1027984
Received: 25 August 2022; Accepted: 05 December 2022;
Published: 05 January 2023.
Edited by:
Diana Vilar-Compte, Instituto Nacional de Cancerologia, MexicoReviewed by:
Aysun Tekin, Mayo Clinic, United StatesPratikkumar Vekaria, School of Medicine Greenville (USC), United States
Copyright © 2023 Volkov, Delpuech, Conrad, Courte, Cravoisy, Nace, Baumann and Gibot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lev Volkov,  bGV2YS52b2xrLnRvdXJzQGdtYWlsLmNvbQ==
bGV2YS52b2xrLnRvdXJzQGdtYWlsLmNvbQ==