
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 14 October 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.728102
This article is part of the Research Topic Sepsis and COVID-19: Cross-Talk in Signalling Pathways and in Therapeutic Perspectives View all 11 articles
 Mohammad Abumayyaleh1*
Mohammad Abumayyaleh1* Iván J. Nuñez-Gil2†
Iván J. Nuñez-Gil2† Ibrahim El-Battrawy1Vicente Estrada2Víctor Manuel Becerra-Muñoz3
Ibrahim El-Battrawy1Vicente Estrada2Víctor Manuel Becerra-Muñoz3 Aitor Uribarri4Inmaculada Fernández-Rozas5Gisela Feltes6Ramón Arroyo-Espliguero7Daniela Trabattoni8
Aitor Uribarri4Inmaculada Fernández-Rozas5Gisela Feltes6Ramón Arroyo-Espliguero7Daniela Trabattoni8 Javier López Pais9Martino Pepe10
Javier López Pais9Martino Pepe10 Rodolfo Romero11María Elizabeth Ortega-Armas12
Rodolfo Romero11María Elizabeth Ortega-Armas12 Matteo Bianco13Thamar Capel Astrua14
Matteo Bianco13Thamar Capel Astrua14 Fabrizio D'Ascenzo15Oscar Fabregat-Andres16Andrea Ballester17
Fabrizio D'Ascenzo15Oscar Fabregat-Andres16Andrea Ballester17 Francisco Marín18
Francisco Marín18 Danilo Buonsenso19Raul Sanchez-Gimenez20
Danilo Buonsenso19Raul Sanchez-Gimenez20 Christel Weiß21Cristina Fernandez Perez22Antonio Fernández-Ortiz2Carlos Macaya2Ibrahim Akin1† and HOPE COVID-19 investigators
Christel Weiß21Cristina Fernandez Perez22Antonio Fernández-Ortiz2Carlos Macaya2Ibrahim Akin1† and HOPE COVID-19 investigatorsBackground: Patients with sepsis with a concomitant coronavirus (COVID-19) infection are related to a high morbidity and mortality rate. We investigated a large cohort of patients with sepsis with a concomitant COVID-19, and we developed a risk score for the estimation of sepsis risk in COVID-19.
Methods: We conducted a sub-analysis from the international Health Outcome Predictive Evaluation Registry for COVID-19 (HOPE-COVID-19-Registry, NCT04334291). Out of 5,837 patients with COVID-19, 624 patients were diagnosed with sepsis according to the Sepsis-3 International Consensus.
Results: In multivariable analysis, the following risk factors were identified as independent predictors for developing sepsis: current smoking, tachypnoea (>22 breath per minute), hemoptysis, peripheral oxygen saturation (SpO2) <92%, blood pressure (BP) (systolic BP <90 mmHg and diastolic BP <60 mmHg), Glasgow Coma Scale (GCS) <15, elevated procalcitonin (PCT), elevated troponin I (TnI), and elevated creatinine >1.5 mg/dl. By assigning odds ratio (OR) weighted points to these variables, the following three risk categories were defined to develop sepsis during admission: low-risk group (probability of sepsis 3.1–11.8%); intermediate-risk group (24.8–53.8%); and high-risk-group (58.3–100%). A score of 1 was assigned to current smoking, tachypnoea, decreased SpO2, decreased BP, decreased GCS, elevated PCT, TnI, and creatinine, whereas a score of 2 was assigned to hemoptysis.
Conclusions: The HOPE Sepsis Score including nine parameters is useful in identifying high-risk COVID-19 patients to develop sepsis. Sepsis in COVID-19 is associated with a high mortality rate.
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) outbreak, which was first emerged in Wuhan, China, in December 2019, has spread rapidly and has had an immense impact on the whole world. Consequently, states have endeavored to slow down the progression of the disease.
The course of coronavirus infectious disease (COVID-19) caused by SARS-CoV-2 is mild in the majority of patients. In 5% of COVID-19 patients, multiorgan dysfunction with an overall mortality rate of 1–11% was observed (1–4). However, sepsis is the main cause of death from the infection, particularly if not diagnosed and treated promptly.
It was revealed that many patients with severe COVID-19 showed general signs of shock (5). These patients met the sepsis and septic shock criteria according to the Sepsis-3 International Consensus (6). However, there are no comparative data available about the incidence and mortality rate in patients suffering from sepsis in COVID-19. In addition, predictors of sepsis have not yet been investigated.
In the international Health Outcome Predictive Evaluation Registry for COVID-19 (HOPE-COVID-19-Registry) (7), we compared baseline characteristics and clinical, laboratory, and radiologic findings in COVID-19 patients suffering from sepsis with those without sepsis at admission. We developed the HOPE Sepsis Score to estimate the risk of developing sepsis during admission. Predictors of mortality were analyzed.
HOPE-COVID-19 (NCT04334291) is an international project. It is designed as a retrospective cohort registry without any financial compensation. The data of 5,837 consecutive hospitalized patients with COVID-19 were gathered. We analyzed all included patients from March 1, 2020, to June 2, 2020. An online database was built and completed by each participating center. Additional information on datasets of the HOPE-COVID-19-Registry is available at www.hopeprojectmd.com. The methodology of the HOPE-COVID-19-Registry has been described previously (7, 8). The study was approved by the Ethics Committee in all involved centers.
The third international Consensus Task Force defined sepsis as life-threatening organ dysfunction due to a dysregulated host response to the infection. Organ failure in patients with sepsis increases in-hospital mortality by greater than 10% (6).
Clinical laboratory investigation consisted of transaminases, glomerular filtration rate (GFR), creatinine, lactate dehydrogenase (LDH), electrolytes, coagulation profile, and complete blood count. Radiological imaging, such as chest radiography or CT, to detect bilateral or unilateral infiltrates was applied. Abnormal blood pressure (BP) was defined as systolic BP (SBP) less than 90 mmHg or diastolic BP (DBP) less than 60 mmHg. Glasgow Coma Scale (GCS) consisted of eye-opening, verbal, and motor responses. Elevated creatinine was defined as an elevation of more than 1.5 mg/dl, elevated troponin I (TnI) more than 0.05 μg/L, and procalcitonin (PCT) more than 0.5 ng/ml. We gathered as primary end point all-cause mortality. Oxygen therapy at admission including high nasal-cannula, non-invasive ventilation, and invasive mechanical ventilation, respiratory insufficiency, heart failure, upper respiratory tract involvement, clinically relevant bleeding, and embolic events as secondary end points were reported. Missing data are addressed in the tables.
Data of continuous variables were performed as mean ± SD with a normal distribution, median (interquartile range) with a non-normal distribution, while categorical variables were presented as frequencies and percentages (%). The Kolmogorov-Smirnov test was used to test the normal distribution. The Mann-Whitney U-test and Student's t-test were used to compare normal or non-normal distributions of continuous variables, respectively. For distribution analysis of categorical variables, Fisher's exact test or chi-squared test was used. We applied a two-tailed Fisher's exact test in tests with a sample size of n = 5 or below. Results are performed with 95% CIs. We estimated the differences in both groups using Kaplan-Meier and applied Log-Rank statistics. Predictors of sepsis were identified by univariate analysis. Predictors with p < 0.0001 were analyzed by the logistic multivariate regression. These variables were used to build a Score system. The Score system was confirmed through comparison with random choice with 10% of all the participants. Harrell's C-index or the area under the receiver operating characteristic curve (AUC-ROC) was used to evaluate the ability of risk scores to predict outcome (C-index measures the goodness of fit of a model, with 0.5 indicating no discrimination and 1.0 indicating perfect prediction). We estimated the mortality risk according to HOPE Sepsis Score using Kaplan-Meier and applied Log-Rank statistics. Sensitivity, specificity, and positive (PPV) and negative predictive values (NPV) of HOPE Sepsis Score to predict the sepsis in low-, intermediate-, and high-risk groups were calculated. Statistical analysis was showed with SPSS (IBM Statistics, Version 23.0. Armonk, NY: IBM Corp). p < 0.05 was recognized as statistically significant.
At baseline, patients suffering from sepsis in COVID-19 were older than non-sepsis patients (≥65 years old; 66.3 vs. 52%; p < 0.001). Patients with sepsis showed more baseline comorbidities, such as arterial hypertension (65.2 vs. 46.9%; p < 0.001), dyslipidemia (41.9 vs. 32.8%; p < 0.001), diabetes mellitus (DM) (25.6 vs. 17.7%; p < 0.001), and current smoking (11.4 vs. 4.5%; p < 0.001), Table 1. Clinical presentations, such as dyspnoea (68.1 vs. 55%; p < 0.001), tachypnoea (46.3 vs. 23.5%; p < 0.001), hemoptysis (6.3 vs. 1.1%; p < 0.001), anosmia or hyposmia (10.4 vs. 5.9%; p < 0.001), and dysgeusia (11.7 vs. 6.3%; p < 0.001), were more observed in the sepsis group as compared to the non-sepsis group. Clinical parameters at admission were worse in patients with sepsis as compared to non-sepsis patients with a decrease in peripheral oxygen saturation (SpO2) <92% and abnormal BP (systolic BP <90 mmHg and/or diastolic BP <60 mmHg; 61.1 vs. 31.1%; p < 0.001; and 16.8 vs. 5.8%; p < 0.001). Similarly, changes in laboratory parameters were also more pronounced in sepsis group (Table 1).
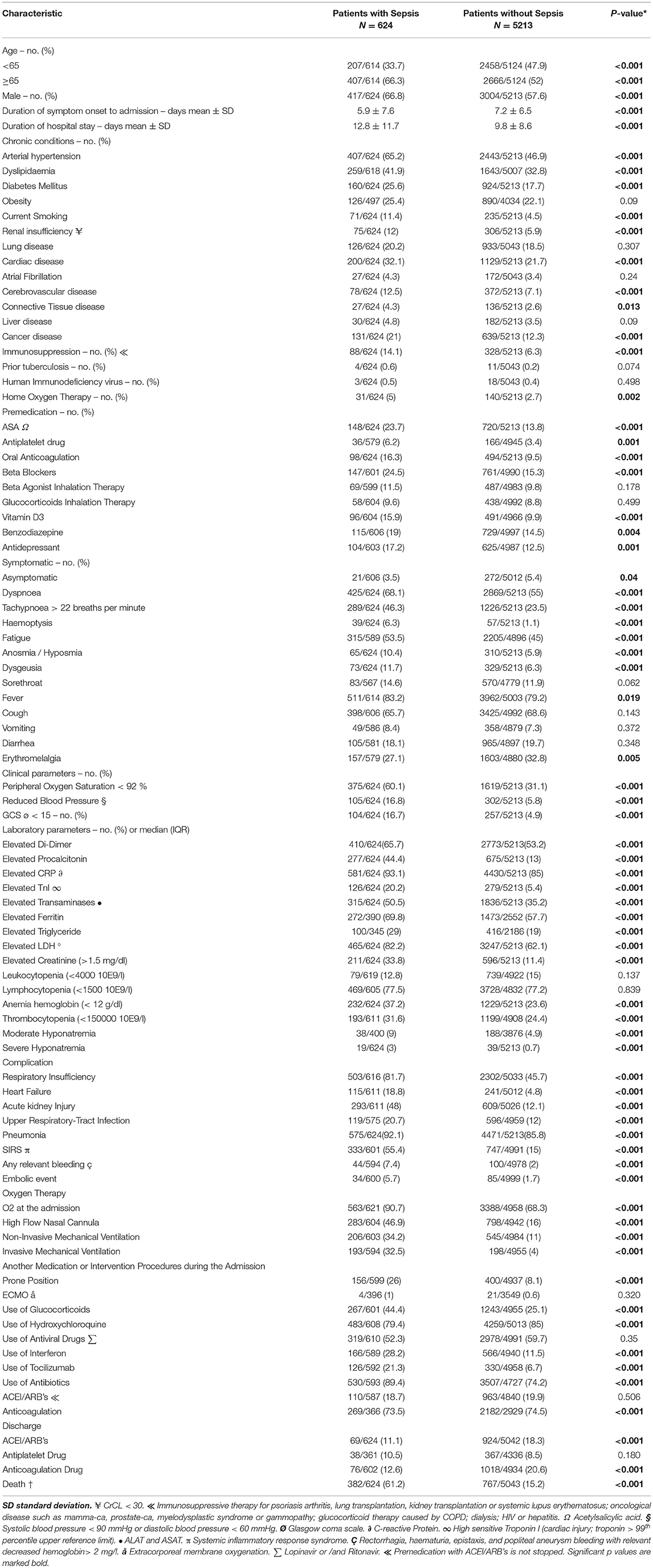
Table 1. Patients with Sepsis as compared to patients without Sepsis; Baseline characteristics, laboratory and radiographic findings, complications, and clinical outcomes.
Non-invasive ventilation and invasive mechanical ventilation were more often required in patients with sepsis as compared to those without sepsis, (34.2 vs. 11%; p < 0.001) and (32.5 vs. 4%; p < 0.001), respectively. Accordingly, the mortality rate was considerably higher in the sepsis group (61.2 vs. 15.2%; p < 0.001; Table 1).
During hospital stay, patients with sepsis more often received glucocorticoids (44.4 vs. 25.1%; p < 0.001), interferon (28.2 vs. 11.5%; p < 0.001), tocilizumab (21.3 vs. 6.7%; p < 0.001), and antibiotics (89.4 vs. 74.2%; p < 0.001). Interestingly, hydroxychloroquine use and antiviral drugs, such as lopinavir and/or ritonavir use, were higher in the non-sepsis group (79.4 vs. 85%; p < 0.001 and 52.3 vs. 59.7%; p = 0.35). Angiotensin-converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB) treatment at admission was not different in both groups (18.7 vs. 19.9%; p = 506; Table 1).
Table 2 presents the result of univariable and multivariable analyses. The multivariable analysis identified the following nine independent predictors to developing sepsis: current smoking (odds ratio, OR 2.43, 95% CI: 1.77–3.33; p < 0.001), tachypnoea (OR 1.60, 95% CI: 1.31–1.96; p < 0.001), hemoptysis (OR 4.30, 95% CI: 2.66–6.96; p < 0.001), reduced SpO2 <92% (OR 2.11, 95% CI: 1.73–2.57; p < 0.001), reduced BP at admission (OR 1.87, 95% CI: 1.08–3.22; p = 0.02), reduced GCS (OR 1.89, 95% CI: 1.42–2.51; p < 0.001), elevated PCT (OR 2.44, 95% CI: 1.99–2.99; p < 0.001), TnI (OR 1.94, 95% CI: 1.48–2.54; p < 0.001), and creatinine (OR 2.24, 95% CI: 1.81–2.78; p < 0.001). We divided the OR value of each variable by the median value of the regression coefficients of all variables (rounded to nearest 0.5 points). A score of 1 was assigned to current smoking, tachypnoea, decreased SpO2, decreased BP, decreased GCS, elevated PCT, TnI, and creatinine, whereas a score of 2 was assigned to hemoptysis. This score can be used to assess the risk for developing sepsis by assigning patients with COVID-19 to three risk groups: a low-risk group from 0 to 2 points, an intermediate-risk group from 3 to 5 points, and a high-risk group from 6 to 10 points (Figure 1). The probability of sepsis risk was 3.1–11.8% in the low-risk group, 24.8–53.8% in the intermediate-risk group, and 58.3–100% in the high-risk group.
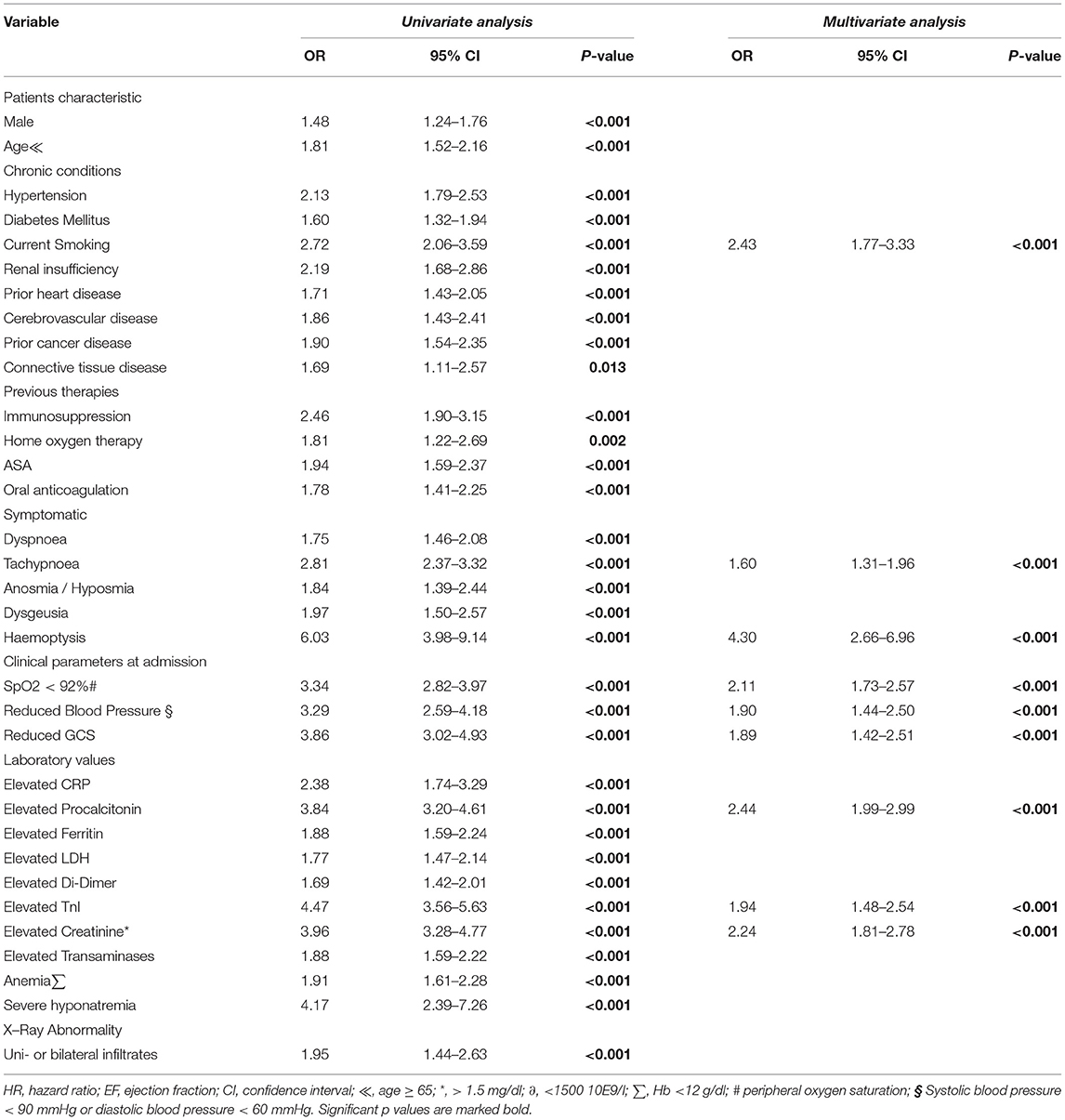
Table 2. Predictors of Sepsis, multivariate analysis.
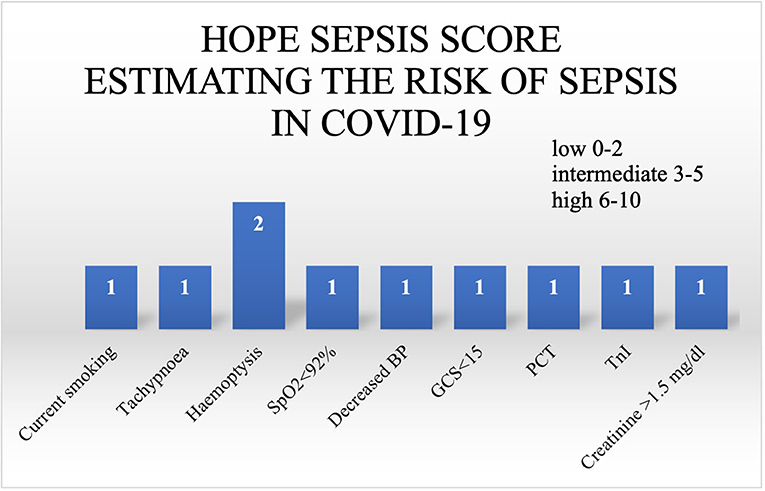
Figure 1. HOPE Sepsis Score, C-index = 0.763 (N = 5,837); tachypnoea >22 breath per minute; SpO2, peripheral oxygen saturation; BP, blood pressure; GCS <15 (Glasgow coma scale); PCT, elevated procalcitonin; TnI, elevated troponin; creatinine, elevated creatinine > 1.5 mg/dl; HOPE, the international Health Outcome Predictive Evaluation.
The final model was applied to the validation cohort (random choice of 10% of all study participants). The C-index for the HOPE Sepsis Score was 0.763, while the C-index for the validation cohort was 0.77 (Table 3). In addition, the sensitivity of the HOPE Sepsis Score to predict sepsis was higher in the intermediate-risk group as compared to high-risk patients (81.1 vs. 34.3%). On the other hand, the specificity and PPV were lower in the intermediate-risk group than in patients with high risk for sepsis, respectively (specificity: 80.3 vs. 99.2% and PPV: 32.4 vs. 66.1%). In addition, estimating the risk of mortality in COVID-19 according to HOPE Sepsis Score was investigated (Figure 2). Clinical characteristics of the validated group, sensitivity, specificity, PPV, and NPV are presented in the Supplementary Materials.
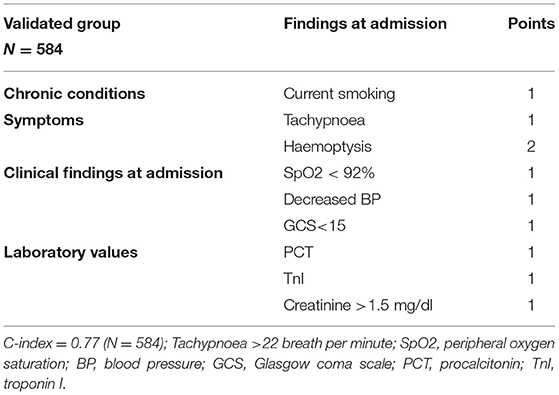
Table 3. The validation of HOPE Sepsis Score; the Risk of developing sepsis in COVID-19 in the validated group (n = 584) as compared to all patients (n = 5837).
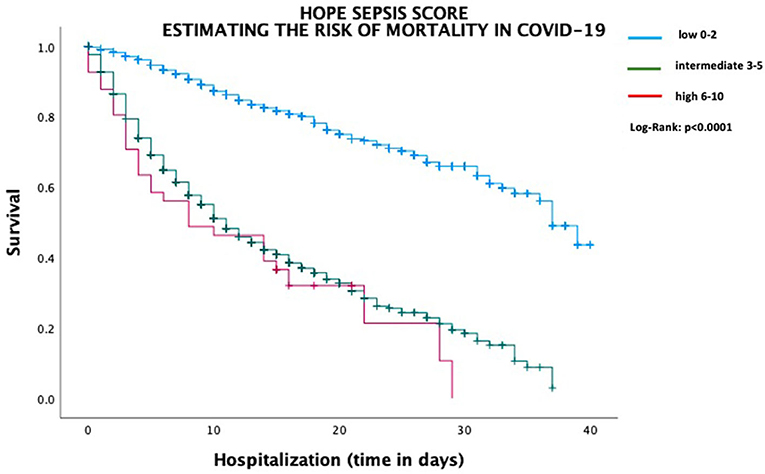
Figure 2. Estimating the risk of mortality in COVID-19 according to HOPE Sepsis Score.
HOPE-COVID-19-Registry shows real-world experience from data worldwide. The present study shows patient characteristics at baseline, in-hospital complications, and mortality, particularly in the participants with sepsis. The main findings of the study are that (1) patients suffering from sepsis in COVID-19 had higher rates of comorbidity, (2) the incidence of sepsis in COVID-19 is estimated at 11%, (3) predictors for developing sepsis are identified, and (4) HOPE Sepsis Score is developed to support physicians to early identifying of COVID-19 patients with sepsis on the basis of chronic conditions, clinical findings, hemodynamic, and laboratory parameters at admission.
Patients with sepsis were older and had more comorbidities as compared to patients with non-sepsis. The incidence of sepsis in COVID-19 is estimated at 11%. In addition, in the sepsis cohort, an increase of inflammatory markers, such as CRP, PCT, and ferritin, was more pronounced than in participants with non-sepsis. This phenomenon is known in patients with sepsis due to excessive inflammation (9). In patients with COVID-19, the immune response seems to be more pronounced and may be based on underlying pathomechanisms: macrophage-activation syndrome, viral sepsis-induced immune paralysis, and dysregulation of an intermediate functional state of the immune system in infected patients with SARS-CoV-2 (10–12). Other laboratory abnormalities were more observed in participants with sepsis than those without sepsis, such as elevated d-dimer, transaminases, creatinine, LDH, anemia, thrombocytopenia, triglyceride, and hyponatremia. These abnormalities indicate that liver and kidney functions were impaired, such as coagulation disorder in patients with sepsis at admission. Clinical Data from 409 US hospitals from 2009 to 2014 in patients showed a slightly lower sepsis rate of 6% as compared to our data (13). Chen et al. reported that dead 119 patients with COVID-19 presented an increase of inflammatory parameters (14). The coagulation disorder may develop disseminated intravascular coagulopathy (DIC) in patients with sepsis. Therefore, it is proposed to establish prophylaxis against venous thromboembolism (VTE) (15). These changes, such as abnormal coagulation function, were observed in patients infected with SARS-CoV-2 (2, 14, 16). Additionally, COVID-19 patients have built antiphospholipid antibodies (17). However, the inflammation could increase procoagulant activity thereby contributing to thrombus formation (18). All these abnormalities may explain the higher rate of thromboembolism and multiorgan dysfunction in patients with sepsis.
HOPE Sepsis Score is developed and validated to support physicians to identify COVID-19 patients with sepsis. The score integrates nine parameters ranging from medical history to clinical and laboratory findings. Collecting the clinical findings, such as current smoking, hemoptysis, tachypnoea, decreased BP, GCS, SpO2, elevated PCT, TnI, and creatinine, at admission is relatively easy and promptly. Concerning this matter, a score of 2 is assigned to hemoptysis that represents an important predictor for developing sepsis. However, Hemoptysis is a less common symptom in patients with COVID-19 (1). As laboratory findings, the HOPE Sepsis Score represents TnI, PCT, and elevated creatinine as predictors for developing sepsis as compared to the sequential failure assessment (SOFA) score, which only included respiratory rate, GCS, BP, and elevated creatinine (6). To summarize, the HOPE Sepsis Score is also useful and feasible in identifying high-risk COVID-19 patients predicted to develop sepsis with a high mortality rate. The C-index for HOPE Sepsis Score was 0.763; the score can also be used to predict sepsis in COVID-19. The C-index of SOFA score in patients who required intensive care unit (ICU) was 0.74, while the C-index in other hospitalized patients was 0.79 (6). In addition, the C-index of qSOFA was 0.66 in ICU while it was 0.81 for non-ICU patients (19). The logistic organ dysfunction score (LODS) can be used to assessing the severity of sepsis in ICU. The C-index of LODS was 0.843 (20). In summary, the C-index of our score is comparable to the recently published scores. Additionally, the sensitivity of the HOPE Sepsis Score to predict sepsis was higher in intermediate as compared to high-risk patients (81.1 vs. 34.3%). On the other hand, the specificity and PPV of the HOPE Sepsis Score to predict the risk of sepsis were lower in patients with intermediate than those with high-risk for sepsis, respectively (specificity: 80.3 vs. 99.2% and PPV: 32.4 vs. 66.1%). However, the sensitivity and specificity of qSOFA ≥ 2 to predict in-hospital mortality were 69 and 55.5%, respectively (21). In 2,112 patients suffering from infections, the calculation of systemic inflammatory response syndrome (SIRS) and qSOFA showed a sensitivity of 52.8 and 19.5% and a specificity of 52.5 and 92.6% for 28-day mortality (22).
The use of antibiotic treatment was significantly higher in patients with sepsis than those without sepsis, followed by hydroxychloroquine and then antiviral drugs. Prone position was more revealed in sepsis as compared to patients with non-sepsis. The co-infection among COVID-19 patients with diverse co-pathogens including bacteria was reported (23). In one observational study, the treatment with hydroxychloroquine was not associated with a lower mortality rate (24). RECOVERY trial did not show a reduction of 28-day-mortality in patients with COVID-19 after lopinavir-ritonavir treatment (25). However, these patients did not suffer from sepsis. In addition, the short duration of prone position associated with better oxygenation did not improve the mortality rate (26). In other clinical trials, prone positioning for 16 hours every day in patients with acute respiratory distress syndrome (ARDS) was reduced to 90-day mortality (27). However, further randomized clinical trials are needed to investigate the safety and efficacy of all treatment options in patients infected by SARS-CoV-2.
The mortality rate was significantly higher in patients with sepsis as compared to the non-sepsis group due to diverse complications (61.2 vs. 15.2%). In addition to respiratory insufficiency, other complications were more observed among patients with sepsis in comparison to non-sepsis participants; these included heart failure, acute kidney injury, pneumonia, bleeding, embolic event, and need for oxygen therapy including high flow nasal cannula, non-invasive, and invasive mechanical ventilation. In New York City, the mortality rate of COVID-19 patients, who received invasive mechanical ventilation, was less than the rate in our sepsis cohort (14.6%) but comparable with the non-sepsis group (28). Additionally, COVID-19 patients with cardiac injury presented a high mortality rate (51.2%) (29). In this regard, our data also showed that elevated TnI was associated with developing sepsis and consequently a high mortality rate. However, data in patients with sepsis with COVID-19 are limited.
At last, in comparison to SARS-CoV with 8,098 cases across 29 countries and Middle East respiratory syndrome (MERS) with 2,494 cases across 27 countries with the case-fatality rate (CFR) of 10% and 35%, the CFR of SARS-CoV-2 in Hubei was 2.9% and outside Hubei 0.4% with respect of challenges to identify all cases particularly with asymptomatic and mild courses (4, 30).
Therefore, patients with more comorbidities are susceptible to suffer from sepsis. Smokers who particularly suffering from hemoptysis and tachypnoea with decreased BP, SpO2, and GCS at admission who show abnormal laboratory as elevated PCT, TnI, and creatinine are more potential to develop sepsis when infected by SARS-CoV-2.
This study has some limitations. It has a retrospective character, not all laboratory tests were done in all patients. In addition, data about blood, urine, and stool culture are missing. External validation of our sepsis score is not performed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University Medical Centre Mannheim, University of Heidelberg, Mannheim, Germany. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MA, IN-G, IE-B, and IA made substantial contributions to the study concept and design. All authors took obtaining ethical approval. Data were collected by MA, IN-G, IE-B, VE, VB-M, AU, IF-R, GF, RA-E, DT, JL, MP, RR, MO-A, MB, TA, FD'A, OF-A, AB, FM, DB, RS-G, CF, AF-O, and CM. MA, IN-G, and IA analysed all data. CW supported the descriptive statistics. IN-G approved the statistical analysis. MA, IN-G, IE-B, and IA prepared the manuscript. All authors contributed to the article and approved the submission version.
Non-conditioned grant (Fundación Interhospitalaria para la Investigación Cardiovascular, FIC, Madrid, Spain). This nonprofit institution had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; nor in the decision to submit the paper for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Cardiovascular Excellence SL for their essential support in the database and HOPE webpage.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.728102/full#supplementary-material
1. Guan WJ Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
3. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
4. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. (2020) 323:1239–42. doi: 10.1001/jama.2020.2648
5. Li H, Liu L, Zhang D, Xu J, Dai H, Tang N, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. (2020) 395:1517–20. doi: 10.1016/S0140-6736(20)30920-X
6. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. (2016) 315:801–10. doi: 10.1001/jama.2016.0287
7. Nunez-Gil IJ, Estrada V, Fernandez-Perez C, Feltes G, Vedia O, Vergara-Uzcategui CE, et al. Health Outcome Predictive Evaluation for COVID 19 international registry (HOPE COVID-19), rationale and design. Contemp Clin Trials Commun. (2020) 20:100654. doi: 10.1016/j.conctc.2020.100654
8. Nunez-Gil IJ, Fernandez-Perez C, Estrada V, Becerra-Munoz VM, El-Battrawy I, Uribarri A, et al. Mortality risk assessment in Spain and Italy, insights of the HOPE COVID-19 registry. Intern Emerg Med. (2021) 16:957–66. doi: 10.1007/s11739-020-02543-5
9. van der Poll T, van de Veerdonk FL, Scicluna BP, Netea MG. The immunopathology of sepsis and potential therapeutic targets. Nat Rev Immunol. (2017) 17:407–20. doi: 10.1038/nri.2017.36
10. Kyriazopoulou E, Leventogiannis K, Norrby-Teglund A, Dimopoulos G, Pantazi A, Orfanos SE, et al. Macrophage activation-like syndrome: an immunological entity associated with rapid progression to death in sepsis. BMC Med. (2017) 15:172. doi: 10.1186/s12916-017-0930-5
11. Lukaszewicz AC, Grienay M, Resche-Rigon M, Pirracchio R, Faivre V, Boval B, et al. Monocytic HLA-DR expression in intensive care patients: interest for prognosis and secondary infection prediction. Crit Care Med. (2009) 37:2746–52. doi: 10.1097/00003246-200910000-00011
12. Giamarellos-Bourboulis EJ, Netea MG, Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe. (2020) 27:992–1000 e3. doi: 10.1016/j.chom.2020.04.009
13. Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, et al. Incidence and trends of Sepsis in US hospitals using clinical vs claims data, 2009-2014. JAMA. (2017) 318:1241–9. doi: 10.1001/jama.2017.13836
14. Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. (2020) 368:m1091. doi: 10.1136/bmj.m1091
15. Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood. (2020) 135:2033–40. doi: 10.1182/blood.2020006000
16. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
17. Zhang Y, Xiao M, Zhang S, Xia P, Cao W, Jiang W, et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. N Engl J Med. (2020) 382:e38. doi: 10.1056/NEJMc2007575
18. Corrales-Medina VF, Musher DM, Shachkina S, Chirinos JA. Acute pneumonia and the cardiovascular system. Lancet. (2013) 381:496–505. doi: 10.1016/S0140-6736(12)61266-5
19. Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. (2016) 315:762–74. doi: 10.1001/jama.2016.0288
20. Le Gall JR, Klar J, Lemeshow S, Saulnier F, Alberti C, Artigas A, et al. The logistic organ dysfunction system. A new way to assess organ dysfunction in the intensive care unit ICU Scoring Group. JAMA. (1996) 276:802–10. doi: 10.1001/jama.276.10.802
21. Perman SM, Mikkelsen ME, Goyal M, Ginde A, Bhardwaj A, Drumheller B, et al. The sensitivity of qSOFA calculated at triage and during emergency department treatment to rapidly identify sepsis patients. Sci Rep. (2020) 10:20395. doi: 10.1038/s41598-020-77438-8
22. Abdullah S, Sorensen RH, Dessau RBC, Sattar S, Wiese L, Nielsen FE. Prognostic accuracy of qSOFA in predicting 28-day mortality among infected patients in an emergency department: a prospective validation study. Emerg Med J. (2019) 36:722–8. doi: 10.1136/emermed-2019-208456
23. Jean SS, Lee PI, Hsueh PR. Treatment options for COVID-19: the reality and challenges. J Microbiol Immunol Infect. (2020) 53:436–43. doi: 10.1016/j.jmii.2020.03.034
24. Geleris J, Sun Y, Platt J, Zucker J, Baldwin M, Hripcsak G, et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N Engl J Med. (2020) 382:2411–8. doi: 10.1056/NEJMoa2012410
25. Group RC. Lopinavir-ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. (2020) 396:1345–52. doi: 10.2139/ssrn.3675410
26. Telias I, Katira BH, Brochard L. Is the prone position helpful during spontaneous breathing in patients with COVID-19? JAMA. (2020) 323:2265–7. doi: 10.1001/jama.2020.8539
27. Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. (2013) 368:2159–68. doi: 10.1056/NEJMoa1214103
28. Goyal P, Choi JJ, Pinheiro LC, Schenck EJ, Chen R, Jabri A, et al. Clinical characteristics of Covid-19 in New York City. N Engl J Med. (2020) 382:2372–4. doi: 10.1056/NEJMc2010419
29. Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. (2020). doi: 10.1001/jamacardio.2020.0950
Keywords: sepsis, score, COVID-19, SARS-CoV-2, outcome
Citation: Abumayyaleh M, Nuñez-Gil IJ, El-Battrawy I, Estrada V, Becerra-Muñoz VM, Uribarri A, Fernández-Rozas I, Feltes G, Arroyo-Espliguero R, Trabattoni D, López Pais J, Pepe M, Romero R, Ortega-Armas ME, Bianco M, Astrua TC, D'Ascenzo F, Fabregat-Andres O, Ballester A, Marín F, Buonsenso D, Sanchez-Gimenez R, Weiß C, Fernandez Perez C, Fernández-Ortiz A, Macaya C, Akin I and HOPE COVID-19 investigators (2021) Sepsis of Patients Infected by SARS-CoV-2: Real-World Experience From the International HOPE-COVID-19-Registry and Validation of HOPE Sepsis Score. Front. Med. 8:728102. doi: 10.3389/fmed.2021.728102
Received: 20 June 2021; Accepted: 06 September 2021;
Published: 14 October 2021.
Edited by:
Reinaldo Salomao, Federal University of São Paulo, BrazilReviewed by:
Kefu Tang, Shanghai JiaoTong University School of Medicine, ChinaCopyright © 2021 Abumayyaleh, Nuñez-Gil, El-Battrawy, Estrada, Becerra-Muñoz, Uribarri, Fernández-Rozas, Feltes, Arroyo-Espliguero, Trabattoni, López Pais, Pepe, Romero, Ortega-Armas, Bianco, Astrua, D'Ascenzo, Fabregat-Andres, Ballester, Marín, Buonsenso, Sanchez-Gimenez, Weiß, Fernandez Perez, Fernández-Ortiz, Macaya, Akin and HOPE COVID-19 Investigators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Abumayyaleh, bW9oYW1tYWQuYWJ1bWF5eWFsZWhAbWVkbWEudW5pLWhlaWRlbGJlcmcuZGU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.