 Lilin Yang1†
Lilin Yang1† Songping Luo
Songping Luo- 1Department of Gynecology and Obstetrics, The First Affiliated Hospital, Guangzhou University of Chinese Medicine, Guangzhou, China
- 2Acupuncture, Moxibustion and Rehabilitation School of Clinical Medicine, Guangzhou University of Chinese Medicine, Guangzhou, China
- 3Second School of Clinical Medicine, Guangzhou University of Chinese Medicine, Guangzhou, China
- 4First School of Clinical Medicine, Guangzhou University of Chinese Medicine, Guangzhou, China
Objective: The aim of this study was to develop a nomogram to predict the risk of premature rupture of membrane (PROM) in pregnant women with vulvovaginal candidiasis (VVC).
Patients and methods: We developed a prediction model based on a training dataset of 417 gravidas with VVC, the data were collected from January 2013 to December 2020. The least absolute shrinkage and selection operator regression model was used to optimize feature selection for the model. Multivariable logistic regression analysis was applied to build a prediction model incorporating the feature selected in the least absolute shrinkage and selection operator regression model. Discrimination, calibration, and clinical usefulness of the prediction model were assessed using the C-index, calibration plot, and decision curve analysis. Internal validation was assessed using bootstrapping validation.
Results: Predictors contained in the prediction nomogram included age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis. The model displayed discrimination with a C-index of 0.684 (95% confidence interval: 0.631–0.737). Decision curve analysis showed that the PROM nomogram was clinically useful when intervention was decided at a PROM possibility threshold of 13%.
Conclusion: This novel PROM nomogram incorporating age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis could be conveniently used to facilitate PROM risk prediction in gravidas.
Introduction
Premature rupture of membrane (PROM) is defined as a spontaneous rupture of embryonic membrane occurring before the onset of labor. PROM occurs in ~8% of all deliveries (1) and can lead to adverse fetal and neonatal outcomes. Adverse outcomes include: for mothers, intra-amniotic infection, postpartum infection, endometritis; and for newborns, cord prolapse, respiratory distress syndrome, sepsis, intraventricular hemorrhage, and even death.
Vulvovaginal candidiasis (VVC) is a common vaginitis that affects 75% of women at least once in their lifetime (2, 3). More than one fifth of women have experienced recurrent VVC (at least 3 symptomatic episodes in a previous year) (4). In high-income countries, recurrent VVC affects about 138 million women annually, and the economic burden from lost productivity is estimated to be up to billion annually (5). Pregnancy increases the incidence of VVC owing to changes of the internal immune environment of the genital tract.
PROM results from the interaction of many factors (6, 7). However, several studies (8–11) have revealed that genital tract infection is the main cause. As the most common cause of vaginitis, VVC plays a significant role in the incidence of PROM. Although, there have been studies regarding the relationship between VVC and PROM, to date, there is no established method for predicting the probability of PROM in pregnant women with VVC. The purpose of this study was to develop a valid but simple prediction tool to assess the risk of PROM in VVC individuals.
Patients and Methods
Patients Study Population
We undertook a study of women with VVC who were hospital in-patients, from January 2013 to December 2020. This study was approved by the Ethical Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine. Clinical data were evaluated, and the inclusion criteria were as follows: diagnosed as VVC in gestation no matter whether cured or not, singleton pregnancies, and delivery of pregnancy at 28–42 weeks via vaginal delivery or cesarean. The exclusion criteria were: cases with twins or multiple pregnancies, and termination of pregnancy at <28 weeks or >42 weeks. Patients who had severe cognitive disorders, or had serious physical constraints were excluded. The clinical data came from the Hospital information management system in the First Affiliated Hospital of Guangzhou University of Chinese Medicine. and were categorized as: basic patient demographics (age, education level, occupation, marital status, BMI before pregnancy, and regular perinatal visits); history of gestation (gravidity, parity, number of previous vaginal deliveries, number of previous cesarean sections, and number of previous abortions); past medical history (history of VVC before pregnancy, history of cervix operation); other information in the current pregnancy (gestational week of VVC diagnosis, symptoms with VVC, cured of VVC during pregnancy, antifungal therapy during pregnancy, bacterial vaginitis, mycoplasma, chlamydia, polyhydramnios, macrosomia, and malpresentation). PROM manifests as amniorrhexis prior to the onset of labor. The diagnosis of VVC and VVC cure were both confirmed by laboratory testing. Based on the Guideline of preconception care and prenatal care of China (2018) (12), the minimum number of prenatal times was seven. Missing minimum one time inspection was considered out of regular perinatal visit.
Statistical Analysis
Statistical analyses were performed using SPSS (Version 22.0) and R software (Version 4.0.3). In R software, Packages (“rms”) and Packages (“rmda”) were operated. All tests were two-sided, and a P-value < 0.05 was considered statistically significant. Categorical variables were presented as the number of cases, percentages (%). The least absolute shrinkage and selection operator (LASSO) method, which is suitable for the reduction of high-dimensional data (13, 14) was used to select the optimal predictive features associated with risk factors in pregnant women with VVC. Feathers with non-zero coefficients in the LASSO regression model were selected. Subsequently, multivariable logistic regression analysis was used to build a prediction model by incorporating the features selected in the LASSO regression model. Sociodemographic variables with a P-value of ≤ 0.05 were included in the model, whereas variables associated with disease and treatment characteristics were all included (15). All potential predictors were used to develop a prediction model for PROM by using the whole cohort. Afterwards, calibration curves were plotted to assess the calibration of the PROM nomogram. A significant test statistic implied that the model did not calibrate perfectly. To quantify the discrimination performance of PROM, Harrell's C-index was measured. The PROM nomogram was subjected to bootstrapping validation (1,000 bootstrap resamples) to calculate a relative corrected C-index (16). Decision curve analysis was conducted to determine the clinical usefulness of the PROM nomogram by quantifying the net benefit; this was calculated by subtracting the proportion of the patients who were false positive and by weighing the relative harm of forgoing interventions compared with the negative consequence of an unnecessary intervention.
Results
Patient Characteristics
A total of 417 patients were enrolled. All the patients were divided into PROM and no PROM groups. Patient data included patient demographics, history of gestation, past medical history, and other information (see Table 1); the incidence of PROM was 33.81%.
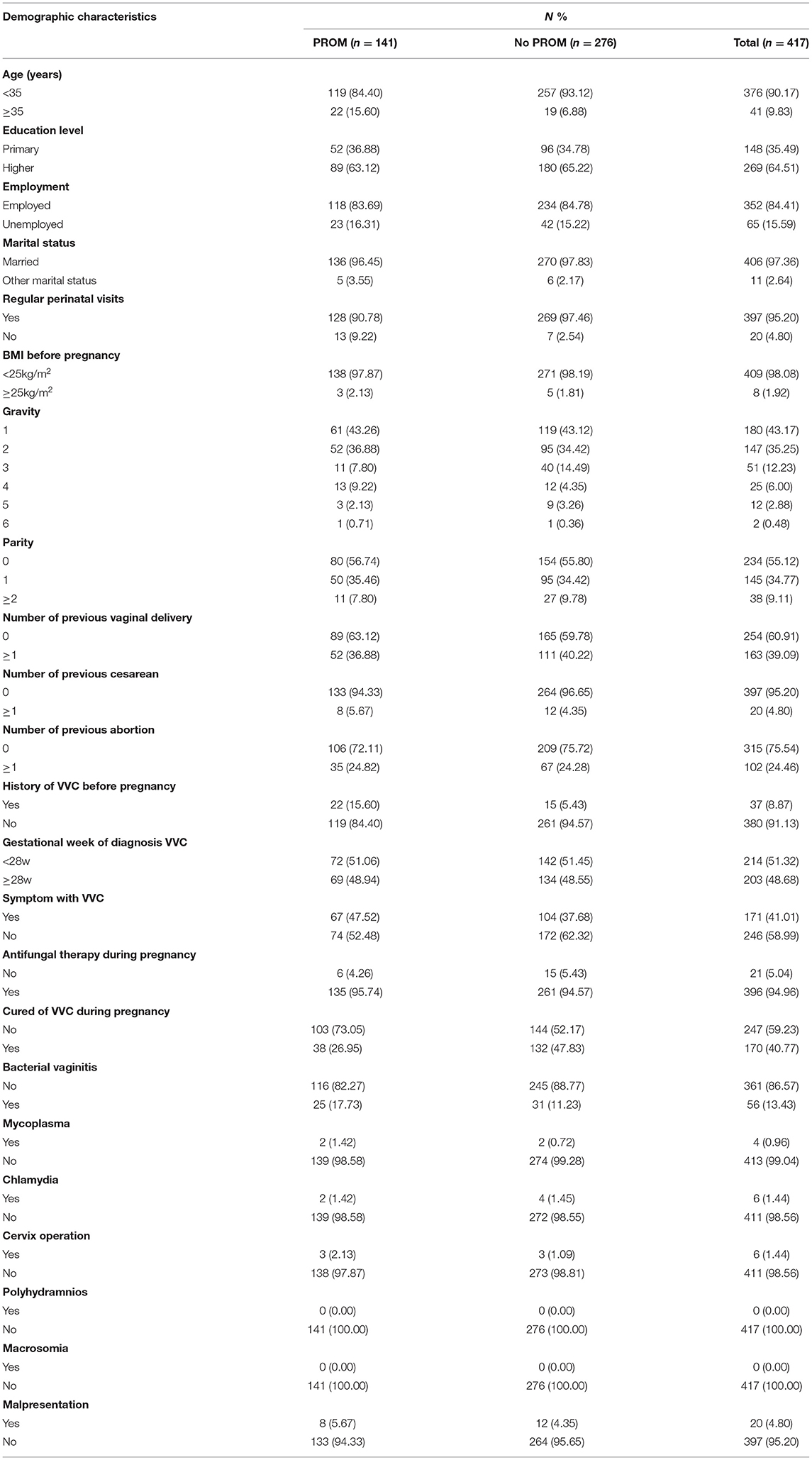
Table 1. Difference between demographic and clinical characteristics of PROM and no PROM groups.
Feature Selection
Of basic demographic, medical history, and treatment features, 23 features were reduced to 6 potential predictors on the basis of 417 patients in the cohort (Figure 1) and were associated with non-zero coefficients in the LASSO regression model. These features included age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis (Table 2).
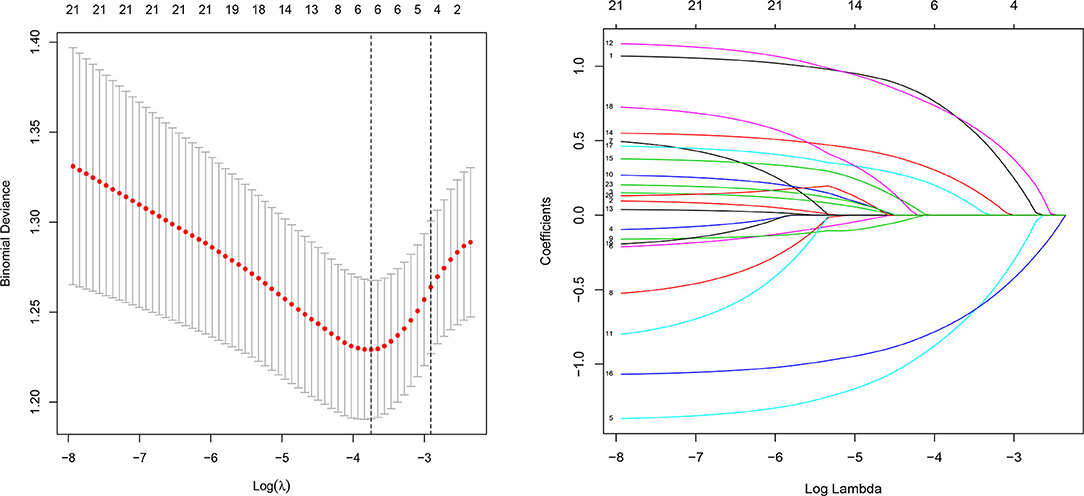
Figure 1. Demographic and clinical feature selection using the LASSO logistic regression model. LASSO, least absolute shrinkage and selection operator; SE, standard error.
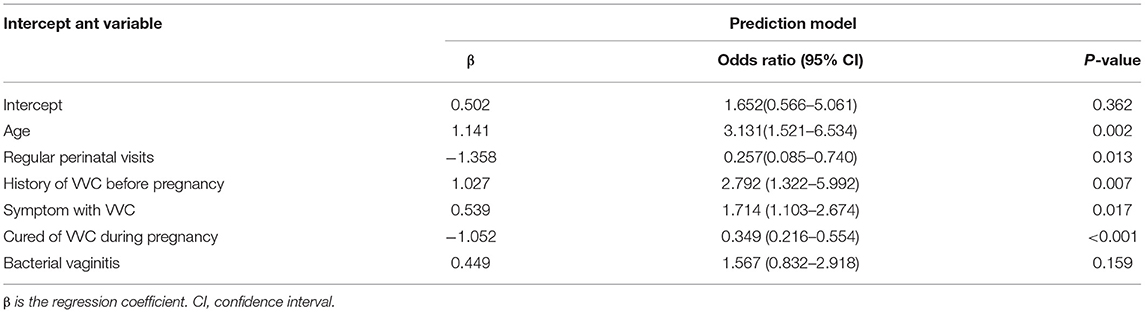
Table 2. Prediction factors for PROM in pregnant patients with VVC.
Development of an Individualized Prediction Model
The results of logistic regression analysis among the use of age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis are given in Table 2. The model that incorporated the above independent predictors was developed and presented as the nomogram (Figure 2).
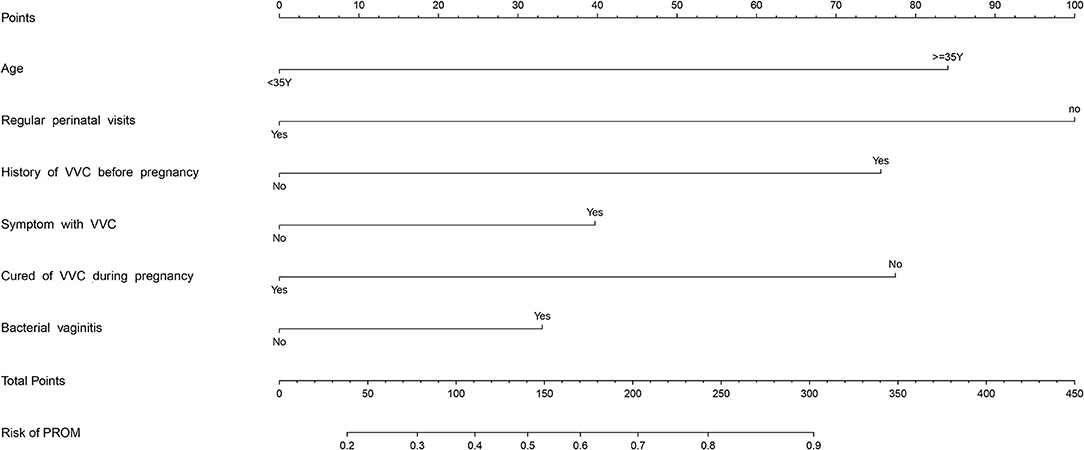
Figure 2. PROM risk assessment tool. Points refers to point for the individual risk factor and add together to the total points.
Apparent Performance of the PROM Risk Nomogram in the Cohort
The calibration curve of the PROM risk nomogram for the prediction of PROM in pregnant women indicated good agreement in this cohort (Figure 3). The C-index for the prediction nomogram was 0.684 (95% confidence interval: 0.631–0.737) for the cohort.
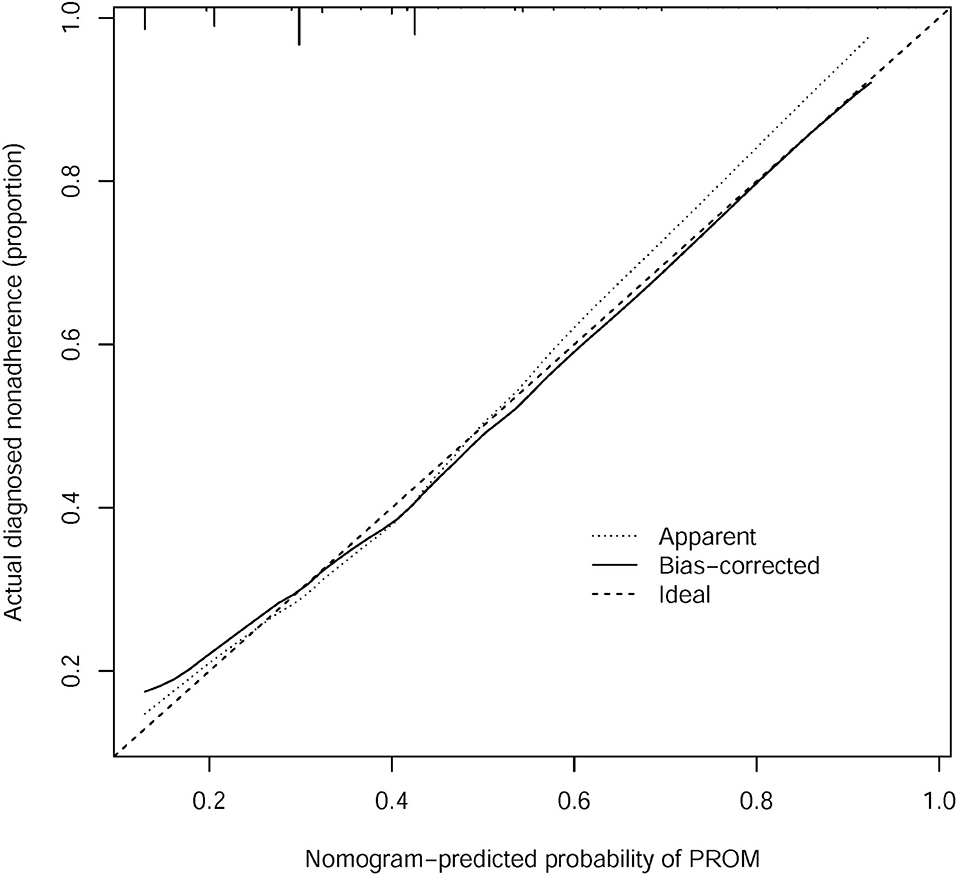
Figure 3. Calibration curves of the PROM nomogram prediction in the cohort.
Clinical use
The decision curve analysis for the PROM nomogram is presented in Figure 4. The decision curve showed that, if the threshold probability of a patient and a doctor was >13 and <34%, respectively, the use of this PROM nomogram to predict PROM risk added more benefit than the scheme. Within this range, net benefit was comparable with several overlaps, on the basis of the PROM risk nomogram.
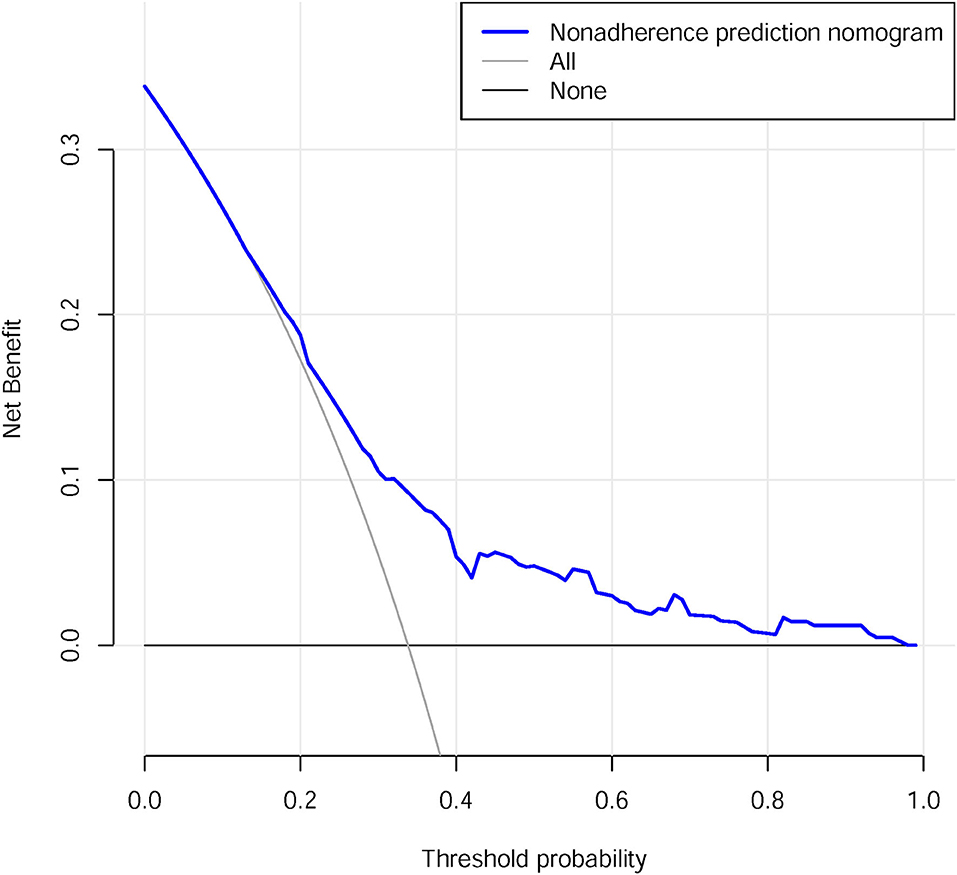
Figure 4. Decision curve analysis for the PROM nomogram.
Discussion
Nowadays, nomograms are widely used as prognostic devices in oncology and medicine. Nomograms depend on user-friendly digital interfaces, increased accuracy, and more easily understood prognoses to improve patient management and clinical decision making. Our research was the first study to develop and validate a new nomogram to predict the risk of PROM in pregnant women with VVC. The covariates included age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis.
One large samples study in East China previously demonstrated that 15.3% of a total of 111,390 pregnant women suffered from PROM (17). In our study, about 33.8% of pregnant women with VVC suffered from PROM, which is double the findings of the previous study that the included population was not especially for VVC pregnant women. Therefore, it is suggested that PROM in pregnant women with VVC should be carefully managed. This nomogram suggested that avoiding pregnancy over the age of 35, regular perinatal visits, early detection, and treatment of VVC may be the key protective factors for PROM in pregnant women with VVC.
PROM and infection have reciprocal causation. Infection could generate PROM, and after PROM, the pathogen may cause a retrograde infection. When a pregnancy is infected, the inflammatory response may produce enzymes which could degrade the membrane, giving rise to rupture (18). Zhang et al. (19) notes that Keap-1/Nrf2 signaling pathway activation following oxidative stress is associated with patients with PPROM (preterm premature rupture of membrane). A related study (20) shows that high Caspase-3, AIF, and low Bcl-2 expression are risk factors for PROM. Infants in the PROM group experienced higher rates of infection, asphyxia, and jaundice.
Advanced maternal age, defined as age ≥35 years at estimated date of delivery, is considered to lead to a higher incidence of obstetric complications and adverse pregnancy outcomes (21). Consistent to this guide, our investigations indicated that advanced maternal age was a risk factor for PROM in gravidas with VVC. It is known that vaginal micro-ecology is closely related to immunological status, and that the body's defense for fighting virulent hyphae gradually decreases with aging. Many studies indicate that advanced maternal age is a strong independent risk factor for adverse outcomes (22–24). Nowadays, women are delaying childbearing to pursue educational and career goals in greater numbers than ever before; as a result, advanced maternal age is a common phenomenon. Despite a fall in the birth rate of the general population of the United States over the past three decades, the birth rate for women aged 33–55 years has risen (25). Clinicians should educate both patients and the public that there is a real danger for mother and child if individuals choose to delay reproduction (26).
To our surprise, regular perinatal visits, had the greatest effect on PROM in pregnant women with VVC. Regular and efficient antenatal visits lead to a high percentage of good outcomes for mothers and infants (27), such that most women visit the hospital for scheduled check-ups during gestation. However, owing to an uneven distribution of medical resources and the uneven development of urban and rural areas in China, some pregnant women with low levels of education or that live in remote mountain areas are not aware of the significance of antenatal care. The government should increase the spread of prenatal care to these individuals. Clinicians are more sensitive to the observation of symptoms; therefore, regular perinatal visits could lead to symptom identification and thus prevent the development of adverse events. Abnormal vaginal discharge has shown a significant association with the occurrence of PROM. Pregnant women who had an abnormal vaginal discharge are more likely to develop PROM (28, 29). Abnormal vaginal discharge is indicative of infection, and infection causes inflammation of the membrane leading to subsequent rupture (30, 31). The symptoms of VVC in pregnancy were similar to those in the non-pregnant state: pruritus vulvae, leucorrhoea with a peculiar smell, flush on the vulva, discomfort, thick cottage-cheese–like discharge associated with vaginal and vulvar pruritus, pain, burning, erythema; in addition, there were quite a few asymptomatic infected individuals. Our study implied that symptoms of VVC were more prone to lead to PROM. A recent study (8) also indicates that abnormal vaginal discharge (adjusted OR = 5.30, 95% CI = 2.07–13.52) is relevant to PROM. At least one vaginal discharge examination is recommended during pregnancy for those women who have no complaints, and this examination is inspected preferably in the first trimester (12). Once VVC is found, it should be treated without delay. The latest WHO guidelines on the management of vaginal discharge (32) recommend that a single dose (oral or vaginal) of azole is a simple and the best treatment for VVC. Here, we again emphasize the importance of antenatal care. Only regular visits could ensure identification and treatment in a timely manner.
Furthermore, history of VVC before pregnancy was also an essential factor for PROM. VVC is a public health problem, vaginal dysbacteriosis and hypoimmunity are the most common pathogenesis of VVC (33). Pregnant women have a 2-fold increase in the prevalence of vaginal colonization by candida species compared with non-pregnant women (2). One study reveals that the prevalence of VVC in pregnant women is 36.5% (34). During pregnancy, the balance of vaginal flora is easily disrupted and disequilibrium is triggered. Because of this susceptible constitution, attention should be paid to those pregnant women with a history of VVC before pregnancy. On the basis of this systematic review (5), recurrent VVC probably affects more than 130 million women in any given year, with a global annual prevalence of 3,871 per 100 000 females. This damaging effect of VVC should be made widely known. In clinical work, clinicians need to attach importance to the past medical history, and medical records should be regarded as essential information.
Bacterial vaginitis is common and caused by a disruption of the microbiological environment in the lower genital tract. In the US, the reported prevalence of bacterial vaginitis among pregnant women ranges from 5.8 to 19.3% (35). Bacterial vaginitis during pregnancy has been associated with adverse obstetrical outcomes including preterm delivery, early miscarriage, postpartum endometritis, and low birth weight (36). Here, our findings showed that bacterial vaginitis increased the risk of PROM for pregnant women with VVC; this may be owing to the concurrent effect, i.e., that bacterial vaginitis and VVC accelerate an inflammatory response. Thus, gravidas with VVC and bacterial vaginitis were susceptible to PROM.
Moreover, during the review of previous literature, some potential risk factors, such as, education level, BMI before pregnancy, malpresentation, and polyhydramnios showed a relationship with PROM. Education in this matter could protect against infection (37).One study associated with assisted reproductive technology observes that intracytoplasmic sperm injection and elevated BMI increase the risk of PROM (38); furthermore, polyhydramnios may result in PROM (39). In addition, Assefa et al. (40) found that gravida with a history of PROM were more prone to develop PROM. Nevertheless, when confounding factors were added, above all of these were not considered in the nomogram lastly.
This PROM risk prediction tool is concise and explicit, and assist clinicians with the early identification of patients at high risk of PROM. The covariates are objective indicators, but not subjective indicators. Moreover, the included information in this nomogram is for almost zero cost.
Lyu et al. (41) provided a model for predicting PPROM based on laboratory data, such as white blood cells, granulocytes, lymphocytes, and neutrophil lymphocyte ratio. Malchi et al. (42) implied that vaginal fluid urea and creatinine were indicators of PROM. Zhan et al. (43) found that routine blood tests were a good indicator for predicting PROM, and Liang et al. (44) suggested that a routine urine test had partial predictive value for PROM. These methods of predicting PROM require collection of blood or urine samples at the time of occurrence of PROM, not prior. In our study, the nomogram is calculated based on existing medical history, allowing prediction of PROM before it happens. Additionally, based on this prediction model, early interventions such as advice of regular perinatal examination and early detection and treatment of VVC will contribute to control the occurrence of PROM.
There were several limitations of our current study. First, the findings need to be externally evaluated in a greater number of pregnant women with VVC. In the future, larger prospective research involving multiple centers, as well as a larger number of patients, should be undertaken with longer periods of follow-up, to validate and improve the nomogram. Secondly, due to the limited number of samples, we did not study the PPROM group separately. PPROM is highly correlated with severe outcomes, and deserves to be investigated further. Certainly, PPROM population will be extracted in our following study.
This study developed a novel nomogram that was relatively accurate in assisting clinicians to assess the risk of PROM in pregnant women with VVC. Age, regular perinatal visits, history of VVC before pregnancy, symptoms with VVC, cured of VVC during pregnancy, and bacterial vaginitis were the factors closely related to PROM in this nomogram. Candida species, maternal and neonatal outcomes, and mechanisms may be the future research directions. In addition, with the development of technology, optical coherence tomography may be a potential tool in the prediction of PROM (45).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethical Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
LY, JG, and SL: project development. LY, HW, and YL: data collection. HW, JG, and XL: data procession. LY and CZ: manuscript writing. SL: manuscript editing. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the following funding agencies: the program of National Natural Science Foundation of China (Grant No. 81904239), the innovation and strength program of the First Affiliated Hospital of the University of Chinese Medicine (Grant No. 2019QN11), the program of Guangzhou Science and Technology Bureau (Grant No. 202102020541).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Waters TP, Mercer B. Preterm prom: prediction, prevention, principles. Clin Obstet Gynecol. (2011) 54:307–12. doi: 10.1097/GRF.0b013e318217d4d3
2. Sobel JD. Vulvovaginal candidosis. Lancet. (2007) 369:1961–71. doi: 10.1016/S0140-6736(07)60917-9
3. Sobel JD. Vaginal infections in adult women. Med Clin North Am. (1990) 74:1573–602. doi: 10.1016/S0025-7125(16)30496-5
4. Foxman B, Muraglia R, Dietz JP, Sobel JD, Wagner J. Prevalence of recurrent vulvovaginal candidiasis in 5 european countries and the united states: results from an internet panel survey. J Low Genit Tract Dis. (2013) 17:340–5. doi: 10.1097/LGT.0b013e318273e8cf
5. Denning DW, Kneale M, Sobel JD, Rautemaa-Richardson R. Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect Dis. (2018) 18:e339–47. doi: 10.1016/S1473-3099(18)30103-8
6. Wheeler ML, Oyen ML. Premature rupture of membranes and severe weather systems. Front Physiol. (2020) 11:524. doi: 10.3389/fphys.2020.00524
7. Dayal S, Hong PL. Premature Rupture of Membranes. (2021). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK532888/ (accessed October 30, 2021).
8. Addisu D, Melkie A, Biru S. Prevalence of preterm premature rupture of membrane and its associated factors among pregnant women admitted in debre tabor general hospital, north west ethiopia: institutional-based cross-sectional study. Obstet Gynecol Int. (2020) 2020:4034680. doi: 10.1155/2020/4034680
9. Tchirikov M, Schlabritz-Loutsevitch N, Maher J, Buchmann J, Naberezhnev Y, Winarno AS, et al. Mid-trimester preterm premature rupture of membranes (pprom): etiology, diagnosis, classification, international recommendations of treatment options and outcome. J Perinat Med. (2018) 46:465–88. doi: 10.1515/jpm-2017-0027
10. McGregor JA, French JI, Seo K. Premature rupture of membranes and bacterial vaginosis. Am J Obstet Gynecol. (1993) 169:463–6. doi: 10.1016/0002-9378(93)90342-G
11. Karat C, Madhivanan P, Krupp K, Poornima S, Jayanthi NV, Suguna JS, et al. The clinical and microbiological correlates of premature rupture of membranes. Indian J Med Microbiol. (2006) 24:283–5. doi: 10.1016/S0255-0857(21)02290-8
12. Qi H, Yang H. Department of Obstetrics and Gynecology Chinese Medical Association. The guideline of preconception care and prenatal care. Chin J Obstetr Gynecol. (2018) 53:7–13. doi: 10.3760/cma.j.issn.0529-286567X.2018.01.003287
13. Sauerbrei W, Royston P, Binder H. Selection of important variables and determination of functional form for continuous predictors in multivariable model building. Stat Med. (2007) 26:5512–28. doi: 10.1002/sim.3148
14. Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Softw. (2010) 33:1–22. doi: 10.18637/jss.v033.i01
15. Xing J, Min L, Zhu S, Zhang H, Zhao Y, Li H, et al. Factors associated with gastric adenocarcinoma and dysplasia in patients with chronic gastritis: a population-based study. Chin J Cancer Res. (2017) 29:341–50. doi: 10.21147/j.issn.1000-9604.2017.04.07
16. Pencina MJ, D'Agostino RB. Overall c as a measure of discrimination in survival analysis: model specific population value and confidence interval estimation. Stat Med. (2004) 23:2109–23. doi: 10.1002/sim.1802
17. Xia H, Li X, Li X, Liang H, Xu H. The clinical management and outcome of term premature rupture of membrane in east china: results from a retrospective multicenter study. Int J Clin Exp Med. (2015) 8:6212–7.
18. van Teeffelen AS, van der Ham DP, Oei SG, Porath MM, Willekes C, Mol BW. The accuracy of clinical parameters in the prediction of perinatal pulmonary hypoplasia secondary to midtrimester prelabour rupture of fetal membranes: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. (2010) 148:3–12. doi: 10.1016/j.ejogrb.2009.10.001
19. Zhang W, Li M, Li N, Liu Z. Regulation of keap-1/nrf2 signaling pathway is activated by oxidative stress in patients with premature rupture of membranes. Med Sci Monit. (2020) 26:e921757. doi: 10.12659/MSM.921757
20. Negara KS, Suwiyoga K, Sudewi R, Astawa NM, Arijana G, Tunas K, et al. The role of caspase-dependent and caspase-independent pathways of apoptosis in the premature rupture of the membranes: a case-control study. Int J Reprod Biomed. (2020) 18:439–48. doi: 10.18502/ijrm.v13i6.7285
21. Radhakrishnan SA. Advanced maternal age (ama). Asian J Nurs Educ Res. (2016) 6:138. doi: 10.5958/2349-2996.2016.00027.6
22. Pinheiro RL, Areia AL, Mota PA, Donato H. Advanced maternal age: adverse outcomes of pregnancy, a meta-analysis. Acta Med Port. (2019) 32:219–26. doi: 10.20344/amp.11057
23. Glick I, Kadish E, Rottenstreich M. Management of pregnancy in women of advanced maternal age: improving outcomes for mother and baby. Int J Womens Health. (2021) 13:751–9. doi: 10.2147/IJWH.S283216
24. Getaneh T, Asres A, Hiyaru T, Lake S. Adverse perinatal outcomes and its associated factors among adult and advanced maternal age pregnancy in northwest ethiopia. Sci Rep. (2021) 11:14072. doi: 10.1038/s41598-021-93613-x
25. Martin JA, Hamilton BE, Osterman MJ, Curtin SC, Matthews TJ. Births: final data for 2012. Natl Vital Stat Rep. (2013) 62:1–68.
26. Sauer MV. Reproduction at an advanced maternal age and maternal health. Fertil Steril. (2015) 103:1136–43. doi: 10.1016/j.fertnstert.2015.03.004
27. Workineh Y, Birhanu S, Kerie S, Ayalew E, Yihune M. Determinants of premature rupture of membrane in southern ethiopia, 2017: case control study design. BMC Res Notes. (2018) 11:927. doi: 10.1186/s13104-018-4035-9
28. Kaye D. Risk factors for preterm premature rupture of membranes at mulago hospital, kampala. East Afr Med J. (2001) 78:65–9. doi: 10.4314/eamj.v78i2.9090
29. Melorose J, Perroy R, Careas S. Cervicovaginal Infection During Pregnancy and Its Relation to Preterm Pre-Labour Rupture of Membranes. (2012). Available online at: https://www.mendeley.com/catalogue/d7438a97-9f45-30ed-86f5-fcf0b0e5a50d/ (accessed October 30, 2021).
30. Zhu J, Ma C, Luan X, Li J, Peng F, Huang L. Inflammasome components and adamts4 in premature rupture of membranes. Mol Med Rep. (2021) 23:1. doi: 10.3892/mmr.2020.11740
31. Zhu J, Ma C, Zhu L, Li J, Peng F, Huang L, et al. A role for the nlrc4 inflammasome in premature rupture of membrane. Plos One. (2020) 15:e237847. doi: 10.1371/journal.pone.0237847
32. Sherrard J, Wilson J, Donders G, Mendling W, Jensen JS. 2018 european (iusti/who) international union against sexually transmitted infections (iusti) world health organisation (who) guideline on the management of vaginal discharge. Int J Std Aids. (2018) 29:1258–72. doi: 10.1177/0956462418785451
33. Sobel JD. Recurrent vulvovaginal candidiasis. Am J Obstet Gynecol. (2016) 214:15–21. doi: 10.1016/j.ajog.2015.06.067
34. Konadu DG, Owusu-Ofori A, Yidana Z, Boadu F, Iddrisu LF, Adu-Gyasi D, et al. Prevalence of vulvovaginal candidiasis, bacterial vaginosis and trichomoniasis in pregnant women attending antenatal clinic in the middle belt of ghana. BMC Preg Childbirth. (2019) 19:341. doi: 10.1186/s12884-019-2488-z
35. Kenyon C, Colebunders R, Crucitti T. The global epidemiology of bacterial vaginosis: a systematic review. Am J Obstet Gynecol. (2013) 209:505–23. doi: 10.1016/j.ajog.2013.05.006
36. Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, Caughey AB, et al. Screening for bacterial vaginosis in pregnant persons to prevent preterm delivery: us preventive services task force recommendation statement. JAMA. (2020) 323:1286–92. doi: 10.1001/jama.2020.2684
37. Na D, Li W, Zhao E, Chan W, Zhou H. Risk factors for candida infection of the genital tract in the tropics. Afri Health Ences. (2014) 14:835–9. doi: 10.4314/ahs.v14i4.10
38. Shiqiao H, Bei X, Yudi G, Lei J. Assisted reproductive technology is associated with premature rupture of membranes. J Matern Fetal Neonatal Med. (2021) 34:555–61. doi: 10.1080/14767058.2019.1610738
39. Hwang DS, Bordoni B. Polyhydramnios. (2021). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK562140/ (accessed October 30, 2021).
40. Assefa NE, Berhe H, Girma F, Berhe K, Berhe YZ, Gebreheat G, et al. Risk factors of premature rupture of membranes in public hospitals at mekele city, tigray, a case control study. BMC Preg Childbirth. (2018) 18:386. doi: 10.1186/s12884-018-2016-6
41. Lyubomirskaya K, Krut Y, Sergeyeva L, Khmil S, Lototska O, Petrenko N, et al. Preterm premature rupture of membranes: prediction of risks in women of zaporizhzhia region of ukraine. Pol Merkur Lekarski. (2020) 48:399–405.
42. Malchi F, Abedi P, Jahanfar S, Talebi F, Faal S, Zahedian M. Vaginal fluid urea and creatinine as indicators of premature rupture of membranes: a systematic review. Reprod Sci. (2021) 28:1–11. doi: 10.1007/s43032-020-00271-x
43. Zhan F, Zhu S, Liu H, Wang Q, Zhao G. Blood routine test is a good indicator for predicting premature rupture of membranes. J Clin Lab Anal. (2019) 33:e22673. doi: 10.1002/jcla.22673
44. Liang H, Xie Z, Liu B, Song X, Zhao G. A routine urine test has partial predictive value in premature rupture of the membranes. J Int Med Res. (2019) 47:2361–70. doi: 10.1177/0300060519841160
Keywords: premature rupture of membrane, nomogram, predictor, vulvovaginal candidiasis, pregnant women
Citation: Yang L, Wang H, Li Y, Zeng C, Lin X, Gao J and Luo S (2021) Development of a Novel Nomogram for Predicting Premature Rupture of Membrane in Pregnant Women With Vulvovaginal Candidiasis. Front. Med. 8:717978. doi: 10.3389/fmed.2021.717978
Received: 12 June 2021; Accepted: 13 October 2021;
Published: 15 November 2021.
Edited by:
Zaleha Abdullah Mahdy, National University of Malaysia, MalaysiaReviewed by:
Idayu Badilla Idris, National University of Malaysia, MalaysiaNurul Basri, Universiti Putra Malaysia, Malaysia
Copyright © 2021 Yang, Wang, Li, Zeng, Lin, Gao and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Gao, Z2pma3RzQGhvdG1haWwuY29t; Songping Luo, Z3luc3BsdW9AaG90bWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship