
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Med., 07 November 2022
Sec. Geriatric Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1021763
 Kerong Chen1†Liwei Xing2†
Kerong Chen1†Liwei Xing2† Bonan Xu3†
Bonan Xu3† Yi Li1Tianyun Liu1Tingjuan Zhang1Hongping Shi1Hanmei Lu1Wengang Zhou4Jianhong Hou5*Hongling Shi1*Dongdong Qin3*
Yi Li1Tianyun Liu1Tingjuan Zhang1Hongping Shi1Hanmei Lu1Wengang Zhou4Jianhong Hou5*Hongling Shi1*Dongdong Qin3*With the aging of the population, the incidence of dysphagia has gradually increased and become a major clinical and public health issue. Early screening of dysphagia in high-risk populations is crucial to identify the risk factors of dysphagia and carry out effective interventions and health management in advance. In this study, the current epidemiology, hazards, risk factors, preventive, and therapeutic measures of dysphagia were comprehensively reviewed, and a literature review of screening instruments commonly used globally was conducted, focusing on their intended populations, main indicators, descriptions, and characteristics. According to analysis and research in the current study, previous studies of dysphagia were predominantly conducted in inpatients, and there are few investigations and screenings on the incidence and influencing factors of dysphagia in the community-dwelling elderly and of dysphagia developing in the natural aging process. Moreover, there are no unified, simple, economical, practical, safe, and easy-to-administer screening tools and evaluation standards for dysphagia in the elderly. It is imperative to focus on dysphagia in the community-dwelling elderly, develop unified screening and assessment tools, and establish an early warning model of risks and a dietary structure model for dysphagia in the community-dwelling elderly.
Dysphagia is a process in which food is not delivered safely and efficiently into the stomach due to structural and/or functional impairment of the organs such as the jaw, lips, tongue, soft palate, throat, and esophagus (1). Aging, degradation of physiological function, tumor, stroke, and other nervous system diseases, as well as other underlying diseases make the elderly population susceptible to dysphagia (2). Approximately 8% of the global population suffer from swallowing problems (3), and research shows that the lifetime prevalence rate of dysphagia is 17.10% in the community-dwelling elderly, rising to 52.60% in high-risk populations (4).
At present, research on dysphagia in the elderly has predominantly focused on populations with a high incidence of dysphagia such as inpatients and those that have had a stroke, and the subjects are mostly elderly inpatients. There are limited surveys on the incidence of dysphagia in the community-dwelling elderly, and few studies on the influencing factors of dysphagia in the naturally aging, community-dwelling population. Early screening of populations at high risk of dysphagia is crucial to identify the risk factors of dysphagia, and perform effective interventions and health management in advance, which may reduce the incidence of dysphagia, prevent complications, lower medical burdens, and save medical resources. In the current study, a literature review was conducted on the research progress in the risk factors, screening assessment, preventive, and therapeutic measures of dysphagia in the elderly with the aim providing a reference for the screening and research of dysphagia in the elderly.
As a syndrome in the elderly, dysphagia has been listed by the World Health Organization (WHO) in the International Classification of Diseases-10 (ICD-10) and the International Classification of Functioning, Health and Disability (ICF) (5), and is a major public health issue worldwide. In the United States, more than half of people older than 60 years have dysphagia, and 60% of residents of nursing homes have experienced dysphagia (5, 6). Nine percent of residents of nursing homes in the Netherlands (7) and 11.4% of people in British communities complained of symptoms of dysphagia (8). In a geriatric Korean community, 33.7% of the population reported symptoms of dysphagia (9). The prevalence of dysphagia is 5.5–12.9% in the elderly in Chinese communities (10), rising to 31.1% in the institutionalized elderly (11). According to one epidemiological survey of 5,943 patients, 2,341 patients (39.4%) had dysphagia, including 51.14% of stroke patients, 34.4% of patients with head and neck cancer, 48.3% of patients with nervous degenerative diseases, and 19.2% of healthy elderly people (12).
Dysphagia hinders the intake of nutrients required by elderly patients, which leads to serious complications such as weight loss, malnutrition, dehydration, aspiration pneumonia, asphyxia, anxiety, and sociopsychological disorders. These complications directly or indirectly influence the long-term prognosis and quality of life (13), prolong hospital stays, and increase hospital readmissions and the risk of death in elderly patients (14). It was reported that over 60,000 people die each year from complications of dysphagia, of which aspiration pneumonia is the most serious complication and the leading cause of death (15). Dysphagia and its complications and sequelae increase the overall utilization of healthcare services and result in a huge consumption of medical resources. It is estimated that annual costs of dysphagia in the US medical care system are between $4 billion and $7 billion US dollars. Moreover, this estimate does not consider indirect costs, such as the economic impact of a patient’s inability to work due to dysphagia symptoms. In addition to medical costs, there are emotional and mental-health-related costs, which seriously impact the quality of life of patients and simultaneously place a heavy burden on the patient’s family, hospitals, and society (16, 17).
Identifying the risk factors of dysphagia in the elderly is the premise and basis for the identification, assessment, and control of these risks. The main risk factors for dysphagia in the elderly are as follows.
Anatomic and physiological changes in elderly patients are believed to be likely to cause dysphagia (18). The incidence of postoperative dysphagia in patients older than 60 years of age was significantly higher compared with that in patients younger than 60 years, suggesting that age is a risk factor for the development of dysphagia. Another study suggests that although the incidence of diseases that are likely to cause dysphagia, such as stroke, increases with age, the physiological changes, and functional decline that occur in natural aging are associated with the occurrence of dysphagia. With aging, factors such as tooth damage, dull neuroreceptors, decrease in salivary secretion and the elasticity of swallowing organs, and weakening of swallowing muscle strength all increase the risk of dysphagia (3, 19). Thus, even in the absence of underlying diseases, natural aging itself affects swallowing which is supported by the findings of Byeon (4) and Holland et al. (8). Therefore, it is recommended that early screening and assessment of dysphagia is performed to facilitate early intervention in the elderly population older than 60 years.
The prevalence of dysphagia is 27–64% in stroke patients, and approximately 50% in the acute phase (20). The figure is over 80% in patients with Parkinson’s disease (21) and 38% in those with multiple sclerosis (22). While, it is 34.4% in those with head and neck cancer (23). The incidence of dysphagia in patients with ossification of the anterior longitudinal ligament (OALL) in the neck is influenced by the thickness of osteophytes, the range of cervical motion, and craniocervical alignment, and OALL occasionally leads to dysphagia due to the anterior osteophytes (20). Skeletal muscle loss is also thought to be a possible cause of dysphagia (21).
The incidence of dysphagia was reported to be 1–80% following anterior cervical surgery (20, 24). Furthermore, Baron et al. (25–27) found the incidence of transient dysphagia was up to 80% after anterior cervical fusion, and even higher in patients older than 60 years. Dysphagia is one of the most common complications after anterior cervical surgery (28). Severe paralysis and tracheotomy may also be risk factors for dysphagia (29). Oropharyngeal dysphagia (OD) is common in elderly patients with hip fractures and is easily overlooked, predisposing patients to life-threatening postoperative pneumonia. Hip fractures often occur in elderly patients with comorbidities such as stroke or dementia. In addition, the incidence of dysphagia is particularly high in patients with hip fractures due to intraoperative intubation. The prevalence of dysphagia was reported to be 7% in patients with hip fractures but 34% after surgery. These findings suggest that the effects of the disease itself, hospitalization, surgery, and intubation on swallowing function may be temporary, but identification of dysphagia after surgery is necessary to prevent consequences such as pneumonia. These data can help clinicians to manage patients with advanced dysphagia.
Pharmacological factors like opioid and topical steroid (24), psychological factor such as depression (22), as well as mealtime (30), and serum albumin levels (31) are all additional influencing factors of dysphagia.
There are no unified standards of screening and assessment tools for dysphagia in elderly individuals worldwide, and multiple screening and assessment tools for dysphagia have been developed according to individual situations. Screening and assessment tools are reviewed in the current study. Table 1 details the name of the assessment tool, the country and intended populations, main indicators, methods and characteristics.
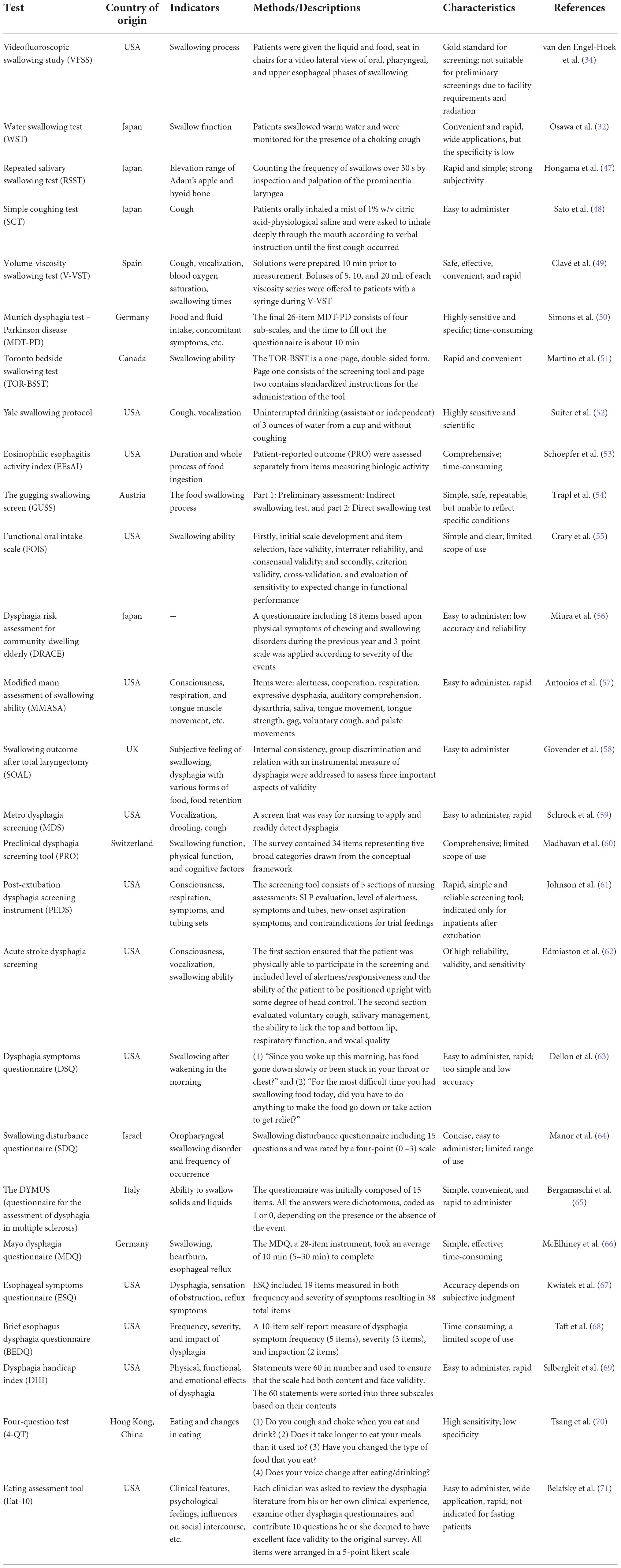
Table 1. Common screening and assessment tools for dysphagia.
In general, there are pros and cons to the various screening tools, and a widely accepted, perfect assessment tool is currently lacking. Munich Dysphagia Test–Parkinson Disease (MDT-PD) includes difficulty in swallowing general food, dysphagia unrelated to food, burden related to dysphagia, and health problems caused by dysphagia. There are 4 major parts, 26 items, and a score of < 3.65 indicates no symptoms of dysphagia. A score of 3.65–4.78 indicates early oropharyngeal dysphagia, and a score of ≥ 4.79 indicates that the patient is at risk of aspiration. In addition, 3-ounce water swallow test, repeated salivary swallowing test, simple swallowing provocation test (S-SPT) and other tests are also applied. The water swallowing test WST (32) is the most classical and most commonly used assessment methods in clinical practice, but the specificity is low, and latent aspirations cannot be effectively predicted for it could only identify the inability of safety concerns when swallowing water in patients with stroke. In addition, the risk of aspiration pneumonia from the use of these methods may adversely affect patient prognosis (33). Videofluoroscopic swallowing study (VFSS) allows real-time visual observation of the swallowing process and qualitative and quantitative analysis, which is regarded as an ideal method and gold standard for diagnosis of dysphagia (34). However, VFSS has drawbacks such as being time-consuming and complicated and causing exposure to radiation, consequently VFSS is unsuitable for early screenings.
In addition, currently available screening instruments for dysphagia are mainly aimed at inpatients with certain diseases or other unique conditions, especially elderly patients, and these tools cannot meet the screening needs of elderly people dwelling in nursing homes and communities.
Due to increased risk of dysphagia in the elderly which is probably the result of complicated risk factors as forementioned, there is clearly a need for preventive and therapeutic measures for dysphagia in the elderly which are individualized according to their specific risk factors.
Prophylactic swallowing exercises can avoid periods of nothing per oral (NPO) which is the commonest preventive measure based on the rule of “use it or lose it” (35). Study has shown that prophylactic exercises may result in maintenance of oral and oropharyngeal musculature, improved swallowing function, and less dysphagia-related aspiration pneumonia (36). Interventions to prevent dysphagia in older adults living in nursing homes included more bedside evaluation, modification of dietary, creating an appropriate environment for swallowing, providing appropriate feeding assistance, appropriate posture or maneuver for swallowing, appropriate rehabilitation program, medication treatment, and stimulation treatment. Among them, modification of dietary was the most frequently used intervention to prevent or reduce aspiration (37). Saliva aspiration prevention like oral anticholinergics, transdermal anticholinergics, intravenous anticholinergics, and salivary gland irradiation, as well as active dysphagia revalidation including bedside swallow exercises, swallow training with electrical stimulation and swallow training with surface electromyographic biofeedback were proven to be effective preventive measures for dysphagia (38).
The primary goal of therapy is an adequate diet without any risk of aspiration, such as utilizing fluid adaptation with thickeners to avoid impaired safety, and postures and maneuvers to compensate biomechanical alterations are also generic protocols (39). Fluid and nutritional adaptation was proven to be therapeutic in older patients with dysphagia by reducing the prevalence of laryngeal vestibule penetrations and tracheobronchial aspirations (40). Due to its unpleasant taste, however, which many patients find problematic to swallow on a daily basis, thus results in low compliance (41). The minimally massive intervention (MMI) was developed to reduce nutritional and respiratory complications in older hospitalized patients with dysphagia (42). The MMI consists of the following steps: (1) dysphagia evaluation with a clinical tool and adaptation of fluids to avoid impaired safety of swallow, (2) nutritional evaluation and a triple adaptation of food with high-calorie, high-protein and high-vitamin to improve patient nutritional status, and (3) oral health and hygiene evaluation and treatment to avoid respiratory pathogen colonization of the oral cavity (43). Preliminary results suggest that the MMI might become a simple and cost-effective strategy to reduce dysphagia complications in the geriatric population with an acute disease admitted to a general hospital (44).
New treatments based on stimulation of sensorial and motor neural pathways promote swallowing function recovery rather than compensating it. Intrapharyngeal or transcutaneous neuromuscular electrical stimulation, as well as chemical or pharmacological stimulation using TRPV1 (transient receptor potential vanilloid 1) agonists like capsaicin and piperine, which heighten sensory stimuli to the afferent pathway of deglutition, are the peripheral stimulation techniques that have got the most attention (45, 46). Because there are few studies and small patient samples, there is minimal scientific evidence for these therapy approaches, but initial findings are intriguing and promising. As a result, therapies for dysphagia in elderly patients are quickly transitioning from compensatory to therapeutic approaches that encourage the restoration of swallow function.
Considering the hazards of dysphagia, screening of dysphagia is crucial for elderly patients. Risk factors including age, illnesses, surgical, and therapeutic factors are the premise and basis for the diagnosis, assessment, and control of dysphagia in the elderly. Screening and assessment tools reported in the last two decades indicated that a widely accepted, perfect assessment tool is yet currently lacking. Some compensatory measures and new treatments based on stimulation of sensorial and motor neural pathways can promote swallowing function recovery. More efforts should be focused on early identification and effective prevention and rehabilitation. Reduced morbidity in elderly populations may be achieved by addressing issues like the most efficient and effective ways to detect malnutrition and dysphagia in high-risk patients and community-dwelling elderly persons.
With the increasing incidence of dysphagia, there is an urgent need to explore barriers and facilitators of different risk factors, screening tools and therapeutic strategies in detail. Limitations still exist throughout the available research including short duration of many interventions, variations in types of participants, differences in the methods used to diagnose dysphagia, poor design, and poor interpretation of results. Many trials that were identified had small sample sizes and lacked the ability to be generalized to a wider population. Dropout rates and lack of true randomization of trials also weaken the available research. To further clarify different risk factors, screening tools and therapeutic strategies underlying dysphagia in the elderly, a need remains for future large-scale multi-center randomized controlled trials, risk prediction model of dysphagia in elderly patients and in-depth mechanism studies, with the aim of minimizing the occurrence of dysphagia in elderly populations.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This study was supported by the National Natural Science Foundation of China (31960178 and 82160923); Applied Basic Research Programs of Science and Technology Commission Foundation of Yunnan Province (2019FA007); Key Laboratory of Traditional Chinese Medicine for Prevention and Treatment of Neuropsychiatric Diseases, Yunnan Provincial Department of Education; Scientific Research Projects for High-level Talents of Yunnan University of Chinese Medicine (2019YZG01); Young Top-Notch Talent in 10,000 Talent Program of Yunnan Province (YNWR-QNBJ-2019-235); National Science and Technology Innovation 2030 Major Program (2021ZD0200900); Yunnan Key Research and Development Program (202103AC100005); and Yunnan Province Fabao Gao Expert Workstation Construction Project (202105AF150037).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Huppertz VAL, Halfens RJG, van Helvoort A, de Groot L, Baijens LWJ, Schols J. Association between oropharyngeal dysphagia and malnutrition in Dutch nursing home residents: results of the national prevalence measurement of quality of care. J Nutr Health Aging. (2018) 22:1246–52. doi: 10.1007/s12603-018-1103-8
2. Blanaø V, Hödl M, Lohrmann C, Amir Y, Eglseer D. Dysphagia and factors associated with malnutrition risk: a 5-year multicentre study. J Adv Nurs. (2019) 75:3566–76. doi: 10.1111/jan.14188
3. Wirth R, Dziewas R, Beck AM, Clavé P, Hamdy S, Heppner HJ, et al. Oropharyngeal dysphagia in older persons – From pathophysiology to adequate intervention: a review and summary of an international expert meeting. Clin Interv Aging. (2016) 11:189–208. doi: 10.2147/cia.S97481
4. Byeon H. Analysis of dysphagia risk using the modified dysphagia risk assessment for the community-dwelling elderly. J Phys Ther Sci. (2016) 28:2507–9. doi: 10.1589/jpts.28.2507
5. Baijens LW, Clavé P, Cras P, Ekberg O, Forster A, Kolb GF, et al. European Society for Swallowing Disorders – European Union Geriatric Medicine Society white paper: oropharyngeal dysphagia as a geriatric syndrome. Clin Interv Aging. (2016) 11:1403–28. doi: 10.2147/cia.S107750
6. Johnston BT. Oesophageal dysphagia: a stepwise approach to diagnosis and management. Lancet Gastroenterol Hepatol. (2017) 2:604–9. doi: 10.1016/s2468-125330001-8
7. van der Maarel-Wierink CD, Meijers JM, De Visschere LM, de Baat C, Halfens RJ, Schols JM. Subjective dysphagia in older care home residents: a cross-sectional, multi-centre point prevalence measurement. Int J Nurs Stud. (2014) 51:875–81. doi: 10.1016/j.ijnurstu.2013.10.016
8. Holland G, Jayasekeran V, Pendleton N, Horan M, Jones M, Hamdy S. Prevalence and symptom profiling of oropharyngeal dysphagia in a community dwelling of an elderly population: a self-reporting questionnaire survey. Dis Esophagus. (2011) 24:476–80. doi: 10.1111/j.1442-2050.2011.01182.x
9. Yang EJ, Kim MH, Lim JY, Paik NJ. Oropharyngeal dysphagia in a community-based elderly cohort: the Korean longitudinal study on health and aging. J Kor Med Sci. (2013) 28:1534–9. doi: 10.3346/jkms.2013.28.10.1534
10. Zhang H, Guo F, Tang M, Dai H, Sheng J, Chen L, et al. Association between skeletal muscle strength and dysphagia among Chinese community-dwelling elderly adults. J Nutr Health Aging. (2020) 24:642–9. doi: 10.1007/s12603-020-1379-3
11. Chen S, Cui Y, Ding Y, Sun C, Xing Y, Zhou R, et al. Prevalence and risk factors of dysphagia among nursing home residents in Eastern China: a cross-sectional study. BMC Geriatr. (2020) 20:352. doi: 10.1186/s12877-020-01752-z
12. Zhang M, Li C, Zhang F, Han X, Yang Q, Lin T, et al. Prevalence of dysphagia in China: an epidemiological survey of 5943 participants. Dysphagia. (2021) 36:339–50. doi: 10.1007/s00455-020-10138-7
13. McCarty EB, Chao TN. Dysphagia and swallowing disorders. Med Clin North Am. (2021) 105:939–54. doi: 10.1016/j.mcna.2021.05.013
14. Maeshima S, Osawa A, Miyazaki Y, Seki Y, Miura C, Tazawa Y, et al. Influence of dysphagia on short-term outcome in patients with acute stroke. Am J Phys Med Rehabil. (2011) 90:316–20. doi: 10.1097/PHM.0b013e31820b13b2
15. ASHA. Adult Dysphagia. (Practiceportal). (2020). Available online at: www.asha.org/Practice-Portal/Clinical-Topics/Adult-Dysphagia/ (accessed Nov 10, 2020).
16. Attrill S, White S, Murray J, Hammond S, Doeltgen S. Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: a systematic review. BMC Health Serv Res. (2018) 18:594.
17. Patel DA, Krishnaswami S, Steger E, Conover E, Vaezi MF, Ciucci MR, et al. Economic and survival burden of dysphagia among inpatients in the United States. Dis Esophagus. (2018) 31:1–7. doi: 10.1093/dote/dox131
18. Li Z, Li G, Chen C, Li Y, Yang C, Xu W, et al. Risk factors for dysphagia after anterior cervical spine surgery. Orthopedics. (2018) 41:e110–6.
19. González-Fernández M, Humbert I, Winegrad H, Cappola AR, Fried LP. Dysphagia in old-old women: prevalence as determined according to self-report and the 3-ounce water swallowing test. J Am Geriatr Soc. (2014) 62:716–20. doi: 10.1111/jgs.12745
20. Nishimura H, Endo K, Aihara T, Murata K, Suzuki H, Matsuoka Y, et al. Risk factors of dysphagia in patients with ossification of the anterior longitudinal ligament. J Orthopaed Surg. (2020) 28:2309499020960564. doi: 10.1177/2309499020960564
21. Cha S, Kim WS, Kim KW, Han JW, Jang HC, Lim S, et al. Sarcopenia is an independent risk factor for dysphagia in community-dwelling older adults. Dysphagia. (2019) 34:692–7. doi: 10.1007/s00455-018-09973-6
22. Lee YH, Jung D, Yun OJ, Lee H, Lee M. Risk factors of dysphagia among community-dwelling middle-aged women: focused on oropharyngeal phase. Gastroenterol Nurs. (2020) 43:164–71. doi: 10.1097/sga.0000000000000419
23. Jiang N, Zhang LJ, Li LY, Zhao Y, Eisele DW. Risk factors for late dysphagia after (chemo)radiotherapy for head and neck cancer: a systematic methodological review. Head Neck. (2016) 38:792–800. doi: 10.1002/hed.23963
24. Okano I, Salzmann SN, Ortiz Miller C, Hoshino Y, Oezel L, Shue J, et al. Risk factors for postoperative dysphagia and dysphonia following anterior cervical spine surgery: a comprehensive study utilizing the hospital for special surgery dysphagia and dysphonia inventory (Hss-Ddi). Spine J. (2021) 21:1080–8. doi: 10.1016/j.spinee.2021.02.011
25. Vanek P, Bradac O, DeLacy P, Saur K, Belsan T, Benes V. Comparison of 3 fusion techniques in the treatment of the degenerative cervical spine disease. Is stand-alone autograft really the “gold standard?”: prospective study with 2-year follow-up. Spine. (2012) 37:1645–51. doi: 10.1097/BRS.0b013e31825413fe
26. Jacobs W, Willems PC, Kruyt M, van Limbeek J, Anderson PG, Pavlov P, et al. Systematic review of anterior interbody fusion techniques for single- and double-level cervical degenerative disc disease. Spine. (2011) 36:E950–60. doi: 10.1097/BRS.0b013e31821cbba5
27. McAfee PC, Cappuccino A, Cunningham BW, Devine JG, Phillips FM, Regan JJ, et al. Lower incidence of dysphagia with cervical arthroplasty compared with ACDF in a prospective randomized clinical trial. J Spinal Disord Tech. (2010) 23:1–8. doi: 10.1097/BSD.0b013e31819e2ab8
28. Anderson KK, Arnold PM. Oropharyngeal dysphagia after anterior cervical spine surgery: a review. Glob Spine J. (2013) 3:273–86. doi: 10.1055/s-0033-1354253
29. Hayashi T, Fujiwara Y, Sakai H, Maeda T, Ueta T, Shiba K. Risk factors for severe dysphagia in acute cervical spinal cord injury. Spinal Cord. (2017) 55:940–3. doi: 10.1038/sc.2017.63
30. Namasivayam-Macdonald AM, Steele CM, Carrier N, Lengyel C, Keller HH. The relationship between texture-modified diets, mealtime duration, and dysphagia risk in long-term care. Can J Diet Pract Res. (2019) 80:122–6. doi: 10.3148/cjdpr-2019-004
31. Byun SE, Kwon KB, Kim SH, Lim SJ. The prevalence, risk factors and prognostic implications of dysphagia in elderly patients undergoing hip fracture surgery in Korea. BMC Geriatr. (2019) 19:356. doi: 10.1186/s12877-019-1382-x
32. Osawa A, Maeshima S, Tanahashi N. Water-swallowing test: screening for aspiration in stroke patients. Cerebrovasc Dis. (2013) 35:276–81. doi: 10.1159/000348683
33. Kertscher B, Speyer R, Palmieri M, Plant C. Bedside screening to detect oropharyngeal dysphagia in patients with neurological disorders: an updated systematic review. Dysphagia. (2014) 29:204–12. doi: 10.1007/s00455-013-9490-9
34. van den Engel-Hoek L, Erasmus CE, van Hulst KC, Arvedson JC, de Groot IJ, de Swart BJ. Children with central and peripheral neurologic disorders have distinguishable patterns of dysphagia on videofluoroscopic swallow study. J Child Neurol. (2014) 29:646–53. doi: 10.1177/0883073813501871
35. Hutcheson KA, Lewin JS. Functional outcomes after chemoradiotherapy of laryngeal and pharyngeal cancers. Curr Oncol Rep. (2012) 14:158–65. doi: 10.1007/s11912-012-0216-1
36. Carnaby-Mann G, Crary MA, Schmalfuss I, Amdur R. “Pharyngocise”: randomized controlled trial of preventative exercises to maintain muscle structure and swallowing function during head-and-neck chemoradiotherapy. Int J Radiat Oncol Biol Phys. (2012) 83:210–9. doi: 10.1016/j.ijrobp.2011.06.1954
37. Chen S, Kent B, Cui Y. Interventions to prevent aspiration in older adults with dysphagia living in nursing homes: a scoping review. BMC Geriatr. (2021) 21:429. doi: 10.1186/s12877-021-02366-9
38. van Snippenburg W, Kröner A, Flim M, Hofhuis J, Buise M, Hemler R, et al. Awareness and management of dysphagia in dutch intensive care units: a nationwide survey. Dysphagia. (2019) 34:220–8. doi: 10.1007/s00455-018-9930-7
39. Ortega O, Martín A, Clavé P. Diagnosis and management of oropharyngeal dysphagia among older persons, state of the art. J Am Med Dir Assoc. (2017) 18:576–82. doi: 10.1016/j.jamda.2017.02.015
40. Rofes L, Arreola V, Romea M, Palomera E, Almirall J, Cabré M, et al. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol Motil. (2010) 22:851–8, e230. doi: 10.1111/j.1365-2982.2010.01521.x
41. Rosenvinge SK, Starke ID. Improving care for patients with dysphagia. Age Ageing. (2005) 34:587–93. doi: 10.1093/ageing/afi187
42. Martin R, Barr A, MacIntosh B, Smith R, Stevens T, Taves D, et al. Cerebral cortical processing of swallowing in older adults. Exp Brain Res. (2007) 176:12–22. doi: 10.1007/s00221-006-0592-6
43. Warnecke T, Dziewas R, Wirth R, Bauer JM, Prell T. Dysphagia from a neurogeriatric point of view : pathogenesis, diagnosis and management. Z Gerontol Geriatr. (2019) 52:330–5. doi: 10.1007/s00391-019-01563-x
44. Ortega O, Sakwinska O, Combremont S, Berger B, Sauser J, Parra C, et al. High prevalence of colonization of oral cavity by respiratory pathogens in frail older patients with oropharyngeal dysphagia. Neurogastroenterol Motil. (2015) 27:1804–16. doi: 10.1111/nmo.12690
45. Rofes L, Arreola V, Martin A, Clavé P. Effect of oral piperine on the swallow response of patients with oropharyngeal dysphagia. J Gastroenterol. (2014) 49:1517–23. doi: 10.1007/s00535-013-0920-0
46. Rofes L, Arreola V, Martin A, Clavé P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut. (2013) 62:1280–7. doi: 10.1136/gutjnl-2011-300753
47. Hongama S, Nagao K, Toko S, Tanida K, Akutagawa M, Kinouchi Y, et al. MI sensor-aided screening system for assessing swallowing dysfunction: application to the repetitive saliva-swallowing test. J Prosthodont Res. (2012) 56:53–7.
48. Sato M, Tohara H, Iida T, Wada S, Inoue M, Ueda K. Simplified cough test for screening silent aspiration. Arch Phys Med Rehabil. (2012) 93:1982–6.
49. Clavé P, Arreola V, Romea M, Medina L, Palomera E, Serra-Prat M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin Nutr. (2008) 27:806–15. doi: 10.1016/j.clnu.2008.06.011
50. Simons JA, Fietzek UM, Waldmann A, Warnecke T, Schuster T, Ceballos-Baumann AO. Development and validation of a new screening questionnaire for dysphagia in early stages of Parkinson’s disease. Parkinsonism Relat Disord. (2014) 20:992–8. doi: 10.1016/j.parkreldis.2014.06.008
51. Martino R, Silver F, Teasell R, Bayley M, Nicholson G, Streiner DL, et al. The Toronto Bedside Swallowing Screening Test (TOR-BSST): development and validation of a dysphagia screening tool for patients with stroke. Stroke. (2009) 40:555–61. doi: 10.1161/strokeaha.107.510370
52. Suiter DM, Sloggy J, Leder SB. Validation of the yale swallow protocol: a prospective double-blinded videofluoroscopic study. Dysphagia. (2014) 29:199–203. doi: 10.1007/s00455-013-9488-3
53. Schoepfer AM, Straumann A, Panczak R, Coslovsky M, Kuehni CE, Maurer E, et al. Development and validation of a symptom-based activity index for adults with eosinophilic esophagitis. Gastroenterology. (2014) 147:1255–66.e21. doi: 10.1053/j.gastro.2014.08.028
54. Trapl M, Enderle P, Nowotny M, Teuschl Y, Matz K, Dachenhausen A, et al. Dysphagia bedside screening for acute-stroke patients: the Gugging Swallowing Screen. Stroke. (2007) 38:2948–52. doi: 10.1161/strokeaha.107.483933
55. Crary MA, Mann GD, Groher ME. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch Phys Med Rehabil. (2005) 86:1516–20. doi: 10.1016/j.apmr.2004.11.049
56. Miura H, Kariyasu M, Yamasaki K, Arai Y. Evaluation of chewing and swallowing disorders among frail community-dwelling elderly individuals. J Oral Rehabil. (2007) 34:422–7. doi: 10.1111/j.1365-2842.2007.01741.x
57. Antonios N, Carnaby-Mann G, Crary M, Miller L, Hubbard H, Hood K, et al. Analysis of a physician tool for evaluating dysphagia on an inpatient stroke unit: the modified mann assessment of swallowing ability. J Stroke Cerebrovasc Dis. (2010) 19:49–57. doi: 10.1016/j.jstrokecerebrovasdis.2009.03.007
58. Govender R, Lee MT, Davies TC, Twinn CE, Katsoulis KL, Payten CL, et al. Development and preliminary validation of a patient-reported outcome measure for swallowing after total laryngectomy (SOAL questionnaire). Clin Otolaryngol. (2012) 37:452–9. doi: 10.1111/coa.12036
59. Schrock JW, Bernstein J, Glasenapp M, Drogell K, Hanna J. A novel emergency department dysphagia screen for patients presenting with acute stroke. Acad Emerg Med. (2011) 18:584–9. doi: 10.1111/j.1553-2712.2011.01087.x
60. Madhavan A, Carnaby GD, Chhabria K, Crary MA. Preliminary development of a screening tool for pre-clinical dysphagia in community dwelling older adults. Geriatrics. (2018) 3:90. doi: 10.3390/geriatrics3040090
61. Johnson KL, Speirs L, Mitchell A, Przybyl H, Anderson D, Manos B, et al. Validation of a postextubation dysphagia screening tool for patients after prolonged endotracheal intubation. Am J Crit Care. (2018) 27:89–96. doi: 10.4037/ajcc2018483
62. Edmiaston J, Connor LT, Loehr L, Nassief A. Validation of a dysphagia screening tool in acute stroke patients. Am J Crit Care. (2010) 19:357–64. doi: 10.4037/ajcc2009961
63. Dellon ES, Irani AM, Hill MR, Hirano I. Development and field testing of a novel patient-reported outcome measure of dysphagia in patients with eosinophilic esophagitis. Aliment Pharmacol Therap. (2013) 38:634–42. doi: 10.1111/apt.12413
64. Manor Y, Giladi N, Cohen A, Fliss DM, Cohen JT. Validation of a swallowing disturbance questionnaire for detecting dysphagia in patients with Parkinson’s disease. Mov Disord. (2007) 22:1917–21. doi: 10.1002/mds.21625
65. Bergamaschi R, Crivelli P, Rezzani C, Patti F, Solaro C, Rossi P, et al. The Dymus questionnaire for the assessment of dysphagia in multiple sclerosis. J Neurol Sci. (2008) 269:49–53. doi: 10.1016/j.jns.2007.12.021
66. McElhiney J, Lohse MR, Arora AS, Peloquin JM, Geno DM, Kuntz MM, et al. The Mayo Dysphagia questionnaire-30: documentation of reliability and validity of a tool for interventional trials in adults with esophageal disease. Dysphagia. (2010) 25:221–30. doi: 10.1007/s00455-009-9246-8
67. Kwiatek MA, Kiebles JL, Taft TH, Pandolfino JE, Bové MJ, Kahrilas PJ, et al. Esophageal symptoms questionnaire for the assessment of dysphagia, globus, and reflux symptoms: initial development and validation. Dis Esophagus. (2011) 24:550–9. doi: 10.1111/j.1442-2050.2011.01202.x
68. Taft TH, Riehl M, Sodikoff JB, Kahrilas PJ, Keefer L, Doerfler B, et al. Development and validation of the brief esophageal dysphagia questionnaire. Neurogastroenterol Motil. (2016) 28:1854–60. doi: 10.1111/nmo.12889
69. Silbergleit AK, Schultz L, Jacobson BH, Beardsley T, Johnson AF. The dysphagia handicap index: development and validation. Dysphagia. (2012) 27:46–52. doi: 10.1007/s00455-011-9336-2
70. Tsang K, Lau ES, Shazra M, Eyres R, Hansjee D, Smithard DG. A new simple screening tool-4qt: can it identify those with swallowing problems? A pilot study. Geriatrics. (2020) 5:11. doi: 10.3390/geriatrics5010011
Keywords: community-dwelling elderly, dysphagia, screening tool, preventive and therapeutic measures, research progress
Citation: Chen K, Xing L, Xu B, Li Y, Liu T, Zhang T, Shi H, Lu H, Zhou W, Hou J, Shi H and Qin D (2022) Research progress in the risk factors and screening assessment of dysphagia in the elderly. Front. Med. 9:1021763. doi: 10.3389/fmed.2022.1021763
Received: 21 August 2022; Accepted: 21 October 2022;
Published: 07 November 2022.
Edited by:
Esther-Lee Marcus, Herzog Hospital, IsraelReviewed by:
Edvard Ehler, Eldis Pardubice, CzechiaCopyright © 2022 Chen, Xing, Xu, Li, Liu, Zhang, Shi, Lu, Zhou, Hou, Shi and Qin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dongdong Qin, cWluZG9uZzEwOEAxNjMuY29t; Jianhong Hou, aGpoanl5QDEyNi5jb20=; Hongling Shi, a21zaGwxQDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.