
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 19 December 2022
Sec. Hematology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1026812
 Han-ying Huang1,2,3†
Han-ying Huang1,2,3† Yun Wang1,2†
Yun Wang1,2† Tobias Herold4†
Tobias Herold4† Robert Peter Gale1,2,5Jing-zi Wang1,3Liang Li1,2
Robert Peter Gale1,2,5Jing-zi Wang1,3Liang Li1,2 Huan-xin Lin1,3*†
Huan-xin Lin1,3*† Yang Liang1,2*†
Yang Liang1,2*†Introduction: There are many different chronic lymphoblastic leukemia (CLL) survival prediction models and scores. But none provide information on expression of immune-related genes in the CLL cells.
Methods: We interrogated data from the Gene Expression Omnibus database (GEO, GSE22762; Number = 151; training) and International Cancer Genome Consortium database (ICGC, CLLE-ES; Number = 491; validation) to develop an immune risk score (IRS) using Least absolute shrinkage and selection operator (LASSO) Cox regression analyses based on expression of immune-related genes in CLL cells. The accuracy of the predicted nomogram we developed using the IRS, Binet stage, and del(17p) cytogenetic data was subsequently assessed using calibration curves.
Results: A survival model based on expression of 5 immune-related genes was constructed. Areas under the curve (AUC) for 1-year survivals were 0.90 (95% confidence interval, 0.78, 0.99) and 0.75 (0.54, 0.87) in the training and validation datasets, respectively. 5-year survivals of low- and high-risk subjects were 89% (83, 95%) vs. 6% (0, 17%; p < 0.001) and 98% (95, 100%) vs. 92% (88, 96%; p < 0.001) in two datasets. The IRS was an independent survival predictor of both datasets. A calibration curve showed good performance of the nomogram. In vitro, the high expression of CDKN2A and SREBF2 in the bone marrow of patients with CLL was verified by immunohistochemistry analysis (IHC), which were associated with poor prognosis and may play an important role in the complex bone marrow immune environment.
Conclusion: The IRS is an accurate independent survival predictor with a high C-statistic. A combined nomogram had good survival prediction accuracy in calibration curves. These data demonstrate the potential impact of immune related genes on survival in CLL.
There are several survival prediction models and scores for chronic lymphocytic leukemia (CLL) including Binet and Rai staging systems, MD Anderson Cancer Center 2007 index score, CLL International Prognostic Index (CLL-IPI), Barcelona-Brno score, International Prognostic Score-A (IPS-A), CLL-01 and a tailored approach (1–5). These models and scores include clinical, laboratory and genetic co-variates such as age, disease stage, Eastern Cooperative Oncology Group (ECOG) performance score, immunoglobulin variable heavy chain (IGHV) mutation state, cytogenetic abnormalities, especially del(11) and del(17p), serum β2-microglobulin, lymphocyte doubling time and others. These models and scores have only modest accuracy with C-statistics of 0.60–0.77 (6). Data on the expression of immune-related genes in CLL cells is not incorporated in any survival prediction, prognostic model, or score.
We developed a survival predictive model we termed the Immune Risk Score (IRS) by analyzing immune-related gene expression data in CLL cells from two publicly available datasets. We evaluated the model in multivariable analyses and verified it in a validation dataset. We combined the IRS with Binet stage and del(17p) cytogenetics data to develop a survival prediction nomogram.
Data from 2 CLL datasets including 642 subjects with micro-array survival data, GSE22762 and CLLE-ES (7, 8), were obtained from the Gene Expression Omnibus (GEO) database and the International Cancer Genome Consortium (ICGC) database. The Data Access Committee approved access to this data under DACO-7056. Gene expression profiles were derived from the microarray of subjects’ peripheral blood or bone marrow in two datasets and normalized between different arrays by sva package used to remove batch effects in high-throughput experiments to reduce dependence, stabilize error rate estimates and improve repeatability (9, 10). Download the list of immune-related genes from the ImmPort database1 for extracting all immune genes in the GEO dataset and the ICGC dataset, to obtain a list of candidate immune genes for further study. The workflow is summarized in Supplementary Figure 1.
The GSE22762 dataset was used for training to construct the IRS model. Univariable Cox regression analyses were used to identify immune-related genes significantly correlated with survival at p < 0.05. We used Least Absolute Shrinkage and Selection Operator (LASSO) Cox regression analyses to identify the best weighting coefficient of immune-related genes for survival. The maximum likelihood estimate of penalty after 1,000-fold cross-validation was determined and the 1-SE criterion was used to determine the optimal value of the penalty parameter λ. These data were used to develop the IRS. The CLLE-ES dataset was used as validation set.
Prediction accuracy of the IRS was quantified using time-dependent receiver-operating characteristic (ROC) curves and the area under the curve (AUC) method. Subjects were divided into high- and low-risk cohorts by the optimal cut-off of risk score in each dataset. Survivals of subjects in the high- and low-risk cohorts were compared by Kaplan–Meier curves with log-rank tests. The GSE22762 and CLLE-ES datasets had clinical co-variates which were included in uni and multivariable Cox regression analyses.
We developed a survival prediction nomogram by combining the IRS with Binet stage and del(17p) cytogenetics data. In the nomogram, each co-variate is assigned a point and added to give a total point corresponding to 1-, 3-, or 5-year survival. The calibration curve showed the relationship between the predicted value and the measured value of the nomogram in the training dataset. The IRS, clinical and laboratory co-variates and nomogram were compared with the time-dependent receiver operating characteristic curve (time-ROC curve) for 5-year survival.
We collected 44 newly diagnosed CLL patients, whose diagnosis was confirmed by histopathology following bone marrow aspiration procedures taking place between 2011 and 2020 at Sun Yat-sen University Cancer Center (SYSUCC), Guangzhou, China. The other inclusion criteria were: No acute infection 2 weeks prior to enrollment; no chronic inflammation or autoimmune disease; and no consumption of immunosuppressive or immunomodulatory drugs. All patients were followed-up until September 2020 through hospital records or phone contact with the patients or relatives who were aware of their illness. This study was approved by the Research Ethics Committee of SYSUCC (Approved number B2021-044-01) and was conducted in accordance with the Declaration of Helsinki.
We verified two immune-related genes (CDKN2A and SREBF2) with the larger weight coefficient according to IRS model, by immunohistochemistry analysis. Several types of immune cells, including monocytes, CD4+ T cells, CD8+T cells, and neutrophils were selected to further explore the relationship between immune genes and the bone marrow immune environment.
Briefly, the paraffin-embedded bone marrow puncture specimens were stained using antibodies against CD4+ T cells (anti-CD4 antibody, ZSGB_BIO, Catalog No. ZA-0519), CD8+ T cells (anti-CD8 antibody, ZSGB_BIO, Catalog No. ZA-0508), monocytes (anti-CD14 antibody, SANTA, Catalog No. sc-58951), neutrophils (anti-CD66b antibody, ABCAM, Catalog No. ab197678), and two immune-related genes: the sterol regulatory element binding transcription factor (SREBF2; anti-SREBF2 antibody, ABCAM, Catalog No. ab30682), and the cyclin dependent kinase inhibitor 2A (CDKN2A; anti-CDKN2A antibody, Affinity, Catalog No. AF0228). Every five duplicate slide was analyzed by two independent researchers in a blinded manner. For the immune cells, researchers recorded the number of positive immune cells and calculated the density of immune cells using Image J software (National Institute of Health, Bethesda, MD, USA). For the immune-related genes, we recorded the staining area and degree of immune protein expression using a 1–3-point system. The points were added up to obtain a total immunohistochemistry analysis score for each immune-related gene.
Subjects were divided into high- or low-risk cohorts at the optimal cut-off IRS which was determined by ROC curves analyses. Prediction accuracy was quantified using time-dependent ROCs and AUCs calculated to determine the Concordance C-Statistic. Survival was defined as the interval from diagnosis to death from any cause. Time-to-therapy (TTT) was defined as the interval from diagnosis to start of 1st or next treatment. A significant proportion of patients in GSE22762 were not analyzed at diagnosis but at a more advanced disease stage and in relapse. Survival and TTT in those patients were calculated as the interval from measurement to the respective event. Survivals were compared in Kaplan–Meier curves using the log-rank test. In univariable Cox regression analyses co-variates with P < 0.05 were used in subsequent multivariable Cox regression analyses. SPSS software version 24.0 (SPSS, Inc., Chicago, IL, USA), R software version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria), and Perl version 5.24.3 (Perl Foundation, Holland, MI, USA) were used for statistical analyses. A two-sided P < 0.05 was considered significant.
Clinical and laboratory co-variates of 632 subjects from GSE22762 and CLLE-ES were displayed in Table 1. LASSO Cox regression analysis was used to determine the five genes of model (shown in Supplementary Figure 2A). The optimal weighting coefficient for each gene was determined by the regularization parameter lambda (shown in Supplementary Figure 2B). Five genes with optimal coefficients were selected to develop the IRS, including CDKN2A, SREBF2, NRIP1, BCL11B, and SIRT1 (Supplementary Table 1). The equation used to calculate the IRS is:
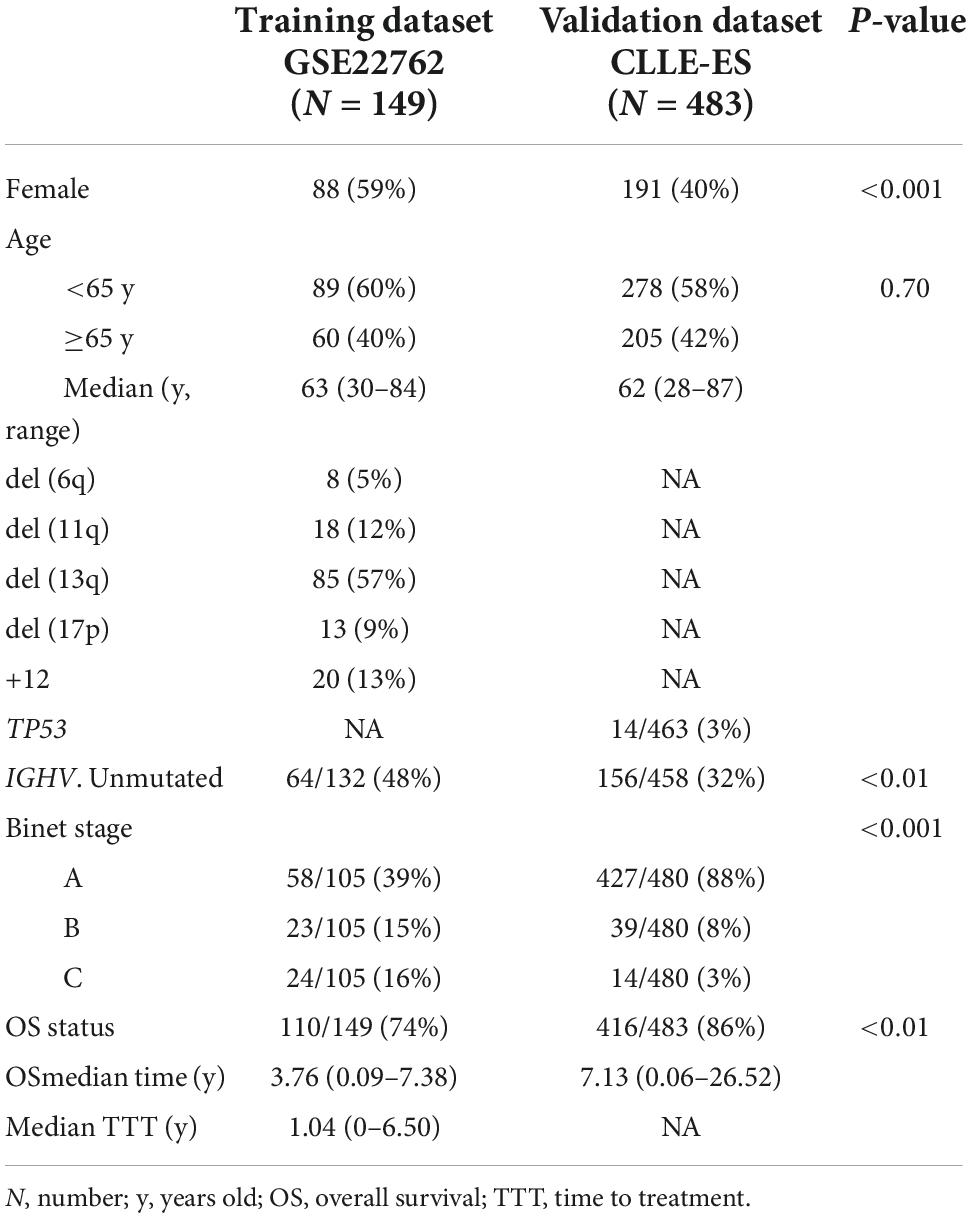
Table 1. Clinical co-variates in the training and validation datasets.
IRS = (0.54 × CDKN2A RNA expression) + (0.27 × SREBF2 RNA expression) − (0.04 × SIRT1 RNA expression) − (0.11 × BCL11B RNA expression) − (0.26 × NRIP1 RNA expression).
We calculated the IRS for each subject in both datasets according to this equation dividing subjects into high- and low-risk cohorts based on the optimal IRS cut-off of the corresponding dataset. The training and validation data sets’ optimal cut-off values are 2.29 and 1.94, respectively.
Sensitivity and specificity of the IRS in each dataset were assessed by time-dependent ROC analyses. AUCs in the training dataset for 1-, 3-, and 5-year survivals were 0.90 [95% Confidence Interval, (CI), 0.78, 0.99), 0.84 (0.73, 0.93), and 0.88 (0.81, 0.96; shown in Figure 1A]. Comparable data for the validation dataset were 0.75 (0.54, 0.87), 0.63 (0.38, 0.80), and 0.64 (0.48, 0.78; shown in Figure 1B). We also compared survival of the high- and low-risk cohorts using Kaplan–Meier curves in each dataset (shown in Figures 1C, D). In the training dataset, subjects were divided into high- and low-risk groups using the optimal cut-off value of IRS. The high- and low-risk groups had 5-year survival of 89% (83, 95%) vs. 6% (0, 17%; P < 0.0001). Comparable survivals in the validation dataset were 98% (95, 100%) vs. 92% (88, 96%; P < 0.001). The IRS in each dataset was an independent prognostic factor in multivariate Cox regression analysis (Table 2). Moreover, time to treatment (TTT) was statistically different between high-risk and low-risk cohorts in the training dataset (P < 0.001, shown in Supplementary Figure 3). In addition, the 64 patients who were initially diagnosed with CLL in the training set were divided into subgroups to further verify the difference in survival between high and low immune score groups, as well as the sensitivity and specificity for predicting survival, all of which were well validated (shown in Supplementary Figure 4).
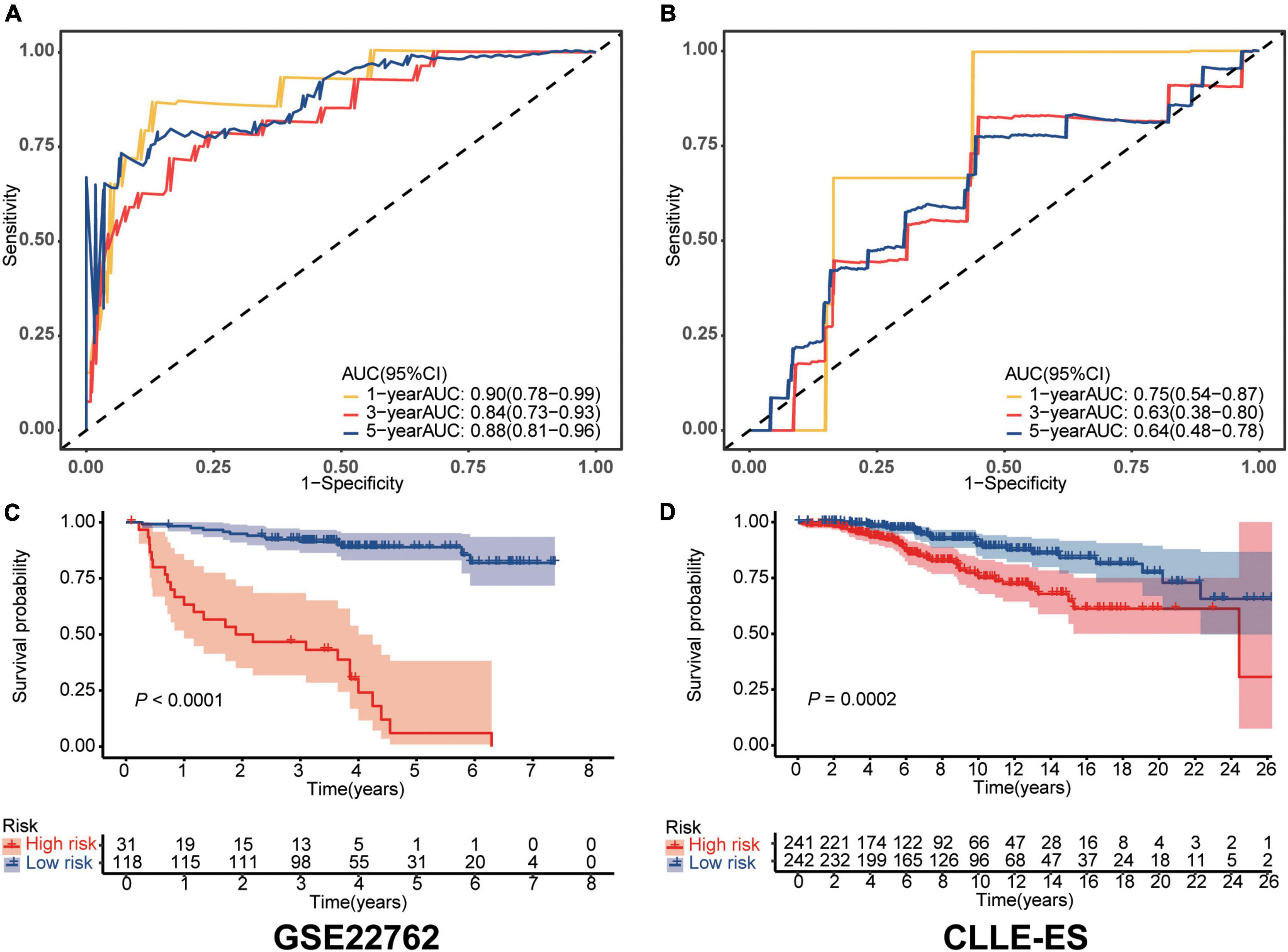
Figure 1. Validation of the immune risk score model. (A,B) Sensitivity and specificity of the IRS model were assessed in each dataset by time-dependent ROC analyses. (C,D) Survival differences between high- and low-risk cohorts in each dataset.

Table 2. Univariable and multivariable regression analyses of survival.
Next, we built a survival nomogram for the training dataset combining the IRS with Binet stage and del(17p) data (shown in Figure 2A). (There were too few deaths and lack of data in the validation cohort for nomogram building.) A calibration curve showed good accuracy predicting 1-, 3-, and 5-year survivals (shown in Figure 2B). The nomogram increased 5-year survival prediction accuracy compared with IRS only, Binet stage only and del(17p) only (shown in Figure 2C). The concordance statistics of the nomogram was 0.87 (0.70, 1.00) compared with concordance statistics of 0.83 (0.64, 1.00), 0.74 (0.53, 0.95), and 0.65 (0.46, 0.85), respectively.
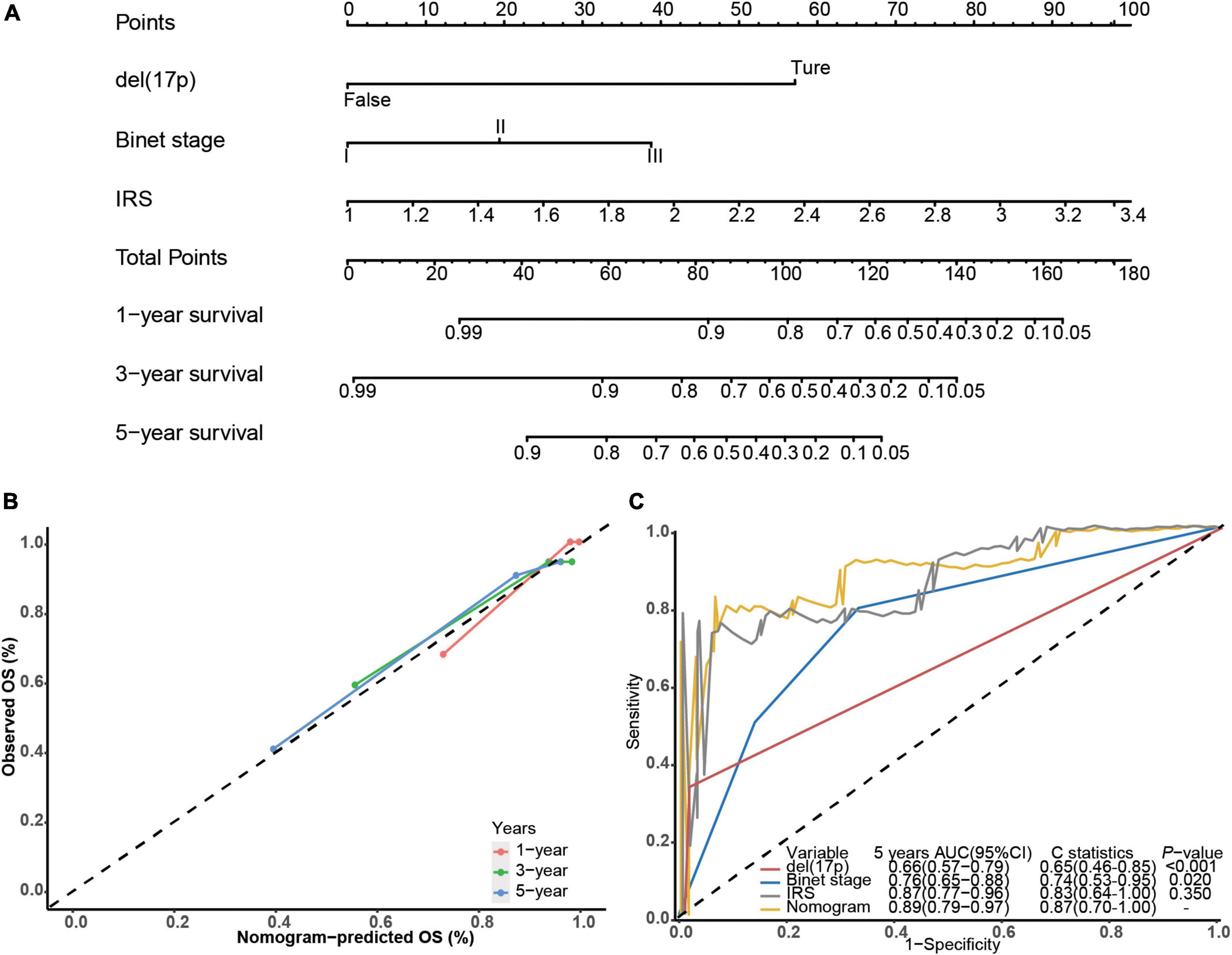
Figure 2. Building the survival nomogram. (A) The combined nomogram plot was built in the training dataset. (B) Time-dependent ROC curves of training nomogram were compared based on co-variates 1-, 3- and 5-year survivals. (C) 5-year ROC curves and C-statistics of the nomogram compared with other co-variates in the training dataset.
Forty-four patients newly diagnosed with CLL were retrospectively enrolled in our study. The age range was 28–78 years old, and the survival time range was 96–3,371 days. Immunohistochemistry analysis experiments confirmed high expression of SREBF2 and CDKN2A proteins in the bone marrow of CLL patients (Figures 3A, B). In addition, the information on each immunohistochemical indicator was shown in the Table 3. According to the best cut-off value of the immunohistochemistry analysis score, the prognosis of CLL patients in the high expression group was significantly worse than that in the low expression group (P < 0.05; Figures 3C, D). Interestingly, SREBF2 expression levels were negatively correlated with the infiltration of CD8+ T cells, CD4+ T cells, CD14+ monocytes, and CD66b+ neutrophils, whereas CDKN2A expression negatively correlated with the presence of CD8+ T cells, CD4+ T cells, and CD66b+ neutrophils (P < 0.05, Figure 3E).
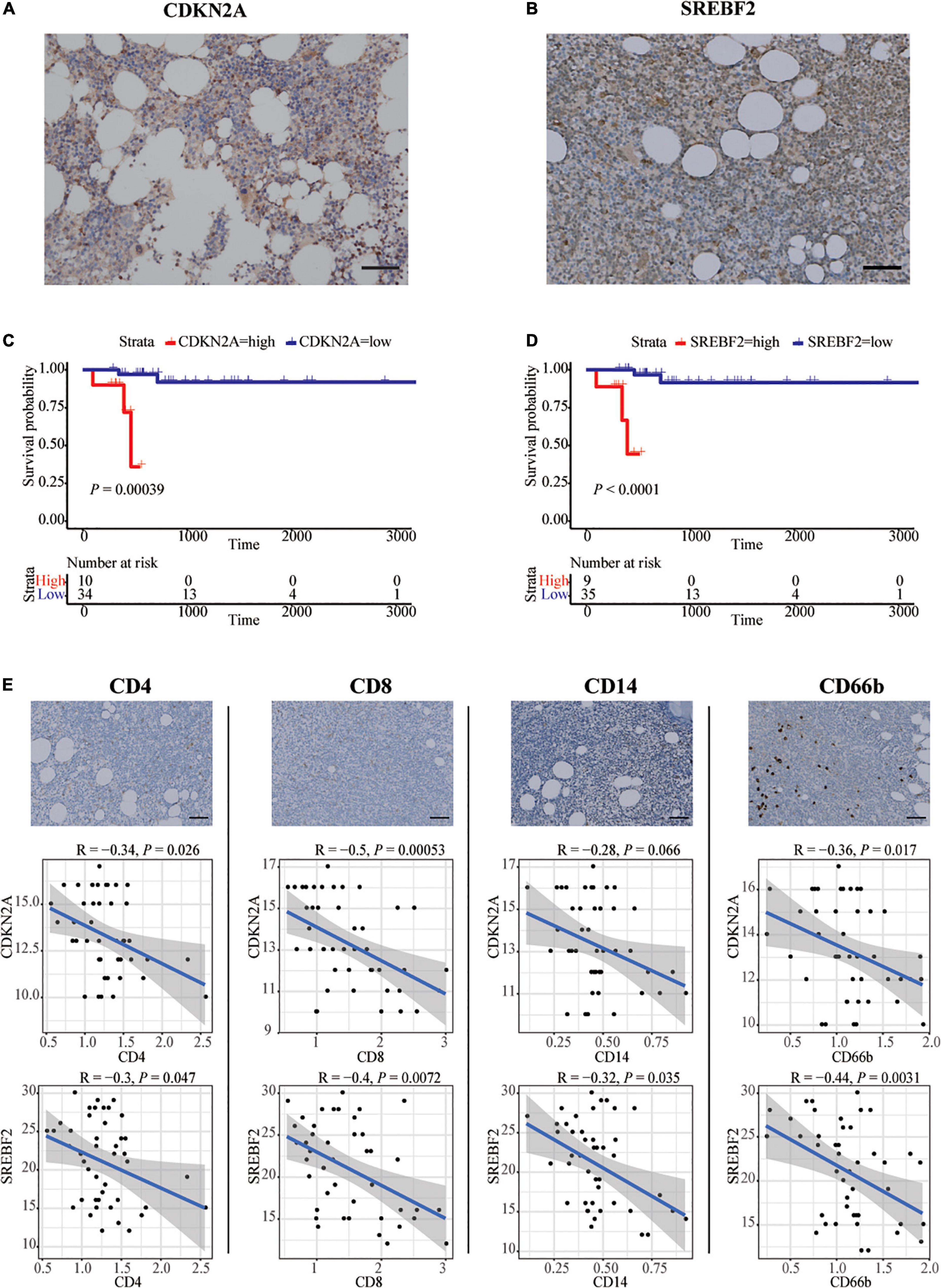
Figure 3. In vitro validation in bone marrow of CLL patients by IHC. (A,B) Representative images of SREBF2, and CDKN2A -positive cells in a bone marrow sample taken from one CLL patient. Scare bar: 50 μm. (C,D) Kaplan–Meier curves for overall survival of CLL patients associated with SREBF2 and CDKN2A expression. (E) Representative images of CD4, CD8, CD14, and CD66b -positive cells in a bone marrow sample taken from one CLL patient. Scare bar: 50 μm. Correlation analysis between two immune-related genes and immune cell types (Spearman analysis).

Table 3. The mean, the best cut-off value, and the number of cases with high and low IHC scores for each immunohistochemical index.
No CLL survival prediction model includes data on expression of immune-related genes in chronic lymphocytic leukemia cells. Using data on immune-related gene expression from the public GSE22762 dataset, we developed a prognostic model, the IRS, which we independently verified in the CLLE-ES dataset. In our model high expression of NRIP1, BCL11B and SIRT1 were associated with a good and high expression of CDKN2A and SREBF2 with poor prognoses. Functions of these genes are summarized in Supplementary Table 2. Areas under the curve (AUC) for 1-year survivals in the training and validation datasets were 0.90 [95% Confidence Interval (CI), 0.78, 0.99] and 0.75 (0.54, 0.87). With the combination of Binet stage and del(17p) cytogenetic data, we developed a nomogram that enhanced the accuracy of survival prediction, with a C-statistic of 0.87 (0.70, 1.00) in the training set. Due to missing data, we were not able to test the nomogram in the validation set.
NRIP1, BCL11B, and SIRT1 are the 3 genes whose elevated expression is linked to better survival. NRIP1, expression is associated with a favorable prognosis in previous CLL studies and may operate via the NF-κB pathway and/or Wnt signaling pathways in CLL (7, 11). Del(17p13) and del(11q22) are associated with low NRIP1 expression as unmutated IGHV state (12, 13). Consequently, high NRIP1 expression in CLL may be a surrogate for absence of one or more of adverse prognostic co-variates. Of note, a recent study identified NRIP1 as a partner of the NRIP1-MIR99AHG fusion in acute myeloid leukemia. Although it is a rare fusion, it is suspected to be associated with poor clinical outcome (14).
BCL11B regulates thymocyte development and is a cancer suppressor gene in T-cell leukemia/lymphoma (15–19). BCL11B inactivation in normal thymocytes triggers cell proliferation, TP53-dependent apoptosis and increases growth of transformed lymphocytes (20). BCL11B up-regulates NKG2D ligands of the major histocompatibility complex class I-related molecules A and B (MICA and MICB), promotes the anti-tumor response of T- and NK-cells and prevents immune evasion of colon cancer cells (21). Down-regulation of BCL11B expression inhibits proliferation and induces apoptosis in malignant T-cells (22, 23). There are no data other than ours on the impact of BCL11B expression in CLL.
SIRT1 is up-regulated in some cancers including acute and chronic myeloid leukemias (AML and CML) but down-regulated in breast and liver cancers (24, 25). Low SIRT1 expression increases abnormal self-renewal of myelodysplastic syndrome (MDS) stem cells by enabling over-acetylation and reducing the activity of TET2 (26). Inhibition of SIRT1 expression promotes the growth of T-cell ALL by activating the NOTCH and NF-κB pathways (27). The impact of SIRT1 expression in other on hematologic cancers is controversial. Two studies reported SIRT1 is over-expressed in primary CLL cells and in the JVM-3 and MEC-2 CLL cell lines and that inhibiting SIRT1 expression might activate the p53 pathway inhibiting cell proliferation and promoting apoptosis in CLL (28, 29).
Increased expression of CDKN2A and SREBF2 correlated with worse survival. CDKN2A is a rather contradictory gene. Manifested as inactivation of CDKN2A and p53 in pancreatic cancer (30). However, CDKN2A is highly expressed in gastric precancerous lesions but decreased expression in gastric cancer stage (31). This appears to have similar changes in hematologic malignancies. In this study, CDKN2A was highly expressed in CLL/SLL. CDKN2A is inactivated when CLL is converted to Richter syndrome; CDKN2A inactivation combined with mutations in TP53, MYC and NOTCH1 are associated with transformation of CLL to Richter syndrome (32–34). At present, the expression level of CDKN2A in CLL patients has not been clearly reported. These data represent different meanings of CDKN2A at different stages. SREBF2 expression is associated with a poor prognosis in T-cell lymphoma, AML, plasma cell myeloma and liver cancer (35–38). There are no data on the impact of SREBF2 expression in CLL.
According to previous research, the presence of immune cells (CD8+ T cells, CD4+ T cells, CD14+ monocytes, and CD66b+ neutrophils) in the bone marrow immune environment correlated positively with good CLL prognosis (39, 40). We hypothesize that upregulation of SREBF2 and CDKN2A may be associated with decreased infiltration of bone marrow immune cells. This may be an underlying mechanism that causes CLL immunosuppression.
Why should immune gene expression in leukemia cells correlate with prognosis? We hypothesize expression of these genes reflects biologic features of the leukemia cells, but it is also possible there is an interaction with the host immune response, cancer micro-environment, both or something else. We also emphasize we are reporting correlations, not necessarily cause-and-effect.
Our study has several limitations. 1st, the datasets we interrogated lacked more important clinical and/or laboratory co-variates (such as CLL-IPI score) limiting our multivariable analyses. 2nd, survival of subjects in the validation set was significantly better than in the training dataset reflecting different therapies and disease stage, which has the advantage of allowing us to term the IRS a prognostic rather than predictive score. However, the very good survival of the high- and low-risk cohorts in the validation cohort decreased but did not negate discrimination power of the IRS. 3rd, the large differences between the datasets make it impossible to define a uniform cut-off. Future studies are necessary to establish an optimal cut off.
In conclusion, we developed and validated a prognostic survival model for CLL based on the expression of 5 immune-related genes which had high accuracy. We also developed a survival nomogram by adding Binet stage and del(17p) cytogenetics data to the IRS which improved the C-statistic. Two immune-related genes were predicted and validated using immunohistochemistry analysis experiments, which may play an important role in the complex bone marrow immune environment.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
This study protocol was reviewed and approved by the Data Access Committee (Approval number DACO-7056) from the ICGC database, without written informed consent. This study was also approved by the Research Ethics Committee of SYSUCC (Approval number B2021-044-01). Research was conducted in accordance with guidelines for human research and was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
H-YH wrote the original manuscript. YL, RG, H-YH, and YW reviewed and edited the manuscript. H-YH and YW performed the software analyses. TH, J-ZW, and LL collected the data. YL and H-XL were responsible for the research design, project administration, and funding. All authors reviewed the final manuscript and agreed to submit for publication.
YL was supported, in part, by Sun Yat-sen University Start-up Funding (Grant no. 201603). YL and RG acknowledge support funding from the Ministry of Science and Technology of China (Grant no. 84000-51200002). H-XL was also supported by the National Natural Science Foundation of China (Grant no. 81773103) and Natural Science Foundation of Guangdong Province (Grant no. 2017A030313617).
Profs. Emili Montserrat (University of Barcelona), Neil Kay (Mayo Clinic), Susan Geyer (Mayo Clinic), Victoria Wang (Dana-Farber Cancer Institute), kindly reviewed the manuscript and offered helpful suggestions. RG acknowledges support from the National Institute of Health Research (NIHR) Biomedical Research Centre funding scheme.
RG was a consultant to BeiGene Ltd., Fusion Pharma LLC., La Jolla NanoMedical Inc., Mingsight Parmaceuticals Inc. CStone Pharmaceuticals, NexImmune Inc. and Prolacta Bioscience; advisor to Antengene Biotech LLC, Medical Director, FFF Enterprises Inc.; partner, AZAC Inc.; Board of Directors, Russian Foundation for Cancer Research Support; and Scientific Advisory Board: StemRad Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1026812/full#supplementary-material
1. Rai K, Sawitsky A, Cronkite E, Chanana A, Levy R, Pasternack B. Clinical staging of chronic lymphocytic leukemia. Blood. (1975) 46:219–34. doi: 10.1182/blood.V46.2.219.bloodjournal462219
2. Binet J, Auquier A, Dighiero G, Chastang C, Piguet H, Goasguen J, et al. A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer. (1981) 48:198–206. doi: 10.1002/1097-0142(19810701)48:1<198::AID-CNCR2820480131>3.0.CO;2-V
3. Wierda W, O’Brien S, Wang X, Faderl S, Ferrajoli A, Do K, et al. Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood. (2007) 109:4679–85. doi: 10.1182/blood-2005-12-051458
4. International CLL-IPI working group. An international prognostic index for patients with chronic lymphocytic leukaemia (CLL-IPI): a meta-analysis of individual patient data. Lancet Oncol. (2016) 17:779–90. doi: 10.1016/S1470-2045(16)30029-8
5. Gonzalez-Gascon Y, Munoz-Novas C, Figueroa I, Hernandez-Sanchez M, Rodriguez-Vicente A, Quijada-Alamo M, et al. Prognosis assessment of early-stage chronic lymphocytic leukemia: are we ready to predict clinical evolution without a crystal ball? Clin Lymphoma Myeloma Leuk. (2020) 20:548–55.e4. doi: 10.1016/j.clml.2020.03.003
6. Kreuzberger N, Damen J, Trivella M, Estcourt L, Aldin A, Umlauff L, et al. Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: a systematic review and meta-analysis. Cochrane Database Syst Rev. (2020) 7:CD012022. doi: 10.1002/14651858.CD012022.pub2
7. Herold T, Jurinovic V, Metzeler K, Boulesteix A, Bergmann M, Seiler T, et al. An eight-gene expression signature for the prediction of survival and time to treatment in chronic lymphocytic leukemia. Leukemia. (2011) 25:1639–45. doi: 10.1038/leu.2011.125
8. Ramsay A, Martinez-Trillos A, Jares P, Rodriguez D, Kwarciak A, Quesada V. Next-generation sequencing reveals the secrets of the chronic lymphocytic leukemia genome. Clin Transl Oncol. (2013) 15:3–8. doi: 10.1007/s12094-012-0922-z
9. Leek J, Johnson W, Parker H, Jaffe A, Storey J. The sva package for removing batch effects and other unwanted variation in high-throughput experiments. Bioinformatics. (2012) 28:882–3. doi: 10.1093/bioinformatics/bts034
10. Leek J, Storey JD. A general framework for multiple testing dependence. Proc Natl Acad Sci USA. (2008) 105:18718–23. doi: 10.1073/pnas.0808709105
11. Zschiedrich I, Hardeland U, Krones-Herzig A, Berriel Diaz M, Vegiopoulos A, Muggenburg J, et al. Coactivator function of RIP140 for NFkappaB/RelA-dependent cytokine gene expression. Blood. (2008) 112:264–76. doi: 10.1182/blood-2007-11-121699
12. Lapierre M, Castet-Nicolas A, Gitenay D, Jalaguier S, Teyssier C, Bret C, et al. Expression and role of RIP140/NRIP1 in chronic lymphocytic leukemia. J Hematol Oncol. (2015) 8:20. doi: 10.1186/s13045-015-0116-6
13. Morabito F, Cutrona G, Mosca L, D’Anca M, Matis S, Gentile M, et al. Surrogate molecular markers for IGHV mutational status in chronic lymphocytic leukemia for predicting time to first treatment. Leuk Res. (2015) 39:840–5. doi: 10.1016/j.leukres.2015.05.005
14. Kerbs P, Vosberg S, Krebs S, Graf A, Blum H, Swoboda A, et al. Fusion gene detection by RNA-sequencing complements diagnostics of acute myeloid leukemia and identifies recurring NRIP1-MIR99AHG rearrangements. Haematologica. (2022) 107:100–11. doi: 10.3324/haematol.2021.278436
15. Wakabayashi Y, Inoue J, Takahashi Y, Matsuki A, Kosugi-Okano H, Shinbo T, et al. Homozygous deletions and point mutations of the Rit1/Bcl11b gene in gamma-ray induced mouse thymic lymphomas. Biochem Biophys Res Commun. (2003) 301:598–603. doi: 10.1016/S0006-291X(02)03069-3
16. Grabarczyk P, Przybylski G, Depke M, Volker U, Bahr J, Assmus K, et al. Inhibition of BCL11B expression leads to apoptosis of malignant but not normal mature T cells. Oncogene. (2007) 26:3797–810. doi: 10.1038/sj.onc.1210152
17. Kamimura K, Ohi H, Kubota T, Okazuka K, Yoshikai Y, Wakabayashi Y, et al. Haploinsufficiency of Bcl11b for suppression of lymphomagenesis and thymocyte development. Biochem Biophys Res Commun. (2007) 355:538–42. doi: 10.1016/j.bbrc.2007.02.003
18. Gutierrez A, Kentsis A, Sanda T, Holmfeldt L, Chen S, Zhang J, et al. The BCL11B tumor suppressor is mutated across the major molecular subtypes of T-cell acute lymphoblastic leukemia. Blood. (2011) 118:4169–73. doi: 10.1182/blood-2010-11-318873
19. Kurosawa N, Fujimoto R, Ozawa T, Itoyama T, Sadamori N, Isobe M. Reduced level of the BCL11B protein is associated with adult T-cell leukemia/lymphoma. PLoS One. (2013) 8:e55147. doi: 10.1371/journal.pone.0055147
20. Wakabayashi Y, Watanabe H, Inoue J, Takeda N, Sakata J, Mishima Y, et al. Bcl11b is required for differentiation and survival of alphabeta T lymphocytes. Nat Immunol. (2003) 4:533–9. doi: 10.1038/ni927
21. Qian M, Geng J, Luo K, Huang Z, Zhang Q, Zhang J, et al. BCL11B regulates MICA/B-mediated immune response by acting as a competitive endogenous RNA. Oncogene. (2020) 39:1514–26. doi: 10.1038/s41388-019-1083-0
22. Huang X, Chen S, Shen Q, Chen S, Yang L, Grabarczyk P, et al. Down regulation of BCL11B expression inhibits proliferation and induces apoptosis in malignant T cells by BCL11B-935-siRNA. Hematology. (2011) 16:236–42. doi: 10.1179/102453311X13025568941961
23. Huang X, Shen Q, Chen S, Chen S, Yang L, Weng J, et al. Gene expression profiles in BCL11B-siRNA treated malignant T cells. J Hematol Oncol. (2011) 4:23. doi: 10.1186/1756-8722-4-23
24. Alves-Fernandes D, Jasiulionis M. The role of SIRT1 on DNA damage response and epigenetic alterations in cancer. Int J Mol Sci. (2019) 20:3153. doi: 10.3390/ijms20133153
25. Li L, Bhatia R. Role of SIRT1 in the growth and regulation of normal hematopoietic and leukemia stem cells. Curr Opin Hematol. (2015) 22:324–9. doi: 10.1097/MOH.0000000000000152
26. Simeoni F, Somervaille T. Revert the SIRT: normalizing SIRT1 activity in myelodysplastic stem cells. Cell Stem Cell. (2018) 23:315–7. doi: 10.1016/j.stem.2018.08.003
27. Okasha S, Itoh M, Tohda S. Sirtuin 1 activation suppresses the growth of T-lymphoblastic leukemia cells by inhibiting NOTCH and NF-kappaB pathways. Anticancer Res. (2020) 40:3155–61. doi: 10.21873/anticanres.14297
28. Bhalla S, Gordon L. Functional characterization of NAD dependent de-acetylases SIRT1 and SIRT2 in B-Cell chronic lymphocytic leukemia (CLL). Cancer Biol Ther. (2016) 17:300–9. doi: 10.1080/15384047.2016.1139246
29. Audrito V, Vaisitti T, Rossi D, Gottardi D, D’Arena G, Laurenti L, et al. Nicotinamide blocks proliferation and induces apoptosis of chronic lymphocytic leukemia cells through activation of the p53/miR-34a/SIRT1 tumor suppressor network. Cancer Res. (2011) 71:4473–83. doi: 10.1158/0008-5472.CAN-10-4452
30. Qian Y, Gong Y, Fan Z, Luo G, Huang Q, Deng S, et al. Molecular alterations and targeted therapy in pancreatic ductal adenocarcinoma. J Hematol Oncol. (2020) 13:130. doi: 10.1186/s13045-020-00958-3
31. Sethi N, Kikuchi O, Duronio G, Stachler M, McFarland J, Ferrer-Luna R, et al. Early TP53 alterations engage environmental exposures to promote gastric premalignancy in an integrative mouse model. Nat Genet. (2020) 52:219–30. doi: 10.1038/s41588-019-0574-9
32. Kohlhaas V, Blakemore S, Al-Maarri M, Nickel N, Pal M, Roth A, et al. Active Akt signaling triggers CLL toward richter transformation via overactivation of Notch1. Blood. (2021) 137:646–60. doi: 10.1182/blood.2020005734
33. Rossi D, Spina V, Gaidano G. Biology and treatment of richter syndrome. Blood. (2018) 131:2761–72. doi: 10.1182/blood-2018-01-791376
34. Chigrinova E, Rinaldi A, Kwee I, Rossi D, Rancoita P, Strefford J, et al. Two main genetic pathways lead to the transformation of chronic lymphocytic leukemia to richter syndrome. Blood. (2013) 122:2673–82. doi: 10.1182/blood-2013-03-489518
35. Poirier S, Samami S, Mamarbachi M, Demers A, Chang T, Vance D, et al. The epigenetic drug 5-azacytidine interferes with cholesterol and lipid metabolism. J Biol Chem. (2014) 289:18736–51. doi: 10.1074/jbc.M114.563650
36. Pandyra A, Mullen P, Kalkat M, Yu R, Pong J, Li Z, et al. Immediate utility of two approved agents to target both the metabolic mevalonate pathway and its restorative feedback loop. Cancer Res. (2014) 74:4772–82. doi: 10.1158/0008-5472.CAN-14-0130
37. Kim Y, Lee Y, Oh T, Shin D, Kim G, Kan S, et al. Emodin sensitizes hepatocellular carcinoma cells to the anti-cancer effect of sorafenib through suppression of cholesterol metabolism. Int J Mol Sci. (2018) 19:3127. doi: 10.3390/ijms19103127
38. Tan Y, Sementino E, Liu Z, Cai K, Testa J. Wnt signaling mediates oncogenic synergy between Akt and Dlx5 in T-cell lymphomagenesis by enhancing cholesterol synthesis. Sci Rep. (2020) 10:15837. doi: 10.1038/s41598-020-72822-w
39. Gonzalez-Rodriguez A, Contesti J, Huergo-Zapico L, Lopez-Soto A, Fernandez-Guizan A, Acebes-Huerta A, et al. Prognostic significance of CD8 and CD4 T cells in chronic lymphocytic leukemia. Leuk Lymphoma. (2010) 51:1829–36. doi: 10.3109/10428194.2010.503820
Keywords: chronic lymphocytic leukemia, gene expression, immune, prognosis, model
Citation: Huang H-y, Wang Y, Herold T, Gale RP, Wang J-z, Li L, Lin H-x and Liang Y (2022) A survival prediction model and nomogram based on immune-related gene expression in chronic lymphocytic leukemia cells. Front. Med. 9:1026812. doi: 10.3389/fmed.2022.1026812
Received: 05 September 2022; Accepted: 28 November 2022;
Published: 19 December 2022.
Edited by:
Yair Herishanu, Tel Aviv Sourasky Medical Center, IsraelReviewed by:
Xin Wang, Shandong Provincial Hospital, ChinaCopyright © 2022 Huang, Wang, Herold, Gale, Wang, Li, Lin and Liang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yang Liang, bGlhbmd5YW5nQHN5c3VjYy5vcmcuY24=; Huan-xin Lin, bGluaHhAc3lzdWNjLm9yZy5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.