
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 21 January 2022
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.804173
 María B. Arriaga1,2,3†
María B. Arriaga1,2,3† Mariana Araújo-Pereira1,2,3†
Mariana Araújo-Pereira1,2,3† Beatriz Barreto-Duarte1,2,4,5†
Beatriz Barreto-Duarte1,2,4,5† Caio Sales1,2,4João Pedro Miguez-Pinto1,2,4Evelyn B. Nogueira1,2,4Betânia M. F. Nogueira1,2,3,6
Caio Sales1,2,4João Pedro Miguez-Pinto1,2,4Evelyn B. Nogueira1,2,4Betânia M. F. Nogueira1,2,3,6 Michael S. Rocha1,2,6,7
Michael S. Rocha1,2,6,7 Alexandra B. Souza8,9Aline Benjamin10Jamile G. de Oliveira11
Alexandra B. Souza8,9Aline Benjamin10Jamile G. de Oliveira11 Adriana S. R. Moreira12
Adriana S. R. Moreira12 Artur T. L. Queiroz2,13
Artur T. L. Queiroz2,13 Moreno M. S. Rodrigues14Renata Spener-Gomes8,9
Moreno M. S. Rodrigues14Renata Spener-Gomes8,9 Marina C. Figueiredo15Betina Durovni11Solange Cavalcante11
Marina C. Figueiredo15Betina Durovni11Solange Cavalcante11 José R. Lapa-e-Silva5,12
José R. Lapa-e-Silva5,12 Afrânio L. Kristki5,12
Afrânio L. Kristki5,12 Marcelo Cordeiro-Santos8,9,16Timothy R. Sterling15
Marcelo Cordeiro-Santos8,9,16Timothy R. Sterling15 Valeria C. Rolla10
Valeria C. Rolla10 Bruno B. Andrade1,2,3,4,7,15* and the RePORT-Brazil consortium
Bruno B. Andrade1,2,3,4,7,15* and the RePORT-Brazil consortiumBackground: There are scarce data on the prevalence and disease presentation of HIV in patients with tuberculosis (TB) and dysglycemia (diabetes [DM] and prediabetes [PDM]), especially in TB-endemic countries.
Methods: We assessed the baseline epidemiological and clinical characteristics of patients with culture-confirmed pulmonary TB, enrolled in a multicenter prospective cohort in Brazil (RePORT-Brazil) during 2015–2019. Dysglycemia was defined by elevated glycated hemoglobin and stratified as PDM or DM. Additionally, we used data from TB cases obtained through the Brazilian National Notifiable Diseases Information System (SINAN), during 2015–2019. In SINAN, diagnosis of diabetes was based on self-report. Logistic regression models were performed to test independent associations between HIV, dysglycemia status, and other baseline characteristics in both cohorts.
Results: In the RePORT-Brazil cohort, the prevalence of DM and of PDM was 23.7 and 37.8%, respectively. Furthermore, the prevalence of HIV was 21.4% in the group of persons with TB-dysglycemia and 20.5% in that of patients with TBDM. In the SINAN cohort, the prevalence of DM was 9.2%, and among the TBDM group the prevalence of HIV was 4.1%. Logistic regressions demonstrated that aging was independently associated with PDM or DM in both the RePORT-Brazil and SINAN cohorts. In RePORT-Brazil, illicit drug use was associated with PDM, whereas a higher body mass index (BMI) was associated with DM occurrence. Of note, HIV was not associated with an increased risk of PDM or DM in patients with pulmonary TB in both cohorts. Moreover, in both cohorts, the TBDM-HIV group presented with a lower proportion of positive sputum smear and a higher frequency of tobacco and alcohol users.
Conclusion: There is a high prevalence of dysglycemia in patients with pulmonary TB in Brazil, regardless of the HIV status. This reinforces the idea that DM should be systematically screened in persons with TB. Presence of HIV does not substantially impact clinical presentation in persons with TBDM, although it is associated with more frequent use of recreational drugs and smear negative sputum samples during TB screening.
Approximately one-quarter of the world population is thought to be infected with Mycobacterium tuberculosis (Mtb) and about 5–10% of those will develop active disease at some point in their lives, which represents a substantial public health problem (1). Several factors are related to the development of active tuberculosis (TB), such as immunological, genetic, and metabolic factors. Importantly, metabolic disorders associated with glycemic status are considered important risk factors for the development active TB and also for unfavorable anti-TB treatment outcomes (2). In addition, the immune deterioration caused by human immunodeficiency virus (HIV) favors the multiplication of Mtb and the progression to active TB (3).
Dysglycemia is a spectrum of metabolic dysfunctions related to glucose metabolism in the body, which includes several diseases, especially prediabetes (PDM) and diabetes (DM) (4). Approximately 422 million people worldwide live with DM, most of whom are in low-and middle-income countries. Likewise, a significant part of the world's population suffers from PDM, an intermediate state of insulin resistance that partially affects the entry of glucose into cells (5, 6). Interestingly, TB is similarly focused on low-and middle-income countries, which is a problem as DM triples the risk of developing active TB (7). Furthermore, 15.3% of people with TB worldwide have DM as a comorbidity (8). Persons with TB-DM usually exhibit a different clinical presentation, which includes higher frequency of extensive or cavitary pulmonary TB, a higher bacillary load in sputum and delayed mycobacterial clearance compared to normoglycemic TB patients (9, 10). Although much has been described on the interaction between TB and DM in different settings, most of the studies investigated a limited number of participants, and larger studies are warranted to better define such interactions. In addition, the clinical outcomes as well as the pathophysiological mechanisms of patients with TB-DM are still poorly understood (7, 11).
In addition to the importance of metabolic disorders, conditions that directly affect the immune response against TB are also a relevant problem as they contribute to more severe manifestations (12). Importantly, people living with HIV (PLWH) are approximately 50 times more likely to develop active TB than those without HIV exposure (12). Moreover, in 2019, PLWH accounted for 1.2 million (8.2%) of the approximately 10 million people with TB worldwide and of those, 208,000 deaths were related to HIV comorbidity (12). On the other hand, persons living with both TB and HIV often experience accelerated HIV disease progression and TB is placed as the most common opportunistic infection inducing high morbidity (12). HIV has been shown to modify the course of TB by causing severe immunosuppression and Mtb dissemination to multiple organs and increased mortality (13, 14).
Brazil has a high burden of TB-DM (8) and TB-HIV (1). Despite the high prevalence of these comorbidities, to our knowledge there is no information that explores in detail the association between HIV and TB-DM and its impact on clinical presentation of affected persons in the country. The scarce information that exists come from studies performed in African populations and with results that are not consistent with each other (15, 16). Because of the abovementioned reasons, studies that examine the overlap of metabolic and immunological diseases associated with TB are needed to better understand the spectrum of disease presentation of patients with multiple comorbidities such as TB-DM-HIV. In the present study, we aimed at contributing to fill this gap in knowledge in the context of TB, dysglycemia, and HIV-infection, through the identification and characterization of HIV prevalence and its association with glycemic status among persons with active pulmonary TB, in the Regional Prospective Observational Research in Tuberculosis (RePORT-Brazil) study, which is a large multicenter prospective cohort of culture-confirmed pulmonary TB persons which has been shown to be representative of the TB cases reported in the Brazilian national TB registry (17, 18). We also investigated such associations in TB cases reported to the Brazilian National TB Registry through the National System of Diseases Notification (SINAN).
All clinical investigations were conducted according to the principles of the Declaration of Helsinki. The RePORT-Brazil protocol, informed consent, and study documents were approved by the institutional review boards at each study site and at Vanderbilt University Medical Center (CAAE: 25102414.3.2009.5543). Participation in RePORT-Brazil was voluntary, and written informed consent was obtained from all such participants.
This was a multicenter prospective observational cohort study of individuals ≥ 18 years old with culture-confirmed pulmonary TB. RePORT-Brazil study sites are located in Manaus (Amazonas state, Northern region), Salvador (Bahia state, Northeastern region), and Rio de Janeiro (Rio de Janeiro state, Southeastern region), with a total of five health units: Instituto Nacional de Infectologia Evandro Chagas, Clínica da Família Rinaldo Delamare, and Secretaria Municipal de Saúde de Duque de Caxias (Rio de Janeiro), Instituto Brasileiro para Investigação da Tuberculose, Fundação José Silveira (Bahia), and Fundação de Medicina Tropical Doutor Heitor Vieira Dourado (Amazonas), representing both a heterogeneous population and the Brazilian cities with highest TB burden (17, 18).
Between 2015 and 2019, TB cases were interviewed for sociodemographic, clinical and epidemiological data such as age, sex, race/ethnicity (self-reported, based on the guidelines of the Ministry of Health of Brazil (19, 20), body mass index (BMI), income, smoking status, passive smoking status (living with someone who smokes), alcohol and illicit drug use, and clinical data such as presence of TB symptoms (cough, fever, weight loss, fatigue, night sweats, chest pain) and had the following tests performed: chest X-ray, HIV serologic test (the test was not performed if the individuals had a previous diagnosis of HIV), CD4 and viral load (if HIV serology was positive or previous diagnosis of HIV-infection), complete blood count, glycated hemoglobin (HbA1c), sputum smear microscopy, Xpert-MTB-RIF (if available) and mycobacterial culture (Lowenstein-Jensen medium or BD BACTEC MGIT). Patients who received TB treatment or fluoroquinolones for >7 days in the 30 days prior to TB diagnosis and pregnant women were excluded. We only analyzed information collected at the study baseline.
SINAN is a system for the notification of transmissible diseases, including TB, that has been implemented, supported, and maintained by the Brazilian Ministry of Health (21). Data were collected from TB patients ≥ 18 years old with information about “diabetes status”, between 2015 and 2019. Persons who were homeless, prisoners, pregnant, or had extrapulmonary TB were excluded, resulting in a population of 279,143 individuals. TB was diagnosed according to the Brazilian Ministry of Health criteria, detailed in the Manual of Recommendations for the TB Control in Brazil (22). After TB diagnosis, the information collected at the baseline and the laboratory results were recorded on a standardized form that, individual characteristics (sex, age, race, education level, alcohol consumption, illicit drug use, smoking habits, and comorbidities), the presence of DM condition (“yes” or “no” options) and HIV-infection, among others (22).
In pulmonary TB cases from RePORT-Brazil, participants with HbA1c ≥ 5.7% were classified as dysglycemic and those with HbA1c <5.7% were considered normoglycemic. Study participants were also classified as having DM (HbA1c ≥ 6.5%), PDM (HbA1c = 5.7–6.4%) or normoglycemia (HbA1c <5.7%), following American Diabetes Association (ADA) guidelines (23).
Categorical variables were presented as proportions and compared using a two-sided Pearson's chi-square test (with Yates's correction) or Fisher's two-tailed test in 2 × 3 or 2 × 2 tables, respectively. Continuous variables were presented as median and interquartile range (IQR) and compared using the Mann Whitney U (between 2 groups) or Kruskal Wallis test (between ≥2 groups). Viral load values and CD4 count were transformed to log10 for analyses. Multinomial and binomial logistic regression models with stepwise method (Wald) were performed to evaluate independent associations between clinical characteristics of pulmonary TB cases and presence of diabetes and/or prediabetes in the Report-Brazil and SINAN cohorts. Parameters with p-values ≤ 0.2 in univariate analyses were included in multivariable models. P-values < 0.05 were considered statistically significant. All the analyses were pre-specified. Statistical analyses were performed using SPSS 24.0 (IBM statistics), Graphpad Prism 9.0 (GraphPad Software, San Diego, CA) and R 3.1.0 (R Foundation, Austria).
RePORT-Brazil enrolled 1,162 patients with culture-positive pulmonary TB during 2015-2019 from the five centers of the consortium. The prevalence of dysglycemia at TB diagnosis was 61.5% (95%CI: 58.6–64.2). Compared to normoglycemic individuals, those with dysglycemia were more likely male (68.8 vs. 61.8%, p = 0.018) and older (39, IQR: 29–52 years, p < 0.001). Among TB-DM cases, 122/275 (44.4%) had previous diagnosis of DM. The dysglycemia group also exhibited higher frequency of self-reported pardo race (n = 388, 54.4%, p = 0.007), a higher median of BMI value (20.5, IQR:18.4–23.1; p < 0.001) and a higher frequency of self-reported weight loss (n = 597, 93%; p = 0.016) but not of other TB symptoms (Supplementary Table 1).
In RePORT-Brazil, the DM and PDM prevalence at TB diagnosis was 23.7% (95%CI: 21.31–26.2%) (n = 275), and 37.8% (95%CI: 35.0–40.6%) (n = 439), respectively (Supplementary Figure 1A). Several clinical characteristics differed between normoglycemic and dysglycemic TB patients, with significant differences in frequency of sex (p = 0.027), age (p < 0.001) race/ethnicity (p < 0.001), BMI values (p < 0.001) and the frequency of self-reported weight loss as a symptom (p = 0.033) between the three groups (Supplementary Table 2).
To evaluate these differences in more detail, we performed pair-wise comparisons between the groups. The highest median age was observed in the DM group (46 years; IQR: 36–55), which was significantly higher than PDM (36, IQR: 26–47) and normoglycemia (31, IQR: 23–42). We also observed differences between PDM and normoglycemia, with p < 0.001 in both comparisons (Supplementary Figure 1B). In addition, the DM group had higher median BMI (21.6, IQR: 19.1–24.4) than PDM (19.9, IQR: 18.4–21.80, p < 0.001) and normoglycemia (19.8, IQR: 17.9–22.0, p < 0.001), but there was no difference between PDM and normoglycemic individuals (p = 0.53) (Supplementary Figure 1B). TB patients with DM more frequently presented with positive smear (p = 0.037), weight loss (p = 0.027) and cough (p = 0.038) than those with normoglycemia (Supplementary Figure 1C). Patients with PDM similarly exhibited higher frequency of weight loss (p = 0.027) compared with persons with normoglycemia at baseline (Supplementary Figure 1C). Of note, 44.4% (n = 122) of the participants with DM already knew about their diagnosis of DM before being enrolled in the study (Supplementary Figure 1D, Supplementary Table 2).
To assess whether the results obtained from the analyses of the RePORT-Brazil cohort mirrored the data from the overall Brazilian TB population, we characterized the TBDM cases reported to the SINAN registry (Supplementary Figure 2). Of 279,143 pulmonary TB cases reported between 2015 and 2019, 25,765 had DM (self-reported), resulting in a prevalence of 9.2% (95%CI: 9.1–9.3%) (Supplementary Table 3, Supplementary Figure 2A). Patients with TB-DM were older (55 years, IQR:46–64) than normoglycemic patients (40 years, IQR:29–54; p < 0.001) (Supplementary Figure 2B), had a higher frequency of abnormal chest X-ray (p < 0.001), positive smear (p < 0.001), positive culture (p < 0.001) and were new cases more frequently reported (p < 0.001) than in normoglycemic patients (Supplementary Figure 2C, Supplementary Table 3). In contrast, normoglycemic persons were more frequently men (p < 0.001), reported greater consumption of alcohol (p < 0.001) and illegal drug use (p < 0.001) and more frequent tobacco use (p < 0.001) than those with DM. Finally, normoglycemic TB patients were mainly black/pardo (p < 0.001) and more frequently had drug-sensitive TB than TB-DM participants (p < 0.001) (Supplementary Table 3).
In RePORT-Brazil, the association between HIV-infection status and dysglycemia at baseline in participants with active pulmonary TB was analyzed according to age, presence of DM or PDM as well as to HbA1c levels (Figure 1). Importantly, the distribution of HbA1c values among persons with TB did not differ significantly according to HIV-infection status (Figure 1A, left panel). In fact, HIV-infection was present in the minority of the active TB cases in all sub-categories of glycemic status. The HIV-infection prevalence in the TB-dysglycemia group was 21.4% (95%CI: 18.6–4.3%) (Figure 1A, right panel). There was a significant difference in the frequency of TB patients with either DM (p < 0.001) or HIV-infection (p < 0.001) according to age category (Figure 1B), whereas there was no significant difference in the distribution of PDM among the different age categories (p = 0.099) (Figure 1B). Of note, the subgroup of older participants (>48 years-old) exhibited the highest frequency of DM (Figure 1B).
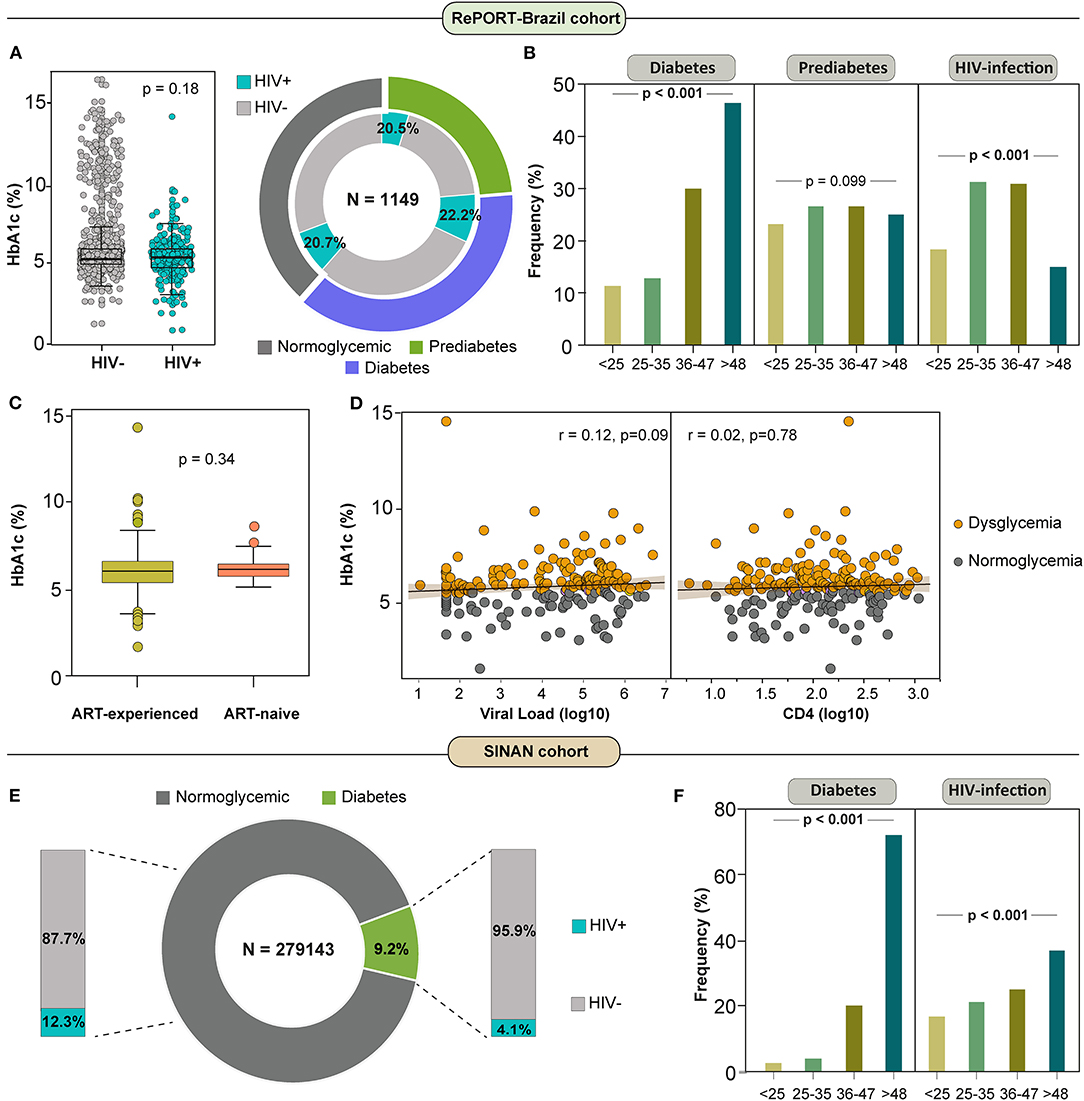
Figure 1. HIV infection among dysglycemic patients with active tuberculosis in RePORT-Brazil and SINAN cohorts. (A) Left panel: Scatter plot comparing distribution of HbA1c levels between subgroups of pulmonary TB cases per HIV infection status. Data were compared using the Mann-Whitney U test. Left panel: Total frequency of HIV infection among diabetic TB patients was 20.5%, among prediabetics was 22·2% and among normoglycemic patients was 20.7% (chi-square test p > 0·05). (B) Frequency of individuals with diagnosis of diabetes, prediabetes and HIV infection in the indicated age category (in years) among pulmonary TB patients is shown. Data were compared using the Pearson's chi-square test. (C) Box plot comparing distribution of HbA1c levels between subgroups of pulmonary TB cases per ART-experience and ART-naive status. Data were compared using the Mann-Whitney U test. (D) Spearman correlation between HbA1c and viral load (log10) levels (Left panel) and CD4 (log10) levels (Right panel) at baseline in pulmonary TB patients grouped according to the dysglycemic status. Line and shaded area represent linear curve fit with 95% confidence interval. (E) Total frequency of HIV infection among diabetic TB patients was 4.1% and among normoglycemic patients was 12.3% (chi-square test p > 0·05). The statistical analyzes were carried out only with the available data, omitting the cases with missing information (14 patients were removed due to lack in HIV status). (F) Frequency of individuals with diagnosis of diabetes and HIV infection in the indicated age category (in years) among pulmonary TB patients is shown. Data were compared using the Pearson's chi-square test. ART, antiretroviral therapy.
Further comparisons revealed no differences in the distribution of HbA1c values between PLWH undertaking antiretroviral therapy (ART) and those who were ART-naïve at the time of study enrollment (Figure 1C). There was a non-significant positive correlation between HbA1c levels and HIV viral load (Figure 1D, left panel) and also between HbA1c concentrations and CD4 T-cell counts (Figure 1D, right panel) when all PLWH were considered regardless of the glycemic status (Figure 1D, left panel). In contrast, in the SINAN cohort, we found a prevalence of HIV-infection in the DM sub-group of 4.1% (95% CI: 3.8–4.3%) (Figure 1E), lower than what was observed in the RePORT-Brazil cohort. Moreover, older TB patients (age >48 years) were more frequently found in in the DM and HIV-infection subgroups (p < 0.001) than other age groups (Figure 1F).
Multinomial logistic regression analyses were performed to test associations between characteristics of active pulmonary TB patients and the presence of PDM or DM in RePORT-Brazil participants. Results demonstrated that increases in age (per 1-year increase) were independently associated with an increased odds of PDM (adjusted odds ratio [aOR]: 1.02, IQR: 1.01–1.03, p < 0.001) or DM (aOR: 1.06, IQR: 1.04–1.07, p < 0.001). Furthermore, self-reported illicit drug use (aOR: 1.74, IQR: 1.23–2.45, p = 0.002) was related to increased odds of PDM but not DM. Higher BMI values (per 1Kg/m2 increase; aOR: 1.09, IQR: 1.05–1.14, p < 0.001) and presence of positive smear at baseline (aOR: 1.61, IQR: 1.08–2.40, p < 0.001) were both independently associated with increased odds of DM but not PDM. Of note, no association was found between presence of HIV-infection and odds of presenting with PDM (p = 0.956) or DM (p = 0.174) in the RePORT-Brazil cohort (Figure 2A).
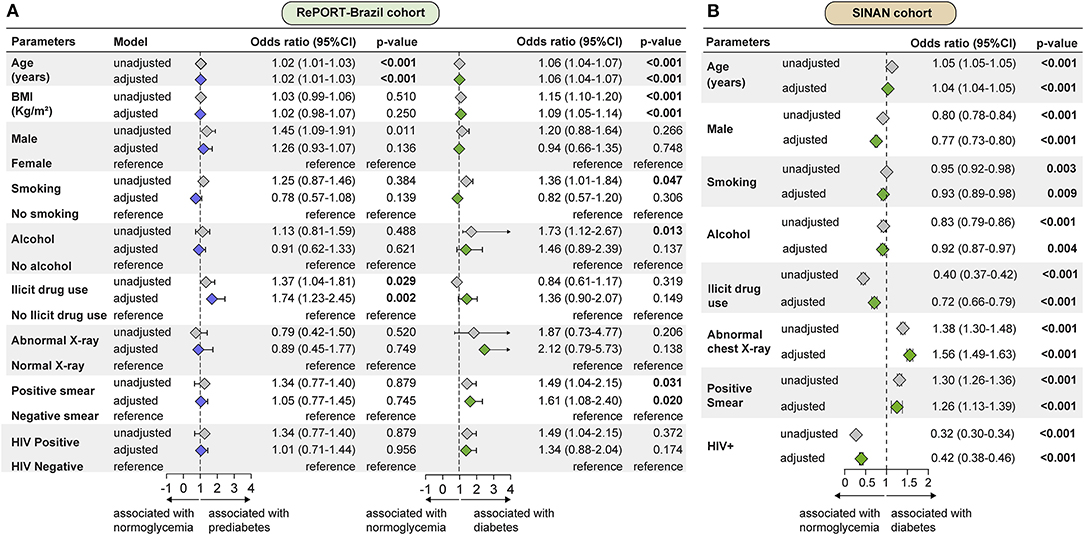
Figure 2. Factors associated with dysglycemia in patients with active pulmonary tuberculosis in RePORT-Brazil and SINAN cohorts. (A) A multinomial logistic regression analyses were used to test association between indicated characteristics of pulmonary TB patients and presence of prediabetes (left panel) or diabetes (right panel). Variables included in the adjusted model exhibited univariate p-values ≤ 0·2 (See Supplementary Table 2 for details). (B) Binomial logistic regression to test association between indicated characteristics of TB patients and presence of diabetes. Only variables with significant p-value in the adjusted model are shown. Variables included in the adjusted model exhibited univariate p-values ≤ 0.2 (See Supplementary Table 3 for details). BMI, Body Mass Index.
To test associations between characteristics of TB and the presence of DM in the SINAN cohort, a binomial logistic regression analysis was performed. In this cohort, aging (per 1-year increase; aOR: 1.04, IQR: 1.04–1.05, p < 0.001), positive smear (aOR: 1.26, IQR: 1.13–1.39, p < 0.001) and abnormal chest X-ray (aOR: 1.56, IQR: 1.49–1.63, p < 0.001) at baseline were independently associated with presence of DM. In contrast, male sex (aOR: 0.77, IQR: 0.73–0.80, p < 0.001), current smoking (aOR: 0.93, IQR:0.89-0.98, p < 0.001), alcohol consumption (aOR: 0.92, IQR: 0.87–0.97, p < 0.001), use of illicit drugs (aOR: 0.72, IQR: 0.66–0.79, p < 0.001) and to live with HIV (aOR: 0.42, IQR: 0.38–0.46, p < 0.001) were all associated with a decreased odds of DM (Figure 2B).
In the RePORT-Brazil cohort, the TBDM-HIV, TBPDM-HIV and TB-HIV groups presented similar frequencies for male sex (≈75.9%, p = 0.002). Interestingly, the highest median age was in the TBDM group (49 years), followed by 36 years in the TBDM-HIV and TBPDM groups, with the lowest median age observed in the TB group (30 years) (p < 0.001) (Table 1). Pardo race was the most reported in the TBDM-HIV group (69.6%). Drug resistance to isoniazid was more frequently observed in the groups with HIV coinfection (p = 0.036) (Table 1).
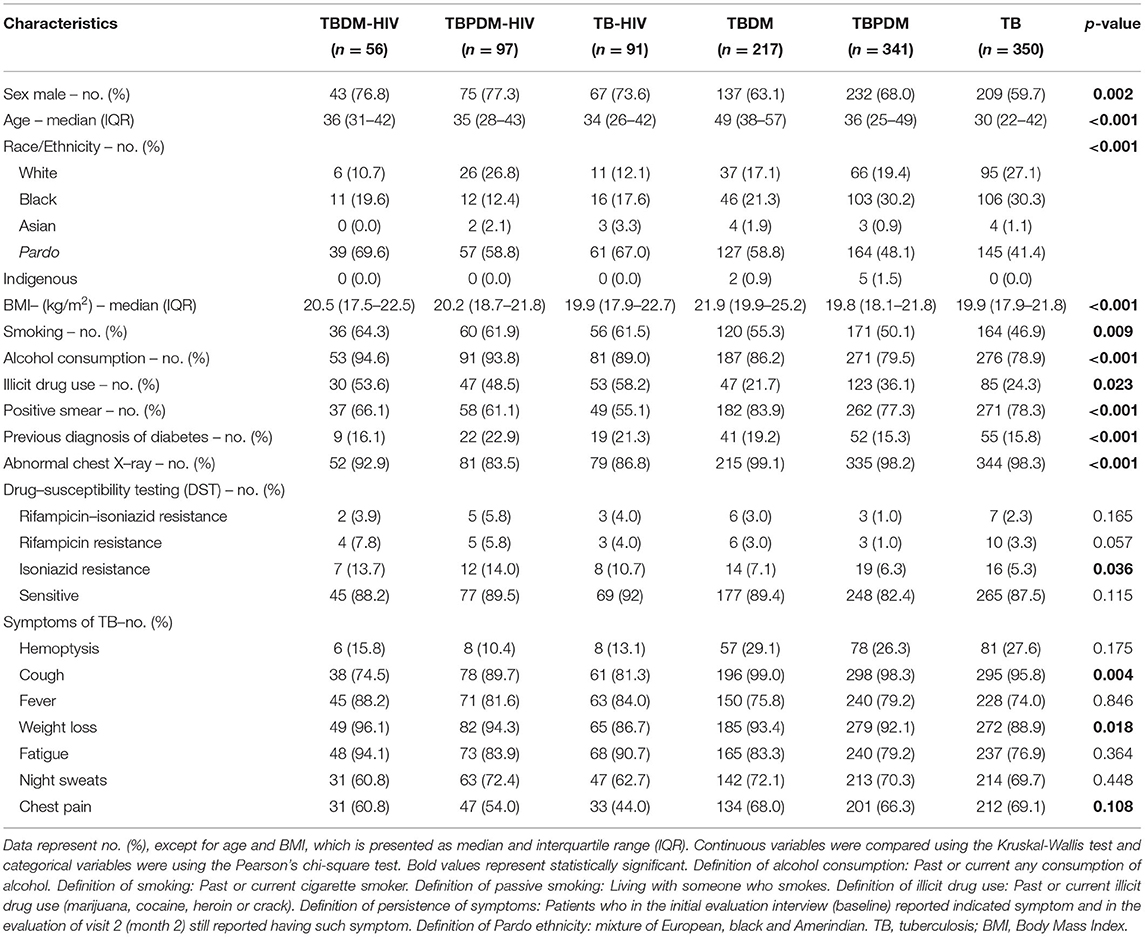
Table 1. Characteristics of TB cases by DM status in RePORT-Brazil cohort.
TB cases with HIV comorbidity displayed lower proportions of abnormal chest radiographs (p < 0.001) and of smear-positive sputum samples (p < 0.001) (Figure 3A, Table 1). We observed that tobacco use (64.3%) and alcohol consumption (94.6%) were significantly more reported in the TBDM-HIV group when compared to the clinical groups without HIV (Figure 3B, Table 1). As expected, regarding to the TB classic symptoms, the participants from the TBDM-HIV group presented a lower frequency of cough (p = 0.004) and a higher percentage of patients with weight loss (p = 0.018) (Figure 3C, Table 1).
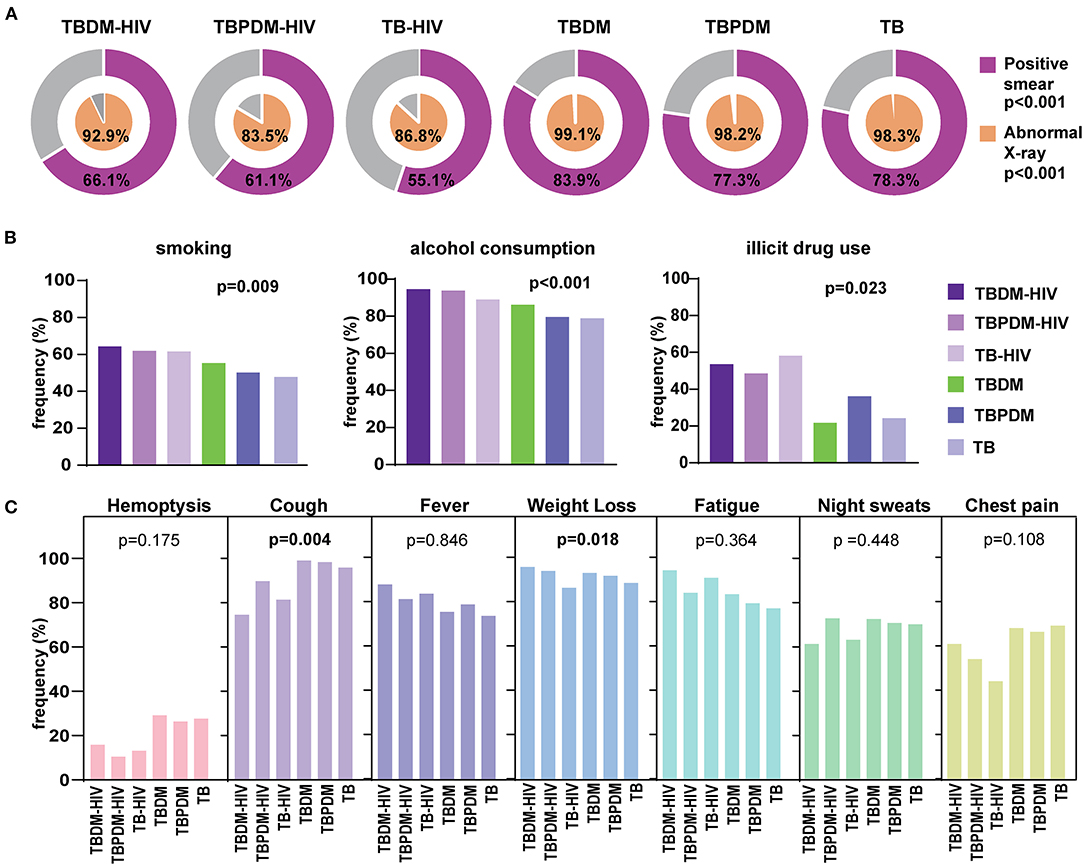
Figure 3. Clinical Characteristics of people with TB according glycemic and HIV status in the RePORT-Brazil cohort. (A) Proportion of positive smears and abnormal X-rays in each study group. (B) Frequency of TB cases according glycemic and HIV status regarding smoking habit, alcohol consumption and illicit drug use (smoking, alcohol, and illicit drug: in the past or at the time of evaluation before anti-TB treatment). (C) Frequency of TB classical symptoms in each study group. The data were compared between the groups using the Pearson's chi-square test. Comparisons with significant p-values are displayed in bold. TB, tuberculosis; DM, diabetes; PDM, prediabetes.
We found a similar clinical profile in the SINAN cohort, where the TBDM-HIV group was characterized by a higher frequency of male sex (70.1%). Furthermore, the highest median age was 55 years among TBDM cases, followed by 49 years in the TBDMHIV group (p < 0.001) (Table 2). Such as in RePORT-Brazil, the pardo race was the most self-reported in all groups. Remarkably, the TBDM-HIV group presented a slight proportion of drug resistance cases, and especially to rifampicin and isoniazid (8.1%) (p < 0.001).
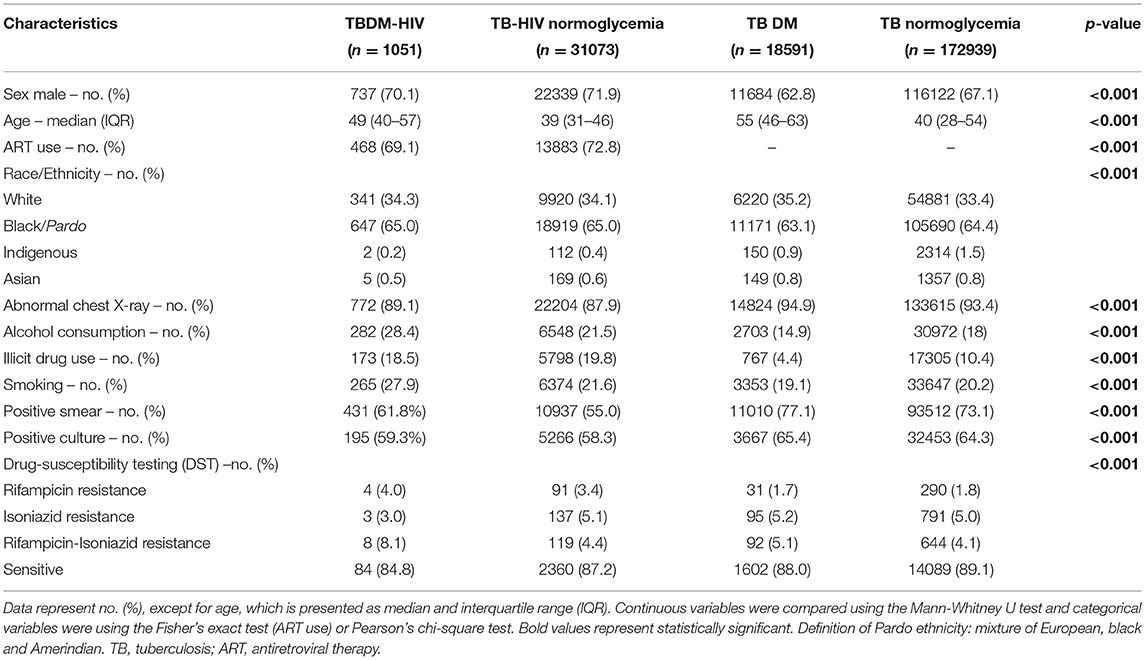
Table 2. Characteristics of TB cases by DM and HIV status in SINAN cohort.
Similar to the abovementioned results on the RePORT-Brazil, in the SINAN cohort we found a low frequency of positive smear in the TBDM-HIV (61.8%) and TB-HIV (55%) groups (p < 0.001) as well as of abnormal X-rays (89.1 and 87.9%, respectively) (p < 0.001) (Figure 4A, Table 2). Furthermore, the positive culture results were also less frequently reported in the groups with HIV comorbidity when compared to the groups of individuals non-exposed to HIV (p < 0.001) (Figure 4B, Table 2). Finally, TBDM-HIV cases more frequently reported the tobacco smoking (27.9%) and alcohol consumption (28.4%) (p < 0.001) (Figure 4C, Table 2).
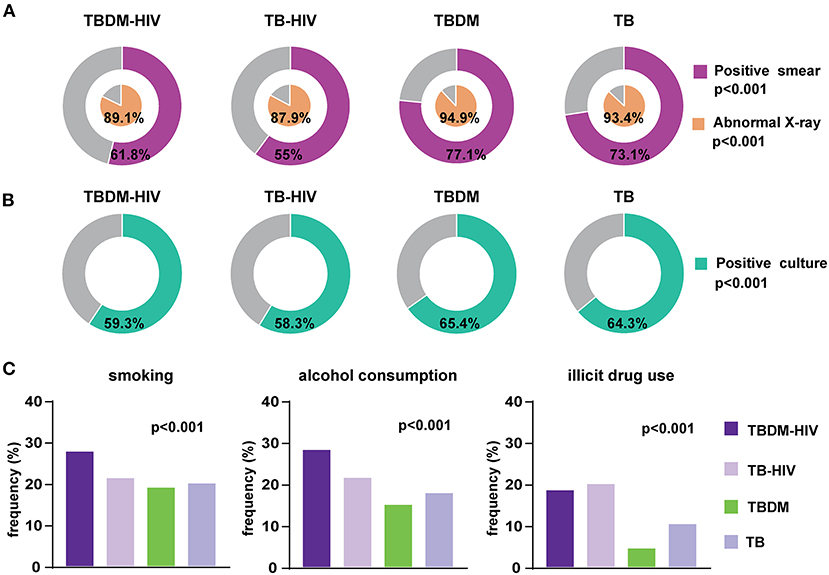
Figure 4. Clinical Characteristics of people with TB according glycemic and HIV status of the SINAN cohort. (A) Proportion of positive smears and abnormal X-rays in each study group. (B) Frequency of positive cultures. (C) TB cases according glycemic and HIV status regarding smoking habit, alcohol consumption and illicit drug use (smoking, alcohol, and illicit drug: in the past or at the time of evaluation before anti-TB treatment). The data were compared between the groups using the Pearson's chi-square test. Comparisons with significant p-values are displayed in bold. TB, tuberculosis; DM, diabetes; PDM, prediabetes.
Characterizing the association between TB, dysglycemia and HIV is important to understand the influence of metabolic and immunologic dysregulation in the presentation of the TB disease. The TB-DM association is frequent worldwide; currently, more TB patients live with DM than with HIV (24). In the RePORT-Brazil cohort, the prevalence of dysglycemia among TB patients at baseline was 61.5% (37.8% PDM and 23.7% DM). This prevalence was higher than that recently reported in Ghana (25), Peru (26) and in the South of Brazil (27). The RePORT-Brazil cohort is large and composed by individuals from different regions of Brazil, and we have recently shown that it is representative of Brazilian patients with TB (18). The present work reports findings consistent with the literature, where TB-dysglycemia (mainly DM) patients have increased BMI values and higher prevalence of weight loss than normoglycemic patients (28). TB-DM patients in RePORT-Brazil exhibited similar characteristics to those in a large cohort of 709,000 Brazilians with TB from 2007 to 2014: mostly men, mean age >40 years and self-reported black or pardo (29).
TB patients more frequently reported smoking and use of illicit drugs and alcohol, which are shared risk factors not only for TB but also for DM (30, 31). The multinomial regression analysis demonstrated that illicit drug use was associated with increased odds of PDM, whereas alcohol use and smoking were associated with DM in the unadjusted model. Also in this analysis, aging was associated with both PDM and DM, and higher BMI was associated with presence of DM. These are factors already described as risk factors for TB in patients with DM, in addition to a lack of glycemic control (32). The majority (55.6%) of the TB-DM patients in the RePORT-Brazil study had no previous diagnosis of dysglycemia, which can be related to a lack of glycemic control that may be contributing to a more severe symptomatology (32), considering that coughing was a symptom associated with DM. The rate of newly diagnosed patients was high compared to other studies (33), representing 66% of DM cases in RePORT Brazil cohort, demonstrating the importance of DM screening at the time of TB diagnosis.
Using data from SINAN, we observed that between 2015 and 2019, the frequency of TB-DM in Brazil was only 9.2%, lower than the global prevalence of 15% and higher than the South American prevalence of 7.7%, calculated from a meta-analysis of more than 200 studies recently conducted around the world (8). When comparing our original data with the results obtained through SINAN, in RePORT-Brazil, patients with TB-DM were more likely to be male, black/pardo, older and more frequently to have a positive sputum smear than persons without DM, reinforcing the idea that the results obtained with RePORT-Brazil are representative of the country's population. However, in contrast to RePORT-Brazil, in SINAN, TB-DM patients had a significantly lower frequency of HIV-infection than those who did not report DM. This difference found in SINAN may be since glycemic control is performed in all the study participants diagnosed with dysglycemia, whereas it is only recommended, and not mandatory, in the national guidelines. In addition, there is a potential underreporting of cases in SINAN, and only DM cases, but not PDM, are notified. We have discussed this limitation in the SINAN database previously (18), where the performance of health and epidemiological indicators was substantially higher in RePORT-Brazil than in the cases notified to SINAN. In the SINAN cohort, there was a lower proportion of males in the TBDM group, probably due to the higher percentage of women diagnosed with diabetes (34). On the other hand, the lower frequency of alcohol, smoking and illicit drug use could be attributed to the fact that this information is self-reported by patients rather than formally investigated (35).
In RePORT-Brazil, most patients with DM or PDM were HIV-seronegative. Other studies had shown this low frequency of HIV-infection in association with DM in Brazil (28, 29). HbA1c levels were also similar in TB patients stratified by HIV status. There is scarce evidence describing the interaction of HbA1c values and HIV in patients with TB. One study described that HbA1c could underestimate real glycemia values in PWLH (36). Furthermore, dysglycemia risk in PLWH has been shown to be increased after initiating ART (37), which could be a potential confounding factor, but HIV-infection was not associated with occurrence of dysglycemia in our study in both cohorts, even when stratified by age. Of note, in the SINAN cohort, presence of HIV-infection was linked to increased likelihood of normoglycemia in the population with pulmonary TB. Thus, the findings presented here from both large cohorts analyzed in this study argue that HIV-infection does not appear to be a determinant of dysglycemia in patients with pulmonary TB in Brazil.
To investigate whether HIV had any influence on dysglycemia in the RePORT-Brazil cohort, we tested for correlations between HbA1c and HIV-1 viral load or CD4 T-cell counts. We found just weak and non-significant correlations, indicating that HIV progression may not influence the occurrence of significant hyperglycemia. A study in PLWH that used fasting plasma glucose to measure glycemia reported that CD4 T-cell counts, and HIV viral load could influence blood glucose levels (38). Further studies are necessary to clarify whether HIV disease progression affects glycemic control by measuring several laboratory parameters simultaneously, such as HbA1c, fasting glucose levels or oral glucose tolerance tests. Our findings clearly corroborate the idea that despite the effect of HIV-infection on the immune system, glucose metabolism does not seem to be highly affected by this infection or disease progression.
We show the groups according to the glycemic status and by HIV infection and we identified that the group of persons with TBDM-HIV present with some peculiar characteristics. Male sex, smoking and alcohol consumption were higher in the TBDM-HIV group. We did not find specific literature to be able to contrast to our results. However, a study in 132 people with HIV described that the male population has a strong association with smoking, and in turn there is a strong interaction between smoking and alcohol consumption in infected men with HIV (39) which is consistent with the results of our study. Immunodeficiency and a decreased inflammatory response can inhibit sputum production in individuals with HIV; such cases also tend to have fewer atypical findings on radiographs (40), which coincides with the overall low percentage of cough and lower frequency of abnormal x-rays found in the TBDM-HIV, TBPDM-HIV and TB-HIV groups. Among the groups of individuals living with HIV, the TBDM-HIV presented a higher proportion of abnormal x-rays and self-reported cough. We hypothesize that presence of DM may boost immunopathological mechanisms that lead to tissue damage and inflammation which results in abnormal radiographs and cough. Reinforcing this idea, we have previously reported that the transcriptome of TB-DM patients exhibits increased representation of neutrophilic inflammation pathways (41), which may contribute at least in part to lung damage leading to cough and altered x-rays.
The present study has some limitations. In RePORT-Brazil, dysglycemia was investigated by means of HbA1c levels; we did not perform fasting glucose levels or oral glucose tolerance tests. Although glycated hemoglobin levels have been reliably used to estimate dysglycemia in several studies, it is possible that the final numbers of DM and PDM would have differed if additional laboratory assessments had been used. In addition, the use of anti-DM drugs was not uniformly recorded. In SINAN, diabetes condition is notified without differentiating if it was self-reported or if it had a laboratory confirmation. Therefore, the accuracy of DM diagnosis may have been affected. Another limitation was that in the RePORT-Brazil cohort, the type of DM was type 2 and in the SINAN cohort the type of DM is not specified in the notification system.
Regardless of its limitations, the present study adds important knowledge to the study of dysglycemia in TB patients in a large well-characterized multicenter cohort from Brazil, enabling the identification of factors associated with PDM and DM in this population. We also demonstrate that the majority of patients with TB-DM had no previous diagnosis of dysglycemia, which may be associated with an underreporting of DM in the SINAN database, and that HIV-infection was not significantly associated with dysglycemia in TB patients. It is important to systematically screen for DM in TB patients and initiate appropriate therapy for both diseases to reduce the dual burden of these major diseases. In 2019, screening for DM in patients diagnosed with TB was implemented in the Brazilian guidelines as a programmatic activity (42), in order to control TB transmission, monitor glycemia and ensure a favorable treatment result. However, the results of this strategy are still being evaluated to find a functional system in the comprehensive care of patients with TB.
Alice M. S. Andrade (Laboratório de Inflamação e Biomarcadores, Instituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil, Multinational Organization Network Sponsoring Translational and Epidemiological Research (MONSTER) Initiative, Salvador, Brazil); Juan M. Cubillos-Angulo (Laboratório de Inflamação e Biomarcadores, Instituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil, Multinational Organization Network Sponsoring Translational and Epidemiological Research (MONSTER) Initiative, Salvador, Brazil, Faculdade de Medicina, Universidade Federal da Bahia, Salvador, Brazil); Hayna Malta-Santos, Jéssica Rebouças-Silva (Laboratório de Inflamação e Biomarcadores, Instituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil, Faculdade de Medicina, Universidade Federal da Bahia, Salvador, Brazil); Saulo R. N. Santos, André Ramos (Instituto Brasileiro para Investigação da Tuberculose, Fundação José Silveira, Salvador, Brazil); Alysson G. Costa (Programa de Pós-Graduação em Medicina Tropical, Universidade do Estado do Amazonas, Manaus, Brazil, Laboratório de Pesquisa Clínica em Micobacteriose, Instituto Nacional de Infectologia Evandro Chagas, Fiocruz, Rio de Janeiro, Brazil); Jaquelane Silva (Programa de Pós-Graduação em Medicina Tropical, Universidade do Estado do Amazonas, Manaus, Brazil); Adriano Gomes-Silva, Flávia M. Sant'Anna, Francine P. Ignácio (Division of Infectious Diseases, Department of Medicine, Vanderbilt University School of Medicine, Nashville, TN, United States); Vanessa Nascimento (Multinational Organization Network Sponsoring Translational and Epidemiological Research (MONSTER) Initiative, Salvador, Brazil, Instituto Brasileiro para Investigação da Tuberculose, Fundação José Silveira, Salvador, Brazil, Escola Bahiana de Medicina e Saúde Pública, Salvador, Brazil); Maria Cristina Lourenço18, Elisangela C. Silva, Mayla Mello (Programa Acadêmico de Tuberculose da Faculdade de Medicina, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The RePORT-Brazil protocol, informed consent, and study documents were approved by the institutional review boards at each study site and at Vanderbilt University Medical Center (CAAE: 25102414.3.2009.5543). The patients/participants provided their written informed consent to participate in this study.
TS, MF, MC-S, VR, and BA: Conceptualization. MA, MA-P, AQ, MMSR, and BA: Data curation. MA, MA-P, BB-D, CS, JM-P, EN, BN, MSR, AS, AB, JdO, AM, RS-G, MF, BD, JL-e-S, AK, SC, VR, TS, MC-S, and BA: Investigation. MA, MA-P, BB-D, and BA: Formal analysis. BD, JL-e-S, AK, SC, VR, TS, MC-S, MF, and BA: Funding acquisition. MA, MA-P, BB-D, and BA: Methodology. MF, TS, and BA: Project administration. MA, MA-P, BB-D, TS, and BA: Resources. MA, MA-P, AQ, MMSR, MF, TS, and BA: Software. TS, and BA: Supervision. MA, MA-P, BB-D, JM-P, CS, EN and BA: Writing—original draft. All authors Writing—review and editing. All authors have read and agreed to the submitted version of the manuscript.
The study was supported in part by the intramural research program of FIOCRUZ (BA.), Fogarty International Center and National Institute of Child Health & Human Development of the National Institutes of Health under (Award Number D43 TW009763 through a research scholarship awarded to MA.) and by the NIH (U01AI069923). BA, J.L-S, AK, and VR. are senior scientists from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil. MA. received a research fellowship from the Fundação de Amparo à Pesquisa do Estado da Bahia (FAPESB), Brazil. MA-P and BB-D received a fellowship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Finance code: 001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the study participants. We also thank the teams of clinical and laboratory platforms of RePORT-Brazil. A special thanks to Elze Leite (FIOCRUZ, Salvador, Brazil), Eduardo Gama (FIOCRUZ, Rio de Janeiro, Brazil), Elcimar Junior (FMT-HVD, Manaus, Brazil), and Hilary Vansell (VUMC, Nashville, USA) for administrative and logistical support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.804173/full#supplementary-material
2. Hensel RL, Kempker RR, Tapia J, Oladele A, Blumberg HM, Magee MJ. Increased risk of latent tuberculous infection among persons with pre-diabetes and diabetes mellitus. Int J Tubercul Lung Dis. (2016) 20:71–8. doi: 10.5588/ijtld.15.0457
3. He X, Eddy JJ, Jacobson KR, Henderson AJ, Agosto LM. Enhanced human immunodeficiency virus-1 replication in CD4+ T cells derived from individuals with latent mycobacterium tuberculosis infection. J Infect Dis. (2020) 222:1550–60. doi: 10.1093/infdis/jiaa257
4. American Diabetes A. Classification and diagnosis of diabetes: standards of medical care in diabetes-−2021. Diabetes Care. (2021) 44:S15–33. doi: 10.2337/dc21-S002
5. Abdul-Ghani MA, Tripathy D, Defronzo RA. Contributions of beta-cell dysfunction and insulin resistance to the pathogenesis of impaired glucose tolerance and impaired fasting glucose. Diabetes Care. (2006) 29:1130–9. doi: 10.2337/dc05-2179
6. Goncalves ANA, Lever M, Russo PST, Gomes-Correia B, Urbanski AH, Pollara G, et al. Assessing the impact of sample heterogeneity on transcriptome analysis of human diseases using MDP Webtool. Front Genet. (2019) 10:971. doi: 10.3389/fgene.2019.00971
7. Hayashi S, Chandramohan D. Risk of active tuberculosis among people with diabetes mellitus: systematic review and meta-analysis. Trop Med Int Health. (2018) 23:1058–70. doi: 10.1111/tmi.13133
8. Noubiap JJ, Nansseu JR, Nyaga UF, Nkeck JR, Endomba FT, Kaze AD, et al. Global prevalence of diabetes in active tuberculosis: a systematic review and meta-analysis of data from 2·3 million patients with tuberculosis. Lancet Global Health. (2019) 7:e448–60. doi: 10.1016/S2214-109X(18)30487-X
9. Singla R, Khan N, Al-Sharif N, Ai-Sayegh MO, Shaikh MA, Osman MM. Influence of diabetes on manifestations and treatment outcome of pulmonary TB patients. Int J Tubercul Lung Dis. (2006) 10:74–9. Available online at: https://www.ingentaconnect.com/contentone/iuatld/ijtld/2006/00000010/00000001/art00014
10. Gil-Santana L, Almeida-Junior JL, Oliveira CA, Hickson LS, Daltro C, Castro S, et al. Diabetes is associated with worse clinical presentation in tuberculosis patients from Brazil: a retrospective cohort study. PLoS ONE. (2016) 11:e0146876. doi: 10.1371/journal.pone.0146876
11. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. (2008) 5:e152. doi: 10.1371/journal.pmed.0050152
13. Geldmacher C, Ngwenyama N, Schuetz A, Petrovas C, Reither K, Heeregrave EJ, et al. Preferential infection and depletion of Mycobacterium tuberculosis-specific CD4 T cells after HIV-1 infection. J Exp Med. (2010) 207:2869–81. doi: 10.1084/jem.20100090
14. Moir S, Chun TW, Fauci AS. Pathogenic mechanisms of HIV disease. Annu Rev Pathol. (2011) 6:223–48. doi: 10.1146/annurev-pathol-011110-130254
15. Bailey SL, Ayles H. Association between diabetes mellitus and active tuberculosis in Africa and the effect of HIV. Trop Med Int Health. (2017) 22:261–8. doi: 10.1111/tmi.12822
16. Oni T, Berkowitz N, Kubjane M, Goliath R, Levitt NS, Wilkinson RJ. Trilateral overlap of tuberculosis, diabetes and HIV-1 in a high-burden African setting: implications for TB control. Eur Respir J. (2017) 50. doi: 10.1183/13993003.00004-2017
17. Hamilton CD, Swaminathan S, Christopher DJ, Ellner J, Gupta A, Sterling TR, et al. RePORT International: Advancing Tuberculosis Biomarker Research Through Global Collaboration. Clin Infect Dis. (2015) 61:S155–159. doi: 10.1093/cid/civ611
18. Arriaga MB, Amorim G, Queiroz AT, Rodrigues MM, Araújo-Pereira M, Nogueira BM, et al. Novel stepwise approach to assess representativeness of a large multicenter observational cohort of tuberculosis patients: the example of RePORT Brazil. Int J Infect Dis. (2021) 103:110–8. doi: 10.1016/j.ijid.2020.11.140
19. Instituto Brasileiro De Geografia E Estatística. Características étnico-raciais da População Classificações e Identidades. (Brazol). (2013).
21. Ministério Da Saúde Do Brasil, and Secretaria De Vigilância Em Saúde. Sistema de Informação de Agravos de Notificação [Online]. (2020) Available online at: http://portalsinan.saude.gov.br/. (accessed August 14, 2020).
22. Ministério Da Saúde Do Brasil, and Secretaria De Vigilância Em Saúde. Manual de Recomendações para o Controle da Tuberculose no Brasil. (2013)
24. Girardi E, Schepisi MS, Goletti D, Bates M, Mwaba P, Yeboah-Manu D, et al. The global dynamics of diabetes and tuberculosis: the impact of migration and policy implications. Int J Infect Dis. (2017) 56:45–53. doi: 10.1016/j.ijid.2017.01.018
25. Yorke E, Boima V, Dey ID, Amissah-Arthur M-B, Ganu V, Amaning-Kwarteng E, et al. Transient impact of dysglycemia on sputum conversion among smear-positive tuberculosis patients in a tertiary care facility in ghana. Clin Med Insights. (2021) 15:11795484211039830. doi: 10.1177/11795484211039830
26. Calderon RI, Arriaga MB, Lopez K, Barreda NN, Sanabria OM, Froes Neto JF, et al. High prevalence and heterogeneity of Dysglycemia in patients with tuberculosis from Peru: a prospective cohort study. BMC Infect Dis. (2019) 19:799. doi: 10.1186/s12879-019-4416-2
27. Beraldo AA, Andrade RLDP, Pinto ÉSG, Da Silva-Sobrinho RA, Saita NM, Monroe AA, et al. Tuberculose e diabetes mellitus: perfil sociodemográfico e clínico em municípios brasileiros. Rev Gaúcha de Enfermagem. (2021) 42. doi: 10.1590/1983-1447.2021.20200247
28. Almeida-Junior JL, Gil-Santana L, Oliveira CA, Castro S, Cafezeiro AS, Daltro C, et al. Glucose metabolism disorder is associated with pulmonary tuberculosis in individuals with respiratory symptoms from Brazil. PLoS ONE. (2016) 11:e0153590. doi: 10.1371/journal.pone.0153590
29. Evangelista MDSN, Maia R, Toledo JP, Abreu RGD, Barreira D. Tuberculosis associated with diabetes mellitus by age group in Brazil: a retrospective cohort study, 2007-2014. Braz J Infect Dis. (2020) 24:130–6. doi: 10.1016/j.bjid.2020.03.005
30. Yu M, Xu C-X, Zhu H-H, Hu R-Y, Zhang J, Wang H, et al. Associations of cigarette smoking and alcohol consumption with metabolic syndrome in a male Chinese population: a cross-sectional study. J Epidemiol. (2014) 24:361–9. doi: 10.2188/jea.JE20130112
31. Pelissari DM, Diaz-Quijano FA. Impact of alcohol disorder and the use of illicit drugs on tuberculosis treatment outcomes: a retrospective cohort study. Arch Public Health. (2018) 76:45. doi: 10.1186/s13690-018-0287-z
32. Khalil NH, Ramadan RA. Study of risk factors for pulmonary tuberculosis among diabetes mellitus patients. Egyptian J Chest Dis Tubercul. (2016) 65:817–23. doi: 10.1016/j.ejcdt.2016.05.009
33. Abdelbary BE, Garcia-Viveros M, Ramirez-Oropesa H, Rahbar MH, Restrepo BI. Tuberculosis-diabetes epidemiology in the border and non-border regions of Tamaulipas, Mexico. Tuberculosis. (2016) 101S:S124–34. doi: 10.1016/j.tube.2016.09.024
34. Abreu RG, Rolim LS, Sousa AIA, Oliveira MRF. Tuberculosis and diabetes: association with sociodemographic characteristics and diagnosis and treatment of tuberculosis. Brazil, 2007-2011. Rev Bras Epidemiol. (2020) 23:e200009. doi: 10.1590/1980-549720200009
35. Santos ML, Coeli CM, Batista JDL, Braga MC, Albuquerque M. Factors associated with underreporting of tuberculosis based on data from Sinan Aids and Sinan TB. Rev Bras Epidemiol. (2018) 21:e180019. doi: 10.1590/1980-549720180019
36. Glesby MJ, Hoover DR, Shi Q, Danoff A, Howard A, Tien P, et al. Glycated haemoglobin in diabetic women with and without HIV infection: data from the Women's Interagency HIV study. Antivir Ther. (2010) 15:571–7. doi: 10.3851/IMP1557
37. Julius H, Basu D, Ricci E, Wing J, Basu JK, Pocaterra D, et al. The burden of metabolic diseases amongst HIV positive patients on HAART attending The Johannesburg Hospital. Curr HIV Res. (2011) 9:247–52. doi: 10.2174/157016211796320360
38. Duro M, Rebelo I, Barreira S, Sarmento-Castro R, Medeiros R, Almeida C. Glycaemic profile changes by highly active antiretroviral therapy in human immunodeficiency virus-infected patients. Int J STD AIDS. (2015) 26:796–802. doi: 10.1177/0956462414554814
39. Bhatta DN, Subedi A, Sharma N. Tobacco smoking and alcohol drinking among HIV infected people using antiretroviral therapy. Tob Induc Dis. (2018) 16:16. doi: 10.18332/tid/86716
40. Abaye GE, Abebe T, Worku A, Tolessa D, Ameni G, Mihret A. Detection of Mycobacterium tuberculosis from the stool of HIV sero-positive individuals suspected of pulmonary tuberculosis. PLoS ONE. (2017) 12:e0177529. doi: 10.1371/journal.pone.0177529
Keywords: dysglycemia, HIV infection, pulmonary tuberculosis, Mycobacterium tuberculosis, diabetes
Citation: Arriaga MB, Araújo-Pereira M, Barreto-Duarte B, Sales C, Miguez-Pinto JP, Nogueira EB, Nogueira BMF, Rocha MS, Souza AB, Benjamin A, de Oliveira JG, Moreira ASR, Queiroz ATL, Rodrigues MMS, Spener-Gomes R, Figueiredo MC, Durovni B, Cavalcante S, Lapa-e-Silva JR, Kristki AL, Cordeiro-Santos M, Sterling TR, Rolla VC, Andrade BB and the RePORT-Brazil consortium (2022) Prevalence and Clinical Profiling of Dysglycemia and HIV Infection in Persons With Pulmonary Tuberculosis in Brazil. Front. Med. 8:804173. doi: 10.3389/fmed.2021.804173
Received: 28 October 2021; Accepted: 14 December 2021;
Published: 21 January 2022.
Edited by:
Zhiliang Hu, Nanjing Second Hospital, ChinaReviewed by:
Lucio Vera-Cabrera, Universidad Autonoma de Nuevo León, MexicoCopyright © 2022 Arriaga, Araújo-Pereira, Barreto-Duarte, Sales, Miguez-Pinto, Nogueira, Nogueira, Rocha, Souza, Benjamin, de Oliveira, Moreira, Queiroz, Rodrigues, Spener-Gomes, Figueiredo, Durovni, Cavalcante, Lapa-e-Silva, Kristki, Cordeiro-Santos, Sterling, Rolla, Andrade and the RePORT-Brazil consortium. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bruno B. Andrade, YnJ1bm8uYW5kcmFkZUBmaW9jcnV6LmJy
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.