 Francisco José Molina1,2*
Francisco José Molina1,2* Luz Elena Botero1
Luz Elena Botero1 Juan Pablo Isaza1
Juan Pablo Isaza1 Luz Elena Cano1,3
Luz Elena Cano1,3 Lucelly López1
Lucelly López1 Lina Marcela Hoyos1Elizabeth Correa1,3
Lina Marcela Hoyos1Elizabeth Correa1,3 Antoni Torres4,5
Antoni Torres4,5- 1Facultad de Medicina, Escuela de Ciencias de la Salud, Universidad Pontificia Bolivariana, Medellín, Colombia
- 2Intensive Care Unit, Clínica Universitaria Bolivariana, Universidad Pontificia Bolivariana, Medellín, Colombia
- 3Corporación para Investigaciones Biológicas, Medellín, Colombia
- 4Department of Pulmonology, University of Barcelona, Barcelona, Spain
- 5Respiratory and Intensive Care Unit, Hospital Clinic of Barcelona, Barcelona, Spain
Background: High levels of different cytokines have been associated in COVID-19 as predictors of mortality; however, not all studies have found this association and its role to cause multi-organ failure and death has not been fully defined. This study aimed to investigate the association of the levels of 10 cytokines with mortality in patients with COVID-19 admitted to the intensive care unit (ICU).
Materials and methods: This is a case-control study nested within a cohort of patients with COVID-19 who were on mechanical ventilation and were not hospitalized for more than 48 h across nine ICUs in Medellín, Colombia. Serum samples were collected upon admission to the ICU and 7 days later and used to measure cytokine levels.
Results: Upon admission, no differences in mortality between the cytokine levels were observed when comparisons were made quantitatively. However, in the multivariate analysis, patients with median IL-1β levels <1.365 pg/ml showed an increase in mortality (OR = 3.1; 1.24<7.71; p = 0.015). On day 7 in the ICU, IL-1β median levels were lower (0.34 vs. 2.41 pg/ml, p = 0.042) and IL-10 higher (2.08 vs. 1.05 pg/ml, p = 0.009) in patients who died. However, in the multivariate analysis, only IL-12p70 was associated with mortality (OR = 0.23; 0.07<0.73; p = 0.012). The mean difference in the levels between day 1 and day 7 decreased in both IFN-γ (3.939 pg/ml, p < 0.039) and in IL-18 (16.312 pg/ml, p < 0.014) in the patients who died. A low IL-1β/IL-10 ratio was associated with mortality on both day 1 and day 7, while an IL-1β/IL-10 ratio below the cut-off on day 7 was associated with decreased survival. The lowest TNFα/IL-10 ratio was associated with mortality only on day 7.
Conclusion: At the time of admission, patients with median IL-1β levels lower than 1.365 pg/ml had increased mortality. An IL-1β/IL-10 ratio <2 at day 7 and IL-12p70 levels >1.666 pg/ml was associated with decreased survival.
Introduction
The coronavirus disease 2019 (COVID-19/SARS-CoV-2) pandemic has resulted in high rates of mortality (43% [95% CI: 0.29<0.58]) in patients with invasive mechanical ventilation (IMV) in intensive care units (ICUs) (1). The global UNITE-COVID study found that older age, IMV, and acute kidney injury (AKI) were the strongest predictors of mortality (2). The “cytokine storm” (CS) is characterized in severe COVID-19 by systemic inflammation with increased ferritin, D-dimers, C-reactive protein (CRP), and cytokines such as tumor necrosis factor-alpha (TNFα), interleukin 1 beta (IL-1β), interleukin-6 (IL-6), interferon-gamma (IFN-γ), and interleukin 18 (IL-18), that leads to multi-organ failure (3).
Ruan et al. found that ± 45% (68/150) of patients hospitalized in two centers in Wuhan, China, for infection of SARS-CoV-2, had died, and had higher levels of IL-6 (4). Fernandez-Botran et al. reported that high levels of IL-6 in hospitalized patients with COVID-19 were associated with the need for ICU admission, and the use of vasopressors (5). Milenkovic et al. in a retrospective cohort study of 318 patients admitted to an ICU in Belgrade, Serbia discovered that IL-6 ≥74.98 pg/ml was a predictor of mortality (6). Sancho Ferrando et al. in 122 patients with COVID-19 at ICU admission, found that the levels of TNFα receptors in their soluble form (sTNFR) 1 and 2 were higher in those who developed acute kidney injury (AKI) and in those who did not survive 30 days (7). McElvaney et al. reported that patients admitted to the ICU had higher values of IL-1β, IL-6, IL-8, and IL-10 (8).
However, Kox et al. described that plasma concentrations of tumor necrosis factor (TNF), IL-6, and IL-8 taken in the first 24 h of ICU admission were lower in patients with acute respiratory distress syndrome (ARDS) in IMV with COVID-19 than in patients with septic shock with or without ARDS and comparable to patients with out-of-hospital cardiac arrest and multiple traumas (9). Bülow Anderberg et al. showed a strong correlation at the time of admission to ICU between the lowest PaO2/FiO2 ratio and increased levels of IL-1Ra, IL-4, IL-6, and IL-8 in 24 adults with COVID-19. There was also a strong correlation of several biomarkers such as IL-4, IL-6, IL-8, IL-10 and TNFα with acute kidney injury; however, cytokines were weakly correlated with mortality except for IL-8 (10).
Li et al. in a study conducted in 40 patients hospitalized in an ICU in Wuhan, China, described how the kinetic variations in IL-6, IL-8, and IL-10 levels were associated with mortality (11). Tong-Minh et al. reported that an increase in procalcitonin (PCT), IL-6, and soluble urokinase-type plasminogen activator receptor (suPAR) in a subsequent day of ICU stay were predictors of in-hospital mortality (12). The dynamics of cytokine release during severe COVID-19 remain unknown. Moreover, whether a CS in severe COVID-19 is the most apt description of the pathogenesis remains to be determined.
We therefore focus on the critically ill patient where the levels of separate cytokines may give only a partial view of a complex and interrelated inflammatory process in the patient with COVID-19. We hypothesized that the plasma levels of cytokines are elevated like other inflammatory mediators in severe SARS-CoV-2 infection and could serve as a biomarker of multi-organ failure and death. This study aimed to characterize the association of 10 cytokine levels with mortality in patients with COVID-19 admitted to ICU with respiratory failure in IMV of samples taken on days 1 and 7 of ICU. Moreover, we sought to determine whether differences in the blood concentrations of cytokines on days 1 and 7 were associated with mortality.
Materials and methods
Study setting
This is a case-control study nested within a cohort of 149 patients included in the original study (13). The patients were >18 years of age with confirmed COVID-19 admitted at nine ICUs in Medellín, Colombia. All patients were on mechanical ventilation and could not have been hospitalized for more than 48 h at the time of ICU admission. The study was conducted between March 1 and July 30, 2021. Of the 149 patients, 39 died, and they were matched with 41 surviving patients to obtain an almost 1:1 ratio by Acute Physiology and Chronic Health disease Classification System (APACHE). The total sample size was 80 patients (Figure 1). Clinical data was retrieved from their electronic medical records. Sequential Organ Failure Assessment (SOFA) score (14), and APACHE II (15) data were collected upon ICU admission. Moreover, blood samples were collected on the day 1 of ICU for routine chemistry. Laboratory tests included white blood cell count (WBC), CRP, ferritin, procalcitonin, D-dimer, creatinine, troponin and ferritin.
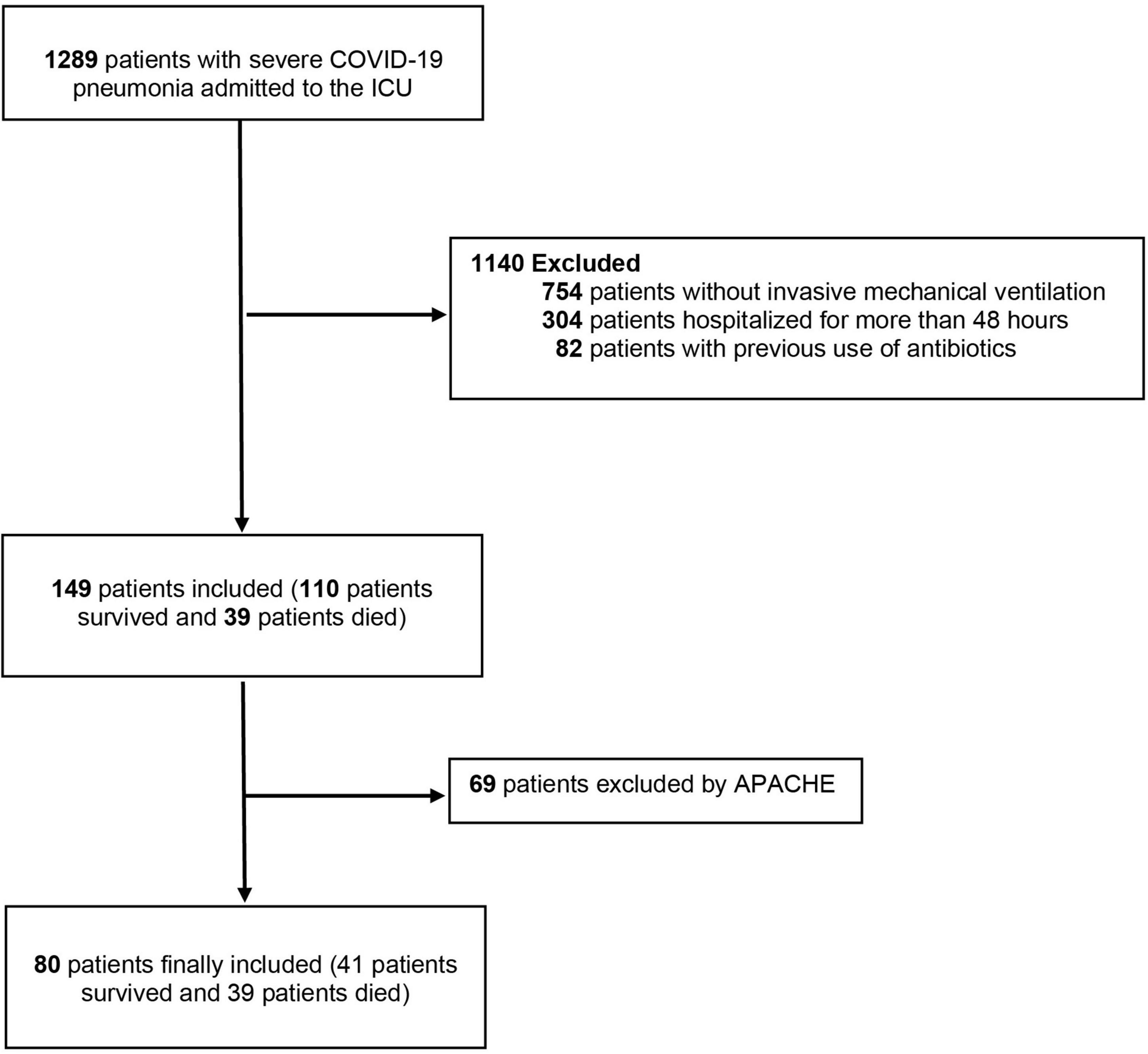
Figure 1. Study flowchart. ICU, intensive care unit; APACHE, Acute Physiology and Chronic Health disease.
COVID-19
The diagnosis of SARS-CoV-2 was confirmed using real-time PCR (RT-PCR) on samples obtained from nasopharyngeal swabs, in an Allplex assay (Seegene, Inc., Seoul, South Korea) to amplify SARS-CoV-2 E, RdRp/s, and N genes.
Cytokine measurements
Venous blood samples were collected upon admission to the ICU and 7 days later, in order to measure cytokine levels. Cytokines were measured at day 7 to determine their predictive value for mortality after the first week of hospitalization in those who were alive. In addition, to measure the dynamic changes with the same time difference, between days 1 and 7, in the mean difference of the serum levels of each cytokine, and its predictive value with mortality. This could generate hypotheses for possible treatments before the fatal outcome occurs.
Serum was obtained from each blood sample by centrifugation for 10 min at 2,000 RPM. Subsequently, each serum sample was stored in cryovials at –80°C until processing. This process was carried out in the BSL2 Research Laboratory of the Faculty of Medicine of the Universidad Pontificia Bolivariana (Medellín, Colombia). For this investigation, a system Human ProcartaPlex TM Multiplex Immunoassay Mix & Match of 10-Plex based on magnetic beads was selected to detect serum biomarkers Ref. PPX-10-MX323G4 (Invitrogen, Whatman, Massachusetts, United States). These analytes included interleukin 1 beta (IL-1β), IL-2, IL-6, IL-10, IL-12p70, IL-17A, interferon-gamma (IFN-γ), recombinant human granulocyte-macrophage colony-stimulating factor (GM-CSF), tumor necrosis factor-alpha (TNFα), and IL-18. Undiluted samples were processed following the manufacturer’ instructions. The 10 cytokines were analyzed using the Luminex® MAGPIX® System (ThermoFisher Scientific, Luminex Corporation 12212 Technology Blvd. Austin, Texas 78727). All samples and standards were measured in duplicate. Primary data were analysed using Xponet ® Software (Luminex, Austin, Texas, United States). This process was done in the Medical and Experimental Micology Laboratory of the Corporación para Investigaciones Biológicas (Medellín, Colombia).
Ethical approval
This study was approved by the ethics committee of the Universidad Pontificia Bolivariana and by the committees of the Clinics and Hospitals that participated in the study. Written informed consent was obtained from the participants or their legal representatives.
Statistical analysis
Continuous variables were presented as medians and 25th and 75th percentiles or mean and standard deviation (SD) depending on the distribution of the variables. Categorical variables were presented as frequencies and percentages. In the comparison of cytokines with mortality and other dichotomous variables, the Mann–Whitney U test was used. To compare the laboratory parameters, APACHE II, and SOFA, Spearman’s correlation coefficient was used. The change in the difference of serum levels of cytokines between days 1 and 7 with mortality was estimated. We calculated crude and adjusted odds ratios (OR)s with their confidence intervals (CI). Multivariate analysis was performed in a logistic regression model with the cytokines after being dichotomized, taking as cut-off points the medians with a statistical significance of <0.25. To evaluate the pro-inflammatory vs. anti-inflammatory activity, the following ratios were calculated: TNFα/IL-10, and IL-1β/IL-10 (16). Data were analyzed using SPSS version 26.0 and visualized using the ggplot2 and reshape2 libraries.
Results
Patient characteristics and cytokine concentrations
The demographic characteristics of the study patients are shown in Table 1. There was higher mortality in men, older age and with a history of hypertension. Table 2 lists the cytokine levels of the 80 patients on the first day of admission, and on day 7 of the 75 patients who were alive. The GM-CSF cytokine did not show any changes after 7 days and was therefore excluded from subsequent analyses.
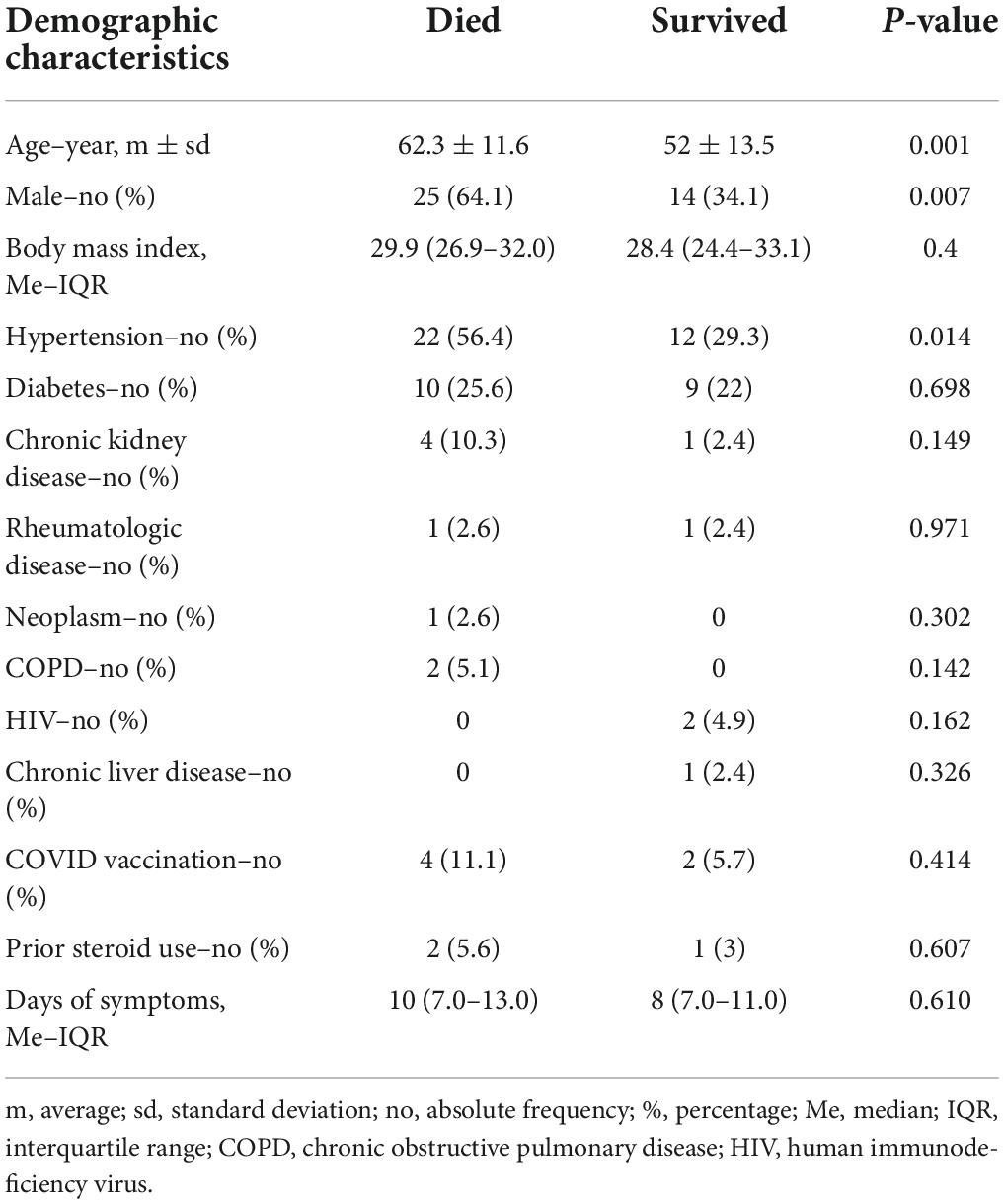
Table 1. Demographic characteristics of patients with COVID-19 pneumonia admitted to intensive care units.
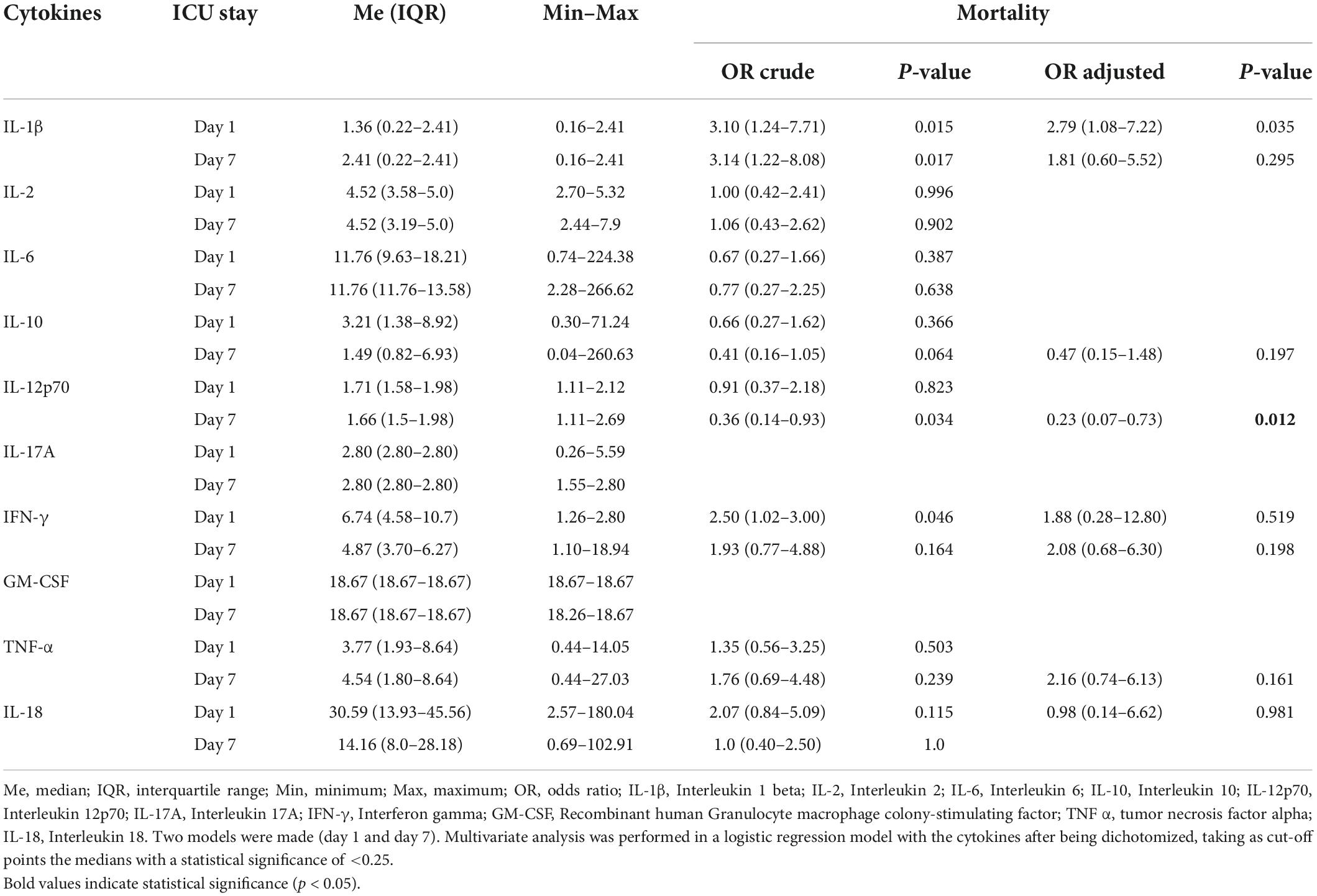
Table 2. Levels of the 10 cytokines and association with mortality on days 1 and 7 of ICU stay.
When comparing the cytokine levels quantitatively, there were no differences between live and dead patients on day 1 (Figure 2). However, when dichotomizing the cytokines according to their median values, we found that IL-1β was associated with mortality, with an OR of 3.1 (1.24<7.71, p = 0.015). When performing a multivariate analysis with the cytokines after being dichotomized, the IL-1β cytokine continued with a statistical association, with an OR of 2.79 (1.08<7.22, p = 0.035), when the median levels were lower than 1.365 pg/ml (Table 2).
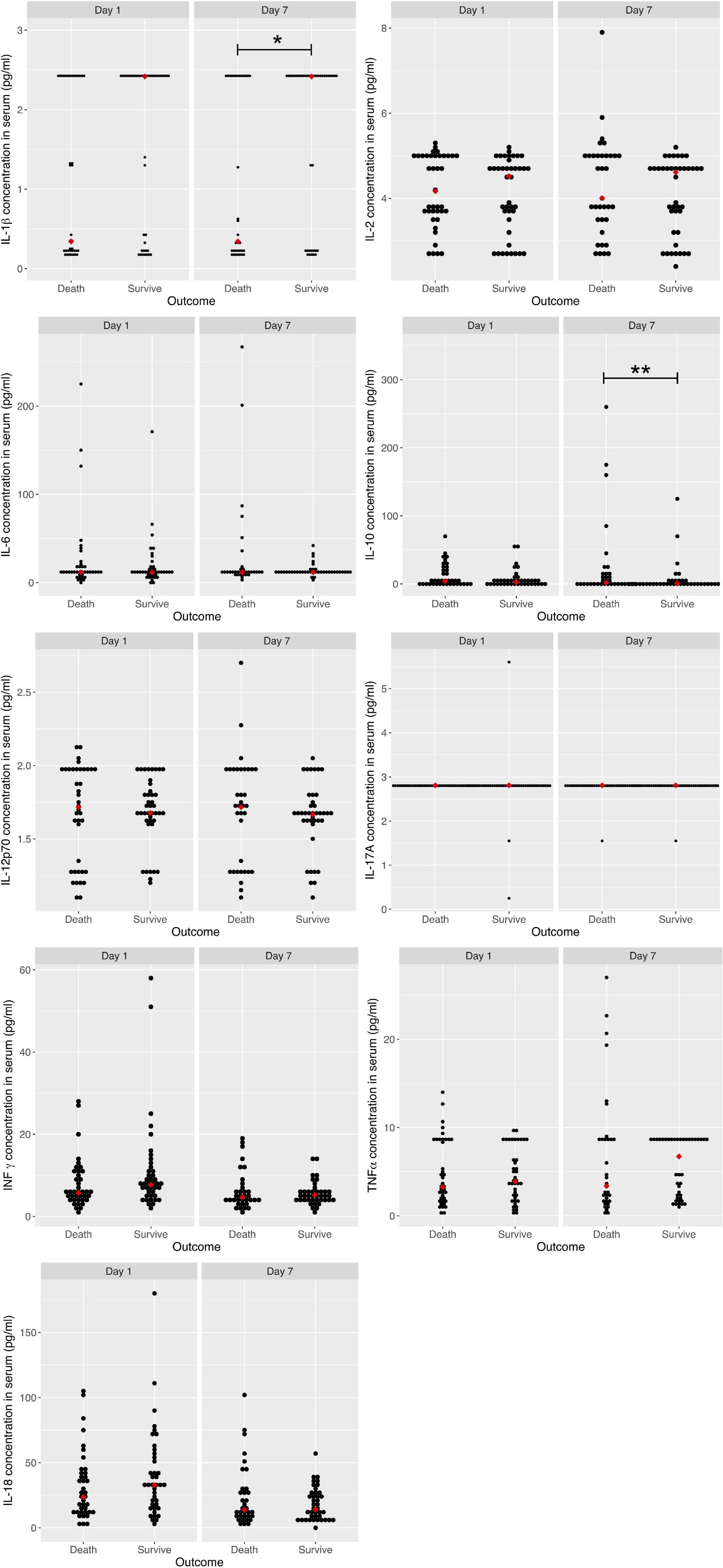
Figure 2. Serum cytokine levels on days 1 and 7 between COVID-19 patients who died and survived. IL-1β, Interleukin 1 beta; IL-2, Interleukin 2; IL-6, Interleukin 6; IL-10, Interleukin 10; IL-12p70, Interleukin 12p70; IL-17A, Interleukin 17A; IFN-γ, Interferon gamma; TNF α, tumor necrosis factor alpha; IL-18, Interleukin 18. *p-value < 0.05 for IL 1 β in serum cytokine concentrations on day 7 between who died and survived; **p-value < 0.01 for IL-10 in serum cytokine concentrations on day 7 between who died and survived.
To determine the predictive value of mortality after the first week of hospitalization, we compared quantitative cytokine levels on day 7 of the patients who survived. Only IL-1β and IL-10 were associated with hospital mortality. The level of IL-1β was lower (0.34 vs. 2.41 pg/ml, p = 0.042) and that of IL-10 higher in patients who died (2.08 vs. 1.05 pg/ml, p = 0.009; Figure 2). When dichotomizing the cytokines according to their median values, we found that IL-1β was associated with mortality, with an OR of 3.14 (1.22<8.08, p = 0.017), and IL-12p70, with an OR of 0.36 (0.14<0.93, p = 0.034). When performing a multivariate analysis with the cytokines after being dichotomized, IL-12p70 continued with a statistical association, with an OR of 0.23 (0.07<0.73, p = 0.012), when median levels were higher than 1.666 pg/ml (Table 2).
Taking the change in the mean difference between the serum levels of each cytokine between days 1 and 7, we found decreases in both IFN-γ (3.939 pg/ml, p < 0.039) and IL-18 (16.312 pg/ml, p < 0.014), in patients who died (Table 3).
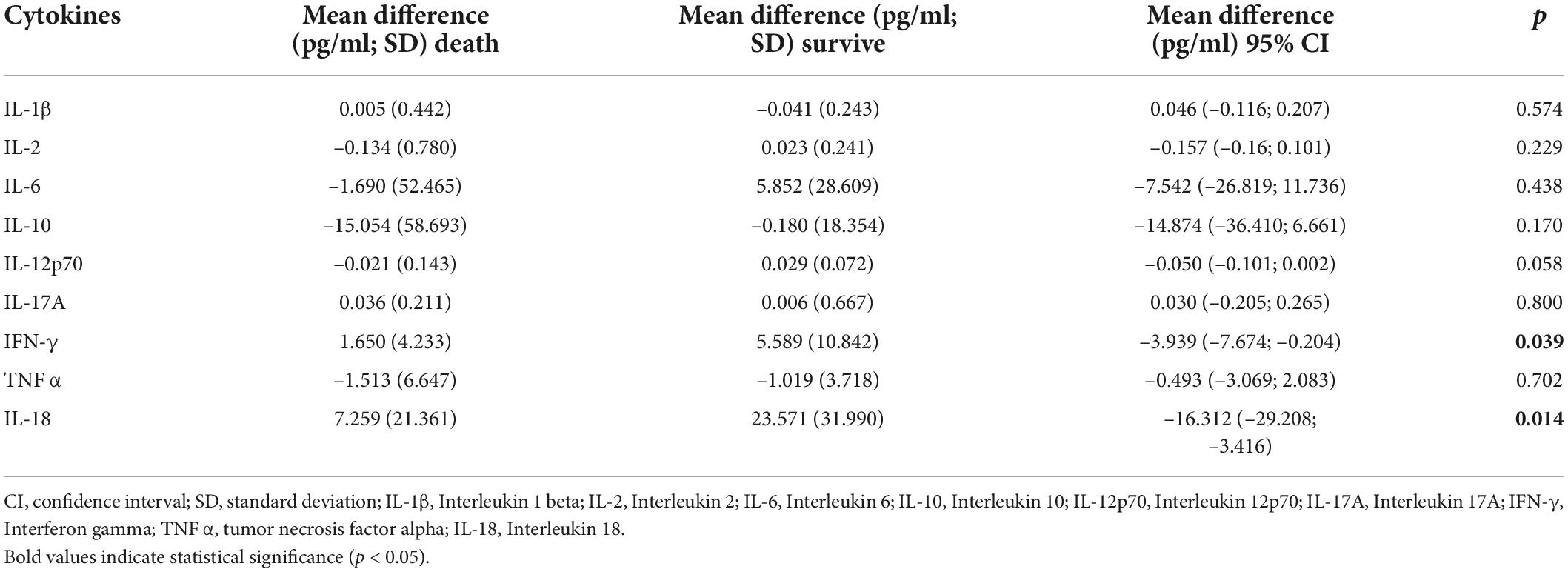
Table 3. Change in the mean difference between the serum levels cytokines between day 1 and day 7 with mortality.
IL-1β/IL-10 and TNFα/IL-10 ratios
A lower IL-1β/IL-10 ratio was associated with mortality on both days 1 and 7. The median on day 1 was 0.15 vs. 0.56 pg/ml (p = 0.048) and on day 7 0.14 vs. 1.63 (p = 0.002). A low TNFα/IL-10 ratio was associated with mortality only on day 7 (median 1.13 vs. 3.12 pg/ml, p = 0.008; Figure 3). The IL-1β/IL-10 ratio on day 7, with a cut-off below 2 [OR = 2.09 (1.05–4.12)], remained significantly associated with decreased survival after adjustments; however, the IL-1β/IL-10 ratio on day 1 lost its statistical significance. The TNFα/IL-10 ratio was not associated with mortality, even when the cut-off was below 4 [OR = 1.76 (0.93–3.31)].
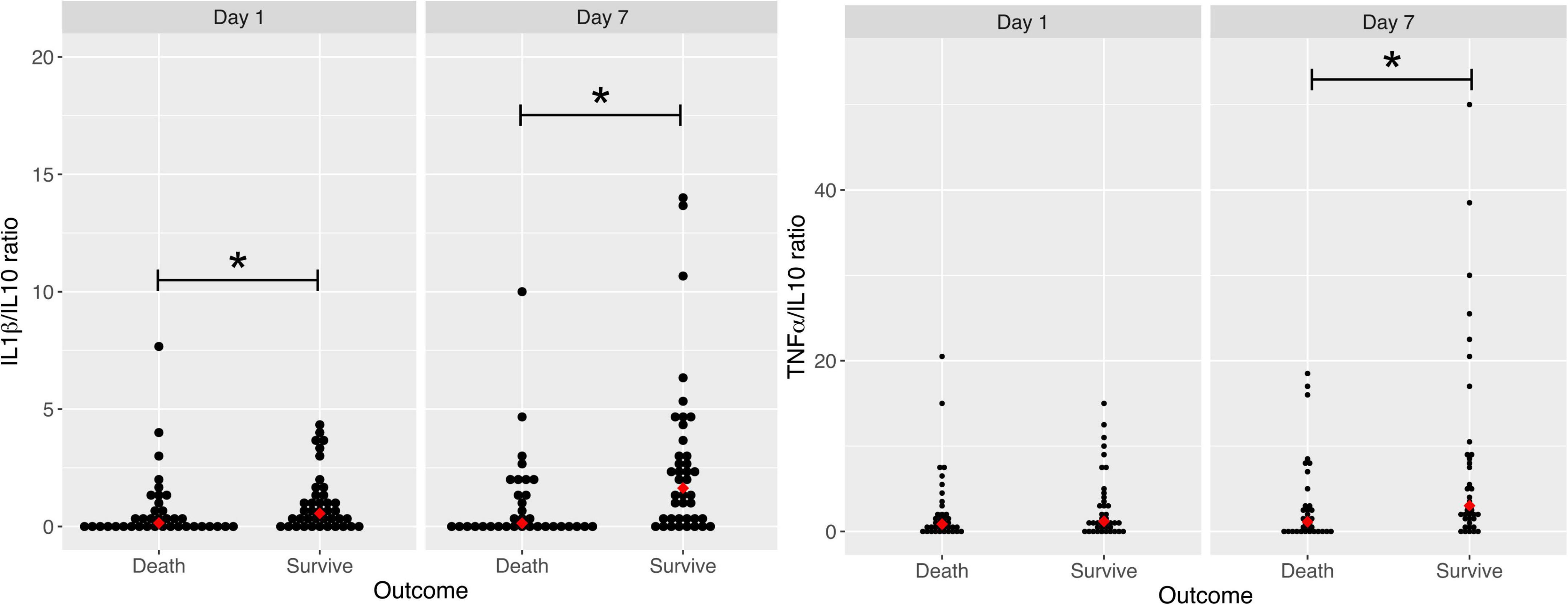
Figure 3. Comparison of IL-1β/IL-10 ratio and TNFα/IL-10 ratio concentrations on days 1 and 7 between COVID-19 patients who died and survived. TNF α, tumor necrosis factor alpha; IL-10, Interleukin 10; IL-1β, Interleukin 1 beta. For IL-1β/IL-10 ratio: *P value = 0.048 **P value = 0.002. TNFα/IL-10 ratio: *P value = 0.008.
Cytokine concentration correlations
We also determined the correlation of serum cytokine levels with APACHE and SOFA severity scores, with laboratory values taken on the first day of ICU admission, and with the probability of developing pulmonary thromboembolism during the ICU stay, with the probability of still being intubated on day 7, and with pulmonary coinfection, defined by positive result of the Biofire® FilmArray® Pneumonia Panel, or of the microbiological cultures of respiratory samples from patients.
Regarding the correlation with the severity scores, only IL-2, taken on the first day of ICU admission, correlated positively and weakly with SOFA (Table 4).
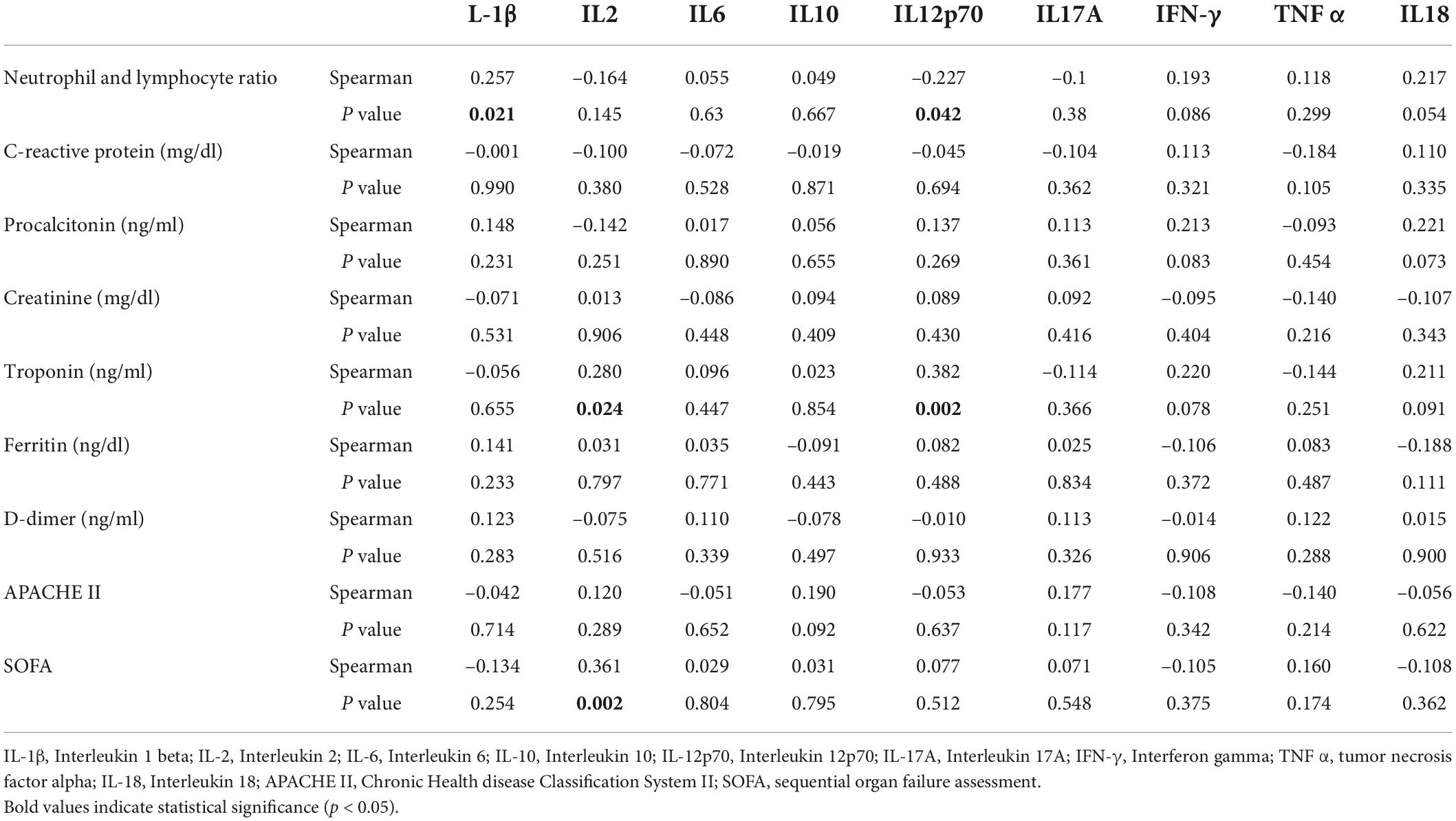
Table 4. Correlation matrix between cytokines with severity scores and laboratories at admission.
Of the laboratory tests taken in the first 24 h of ICU admission, the only test that correlated with any cytokine measured on day 1 was troponin, which correlated with IL-2 and IL-12p70, both weakly and positively. Regarding inflammatory response markers, only IL-1β positively (but weakly) and IL-12p70 negatively (but weakly) correlated with the neutrophil and lymphocyte ratio. No cytokine correlated with C-reactive protein or procalcitonin.
With respect to medical complications during the stay, only IL-2, taken on the first day of ICU admission, correlated with the probability of developing pulmonary thromboembolism during the ICU stay. Neither cytokine correlated with the probability of still being intubated on day 7. Moreover, neither cytokine correlated with pulmonary coinfection (Table 5).

Table 5. Cytokine concentration and correlation with pulmonary coinfection, mechanical ventilation on day 7 and pulmonary thromboembolism.
Discussion
In our study, when comparing cytokine levels in their quantitative form, there were no differences between live and dead patients on day 1. However, in the multivariate analysis we found that IL-1β was the only cytokine associated with mortality in patients who had median levels lower than 1.365 pg/ml compared to those who had higher values.
The SARS-CoV-2 has been considered to trigger an increased activation of macrophages and natural killer (NK) cells with a fulminant release of cytokines known as “CS” (17). The over-production of IL-1β acts on its receptor in tissue macrophages for the generation of more cytokines, which can lead to a vicious cycle resulting in multiple organ dysfunction in the patient (18). Treatment with anakinra, a recombinant human IL-1Ra, which limits the binding of IL-1β with its receptor, has been studied to prevent respiratory failure in patients with COVID-19 (19). However, according to our results, patients with median levels >1,365 pg/ml have a better outcome, and therefore treatment with anakinra would not be useful. One possible explanation is that the peak of IL-1β is early, before severe symptoms of the disease appear, and thus in critically ill patients requiring IMV, blood concentrations of IL-1β are at low levels and are associated with mortality (20).
The soluble urokinase plasminogen activator receptor (suPAR) is increased earlier than IL-1β, and plasma suPAR ≥ 6 ng/ml have been used in the SAVE-MORE study to guide the use of anakinra in hospitalized patients without respiratory failure defined by the use of high-flow oxygen (HFO), non-invasive ventilation (NIV) or IMV (21). suPAR levels were not measured in our study. It would be interesting to explore its relationship with IL-1β and its association with mortality.
A recent meta-analysis showed that several biomarkers including 10 cytokines are associated with severity and mortality in COVID-19 (22). Herr mentioned that a classical “CS” as seen in other conditions was not observed (23). The results of our study are in keeping with this statement. We found no association between serum IL-6 levels and mortality, as other studies have reported (24, 25).
There were no differences between live and dead patients in their conditions of immunosuppression at admission (rheumatologic disease, neoplasm, HIV, cirrhosis and prior steroid use), or at the time of onset of symptoms. To determine which phase of the inflammatory response predominated in the patients, we analyzed the IL-1β/IL-10 and the TNFα/IL-10 ratios as biomarkers of the balance between key pro- to anti-inflammatory levels. The lowest IL-1β/IL-10 ratio was associated with mortality on days 1 and 7, however, when analyzing a value or cut-off point associated with mortality, only the IL-1β/IL-10 ratio on day 7 remained significantly associated with decreased survival. A TNFα/IL-10 lower ratio was associated with mortality only on day 7. Moreover, we did not find a cut-off point that was associated with mortality. These results suggest that anti-inflammatory activity was predominant.
One possible explanation is that the anti-inflammatory activity of IL-10 has greater value. We found that the IL-10 median levels were higher on day 7 of ICU stay in patients who died. A meta-analysis showed that higher levels of IL-10 are associated with severity and mortality in patients with COVID-19 (26). Dorgham et al. detected elevated levels of IL-10 in patients with IMV and requiring extracorporeal membrane oxygenation (ECMO) (27). Lu et al. proposed that a sudden and strong elevation of IL-10 could play a role in lung injury in COVID-19 patients (28). Balzanelli et al. proposed an alternative “Trojan Horse” hypothesis where people who suddenly died would have shown a viral/bacterial/fungi coinfection with possible low expression of IL-10 (29).
Another possible conclusion is that the inflammatory activity provided by IL-1β and TNFα of patients who died is already decreased. Although median levels of IL-1β lower than 1.365 pg/ml were associated with mortality, we did not find similar results with TNF. Anderberg et al. identified that the TNFα/IL-10 ratio was correlated with multiple organ failure and mortality (10). A study by Jia et al. found that among 107 patients, those who were in the ICU with COVID-19, had higher values of TNFα, which was an independent risk factor for death (30). The interaction of the SARS-CoV-2 with angiotensin-converting enzyme 2 (ACE2) in alveolar epithelial cells is made possible by TNF-α, so anti-TNFα therapy could have a therapeutic role (31, 32).
The macrophages and dendritic cells produce IL-12 to activate NK cells and induce the secretion of IFN-γ as a defense mechanism against SARS-CoV-2 infection. This occurs in the early stages of the disease to limit the spread of the virus (33). In a study comprising 95 patients who had less than 10 days of COVID-19 symptoms, lower IL-12 levels were found in patients with severe disease (34). Other reports link IL-12 with severity. For example, Moll-Bernardes et al. in 167 hospitalized hypertensive patients with COVID-19 discovered that IL-12p70 were strongly associated with progression of symptoms to more severe forms of the disease (35). Studies on the association of IL-12 (p70) with mortality in COVID-19 are more limited. The multivariate analysis found that IL-12p70 was the only cytokine associated with mortality on day 7 of ICU stay when median levels were >1.666 pg/ml, i.e., those patients with levels <1.666 pg/ml have a 23% greater probability of survive than those with higher values. All patients at day 7 had received steroids for the management of COVID-19, and no patients were treated with anakinra or tocilizumab.
The main difference between days 1 and 7 was a decrease in IFN-γ and IL-18 levels in patients who had died. Trouillet-Assant et al. observed that the elevation of IFN-α 2 occurred on the first week of symptom onset, and then tapered off in 26 critically ill patients with COVID-19. Patients who did not present high IFN-α 2 peaks required IMV and a longer ICU stay (36). With a median of 9 days of symptom onset from day 1 of stay, we would expect lower levels of IFN on day 7. Bülow Anderberg et al. found that blood concentrations of IFN γ were elevated at hospital admission, appearing 11 days after initial symptoms appeared in patients with respiratory failure (10). Hence, IFN γ levels may reflect the later stages of the disease. Tang et al. mentioned that IFN- γ had no role in the survival analyses of 71 patients, and its level was lower in critically severe patients compared to those with mild symptoms (37).
Macrophages produce IL-18 to stimulate the production of IFN-γ for optimal viral host defense (38). IL-18 release induces ferritin, explaining the hyperferritinemia. Satış et al. reported that IL-18 serum concentrations above the cut-off value of 576 pg/ml on admission were associated with an 11.7-fold increased risk of ICU admission, in 58 COVID-19 patients (39). Dorgham et al. detected decreased levels of IL-18 in ECMO patients who died (27).
Neutrophil/lymphocyte ratios have been associated with mortality in COVID-19 (40). We found that only IL-1β and IL-12p70 correlated with the neutrophil and lymphocyte ratio. No cytokine correlated with C-reactive protein or procalcitonin. Moreover, that troponin correlates with IL-2 and IL-12p70. Song et al. noticed that TNFα, IL-8 and IL-6, were higher in 64 critically ill patients with cardiac dysfunction (41).
The strengths of our study are listed as follows: (1) This is a multicenter Latin American study; (2) Our investigation comprised critically ill patients on mechanical ventilation; (3) The serum samples were taken early in the course of their hospitalization with follow-up samples taken on day 7, covering the dynamic changes of the disease; (4) We measured different correlations of cytokine concentration with laboratory tests, pulmonary thromboembolism and pulmonary coinfection.
The limitations of this study include: (1) We did not measure viral titers and therefore, do not know whether they correlate with cytokines; Guo et al. described that the virus titers were correlated with the cytokines (42); (2) The sample size could be considered small; (3) We do not know the relationship of serum cytokines with the immune and inflammatory response at the pulmonary level; (4) We did not measure macrophages, helper/inducible T lymphocyte (CD3+ CD4+ %) or inhibitory/cytotoxic T lymphocyte (CD3+ CD8+ %) levels to analyze its correlation with cytokines.
In conclusion, on day 1 of ICU stay, IL-1β was the only cytokine that has a statistical association, with an increase in mortality in those patients who had median levels <1.365 pg/ml. On day 7 of ICU stay, IL-12p70 was associated with mortality when median levels were >1.666 pg/ml and the IL-1β/IL-10 ratio cut-off was <2. A classical “CS” was not observed in this study. The inflammatory activity of patients who died was already decreased. Anakinra or tocilizumab therapy might not be useful in our patients.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Universidad Pontificia Bolivariana Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Funding
This study was funded by Minciencias, Colombia, 121084468048.
Acknowledgments
Acknowledgment to the Institutions participating in the study with the respective collaborators: Clínica Universitaria Bolivariana, Francisco Molina. Clínica El Rosario Tesoro, Álvaro Ochoa. Clínica CardioVid, Juan David Uribe. Clínica Sagrado Corazón, Nelson Fonseca. Clínica Las Américas Auna, Bladimir Gil. Clínica Medellín, Juan Echeverry. Hospital La María, Marco González. Hospital Manuel Uribe Ángel, Victoria Ángel. Hospital Pablo Tobón Uribe, Gisella de la Rosa.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chang R, Elhusseiny KM, Yeh Y-C, Sun W-Z. COVID-19 ICU and mechanical ventilation patient characteristics and outcomes—a systematic review and meta-analysis. PLoS One. (2021) 16:e0246318. doi: 10.1371/journal.pone.0246318
2. Greco M, De Corte T, Ercole A, Antonelli M, Azoulay E, Citerio G, et al. Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: the global unite-COVID study. Intens Care Med. (2022) 48:690–705.
3. Behrens EM, Koretzky GA. Review: cytokine storm syndrome: looking toward the precision medicine era. Arthritis Rheumatol. (2017) 69:1135–43.
4. Ruan Q, Yang K, Wang W, Jiang L, Song J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intens Care Med. (2020) 46:846–8. doi: 10.1007/s00134-020-05991-x
5. Fernandez-botran R, Furmanek S, Sekhar R, Cahill M, Carrico R, Akca O, et al. Association and predictive value of biomarkers with severe outcomes in hospitalized patients with SARS-CoV-2 infection. Cytokine. (2022) 149:155755.
6. Milenkovic M, Hadzibegovic A, Kovac M, Jovanovic B, Stanisavljevic J, Djikic M, et al. D-dimer, CRP, PCT, and IL-6 levels at admission to ICU Can predict in-hospital mortality in patients with COVID-19 pneumonia. Oxid Med Cell Longev. (2022) 2022:8997709. doi: 10.1155/2022/8997709
7. Ferrandoa ES, Hanslin K, Hultstro M, Larssone A, Frithiofa R, Lipcsey M. Soluble TNF receptors predict acute kidney injury and mortality in critically ill COVID-19 patients: a prospective observational study. Cytokine. (2022) 149:155727. doi: 10.1016/j.cyto.2021.155727
8. McElvaney OJ, McEvoy NL, McElvaney OF, Carroll TP, Murphy MP, Dunlea DM, et al. Characterization of the inflammatory response to severe COVID-19 illness. Am J Respir Crit Care Med. (2020) 202:812–21.
9. Kox M, Waalders NJB, Kooistra EJ, Gerretsen J, Pickkers P. Cytokine levels in critically ill patients with COVID-19 and other conditions. JAMA. (2020) 324:1565–7.
10. Bülow Anderberg S, Luther T, Berglund M, Larsson R, Rubertsson S, Lipcsey M, et al. Increased levels of plasma cytokines and correlations to organ failure and 30-day mortality in critically ill COVID-19 patients. Cytokine. (2021) 138:155389. doi: 10.1016/j.cyto.2020.155389
11. Li J, Rong L, Cui R, Feng J, Jin Y, Chen X, et al. Dynamic changes in serum IL-6, IL-8, and IL-10 predict the outcome of ICU patients with severe COVID-19. Ann Palliat Med. (2021) 10:3706–14. doi: 10.21037/apm-20-2134
12. Tong-Minh K, Does Y, Rosmalen J, Ramakers C, Gommers D, Gorp E, et al. Joint modeling of repeated measurements of different biomarkers predicts mortality in COVID-19 patients in the intensive care unit. Biomark Insights. (2022) 17:11772719221112370. doi: 10.1177/11772719221112370
13. Molina, FJ, Botero LE, Isaza JP, Cano LE, López L, Tamayo L, et al. Diagnostic inside the text. concordance between BioFire® FilmArray® Pneumonia Panel and culture in patients with COVID-19 pneumonia admitted to intensive care units: the experience of the third wave in eight hospitals in Colombia. Crit Care. (2022) 26:130. doi: 10.1186/s13054-022-04006-z
14. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intens Care Med. (1996) 22:707–10.
16. Tsurumi A, Que YA, Ryan CM, Tompkins RG, Rahme LG. TNF-α/IL-10 ratio correlates with burn severity and may serve as a risk predictor of increased susceptibility to infections. Front Public Heal. (2016) 4:216.
17. Karakike E, Giamarellos-Bourboulis EJ. Macrophage activation-like syndrome: a distinct entity leading to early death in sepsis. Front Immunol. (2019) 10:55. doi: 10.3389/fimmu.2019.00055
18. Del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43.
19. Kyriazopoulou E, Panagopoulos P, Metallidis S, Dalekos GN, Poulakou G, Gatselis N, et al. An open label trial of anakinra to prevent respiratory failure in COVID-19. Elife. (2021) 10:e66125. doi: 10.7554/eLife.66125
20. Cavalli G, Colafrancesco S, Emmi G, Imazio M, Lopalco G, Maggio MC, et al. Interleukin 1α: a comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun Rev. (2021) 20:102763. doi: 10.1016/j.autrev.2021.102763
21. Kyriazopoulou E, Poulakou G, Milionis H, Metallidis S, Adamis G, Tsiakos K, et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: a double-blind, randomized controlled phase 3 trial. Nat Med. (2021) 27:1752–60.
22. Qin R, He L, Yang Z, Jia N, Chen R, Xie J, et al. Identification of parameters representative of immune dysfunction in patients with severe and fatal COVID-19 infection: a systematic review and meta-analysis. Clin Rev Allergy Immunol. (2022) 1–33. [Epub ahead of print]. doi: 10.1007/s12016-021-08908-8
23. Herr C, Mang S, Mozafari B, Guenther K, Speer T, Seibert M, et al. Distinct patterns of blood cytokines beyond a cytokine storm predict mortality in COVID-19. J Inflamm Res. (2021) 14:4651–67. doi: 10.2147/JIR.S320685
24. Laguna-goya R, Utrero-rico A, Talayero P, Lasa-lazaro M, Aguado JM, Martinez-lopez J. IL-6–based mortality risk model for hospitalized patients with COVID-19. J Allergy Clin Inmunol. (2020) 146:799–807.e9.
25. Dhar SK, Vishnupriyan K, Damodar S, Gujar S, Das M. IL-6 and IL-10 as predictors of disease severity in COVID-19 patients: results from meta-analysis and regression. Heliyon. (2021) 7:e06155. doi: 10.1016/j.heliyon.2021.e06155
26. Alshammary AF, Alsughayyir JM, Alharbi KK, Al-Sulaiman AM, Alshammary HF, Alshammary HF. T-Cell subsets and interleukin-10 levels are predictors of severity and mortality in COVID-19: a systematic review and meta-analysis. Front Med. (2022) 9:852749. doi: 10.3389/fmed.2022.852749
27. Dorgham K, Quentric P, Gôkkaya M, Marot S, Parizot C, Sauce D, et al. Distinct cytokine profiles associated with COVID-19 severity and mortality. J Allergy Clin Inmunol. (2020) 147:2098–107.
28. Lu L, Zhang H, Dauphars DJ, He Y-W. A potential role of Interleukin 10 in COVID-19 pathogenesis. Adv Insect Phys. (2020) 42:72–80.
29. Balzanelli MG, Distratis P, Aityan SK, Amatulli F, Catucci O, Cefalo A, et al. An alternative “Trojan Horse” hypothesis for COVID-19: immune deficiency of IL-10 and SARS-CoV-2 biology. Endocr Metab Immune Disord Drug Targets. (2021) 22:1–5. doi: 10.2174/1871530321666210127141945
30. Jia F, Wang G, Xu J, Long J, Deng F, Jiang W. Role of tumor necrosis factor-α in the mortality of hospitalized patients with severe and critical COVID-19 pneumonia. Aging. (2021) 13:23895–912. doi: 10.18632/aging.203663
31. Haga S, Yamamoto N, Nakai-Murakami C, Osawa Y, Tokunaga K, Sata T, et al. Modulation of TNF-α-converting enzyme by the spike protein of SARS-CoV and ACE2 induces TNF-α production and facilitates viral entry. Proc Natl Acad Sci U S A. (2008) 105:7809–14. doi: 10.1073/pnas.0711241105
32. Guo Y, Hu K, Li Y, Lu C, Ling K, Cai C, et al. Targeting TNF-α for COVID-19: recent advanced and controversies. Front Public Heal. (2022) 10:833967. doi: 10.3389/fpubh.2022.833967
33. Guo Y, Cao W, Zhu Y. Immunoregulatory functions of the IL-12 family of cytokines in antiviral systems. Viruses. (2019) 11:772.
34. Tjan LH, Furukawa K, Nagano T, Kiriu T, Nishimura M, Arii J, et al. Early differences in cytokine production by severity of coronavirus disease 2019. J Infect Dis. (2021) 223:1145–9.
35. Moll-Bernardes R, de Sousa AS, Macedo AVS, Lopes RD, Vera N, Maia LCR, et al. IL-10 and IL-12 (P70) levels predict the risk of COVID-19 progression in hypertensive patients: insights from the brace-corona trial. Front Cardiovasc Med. (2021) 8:702507. doi: 10.3389/fcvm.2021.702507
36. Trouillet-Assant S, Viel S, Gaymard A, Bitker L, Belot A. Type I IFN immunoprofiling in COVID-19 patients. J Allergy Clin Inmunol. (2020) 146:206–8. doi: 10.1016/j.jaci.2020.04.029
37. Tang Y, Sun J, Pan H, Yao F, Yuan Y, Zeng M, et al. Aberrant cytokine expression in COVID-19 patients?: associations between cytokines and disease severity. Cytokine. (2021) 143:155523.
38. Arend W, Palmer G, Gabay C. IL-1, IL-18, and IL-33 families of cytokines. Immunol Rev. (2008) 223:20–38.
39. Satış H, Özger HS, Aysert Yıldız P, Hızel K, Gulbahar Ö, Erbaş G, et al. Prognostic value of interleukin-18 and its association with other inflammatory markers and disease severity in COVID-19. Cytokine. (2021) 137:155302. doi: 10.1016/j.cyto.2020.155302
40. Li X, Liu C, Mao Z, Xiao M, Wang L, Qi S, et al. Predictive values of neutrophil-to-lymphocyte ratio on disease severity and mortality in COVID-19 patients: a systematic review and meta-analysis. Crit Care. (2020) 24:647. doi: 10.1186/s13054-020-03374-8
41. Song Y, Gao P, Ran T, Qian H, Guo F, Chang L, et al. High inflammatory burden: a potential cause of myocardial injury in critically ill patients with COVID-19. Front Cardiovasc Med. (2020) 7:128. doi: 10.3389/fcvm.2020.00128
Keywords: COVID-19, SARS-CoV-2, cytokines, mortality, intensive care units, pneumonia
Citation: Molina FJ, Botero LE, Isaza JP, Cano LE, López L, Hoyos LM, Correa E and Torres A (2022) Cytokine levels as predictors of mortality in critically ill patients with severe COVID-19 pneumonia: Case-control study nested within a cohort in Colombia. Front. Med. 9:1005636. doi: 10.3389/fmed.2022.1005636
Received: 05 August 2022; Accepted: 12 September 2022;
Published: 29 September 2022.
Edited by:
Diego Ripamonti, Papa Giovanni XXIII Hospital, ItalyReviewed by:
Wilmer Silva Caso, Peruvian University of Applied Sciences, PeruAileen Faist, University Hospital Münster, Germany
Copyright © 2022 Molina, Botero, Isaza, Cano, López, Hoyos, Correa and Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco José Molina, ZnJhbmNpc2NvLm1vbGluYUB1cGIuZWR1LmNv