 Miriam C. Banas1*
Miriam C. Banas1* Georg A. Böhmig2
Georg A. Böhmig2 Ondrej Viklicky3,4
Ondrej Viklicky3,4 Lionel P. Rostaing5,6
Lionel P. Rostaing5,6 Thomas Jouve5
Thomas Jouve5 Lluis Guirado7Carme Facundo7
Lluis Guirado7Carme Facundo7 Oriol Bestard8Hermann-Josef Gröne9
Oriol Bestard8Hermann-Josef Gröne9 Kazuhiro Kobayashi10Vladimir Hanzal4
Kazuhiro Kobayashi10Vladimir Hanzal4 Franz Josef Putz1
Franz Josef Putz1 Daniel Zecher1
Daniel Zecher1 Tobias Bergler1
Tobias Bergler1 Sindy Neumann11
Sindy Neumann11 Victoria Rothe11
Victoria Rothe11 Amauri G. Schwäble Santamaria11Eric Schiffer11
Amauri G. Schwäble Santamaria11Eric Schiffer11 Bernhard Banas1
Bernhard Banas1- 1Department of Nephrology, University Hospital Regensburg, Regensburg, Germany
- 2Division of Nephrology and Dialysis, Department of Medicine III, Medical University of Vienna, Vienna, Austria
- 3Transplant Laboratory, Institute for Clinical and Experimental Medicine (IKEM), Prague, Czechia
- 4Department of Nephrology, Institute for Clinical and Experimental Medicine (IKEM), Prague, Czechia
- 5Nephrology, Hemodialysis, Apheresis and Kidney Transplantation Department, Grenoble University Hospital, Grenoble, France
- 6Faculty of Health, Grenoble Alpes University, Grenoble, France
- 7Nephrology Department, Fundació Puigvert, Instituto de Investigaciones Biomédicas Sant Pau (IIB-Sant Pau), Medicine Department-Universitat Autónoma de Barcelona, REDinREN, Instituto de Investigación Carlos III, Barcelona, Spain
- 8Vall d'Hebron University Hospital (HUVH), Vall d'Hebron Research Institute (VHIR), Barcelona, Spain
- 9Institute of Pharmacology, Philipps-University, Marburg, Germany
- 10Institute of Pharmacology, University of Marburg, Marburg, Germany
- 11numares AG, Regensburg, Germany
Background: In an earlier monocentric study, we have developed a novel non-invasive test system for the prediction of renal allograft rejection, based on the detection of a specific urine metabolite constellation. To further validate our results in a large real-world patient cohort, we designed a multicentric observational prospective study (PARASOL) including six independent European transplant centers. This article describes the study protocol and characteristics of recruited better patients as subjects.
Methods: Within the PARASOL study, urine samples were taken from renal transplant recipients when kidney biopsies were performed. According to the Banff classification, urine samples were assigned to a case group (renal allograft rejection), a control group (normal renal histology), or an additional group (kidney damage other than rejection).
Results: Between June 2017 and March 2020, 972 transplant recipients were included in the trial (1,230 urine samples and matched biopsies, respectively). Overall, 237 samples (19.3%) were assigned to the case group, 541 (44.0%) to the control group, and 452 (36.7%) samples to the additional group. About 65.9% were obtained from male patients, the mean age of transplant recipients participating in the study was 53.7 ± 13.8 years. The most frequently used immunosuppressive drugs were tacrolimus (92.8%), mycophenolate mofetil (88.0%), and steroids (79.3%). Antihypertensives and antidiabetics were used in 88.0 and 27.4% of the patients, respectively. Approximately 20.9% of patients showed the presence of circulating donor-specific anti-HLA IgG antibodies at time of biopsy. Most of the samples (51.1%) were collected within the first 6 months after transplantation, 48.0% were protocol biopsies, followed by event-driven (43.6%), and follow-up biopsies (8.5%). Over time the proportion of biopsies classified into the categories Banff 4 (T-cell-mediated rejection [TCMR]) and Banff 1 (normal tissue) decreased whereas Banff 2 (antibody-mediated rejection [ABMR]) and Banff 5I (mild interstitial fibrosis and tubular atrophy) increased to 84.2 and 74.5%, respectively, after 4 years post transplantation. Patients with rejection showed worse kidney function than patients without rejection.
Conclusion: The clinical characteristics of subjects recruited indicate a patient cohort typical for routine renal transplantation all over Europe. A typical shift from T-cellular early rejections episodes to later antibody mediated allograft damage over time after renal transplantation further strengthens the usefulness of our cohort for the evaluation of novel biomarkers for allograft damage.
Introduction
Despite a steady improvement of patient and organ survival after renal transplantation, allograft rejection continues to pose a risk of graft damage. In the first week and month after transplantation, T-cell-mediated rejection (TCMR) in particular is more common, while later antibody-mediated rejection (ABMR) accounts for the majority of immunological graft damages (1, 2).
Changes in kidney function, a decrease in urine output, or an increase in proteinuria may reflect transplant rejection during routine clinical patient care. Kidney biopsies are still current gold standard for diagnosing an allograft rejection, but as an invasive procedure it carries the risk of bleeding and other complications. The latter limits the routine use of serial biopsies, and the diagnosis of rejection is often made at an advanced stage of irreversible tissue injury. At many transplant units, protocol biopsies have been introduced to potentially detect the acute rejection already in a sub-clinical state (3). However, with serial biopsies, it is unlikely that all rejection episodes will be detected upon onset, not to speak of complications associated with such a costly approach (4).
Biomarkers in the urine could help to detect rejections early and non-invasively, whereby an appropriate sensitivity and specificity as well as a quick diagnosis are necessary for the clinical routine (5, 6).
Recently, we developed a novel, non-invasive method to detect the graft rejection via a characteristic constellation of the urine metabolites alanine, citrate, lactate, and urea investigated by NMR spectroscopy (7). In a first monocentric prospective observational (UMBRELLA) study which included 109 patients, the test performance reached an area under the curve (AUCROC) value of 0.84 when combining metabolomic analysis and corresponding estimated glomerular filtration rate (eGFR) values at time of urine sampling (8).
The subsequently following PARASOL study presented here is an open, international, multicenter, prospective, observational study, in which the diagnostic accuracy for the urinary metabolite constellation initially assessed in the UMBRELLA study will be validated in an independent cohort resembling the routine kidney transplantation programs in six different European transplant centers. The study is based on a reasonable number of patients recruited with their respective urine samples and renal allograft biopsies, such as both protocol and event-driven biopsies.
Materials and Methods
Study Design
Urine samples were taken from adult (≥18 years) renal or combined renal and pancreas transplant patients prior to a kidney biopsy that was performed according to local center standards as protocol or event-driven biopsies. The target population is thus within the clinical routine and planned for renal allograft biopsies. The patient population consists of patients recruited at least 14 days after transplantation. To ensure broad real-world spectrum of biopsy results, all patients scheduled for a renal allograft biopsy were screened for eligibility.
Between June 2017 and March 2020, 972 transplant recipients were included (1,230 urine samples and matched biopsies, respectively). According to biopsy results, patients were retrospectively assigned to a case group [Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other findings (other non-rejection changes)], a control group [(no rejection): Banff categories 1 (normal biopsy), 5I (mild interstitial fibrosis and atrophy (IFTA)], and an additional group [Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes)]. Criteria for subject categorization—based on the rules of the Banff classification—are detailed in Figure 1.
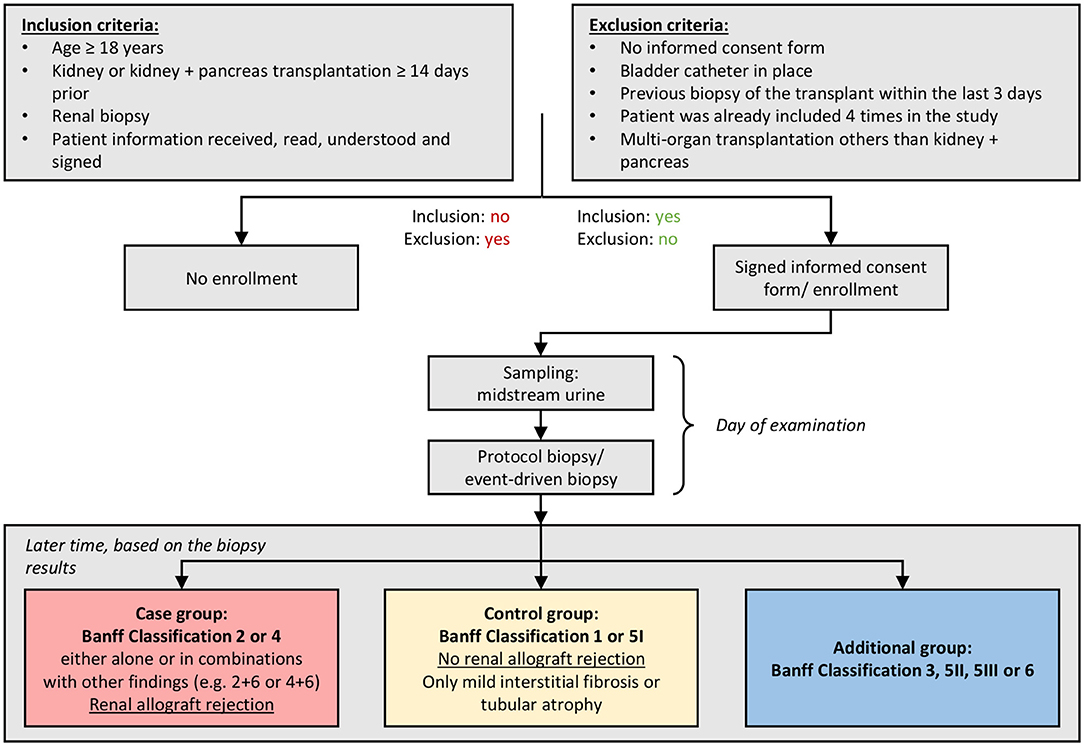
Figure 1. Study sequence. Patients who received a kidney or kidney and pancreas transplantation ≥14 days prior were selected according to the inclusion criteria of the PARASOL study. After informed consent discussion and signed informed consent form, the clinical data were recorded, the midstream urine sample was collected, and the kidney biopsy was taken within the clinical routine. According to biopsy results, patients were assigned either to a case group [Banff category 2 (antibody-mediated rejection [ABMR]) or 4 (T-cell-mediated rejection [TCMR]), either alone or in combination with other findings (other non-rejection changes)], a control group [(no rejection): Banff categories 1 (normal biopsy), 5I (mild interstitial fibrosis and atrophy (IFTA)], and an additional group [Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes)]. The study was then ended for the participant.
Clinical routine shows that patients of the target population may be biopsied several times. In this context, PARASOL collected data on the day of the examination (cross-sectional data), but did not take any data over time (longitudinal data) into account. This resulted in the possibility that some patients were included in the study several times. These patients signed the informed consent forms again and new patient identification numbers were given (at a maximum of four times). The study sequence is similar to an initial recruitment (Table 1).
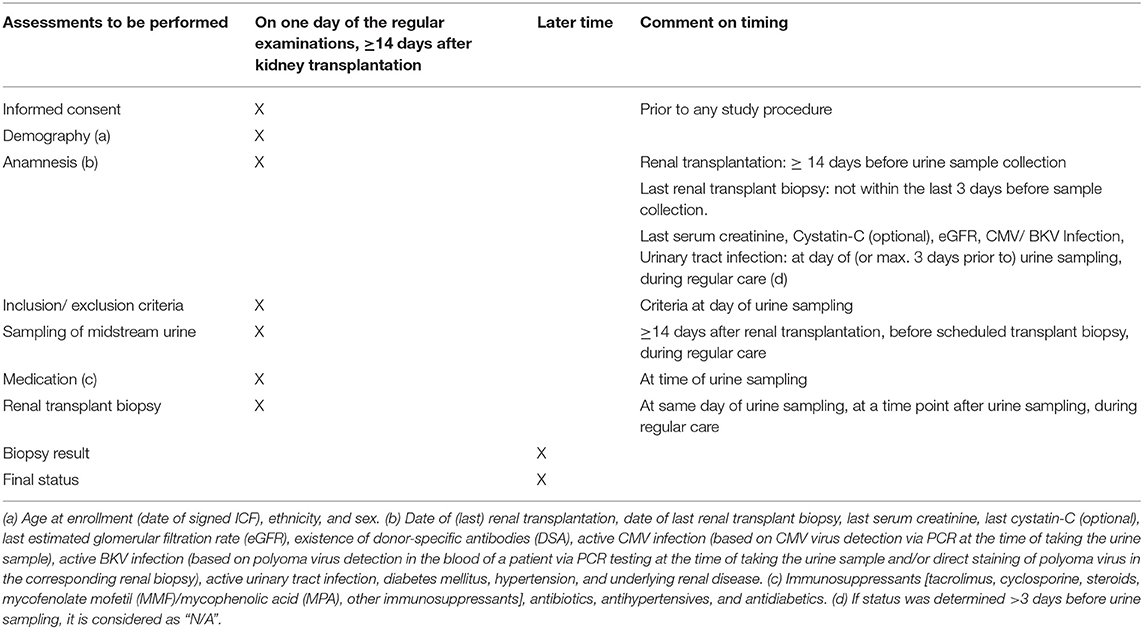
Table 1. Examination matrix.
To preclude an interaction between the biopsy procedure and the results of the NMR analysis samples were obtained before biopsies and, in case of two or more sequential biopsies, a sufficiently large interval between the biopsies was defined in the protocol to prevent possible blood residues in urine affecting the NMR analysis of the second sample. In addition, we defined an upper limit for re-recruitment of a patient. The goal was to include an adequate number of patients to get a representative reflection of the biological variance in the study population. Therefore, a maximum of four biopsies per patient could be included in the study. The patients, such as not willing to participate, with a bladder catheter in place, with a previous biopsy of the transplant within the last 3 days, already included four times in the study, and after multi-organ transplantation other than kidney and pancreas, are excluded from the study. Respective clinical data (e.g., date of transplantation, medication, donor-specific anti-HLA IgG antibodies (DSA), former rejections, and infections) were collected on the day of the examination and the urine sample was taken immediately before the planned biopsy. The report of the kidney histopathology analysis, as clinical reference standard, was added to the study documentation after becoming available. Definition of DSA was done individually according to local center standards. The threshold for the positivity was defined as 800–1,000 mean fluorescence intensity (MFI) depending on the local protocol and assay used. The centers used mixed and single antigen (SAB) class I and class II bead assays. No follow-up appointments were planned for the study participants.
The study was approved by the local Ethics Committees of all participating centers. The written informed consent was received from participants prior to study inclusion.
Kidney Biopsies
The results of morphologic renal allograft evaluation were documented as the reference standard. The study included protocol biopsies (as per local center protocol), event-driven biopsies, as well as follow-up biopsies performed for monitoring of treatment responses. Specimens were evaluated in the context of center routine by experienced local renal pathologists following the rules of the 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology (9). For analysis in relation to biomarker results, biopsies were grouped according to Banff diagnostic categories as follows: (i) case group (rejection): Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other findings (other non-rejection changes) (ii) control group (no rejection): Banff categories 1 (normal biopsy), 5I (mild IFTA) (iii) additional group: [Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes)], respectively.
NMR-Analysis
Spontaneous mid-stream urine samples were collected and measured by NMR spectroscopy at numares AG (Regensburg, Germany). For this, a volume of 600 μl of each urine sample was mixed with 150 μl of Axinon® urine additive solution in a centrifuge tube. The samples were centrifuged at 20,000 g for 10 min at 20°C, and 600 μl of the supernatant were transferred to 5 mm NMR tubes and kept at 2–6°C until measurement. All measurements were carried out on a Bruker Avance II + 600 MHz NMR-spectrometer as already described before (7). Using the Axinon® renalTX-SCORE® system, urinary metabolite quantification and test results were generated in a fully automated manner. The resulting score correlates with the probability of allograft rejection and ranges between 0 and 100 with low to high probability and is based on an NMR-based pattern encompassing the metabolites alanine, citrate, lactate, and urea.
Statistical Analysis Strategy
Statistical analyses were planned in two ways: a descriptive analysis and a performance analysis. The former was to address the patient data and highlight demographic facts using clinical data derived from the corresponding case report form (CRF). It was planned that important variables, such as sex, age, ethnicity, and various disease factors of the patients would be investigated. Furthermore, all variables were considered to be used for the performance analysis.
It was clear that it may be necessary to exclude patient data from the performance analysis in case that technically no renalTX-SCORE output could be determined by NMR measurement. The performance analysis should use standard methods and assess conventional parameters for evaluating the quality of the diagnostic patterns developed. Particular attention to the area under the receiver operating characteristic (ROC) curve (AUCROC), specificity, and sensitivity should be paid. In addition, certain subgroup performance analyses should be obtained in concerns of different cut-off values with regard to specificity and sensitivity.
Sample Size Estimation
The number of cases was based on the observed values for the AUCROC values of the NMR-based patterns obtained in the UMBRELLA (8) study for the detection of acute renal allograft rejection (AUCROC = 0.75). In particular, the number of cases in the multicenter validation should be large enough to prove a difference between the AUCROC value of the developed NMR-based tests and a minimum AUCROC (null hypothesis H0) of 0.675 at the level of significance α = 5% with a power of 80%. The percentage of positive biopsy results (prevalence of acute Banff 4 renal allograft rejection) in the UMBRELLA collective was 27% (54/203 biopsies). The expected percentage of positive biopsy results in the PARASOL study was therefore estimated to be 30%. Accordingly, 151 rejections (cases) and 334 controls were needed. The indicated number of cases was calculated using the MedCalc v.12.7.7.0-64 bit, observing a two-tailed binomial test with a power of 80%. To compensate for the losses in recruiting, withdrawal of consent, insufficient urine quantities, losses, etc., a 15% safety margin was calculated so that recruiting should include 174 cases: renal allograft rejection Banff 2, 4, either alone or in combination with other findings, e.g., 2 + 6 or 4 + 6, and 384 controls: Banff classification 1 and 5I.
The estimated number of cases was exceeded with 237 cases instead of estimated 174 cases and 541 controls instead of the planned 384.
Primary Endpoint
The primary endpoint of the study is the respective AUCROC value of the ROC curve for the NMR-based pattern. Acute renal allograft rejection is defined according to the Banff classification and categorized 2 (ABMR), 4 (TCMR), either alone or in combinations with other findings, e.g., 2 + 6 or 4 + 6. The AUCROC values and their 95% CIs are determined as a measure of diagnostic accuracy. It should be tested whether the diagnostic accuracy is to be proven with an AUCROC value of at least 0.675 under the assumption that the observed AUCROC value itself is 0.75.
Secondary Endpoint
As a secondary endpoint, the recruited collective will be analyzed with respect to the determination of cut-off values associated with a sensitivity and specificity of 90% and the respective specificity at 90% sensitivity and sensitivity at 90% specificity including the 95% CI for the exact definition of the NMR-based pattern to detect renal allograft rejection. In addition, for the cut-off values determined, the sensitivities and specificities in patients with Banff classification 3, 5II, 5III, and 6 will be determined in a subgroup analysis if enough samples are available. Furthermore, the demographic and clinical parameters will be used to examine whether individual parameters or a group of these parameters are suitable for reliably predicting the occurrence of renal allograft rejection in this large, non-stratified patient group.
Results
In the context of PARASOL (multicenter observational prospective trial including six European transplant centers), a total of 1,230 urine samples for metabolite evaluation and corresponding histopathology results (972 patients; 1.3 samples per patient) were collected (recruitment period between June 2017 and March 2020).
Table 2 provides sample and patient characteristics for the overall cohort and individual centers. Among 1,230 biopsy specimens, 237 samples (19.3%) were assigned to the case group, 541 to the control group (44.0%), and 452 (36.7%) samples were assigned to the additional group. Overall, 810 samples (65.9%) were obtained from male patients and 420 (34.1%) from female patients. The mean recipient age at the time of study inclusion was 53.7 ± 13.8 years (range 19–84 years) and most of the patients were Caucasian (96.3%).
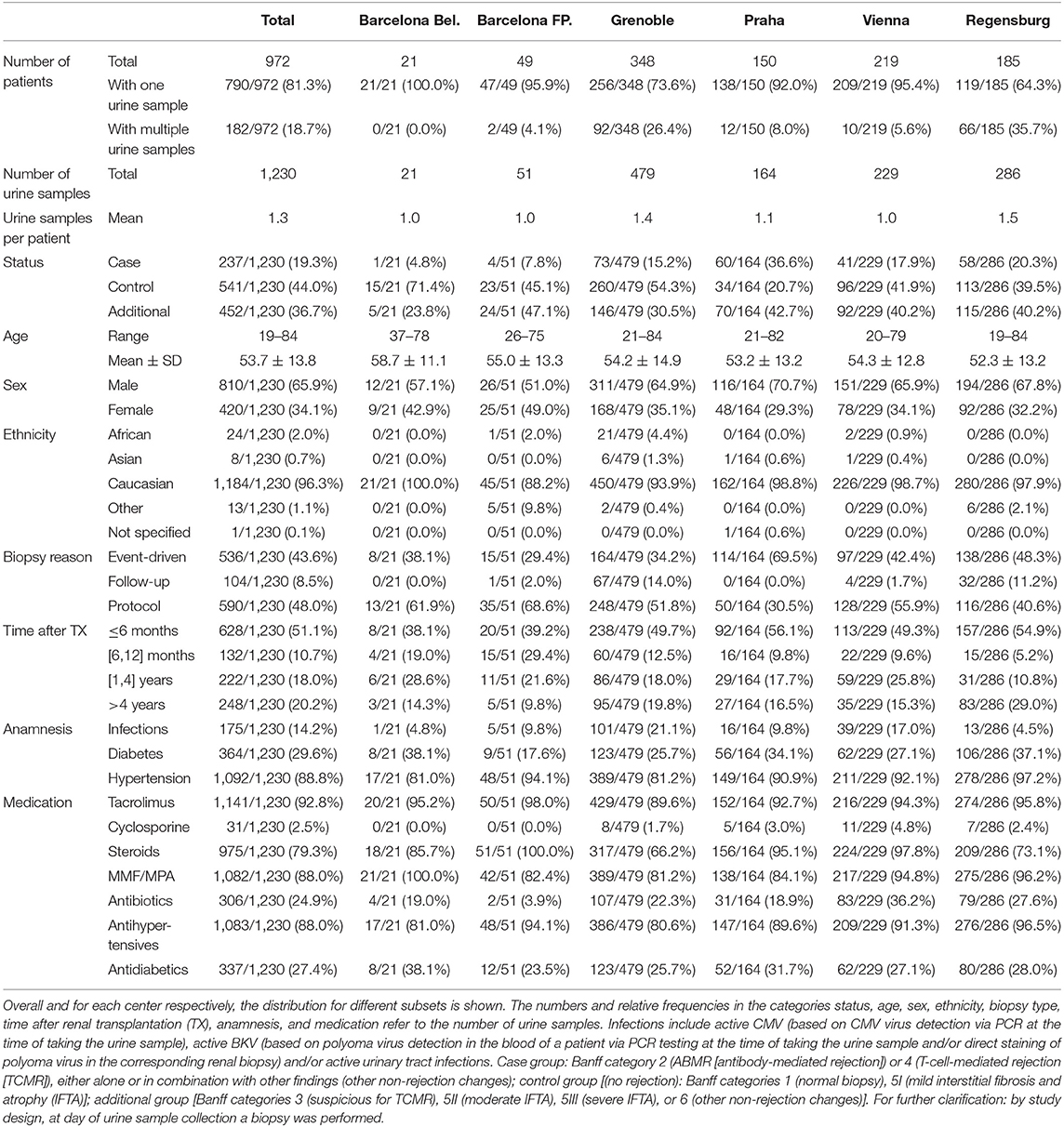
Table 2. Urine sample characteristics collected by the six different study centers.
Tacrolimus (92.8%), mycophenolate mofetil (88.0%), and steroids (79.3%) were the most frequently used immunosuppressive drugs. Antihypertensives and antidiabetics were used in 88.0 and 27.4% of the patients, respectively. About 88.8% of patients suffered from hypertension, 29.6% were diabetics, and 14.2% had any infection (BKV, CMV, or urinary tract infection) at the time of inclusion into the study.
Of the 1,230 urine samples, 628 (51.1%) were collected within the first 6 months after transplantation, 132 (10.7%) between 6 and 12 months, 222 (18.0%) between 1 and 4 years, and 248 (20.2%) more than 4 years after transplantation. Most of the samples [590 (48.0%)] were in the context of protocol biopsies, followed by event-driven biopsies [536 (43.6%)], and follow-up biopsies [104 (8.5%)].
The distribution of biopsy types for case, control, and additional group differed in the groups. In the case group, 62.9% event-driven biopsies were noted, 24.1% protocol biopsies, and 13.1% follow-up biopsies. In the control group, 71.3% protocol biopsies, 23.1% event-driven biopsies, and 5.5% follow-up biopsies were seen. The additional group consisted of 58.0% event-driven biopsies, 32.5% protocol biopsies, and 9.5% follow-up biopsies (Figure 2 and Supplementary Table S1). Additionally Supplementary Figure S1 and Supplementary Table S2 show the distribution of the case, control, and additional groups within each of the three biopsy reasons: event-driven, follow-up, and protocol.
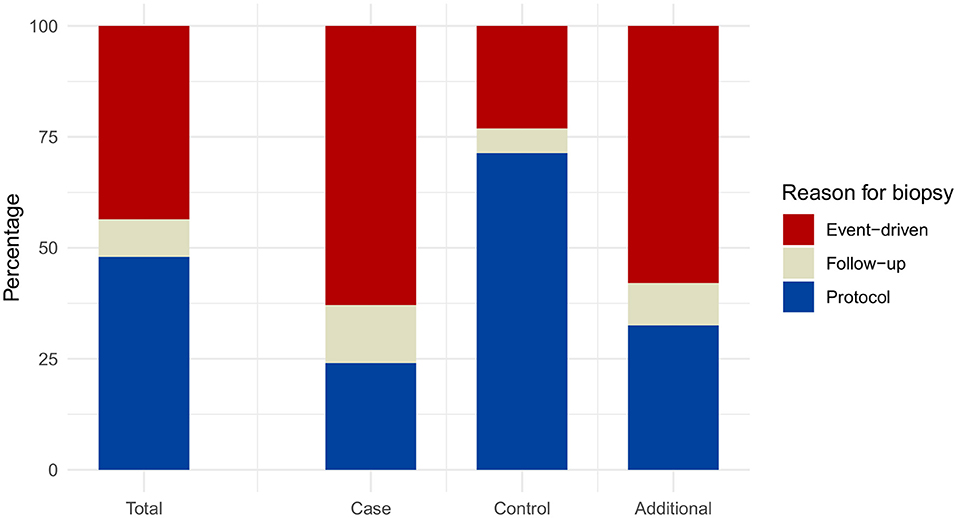
Figure 2. Distribution of the reasons for biopsy. Relative frequencies are displayed for the total number of samples (irrespective of the group assignment), as well as for each of the status groups. Case group: Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other non-rejection changes; Control group: Banff categories 1 (normal biopsy), 5I (mild IFTA); Additional group: Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes).
Distribution of Banff Categories Within Case (Rejection), Control, and Additional Group
Most of the biopsies (44.0%) were assigned to the control group, corresponding histopathology showed classification into the Banff categories 1 (normal biopsy) (28.0% out of all biopsies) and Banff 5I (mild IFTA) (16.0% out of all biopsies) for the largest proportion of findings, followed by other combinations (15.2%) and allograft fibrosis classified as Banff grades 5 II (moderate IFTA) and III (severe IFTA) (10.0%) both belonging to the additional group (Figure 3 and Supplementary Table S3).
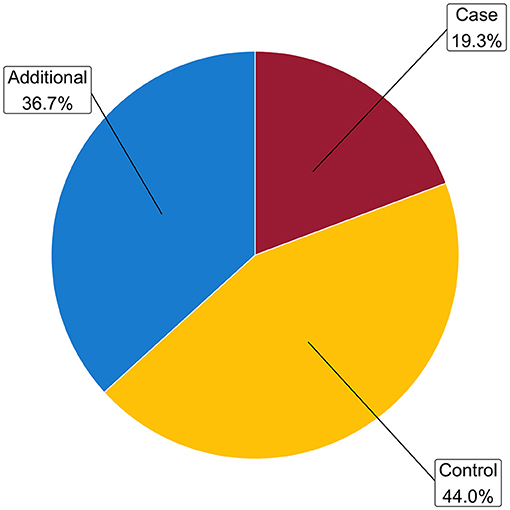
Figure 3. Distribution of the status groups. Relative frequencies are derived from the total number of samples. Case group: Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other findings (other non-rejection changes); control group [(no rejection): Banff categories 1 (normal biopsy), 5I (mild IFTA); additional group (Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes)].
Within the group of rejection, ABMR (Banff 2) represented the largest proportion (64.6%), followed by TCMR (Banff 4: 30.4%). Combined ABMR and TCMR was infrequent (5.1%) (Figure 4 and Supplementary Table S3). The control group showed further a higher proportion of Banff 1 (63.6%) than of Banff 5I (36.4%) graded biopsies (Figure 4 and Supplementary Table S3). In the additional group, the highest proportion of pathology findings belongs to other combinations (41.4%), Banff 5II and III (27.2%), followed by Banff 6 (17.0%) and Banff 3 (14.4%) (Figure 4 and Supplementary Table S3).
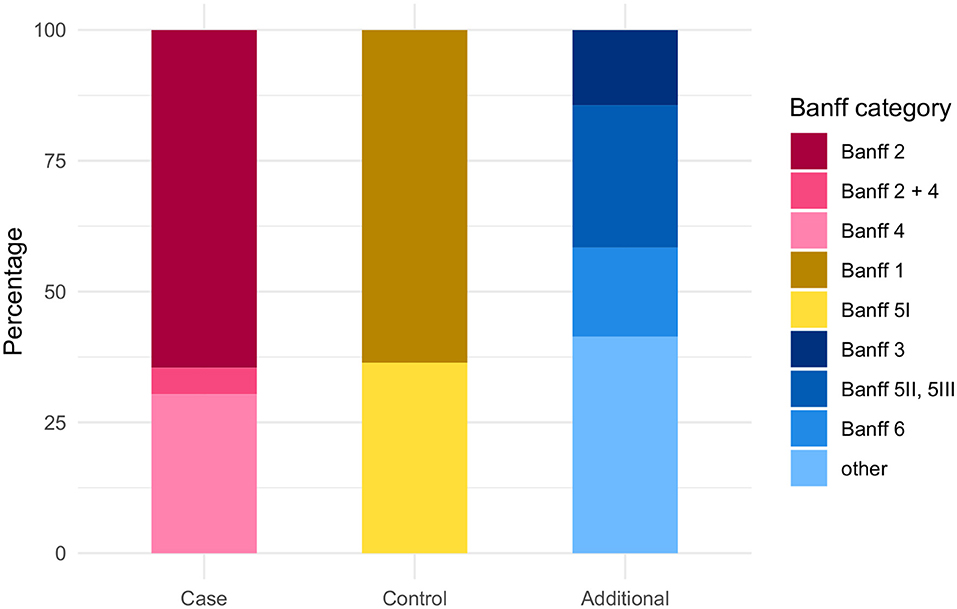
Figure 4. Distribution of Banff categories among the case, control, and additional group. Case group: Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other non-rejection changes; Control group: Banff categories 1 (normal biopsy), 5I (mild IFTA); Additional group: Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes).
Type of Renal Allograft Rejections Dependent From Time After Transplantation
Within the case group, ABMR classified as Banff 2 category (either isolated or in combination with other lesions) represented a large group of rejections with 42.0% already within the first 6 months post transplantation. With increasing time post-transplantation, the proportion of antibody mediated rejection increased up to 84.2% (after 4 years). TCMR (Banff 4 and Banff 4 + x) decreased from 50.7 to 11.8% over time. The combination of both stayed stable with 7.3% and 4.0% (Figure 5A and Supplementary Table S4).
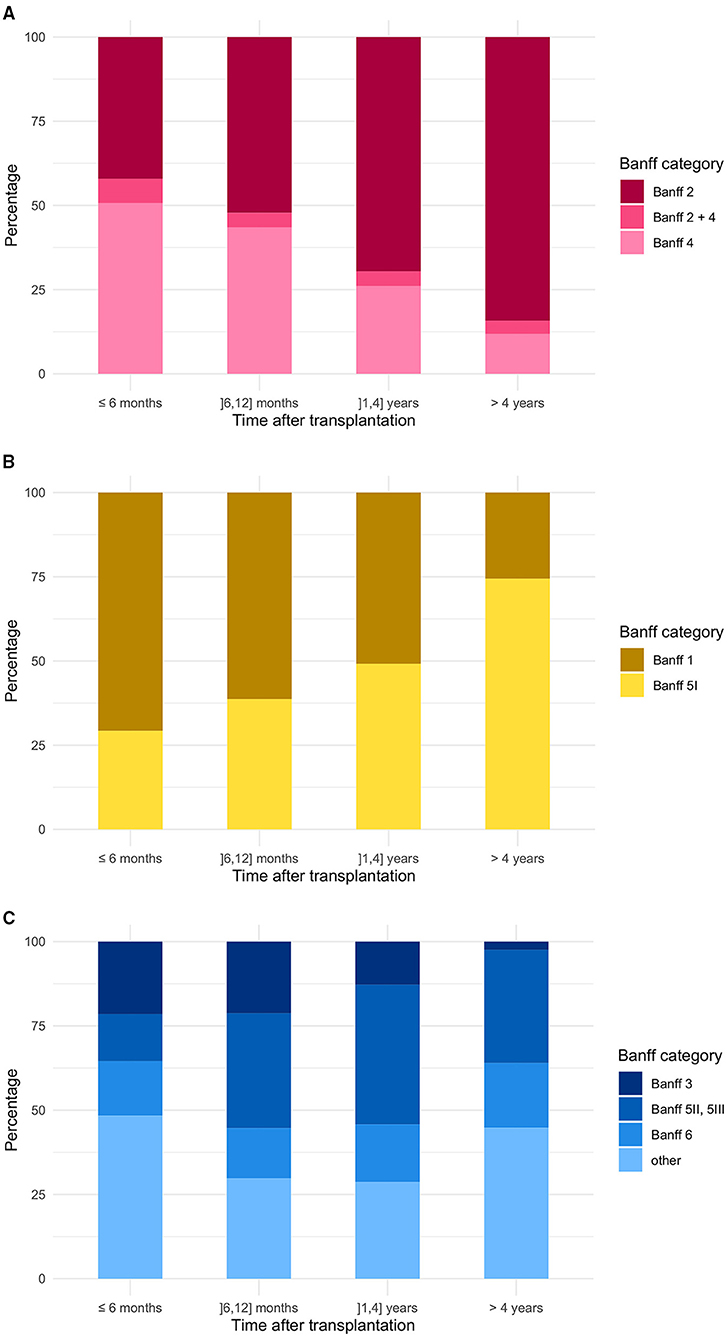
Figure 5. Banff category distribution in concerns of time after renal transplantation (A) in the case group, (B) in the control group, and (C) in the additional group. Case group: Banff category 2 (ABMR) or 4 (TCMR), either alone or in combination with other non-rejection changes; Control group: Banff categories 1 (normal biopsy), 5I (mild IFTA); Additional group: Banff categories 3 (suspicious for TCMR), 5II (moderate IFTA), 5III (severe IFTA), or 6 (other non-rejection changes).
In the control group within the first 6 months, most biopsy samples were assigned to Banff 1 (70.8%), whereas after 4 years, almost 75% of biopsies of the control group were classified as Banff 5I (Figure 5B and Supplementary Table S4).
In the additional group, the proportion of borderline rejections (Banff 3) decreased from 21.5 to 2.4% over time, whereas the amount of graft fibrosis represented by Banff 5II and III findings increased to 33.6% (Figure 5C and Supplementary Table S4).
Detection of Donor-Specific Antibodies (DSA) Dependent on Sample Classification and Banff Categories
For 257 of the 1,230 samples, positive corresponding DSA results were documented (20.9%) (Table 3). Within the case group for 43.5% of the samples (103/237), DSAs were noted. 84 from these samples (81.6%) showed ABMR (Banff 2). Simultaneous presence of DSA in blood was documented for only 80/541 samples (14.8%) from the control group patients. Therein, in the subgroup associated with Banff 1 findings in the biopsy 46/80 (57.5%) samples corresponded to patients with DSA, in the subgroup with Banff 5I lesion, the rate was 34/80 (42.5%). In the additional group, 74/452 (16.4%) samples were associated with DSA.
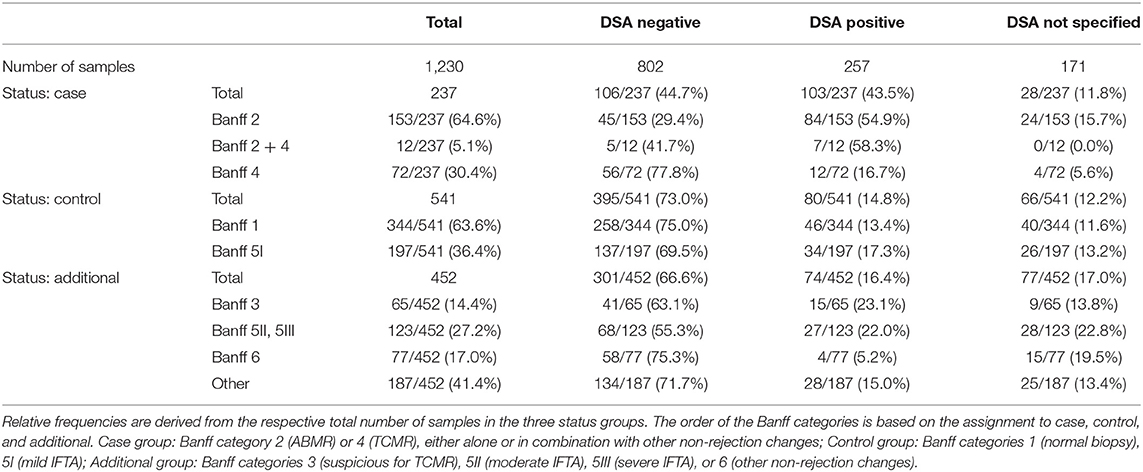
Table 3. Existence of donor-specific anti-HLA IgG antibodies (DSA) in the status groups and each of the Banff categories.
Distribution of Chronic Kidney Disease (CKD) Stages Among Status, Time After Renal Transplantation, and Recipient Age
Kidney function was seen to be dependent on the status (case/control/additional), time after transplantation, and the recipient age.
Regarding the severity of CKD of the study population, patients with allograft rejections and from the additional group showed significantly worse kidney function than controls (samples 318 corresponding with CKD stage 4 or 5 32.9% in cases vs. 11.4% in controls vs. 32.6% in the additional group; Table 4). Whereas control group samples were associated with good allograft function up to 4 years, case group samples and additional group samples corresponded with worse kidney function (Table 4).
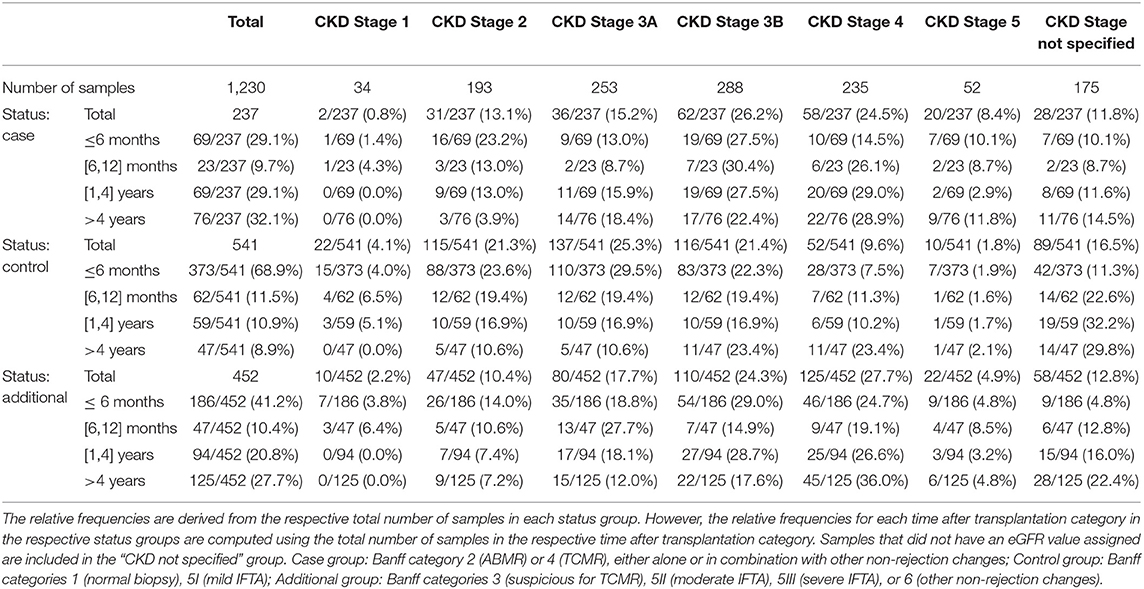
Table 4. Distribution of chronic kidney disease (CKD) stages among status groups and time after renal transplantation (TX).
With regards to the allograft recipient age, it could be seen that controls showed a better renal function within all age groups compared with cases and samples from the additional group (Table 5).
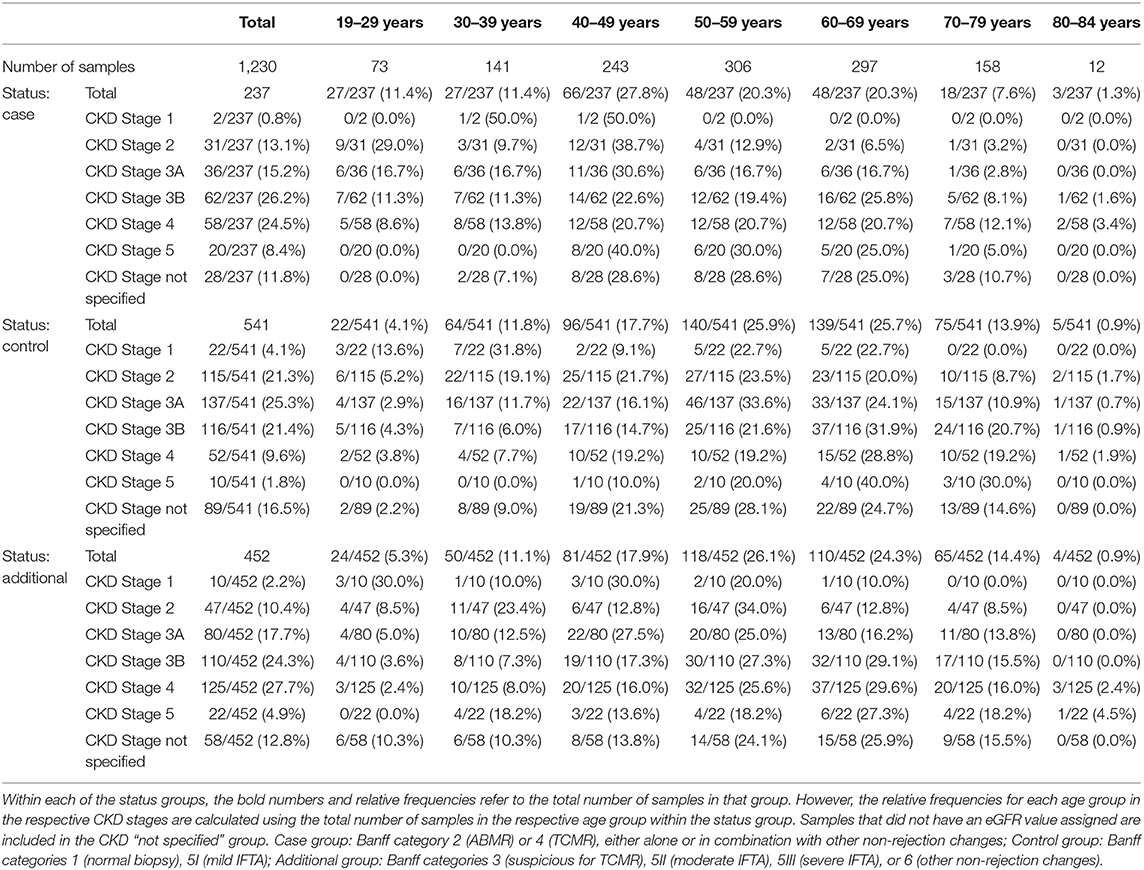
Table 5. Distribution of CKD stages in different age groups shown for case, control and additional group.
Discussion
For patients with end stage renal disease, kidney transplantation is the renal replacement therapy of choice as it significantly improves the life quality and life expectancy (10). However, by far not all suitable patients can be offered a donor kidney as both post-mortal and living kidney donation are limited. With the observed increase in patients in the majority of countries worldwide suffering from renal disease, the gap between donor kidneys available and renal transplantation needed is more and more widening (11–13). One of the reasons of this observation is that renal allograft survival is limited and often shorter as the survival of recipient. In consequence, increasing numbers of patients with end stage renal disease need more than only one kidney transplantation and in countries with a very high rate of post-mortal organ donors, such as Spain, loss of a previous allograft is nowadays one of the main causes for listing patients for renal transplantation (14–23)1.
Therefore, one of the major goals in transplant medicine is to prolong the time of allograft survival, especially as more and more allografts with extended donor criteria have to be used to overcome organ shortage (2, 24–28). Despite major improvements in transplant patient care and therein immunosuppressive treatment, acute and chronic rejection processes often irreversibly damaging renal allograft tissues are still a major risk for premature allograft loss (1, 2, 29). Strategies to completely prevent allograft rejection are still missing, and diagnostic procedures for early detection of rejection are still suboptimal.
Until now, a histopathological evaluation of a renal allograft biopsy is the gold standard to detect the cause of an allograft malfunction after extra renal problems, such as perfusion deficits or urinary obstruction could be ruled out (1, 3, 4). Molecular analyses of renal tissue samples become more and more important and look very promising to become routine in the future, however, so far in many countries, this technique is not available due to its costs not routinely covered by medical insurance companies.
Several biomarkers have been previously described mainly in blood samples to detect allograft damage without performing renal biopsies, and costs and insufficient proof of usefulness under routine conditions are among the reasons for only limited use in daily clinical practice so far (5, 6, 30–35).
A characteristic urinary metabolite constellation for the detection of TCMR in renal allografts has been previously described by our group (7, 8). In combination with the eGFR values of patient, this test was previously proposed as a valuable support in biopsy decision-making and routine follow-up after renal transplantation. However, so far two main reasons limit the use of this test system in the clinic. The one is that all results generated so far were based on single center studies. The second reason is that the original cohort used to develop the test system was dominated by cellular rejections as these could be easily diagnosed in corresponding kidney biopsies at the time of development.
To overcome these limitations, the PARASOL study was initiated as a further completely independent validation study. Major aims of the PARASOL study were evaluation of the test system completely under routine conditions in six large, different European transplant centers. All centers were completely free in including suitable patients transplanted with donor organs retrieved as usually done in the respective country. Additionally, all treatment strategies, i.e., for immunosuppressive therapy, concomitant medication, routine follow-up visits, and renal biopsy, were on purpose not standardized to recruit a study population typical for renal transplant recipients all over Europe.
Successful recruitment of the study is described here along with an in-depth analysis of the study population, urine samples collected and correlation of these with biopsy findings, and analyses for the presence of donor specific antibodies in blood samples of the allograft recipients at the time of renal biopsies. All biopsies were evaluated by experienced renal pathologists according to the Banff classification systematics. Taking clinical findings, laboratory values, and histopathological results into account, the patients were grouped by the investigators into so called “cases,” “controls,” and “additional,” respectively. This will allow not only to discriminate rejecting from non-rejecting allografts. With this strategy, changes in the urine metabolome can be also correlated with pre-existing, i.e., donor-derived and de novo allograft damages over time and of all types, such as cellular and antibody mediated acute and chronic allograft lesions.
The complete documentation of 1,230 urine samples along with corresponding histopathology reports and blood analyses for donor specific antibodies from 972 different patients (approximately one third of them with rebiopsies during the study), will allow to evaluate the urinary metabolite changes for a wide variety of different allograft damages alone or in combination and with different severity, all being representative for typical patient courses after renal transplantation.
Future goals for the test progress are the validation of previous findings in an actual multicenter setting, detection and differentiating antibody-mediated rejection from cellular rejection and recognition of potential disruptive factors other causes of allograft damage.
In conclusion, the clinical part of the PARASOL study as an international, multicenter study representative for typical renal transplant patients in Europe could be finished successfully. All urine samples, renal biopsy pathology results, and biographic and clinical patient data are validated and now available for further spectroscopic and metabolomic analyses.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University Regensburg (principal investigator #16-315-101) and Local Ethics Committees. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MB, GB, OV, LR, SN, ES, and BB designed the study. LG, OB, and H-JG gave conceptual advice to the study protocol and the enrollment strategy. MB, GB, OV, LR, LG, OB, and BB were local principal investigators for the participating transplant centers and enrolled together with their study personnel all participating patients. H-JG and KK gave advice on histopathological evaluation and classification of renal biopsy findings. MB, SN, VR, AS, TJ, CF, DZ, TB, FP, VH, and ES collected study material and data and were responsible for raw data controls. SN, VR, AS, and ES supervised and evaluated metabolomic analyses and performed statistical evaluations. MB and BB wrote the manuscript. All authors evaluated study data and contributed to the writing of the manuscript.
Funding
This study was sponsored by numares AG.
Conflict of Interest
SN, VR, AS, and ES report personal fees from numares AG, outside the submitted work. In addition, SN has a patent WO2018167157A1 pending that is directly related to this work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank Lydia Walkowski for her meticulous collection of patient data and samples, Stefanie Kühn and Torsten Schramm for their great work in data entry, and Markus Fuhrmann and Christiane Kiske from numares for excellent technical assistance. We would also like to thank the study coordinators and nurses from all centers who helped with sample management.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.780585/full#supplementary-material
Abbreviations
ABMR, antibody-mediated rejection; AUCROC, area under the ROC curve, CKD, chronic kidney disease; DSA, donor-specific anti-HLA IgG antibodies; eGFR, estimated glomerular filtration rate; NMR, nuclear magnetic resonance spectroscopy; ROC, receiver operating characteristic; TCMR, T-cell- mediated rejection; MFI, mean fluorescene intensity; MMF, mycofenolate mofetil; MPA, mycophenolic acid.
Footnotes
References
1. Nankivell BJ, Alexander SI. Rejection of the kidney allograft. N Engl J Med. (2010) 363:1451–62. doi: 10.1056/NEJMra0902927
2. Hariharan S, Israni AK, Danovitch G. Long-term survival after kidney transplantation. N Engl J Med. (2021) 385:729–43. doi: 10.1056/NEJMra2014530
3. Chapman JR. Do protocol transplant biopsies improve kidney transplant outcomes? Curr Opin Nephrol Hypertens. (2012) 21:580–6. doi: 10.1097/MNH.0b013e32835903f4
4. Tøndel C, Vikse BE, Bostad L, Svarstad E. Safety and complications of percutaneous kidney biopsies in 715 children and 8573 adults in Norway 1988-2010. Clin J Am Soc Nephrol. (2012) 7:1591–7. doi: 10.2215/CJN.02150212
5. Lo DJ, Kaplan B, Kirk AD. Biomarkers for kidney transplant rejection. Nat Rev Nephrol. (2014) 10:215–25. doi: 10.1038/nrneph.2013.281
6. Suthanthiran M, Schwartz JE, Ding R, Abecassis M, Dadhania D, Samstein B, et al. Urinary-cell mRNA profile and acute cellular rejection in kidney allografts. N Engl J Med. (2013) 369:20–31. doi: 10.1056/NEJMoa1215555
7. Banas M, Neumann S, Eiglsperger J, Schiffer E, Putz FJ, Reichelt-Wurm S, et al. Identification of a urine metabolite constellation characteristic for kidney allograft rejection. Metabolomics. (2018) 14:116. doi: 10.1007/s11306-018-1419-8
8. Banas MC, Neumann S, Pagel P, Putz FJ, Krämer BK, Böhmig GA, et al. A urinary metabolite constellation to detect acute rejection in kidney allografts. EBioMedicine. (2019) 48:505–12. doi: 10.1016/j.ebiom.2019.10.007
9. Roufosse C, Simmonds N, Clahsen-van Groningen M, Haas M, Henriksen KJ, Horsfield C, et al. A 2018 Reference guide to the banff classification of renal allograft pathology. Transplantation. (2018) 102:1795–814. doi: 10.1097/TP.0000000000002366
10. Jofré R, López-Gómez JM, Moreno F, Sanz-Guajardo D, Valderrábano F. Changes in quality of life after renal transplantation. Am J Kidney Dis. (1998) 32:93–100. doi: 10.1053/ajkd.1998.v32.pm9669429
11. McCullough KP, Morgenstern H, Saran R, Herman WH, Robinson BM. Projecting ESRD incidence and prevalence in the United States through 2030. J Am Soc Nephrol. (2018) 30:127–35. doi: 10.1681/ASN.2018050531
12. Wetmore JB, Collins AJ. Meeting the world's need for maintenance dialysis. J Am Soc Nephrol. (2015) 26:2601–3. doi: 10.1681/ASN.2015060660
13. Vanholder R, Domínguez-Gil B, Busic M, Cortez-Pinto H, Craig JC, Jager KJ, et al. Organ donation and transplantation: a multi-stakeholder call to action. Nat Rev Nephrol. (2021) 17:554–68. doi: 10.1038/s41581-021-00425-3
14. Ojo AO, Morales JM, González-Molina M, Steffick DE, Luan FL, Merion RM, et al. Comparison of the long-term outcomes of kidney transplantation: USA versus Spain. Nephrol Dial Transplant. (2013) 28:213–20. doi: 10.1093/ndt/gfs287
15. Perl J, Zhang J, Gillespie B, Wikström B, Fort J, Hasegawa T et al. Reduced survival and quality of life following return to dialysis after transplant failure: the dialysis outcomes and practice patterns study. Nephrol Dial Transplant. (2012) 27:4464–72. doi: 10.1093/ndt/gfs386
16. Coupel S, Giral-Classe M, Karam G, Morcet JF, Dantal J, Cantarovich D et al. Ten-year survival of second kidney transplants: impact of immunologic factors and renal function at 12 months. Kidney Int. (2003) 64:674–80. doi: 10.1046/j.1523-1755.2003.00104.x
17. Clark S, Kadatz M, Gill J, Gill JS. Access to kidney transplantation after a failed first kidney transplant and associations with patient and allograft survival: an analysis of national data to inform allocation policy. Clin J Am Soc Nephrol. (2019) 14:1228–37. doi: 10.2215/CJN.01530219
18. Heaphy ELG, Poggio ED, Flechner SM, Goldfarb DA, Askar M, Fatica R et al. Risk factors for retransplant kidney recipients: relisting and outcomes from patients' primary transplant. Am J Transplant. (2014) 14:1356–67. doi: 10.1111/ajt.12690
19. Johnston O, Rose CL, Gill JS, Gill JS. Risks and benefits of preemptive second kidney transplantation. Transplantation. (2013) 95:705–10. doi: 10.1097/TP.0b013e31827a938f
20. Girerd S, Girerd N, Duarte K, Giral M, Legendre C, Mourad G, et al. Preemptive second kidney transplantation is associated with better graft survival compared with non-preemptive second transplantation: a multicenter French 2000-2014 cohort study. Transpl Int. (2018) 31:408–23. doi: 10.1111/tri.13105
21. Wong G, Chua S, Chadban SJ, Clayton P, Pilmore H, Hughes PD, et al. Waiting time between failure of first graft and second kidney transplant and graft and patient survival. Transplantation. (2016) 100:1767–75. doi: 10.1097/TP.0000000000000953
22. Herrero E, Portillo JA, Ballestero R, Correas MÁ, Domínguez M, Ramos E, et al. Experiencia en terceros, cuartos y quintos trasplantes renales y sus complicaciones. Arch Esp Urol. (2017) 70:815–23.
23. Beltrán Catalán S, Sancho Calabuig A, Molina P, Vizcaíno Castillo B, Gavela Martínez E, Kanter Berga J, et al. Impact of dialysis modality on morbimortality of kidney transplant recipients after allograft failure. Analysis in the presence of competing events. Nefrologia. (2021) 41:200–9. doi: 10.1016/j.nefro.2020.12.007
24. Noble J, Jouve T, Malvezzi P, Süsal C, Rostaing L. Transplantation of marginal organs: immunological aspects and therapeutic perspectives in kidney transplantation. Front Immunol. (2019) 10:3142. doi: 10.3389/fimmu.2019.03142
25. Port FK, Bragg-Gresham JL, Metzger RA, Dykstra DM, Gillespie BW, Young EW, et al. Donor characteristics associated with reduced graft survival: an approach to expanding the pool of kidney donors. Transplantation. (2002) 74:1281–6. doi: 10.1097/00007890-200211150-00014
26. Aubert O, Kamar N, Vernerey D, Viglietti D, Martinez F, Duong-Van-Huyen JP, et al. Long term outcomes of transplantation using kidneys from expanded criteria donors: prospective, population based cohort study. BMJ. (2015) 351. doi: 10.1136/bmj.h3557
27. Sung RS, Guidinger MK, Leichtman AB, Lake C, Metzger RA, Port FK, et al. Impact of the expanded criteria donor allocation system on candidates for and recipients of expanded criteria donor kidneys. Transplantation. (2007) 84:1138–44. doi: 10.1097/01.tp.0000287118.76725.c1
28. Metzger RA, Delmonico FL, Feng S, Port FK, Wynn JJ, Merion RM. Expanded criteria donors for kidney transplantation. Am J Transplant. (2003) 3(Suppl. 4):114–25. doi: 10.1034/j.1600-6143.3.s4.11.x
29. Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant. (2004) 4:378–83. doi: 10.1111/j.1600-6143.2004.00332.x
30. Gwinner W, Metzger J, Husi H, Marx D. Proteomics for rejection diagnosis in renal transplant patients: Where are we now? World J Transplant. (2016) 6:28–41. doi: 10.5500/wjt.v6.i1.28
31. Macpherson NA, Moscarello MA, Goldberg DM. Aminoaciduria is an earlier index of renal tubular damage than conventional renal disease markers in the gentamicin-rat model of acute renal failure. Clin Invest Med. (1991) 14:101–10.
32. Millán O, Budde K, Sommerer C, Aliart I, Rissling O, Bardaji B, et al. Urinary miR-155-5p and CXCL10 as prognostic and predictive biomarkers of rejection, graft outcome and treatment response in kidney transplantation. Br J Clin Pharmacol. (2017) 83:2636–50. doi: 10.1111/bcp.13399
33. Suhre K, Schwartz JE, Sharma VK, Chen Q, Lee JR, Muthukumar T, et al. Urine metabolite profiles predictive of human kidney allograft status. J Am Soc Nephrol. (2016) 27:626–36. doi: 10.1681/ASN.2015010107
34. Bloom RD, Bromberg JS, Poggio ED, Bunnapradist S, Langone AJ, Sood P, et al. Cell-Free DNA and active rejection in kidney allografts. J Am Soc Nephrol. (2017) 28:2221–32. doi: 10.1681/ASN.2016091034
Keywords: kidney transplant rejection, urinary metabolites, biomarker, NMR-spectroscopy, non-invasive test
Citation: Banas MC, Böhmig GA, Viklicky O, Rostaing LP, Jouve T, Guirado L, Facundo C, Bestard O, Gröne H-J, Kobayashi K, Hanzal V, Putz FJ, Zecher D, Bergler T, Neumann S, Rothe V, Schwäble Santamaria AG, Schiffer E and Banas B (2022) A Prospective Multicenter Trial to Evaluate Urinary Metabolomics for Non-invasive Detection of Renal Allograft Rejection (PARASOL): Study Protocol and Patient Recruitment. Front. Med. 8:780585. doi: 10.3389/fmed.2021.780585
Received: 21 September 2021; Accepted: 01 December 2021;
Published: 07 January 2022.
Edited by:
Tujin Shi, Pacific Northwest National Laboratory (DOE), United StatesReviewed by:
Michifumi Yamashita, Cedars Sinai Medical Center, United StatesBurkhard Tönshoff, Heidelberg University Hospital, Germany
Rong-Hai Deng, Sun Yat-sen University, China
Copyright © 2022 Banas, Böhmig, Viklicky, Rostaing, Jouve, Guirado, Facundo, Bestard, Gröne, Kobayashi, Hanzal, Putz, Zecher, Bergler, Neumann, Rothe, Schwäble Santamaria, Schiffer and Banas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miriam C. Banas, bWlyaWFtLmJhbmFzQHVrci5kZQ==