
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 27 January 2022
Sec. Rheumatology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.808608
This article is part of the Research Topic Rheumatic Diseases and Infection View all 7 articles
 Borja Del Carmelo Gracia1Luis Sáez2Lucio Pallarés3Jose Velilla2Adela Marín1Luis Martinez-Lostao4Carmen Pilar Simeón5
Borja Del Carmelo Gracia1Luis Sáez2Lucio Pallarés3Jose Velilla2Adela Marín1Luis Martinez-Lostao4Carmen Pilar Simeón5 Patricia Fanlo6*
Patricia Fanlo6*Objectives: COVID-19 outcomes in population with systemic autoimmune diseases (SAD) remain poorly understood. The aim was to examine demographic and clinical factors associated with COVID-19 infection in people with rheumatic disease.
Methods: Two phases cross-sectional survey of individuals with rheumatic disease in April 2020 and October 2020. COVID infection, severity of disease, age, sex, smoking status, underlying rheumatic disease diagnosis, comorbidities and rheumatic disease medications taken immediately prior to infection were analyzed.
Results: A total of 1,529 individuals with autoimmunity disease diagnosis were included. Out of 50 positive patients, 21 required telephone medical assistance, 16 received assessment by primary care physician, 9 were evaluated in Emergency Department and 4 patient required hospitalization. Multivariate analysis was performed without obtaining differences in any of the systemic autoimmune diseases. Regarding the treatments, significant differences were found (p 0.011) in the treatment with anti-TNF-alpha agents with OR 3.422 (1.322–8.858) and a trend to significance (p 0.094) was observed in patients receiving mycophenolate treatment [OR 2.016 (0.996–4-081)].
Conclusions: Anti-TNF-alpha treatment was associated with more than 3-fold risk of suffering from SARS-CoV-2 infection, although in all cases infection was mild. Cumulative incidence in patients with SAD was up to 5 times higher than general population but with great differences between autoimmune diseases.
- Cumulative incidence of SARS-CoV-2 infection in autoimmune population is up to five times higher than general population.
- Anti-TNF-alpha treatment may be associated with a more than 3-fold risk of suffering from SARS-CoV-2 infection.
In 12 March 2020, the World Health Organization (WHO) declared the global outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease 2019 (COVID-19) a pandemic. The main symptoms of respiratory infection include fever and cough in 88.5 and 68.6% of the patients, respectively (1–3). The presence and the number of comorbidities (e.g., arterial hypertension, coronary heart disease), age and lifestyle factors such as smoking appear to have deteriorating effects on the course of the infection (3).
COVID-19 is a serious disease in different groups of patients, and today we know that this severity is due to the hypersensitivity immune response that the virus produces at the pulmonary and systemic level.
Secondary to the presence of comorbidities and mechanism of immune hyperresponsiveness, patients with systemic autoimmunity diseases (SAD) may face a particular risk as their disease. On one side, these patients may be associated with an increased risk of infections due to immunosuppression (4, 5) and on the other, immunosuppression itself can positively or negatively alter the abnormal immune response that seems to be responsible for the most severe disease complications such as interstitial pneumonia (6).
Due to robust knowledge of the course of SARS-CoV-2 infection in patients with SAD is scarce, scientific evidence-based recommendations for the management of COVID-19 in patients with rheumatic disorders and anti-rheumatic treatments are limited (7).
The Spanish group of Autoimmunity diseases (GEAS) developed at an early-stage first concise recommendations for the management of patients with SAD during the COVID- 19 pandemic. Interruption or reduction of immunosuppressive treatment was not recommended as this might result in relapses or flares, that consequently could require the increase of amount of immunosuppressive therapy (e.g., additional glucocorticoids and/or immunosuppressive therapy).
Incidence, course of COVID-19 and including lethal outcomes, vary considerably in different cohorts according to pre-existing conditions and healthcare systems. Investigation of special disease groups may contribute to a better understanding of the role of the immune system regarding the risk to get infected or to develop a more severe course of COVID-19. Based on the clinical information published to date from the outbreak caused by coronaviruses, there is no overwhelming evidence that patients with rheumatic diseases are at an increased risk compared with other kinds of patients (8–10).
Therefore, patients with SAD, who are treated with different types, combinations and dosages of immunomodulatory therapies represent an interesting population to collect data regarding SARS- CoV-2 infection.
Registries with a large number of case reports are required to answer the question of whether antirheumatic drugs increase or decrease the risk for a severe course of SARS-CoV-2 infection. As necessary data cannot be extracted from clinical charts or health insurance records, GEAS decided to establish a web-survey, which allows a rapid and timely collection of patient information of autoimmunity patients in real life in Spain. This web-survey let us to analyze the real incidence and clinical course of SARS-CoV-2 infections in patients, developing a guidance for the management of SAD patients during the COVID-19 pandemic and being able to lead future researches based on the obtained results.
This cross-sectional study was performed by GEAS and was approved by the local Ethics Committee. All outpatients with SAD were eligible. In cooperation with biostatisticians and data-protection specialists to ensure mutual understanding of research objectives and scientifically and legally appropriate data collection, a database-driven online questionnaire was developed and launched on 16 April 2020 known as COVID-GEAS-1. This survey used the google form platform and the target population was patients with SAD. It remained open for 2 weeks and consisted of 28 items on demographic data, systemic autoimmune disease, symptomatology, evolution and healthcare needs, contact with other COVID patients, diagnosis of COVID by nasal swab and other concomitant treatments.
The same online survey (COVID-GEAS-2) was sent on 5 October opened for a period of 15 days.
The database includes nationality, age, detailed rheumatological diagnosis, antirheumatic medication at time of study and changes in the last 3 months. In addition, the contact with COVID patients as well as conducting diagnostic tests and the course and outcome of the SARS-CoV-2 infection are also key parameters. Missing data on diagnosis, outcome and therapies can be queried by directly contacting by mail. Periodic critical evaluation of the registry is carried out by the task force to ensure that the objectives are being met.
In the first survey, only nasopharyngeal swab was included as a diagnosis. In the second cut, the fast antibody test and serological test were included.
Data entered in an electronic case report form with the URL https://es.surveymonkey.com/r/encuestaGEAScovid19 are directly stored by survey-monkey database into an SQL-database on a dedicated server located in Spain and certified according to DIN ISO/IEC 27001 using encryption and secure communication protocols (SSL/TLS and HTTPS). Data entered in these forms are checked for plausibility immediately. Web-forms use dynamic menus and subquestions. Data allowing for identification of individual patients are omitted, and reidentification is only possible via local files. Aragon's ethics committee authorized the survey and it was approved by the Spanish Agency for Medicines and Health Products (AEMPS).
The survey was addressed to national and regional associations of systemic autoimmune diseases such as Systemic Lupus Erythematosus (SLE), Bechet, Scleroderma, Sarcoidosis, APS, and Sjögren's syndrome. Most of them have been informed directly using established dissemination channels of the GEAS. Other systems as twitter and Facebook were used as dissemination channels.
The prevalence of SARS-CoV-2 infection was expressed as the percentage [with 95% confidence interval (CI)] of cases with SARS-CoV-2 infection confirmed by nasopharyngeal swab, fast test and/or serological test on the total number of patients included in the study. The proportion of patients with confirmed SARS-CoV-2 infection in our cohort was compared to those reported for the general population of Spain, using the Fisher exact test. Statistical significance was defined as P < 0.05.
The proportion of patients with confirmed SARS-CoV-2 infection in our cohort was compared to those reported for the general population of Spain, using the Pearson test. Statistical significance was defined as P < 0.05. Analysis was performed descriptively using SPSS Statistics v 25.00.
On 16th of April 2020, the first survey (COVID-GEAS-1) was sent to all SAD association partners, regardless of their treatment, collecting a total of 1,140 responses in a mean time of 8 days (3–13 days). The objective of this survey was to know the association of COVID with SAD patients at the worst epidemic moment of the pandemic in Spain as well as the incidence and severity of the COVID-19. Most patients were female (90.96%); the median age was 45.3 ± 11.4 years. According to the distribution by systemic autoimmune disease, 563 patients (49.3%) had been diagnosed of SLE, 179 (15.7%) SC, 248 (21.8%) SS, 198 APS, 72 SA, 68 BD, 61 vasculitis (VAS), and 35 patients were diagnoses of rheumatoid arthritis (RA).
Regarding the treatment, 666 patients had started hydroxychloroquine treatment at least 3 months prior to the survey and 512 were under active treatment with corticosteroids with a mean dose of 6.18 ± 4.67 mg/day. A total of 458 patients added one or more immunosuppressive agent: 105 patients azathioprine, 165 mycophenolate, 9 cyclophosphamide, 155 methotrexate, 11 leflunomide, 36 tacrolimus and 18 cyclosporine A. Biological treatment had been used in 155 patients in the last 6 months; 52 of them Rituximab, 47 belimumab, 9 tocilizumab, 38 anti-TNF-alpha and other biological treatments in 10 more cases.
At the time of the survey, 80 patients had reported a previous close contact with symptomatic patients and 35 patients with confirm COVID-19 patients. Twenty-four patients presented symptoms compatible with COVID-19 and 101 patients had undergone SARS-CoV-2 test a maximum of 15 days before with 19 positive results (21.6%). A 26.3% (5) of the total positives were asymptomatic. A total of 20 patients required health care, 4 were followed by telephone, 6 required to see their primary care physician, 6 were admitted to the emergency department and 4 required hospital admission, one of them entered to intensive care unit.
The second survey (COVID-GEAS-2) was sent on 5th of October 2020 with a total of 389 responses with the same objective as COVID-GEAS-1 and mean time of responses was 9 days (range 1–26 days). Similarly, many of the patients were women (92.55%) with a mean age of 40 years. A total of 120 patients (30.8%) were diagnosed of SLE, 81 (20.8%) SC, 132 (33.9%) SS, 26 APS, 4 BD, 49 SA, 12 VAS, and 9 RA. Regarding treatment, 135 patients were on immunosuppressive treatment: 25 azathioprine, 47 mycophenolate, 52 methotrexate, 5 leflunomide, 6 cyclosporine A and 1 patient with cyclophosphomide. A total of 49 patients associated biological treatment, 11 rituximab, 13 belimumab, 3 tocilizumab, 16 anti-TNF-alpha and 6 other biological therapies. Of the total of participants, 28 had presented close contact with people with compatible symptoms, 8 of them with COVID-positive patients. A total of 196 tests were performed with 31 positives (8%). Of the positive patients, 21 were asymptomatic, 17 required telephone medical assistance, 10 received assessment by primary care physician, 3 were evaluated in Emergency Department and 1 patient required hospitalization.
Regarding the global characteristics of the two surveys, a total of 1,360 patients (91.1%) were Caucasian and 114 (7.6%) Hispanic. The rest, 19 patients (1.3%), were classified in other ethnicities. According to the distribution by regions, 336 (22.9%) of the patients lived in Madrid, 188 (12.8%) Andalucía, 181 (12.3%) Cataluña, 116 (7.9%) Valencia, 110 (7.5%) Castilla y León, 94 (6.4%) Aragón, 83 (5.7%) Galicia, 77 (5.2%) Navarra, 56 (3.8%) País Vasco, 44 (3%) Asturias, 42 (2.9%) Murcia, 41 (2.8%) Castilla La Mancha, 33 (2.2%) Canarias, 33 (2.2%) Baleares, 30 (2%) Cantabria, 15 (1%) Baleares, 13 (0.9%) Extremadura and 8 (0.5%) La Rioja.
The demographic, clinical, diagnosis and therapies data from both surveys were compared, with the results shown in Table 1.
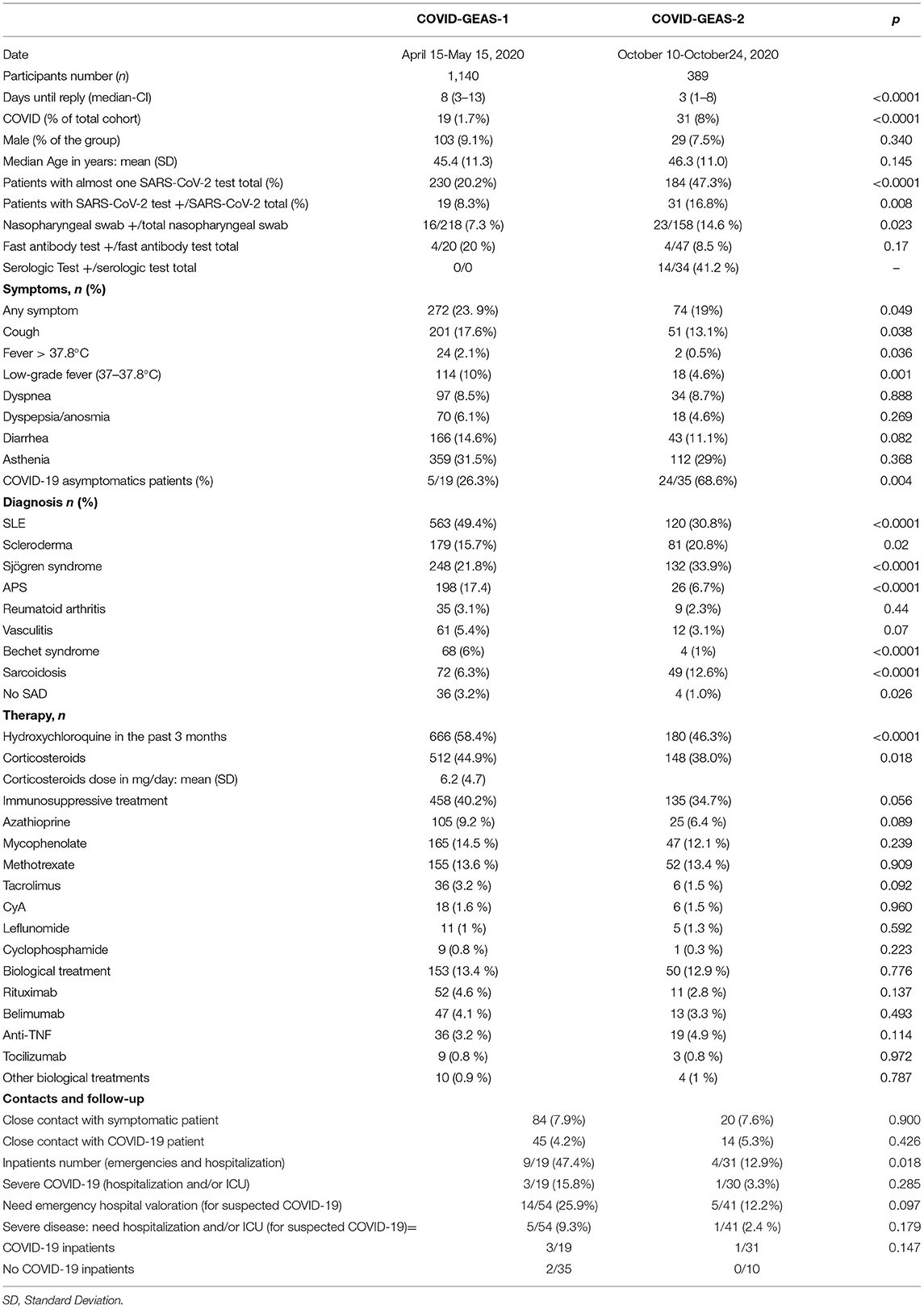
Table 1. Demographic data, clinical characteristics and treatment of the patients of the two surveys.
The joint cumulative incidence of the two surveys was analyzed and compared with the total cumulative incidence in Spain, obtaining results 3.925 times higher in the group of patients with systemic autoimmune diseases (Figure 1).
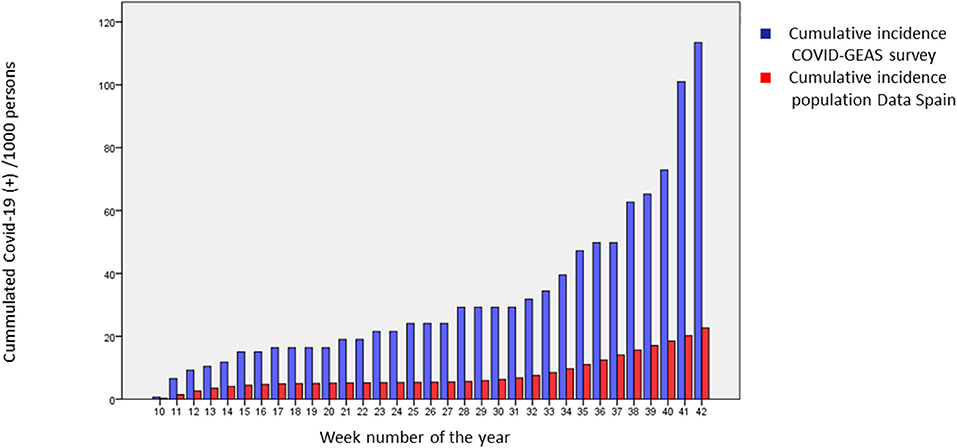
Figure 1. Comparative between cumulative incidence of Spain and COVID-GEAS survey. The proportion of patients with confirmed SARS-CoV-2 infection in our cohort was compared to those reported for the general population of Spain, using the Pearson test.
The patients diagnosed with SARS-CoV-2 infection were jointly analyzed because there were no significant differences in the survival curves (log rank 0.566). By ethnicity, 48 patients were Caucasian and 2 Hispanic. The data were compared with the patients without a confirmed diagnosis of COVID-19 obtaining the results shown in Table 2.
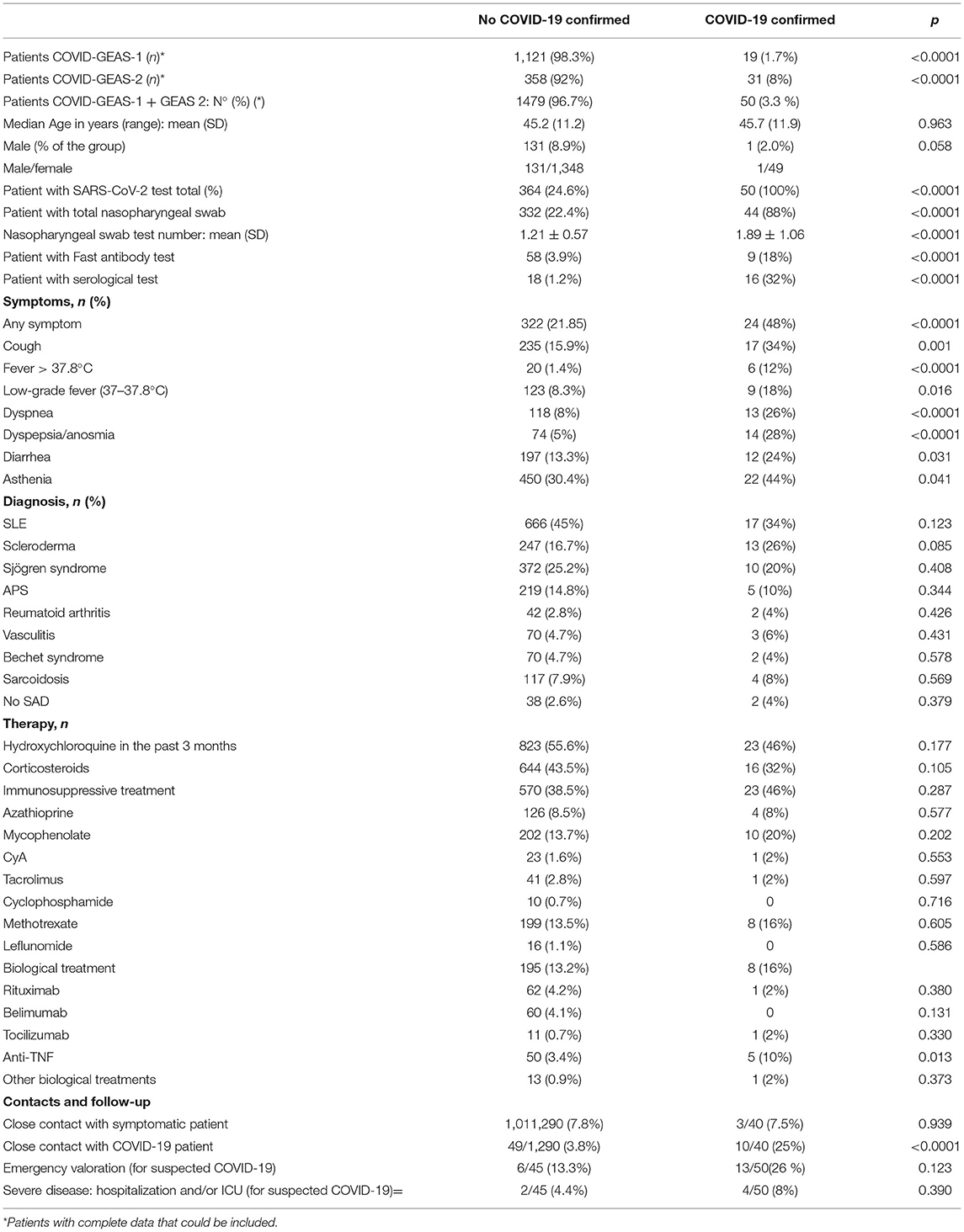
Table 2. Comparison of patients diagnosed with SARS-CoV-2 infection.
The 50 patients diagnosed of COVID-19 infection were analyzed. A total of 17 patients (34%) were diagnosed of SLE, 13 (26%) SC, 10 (20%) SS, 5 APS (10%), 2 BD (4%), 2 RA (4%) and 2 did not meet established SAD criteria (4%). Regarding treatment, 23 patients were on hydroxychloroquine treatment (46%) and 16 patients on glucocorticoid treatment (32%). Of all patients infected by COVID-19 23 patients were on immunosuppressive treatment: 4 azathioprine, 10 mycophenolate, 8 methotrexate, 1 cyclosporine A, and 1 patient with tacrolimus. A total of 8 patients associated biological treatment, 1 with rituximab, 1 tocilizumab, 5 anti-TNF-alpha and 1 omalizumab. Regarding evolution, 24 did not need medical attention, 13 were evaluated in Emergency Department and 4 patients required hospitalization, one of them in intensive care unit.
Of the 17 patients who required some medical attention, all of them were women. The most frequent SAD was SLE in 6 patients (35.29%) followed by scleroderma in 5 (29.41%), Sjögren's syndrome in 3 (17.65%), 2 Sarcoidosis (11.76%) and one vasculitis (5.88%). A total of 10 (58.8%) patients were in active treatment with glucocorticoids (increasing to 100% of the patients who required hospitalization) and 9 (52.9%) in treatment with Hydroxychloroquine. Eleven patients (64.7%) were on immunosuppressive treatment, the most frequent mycophenolate with 6 patients (35.29%) and methotrexate in 4 patients (23.53%). Only one patient in the emergency department assistance group was under treatment with biological drugs. Detailed results are shown in Figure 2.
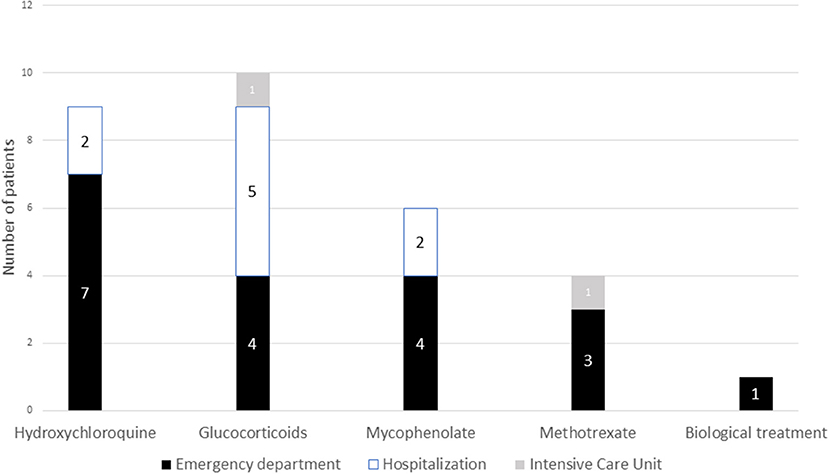
Figure 2. Association between the treatment of systemic autoimmune diseases and severity. Number of patients in each of the immunosuppressive treatments and type of need for hospital care.
Of the total of 666 patients with SLE analyzed, 17 (2.5%) had active infection by SARS-CoV-2. Of the 247 patients diagnosed with SC, 13 (5%) presented confirmation of infection during the follow-up period. In the subgroup of patients with SS, made up of 372 patients, 7 (1.8%) had active infection. Of the 219 patients with a diagnosis of APS, five patients had confirmed infection. Finally, of the rest of the patients analyzed (221) with other SAD, 9 patients presented active infection by SARS-CoV-2.
The cumulative incidence of COVID-19 for each of the SAD between weeks 10 and 42 of the 2020 was analyzed, obtaining the results obtained in Figure 3.

Figure 3. Cumulative incidence of COVID-19 for each of the SAD. Accumulated incidence in the weeks of 2020 for each of the autoimmune diseases. SLE, systemic lupus erythematosus; APS, antiphospholipid syndrome.
Multivariate analysis (COX regression) was performed without obtaining differences in any of the SAD. Regarding the treatments, significant differences were found (p 0.011) in the treatment with anti-TNF-alpha with OR 3.422 (1.322–8.858). Similarly, a trend to significance (p 0.094) was observed in patients receiving mycophenolate treatment [OR 2.016 (0.996–4-081)]. Of the 60 patients under active treatment with belimumab, none of them had confirmed SARS-CoV-2 infection.
In this study, SARS-CoV-2 infection was evaluated among 1,529 patients with SAD residing in Spain with an incidence of SARS-CoV-2 infection comparable to that observed in other European countries.
Global exact incidence and prevalence in Spain of systemic lupus erythematosus, scleroderma or systemic vasculitis actually is unknown but the incidence is possible <1% of the Spanish population.
The Spanish population reached on January 1, 2020 reached 47.4 million inhabitants. In relation to these data, in Spain there would be a total of almost half a million patients with a diagnosis of systemic autoimmune disease.
Although the sample of patients is small, we do understand that it can help to clarify whether or not this type of vulnerable population is at greater risk of contracting the infection.
Our results are consistent with the data in the literature so far available on COVID-19 and immunosuppressive treatment (4, 7, 11). If it is not protective, at least no warnings suggestive of a pejorative evolution of COVID-19 have been detected. However, these studies do not fully clarify whether or not patients with immunosuppressive therapy are at increased risk of developing severe forms of COVID-19 compared with the general population (12).
In our study, anti-TNF treatment was associated with a >3-fold risk of suffering from SARS-CoV-2 infection, although in all cases it was with mild symptoms. This could suggest that although the risk of infection with this immunosuppressive treatment appears to be higher, the severity of symptoms in all cases was mild, suggesting that the use of TNF-alpha inhibitors could be a potential treatment for acute respiratory failure caused by SARS-CoV-2 infection (13). Similarly, the use of mycophenolate showed a trend to significance with a risk increased twice, which would be similar to what is currently published. Although in vitro studies had showed promising results for mycophenolate against SARS-CoV-2 (14), the in vivo studies suggest that its use is likely to cause more harm than benefit and hence is not likely to be useful against coronavirus infections (15, 16). Interestingly, no case of SARS-CoV-2 infection was found in the group of patients with belimumab, which could suggest the possibility of the B lymphocyte having some role in SARS-CoV-2 infection. Woodruff et al. (17) found extrafollicular B cell activation in critically ill patients with COVID-19, similar to what has been observed in autoimmunity.
Pablos et al. (18) investigated the prevalence of COVID-19 in seven Spanish hospitals providing medical care for a population of 2.9 million patients and found a comparable prevalence of the infection in SS and SC showed a higher prevalence of SARS-CoV-2 infection in comparison with the general population; in contrast, prevalence in SLE patients was similar to that of the reference population.
Our study shows a cumulative incidence up to four times higher than the general population, although with large discrepancies in each of the autoimmune diseases, mainly due to patients' increased susceptibility to infections, the deeper immune-system impairment and favored by the high exposure to the virus at medical facilities before the restriction measures on individual movement (19). The higher prevalence of COVID-19 in SAD compared to that found in general population was further emphasized by some demographic observations; in particular, ASD patients showed lower mean age, as well as a higher percentage of females. These findings are in counter tendency with respect to the epidemiology of COVID-19 symptomatic patients, which are prevalently male, aged >60 years.
Similarly to the study previously mentioned, patients with SC showed a higher cumulative incidence, as well as patients with undifferentiated connective tissue disease and VAS. In contrast, patients with SS, SLE, and APS did not show a higher incidence. This unexpected discrepancy among SAD patients might be explained at least partly by the age, the higher proportion of females and the different treatment among autoimmunity diseases.
In Pablos et al. study (18), patients with autoimmune disease had an increased risk of intensive care/mechanical ventilation [adjusted OR for mechanical ventilation 3.11 (95% CI: 1.07–9.05), p = 0.04]. However, this did not associate a statistically significant higher mortality (6%) or an overall hospital admission rate. However, other comorbidities, disease activity or the use of immunosuppressive drugs were not analyzed. Our study shows that, although the incidence is higher than in the general population, overall the rate of hospital admission, ventilation, or death is much lower than that reported in the general population. These data must be analyzed very cautiously since, as it is an online survey, it is very possible that there could be a selection bias, with less participation of patients who may have presented more severe forms of the disease.
The Global Rheumatology Alliance has established a registry of SAD patients with COVID-19 infection (10). This is an international initiative, supported by ACR and the EULAR with the possibility to include SAD patients affected by COVID-19 from all over the world. This study showed a high rate of hospitalization (46%) and mortality (9%) altogether, with SLE and VAS patients showing a higher propensity to be hospitalized than other patients do. These data are different from those obtained in our study, where the levels of hospitalization and severity are clearly lower than those of the general population. Similarly, treatment with doses >10 mg of prednisone was associated with hospitalization, something that did not happen in our study and that, given that the only treatment established as effective for severe SARS-CoV-2 infection is the use of corticosteroids, it could be very controversial. We did not find a significant association between antimalarial use and hospitalization in adjusted analyses as has been shown in multiple previously published studies the use of hydroxychloroquine was not associated with a decrease in hospitalization (20–22).
Strengths of our study include the first serial large analysis of patients with rheumatic diseases and COVID-19 with patient participation. All case data were entered by patients or their relatives. The registry includes cases from all over Spain suggesting that our findings are more generalizable than single-center or regional studies. Since the registry's inclusion criteria aren't restricted to those with rheumatic disease and COVID-19, that includes the ability to make comparisons with those who do not have COVID-19. Furthermore, the performance of multiple surveys allows a more optimal integration of data from a similar cohort of patients as well as a better representation of the cumulative incidence.
Despite these strengths, there are important limitations to these registry data. The COVID-GEAS registry is voluntary and does not capture all cases of COVID-19 in patients with rheumatic disease.
This approach to data collection places limitations on causal conclusions and temporal relationships and therefore we can only make limited inferences based on our results. It is a survey that has its limitations in the first place, not all patients have access to digital support to be able to carry it out. The digital divide in Spain is high and, above all, it is greater the older the patients.
Patients with more severe disease, admitted to UCI or hospital wards, have possibly not been able to answer this survey. But it can help us to have an idea of the cases of asymptomatic or oligosymptomatic infection and with less serious disease.
There is selection bias due to several factors, including geographic location, hospitalization status and disease severity, with the mild cases most likely to be captured, which quite possibly explains this remarkable increase in cumulative incidence compared to other published series.
Another important limitation is the significant discrepancy from the number of responses between the two surveys. It is possible that there were more responses in the first survey because it coincided with the first wave of infection in Spain and also coincided with the state of alarm and home confinement.
The second survey coincided with the end of the second wave and there was no longer any state of alarm and the experts no longer found themselves trusting. The fact that the patients were trusting in their home makes them have more time to be able to answer these types of surveys.
In terms of diagnostic tests, despite the fact that the nasopharyngeal swab was not as accurate as the fast antibody test and serological test, we didn't include these tests in the first survey, because in Spain these tests were not available in the public health system at the time the survey was carried out.
This series of cases demonstrates that the majority of patients with rheumatic diseases captured in our registry recover from COVID-19 although the real incidence of SARS-CoV-2 infection in autoimmunity patients is much higher possibly, due to the underestimation of mild or moderate cases that do not require specific attention. In some cases, exposure to specific medication classes is associated with lower odds of hospitalization; however, these findings should be interpreted with caution because of a high risk of bias.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This work was supported by SEMAIS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Our project has been carried out thanks to the collaboration of patients from several patient societies throughout Spain, and we would like to thank them for the time they have spent giving feedback. We also want to thank the support of SEMAIS (Multidisciplinary Spanish Society of Systemic Autoimmune diseases).
1. Li L-Q, Huang T, Wang Y-Q, Wang Z-P, Liang Y, Huang T-B, et al. COVID-19 patients' clinical characteristics, discharge rate, and fatality rate of meta-analysis. J Med Virol. (2020) 92:577–83. doi: 10.1002/jmv.25757
2. Dai H, Zhang X, Xia J, Zhang T, Shang Y, Huang R, et al. High-resolution chest CT features and clinical characteristics of patients infected with COVID-19 in Jiangsu, China. Int J Infect Dis. (2020) 95:106–12. doi: 10.1016/j.ijid.2020.04.003
3. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China. JAMA. (2020) 323:1239. doi: 10.1001/jama.2020.2648
4. Favalli EG, Ingegnoli F, De Lucia O, Cincinelli G, Cimaz R, Caporali R. COVID-19 infection and rheumatoid arthritis: faraway, so close! Autoimmun Rev. (2020) 19:102523. doi: 10.1016/j.autrev.2020.102523
5. Meroni PL, Zavaglia D, Girmenia C. Vaccinations in adults with rheumatoid arthritis in an era of new disease-modifying anti-rheumatic drugs. Clin Exp Rheumatol. (2018) 36:317–28.
6. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
7. Monti S, Balduzzi S, Delvino P, Bellis E, Quadrelli VS, Montecucco C. Clinical course of COVID-19 in a series of patients with chronic arthritis treated with immunosuppressive targeted therapies. Ann Rheum Dis. (2020) 79:667–8. doi: 10.1136/annrheumdis-2020-217424
8. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
9. Figueroa-Parra G, Aguirre-Garcia GM, Gamboa-Alonso CM, Camacho-Ortiz A, Galarza-Delgado DA. Are my patients with rheumatic diseases at higher risk of COVID-19? Ann Rheum Dis. (2020) 79:839–40. doi: 10.1136/annrheumdis-2020-217322
10. Gianfrancesco M, Hyrich KL, Hyrich KL, Al-Adely S, Al-Adely S, Carmona L, et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis. (2020) 79:859–66. doi: 10.1136/annrheumdis-2020-217871
11. Sanchez-Piedra C, Diaz-Torne C, Manero J, Pego-Reigosa JM, Rúa-Figueroa Í, Gonzalez-Gay MA, et al. Clinical features and outcomes of COVID-19 in patients with rheumatic diseases treated with biological and synthetic targeted therapies. Ann Rheum Dis. (2020) 79:988–90. doi: 10.1136/annrheumdis-2020-217948
12. Marques C, Pinheiro MM, Reis Neto ET, Dantas AT, Ribeiro FM, Melo AKG. COVID-19 in patients with rheumatic diseases: what is the real mortality risk? Ann Rheum Dis. (2020). doi: 10.1136/annrheumdis-2020-218388. [Epub ahead of print].
13. Tobinick E. TNF-α inhibition for potential therapeutic modulation of SARS coronavirus infection. Curr Med Res Opin. (2020) 20:39–40. doi: 10.1185/030079903125002757
14. Lin MH, Moses DC, Hsieh CH, Cheng SC, Chen YH, Sun CY, et al. Disulfiram can inhibit MERS and SARS coronavirus papain-like proteases via different modes. Antiviral Res. (2018) 150:155–63. doi: 10.1016/j.antiviral.2017.12.015
15. Al Ghamdi M, Alghamdi KM, Ghandoora Y, Alzahrani A, Salah F, Alsulami A, et al. Treatment outcomes for patients with Middle Eastern Respiratory Syndrome Coronavirus (MERS CoV) infection at a coronavirus referral center in the Kingdom of Saudi Arabia. BMC Infect Dis. (2016) 16:174. doi: 10.1186/s12879-016-1492-4
16. Mo Y, Fisher D. A review of treatment modalities for Middle East Respiratory Syndrome. J Antimicrob Chemother. (2016) 71:3340–50. doi: 10.1093/jac/dkw338
17. Woodruff M, Ramonell R, Nguyen D, Cashman KS, Saini AS, Hadded NS, et al. Extrafollicular B cell response correlate with neutralizing antibodies and morbidity in COVID-19. Nat Immunol. (2020) 21:1506–16. doi: 10.1038/s41590-020-00814-z
18. Pablos J, Galindo M, Carmona L, Lledó A, Retuerto M, Blanco R, et al. Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: a multicentric matched cohort study. Ann Rheum Dis. (2020) 79:1544–9. doi: 10.1136/annrheumdis-2020-218296
19. Ferri C, Giuggioli D, Raimondo V, L'Andolina M, Tavoni A, Cecchetti R, et al. COVID-19 and rheumatic autoimmune systemic diseases: report of a large Italian patients series. Clin Rheumatol. (2020) 39:3195–204. doi: 10.1007/s10067-020-05334-7
20. Shah S, Das S, Jain A, Misra DP, Negi VS. A systematic review of the prophylactic role of chloroquine and hydroxychloroquine in coronavirus disease-19 (COVID-19). Int J Rheum Dis. (2020) 23:613–9. doi: 10.1111/1756-185X.13842
21. Tang W, Cao Z, Han M, Wang Z, Chen J, Sun W, et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial. BMJ. (2020) 14:369. doi: 10.1136/bmj.m1849
Keywords: COVID-19 infection, SARS-CoV-2, systemic autoimmune disease, survey, systemic erythematosus lupus, corticosteroids, anti-TNF
Citation: Gracia BDC, Sáez L, Pallarés L, Velilla J, Marín A, Martinez-Lostao L, Simeón CP and Fanlo P (2022) COVID GEAS: COVID-19 National Survey in Patients With Systemic Autoimmune Diseases. Front. Med. 8:808608. doi: 10.3389/fmed.2021.808608
Received: 03 November 2021; Accepted: 07 December 2021;
Published: 27 January 2022.
Edited by:
Jixin Zhong, Huazhong University of Science and Technology, ChinaReviewed by:
Zhiqiang Qin, University of Arkansas for Medical Sciences, United StatesCopyright © 2022 Gracia, Sáez, Pallarés, Velilla, Marín, Martinez-Lostao, Simeón and Fanlo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patricia Fanlo, cGF0cmljaWFmYW5sb0B5YWhvby5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.