 David Clofent1,2
David Clofent1,2 Eva Polverino1,2*
Eva Polverino1,2* Almudena Felipe1,2
Almudena Felipe1,2 Galo Granados1,2Marta Arjona-Peris1,2Jordi Andreu3Ana L. Sánchez-Martínez3
Galo Granados1,2Marta Arjona-Peris1,2Jordi Andreu3Ana L. Sánchez-Martínez3 Diego Varona3Laura Cabanzo3Jose M. Escudero3Antonio Álvarez1,2,4Karina Loor1,2Xavier Muñoz1,2,4Mario Culebras1,2 on behalf of the Se-COVID-19 team
Diego Varona3Laura Cabanzo3Jose M. Escudero3Antonio Álvarez1,2,4Karina Loor1,2Xavier Muñoz1,2,4Mario Culebras1,2 on behalf of the Se-COVID-19 team- 1Department of Respiratory Medicine, Vall D'Hebron University Hospital, Barcelona, Spain
- 2Vall D'Hebron Institut de Recerca (VHIR), Barcelona, Spain
- 3Radiology Department, Vall D'Hebron University Hospital, Barcelona, Spain
- 4CIBER Enfermedades Respiratorias (CIBERES), Barcelona, Spain
Background: Interstitial lung sequelae are increasingly being reported in survivors of COVID-19 pneumonia. An early detection of these lesions may help prevent the development of irreversible lung fibrosis. Lung ultrasound (LUS) has shown high diagnostic accuracy in interstitial lung disease (ILD) and could likely be used as a first-line test for post-COVID-19 lung sequelae.
Methods: Single-center observational prospective study. Follow-up assessments of consecutive patients hospitalized for COVID-19 pneumonia were conducted 2–5 months after the hospitalization. All patients underwent pulmonary function tests (PFTs), high-resolution computed tomography (HRCT), and LUS. Radiological alterations in HRCT were quantified using the Warrick score. The LUS score was obtained by evaluating the presence of pathological B-lines in 12 thoracic areas (range, 0–12). The correlation between the LUS and Warrick scores was analyzed.
Results: Three hundred and fifty-two patients who recovered from COVID-19 pneumonia were recruited between July and September 2020. At follow-up, dyspnea was the most frequent symptom (69.3%). FVC and DLCO alterations were present in 79 (22.4%) and 234 (66.5%) patients, respectively. HRCT showed relevant interstitial lung sequelae (RILS) in 154 (43.8%) patients (Warrick score ≥ 7). The LUS score was strongly correlated with the HRCT Warrick score (r = 0.77) and showed a moderate inverse correlation with DLCO (r = −0.55). The ROC curve analysis revealed that a LUS score ≥ 3 indicated an excellent ability to discriminate patients with RILS (sensitivity, 94.2%; specificity, 81.8%; negative predictive value, 94.7%).
Conclusions: LUS could be implemented as a first-line procedure in the evaluation of Post-COVID-19 interstitial lung sequelae. A normal LUS examination rules out the presence of these sequelae in COVID-19 survivors, avoiding the need for additional diagnostic tests such as HRCT.
Introduction
The global coronavirus disease 2019 (COVID-19) pandemic has reached unprecedented dimensions, with more than 246 million cases and 5 million deaths worldwide (1). Multiple studies published over the last year have described the pathogenesis and clinical characteristics of this disease (2, 3); however, the long-term sequelae of COVID-19 remain uncertain (4).
In previous viral epidemics such as those caused by MERS-CoV and SARS-CoV, a variable percentage of survivors developed interstitial lung disease (ILD), including pulmonary fibrosis (PF) (5–9). On a similar note, several recent reports have described early respiratory sequelae following COVID-19, such as persistent symptoms, impaired pulmonary function, and interstitial lung abnormalities (10–16). The histological findings in lung biopsies of these patients seem to be suggestive of organizing pneumonia and pneumonitis in a recent study (17). However, the magnitude, severity, and reversibility of these sequelae remain to be defined, and close follow-up after COVID-19 pneumonia is needed. Although different follow-up protocols have been published so far, the proposed diagnostic procedures are quite heterogeneous (18–23). For example, while chest imaging is always recommended in the initial evaluation, there is no consensus on the differential use of chest radiography (CXR) vs. computed tomography (CT). Interestingly, lung ultrasound (LUS) has not yet been considered in any of these protocols.
In the last decades, LUS has proven to be a suitable alternative to conventional radiological methods in multiple kinds of lung diseases (24–27). During the current pandemic, numerous studies have reported the usefulness of LUS as a front-line tool in the diagnosis and management of SARS-CoV-2 acute pneumonia (28–31). However, its applicability in the detection of post-COVID-19 interstitial sequelae is yet to be defined.
LUS has been previously validated for the detection of ILD secondary to other causes. Several studies, mostly those involving connective tissue disease-associated ILD, have shown significant superiority of LUS over CXR and, most importantly, similar sensitivity and negative predictive value in comparison with CT (32–37). In addition, ultrasonography can easily be considered a first-line tool because it is non-invasive, non-ionizing, and inexpensive.
Thus, the aim of this study was to describe the diagnostic accuracy of LUS in the assessment of early interstitial sequelae after COVID-19 pneumonia in comparison with CT.
Methods
Ethics Statement
Ethics approval was obtained prior to the start of the study by the Medical Ethics Committee of Vall d'Hebron Barcelona University Hospital [PR(AG)461/2020]. Written informed consent was obtained from all the patients before their inclusion.
Study Design and Participants
This single-center observational prospective study evaluated 362 survivors hospitalized for COVID-19 pneumonia between March 3, 2020 and April 29, 2020 at Vall d'Hebron University Hospital, Barcelona, Spain. Patients were included consecutively if they visited the dedicated post-COVID-19 outpatient clinic at our respiratory department between July 20, 2020, and September 21, 2020.
Patients visited the clinic at least 2 months after their hospital discharge. Patients recovered from severe pneumonia were visited first for medical reasons. We excluded patients with previously diagnosed ILD, congestive heart failure and those who declined to participate. Baseline information was retrieved from medical records. All patients were interviewed face-to-face by experienced pulmonologists and underwent pulmonary function tests (PFTs), including spirometry and measurement of the carbon monoxide diffusing capacity (DLCO) and high-resolution CT (HRCT) and LUS. HRCT and LUS were performed no more than 15 days apart.
Pulmonary Function Tests
Lung-function tests were performed at our dedicated laboratory by using Master-Lab equipment (E. Jaeger, Germany) in accordance with international protocols and GLI reference values (38–40). Pulmonary parameters included forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), FEV1/FVC ratio, and lung diffusing capacity for carbon monoxide (DLCO). Lung volumes and post-bronchodilation tests were not performed.
Chest HRCT
HRCT examinations were performed by a standard protocol using Siemens Somatom Force Dual Source CT and Siemens Somatom Definition AS+ scanners. Scans were obtained at full inspiration from the apex to the lung base in the supine position. All chest CT scans were reconstructed with a 1.5-mm slice thickness. Iodine contrast agents were not used.
HRCT images were evaluated according to the Fleischner Society glossary (41), and the following findings were evaluated: ground-glass opacities (GGO), consolidation, septal/subpleural lines (including parenchymal bands and reticular pattern), irregular pleura, nodules, subpleural cysts, architectural distortions, traction bronchiectasis, honeycombing, atelectasis, pleural effusion, and mosaic attenuation patterns.
Pulmonary involvement was quantified according to the Warrick score, which has been previously validated in scleroderma-related ILD (42, 43) and is widely used in ultrasonography studies (32–35). This score is obtained by summing the scores for five basic radiological ILD findings (from 0 to 5) and the extent of these changes (from 0 to 3). The total score ranges from 0 to 30, and a minimum score of 7 has been validated as the best cut-off point for predicting pulmonary disease in ILD (43). We implemented this cut-off point in our population and therefore classified patients with relevant interstitial lung sequelae (RILS) as those with a Warrick score ≥ 7. A more detailed explanation of the Warrick score is provided in Table 1.
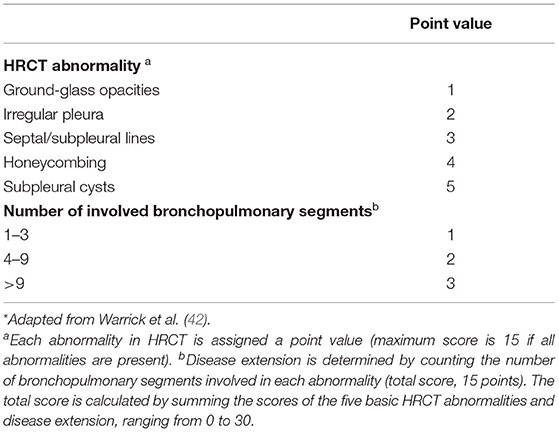
Table 1. Warrick score for HRCT involvement*.
Each HRCT image was evaluated by two blinded, independent thoracic radiologists who calculated the Warrick score. The final Warrick score was the average of the two independent reads if the difference was 4 points or less (variability < 13.3%). In cases with a greater difference, both radiologists met and performed a third consensual assessment.
Lung Ultrasound
LUS examinations were performed using a Sonosite M-Turbo system equipped with a 2–5-MHz convex transducer. A team of four pulmonologist with expertise in LUS conducted all the examinations. Every patient underwent LUS at the follow-up visit by one of the four examiners mentioned, who was always in a separate consultation, blinded to the clinical and other exploration findings.
The scan protocol consisted of a complete examination of all intercostal spaces, which were divided into 12 thoracic areas (two posterior, two lateral, and two anterior for each side) (Figure 1). Abnormalities such as pleural line alterations, B-line artifacts, pleural effusion, and consolidations were registered for each thoracic area (Figure 2). B-lines were defined as laser-like vertical hyperechoic reverberation artifacts that arise from the pleural line extending to the bottom of the screen, moving synchronously with lung sliding (44). Each thoracic area was considered pathological when three or more B-lines were present in any intercostal space (44). We developed a B-line score by summing 1 point for each thoracic area with pathological B-lines (score range, 0 to 12). The inter-observer agreement was evaluated retrospectively by a blinded and simultaneous review of 250 saved clips by the four examiners.
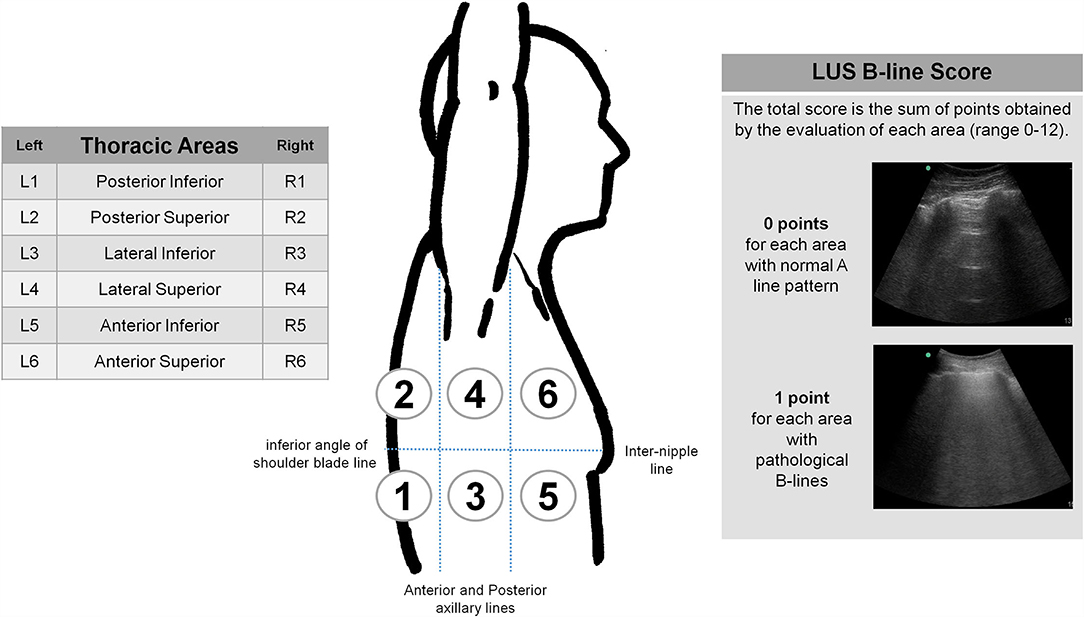
Figure 1. Thoracic areas for LUS examination protocol. Anatomical landmarks: Anterior and posterior axillary lines (for anterior, lateral and posterior areas). Inter-nipple line and inferior angle of shoulder blade line (for superior and inferior areas). Sternum and vertebral spine (for right and left sides).
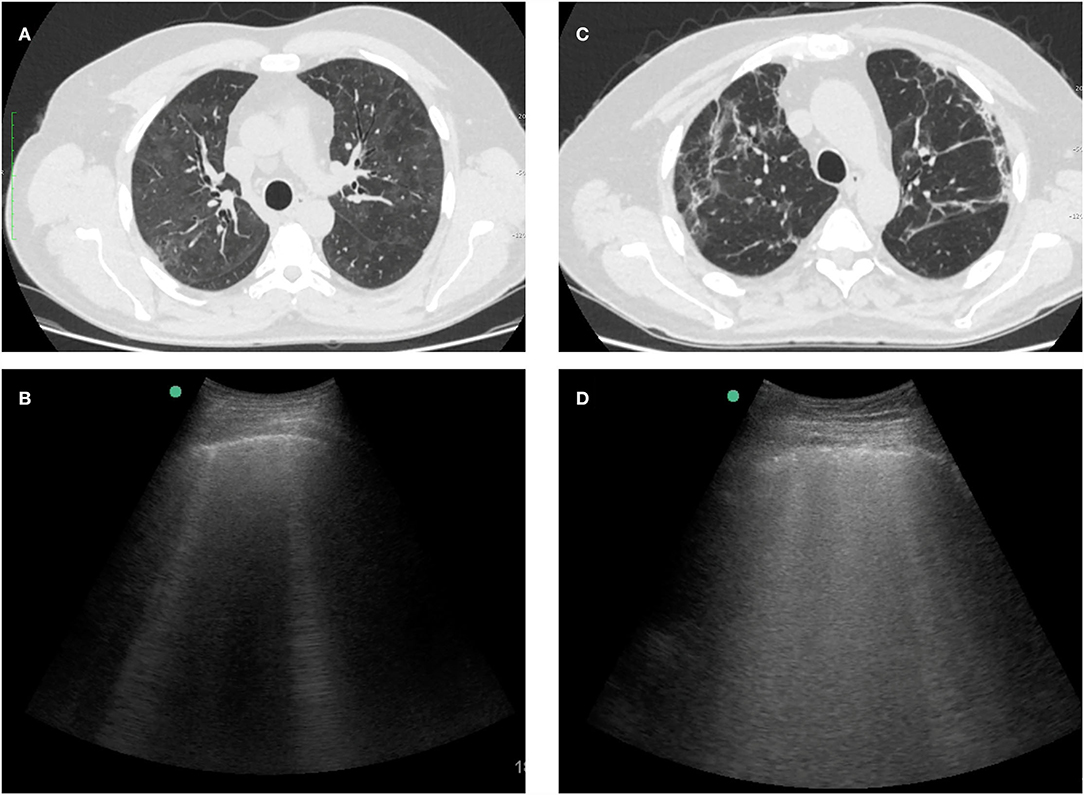
Figure 2. Examples of HRCT and LUS images from 2 patients with interstitial lung sequelae after COVID-19. (A) Persistent diffuse ground-glass opacities on HRCT. (B) LUS of the same patient with isolated B-lines and absence of pleural line abnormalities. (C) Subpleural lines and parenchymal bands on HRCT. (D) LUS of the same patient with confluent B-lines and blurred pleural line.
Outcomes
Primary endpoint was to establish the accuracy of LUS in the detection of relevant interstitial lung sequelae (RILS) in COVID-19 survivors in comparison with HRCT.
Statistical Analysis
All data were analyzed using Stata software (StataCorp. 2017; Stata statistical software: Release 15 College Station, TX, StataCorp LLC, USA). Descriptive analysis was performed according to the pneumonia severity groups and the presence of RILS at follow-up. For the qualitative variables, frequencies and percentages were compared using the chi-square test or Fisher's exact test. For the quantitative variables, means (SD) and medians (IQR) were calculated and compared using the Mann-Whitney U-test. The normality of the distribution was analyzed using the Shapiro–Wilk test. The p-value was computed from the Spearman rank correlation coefficient when the variable was continuous and from the χ2 test if the variable was categorical. Statistical significance was set at p < 0.05.
The sample size was not calculated because of the lack of reports defining the frequency of pulmonary sequelae in COVID-19 survivors when our study was designed.
LUS inter-observer agreement was evaluated for 250 measurements by using a contingency table and calculating the kappa index of agreement.
A Pearson correlation analysis was performed between the LUS score, HRCT Warrick score, and PFT variables.
Receiver operating characteristic (ROC) curves were plotted to analyze area under the curves (AUC). A cut-off point in the LUS score was obtained according to Youden index as the value corresponding to a HRCT Warrick score of ≥7.
Results
Study Population
Three-hundred and sixty-two patients who had recovered from COVID-19 pneumonia after hospitalization were evaluated. Patients with previously diagnosed ILD (n = 3), congestive heart failure (n = 2) and those who declined to participate (n = 5) were excluded. Consequently, 352 patients were included in our study. Their demographic and clinical characteristics are presented in Table 2. The median duration (IQR) of hospitalization was 9.5 [6.0–21.0] days, and 115 (32.7%) patients were admitted to the intensive care unit (ICU), with a median hospitalization period of 12 (6–21) days. Eighty-one patients (23.0%) required IMV, 51 (14.5%) required NIMV or HFNC, 109 (31.0%) required LFO, and 111 (31.5%) had mild pneumonia with no oxygen therapy requirement.
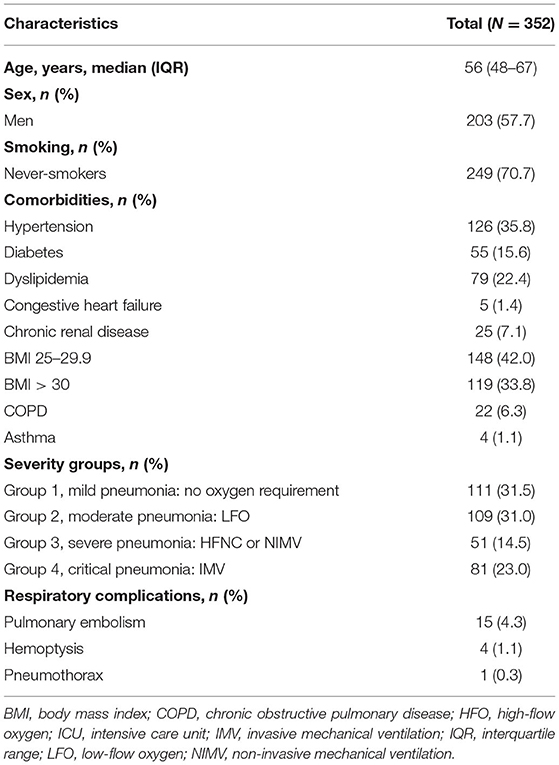
Table 2. Baseline characteristics of the study population.
Symptoms, PFT, HRCT at Follow-Up
The follow-up characteristics of the included patients are shown in Tables 3, 4. The median time (IQR) from hospital admission to the follow-up visit was 90 (64.0–114.0) days. Two hundred and forty-four (69.3%) patients had some persistent symptoms, with the most frequent symptoms being dyspnea (48.3%), fatigue (36.6%), and myalgia or arthralgia (24.1%). In assessments of pulmonary function, FVC and DLCO alterations (<80% of the lower limit range) were present in 79 (22.4%) and 234 (66.5%) patients, respectively. HRCT abnormalities at follow-up were also observed. Ground-glass opacities, consolidations, septal and subpleural lines, and mosaic attenuation patterns were observed in 244 (69.3%), 33 (9.4%), 229 (65.1%), and 88 (25%) patients, respectively. Fibrotic changes such as architectural distortion and traction bronchiectasis were found in 47 (13.4%) and 26 (7.4%) patients, respectively. Only 18 (5.1%) patients had subpleural cysts, and 4 (1.1%) had honeycomb cysts. When the Warrick score was calculated, 154 (43.8%) patients had a score ≥ 7 (RILS group), and 198 (56.2%) had a score < 7. None of the patients with a Warrick score below 7 showed any fibrotic alterations.
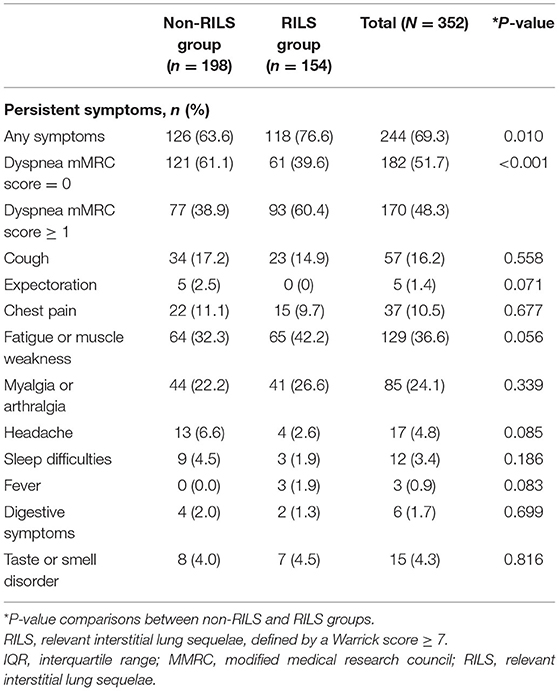
Table 3. Persistent symptoms at follow-up in relevant interstitial lung sequelae (RILS) groups classified by the Warrick score.
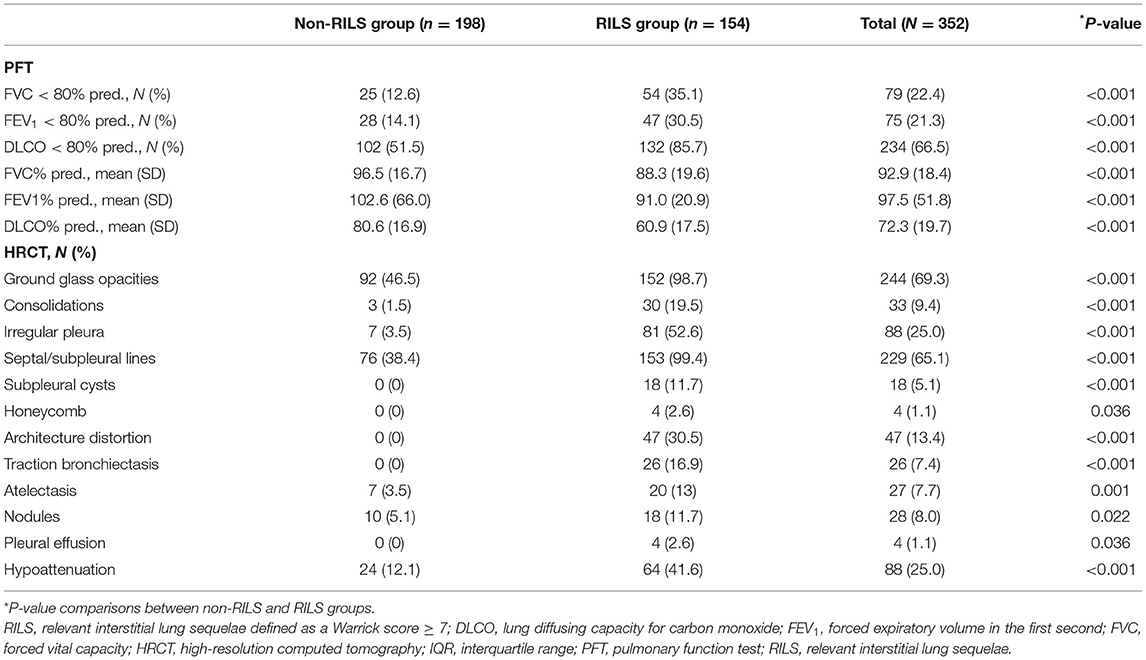
Table 4. PFT and HRCT findings at follow-up in relevant interstitial lung sequelae (RILS) groups categorized by the Warrick score.
Lung Ultrasound
The LUS findings of 352 patients at follow-up evaluations are shown in Table 5. Pleural line thickening in any area was found in 190 (53.9%) patients, and among them, only 12 presented with pleural line fragmentation. Pleural line thickening was significantly higher in the RILS group, and all patients with pleural line fragmentation were in this group. Only 3 patients showed pleural effusion and only 13 showed consolidations. In assessments of B-lines, 257 (73.0%) patients presented with pathological B-lines in any area. Among them, 52 (14.8%) patients presented coalescent B-lines, without significant differences between the RILS and non-RILS groups. Posterior-inferior areas showed a higher frequency of pathological B-lines.
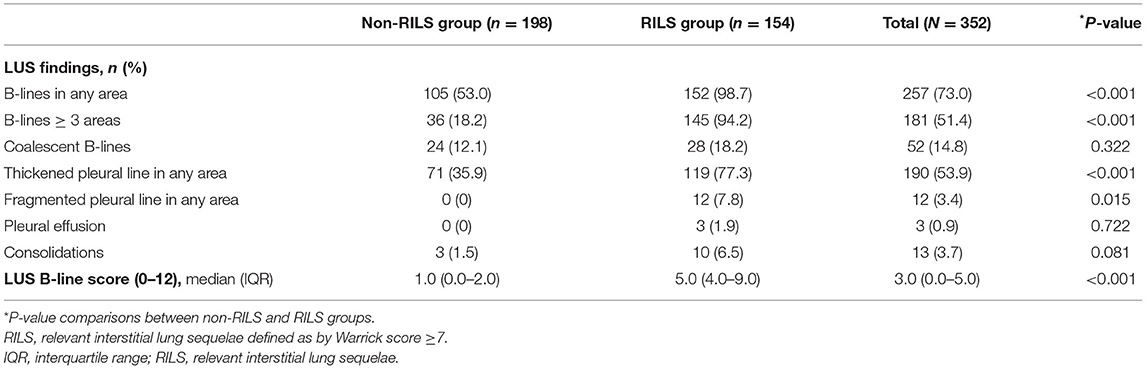
Table 5. LUS findings at follow-up in relevant interstitial lung sequelae (RILS) groups categorized according to the Warrick score.
The median (IQR) B-line score was significantly higher in patients in the RILS group (5.0 [4.0–9.0] vs. 1.0 [0.0–2.0], p < 0.001). The B-line score was strongly correlated with the HRCT Warrick score (r = 0.77) and showed a moderate inverse correlation with DLCO (r = −0.55) (Figure 3).
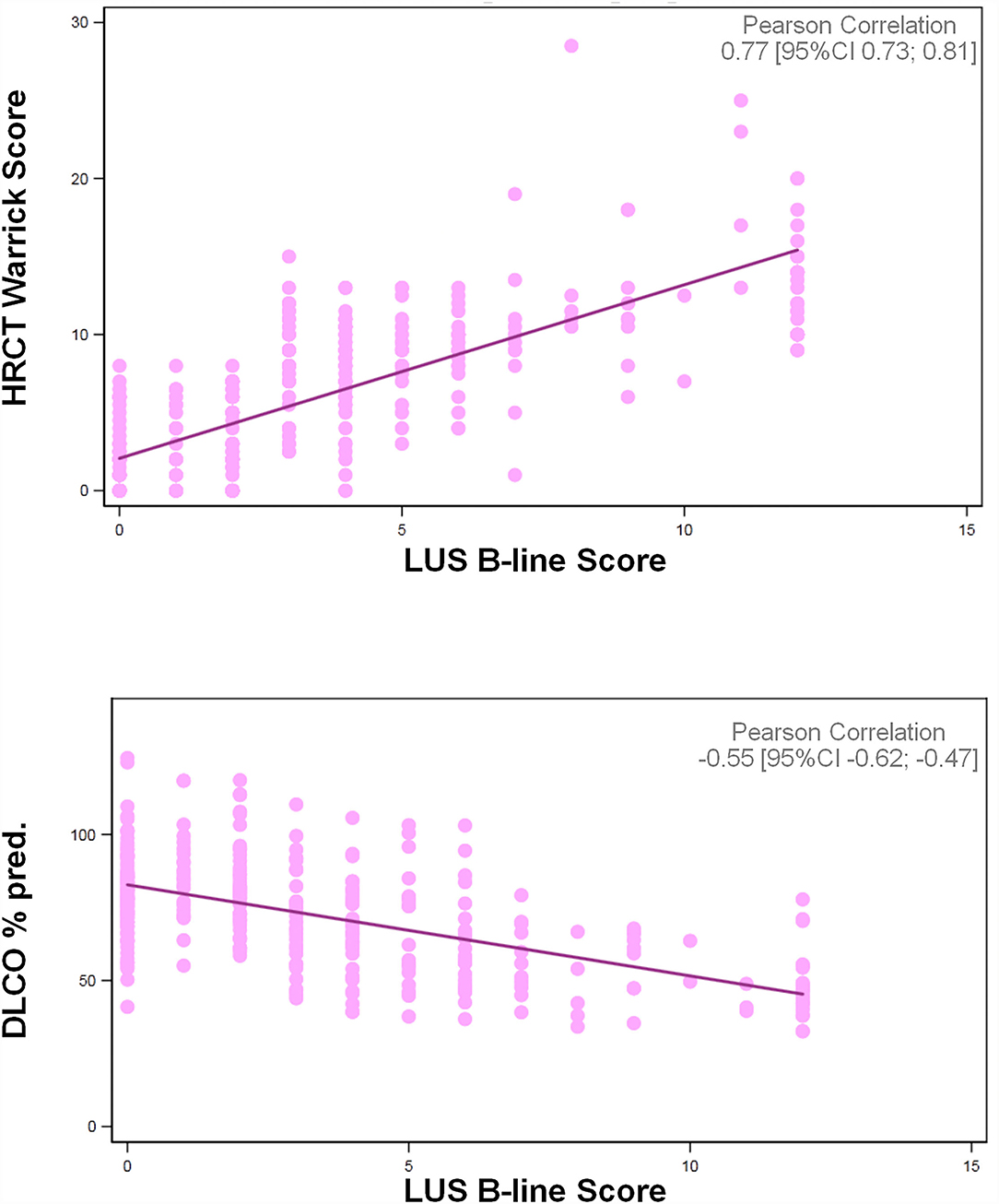
Figure 3. Correlations of LUS B-line score with HRCT Warrick Score and DLCO%pred.
The ROC curve analysis showed that a B-line score of 3 or more was the best cut-off point to discriminate patients with RILS (Warrick score ≥ 7) (Figure 4). This value represented the best compromise between sensitivity (94.16%) and specificity (81.82%). The corresponding negative and positive predictive values were 94.74 and 80.11%, respectively, and the AUC was 0.92.
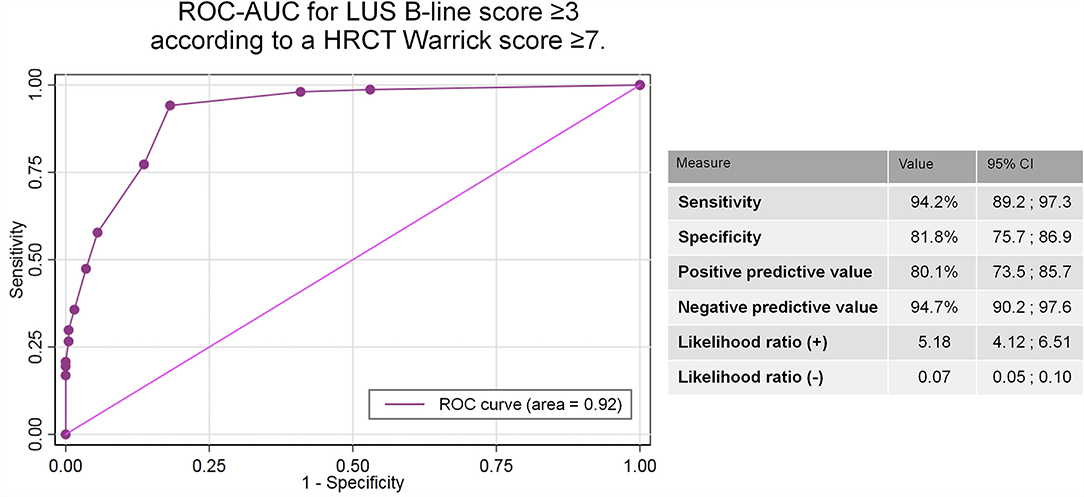
Figure 4. AUC-ROC to determine the LUS B-line score ability to discriminate patients with relevant interstitial lung sequelae after COVID-19 according to a HRCT Warrick score ≥ 7.
The B-line score showed excellent inter-observer agreement with a kappa value of 0.90 (95% CI 0.86–0.94). Detection of pleural-line abnormalities showed a poor inter-observer agreement, with a kappa index of 0.48 (95% CI 0.41–0.56).
Discussion
To our knowledge, this is the first large study focusing on the role of LUS for the evaluation of early interstitial sequelae in COVID-19 survivors. The presence of pathological B-lines showed excellent ability to discriminate these persistent abnormalities in comparison with HRCT, supporting the use of LUS as a first-line procedure to rule out post-COVID-19 lung sequelae.
We report the follow-up findings for 352 patients evaluated 2–5 months after hospitalization for COVID-19 pneumonia. A high prevalence of functional and radiological sequelae was observed in our population, likely due to the high proportion of severe pneumonia cases. Indeed, data from larger series support the same prevalence rates of persistent radiological abnormalities (11–15), including fibrotic changes, in almost 35% of the severe cases (13). Similarly, lung function impairment, particularly decreased DLCO, has also been widely reported (22 to 82% of patients) and seems to be related to the severity of the pneumonia episode (14–16).
The natural history of COVID-19 lung sequelae is still unknown, and it is unclear whether full recovery can be expected in all cases. In addition, long COVID is another clinical entity that adds complexity to these uncertainties, as affected patients can manifest persistent respiratory symptoms without evidence of radiological or functional abnormalities on usual explorations (45, 46). As this new condition requires a complete investigation of potential pulmonary and extra-pulmonary complications, the presence of pulmonary sequelae should be ruled out.
Therefore, effective diagnostic tests are required for a correct identification and monitoring of patients with post-COVID-19 interstitial lung sequelae. Considering the immensely large population affected, an easy, low-cost, and reproducible diagnostic procedure is crucial to manage this clinical challenge. The belief that LUS could be useful for this purpose motivated the present study.
To date, only one report of 38 patients has described the use of LUS for detection of COVID-19 lung sequelae compared to HRCT (47). In this study, LUS results showed a high agreement rate compared to HRCT, but also a high proportion of false-negative findings in patients with milder forms.
In our study, 352 patients underwent complete LUS exploration of all intercostal spaces, and the findings were quantified in a 12-area score. We searched for the presence of a “lung interstitial syndrome” pattern, which was defined by the presence of multiple B-lines (44). These artifacts have very low specificity since they are present in different diseases, but they have high sensitivity, particularly in the detection of ILD (32–34). Various methods have been proposed for the evaluation of this pattern, and the reliability of these methods remains a topic of debate (48, 49). Quantification of the total number of B-lines has been extensively used (32–34); however, some authors have reported relevant variabilities among transducers and raters which could cause an important bias (50, 51). Semi-quantitative methods based on visual estimation of the percentage of space occupied by B-lines have also been proposed (52), but they probably lead to similar disadvantages. The application of traditional aeration LUS scores is also controversial in ILD, as the grade of deaireation has not proved to be able to discriminate between different degrees of interstitial involvement (53).
In our report, we implemented a simplified method since our goal was to discriminate patients with potential interstitial lung sequelae after COVID-19 and not to evaluate the grade or type of abnormalities. Based on the definition of the ICC-LUS (44), we considered pathological areas as those with more than two B-lines, and each area was scored 1 point out of a total of 12 thoracic areas. This score was strongly correlated with the HRCT Warrick score and showed excellent inter-observer reliability. Furthermore, a score ≥ 3 showed high sensitivity and specificity values (94.2 and 81.8%, respectively) and a negative predictive value of 94.7%. These solid results suggest that normal LUS examinations could rule out the presence of ILD in COVID-19 survivors, avoiding the need for additional diagnostic tests such as HRCT.
Pleural line abnormalities such as thickening and fragmentation have also been described as useful sonographic signs for the diagnosis of ILD. Various studies in the last decade have shown that pleural line measurements could be particularly accurate in ruling out pulmonary fibrosis (34, 35, 53). Pleural line abnormalities were frequent in our cohort, especially in the RILS group. However, we did not perform a pleural line measurement; therefore, our evaluation was subjective and derived on a poor inter-observer reliability. For these reasons, we did not include this finding in our score nor did we attempt to evaluate its diagnostic accuracy. Further studies are required to evaluate the significant pleural alterations identified by LUS in these patients.
Early identification of persistent post-COVID-19 interstitial sequelae seems to be crucial, particularly since it may facilitate prompt initiation of treatments to prevent permanent fibrotic changes. Furthermore, given the increasing number of cases worldwide, a diagnostic test available for large populations is essential. The technical characteristics of LUS seem suitable for this purpose since sonography is low-cost, non-ionizing, repeatable, and reproducible in outpatient clinics. Moreover, expertise and skills in LUS can be obtained with a short training trajectory (54), and the technique can be implemented in primary care to reach larger populations. Our report suggests that LUS yields high diagnostic accuracy for the detection of post-COVID-19 early sequelae. In particular, its high sensitivity and negative predictive values support its use as a first-line procedure to rule out these abnormalities in a potentially large population of patients. LUS implementation as a first-line examination could reduce the use of HRCT and help select patients who require more intensive follow-up, thereby improving the efficiency of health care assistance.
Strengths and Limitations
The present study has some remarkable strengths. First, it is the largest prospective cohort published for this objective. Patients were recruited consecutively, and the same complete protocol was performed in a short time period. HRCT images, considered as the gold-standard, were evaluated by two independent thoracic radiologists, and in cases with significant differences, both radiologists met and performed a third consensual assessment. In addition, LUS operators were blinded to the clinical and radiological data and achieved excellent interobserver agreement. Finally, this was a reproducible and real-life study, since LUS was performed in the outpatient clinic by pulmonologists.
Yet, as in any study, there are some limitations. The order of follow-up visits was based on disease severity, potentially causing a relevant bias in the descriptive analysis. Consequently, the study population included a low percentage of mild cases, since many patients in this group had still not visited for follow-up assessments when we stopped study recruitment. However, none of these limitations, which are typical of a real-life study, influenced the primary objective. Another limitation is that we used the Warrick score, which has been validated in scleroderma-related ILD, to grade HRCT abnormalities because of the absence of any other specific score. Moreover, a Warrick cut-off point of ≥7 could lead to the underdiagnosis of milder forms of ILD. In our favor, it is likely that minor abnormalities are not clinically relevant in COVID-19 sequelae, since they could represent an intermediate step toward full recovery. In addition, this score has been widely applied in previous LUS reports of other ILDs and includes the main interstitial abnormalities found in COVID-19 survivors. Nevertheless, more studies are needed to describe how these lesions will evolve over time and whether LUS will continue to play a role in their detection.
Conclusions
LUS could be implemented as a first-line procedure in the evaluation of interstitial lung sequelae after COVID-19 pneumonia. The identification of pathological B-lines in a twelve-area score showed a high negative predictive value for the detection of these abnormalities. Consequently, a normal LUS examination could rule out the presence of ILD in COVID-19 survivors, avoiding the need for additional diagnostic tests such as HRCT.
Data Availability Statement
The datasets presented in this article are not readily available because approval from the relevant authorities is required. Requests to access the datasets should be directed to ZGNsb2ZlbnRAdmhlYnJvbi5uZXQ=.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Ethics Committee of Vall d'Hebron Barcelona University Hospital [PR(AG)461/2020]. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
DC is the guarantor of the paper and takes full responsibility for the content of the manuscript, including data and analysis. DC, MC, and EP conceived and designed the study, analyzed the data, and drafted the manuscript. Statistical analysis was performed by Santiago Pérez-Hoyos. DC, AF, GG, and MA performed lung ultrasound examinations in all patients. JA, AS, DV, LC, and JE conducted the chest HRCT examinations in all patients. XM, AA, and KL critically reviewed the manuscript for relevant intellectual content. All authors approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to acknowledge the contributions of Cristina Berastegui, Miriam Barrecheguren, José Cardoso, Maria Jesús Cruz, David Espejo, Antia Ferreiro, Jaume Ferrer, M. Ángeles Jiménez, Manuel López, Íñigo Ojanguren, Jeisson Osorio, Mercedes Pallero, Florencia Pilia, Ma Antonia Ramon, Eva Revilla, Christian Romero, Berta Sáez, Maria Sáez, Júlia Sampol, Eduardo Vélez, and Ana Villar, who were members of the Se-COVID-19 team. The Se-COVID-19 team conducted clinical follow-up assessments of all patients. They requested for procedures and informed the patients of their results, applying the clinical measures that they deemed appropriate in each case. The authors would also like acknowledge the contributions of the Medicine Department of the Universitat Autònoma de Barcelona.
Abbreviations
ARDS, acute respiratory syndrome; AUC, area under the curve; BMI, body mass index; COVID-19, coronavirus disease 2019; CT, computed tomography; CXR, chest radiography; DLCO, carbon monoxide diffusing capacity; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; GGO, ground-glass opacity; HFO, high-flow oxygen; HRCT, high resolution computed tomography; ICU, intensive care unit; IQR, inter-quartile range; ILD, interstitial lung disease; IMV, invasive mechanical ventilation; LFO, low-flow oxygen; LUS, lung ultrasound; MERS, middle east respiratory syndrome coronavirus; NIMV, non-invasive mechanical ventilation; PF, pulmonary fibrosis; PFT, pulmonary function tests; RILS, relevant interstitial lung sequelae; SARS-CoV, severe acute respiratory syndrome coronavirus; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SD, standard deviation.
References
1. WHO. Available online at: https://covid19.who.int/ (accessed November 10, 2021).
2. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. (2020) 324:782–93. doi: 10.1001/jama.2020.12839
3. Cevik M, Kuppalli K, Kindrachuk J, Peiris M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ. (2020) 371:m3862. doi: 10.1136/bmj.m3862
4. Yelin D, Wirtheim E, Vetter P, Kalil AC, Bruchfeld J, Runold M, et al. Long-term consequences of COVID-19: research needs. Lancet Infect Dis. (2020) 20:1115–7. doi: 10.1016/S1473-3099(20)30701-5
5. Cheung OY, Chan JW, Ng CK, Koo CK. The spectrum of pathological changes in severe acute respiratory syndrome (SARS). Histopathology. (2004) 45:119–24. doi: 10.1111/j.1365-2559.2004.01926.x
6. Ketai L, Paul NS, Wong KT. Radiology of severe acute respiratory syndrome (SARS): the emerging pathologic-radiologic correlates of an emerging disease. J Thorac Imaging. (2006) 21:276–83. doi: 10.1097/01.rti.0000213581.14225.f1
7. Tse GM, To KF, Chan PK, Lo AW, Ng KC, Wu A, et al. Pulmonary pathological features in coronavirus associated severe acute respiratory syndrome (SARS). J Clin Pathol. (2004) 57:260–5. doi: 10.1136/jcp.2003.013276
8. Ng CK, Chan JW, Kwan TL, To TS, Chan YH, Ng FY et al. Six month radiological and physiological outcomes in severe acute respiratory syndrome (SARS) survivors. Thorax. (2004) 59:889–91. doi: 10.1136/thx.2004.023762
9. Hui DS, Wong KT, Ko FW, Tam LS, Chan DP, Woo J, et al. The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors. Chest. (2005) 128:2247–61. doi: 10.1378/chest.128.4.2247
10. Carfì A, Bernabei R, Landi F. Persistent symptoms in patients after acute COVID-19. JAMA. (2020) 324:603–5. doi: 10.1001/jama.2020.12603
11. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
12. Wang Y, Dong C, Hu Y, Li X, Ren L, Gu X, et al. Temporal changes of CT findings in 90 patients with COVID-19 pneumonia: a longitudinal study. Radiology. (2020) 296:E55–64. doi: 10.1148/radiol.2020200843
13. Han X, Fan Y, Alwalid O, Li N, Jia X, Yuan M, et al. Six-month follow-up chest CT findings after severe COVID-19 pneumonia. Radiology. (2021) 299:E177–86. doi: 10.1148/radiol.2021203153
14. Guler SA, Ebner L, Aubry-Beigelman C, Bridevaux PO, Brutsche M, Clarenbach C, et al. Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J. (2021) 57:2003690. doi: 10.1183/13993003.03690-2020
15. González J, Benítez ID, Carmona P, Santisteve S, Monge A, Moncusí-Moix A, et al. Pulmonary function and radiologic features in survivors of critical COVID-19: a 3-month prospective cohort. Chest. (2021) 160:187–98. doi: 10.1016/j.chest.2020.12.057
16. Mo X, Jian W, Su Z, Chen M, Peng H, Peng P, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J. (2020) 55:2001217. doi: 10.1183/13993003.01217-2020
17. Culebras M, Loor K, Sansano I, Persiva Ó, Clofent D, Polverino E, et al. Se-COVID-19 team. Histological findings in transbronchial cryobiopsies obtained from patients after COVID-19. Chest. (2021) 25:S0012-3692(21)04053-8. doi: 10.1016/j.chest.2021.09.016
18. Zheng Z, Yao Z, Wu K, Zheng J. Patient follow-up after discharge after COVID-19 pneumonia: considerations for infectious control. J Med Virol. (2020) 92:2412–9. doi: 10.1002/jmv.25994
19. Raghu G, Wilson KC. COVID-19 interstitial pneumonia: monitoring the clinical course in survivors. Lancet Respir Med. (2020) 8:839–42. doi: 10.1016/S2213-2600(20)30349-0
20. George PM, Barratt SL, Condliffe R, Desai SR, Devaraj A, Forrest I, et al. Respiratory follow-up of patients with COVID-19 pneumonia. Thorax. (2020) 75:1009–16. doi: 10.1136/thoraxjnl-2020-215314
21. Sibila O, Molina-Molina M, Valenzuela C, Ríos-Cortés A, Arbillaga-Etxarri A, García YT. Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) consensus for post-COVID-19 clinical follow-up. Open Respir Arch. (2020) 2:278–83. doi: 10.1016/j.opresp.2020.09.002
22. Rubin GD, Ryerson CJ, Haramati LB, Sverzellati N, Kanne JP, Raoof S, et al. The role of chest imaging in patient management during the COVID-19 pandemic: a multinational consensus statement from the Fleischner society. Chest. (2020) 158:106–16. doi: 10.1148/radiol.2020201365
23. Bai C, Chotirmall SH, Rello J, Alba GA, Ginns LC, Krishnan JA, et al. Updated guidance on the management of COVID-19: from an American Thoracic Society/European Respiratory Society coordinated International Task Force (29 July 2020). Eur Respir Rev. (2020) 29:200287. doi: 10.1183/16000617.0287-2020
24. Karthika M, Wong D, Nair SG, Pillai LV, Mathew CS. Lung ultrasound: the emerging role of respiratory therapists. Respir Care. (2019) 64:217–29. doi: 10.4187/respcare.06179
25. Bouhemad B, Zhang M, Lu Q, Rouby JJ. Clinical review: bedside lung ultrasound in critical care practice. Crit Care. (2007) 11:205. doi: 10.1186/cc5668
26. Lichtenstein DA. BLUE-protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill. Chest. (2015) 147:1659–70. doi: 10.1378/chest.14-1313
27. Gao YQ, Qiu RX, Liu J, Zhang L, Ren XL, Qin SJ. Lung ultrasound completely replaced chest X-ray for diagnosing neonatal lung diseases: a 3-year clinical practice report from a neonatal intensive care unit in China. J Matern Fetal Neonatal Med. (2020) 9:1–8. doi: 10.1080/14767058.2020.1830369
28. Bonadia N, Carnicelli A, Piano A, Buonsenso D, Gilardi E, Kadhim C, et al. Lung ultrasound findings are associated with mortality and need for intensive care admission in COVID-19 patients evaluated in the emergency department. Ultrasound Med Biol. (2020) 46:2927–37. doi: 10.1016/j.ultrasmedbio.2020.07.005
29. Biasucci DG, Buonsenso D, Piano A, Bonadia N, Vargas J, Settanni D, et al. Lung ultrasound predicts non-invasive ventilation outcome in COVID-19 acute respiratory failure: a pilot study. Minerva Anestesiol. (2021) 87:1006–16. doi: 10.23736/S0375-9393.21.15188-0
30. Torres-Macho J, Sánchez-Fernández M, Arnanz-González I, Tung-Chen Y, Franco-Moreno AI, Duffort-Falcó M, et al. Prediction accuracy of serial lung ultrasound in COVID-19 hospitalized patients (Pred-Echovid Study). J Clin Med. (2021) 10:4818. doi: 10.3390/jcm10214818
31. Volpicelli G, Gargani L, Perlini S, Spinelli S, Barbieri G, Lanotte A, et al. Lung ultrasound for the early diagnosis of COVID-19 pneumonia: an international multicenter study. Intensive Care Med. (2021) 47:444–54. doi: 10.1007/s00134-021-06373-7
32. Doveri M, Frassi F, Consensi A, Vesprini E, Gargani L, Tafuri M, et al. Ultrasound lung comets: new echographic sign of lung interstitial fibrosis in systemic sclerosis. Reumatismo. (2008) 60:180–4. doi: 10.4081/reumatismo.2008.180
33. Gargani L, Doveri M, D'Errico L, Frassi F, Bazzichi ML, Delle Sedie A, et al. Ultrasound lung comets in systemic sclerosis: a chest sonography hallmark of pulmonary interstitial fibrosis. Rheumatology. (2009) 48:1382–7. doi: 10.1093/rheumatology/kep263
34. Barskova T, Gargani L, Guiducci S, Randone SB, Bruni C, Carnesecchi G, et al. Lung ultrasound for the screening of interstitial lung disease in very early systemic sclerosis. Ann Rheum Dis. (2013) 72:390–5. doi: 10.1136/annrheumdis-2011-201072
35. Sperandeo M, De Cata A, Molinaro F, Trovato FM, Catalano D, Simeone A, et al. Ultrasound signs of pulmonary fibrosis in systemic sclerosis as timely indicators for chest computed tomography. Scand J Rheumatol. (2015) 44:389–98. doi: 10.3109/03009742.2015.1011228
36. Manolescu D, Oancea C, Timar B, Traila D, Malita D, Birsasteanu F, et al. Ultrasound mapping of lung changes in idiopathic pulmonary fibrosis. Clin Respir J. (2020) 14:54–63. doi: 10.1111/crj.13101
37. Tardella M, Gutierrez M, Salaffi F, Carotti M, Ariani A, Bertolazzi C, et al. Ultrasound in the assessment of pulmonary fibrosis in connective tissue disorders: correlation with high-resolution computed tomography. J Rheumatol. (2012) 39:1641–7. doi: 10.3899/jrheum.120104
38. Miller MR, Hankinson J, Brusasco V, urgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. (2005) 26:319–38. doi: 10.1183/09031936.05.00034805
39. Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. (2012) 40:1324–43. doi: 10.1183/09031936.00080312
40. Stanojevic S, Graham BL, Cooper BG, Thompson BR, Carter KW, Francis RW, et al. Official ERS technical standards: global Lung Function Initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur Respir J. (2017) 50:1700010. doi: 10.1183/13993003.00010-2017
41. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. (2008) 246:697–722. doi: 10.1148/radiol.2462070712
42. Warrick JH, Bhalla M, Schabel SI, Silver RM. High resolution computed tomography in early scleroderma lung disease. J Rheumatol. (1991) 18:1520–8.
43. Diot E, Boissinot E, Asquier E, Guilmot JL, Lemarié E, Valat C, et al. Relationship between abnormalities on high-resolution CT and pulmonary function in systemic sclerosis. Chest. (1998) 114:1623–9. doi: 10.1378/chest.114.6.1623
44. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. (2012) 38:577–91. doi: 10.1007/s00134-012-2513-4
45. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. London: National Institute for Health and Care Excellence (UK) (2020).
46. Crook H, Raza S, Nowell J, Young M, Edison P. Long covid-mechanisms, risk factors, and management. BMJ. (2021) 374:n1648. doi: 10.1136/bmj.n1648
47. Giovannetti G, De Michele L, De Ceglie M, Pierucci P, Mirabile A, Vita M, et al. Lung ultrasonography for long-term follow-up of COVID-19 survivors compared to chest CT scan. Respir Med. (2021) 181:106384. doi: 10.1016/j.rmed.2021.106384
48. Sperandeo M, Trovato GM, Catalano D. Quantifying B-lines on lung sonography: insufficient evidence as an objective, constructive, and educational tool. J Ultrasound Med. (2014) 33:362–5. doi: 10.7863/ultra.33.2.362
49. Corradi F, Via G, Forfori F, Brusasco C, Tavazzi G. Lung ultrasound and B-lines quantification inaccuracy: B sure to have the right solution. Intensive Care Med. (2020) 46:1081–3. doi: 10.1007/s00134-020-06005-6
50. Haaksma ME, Smit JM, Heldeweg MLA, Pisani L, Elbers P, Tuinman PR. Lung ultrasound and B-lines: B careful. Intensive Care Med. (2020) 46:544–5. doi: 10.1007/s00134-019-05911-8
51. Quarato CMI, Verrotti DI Pianella V, Sperandeo M. Count of B-lines: a matter with persistent limitations. J Rheumatol. (2020) 47:158–9. doi: 10.3899/jrheum.190823
52. Gargani L. Lung ultrasound: a new tool for the cardiologist. Cardiovasc Ultrasound. (2011) 9:6. doi: 10.1186/1476-7120-9-6
53. Lacedonia D, Scioscia G, Giardinelli A, Quarato CMI, Sassani EV, Foschino Barbaro MP, et al. The role of transthoracic ultrasound in the study of interstitial lung diseases: high-resolution computed tomography versus ultrasound patterns: our preliminary experience. Diagnostics. (2021) 11:439. doi: 10.3390/diagnostics11030439
Keywords: COVID-19, SARS-CoV-2, lung ultrasound (LUS), ultrasonography, pulmonary sequelae, interstitial lung disease (ILD)
Citation: Clofent D, Polverino E, Felipe A, Granados G, Arjona-Peris M, Andreu J, Sánchez-Martínez AL, Varona D, Cabanzo L, Escudero JM, Álvarez A, Loor K, Muñoz X and Culebras M (2022) Lung Ultrasound as a First-Line Test in the Evaluation of Post-COVID-19 Pulmonary Sequelae. Front. Med. 8:815732. doi: 10.3389/fmed.2021.815732
Received: 15 November 2021; Accepted: 20 December 2021;
Published: 13 January 2022.
Edited by:
Rodrigo Torres-Castro, University of Chile, ChileReviewed by:
Jing Liu, Beijing Chaoyang District Maternal and Child Healthcare Hospital, ChinaEmanuele Pivetta, Città Della Salute e Della Scienza University Hospital, Italy
Danilo Buonsenso, Catholic University of the Sacred Heart, Italy
Copyright © 2022 Clofent, Polverino, Felipe, Granados, Arjona-Peris, Andreu, Sánchez-Martínez, Varona, Cabanzo, Escudero, Álvarez, Loor, Muñoz and Culebras. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eva Polverino, ZXZhLnBvbHZlcmlub0B2aGlyLm9yZw==