
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med., 02 November 2021
Sec. Dermatology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.735585
This article is part of the Research TopicRecent Advances in Keratinocyte Carcinomas: from Molecular Mechanisms to Clinical PerspectivesView all 8 articles
 Dana E. Rollison1*†
Dana E. Rollison1*† Jane L. Messina2†
Jane L. Messina2† Basil S. Cherpelis3†Neil A. Fenske3†Michael J. Schell4†
Basil S. Cherpelis3†Neil A. Fenske3†Michael J. Schell4† Dennis O. Adeegbe5†
Dennis O. Adeegbe5† Yayi Zhao1†
Yayi Zhao1† Rossybelle P. Amorrortu1†Afua A. Akuffo5†
Rossybelle P. Amorrortu1†Afua A. Akuffo5† Rebecca S. Hesterberg5†Pearlie K. Epling-Burnette5†
Rebecca S. Hesterberg5†Pearlie K. Epling-Burnette5†Ultraviolet radiation exposure (UVR) is a risk factor for cutaneous squamous cell carcinoma (cuSCC) and has been shown to be positively associated with circulating immunosuppressive regulatory T cells (“Tregs”). However, the risk of cuSCC in association with circulating Tregs has not been studied. The aim of this study was to determine whether circulating Treg levels are associated with cuSCC development, particularly in the context of high UVR. Blood and spectrophotometer-based UVR measurements were obtained on 327 immunocompetent individuals undergoing routine skin cancer screenings at baseline and followed for up to 4 years for incident cuSCC development within a prospective cohort study. Proportions of phenotypically distinct Tregs, especially CCR4hi and CLA+ cells which are associated with activation and homing, respectively, were measured by flow cytometry. Tregs in cuSCC tumors were assessed using immunohistochemistry and graded for solar elastosis, a measure of cumulative UVR damage. Of several Treg phenotypes examined, higher levels of circulating CCR4hi Tregs at baseline were significantly associated with increased risk of subsequent cuSCC; those with higher levels of both CCR4hi and UVR were four times more likely to develop cuSCC compared to those with lower levels of both (Hazard Ratio = 4.11, 95% CI = 1.22–13.90). Within cuSCC tumors, CCR4hi Tregs were positively associated with solar elastosis. Results show that a higher proportion of CCR4hi peripheral Tregs predicts incident cuSCC up to 4 years, especially among highly UV-exposed individuals. Research of the underpinning biology of Tregs in UVR-associated skin damage may possibly reveal novel opportunities for screening, prevention, and treatment.
Keratinocyte carcinomas (KC) including cutaneous squamous cell carcinoma (cuSCC) and basal cell carcinoma (BCC) are the most commonly diagnosed cancers in the U.S. (1–3), with more than five million KC cases diagnosed each year (4). CuSCC typically comprised 20% of KC (1, 5) however trends are increasing with a recent study reporting a 1:1 ratio of cuSCC to BCC in adults ages 65+ (4). CuSCC is more often aggressive than BCC, with 4,000 people dying from invasive cuSCC in the U.S. each year (6). Ultraviolet (UV) radiation exposure (UVR) is the major environmental risk factor for KC, and chronic lifetime UVR has been associated specifically with cuSCC risk (2, 7–9). While chronic lifetime UVR results in the accumulation of UVR-induced DNA damage (9), leading to skin carcinogenesis (10, 11), UVR may also contribute to cuSCC development through an immunosuppressive pathway. Immunosuppression is a well-established risk factor for cuSCC, with heart, kidney, blood, and marrow transplant patients experiencing 16- to 68- fold risks of cuSCC compared to the general population (12, 13). Furthermore, long term use of oral corticosteroids has been associated with increased cuSCC risk among immunocompetent individuals (14). While mouse studies have shown that UVR is immunosuppressive (15, 16), no epidemiologic studies have sought to measure the interplay between UVR and immune function in relation to cancer etiology in humans.
UVR can lead to systemic immune suppression as well as antigen-specific immune tolerance due to the induction of regulatory T cells (“Tregs”) which are known to have immunosuppressive effects (16, 17). Specifically, in mice, thymically-derived Tregs increase following exposure to low doses of UVR in the absence of tumors (18). In humans, clinical studies in patients with multiple sclerosis and psoriasis have shown that circulating Tregs are induced after treatment with UV phototherapy (15, 19, 20). The expansion of Tregs in circulation is mediated by antigen activation which enables their suppressive mechanisms and can trigger homing into the skin (16, 18). Studies have identified subpopulations of Tregs that display specific markers associated with skin homing, including the carbohydrate epitope cutaneous lymphocyte-associated antigen (CLA) that binds E-selectin and initiates tethering and rolling along cutaneous venules (18, 21, 22). Compared to Tregs in circulation, tumor-infiltrating Tregs contain an activated population responsive to cognate self-antigen capable of eliciting immune suppression (23). Unlike naïve Tregs that express the molecules CD45RA and CD27 (Naïve), activated Tregs downregulate both of these surface molecules (24, 25) and induce the expression of C-C chemokine receptor 4 (CCR4) (26) that also contributes to skin trafficking along with expression of CLA (27, 28).
We previously observed that recent UVR was positively correlated with CD45RA−/CD27− activated Tregs, CLA+ and CCR4hi Tregs in a cross-sectional analysis of baseline samples from a subset of skin cancer screening patients participating in a prospective cohort study of skin cancer in Tampa, FL, the Viruses in Skin Cancer (VIRUSCAN) Study (29). To determine whether UVR and circulating Tregs at baseline were associated with subsequent diagnosis of cuSCC, we conducted a prospective analysis among the same VIRUSCAN participants.
The VIRUSCAN Study population and methods have been described in detail previously (30). Briefly, individuals age 60+ undergoing routine skin cancer screening exams at the University of South Florida (USF) Dermatology Clinic were enrolled between July 2014 and August 2017 and followed for subsequent KC diagnosis through September 2018. Four hundred twenty-one participants were enrolled in the first year and confirmed not to have a prevalent KC at enrollment. Of these, 327 returned for at least one follow-up visit, had available circulating Treg flow cytometry results and were included in the current analysis. Four participants were missing baseline spectrophotometer readings and were excluded from the analyses related to UVR. One participant was missing self-reported sun sensitivity and was excluded from the full Cox regression model of cuSCC. This study was approved by the USF Institutional Review Board and all patients provided written informed consent.
Study participants completed an electronic questionnaire at baseline including information on demographics, skin cancer risk factors, and medical history (30). A Konica Minolta CM-600D spectrophotometer with SpectraMagic NX Lite USB Ver.25 software was used to obtain quantitative and objective measurements of recent UVR exposure at baseline. Specifically, spectrophotometer readings of skin pigmentation were obtained from the sun-unexposed inner upper arm (i.e., the axilla) and sun-exposed forearm. The degree of recent tanning in response to recent UVR exposure was measured by calculating the difference between the pigment readings on the forearm and the axilla using the Commission Internationale de I'Éclair age (CIE) L*a*b* system and CIE76 formula: ΔE*ab = [(ΔL*)2 + (Δa*)2 + (Δb*)2]1/2 (31). This measurement has been validated as a quantitative marker of UVR exposure experienced in the past week (30). Additionally, the brightness measure L* obtained from the unexposed axilla was previously reported to be associated with the melanin index (32), and was found to be associated with self-reported untanned skin color among VIRUSCAN Study participants (30).
Blood samples were obtained at baseline and Peripheral Blood Mononuclear Cells (PBMCs) were isolated and frozen for future use. PBMCs were thawed, and proportions of circulating Tregs were determined by flow cytometry analysis, as described previously (29). Flow cytometry assays were performed using PBMCs with data acquired on an LSR II flow cytometer (BD Biosciences) and analyzed using FlowJo v9 (FlowJo, RRID:SCR_008520, BD Bioscience) to examine the proportions of CD8+ and CD4+ T cells, total Tregs and Treg subpopulations as defined in Supplementary Figure 1, and as previously described (29).
Study follow-up visits were integrated into routine clinical care with total body skin exams for skin cancer screening occurring every 6–12 months. During these exams, the entire integument was examined for suspicious lesions, including the scalp, underarms, groin, and buttocks. When indurated cutaneous lesions suspected to be malignant were identified, they were biopsied, formalin-fixed, and sent for pathology review per standard clinical protocol. Study coordinators reviewed pathology reports to identify incident cases of KC diagnosed among cohort participants. Clinical characteristics of the KC tumors were recorded, including date and stage of diagnosis, anatomic location of the tumor, and treatment received. Participants were considered cuSCC cases if they were not diagnosed with KC at baseline and developed at least 1 incident cuSCC, basosquamous, or SCC/BCC merged tumor during the follow-up period. Participants who were not diagnosed with the above described lesions were considered to be non-cases. Person-time for incident cuSCC cases was calculated as the number of days between study enrollment and time when the first incident cuSCC was biopsied, while the person-time for non-case participants was calculated as the number of days between enrollment and the last total body skin exam.
Formalin fixed paraffin embedded (FFPE) tumor tissue recuts were obtained from the USF Pathology department for 8 cuSCC tumors identified from 7 participants during the first year of follow-up. To augment the sample size for the tumor analysis, recuts of 16 cuSCC tumors diagnosed at the time of study enrollment were also included. These recuts were from 12 participants who were excluded from the main prospective analysis. The study dermatopathologist confirmed all cuSCC diagnoses and graded the degree of solar elastosis present in the adjacent normal tissue, a measure of cumulative UVR (30). Solar elastosis was graded on a 4-point scale: 0: no presence of elastotic fibers or very occasional elastotic fibers; 1: scattered elastotic fibers lying as individual units between collagen bundles; 2: densely scattered elastotic fibers distributed predominantly as bushels rather than individual units; 3: dense aggregates of elastotic fibers forming amorphous deposits of blue-gray material with lost fiber texture (33–35).
The cuSCC FFPE tumor recuts were mounted on glass slides and underwent immunohistochemistry (IHC) for CD3/FoxP3 and CCR4/FoxP3 using a two-color procedure. All slides were stained using a Ventana Discovery XT automated system (Ventana Medical Systems, Tucson, AZ) with proprietary reagents. Slides were deparaffinized on the automated system with EZ Prep solution. Heat-induced antigen retrieval using Cell Conditioning 1 was used for all stains. For the FoxP3/CCR4 two-color stain, the mouse primary antibody to Foxp3 (Abcam Cat# ab20034, RRID:AB_445284, clone 236A/E7, 1:400) and the rabbit primary antibody to CCR4 (LS Bioscience, Seattle, WA, 1:800, discontinued since staining was performed) were incubated for 28 min. The anti-mouse secondary antibody was incubated for 4 min and visualized with the Ventana anti-rabbit diaminobenzidine (DAB) multimeter; the anti-rabbit secondary antibody was incubated for 16 min and visualized with alkaline phosphatase. For the CD3/FoxP3 double stain, the mouse primary antibody to CD3 (prediluted, Ventana) and the rabbit primary antibody to FoxP3 (Abcam Cat# ab20034, RRID:AB_445284, 1:25) were incubated for 60 min. The anti-mouse secondary antibody was incubated for 4 min and visualized with DAB and the anti-rabbit secondary antibody was incubated for 4 min and visualized with alkaline phosphatase. For all stains, the detection system used was the Ventana OmniMap kit and slides were counterstained with hematoxylin, dehydrated, and coverslipped.
The IHC stained slides were imaged using an Aperio AT2 whole slide scanner (Leica Biosystems Inc., Vista, California) with a 20X 0.7NA objective lens. The whole slide images were viewed using the Aperio Imagescope software (RRID:SCR_014311) and identical sized rectangular regions of interest (ROIs) were annotated under the guidance of the study pathologist, focusing on areas of greatest inflammation. These ROIs were extracted into TIFF format images and imported into Definiens Tissue Studio image analysis software (Definiens AG, Munich, Germany) where cell and nucleus detection algorithms were used to enumerate the number of positive cell and negative cells for each marker. Identical intensity thresholds for cell positivity were used for all images stained with the same marker and confirmed by study pathologist.
Participants' demographic and other baseline characteristics were described separately for patients who developed incident cuSCC and those who did not. Log-rank p-values were calculated to compare the time-to-incidence between categories of each variable. To understand the effect of UVR on the development of incident cuSCC, the cumulative incidence of cuSCC was plotted, stratified by tertiles of UVR as determined using spectrophotometer data obtained from all participants who returned to the clinic at least once. Age- and sex-adjusted Cox proportional hazard ratios (HR) and 95% confidence intervals (95% CI) were calculated to estimate the associations between UVR levels in the middle and highest tertiles vs. the lowest tertile and the risk of incident cuSCC. Based on similarity of the incidence curves and the estimated HR's, the categories of the middle and high tertiles of UVR were combined and compared to the lowest tertile.
Given limited pre-existing knowledge regarding the clinical utility of Treg cut points, the levels of each Treg subpopulation were categorized into three categories using the reduced monotonic regression method (36) to differentiate between the cuSCC risk groups. This method maximizes the difference in predicted risk, while maintaining the sample size of each category at ≥10%. Resulting cut points for categorizing higher, medium and lower Tregs within each subpopulation defined were as follows: 81.7 and 88.9 for CCR4hi Tregs, 59.4 and 66.2 for CLA+ Tregs, and 8.05 and 13.7 for CD45RA−/CD27− Tregs. Cumulative incidence of cuSCC was plotted for each Treg category (Supplementary Figure 2), and corresponding age- and sex-adjusted Cox regression HR's and 95% CI's were calculated to estimate the association between Treg levels in the middle and highest categories vs. the lowest category and the risk of incident cuSCC. For each Treg subpopulation, the categories of the middle and high groups of Treg levels were combined and compared to the lowest level, based on similarity of the incidence curves and the estimated HR's. Subsequently, the cumulative incidence curve for cuSCC was plotted by higher vs. lower circulating Tregs, separately for CCR4hi Treg, CLA+ Treg, and CD45RA−/CD27− Tregs. To account for potential confounding effects, a stepwise elimination process was implemented including the following variables: age, sex, recent UVR, job working under the sun, sun sensitivity, self-reported skin color, spectrophotometer-measured skin color, hair color, number of moles on body, and history of KC, along with the measurements of circulating Tregs. The variables retained (age, sex, and sun sensitivity) were included in the full Cox regression model. Cox regression HR and 95% CI were calculated to estimate the association between higher vs. lower circulating Tregs and the risk of incident cuSCC using both the age- and sex-adjusted model and the full model, separately for each Treg subpopulation.
Treg subpopulations that were significantly associated with incident cuSCC advanced to the next stage, where a joint effects analysis was conducted between UVR and each of the Treg phenotypes. Categorical variables representing different combinations of UVR levels and circulating Treg levels were created by grouping participants into those with lower CCR4hi Treg and lower UVR exposure level (reference group), higher CCR4hi Treg and lower UVR, lower CCR4hi Treg and higher UVR, and higher CCR4hi Treg and higher UVR. Cox models were then used to estimate the association between having both higher UVR and higher circulating Treg and the development of cuSCC. To assess whether the proportional hazard assumption was upheld for each model, the time-dependent coefficient was plotted across time of follow-up, followed by a formal score test to determine if the slope of the time-dependent coefficient deviated significantly from 0. In the single case of assumption violation (CLA+ Tregs in association with cuSCC), the data were restricted to the first 3 years during which the test for the proportional hazards assumption (37) was upheld. Model fitness was compared using analysis of deviance.
To examine the association between presence of Tregs in 24 cuSCC tumor tissues and solar elastosis in the adjacent normal tissue, the mean and standard deviation for each IHC-measured tumor T cell subpopulation was reported for each level of solar elastosis. The association between each tumor T cell subpopulation and increasing levels of solar elastosis was calculated using the Jonckheere-Terpstra trend test.
All analyses were conducted using R Statistical package, version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
Baseline characteristics of the participants enrolled in the VIRUSCAN cohort are described in Table 1, separately for those who subsequently developed cuSCC and those who did not. There were no significant differences between the two groups for most of the factors assessed, including age, sex, natural hair color, number of moles on the body, natural skin tone, ever having had a job working in the sun or history of a KC. The spectrophotometer-based measurements of sun-unexposed underarm skin also did not significantly differ between the two groups. However, self-reported lighter skin tone and a severe sunburn in reaction to 1 h of sun exposure were both significantly more common among those who subsequently developed cuSCC than those that did not (Table 1).
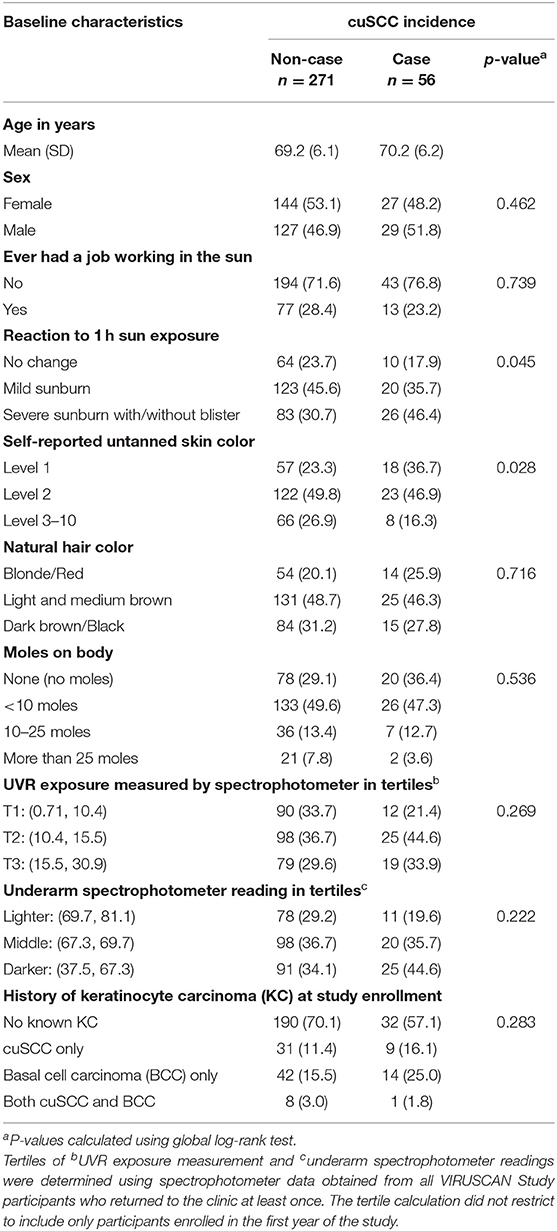
Table 1. Baseline characteristics of 327 skin cancer screening patients enrolled in year 1 of the VIRUSCAN Study compared between those that subsequently developed cutaneous squamous cell carcinoma (cuSCC) and those that did not.
Among the 327 cohort participants, median follow-up time was 1,083 days, and the total follow-up time observed was 816 person-years. A total of 56 participants were diagnosed with at least one incident cuSCC during follow-up, corresponding to a cuSCC incidence rate of 6.86 per 100 person-years. Supplementary Figure 3 depicts the cumulative incidence rates for cuSCC by categories of recent UVR. The cumulative incidence of cuSCC was similar for participants whose recent UVR was in the middle and highest tertiles (Supplementary Figure 3A). When these two groups were combined and compared to those in the lowest tertile of recent UVR, a 74% increased risk of cuSCC associated with higher vs. lower recent UVR was observed, although not statistically significant (HR = 1.74, 95% CI = 0.87–3.49) (Supplementary Figure 3B).
Incidence of cuSCC was plotted for higher vs. lower circulating levels of CCR4hi, CLA+, and CD45RA−/CD27− Tregs in Figure 1. Participants with higher circulating levels of these phenotypic subsets of Tregs assessed at baseline experienced higher incidence of cuSCC compared to those with lower levels, with the greatest separation of incidence curves observed for CCR4hi Tregs (Figure 1A). The differences in cuSCC incidence between higher and lower levels of CLA+ Tregs was most pronounced within the first 3 years of follow-up, with the cumulative incidence curves converging after year three. The proportional hazards assumption was violated for CLA+ Tregs thus, the HR for CLA+ Tregs was calculated for the first 3 years of follow up only.
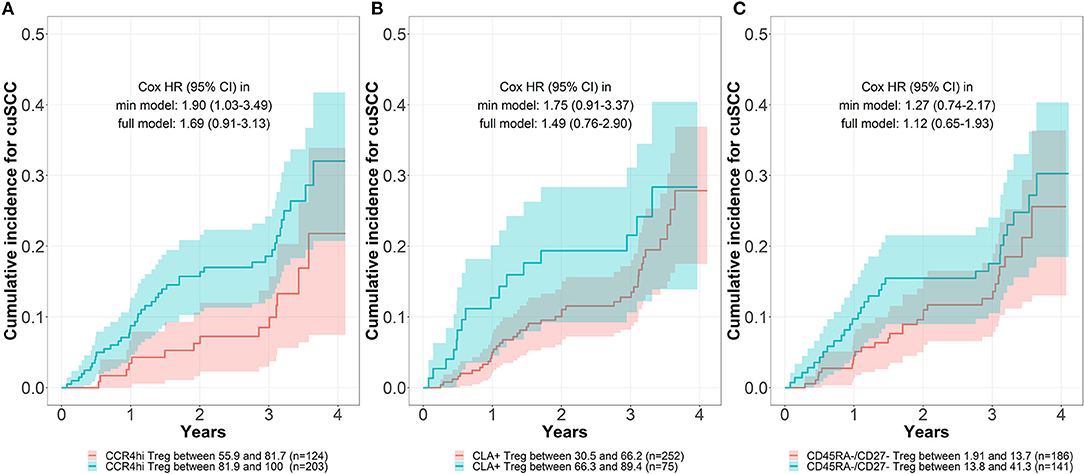
Figure 1. Cumulative incidence for cutaneous squamous cell carcinoma (cuSCC) by baseline levels of circulating Tregs. The cumulative incidence for cuSCC stratified by levels of baseline circulating Treg, separately for CCR4hi Treg (A), CLA+ Treg (B), and CD45RA−/CD27− Treg cells (C), as determined by the reduced monotonic regression in combination with visual inspection of the cumulative incidence curves. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated using Cox proportional hazard models. The minimum (min) model was adjusted for age and sex, and the full model was further adjusted for self-reported skin reaction to 1 h of sun exposure.
After adjusting for age and sex, cohort participants with higher levels of CCR4hi Tregs in circulation at baseline experienced a statistically significant 90% increased risk of subsequent cuSCC compared to those with lower levels of CCR4hi Tregs in circulation at baseline (Figure 1A: HR = 1.90, 95% CI = 1.03–3.49). After further adjustment for self-reported skin's reaction to 1 h of sun exposure, the hazard ratio remained elevated but was no longer statistically significant (HR = 1.69, 95% CI = 0.91–3.13). Cohort participants with higher levels of circulating CLA+ Tregs at baseline also experienced an increased risk of subsequent cuSCC, although this risk was not statistically significant with adjustment for age and sex (HR = 1.75, 95% CI = 0.91–3.37) or after further adjustment for skin's reaction to sun exposure. There was no increased risk of cuSCC associated with higher levels of circulating CD45RA−/CD27− Tregs at baseline. Addition of CLA+ Treg to the existing CCR4hi Treg model did not significantly improve the model fitness (p = 0.77).
Figure 2 depicts the cuSCC incidence among four groups of cohort participants defined by combinations of higher vs. lower UVR and higher vs. lower enrichment of CCR4hi Tregs at baseline. The highest incidence of cuSCC was observed in those with higher recent UVR and higher levels of CCR4hi Tregs, with the risk of cuSCC being four times that of those with lower UVR and lower levels of CCR4hi Tregs (HR = 4.11, 95% CI = 1.22–13.90), an association that remained statistically significant after further adjustment for self-reported skin reaction to the sun (HR = 3.56, 95% CI = 1.06–12.18). Supplementary Figure 4 shows illustrative examples of the solar elastosis grading and corresponding IHC staining performed on the cuSCC tumors. Among the 24 cuSCC tumors investigated by IHC staining, higher levels of solar elastosis (i.e., cumulative sun damage) measured in the adjacent normal tissue were significantly associated with higher proportions of CCR4-expressing T cells, as well as CCR4 and FoxP3 co-expressing Tregs in the tumor (Table 2).
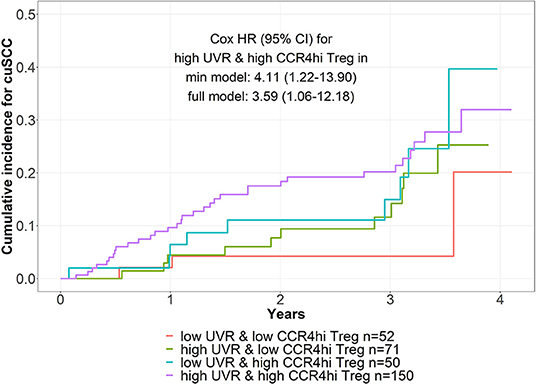
Figure 2. Joint effects of CCR4hi Treg and spectrophotometer measured UV exposure (UVR) on risk of incident cutaneous squamous cell carcinoma (cuSCC). Cumulative incidence of cuSCC incidence among four groups of cohort participants defined by combinations of higher vs. lower UVR and higher vs. lower CCR4hi Tregs at baseline. The minimum (min) model was adjusted for age and sex, and the full model was further adjusted for self-reported skin reaction to 1 h of sun exposure.
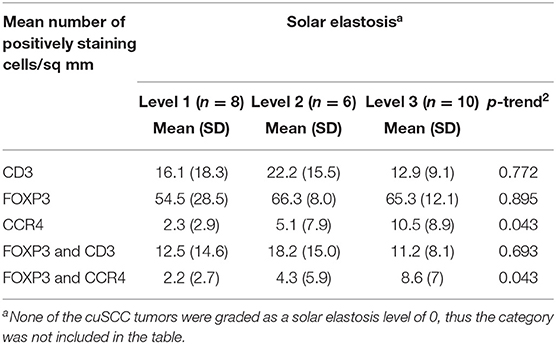
Table 2. Associations between T cell subpopulations identified in incident cutaneous squamous cell carcinoma (cuSCC) and levels of solar elastosis in the normal tissue adjacent to tumor.
In summary, while controlling for factors including age, gender, and skin sensitivity to sun exposure, participants with higher levels of circulating CCR4hi Tregs at baseline had a higher risk of developing cuSCC up to 4 years later. The risk of developing cuSCC was especially elevated among participants who had both higher levels of circulating CCR4hi Tregs and higher levels of recent UVR exposure. In addition, CCR4hi Tregs were more likely to be present in cuSCC tumors arising in areas of the skin that showed evidence of cumulative sun damage.
Our previous cross-sectional analysis demonstrated that higher levels of UVR, a well-documented risk factor for KC, were significantly associated with higher proportions of defined circulating Treg subpopulations, but not with total Tregs (29). In the current study with prospective monitoring for up to 4 years, individuals with higher circulating CCR4hi Tregs and higher levels of UVR measured by a spectrophotometer were approximately four times more likely to develop cuSCC compared to those with lower CCR4hi Tregs and lower UVR. Furthermore, the presence of Tregs expressing CCR4 in cuSCC tumors was associated with the presence of solar elastosis (cumulative sun damage) in the adjacent normal tissue was verified in a subset of patients. UVR may contribute to carcinogenesis by promoting skin infiltration associated with tissue remodeling that is induced through UVR-induced skin damage. We have shown previously that subpopulations of Tregs differ by age, sex, and race with lighter skinned individuals demonstrating higher levels of circulating activated Tregs at baseline associated with higher UVR (29). Adjustment for these factors demonstrated the independent contribution of circulating activated CCR4hi Tregs as a predictor of cuSCC. Of note, there was no evidence that natural skin tone modified the association of activated Tregs and cuSCC (HRlighter = 1.86, 95% CI = 0.74–4.69 vs. HRdarker = 1.83, 95% CI = 0.81–4.21, Pinteraction = 0.92).
In immunocompetent hosts, developing neoplasms are shaped by factors present in the local microenvironment. While this process has been shown using elegant mouse models, factors leading to the permissive growth of naturally arising human tumors is poorly understood. At the time of detection, Tregs are frequently expanded in cancer patients including breast (38), pancreatic (39, 40), colon (41), non-small cell lung (42, 43) as well as hematological cancers (44–47). The majority of peripheral Tregs in healthy individuals typically display a CD3+CD4+FOXP3+CD25+CD127dimCD27+CD45RA+ phenotype with changes noted in the phenotype during activation (29, 45, 48). High levels of chemokine receptor CCR4 on Tregs in peripheral blood have been associated with the presence of active rheumatoid arthritis, with levels of CCR4 on Tregs positively correlating to disease severity (49). In patients with ovarian carcinoma, the host response to the tumor has been shown to be inhibited by Foxp3+CCR4+ Tregs recruited to the tumor by chemokines including CCL22 (50) and the CCR4-CCL22 axis appears to be operational in tolerized cardiac allografts (51). In our study, the previously observed co-expression of CCR4 and CLA (29) raises the possibility that this subset of Tregs migrate into the skin where they accumulate over years and dampen immune surveillance and contribute to tumor escape, hence subsequent cuSCC development. Based on infection models, the majority of CCR4+ lymphocytes are in an activated state and appear to exert suppressive functions by secreting a number of immunosuppressive cytokines (52).
Participants enrolled in the first year of the VIRUSCAN Study and included in this analysis were followed for up to 4 years. The incidence plots suggest that the magnitude of the association between baseline activated CCR4hi Tregs in circulation and subsequent cuSCC may increase over time. However, it is unclear whether CCR4hi Tregs are driving the effect on cuSCC independently, or in combination with CLA+ Treg. As previously described, CCR4hi Tregs and CLA+ Tregs are strongly correlated (29) and few study participants had lower CCR4hi Treg levels but higher CLA+ Treg levels. Thus, teasing apart the effect of CLA+ Treg from CCR4hi Treg will require a larger sample size. Future expansion of the present analysis to all VIRUSCAN Study participants with extended follow-up time will allow us to further investigate the independent and joint effects of CCR4hi Treg and CLA+ Treg on the development of cuSCC while examining potential differences in risk with increasing follow-up time. Furthermore, future studies are needed to validate the clinical utility of the Treg cut points defined here.
The present study is the first to investigate activated CCR4hi Tregs in circulation as a predictor of cuSCC in the context of recent UVR. Our ability to identify proportional increases in CCR4hi and Foxp3 expressing T cells in KC tissue in patients with evidence of increasing chronic UVR suggests they may play a direct role in exerting local immunosuppression in susceptible individuals. While cumulative UVR is a known risk factor for cuSCC and may be considered when determining the appropriateness and frequency of total body skin exams for skin cancer screening, a majority of individuals in the present study (82.9%) did not develop cuSCC during the follow-up period. Therefore, novel biomarkers of risk, such as distinct subsets of activated Tregs in circulation such as the described CCR4hi Tregs could be critically important for more accurate risk stratification of patients for cuSCC prevention and screening. Furthermore, a better understanding of the biological underpinnings of the observed associations between activated Tregs in circulation and cuSCC may lead to the development of novel prevention and/or treatment strategies. In this regard, anti-CCR4 antibodies have been evaluated as a potential strategy to remove CCR4-expressing Tregs from the tumor microenvironment to enhance effector T cell function. Such strategy could be explored for depletion of circulating CCR4hi Treg populations in patients deemed high risk for cuSCC development (26).
The datasets presented in this article are not readily available in order to protect participant confidentiality and privacy. Requests to access the datasets should be directed to ZGFuYS5yb2xsaXNvbkBtb2ZmaXR0Lm9yZw==.
The studies involving human participants were reviewed and approved by University of South Florida Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
DER, PE-B, DA, MS, and JM contributed to the conception and design of the study. JM, RH, and AA carried out the experiments. BC and NF assisted in patient recruitment. YZ performed the statistical analysis. DER, YZ, RA, and PE-B wrote the original draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted manuscript.
This work was supported by the National Cancer Institute at the National Institutes of Health (Grant R01-CA177586) and a Moffitt Cancer Center Team Science grant. This work was also supported by the Flow Cytometry Core, Participant Research, Interventions, and Measurement (PRISM), Analytic Microscopy and Tissue Cores at the H. Lee Moffitt Cancer Center and Research Institute, a comprehensive cancer center designated by the National Cancer Institute and funded in part by Moffitt's Cancer Center Support Grant [P30-CA076292]. The funders were not involved in the study design, data collection/analysis, or manuscript preparation.
DER and PE-B filled a provisional Patent titled “Methods of detecting risk of a cancer,” application serial #63/041,676 filed on 6/19/2020. DER serves on the Board of Directors for NanoString Technologies, Inc. PE-B and the Moffitt Cancer Center and Research Institute received payment from licensing unrelated technology to Celgene Corporation and have an appropriate conflict-of-interest management plan. AA is currently employed by AstraZeneca.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This work was presented in part at the annual meeting of the American Association for Cancer Research (AACR), held virtually on June 22, 2020 and at the Keratinocyte Carcinoma Consortium (KeraCon) Virtual Scientific Research Meeting, held on March 16, 2021.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.735585/full#supplementary-material
1. Albert MR, Weinstock MA. Keratinocyte carcinoma. CA Cancer J Clin. (2003) 53:292–302. doi: 10.3322/canjclin.53.5.292
2. Leiter U, Keim U, Garbe C. Epidemiology of skin cancer: update 2019. Adv Exp Med Biol. (2020) 1268:123–39. doi: 10.1007/978-3-030-46227-7_6
3. Rogers HW, Weinstock MA, Harris AR, Hinckley MR, Feldman SR, Fleischer AB, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Archiv Dermatol. (2010) 146:283–7. doi: 10.1001/archdermatol.2010.19
4. Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatol. (2015) 151:1081–6. doi: 10.1001/jamadermatol.2015.1187
5. Lee DA, Miller SJ. Nonmelanoma skin cancer. Facial Plastic Surg Clin North Am. (2009) 17:309–24. doi: 10.1016/j.fsc.2009.04.004
6. Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, (2012). J Am Acad Dermatol. (2013) 68:957–66. doi: 10.1016/j.jaad.2012.11.037
7. Moan J, Grigalavicius M, Baturaite Z, Dahlback A, Juzeniene A. The relationship between UV exposure and incidence of skin cancer. Photodermatol Photoimmunol Photomed. (2015) 31:26–35. doi: 10.1111/phpp.12139
8. Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer. J Photochem Photobiol B Biol. (2001) 63:8–18. doi: 10.1016/s1011-1344(01)00198-1
9. Savoye I, Olsen CM, Whiteman DC, Bijon A, Wald L, Dartois L, et al. Patterns of ultraviolet radiation exposure and skin cancer risk: the E3N-SunExp study. J Epidemiol. (2018) 28:27–33. doi: 10.2188/jea.JE20160166
10. Didona D, Paolino G, Bottoni U, Cantisani C. Non melanoma skin cancer pathogenesis overview. Biomedicines. (2018) 6:6. doi: 10.3390/biomedicines6010006
11. Rass K, Reichrath J. UV damage and DNA repair in malignant melanoma and nonmelanoma skin cancer. Adv Exp Med Biol. (2008) 624:162–78. doi: 10.1007/978-0-387-77574-6_13
12. Jensen P, Hansen S, Moller B, Leivestad T, Pfeffer P, Geiran O, et al. Skin cancer in kidney and heart transplant recipients and different long-term immunosuppressive therapy regimens. J Am Acad Dermatol. (1999) 40(2 Pt 1):177–86.
13. Omland SH, Gniadecki R, Haedersdal M, Helweg-Larsen J, Omland LH. Skin cancer risk in hematopoietic stem-cell transplant recipients compared with background population and renal transplant recipients: a population-based cohort study. JAMA Dermatol. (2016) 152:177–83. doi: 10.1001/jamadermatol.2015.3902
14. Karagas MR, Waterboer T, Li Z, Nelson HH, Michael KM, Bavinck JN, et al. Genus beta human papillomaviruses and incidence of basal cell and squamous cell carcinomas of skin: population based case-control study. BMJ. (2010) 341:c2986. doi: 10.1136/bmj.c2986
15. Breuer J, Schwab N, Schneider-Hohendorf T, Marziniak M, Mohan H, Bhatia U, et al. Ultraviolet B light attenuates the systemic immune response in central nervous system autoimmunity. Ann Neurol. (2014) 75:739–58. doi: 10.1002/ana.24165
16. Schwarz T. 25 years of UV-induced immunosuppression mediated by T cells-from disregarded T suppressor cells to highly respected regulatory T cells. Photochem Photobiol. (2008) 84:10–8. doi: 10.1111/j.1751-1097.2007.00223.x
17. Bruhs A, Schwarz T. Ultraviolet radiation-induced immunosuppression: induction of regulatory T cells. Methods Mol Biol. (2017) 1559:63–73. doi: 10.1007/978-1-4939-6786-5_5
18. Yamazaki S, Nishioka A, Kasuya S, Ohkura N, Hemmi H, Kaisho T, et al. Homeostasis of thymus-derived Foxp3+ regulatory T cells is controlled by ultraviolet B exposure in the skin. J Immunol. (2014) 193:5488–97. doi: 10.4049/jimmunol.1400985
19. Saito C, Maeda A, Morita A. Bath-PUVA therapy induces circulating regulatory T cells in patients with psoriasis. J Dermatol Sci. (2009) 53:231–3. doi: 10.1016/j.jdermsci.2008.09.011
20. Kubo R, Muramatsu S, Sagawa Y, Saito C, Kasuya S, Nishioka A, et al. Bath-PUVA therapy improves impaired resting regulatory T cells and increases activated regulatory T cells in psoriasis. J Dermatol Sci. (2017) 86:46–53. doi: 10.1016/j.jdermsci.2017.01.001
21. Yu C, Fitzpatrick A, Cong D, Yao C, Yoo J, Turnbull A, et al. Nitric oxide induces human CLA(+)CD25(+)Foxp3(+) regulatory T cells with skin-homing potential. J Allergy Clin Immunol. (2017) 140:1441–4.e6. doi: 10.1016/j.jaci.2017.05.023
22. Ferran M, Romeu ER, Rincon C, Sagrista M, Gimenez Arnau AM, Celada A, et al. Circulating CLA+ T lymphocytes as peripheral cell biomarkers in T-cell-mediated skin diseases. Exp Dermatol. (2013) 22:439–42. doi: 10.1111/exd.12154
23. Tanaka A, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Cell Res. (2017) 27:109–18. doi: 10.1038/cr.2016.151
24. Miyara M, Yoshioka Y, Kitoh A, Shima T, Wing K, Niwa A, et al. Functional delineation and differentiation dynamics of human CD4+ T cells expressing the FoxP3 transcription factor. Immunity. (2009) 30:899–911. doi: 10.1016/j.immuni.2009.03.019
25. Nolte MA, van Olffen RW, van Gisbergen KP, van Lier RA. Timing and tuning of CD27-CD70 interactions: the impact of signal strength in setting the balance between adaptive responses and immunopathology. Immunol Rev. (2009) 229:216–31. doi: 10.1111/j.1600-065X.2009.00774.x
26. Sugiyama D, Nishikawa H, Maeda Y, Nishioka M, Tanemura A, Katayama I, et al. Anti-CCR4 mAb selectively depletes effector-type FoxP3+CD4+ regulatory T cells, evoking antitumor immune responses in humans. Proc Natl Acad Sci USA. (2013) 110:17945–50. doi: 10.1073/pnas.1316796110
27. Campbell DJ. Control of regulatory T cell migration, function, and homeostasis. J Immunol. (2015) 195:2507–13. doi: 10.4049/jimmunol.1500801
28. Hirahara K, Liu L, Clark RA, Yamanaka K, Fuhlbrigge RC, Kupper TS. The majority of human peripheral blood CD4+CD25highFoxp3+ regulatory T cells bear functional skin-homing receptors. J Immunol. (2006) 177:4488–94. doi: 10.4049/jimmunol.177.7.4488
29. Hesterberg RS, Amorrortu RP, Zhao Y, Hampras S, Akuffo AA, Fenske N, et al. T regulatory cell subpopulations associated with recent ultraviolet radiation exposure in a skin cancer screening cohort. J Immunol. (2018) 201:3269–81. doi: 10.4049/jimmunol.1800940
30. Amorrortu RP, Fenske NA, Cherpelis BS, Vijayan L, Zhao Y, Balliu J, et al. Viruses in skin cancer (VIRUSCAN): study design and baseline characteristics of a prospective clinic-based cohort study. Cancer Epidemiol Biomark Prevent. (2020) 29:39–48. doi: 10.1158/1055-9965.Epi-19-0446
32. Clarys P, Alewaeters K, Lambrecht R, Barel A. Skin color measurements: comparison between three instruments: the Chromameter®, the DermaSpectrometer® and the Mexameter®. Skin Res Technol. (2000) 6:230–8. doi: 10.1034/j.1600-0846.2000.006004230.x
33. Karagas MR, Zens MS, Nelson HH, Mabuchi K, Perry AE, Stukel TA, et al. Measures of cumulative exposure from a standardized sun exposure history questionnaire: a comparison with histologic assessment of solar skin damage. Am J Epidemiol. (2007) 165:719–26. doi: 10.1093/aje/kwk055
34. Kuklinski LF, Zens MS, Perry AE, Green AC, Karagas MR. Skin microtopography as a measure of photoaging and risk of squamous cell carcinoma of the skin in a US population. Photodermatol Photoimmunol Photomed. (2017) 33:41–8. doi: 10.1111/phpp.12280
35. Thomas NE, Kricker A, From L, Busam K, Millikan RC, Ritchey ME. Associations of cumulative sun exposure and phenotypic characteristics with histologic solar elastosis. Cancer Epidemiol. (2010) 19:2932–41. doi: 10.1158/1055-9965.Epi-10-0686
37. Zhang Z, Reinikainen J, Adeleke KA, Pieterse ME, Groothuis-Oudshoorn CG. Time-varying covariates and coefficients in Cox regression models. Ann Transl Med. (2018) 6:121. doi: 10.21037/atm.2018.02.12
38. Núñez NG, Tosello Boari J, Ramos RN, Richer W, Cagnard N, Anderfuhren CD, et al. Tumor invasion in draining lymph nodes is associated with Treg accumulation in breast cancer patients. Nat Commun. (2020) 11:3272. doi: 10.1038/s41467-020-17046-2
39. Cheng H, Luo G, Jin K, Fan Z, Huang Q, Gong Y, et al. Kras mutation correlating with circulating regulatory T cells predicts the prognosis of advanced pancreatic cancer patients. Cancer Med. (2020) 9:2153–9. doi: 10.1002/cam4.2895
40. Tang Y, Xu X, Guo S, Zhang C, Tang Y, Tian Y, et al. An increased abundance of tumor-infiltrating regulatory T cells is correlated with the progression and prognosis of pancreatic ductal adenocarcinoma. PLoS ONE. (2014) 9:e91551. doi: 10.1371/journal.pone.0091551
41. Zhang X, Kelaria S, Kerstetter J, Wang J. The functional and prognostic implications of regulatory T cells in colorectal carcinoma. J Gastroint Oncol. (2015) 6:307–13. doi: 10.3978/j.issn.2078-6891.2015.017
42. Tao H, Mimura Y, Aoe K, Kobayashi S, Yamamoto H, Matsuda E, et al. Prognostic potential of FOXP3 expression in non-small cell lung cancer cells combined with tumor-infiltrating regulatory T cells. Lung Cancer. (2012) 75:95–101. doi: 10.1016/j.lungcan.2011.06.002
43. Xie M, Wei J, Xu J. Inducers, attractors and modulators of CD4(+) Treg cells in non-small-cell lung cancer. Front Immunol. (2020) 11:676. doi: 10.3389/fimmu.2020.00676
44. Mailloux AW, Epling-Burnette PK. Effector memory regulatory T-cell expansion marks a pivotal point of immune escape in myelodysplastic syndromes. Oncoimmunology. (2013) 2:e22654. doi: 10.4161/onci.22654
45. Mailloux AW, Sugimori C, Komrokji RS, Yang L, Maciejewski JP, Sekeres MA, et al. Expansion of effector memory regulatory T cells represents a novel prognostic factor in lower risk myelodysplastic syndrome. J Immunol. (2012) 189:3198–208. doi: 10.4049/jimmunol.1200602
46. Ustun C, Miller JS, Munn DH, Weisdorf DJ, Blazar BR. Regulatory T cells in acute myelogenous leukemia: is it time for immunomodulation? Blood. (2011) 118:5084–95. doi: 10.1182/blood-2011-07-365817
47. Jadidi-Niaragh F, Ghalamfarsa G, Yousefi M, Tabrizi MH, Shokri F. Regulatory T cells in chronic lymphocytic leukemia: implication for immunotherapeutic interventions. Tumour Biol. (2013) 34:2031–9. doi: 10.1007/s13277-013-0832-x
48. Halim L, Romano M, McGregor R, Correa I, Pavlidis P, Grageda N, et al. An atlas of human regulatory T helper-like cells reveals features of Th2-like Tregs that support a tumorigenic environment. Cell Rep. (2017) 20:757–70. doi: 10.1016/j.celrep.2017.06.079
49. Li N, Wei W, Yin F, Chen M, Ma TR, Wu Q, et al. The abnormal expression of CCR4 and CCR6 on Tregs in rheumatoid arthritis. Int J Clin Exp Med. (2015) 8:15043–53.
50. Curiel TJ, Coukos G, Zou L, Alvarez X, Cheng P, Mottram P, et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat Med. (2004) 10:942–9. doi: 10.1038/nm1093
51. Lee I, Wang L, Wells AD, Dorf ME, Ozkaynak E, Hancock WW. Recruitment of Foxp3+ T regulatory cells mediating allograft tolerance depends on the CCR4 chemokine receptor. J Exp Med. (2005) 201:1037–44. doi: 10.1084/jem.20041709
Keywords: epidemiology, regulatory T cells, ultraviolet radiation exposure, cutaneous squamous cell carcinoma, risk stratification
Citation: Rollison DE, Messina JL, Cherpelis BS, Fenske NA, Schell MJ, Adeegbe DO, Zhao Y, Amorrortu RP, Akuffo AA, Hesterberg RS and Epling-Burnette PK (2021) Circulating Immunosuppressive Regulatory T Cells Predict Risk of Incident Cutaneous Squamous Cell Carcinoma. Front. Med. 8:735585. doi: 10.3389/fmed.2021.735585
Received: 02 July 2021; Accepted: 04 October 2021;
Published: 02 November 2021.
Edited by:
Salvador Gonzalez, University of Alcalá, SpainReviewed by:
Elisabetta Palazzo, University of Modena and Reggio Emilia, ItalyCopyright © 2021 Rollison, Messina, Cherpelis, Fenske, Schell, Adeegbe, Zhao, Amorrortu, Akuffo, Hesterberg and Epling-Burnette. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dana E. Rollison, ZGFuYS5yb2xsaXNvbkBtb2ZmaXR0Lm9yZw==
†ORCID: Dana E. Rollison orcid.org/0000-0002-3171-8045
Jane L. Messina orcid.org/0000-0002-0332-0224
Basil S. Cherpelis orcid.org/0000-0002-0332-0224
Neil A. Fenske orcid.org/0000-0002-0057-2434
Michael J. Schell orcid.org/0000-0003-4594-6601
Dennis O. Adeegbe orcid.org/0000-0001-9233-3328
Yayi Zhao orcid.org/0000-0003-0806-823X
Rossybelle P. Amorrortu orcid.org/0000-0001-6851-0179
Afua A. Akuffo orcid.org/0000-0002-7634-1608
Rebecca S. Hesterberg orcid.org/0000-0003-0472-7517
Pearlie K. Epling-Burnette orcid.org/0000-0002-2228-8784
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.