
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 15 December 2021
Sec. Intensive Care Medicine and Anesthesiology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.767182
 Jörn Grensemann*
Jörn Grensemann* Emma Möhlenkamp
Emma Möhlenkamp Philipp BreitfeldPischtaz A. Tariparast
Philipp BreitfeldPischtaz A. Tariparast Tanja PetersMark A. PunkeStefan Kluge
Tanja PetersMark A. PunkeStefan Kluge Martin Petzoldt
Martin PetzoldtBackground: Tracheal intubation in patients with an expected difficult airway may be facilitated by videolaryngoscopy (VL). The VL viewing axis angle is specified by the blade shape and visualization of the larynx may fail if the angle does not meet anatomy of the patient. A tube with an integrated camera at its tip (VST, VivaSight-SL) may be advantageous due to its adjustable viewing axis by means of angulating an included stylet.
Methods: With ethics approval, we studied the VST vs. VL in a prospective non-inferiority trial using end-tidal oxygen fractions (etO2) after intubation, first-attempt success rates (FAS), visualization assessed by the percentage of glottis opening (POGO) scale, and time to intubation (TTI) as outcome parameters.
Results: In this study, 48 patients with a predicted difficult airway were randomized 1:1 to intubation with VST or VL. Concerning oxygenation, the VST was non-inferior to VL with etO2 of 0.79 ± 0.08 (95% CIs: 0.75–0.82) vs. 0.81 ± 0.06 (0.79–0.84) for the VL group, mean difference 0.02 (−0.07 to 0.02), p = 0.234. FAS was 79% for VST and 88% for VL (p = 0.449). POGO was 89 ± 21% in the VST-group and 60 ± 36% in the VL group, p = 0.002. TTI was 100 ± 57 s in the VST group and 68 ± 65 s in the VL group (p = 0.079). TTI with one attempt was 84 ± 31 s vs. 49 ± 14 s, p < 0.001.
Conclusion: In patients with difficult airways, tracheal intubation with the VST is feasible without negative impact on oxygenation, improves visualization but prolongs intubation. The VST deserves further study to identify patients that might benefit from intubation with VST.
Tracheal intubation is required for mechanical ventilation during general anesthesia and to prevent aspiration of secretions. Commonly, direct laryngoscopy (DL) is used, but this technique may fail in patients with a difficult airway (1), e.g., in patients scheduled for otorhinolaryngologic or oral and maxillofacial surgery. Besides intubation with a bronchoscope that is still regarded as the gold standard, videolaryngoscopy (VL) has evolved as a valuable alternative technique in patients with an expected or unexpected difficult airway (2–4). However, VL has some limitations and may fail due to insufficient visualization of the larynx or impossible tube advancement. Recently, a tracheal tube with an integrated camera has been introduced (VST, VivaSight-SL, Ambu A/S, Ballerup, Denmark) that may allow for direct guidance of the tube and may aid in tracheal intubation in patients with difficult airways (5). This tube has been evaluated under the clinical conditions in intensive care patients (6) and patients with morbid adiposity compared with DL (7), but there is a paucity of data in patients with difficult airways, so far. As opposed to VL, the camera axis of VST may be adjusted individually by modifying the angulation of a stylet and by direct steering of the tip of the tube during tube advancement which may provide a benefit in the cases of difficult airways.
Therefore, we assessed the feasibility of intubation with the VST in patients with a predicted difficult airway compared with VL in a prospective randomized non-inferiority trial. Due to the paucity of data in these patients, we chose end-tidal oxygen fractions (etO2) after intubation as an important safety parameter for the primary outcome measure and to ensure adequate oxygenation throughout the intubation procedure.
The study was approved by the Ethics Committee of the Hamburg Chamber of Physicians (PV7276, June 6, 2020, chairman Prof. Dr. Carstensen). All patients provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki, adheres to the current CONSORT guideline, and was registered prior to patient enrolment with ClinicalTrials.gov (NCT04501692) on August 6, 2020.
The VivaOP trial was a prospective randomized non-inferiority trial with a 1:1 allocation ratio conducted in the Center of Anesthesiology and Intensive Care Medicine at the University Medical Center, Hamburg-Eppendorf, Germany.
Patients were eligible if they were at least 18 years old, required transoral tracheal intubation for elective ear, nose, and throat (ENT), or oral and maxillofacial (OMF) surgery, and had an expected difficult airway. To assess airway difficulty, all patients received a structured preoperative airway risk evaluation in line with the standards of the Department of Anesthesiology, such as physical examination, medical history, assessment of the Simplified Airway Risk Index (SARI) (8, 9), Wilson score (10), upper-lip-bite-test (11), and transnasal videoendoscopy, if appropriate. Individuals with an expected difficult airway as rated by the responsible anesthetist in the Pre-assessment Clinic were included while patients with a verified indication for awake tracheal intubation (e.g., via a bronchoscope), transnasal tracheal intubation, rapid-sequence induction, and loose teeth were excluded.
Physicians with a specialization in airway management, i.e., anesthesiology specialists and experienced fellows were chosen as participators and their duration of work experience recorded. All participating anesthetists were trained with the VST in a structured manikin airway training to avoid bias due to insufficient skill level with this device.
Patients randomized to the intervention group received tracheal intubation with a VST. Depending on gender, size of the patient, and planned surgery, tubes with inner diameters of 7.0, 7.5, and 8.0 were available. The tubes camera was connected to an Ambu aView monitor (Ambu A/S, Ballerup, Denmark). The VST with its included rigid stylet was pre-formed to a predetermined standardized angle obtained by prior trials on a manikin set up for a difficult airway and could be modified by the intubating anesthetist. A depiction of the setup and the curvature is provided in Figure 1. To prevent from soiling of the camera by secretions or mucosal contact, the tongue was elevated with a Macintosh type laryngoscope.
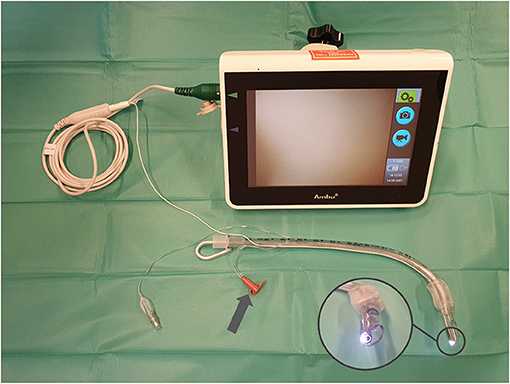
Figure 1. Depiction of the setup of VivaSight-SL tubes. Prepared “optimal” stylet angulation achieved by superposition of 60 intubations in a pretrial manikin training (prepared for difficult airways) by 15 operators. VivaSight-SL tube connected to aView monitor; arrow indicates camera rinsing port; inset depicts camera of tube.
Patients randomized to the control group received tracheal intubation with a C-MAC videolaryngoscope (Karl Storz SE & Co. KG, Tuttlingen, Germany) with a size 3 or 4 Macintosh type blade.
Anesthesia management, the choice of the blade and tube size, as well as the use of adjuncts, such as stylets, introducers, or forceps or airway optimization maneuvers as backward upward rightward pressure (BURP) or optimum external laryngeal manipulation (OELM) were at the discretion of the responsible anesthetist. The tube size was chosen prior to randomization. All intubations were recorded through the respective monitors for later review.
Pre-oxygenation was performed for 5 min with a tight sealing face mask connected to the anesthesia rebreathing circuit (Perseus A500 Anesthesia Workstation, Drägerwerk, Lübeck, Germany). The circuit was flushed before the beginning of pre-oxygenation and an oxygen flow of 15 L/min was maintained throughout.
The primary outcome measure was the lowest end-tidal fraction of oxygen within 2 min after intubation (12). Secondary outcome parameters were the first attempt success rate, the overall success rate with a failure defined as transition to a different device or VL blade type (hyperangulated blade), time to successful intubation, time to successful intubation with one attempt, and total and average number of attempts. Furthermore, the end-tidal carbon dioxide (etCO2) after intubation and Cormack-Lehane grade (13) were obtained. The percentage of glottis opening (POGO) scale (14) was measured from the recorded videos from the frame with the largest glottis orifice area. Intubation difficulty, quality of glottis visualization, and ease of tube advancement were rated on visual analog scales (0–100, lower values better). The complications during intubation as regurgitation, aspiration, hypotension (systolic blood pressure below 70 mmHg), and hypoxia (pulse oximetric saturation below 80%) were recorded (Infinity Delta vital signs monitor, Drägerwerk AG, Lübeck, Germany). Time to successful intubation was measured from the laryngoscope blade passing the teeth to the first of at least three positive, non-declining etCO2 readings (no visual decrease in capnography) obtained by side stream capnography (Perseus A500 Anesthesia Workstation, Drägerwerk AG, Lübeck, Germany).
A priori power analysis indicated a required sample size of 48 patients randomized 1:1 to either VST or VL. This calculation was based on an expected end-tidal fraction of oxygen after intubation of 80% with a SD of 8%, and a non-inferiority margin of 10%, with errors of α = 0.025 and β = 0.2 (PASS version 08.0.6, NCSS, LLC. Kaysville, UT, USA) (12).
Patients were randomized in the operating theater immediately prior to anesthesia induction and after the anesthetist was assigned to the patient and the anesthetist had chosen the required tracheal tube diameter as well as the desired laryngoscope blade size. The randomization codes were obtained from sealed opaque envelopes.
Microsoft Excel 2019 (Microsoft Corp., Redmond, WA, USA) was used for data management and the SPSS statistical software package (version 25, IBM Inc., Armonk, NY, USA) was used for statistical analysis. The t-tests and contingency tables with chi-square and Fisher's tests were used, as applicable. Two-tailed p < 0.05 were regarded as statistically significant.
From August 27, 2020, to February 12, 2021, 48 patients receiving tracheal intubation were randomized to either camera-assisted intubation with the VST or intubation with VL in a 1:1 ratio (as shown in Figure 2). The baseline characteristics of patients are shown in Table 1. Groups had similar values for baseline saturation of oxygen, and end-tidal fractions of oxygen and carbon dioxide after pre-oxygenation (as shown in Table 2). All patients received intubation in deep anesthesia and were paralyzed.
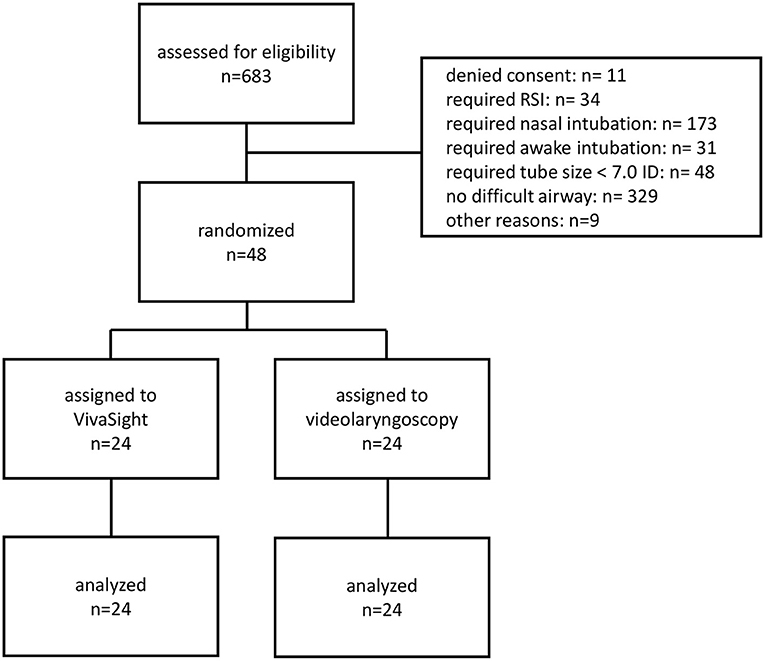
Figure 2. CONSORT diagram. RSI, rapid sequence induction.
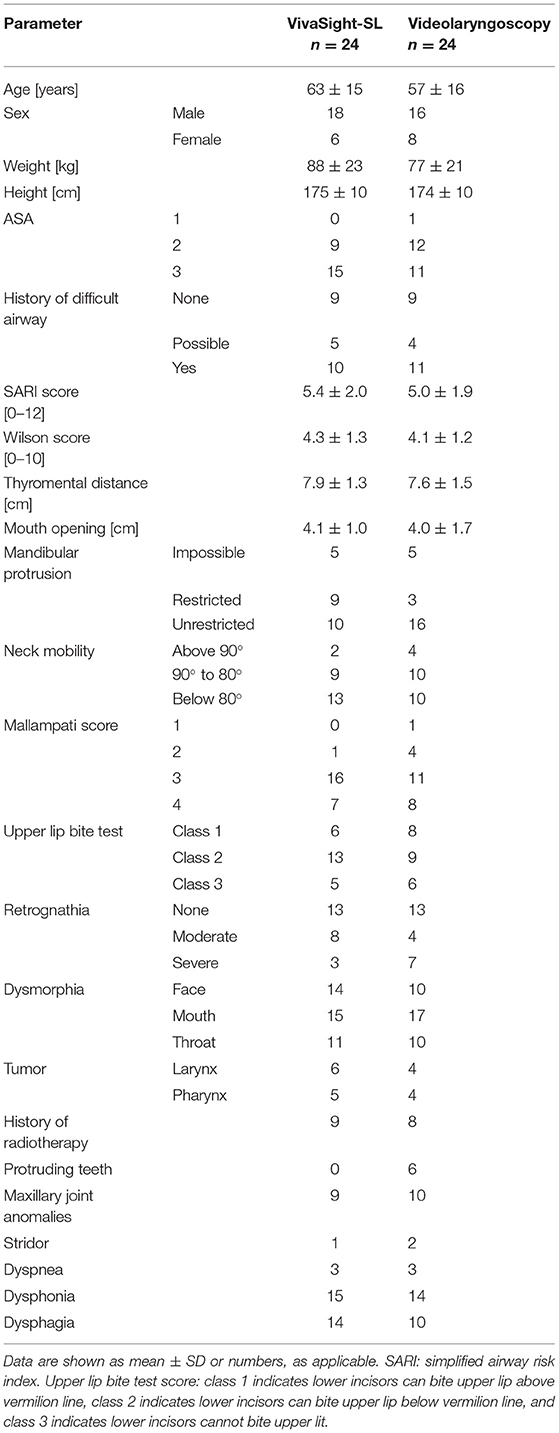
Table 1. The patient characteristics and airway conditions.
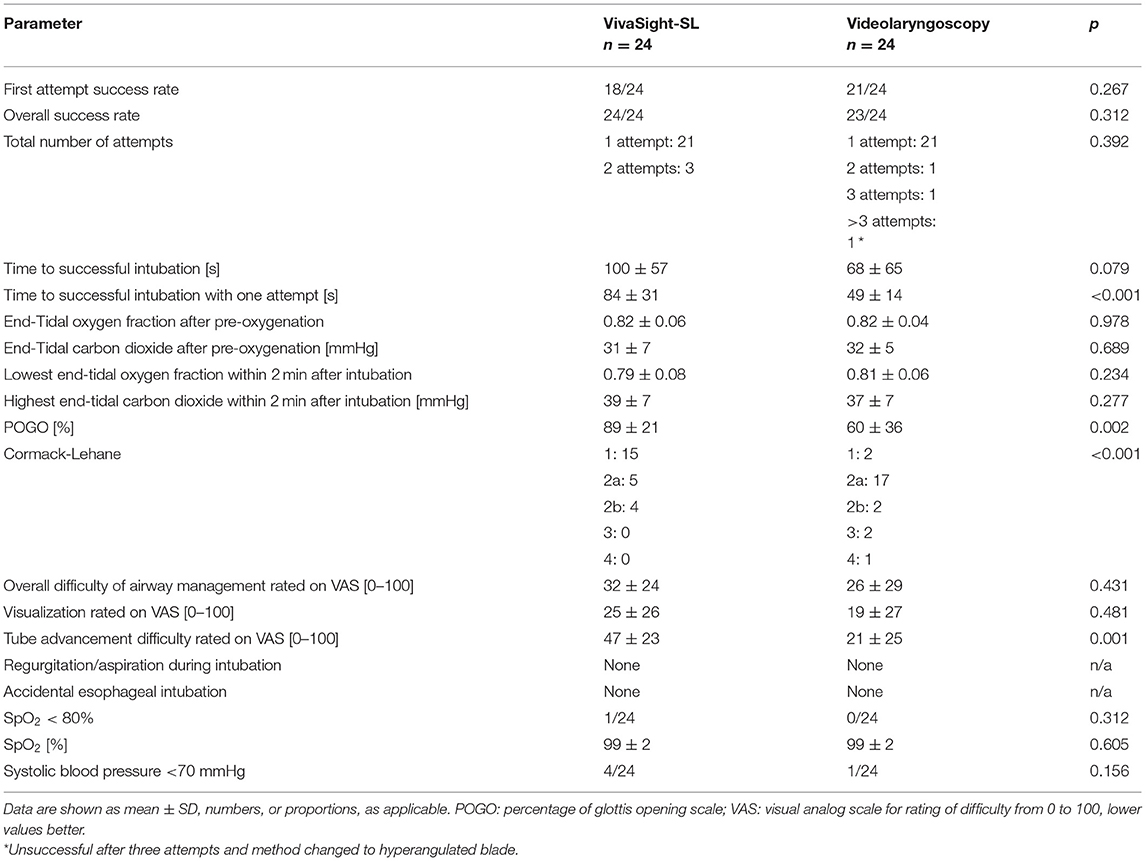
Table 2. Outcome parameters.
Concerning the oxygenation after airway management, intubation with the VST was non-inferior to VL with a post-intubation fraction of oxygen of 0.79 ± 0.08 (95% CIs: 0.75–0.82) in the VST group versus 0.81 ± 0.06 (0.79–0.84) in the VL group with a mean difference of 0.02 (95% CIs: −0.07; 0.02), p = 0.234. The first attempt success rate was 79% in the VST group and 88% in the control group, p = 0.449. The overall success rate in the VST group was 100 and 96% in the VL group (p = 0.312) with one patient requiring a laryngoscopy with a hyperangulated blade. POGO was 89 ± 21% in the VST-group versus 60 ± 36% in the VL group, p = 0.002. While time to successful intubation did not statistically differ between the groups, time to successful intubation in the first attempt was prolonged in the VST group (84 ± 31 s vs. 49 ± 14 s, p < 0.001). A graphical depiction is given in Figure 3. Tube advancement was rated to be more difficult for the VST (visual analog scale 0–100, lower values better: 47 ± 23 vs. 21 ± 25, p = 0.001). Other parameters did not differ between the groups. Regurgitation, aspiration, or accidental esophageal intubation did not occur in any patient. An overview on results is given in Table 2. Anesthetists professional experience was 16 ± 5 years in the VST and 15 ± 5 years in the VL group, p = 0.277. The pre-trial VST angulation studies with a manikin yielded an angle of 85 degrees. Results of an evaluation of this setup in a manikin trial are reported in Supplementary Table 1.
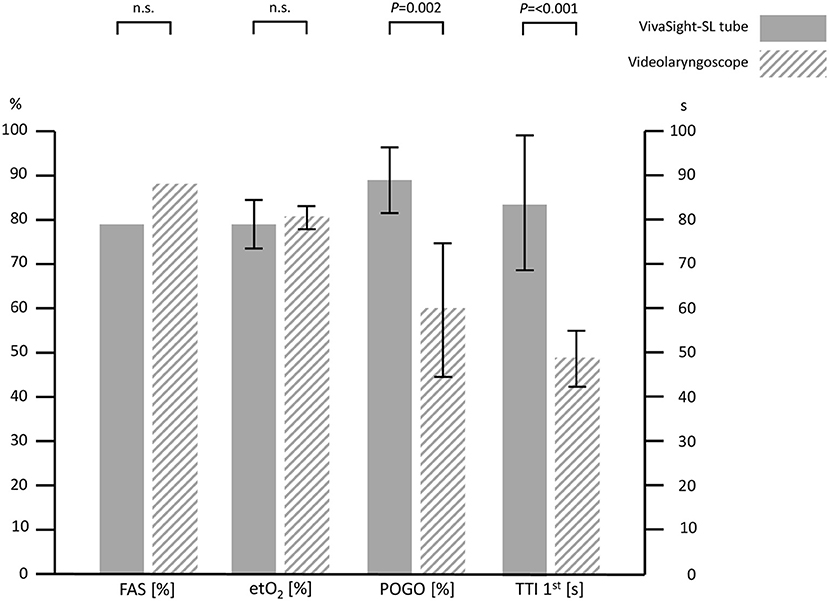
Figure 3. Overview of success rate, oxygenation, visualization, and duration for VivaSight and videolaryngoscopy. FAS, first attempt success rate; etO2, end-tidal oxygen fraction after intubation; POGO, percentage of glottis opening scale; TTI 1st, time to intubation with success in the first attempt. Error bars indicate 95% CIs; n.s., not statistically significant.
In this prospective randomized trial comparing tracheal intubation assisted by a tube-mounted camera (VST) with intubation by VL in patients with a predicted difficult airway, we found no difference concerning oxygenation during airway management or the first attempt success rate. While time to intubation with the VST was prolonged compared with VL, visualization of the larynx by the VST was improved as compared with VL. However, tube advancement was rated more difficult using the VST. No significant differences were found for other parameters, particularly not for complications, such as hypoxia, hypotension, regurgitation, or accidental esophageal intubation.
So far, the VST has been evaluated for tracheal intubation in patients with a predicted non-difficult airway in intensive care (6), in patients with morbid obesity (7), via supraglottic airway devices (15, 16), in manikins (17–21), in a cadaver study (22), and for the guidance of percutaneous dilatational tracheostomy (23, 24).
Awake intubation via bronchoscopy is often regarded as the gold standard technique for the management of the expected difficult airway (3), but this method may be complex, difficult to learn, expensive, time-consuming, and requires thorough patient preparation. Awake videolaryngoscopy has been found to be a safe and effective alternative in carefully selected patients (25). Videolaryngoscopy plays a key role in unexpected difficult airways (4, 26), but the angle of the attached camera is fixed in both Macintosh style and hyperangulated blades. Therefore, visualization of the larynx may result in inadequate viewing conditions. In particular, a restricted epiglottis motion with the epiglottis being adherent to the pharynx [grade 3 view according to Cook (27)] is a pitfall and possible limitation of VL and rather a domain of flexible intubation methods (28). Beyond bronchoscopic and videolaryngoscopic intubation techniques further video-guided techniques using tube or stylet mounted cameras have been introduced but their role for the management of the expected or unexpected difficult intubation remains unclear (29).
In cases of insufficient visualization of the larynx for intubation, a hyperangulated blade or flexible bronchoscopy may be used to obtain visualization of the larynx with a more advantageous viewing angle. With the VST, the axis of the camera may be individually adjusted by angulation of the stylet, presumably explaining the improved laryngeal viewing conditions with a higher POGO score for the VST found in our study. For visualization during VL, it has been shown that insufficient laryngeal views above Cormack/Lehane grade 2 are associated with an increased failure rate of the method (30). Failure rates for VL depend on the type of VL, as well, with first pass success rates ranging from below 40% to above 90% (31). Although visualization was superior for the VST group in our study, we could not show a decrease in failure rate. Interestingly, the most common cause for failure of intubation with VL is the inability to direct the tube toward the laryngeal inlet (32). Presumably, the VST provides a benefit in this respect as the camera provides direct guidance.
The number of intubation attempts did not differ in our study. Previously, more than two attempts have been associated with an increase in complications (33) and strategies have been suggested to increase the rate of first attempt success of intubation, one strategy focusing on the selection of an adequate device for the respective predicted difficult airway (34).
For VL, an overall intubation time of approximately 50–60 s has been reported in human subjects with a difficult airway (31). For the VST, approximately 30 s have been reported previously, but these results were obtained in patients without difficult airways (6). This contrasts with the required duration for intubation in our study with the VST needing nearly three times longer, only counting intubations that were successful on first attempt. We could not find any negative effects as desaturation or a higher rate of hypotension in our patients, but we presume that the prolonged intubation increases complications in patients prone to hypoxia, i.e., in critically ill patients or patients with morbid obesity (35, 36). This may limit the usefulness of the VST to elective cases without risk for hypoxia.
We chose to use a Macintosh-style VL for the control group, angulated at approximately 30 degrees, while hyperangulated blades are angulated at approximately 60 degrees (28, 37). For the VST, we used an angulation of approximately 85 degrees as obtained prior to the beginning of our study that was more pronounced than typical hyperangulated laryngoscope blades. For VL with hyperangulated blades, laryngoscopic view is often improved compared with Macintosh blades, but a common problem arises when attempting to advance the tube through the laryngeal inlet because the tube may hit the anterior tracheal wall at a nearly perpendicular angle, hindering further tube advancement (37), explaining why tube advancement in our study was rated more difficult with the VST as compared with VL.
Recently, a video stylet inserted into a tracheal tube providing camera guidance has been evaluated for intubation in patients with cervical immobilization showing a significantly lower first attempt success rate and prolonged time to intubation as compared with VL (29). As the basic principles of intubation with camera guidance resemble the VST approach, and the results are comparable with our study results, tube-camera guided intubation might indeed be inferior to a laryngoscope approach in the clinical settings, but further data are required.
Our study has the following limitations. Our choice of calculating the sample size for etO2 as the primary endpoint may be questionable as first attempt success rates are widely accepted as endpoints for studies evaluating airway devices. However, sufficient oxygenation is paramount in airway management and an important safety parameter and thus chosen purposely. Our sample size was adequately powered to show non-inferiority for oxygenation but may be underpowered for the first attempt success rate. However, we provide the first data in human subjects for use of the VST in the predicted difficult airways. The learning curve for the VST may not have had reached its peak after the manikin training, but all participating anesthetists were highly experienced in airway management, such as the management of predicted and unexpected difficult airway scenarios.
Tracheal intubation with the VST in patients with an expected difficult airway is feasible, and oxygenation was not inferior as an important safety parameter in the VST group. The first pass success rate in our cohort did not differ between groups. Visualization of the larynx with the VST was superior to VL but time to intubation was prolonged with the VST. We believe further studies are warranted to define which cohorts of patients might benefit from intubation with the VST.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Hamburg Chamber of Physicians (No. PV7276, June 6, 2020). The patients/participants provided their written informed consent to participate in this study.
JG designed the study, wrote the manuscript, performed the statistical analysis, and interpreted the data. EM recruited the patients, acquired the data, helped to write the manuscript, and helped with the statistical analysis. PB and TP helped to recruit the patients and to acquire the data. PT helped with the statistical analysis and to interpret the data. MAP helped to acquire the data and to revise the manuscript. SK helped to interpret the data and to revise the manuscript. MP designed the study, helped to acquire the data, interpreted the data, and revised the manuscript. All authors read and approved the final manuscript.
This study was funded exclusively from the departmental resources including the acquisition of the VivaSight-SL tracheal tubes.
JG has received research support from Adroit Surgical, Ambu, ETView, and Infectopharm, and received consultant and lecture fees from Drägerwerk, Fresenius Medical, GE Healthcare, and Smith Medical; SK received research support from Ambu, Daiichi Sankyo, ETView Ltd., Fisher & Paykel, Pfizer, and Xenios, lecture fees from Astra, C.R.Bard, Baxter, Biotest, Cytosorbents, Daiichi Sankyo, Fresenius, Gilead, Mitsubishi Tanabe Pharma, MSD, Pfizer, Philips, and Zoll, and consultant fees from Bayer, Fresenius, Gilead, MSD, and Pfizer; MP received a research grant awarded by Verathon.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Dr. Hans O. Pinnschmidt for his valuable help with the power analysis.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.767182/full#supplementary-material
1. Grensemann J, Simon M, Kluge S. Airway management in intensive care and emergency medicine: what is new? Med Klin Intensivmed Notfmed. (2019) 114:334–41. doi: 10.1007/s00063-018-0498-7
2. Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. S1 Guideline Airwaymanagement, AWMF-Register No. 001/028 (2015). Available online at: https://www.awmf.org/leitlinien/detail/ll/001-028.html
3. Ahmad I, El-Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, Mir F, et al. Difficult airway society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. (2020) 75:509–28. doi: 10.1111/anae.14904
4. Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult airway society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. (2015) 115:827–48. doi: 10.1093/bja/aev371
5. Barak M, Putilov V, Meretyk S, Halachmi S. ETView tracheoscopic ventilation tube for surveillance after tube position in patients undergoing percutaneous nephrolithotomy. Br J Anaesth. (2010) 104:501–4. doi: 10.1093/bja/aeq024
6. Grensemann J, Eichler L, Wang N, Jarczak D, Simon M, Kluge S. Endotracheal tube-mounted camera-assisted intubation versus conventional intubation in intensive care: a prospective, randomised trial (VivaITN). Crit Care. (2018) 22:235. doi: 10.1186/s13054-018-2152-4
7. Barak M, Assalia A, Mahajna A, Bishara B, Braginski A, Kluger Y. The use of VivaSight single lumen endotracheal tube in morbidly obese patients undergoing laparoscopic sleeve gastrectomy. BMC Anesthesiol. (2014) 14:31. doi: 10.1186/1471-2253-14-31
8. Norskov AK, Wetterslev J, Rosenstock CV, Afshari A, Astrup G, Jakobsen JC, et al. Effects of using the simplified airway risk index vs usual airway assessment on unanticipated difficult tracheal intubation - a cluster randomized trial with 64,273 participants. Br J Anaesth. (2016) 116:680–9. doi: 10.1093/bja/aew057
9. el-Ganzouri AR, McCarthy RJ, Tuman KJ, Tanck EN, Ivankovich AD. Preoperative airway assessment: predictive value of a multivariate risk index. Anesth Analg. (1996) 82:1197–204. doi: 10.1213/00000539-199606000-00017
10. Detsky ME, Jivraj N, Adhikari NK, Friedrich JO, Pinto R, Simel DL, et al. Will this patient be difficult to intubate?: The rational clinical examination systematic reviewwill this patient be difficult to intubate? Will this patient be difficult to intubate? JAMA. (2019) 321:493–503. doi: 10.1001/jama.2018.21413
11. Khan ZH, Kashfi A, Ebrahimkhani E. A comparison of the upper lip bite test (a simple new technique) with modified mallampati classification in predicting difficulty in endotracheal intubation: a prospective blinded study. Anesth Analg. (2003) 96:595–9. doi: 10.1213/00000539-200302000-00053
12. Vourc'h M, Baud G, Feuillet F, Blanchard C, Mirallie E, Guitton C, et al. High-flow nasal cannulae versus non-invasive ventilation for preoxygenation of obese patients: the PREOPTIPOP randomized trial. EClinicalMedicine. (2019) 13:112–9. doi: 10.1016/j.eclinm.2019.05.014
13. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. (1984) 39:1105–11. doi: 10.1111/j.1365-2044.1984.tb08932.x
14. Levitan RM, Ochroch EA, Kush S, Shofer FS, Hollander JE. Assessment of airway visualization: validation of the percentage of glottic opening (POGO) scale. Acad Emerg Med. (1998) 5:919–23. doi: 10.1111/j.1553-2712.1998.tb02823.x
15. Gaitini LA, Yanovski B, Mustafa S, Hagberg CA, Mora PC, Vaida SJ. A feasibility study using the VivaSight single lumen to intubate the trachea through the fastrach laryngeal mask airway: a preliminary report of 50 cases. Anesth Analg. (2013) 116:604–8. doi: 10.1213/ANE.0b013e31827b278f
16. Huitink JM, Koopman EM, Bouwman RA, Craenen A, Verwoert M, Krage R, et al. Tracheal intubation with a camera embedded in the tube tip (Vivasight). Anaesthesia. (2013) 68:74–8. doi: 10.1111/anae.12065
17. Gawlowski P, Smereka J, Madziala M, Cohen B, Ruetzler K, Szarpak L. Comparison of the ETView single lumen and macintosh laryngoscopes for endotracheal intubation in an airway manikin with immobilized cervical spine by novice paramedics: a randomized crossover manikin trial. Medicine. (2017) 96:e5873. doi: 10.1097/MD.0000000000005873
18. Kurowski A, Szarpak L, Truszewski Z, Czyzewski L. Can the ETView VivaSight SL rival conventional intubation using the macintosh laryngoscope during adult resuscitation by novice physicians?: A randomized crossover manikin study. Medicine. (2015) 94:e850. doi: 10.1097/MD.0000000000000850
19. Truszewski Z, Szarpak L, Czyzewski L, Evrin T, Kurowski A, Majer J, et al. A comparison of the ETView VivaSight SL against a fiberoptic bronchoscope for nasotracheal intubation of multitrauma patients during resuscitation. A randomized, crossover, manikin study. Am J Emerg Med. (2015) 33:1097–9. doi: 10.1016/j.ajem.2015.04.078
20. Truszewski Z, Szarpak L, Smereka J, Kurowski A, Evrin T, Czyzewski L. Comparison of the VivaSight single lumen endotracheal tube and the macintosh laryngoscope for emergency intubation by experienced paramedics in a standardized airway manikin with restricted access: a randomized, crossover trial. Am J Emerg Med. (2016) 34:929–30. doi: 10.1016/j.ajem.2016.02.054
21. Karczewska K, Szarpak L, Smereka J, Dabrowski M, Ladny JR, Wieczorek W, et al. ET-View compared to direct laryngoscopy in patients with immobilized cervical spine by unexperienced physicians: a randomized crossover manikin trial. Anaesthesiol Intensive Ther. (2017) 49:274–82. doi: 10.5603/AIT.a2017.0047
22. Truszewski Z, Krajewski P, Fudalej M, Smereka J, Frass M, Robak O, et al. A comparison of a traditional endotracheal tube versus ETView SL in endotracheal intubation during different emergency conditions: a randomized, crossover cadaver trial. Medicine. (2016) 95:e5170. doi: 10.1097/MD.0000000000005170
23. Grensemann J, Eichler L, Hopf S, Jarczak D, Simon M, Kluge S. Feasibility of an endotracheal tube-mounted camera for percutaneous dilatational tracheostomy. Acta Anaesthesiol Scand. (2017) 61:660–7. doi: 10.1111/aas.12904
24. Grensemann J, Eichler L, Kahler S, Jarczak D, Simon M, Pinnschmidt HO, et al. Bronchoscopy versus an endotracheal tube mounted camera for the peri-interventional visualization of percutaneous dilatational tracheostomy - a prospective, randomized trial (VivaPDT). Crit Care. (2017) 21:330. doi: 10.1186/s13054-017-1901-0
25. Alhomary M, Ramadan E, Curran E, Walsh SR. Videolaryngoscopy vs. fibreoptic bronchoscopy for awake tracheal intubation: a systematic review and meta-analysis. Anaesthesia. (2018) 73:1151–61. doi: 10.1111/anae.14299
26. Heidegger T. Management of the difficult airway. N Engl J Med. (2021) 384:1836–47. doi: 10.1056/NEJMra1916801
27. Cook TM. A new practical classification of laryngeal view. Anaesthesia. (2000) 55:274–9. doi: 10.1046/j.1365-2044.2000.01270.x
28. Pearce AC, Duggan LV, El-Boghdadly K. Making the grade: has cormack and lehane grading stood the test of time? Anaesthesia. (2021) 76:705–9. doi: 10.1111/anae.15446
29. Yoon HK, Lee HC, Park JB, Oh H, Park HP. McGrath MAC videolaryngoscope versus optiscope video stylet for tracheal intubation in patients with manual inline cervical stabilization: a randomized trial. Anesth Analg. (2020) 130:870–8. doi: 10.1213/ANE.0000000000004442
30. Aziz MF, Healy D, Kheterpal S, Fu RF, Dillman D, Brambrink AM. Routine clinical practice effectiveness of the glidescope in difficult airway management: an analysis of 2,004 glidescope intubations, complications, and failures from two institutions. Anesthesiology. (2011) 114:34–41. doi: 10.1097/ALN.0b013e3182023eb7
31. Kleine-Brueggeney M, Greif R, Schoettker P, Savoldelli GL, Nabecker S, Theiler LG. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. BJA. (2016) 116:670–9. doi: 10.1093/bja/aew058
32. Sakles JC, Mosier JM, Chiu S, Keim SM. Tracheal intubation in the emergency department: a comparison of GlideScope® video laryngoscopy to direct laryngoscopy in 822 intubations. J Emerg Med. (2012) 42:400–5. doi: 10.1016/j.jemermed.2011.05.019
33. Buis ML, Maissan IM, Hoeks SE, Klimek M, Stolker RJ. Defining the learning curve for endotracheal intubation using direct laryngoscopy: a systematic review. Resuscitation. (2016) 99:63–71. doi: 10.1016/j.resuscitation.2015.11.005
34. Natt BS, Malo J, Hypes CD, Sakles JC, Mosier JM. Strategies to improve first attempt success at intubation in critically ill patients. Br J Anaesth. (2016) 117:i60–8. doi: 10.1093/bja/aew061
35. Nolan JP, Kelly FE. Airway challenges in critical care. Anaesthesia. (2011) 66 (Suppl. 2):81–92. doi: 10.1111/j.1365-2044.2011.06937.x
36. Baraka AS, Taha SK, Siddik-Sayyid SM, Kanazi GE, El-Khatib MF, Dagher CM, et al. Supplementation of pre-oxygenation in morbidly obese patients using nasopharyngeal oxygen insufflation. Anaesthesia. (2007) 62:769–73. doi: 10.1111/j.1365-2044.2007.05104.x
Keywords: airway management (MeSH), intubation (intratracheal), respiration (artificial), laryngoscopy, laryngoscope and intubation, VivaSight
Citation: Grensemann J, Möhlenkamp E, Breitfeld P, Tariparast PA, Peters T, Punke MA, Kluge S and Petzoldt M (2021) Tracheal Tube-Mounted Camera Assisted Intubation vs. Videolaryngoscopy in Expected Difficult Airway: A Prospective, Randomized Trial (VivaOP Trial). Front. Med. 8:767182. doi: 10.3389/fmed.2021.767182
Received: 30 August 2021; Accepted: 16 November 2021;
Published: 15 December 2021.
Edited by:
Mert Şentürk, Istanbul University, TurkeyReviewed by:
Jo Mourisse, Radboud University Nijmegen, NetherlandsCopyright © 2021 Grensemann, Möhlenkamp, Breitfeld, Tariparast, Peters, Punke, Kluge and Petzoldt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jörn Grensemann, ai5ncmVuc2VtYW5uQHVrZS5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.