 Elodia Nataly Díaz-De la Cruz1
Elodia Nataly Díaz-De la Cruz1 José Ignacio Cerrillos-Gutiérrez2Andrés García-Sánchez1
José Ignacio Cerrillos-Gutiérrez2Andrés García-Sánchez1 Carlos Gerardo Prado-Nevárez2
Carlos Gerardo Prado-Nevárez2 Jorge Andrade-Sierra2Basilio Jalomo-Martínez2Adriana Banda-López2Enrique Rojas-Campos2
Jorge Andrade-Sierra2Basilio Jalomo-Martínez2Adriana Banda-López2Enrique Rojas-Campos2 Alejandra Guillermina Miranda-Díaz1*
Alejandra Guillermina Miranda-Díaz1*- 1Department of Physiology, University Health Sciences Center, Universidad de Guadalajara, Guadalajara, Mexico
- 2Department of Nephrology and Organ Transplant Unit, National Western Medical Centre, Mexican Institute of Social Security, Specialties Hospital, Guadalajara, Mexico
Patients with end-stage renal disease (ESRD) present alterations in mineral and bone metabolism. Hyperphosphatemia in ESRD is considered an independent risk factor for cardiovascular disease (CVD), increasing morbidity, and mortality. Sevelamer hydrochloride is a calcium-free, non-absorbable phosphate-chelating polymer. Calcium carbonate chelator is helpful in controlling serum phosphate levels. There is insufficient information on the influence of sevelamer hydrochloride and calcium carbonate on the behavior of oxidative stress (OS) markers and inflammation in patients on hemodialysis (HD). A randomized open clinical trial was carried out on patients to evaluate sevelamer hydrochloride and calcium carbonate influence at 6 months of study follow-up. Levels of oxidants (LPO, NO, and 8-isoprostanes), antioxidants (SOD and TAC), oxidative DNA damage (8-OHdG and hOGG1), pro-inflammatory cytokines (IL-6 and TNF-α), and inflammation markers (ferritin and C-reactive protein) were measured with colorimetric and ELISA methods. We found a significant increase in oxidants LPO and NO, and antioxidants SOD and TAC, and downregulation of IL-6 and TNF-α. Ferritin decrease at 6 months follow-up in the sevelamer hydrochloride group. Increase in C-reactive protein was found in the group of patients treated with calcium carbonate. In conclusion, we found an oxidative state imbalance with increase in LPO and NO oxidants. The activity of the antioxidant enzymes (SOD and TAC) was also found to increase, suggesting a compensatory effect in the face of increase in oxidants. The same phenomenon was observed with increase in the oxidative damage marker to DNA and the increase in the DNA repair enzyme, suggesting a compensatory effect. Pro-inflammatory cytokines were predominantly downregulated by TNF-α in the group that ingested sevelamer hydrochloride in the final determination at 6 months of follow-up. Serum ferritin levels decreased significantly at the end of follow-up in patients on HD in the sevelamer hydrochloride group. The management of hyperphosphatemia with sevelamer hydrochloride appears to have obvious anti-inflammatory and antioxidant benefits.
Introduction
Disorders of mineral and bone metabolism are frequent complications in patients with end-stage renal disease (ESRD). Hyperphosphatemia is an inevitable consequence of ESRD, the presence of which is associated with increased morbidity and mortality (1). Oxidative stress (OS) is characterized by an imbalance between decrease in antioxidant defense mechanisms and increase in oxidant products. OS appears in early stages of chronic kidney disease (CKD), progresses along with worsening kidney failure, and is aggravated by the hemodialysis (HD) process. Observational studies have reported that hyperphosphatemia is an independent risk factor for cardiovascular disease (CVD) capable of increased mortality in patients on dialysis (2). Control of serum phosphorus (Pi) is key to improving clinical outcomes for patients on dialysis. The predominant drug treatment for hyperphosphatemia has been calcium-based phosphate binders (calcium carbonate or calcium acetate). However, calcium salts are related to arterial calcification (3). New phosphate binders have made it possible to dispense with calcium in the formulation (4). Sevelamer hydrochloride is a non-absorbable, calcium-free phosphate-chelating polymer that has been available since 1998 (5). Sevelamer hydrochloride is an anion exchange resin, allowing it to exchange negatively charged ions. Sevelamer hydrochloride has a high affinity for phosphate ions and exerts its therapeutic action in the intestine, exchanging chloride for phosphate and forming an insoluble compound that is excreted in feces (6).
Figure 1 briefly shows the binding mechanism of sevelamer hydrochloride and calcium carbonate with ingested Pi. Some studies have reported potential benefits of the use of sevelamer hydrochloride. However, there are insufficient data to establish the superiority of phosphate binders without calcium content over those containing calcium with CVD development (7). Sevelamer hydrochloride helps prevent calcium overload, reduces hyperphosphatemia, and translates into better clinical results. Sevelamer hydrochloride is associated with better survival in patients on HD (8). Experimental, observational, and clinical trials have shown sevelamer hydrochloride to have pleiotropic effects beyond the control of hyperphosphatemia. Sevelamer hydrochloride acts on inflammation, OS, lipid profile, atherogenesis, vascular calcification, and endothelial dysfunction, and reduces uremic toxins (9, 10). Patients on HD have a high risk of mortality from all causes and cardiovascular events. Excessive OS and chronic inflammation emerge as new contributors of accelerated atherosclerosis and elevated mortality in ESRD. Patients on HD show an increase in free radicals due to retention of uremic toxins, reduction in antioxidants, activation of leukocytes, infectious processes, and presence of comorbidities (11). The potential benefits of sevelamer hydrochloride to decrease inflammation and OS markers need to be studied (12).
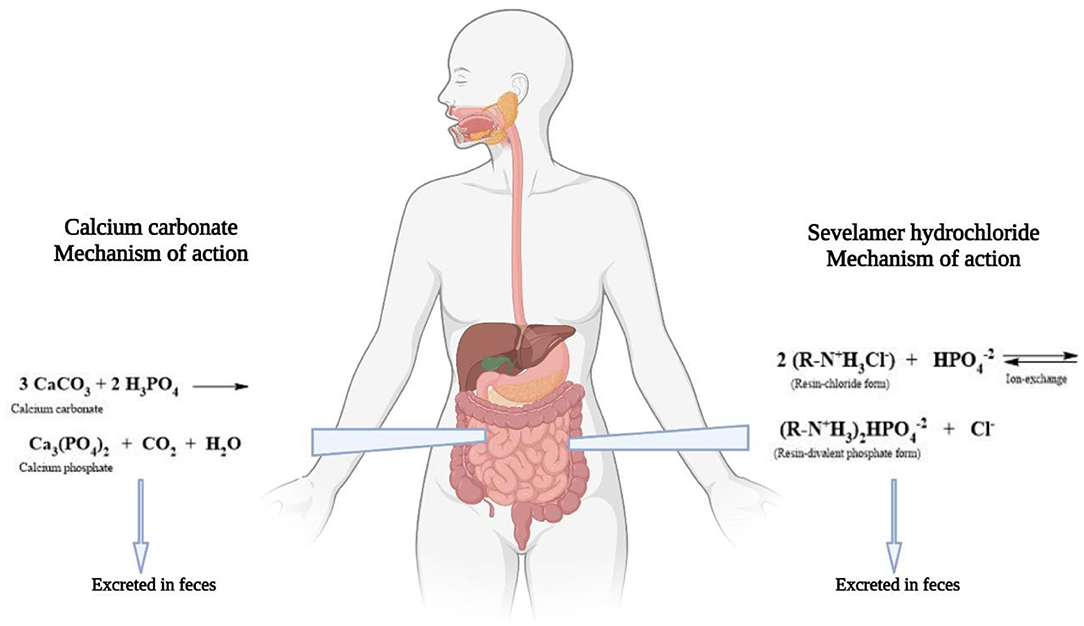
Figure 1. Sevelamer hdyrochloride and calcium carbonate mechanism. Binding of sevelamer hydrochloride and calcium carbonate with phosphate. Right side shows the ion exchange between the resin and the phosphate. Left side shows the reaction between calcium carbonate and phosphate.
The purpose of the study was to evaluate the influence of sevelamer hydrochloride and calcium carbonate on OS markers and inflammation in patients on HD at 6 months of follow-up.
Patients and Methods
Patients
A randomized open clinical trial was carried out on patients to evaluate sevelamer hydrochloride and calcium carbonate influence at 6 months of study follow-up. An open randomized clinical trial was designated, because it was not possible to mask the drugs. The medications were obtained through a prescription that was exchanged at the pharmacy by the patient himself. The initial doses of sevelamer hydrochloride were two tablets of 800 mg every 12 h. It was necessary to adjust the dose (±1 tablet) each month to achieve a target serum Pi of 5 mg/dl and considering drug tolerance. Serum Pi was monitored each month to determine the need for dose adjustment using a colorimetric method for its determination. The doses administered at the end of the study were 1,600, 2,400, and 3,200 mg. The titration of the drug was gradual and according to each patient requirement (13).
Randomization and treatment allocation were based on simple randomization using the Microsoft Excel software that generates random numbers. Male and female patients aged 18–60 years were included. Medications were administered for comorbidities, for arterial hypertension (nifedipine, metoprolol, losartan), for DM (insulin), for anemia (folic acid, erythropoietin). The diet of ESRD patients includes limiting fluids, consuming a low-protein diet, and reducing their intake of salt, potassium, Pi, and other electrolytes. In ESRD patients it is important to consume enough calories to avoid losing weight. No dietary supplements were administered. All patients who have ESRD, with GFR < 10 ml/min/1.73 m2, were subjected to three HD sessions per week with the same type of filter without the possibility of determining albuminuria. The patients were attended in the HD Unit of the Department of Nephrology of the High Specialty Medical Unit of the Mexican Institute of Social Security (IMSS) in Guadalajara, Jalisco, Mexico. Patients who ingested antioxidants (vitamins E and C) 3 months before the study and patients with clinical or biochemical data of an infectious process were not included. Patients who withdrew informed consent, with <80% adherence to treatment and patients with adverse drug events were excluded from the study.
Data Collection
Sixty-four patients were enrolled, and two intervention groups with 32 patients were formed. One group was composed of patients treated with sevelamer hydrochloride, and the other was made up of patients treated with calcium carbonate. Treatment adherence was verified by the investigator in charge of prescribing the drug to each patient. Adherence was determined by recording the drug supply of a pharmacy according to the stipulated time and loaded into the file of each patient. Body mass index (BMI) and treatment group were recorded. Biochemical data were obtained the first day of treatment immediately before starting HD and at 6 months of follow-up: hemoglobin, urea, uric acid, cholesterol, triglycerides, albumin, urea, serum creatinine, and uric acid, serum electrolytes (sodium, potassium, chlorine, Pi, calcium, and magnesium), ferritin, iron saturation, bicarbonate, C-reactive protein (CRP), vitamin D, pH, and parathyroid hormone (PTH). Venous blood samples, 5 ml, were collected in a dry tube and 5 ml in a tube with 7.2 mg of dipotassium ethylene-diamine-tetra-acetic acid (K2 EDTA). The samples were centrifuged at 3,500 rpm for 10 min to obtain serum and plasma. Six months after starting treatment (sevelamer hydrochloride or calcium carbonate), blood samples were collected to compare the results. The aliquots obtained were stored at −80°C to analyze later inflammation markers, oxidants, antioxidants, and oxidative damage to DNA.
OS Markers
Lipoperoxidation (LPO) Products
The levels of LPO in plasma were measured using an FR22 assay kit (Oxford Biomedical Research Inc., Oxford, MI, United States) and according to the instructions of the manufacturer.
8-iso Prostaglandin F2α 8-Isoprostanes (8-IP)
An immunoassay reagent kit from Abcam Company® (Cambridge, England) was used according to the instructions of the manufacturer.
Nitric Oxide (NO)
Before determining NO levels, the serum samples were deproteinized by adding 6 mg of zinc sulfate to 400 μl of the sample vortex for 1 min, and the samples were centrifuged at 10,000 × g for 10 min at 4°C. The determination of NO was carried out per the kit (NB98; Oxford Biochemical Research Inc., Oxford, MI, United States).
Antioxidants
Superoxide Dismutase (SOD)
The instructions of the kit manufacturer (SOD No. 706002; Cayman Chemical Company®, Ann Arbor, Michigan, USA) were followed to measure SOD activity. The levels are reported in U/ml.
Total Antioxidant Capacity (TAC)
Evaluations of total antioxidant capacity (TAC) were performed according to the instructions of the kit manufacturer (Total Antioxidant Power Kit, No. TA02.090130; Oxford Biomedical Research®, Oxford, MI, United States).
Marker of Oxidative DNA Damage
The serum levels of 8-hydroxy-2′-deoxyguanosine (8-OHdG) were measured using an 8-hydroxy-2-deoxyguanosine ELISA kit ab201734 (Abcam®, Cambridge, MA, United States).
DNA Repair Enzyme—Oxoguanine Glycosylase
It was performed by the manufacturer of human 8-oxoguanine DNA glycosidase (hOGG1) ELISA kit no. MBS702793, MyBioSource® (San Diego, USA).
Pro-inflammatory Cytokines
TNF-α and IL-6
The sandwich ELISA method of the commercial 900-K25 and 900-K16 kit suggested by the manufacturer Peprotech (New Jersey, USA) was followed. The absorbances of the wells were recorded at 405 nm with a correction of 650 nm.
Ferritin and C-Reactive Protein (CRP)
They were determined by immuno-turbidimetry. Antibody-coated latex particles were agglutinated by ferritin or CRP present in the patient sample. The agglutination process caused an absorbance change proportional to the concentration of the inflammation marker in the sample, and the concentration in the sample was determined by comparison with a standard.
Statistical Analysis
Sample size calculation was performed by comparing two means formula (14). In the available literature, we did not find longitudinal studies on the effect of sevelamer on OS markers. Therefore, we used as a reference the variation of TNF-α in patients on HD treated with sevelamer reported by Peres et al. (13). There were no losses from the included population. The patients underwent HD three times a week with the same type of filter; no intention-to-treat analysis was required. The results are presented in measures of central tendency and dispersion for quantitative variables. Qualitative variables are shown in frequencies and percentages. The Kolmogorov–Smirnov test was performed to determine the normality of the data. For intra-group differences, the Wilcoxon rank test was performed according to the distribution obtained. Mann–Whitney U-test or Student's t-test was performed on independent samples for treatment inter-group differences. ANOVA or Kruskal-Wallis test was performed for dose inter-group differences. All results with a value of p ≤ 0.05 were documented as statistically significant.
Ethical Considerations
The study was followed under the ethical principles for medical research in human beings stipulated in the declaration of Helsinki 64th General Assembly, Fortaleza Brazil, October 2013, and the Standards of Good Clinical Practice according to the guidelines of the International Conference on Harmonization. Under the General Health Law's provisions following the Regulations of the General Health Law on Research for Health Article 17 of Mexico, the study corresponds to category III. All the patients signed the Low Information Consent in the presence of witnesses. The study was evaluated and approved by the Local Ethics and Research Committee at the Centro Médico Nacional de Occidente, Instituto Mexicano del Seguro Social (R-2021-1301-063).
Results
Sixty-four patients were included, 32 in the sevelamer hydrochloride group and 32 patients in the calcium carbonate group. Thirty-eight female and 26 male patients were included. Body weight was similar in both groups, 64.79 ± 19.1 kg of patients treated with sevelamer hydrochloride and 63.55 ± 22.46 kg of those treated with calcium carbonate. The time in the HD program was also similar, 8.06 ± 4.78 years in the sevelamer hydrochloride group and 7.05 ± 5.06 years in the group treated with calcium carbonate. In the sevelamer hydrochloride group, a normal BMI was found in 64.5% of the patients, 12.9% were overweight, and 22.6% were obese. In the calcium carbonate group, the BMI was normal in 71.4%, 14% of the patients were overweight, and 14.3% were obese. 74.2% of the patients in the sevelamer hydrochloride group and 71.4% of the patients treated with calcium carbonate had diabetes mellitus (DM). 32.3% of the patients treated with sevelamer hydrochloride and 19% of those treated with calcium carbonate had arterial hypertension (AH) (Table 1).
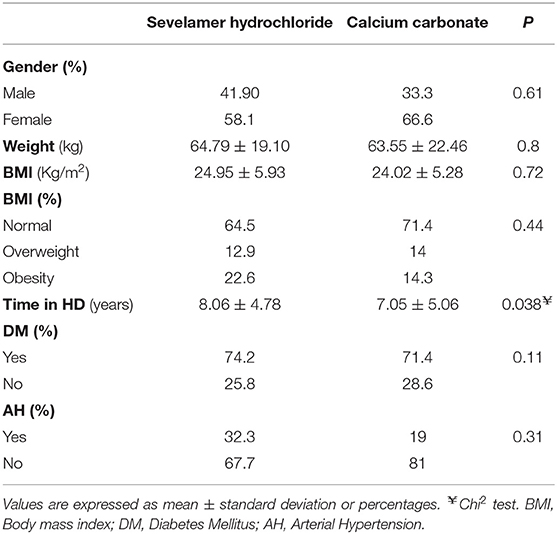
Table 1. Baseline anthropometric data.
Table 2 shows the causes of kidney failure in both treatment groups. The unknown cause is highlighted.
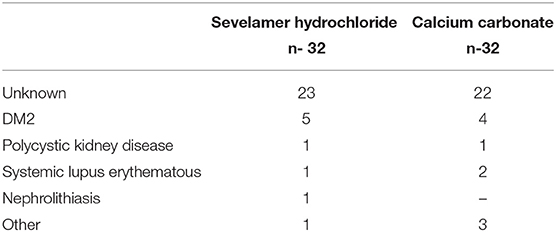
Table 2. ESRD causes.
Biochemical Data
The baseline hemoglobin levels in both groups were similar, 10.5 ± 1.63 mg/dl in the sevelamer hydrochloride group and 10.14 ± 2.23 mg/dl in the calcium carbonate group. In the determination at six months of follow-up, the hemoglobin levels in the sevelamer hydrochloride group increased to 12.15 ± 1.93 mg/dl (p = 0.001) without observing changes in those who received calcium carbonate. 10.85 ± 2.57 mg/dl (p = 0.23). Ferritin levels decreased significantly in the sevelamer hydrochloride group, 201.67 ± 60.39 ng/ml with respect to the 396.24 ± 709.77 ng/ml in the calcium carbonate group (p = 0.004). CRP levels showed an increase in both groups (Table 3).
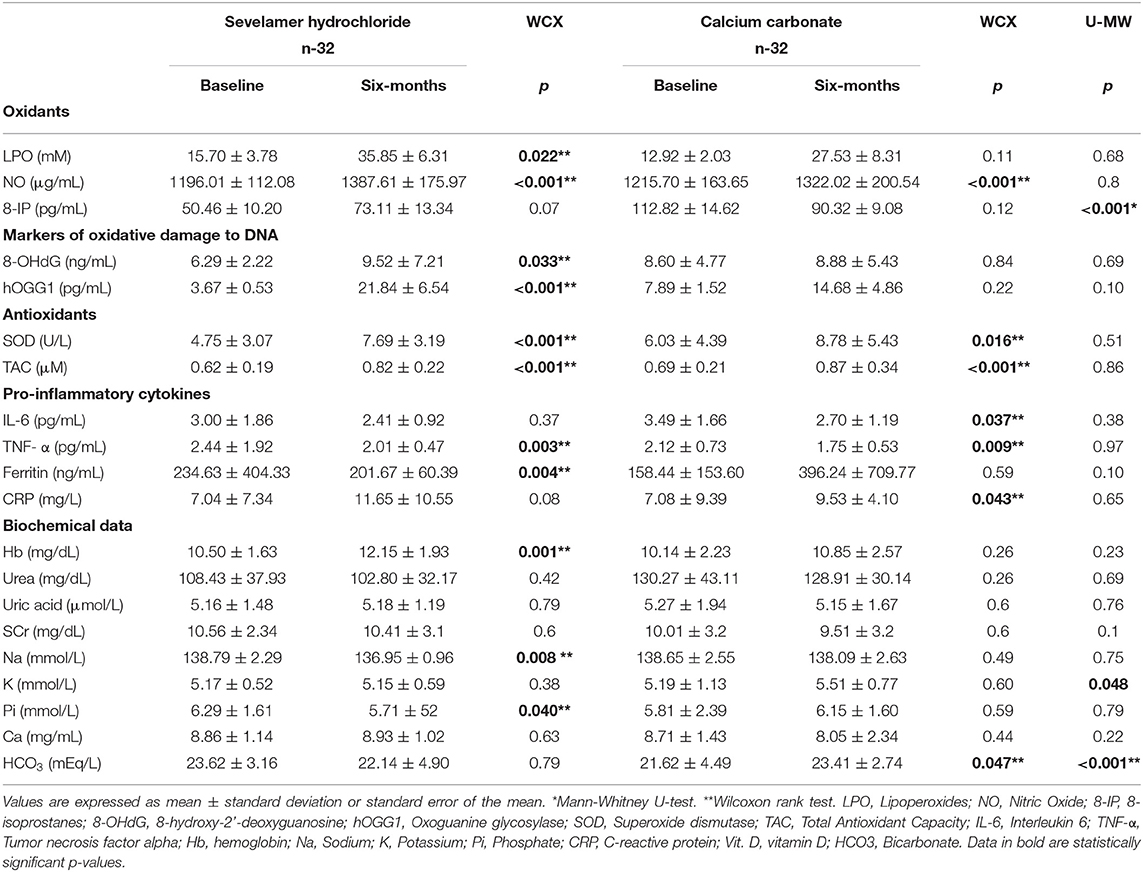
Table 3. Sevelamer hydrochloride or Calcium carbonate dose.
OS Markers
LPO, 8-IP, NO
The LPO levels increased significantly between the baseline levels 15.7 ± 3.79 mM and the final determination 35.85 ± 6.32 mM (p = 0.022) in the sevelamer hydrochloride group. The same behavior was observed in basal NO levels 1,196.01 ± 112.08 μg/ml compared with the increase found at the end of follow-up, 1,387.61 ± 175.97 μg/ml (p = 0.001). The group treated with calcium carbonate had similar results between the baseline and 6 months of treatment. The 8-IP levels in the sevelamer hydrochloride group were 50.46 ± 10.2 vs. 73.11 ± 13.34 pg/ml (p = 0.07) (Table 3).
Antioxidants
The activity of the SOD enzyme was found to be significantly increased in the final determination of those treated with sevelamer hydrochloride, 7.69 ± 3.19 U/L (p < 0.001) and with calcium carbonate, 8.78 ± 5.43 U/L (p = 0.016). The levels of TAC were significant increased at the end of the follow-up for the sevelamer hydrochloride (0.82 ± 0.22 μM, p < 0.001) and calcium carbonate, (0.87 ± 0.34 μM, p < 0.001) groups (Table 3).
Pro-inflammatory Cytokines
We found a significant decrease in the expression of the pro-inflammatory cytokine TNF-α between baseline levels, 2.44 ± 1.92 pg/ml, and the final result, 2.01 ± 1.47 pg/ml (p = 0.003), in patients treated with sevelamer hydrochloride. The same behavior was observed in those who received calcium carbonate between the expression of basal TNF-α, 2.12 ± 0.73 pg/ml, and final result, 1.75 ± 0.53 pg/ml (p = 0.009). Ferritin levels were decreased at the end of follow-up 201.67 ± 60.39 ng/ml (p = 0.04), in the patients who ingested sevelamer hydrochloride. CRP levels were increased in the patients treated with calcium carbonate, 10.66 ± 6.07 mg/L (p = 0.008) (Table 3).
Oxidative Damage to DNA
The expression of the oxidative DNA damage marker (8-OHdG) in the final determination increased, 9.52 ± 7.21 ng/ml (p = 0.033), compared with the baseline determination of 6.29 ± 2.22 ng/ml in the hydrochloride sevelamer group. The same behavior was observed with the DNA repair enzyme in the final determination, 21.84 ± 6.54 pg/ml (p < 0.001), of the patients treated with sevelamer hydrochloride compared with the baseline value of 3.67 ± 0.53 pg/ml. The group that ingested calcium carbonate did not change the levels between the baseline and final determination (Table 3).
Hemodialysis and Sevelamer Hydrochloride Dose
Three daily doses (1,600, 2,400, and 3,200 mg) of sevelamer hydrochloride were administered to the patients in the HD program. Patients who ingested 3,200 mg had a significant increase in LPO in the final determination of the study, 48.85 ± 42.79 mM (p = 0.011), compared with the baseline level of 9.18 ± 4.52 mM. NO levels were also increased in the final determination in patients who received 1,600 mg, 1,372.14 ± 177.5 μg/ml (p = 0.031), and 3,200 mg, 1,319.25 ± 158.35 μg/ml (p = 0.028). The DNA repair enzyme was found to be significantly increased in the final determination in patients who ingested 1,600 mg of sevelamer hydrochloride 17.74 ± 9.02 (p = 0.028).
The activity of the antioxidant enzyme SOD was significantly increased at 6 months of follow-up only in patients who ingested 1,600 mg of sevelamer hydrochloride 0.91 ± 0.25 μM (p = 0.047). TAC levels were found to be increased in the final determination in patients who ingested 1,600 mg, 0.91 ± 0.25 μM, (p = 0.004), and 3,200 mg, 0.85 ± 0.28 μM (p = 0.011) of sevelamer hydrochloride.
The expression of IL-6 decreased significantly in the final determination in those who ingested 1,600 mg, 2.3 ± 1.01 pg/ml (p = 0.03). The expression of TNF-α decreased at the end of the study in those who ingested 3,200 mg, 1.8 ± 0.54 pg/ml (p = 0.038). Hemoglobin significantly improved in the final determination in patients who ingested 1,600 mg, 12.13 ± 2.81 mg/day (p = 0.012), and 3,200 mg, 11.2 ± 1.63 mg/dl (p = 0.03) of sevelamer hydrochloride. Ferritin levels decreased significantly at the end of the study in those who ingested 1,600 mg, 190.99 ± 282.23 ng/ml, (p = 0.028), and 3,200 mg, 231.47 ± 154.03 ng/ml (p = 0.05) of sevelamer hydrochloride. The levels of CRP, 9.63 ± 7.36 mg/L (p = 0.043), and vitamin D, 28.7 ± 12.65 nmol/L (p = 0.018), increased at the end of the study in patients who ingested 1,600 mg of sevelamer hydrochloride (Table 4).
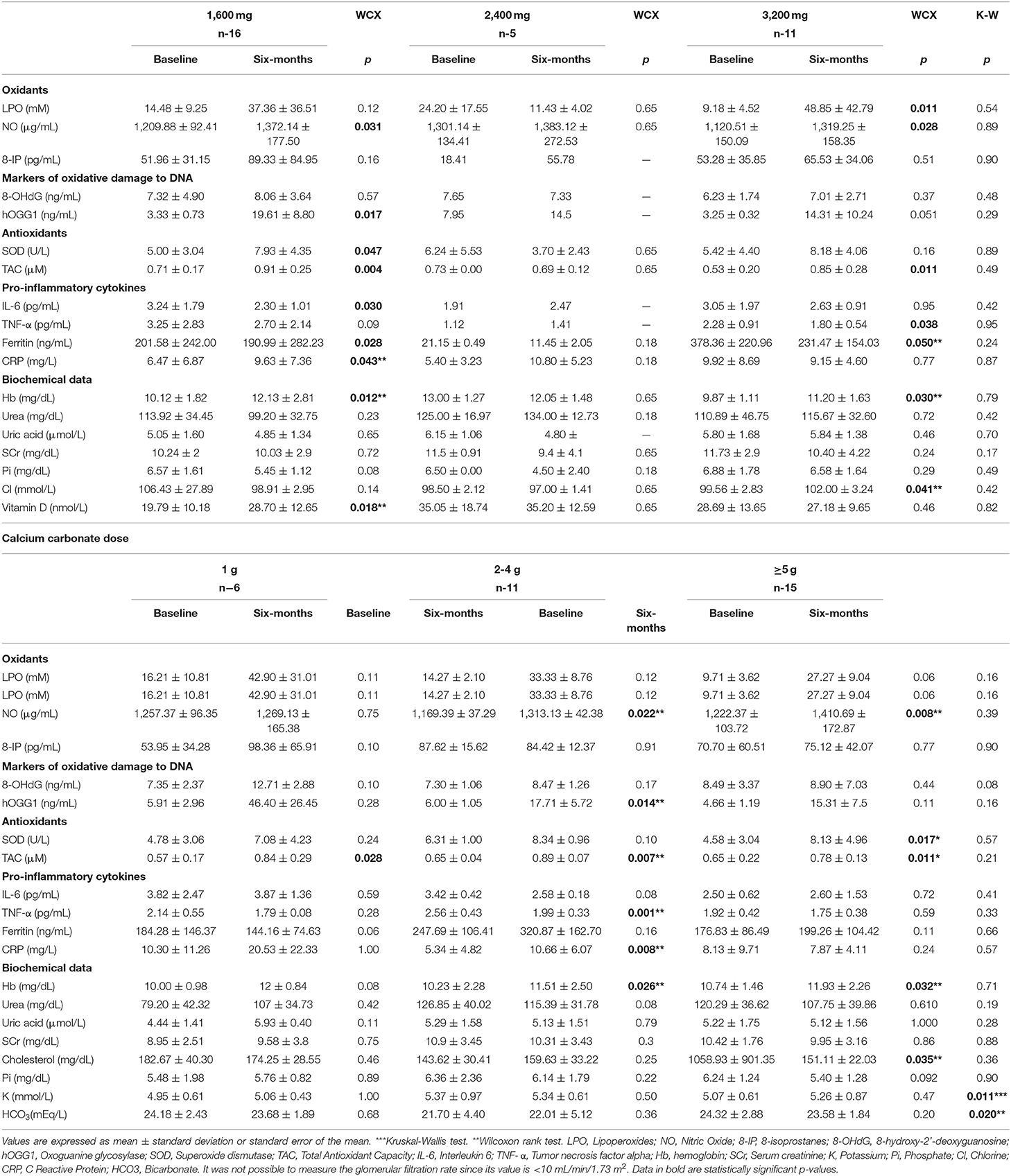
Table 4. Doses of sevelamer hydrochloride intervention Calcium carbonate dose.
Hemodialysis and Calcium Carbonate Dose
Patients who ingested calcium carbonate in daily doses of 2–4 g showed an increase in NO, 1,313.13 ± 42.38 μg/ml (p = 0.043), and even those who ingested ≥ 5 g per day had increased NO levels at 6 months of follow-up, 1,410.69 ± 172.87 μg/ml (p = 0.008). The DNA repair enzyme was significantly increased at the final determination in patients who ingested 2–4 g of calcium carbonate, 16.23 ± 5.78 pg/ml (p = 0.009).
The activity of the antioxidant enzyme SOD was significantly increased in those who ingested ≥ 5 g in the final determination of the study, 8.13 ± 4.96 U/L (p = 0.017). TAC was determined to be significantly increased at 6 months of follow-up in those who ingested 1 (0.84 ± 0.29 μM, p = 0.028), 2–4, (0.89 ± 0.07 μM, p = 0.007), and ≥ 5 g (0.7 8 ± 0.13 μM (p = 0.011).
The expression of TNF-α decreased significantly in the final determination of those who ingested 2–4 g, 1.99 ± 0.33 pg/ml (p = 0.001). Hemoglobin improved with the doses of 2–4 (11.51 ± 2.5 mg/dl) and ≥5 g (11.93 ± 2.26 mg/dl, p =0.032). CRP was significantly increased in patients who ingested 2–4 g at 6-month follow-up 10.66 ± 6.07 mg/L (p = 0.008). PTH was significantly increased in patients who ingested 1 g of calcium carbonate, 652.86 ± 217.31 pg/ml (p = 0.043) (Table 4).
Correlation Between Clinical Data and Markers of Inflammation and OS
Table 5 shows the moderate negative correlations found between SOD and PTH (rho = −0.052, p = 0.035), TAC and CRP (rho = −0.58, p = 0.017), for sevelamer hydrochloride. For calcium carbonate, moderate negative correlations were found for hOGG1 and HCO3 (rho = −0.68, p = 0.05), and LPO and pH (rho = −0.67, p = 0.035). Those with high correlations included 8-OHdG and urea (rho = −0.7, p = 0.024), and hOGG1 and K (rho = 0.7, p = 0.038) (Table 5).
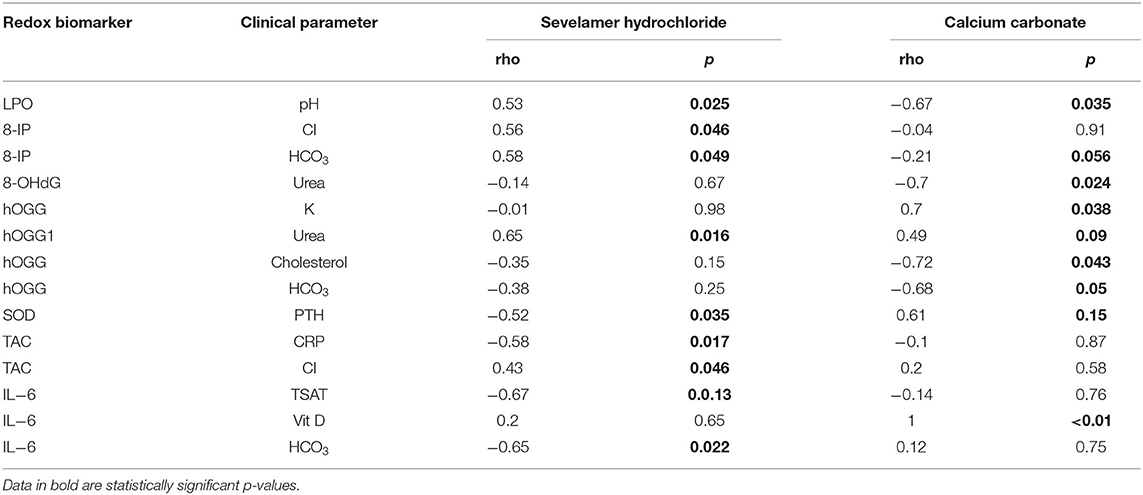
Table 5. Correlation between oxidative stress markers and clinical parameters.
Discussion
Most patients on HD are treated with phosphate binders to reduce serum levels and intestinal absorption of this mineral (15). It is known that dietary Pi restriction is not sufficient to maintain serum concentration within recommended levels. The management of hyperphosphatemia includes various chelators, such as sevelamer hydrochloride and calcium carbonate (16). Sevelamer has been observed in previously published research to reduce the absorption of advanced glycation products (AGE), bacterial toxins, and bile acids, suggesting that this mechanism reduces inflammatory, oxidative, and atherogenic stimuli in addition to its direct action of reducing serum Pi (17). Recently, some antioxidant and anti-inflammatory pleiotropic effects of sevelamer hydrochloride not associated with Pi depletion have been described (18). Elevated extracellular Pi causes mitochondrial OS related to mitochondrial hyperpolarization (19). The binding of Pi to sevelamer hydrochloride could explain the antioxidant mechanism by reducing mitochondrial OS. In this clinical study, the influence of sevelamer hydrochloride and calcium carbonate on markers of inflammation, oxidants, antioxidants, and oxidative DNA damage in patients on HD with 6 months of follow-up was evaluated (Figure 2).
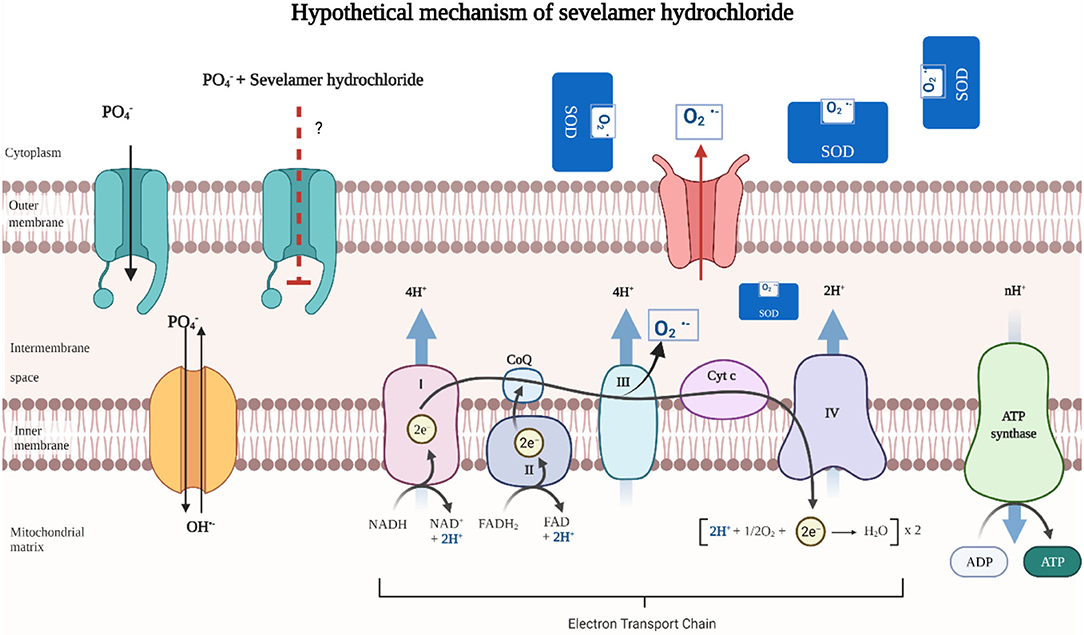
Figure 2. Hypothetical mechanism of sevelamer hydrochloride in oxidative stress (OS). Increase in extracellular Pi causes mitochondrial OS conditioned by mitochondrial hyperpolarization produced by a phosphate-hydroxyl exchange. Hyperpolarization stimulates the electron transport chain and increases the concentration of superoxide radicals by complex III. The binding of Pi to sevelamer hydrochloride could explain the antioxidant mechanism by reducing mitochondrial OS (20).
Calcium carbonate is the first-line treatment for lowering Pi in ESRD. However, its main effect is to avoid significant hyperphosphatemia without normalizing Pi serum levels. Adequate adherence to treatment with calcium carbonate avoids the uncontrolled rise of hyperphosphatemia (21).
Lipoperoxidation produces increased OS, leading to the formation of molecules such as aldehydes (malondialdehyde), and whose measurement is used to determine OS (22). HD can remove water-soluble, low molecular-weight LPO products. However, the HD process can also favor the increase in LPO depending on the time spent in the HD program (23). The prolonged stay of a patient in renal replacement therapy is considered a contributing factor to increasing inflammation and OS (24). In this study, the results at 6-months follow-up showed an increase in LPO in patients treated with the 3,200 mg dose of sevelamer hydrochloride.
NO is a molecule with a wide variety of fundamental physiological functions, such as maintenance of muscle tone. It is an intracellular messenger, a cytotoxic agent, and has a primordial effect on the vascular endothelium. NO has specific functions in the kidney, regulating hemodynamics, salt and water reabsorption, renin secretion, and tubule-glomerular feedback. Its bioavailability abnormalities are causally related to various cardiovascular and renal disorders (20). In patients with ESRD, there could be decreased NO synthesis due to kidney damage (25). The disturbed balance of NO is related to the imbalance of endothelin-1 (ET-1) (26). NO is involved in the pathogenesis of hypertension and rebound hypotension during the HD process (27). The female gender tends to have better kidney function and higher NO concentration (as usual) due to the action of estrogens (28). According to previous studies, the bioavailability of NO in patients with DM is low (29, 30). Endothelial dysfunction is a key step in the development of atherosclerosis in HD. Endothelial dysfunction has been attributed to altered NO bioactivity and increased formation of oxygen-derived free radicals. The underlying mechanisms of the altered bioavailability of NO in patients on HD are not fully understood. However, the activation of cytokines during HD can increase NO production (31, 32). The increase in NO levels in the patients who ingested sevelamer hydrochloride could suggest that they were under nitrosative stress in the final follow-up. This phenomenon occurred in patients who ingested doses of 1,600 and 3,200 mg. In the group that ingested calcium carbonate, NO levels also increased in the determination at 6 months of follow-up and when the patients ingested amounts >2 g, suggesting that they were also under nitrosative stress.
8-Hydroxy-2-deoxyguanosine (8-OHdG) is a marker that determines oxidative damage to DNA (33, 34). OS determined by the 8-OHdG marker is an independent predictor of all-cause mortality and morbidities in patients on HD (35, 36). Previously, it has been found that the oxidative damage to DNA evaluated with the marker 8-OHdG in peripheral blood lymphocytes increased more in patients on chronic HD than in non-dialyzed patients (37). On the other hand, sevelamer hydrochloride has previously been reported to have the ability to reduce oxidative damage to genetic material (38). The authors of a recent study reported the potential effect of sevelamer treatment on inflammation and possible oxidative RNA modifications (39). The results obtained at 6 months of follow-up of the patients on HD included in these studies who ingested sevelamer hydrochloride showed a significant increase in the oxidative DNA damage marker different from previously reported.
Repair of oxidative DNA damage is essential to maintain the integrity of genetic material, prevent mutagenesis, and decrease damage caused by reactive oxygen species. The hOGG1 enzyme is responsible for identifying and repairing oxidative damage to DNA through base cleavage mechanisms (40). High levels of pro-inflammatory cytokines and certain oxidants can decrease the activity of the DNA repair enzyme, especially in patients with ESRD (41, 42). The authors of a recent publication reported the downregulation of DNA repair enzymes in patients dependent on the type of peritoneal transport (43). Significant increase in oxidative DNA damage repair enzyme levels in patients treated with sevelamer hydrochloride, at 6 months of follow-up, is notable, especially in those who ingested 1,600 mg of the phosphate binder. Given this finding, we could hypothesize that the significant increase in DNA repair enzyme in the sevelamer hydrochloride group of patients on HD could be compensating for the increased oxidative damage marker in DNA. In contrast, no modification of the oxidative DNA damage marker or DNA repair enzyme was observed in those who ingested calcium carbonate.
The SOD enzyme is the first antioxidant defense of the body. The dismutation of the superoxide anion characterizes the SOD enzyme into oxygen and hydrogen peroxide (44). Increased activity of the antioxidant enzyme SOD in patients on HD with or without hyperglycemic status is well-documented. Increased SOD activity is considered an indicator of future vascular complications in patients on HD (45, 46). Elevated extracellular Pi causes mitochondrial OS related to mitochondrial hyperpolarization (20). The binding of Pi to sevelamer hydrochloride could explain the antioxidant mechanism by reducing mitochondrial OS. In this study, a significant increase in the activity of the SOD enzyme was found in the groups treated with sevelamer hydrochloride and with calcium carbonate in the determination at 6 months of follow-up. The increase in the activity of the SOD enzyme was notorious in those who ingested 3,200 mg of sevelamer hydrochloride (Figure 2).
Total antioxidant capacity determines the sum of endogenous and exogenous antioxidants (47). Advanced glycation end (AGE) products are excreted in the urine of subjects with normal renal function. However, in patients with ESRD who require HD, AGE products accumulate in the body from insufficient urinary excretion and limited clearance during dialysis (48). Treatment with sevelamer hydrochloride has previously been reported to reduce systemic and cellular AGE levels by restoring innate antioxidant defenses, improving inflammatory status, and reducing chronic OS (49, 50). At the end of the follow-up period of this study, SOD enzyme activity and TAC levels were found to be increased in the groups treated with sevelamer hydrochloride and calcium carbonate. These findings could suggest an attempt to compensate for the increase in oxidant molecules LPO and NO.
Mediators that orchestrate inflammatory response are cytokines. Among the cytokines, IL-6, and TNF-α have profound effects on the pro-inflammatory process in patients undergoing HD (51). According to our results, sevelamer hydrochloride showed an anti-inflammatory effect (52). Sevelamer hydrochloride can bind the endotoxins present in the intestinal lumen. In this way, the negatively charged lipid. Endotoxins are a powerful stimulus with the ability to activate the innate immune system that favors the transcription and production of pro-inflammatory cytokines. A part of endotoxins binds to sevelamer. In this way, sevelamer hydrochloride could exert its anti-inflammatory effect (53, 54). IL-6 decreased significantly in the determination at 6 months of follow-up in patients who ingested calcium carbonate and those who ingested 1,600 mg of sevelamer hydrochloride. TNF-α showed downregulation at 6 months of follow-up in the sevelamer hydrochloride and calcium carbonate groups. TNF-α decreased its levels primarily in those who ingested 3,200 mg of sevelamer hydrochloride and in those who ingested 2–4 g of calcium carbonate.
Sevelamer hydrochloride (more significant effect) and calcium carbonate showed anti-inflammatory and antioxidant effects independent of the phosphate inhibitory effect as previously reported (55, 56). Inflammatory markers, such as CRP, progressively increase with deterioration in renal function (57). Available data, such as CRP, TNF-α, IL-6, and arteriovenous fistula dysfunction, demonstrated that these systemic inflammatory markers were elevated in patients on HD (58). CRP was found to be increased in the final determination at the follow-up in those who ingested calcium carbonate, 2–4 g of calcium carbonate, and 1,600 mg of sevelamer hydrochloride. Alteration of serum ferritin may be a determining factor in mortality in adults on HD, and high ferritin levels lead to high mortality (59). The alteration of serum ferritin can be a determining factor in mortality in adults on HD. At the end of the follow-up of the patients who ingested sevelamer hydrochloride, ferritin levels decreased. In patients who ingested 1,600 and 3,200 mg of sevelamer hydrochloride, ferritin levels were decreased (Figure 3).
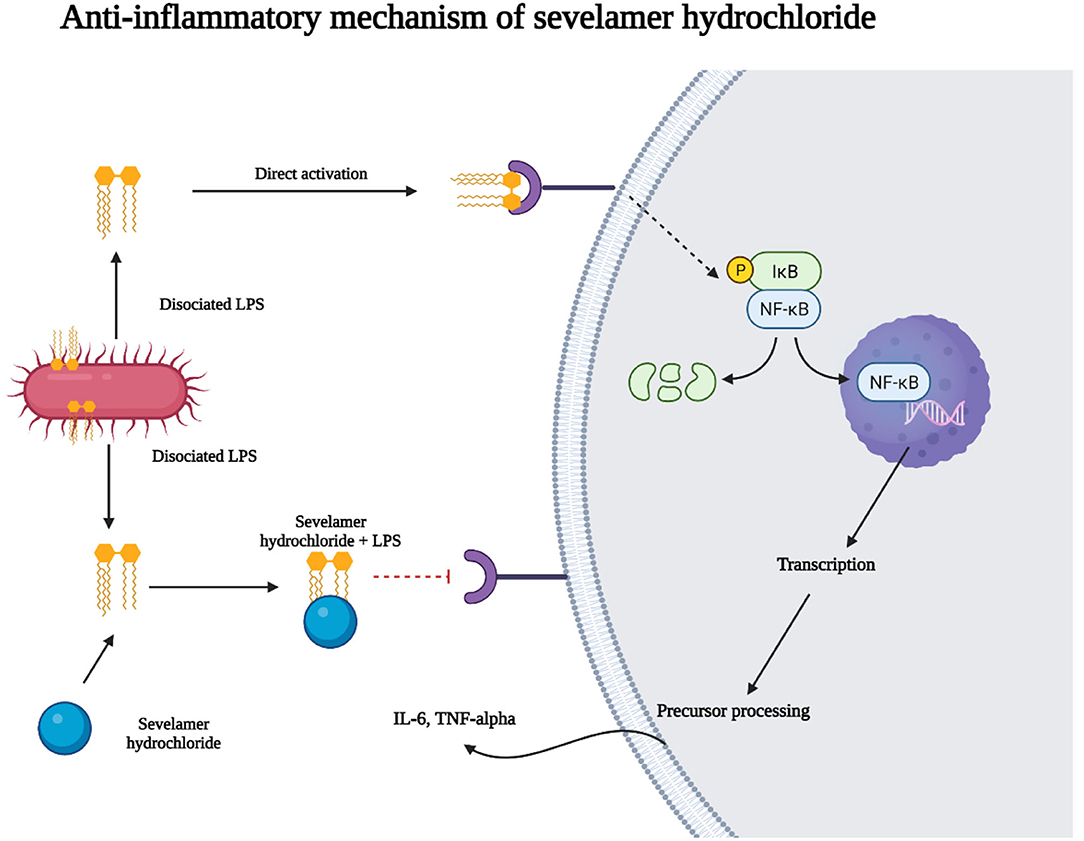
Figure 3. Anti-inflammatory of sevelamer hydrochloride. Sevelamer hydrochloride can bind to endotoxins present in the intestinal lumen. In this way, the negatively charged lipid A portion of endotoxins binds to sevelamer. Endotoxins are a component of the cell wall of gram-negative bacteria and are a potent stimulus for activating the innate immune system that leads to the transcription of pro-inflammatory cytokines. In this way, sevelamer hydrochloride could exert its anti-inflammatory effect.
Conclusions
The pleiotropic antioxidant and anti-inflammatory effects of sevelamer hydrochloride were fundamental in the results of this research study. OS was manifested by a significant increase in LPO and NO levels in the final determination at 6 months of follow-up in the sevelamer hydrochloride group and with the intake of 1,600 and 3,200 mg. The increase in NO at the end of the follow-up favored OS in the calcium carbonate group when they ingested doses of 2–4 and >5 g. OS is not only explained by the intake of Pi binders. ESRD and HD could play an essentially active role in their presence. As a probable compensatory mechanism for the increase in OS markers, levels of antioxidant enzymes were found to be increased at 6 months of follow-up. Increase in the SOD enzyme and TAC activity was observed in the sevelamer hydrochloride group and calcium carbonate groups in the final determination at the follow-up. A more significant increase in SOD activity was observed when the patients ingested 1,600 and 3,200 mg of sevelamer hydrochloride. In the calcium carbonate group, the increase in TAC was observed when they ingested from 1, 2–4, and more than 5 g. The behavior of pro-inflammatory cytokines was downregulated; primarily, TNF-α decreased its levels in the final determination at six months of follow-up in the groups that ingested sevelamer hydrochloride and calcium carbonate. Decrease in TNF-α is predominant in those who ingested 2–4 g of calcium carbonate or 3,200 mg of sevelamer hydrochloride. IL-6 decreased in those who ingested 1,600 mg of sevelamer hydrochloride and in the final determination of the calcium carbonate group, suggesting that both phosphate inhibitors have anti-inflammatory effects. Ferritin levels decreased significantly at 6 months of follow-up in the sevelamer hydrochloride group. This phenomenon was predominantly observed when they ingested the 1,600 and 3,200 mg doses, suggesting an anti-inflammatory improvement.
Contrary to the sevelamer hydrochloride, those who ingested calcium carbonate did not show changes in their levels. CRP levels increased in the final determination of the calcium carbonate group. The beneficial influence of sevelamer hydrochloride on pro-inflammatory cytokines and OS markers could be essential in managing phosphate binders in patients on HD by offering advantages in morbidity. However, the mechanism of action of sevelamer hydrochloride in OS is not fully understood. Long-term studies with a larger number of patients are required to know all the benefits that they can provide to patients with ESRD.
Study Limitations
The limitations of this study are based on the small number of patients in the HD program and the short follow-up time. We consider it worthwhile to design another stratified analysis that considers several phosphorus inhibitors for different follow-up times.
Study Strengths
The study offers a broader view on the simple use of two phosphate binders, the widely known calcium carbonate, and sevelamer hydrochloride, with probable anti-inflammatory pleiotropic effects. The information reported on the impact of sevelamer hydrochloride on the repair of oxidative DNA damage is scarce. In this study, we found the overexpression of the DNA repair enzyme possibly compensating for the significant increase in the oxidative DNA damage marker in patients on HD. This study provides new information on the possible regulatory effects of sevelamer hydrochloride on DNA repair.
Data Availability Statement
The data raw that support the conclusions of this article will be made available by the authors, with prior authorization from the Research and Ethics Committee.
Ethics Statement
The study was followed under the ethical principles for medical research in human beings stipulated in the declaration of Helsinki 64th General Assembly, Fortaleza Brazil, October 2013, and the Standards of Good Clinical Practice according to the guidelines of the International Conference on Harmonization. Under the General Health Law's provisions following the Regulations of the General Health Law on Research for Health Article 17 of Mexico, the study corresponds to category III. All the patients signed the Low Information Consent in the presence of witnesses. The study was evaluated and approved by the Local Ethics and Research Committee at the CentroMédico Nacional de Occidente, Instituto Mexicano del Seguro Social (R-2021-1301-063).
Author Contributions
ED-D, AG-S, AGM-D, and JC-G: conception and design. CP-N, JA-S, BJ-M, AB-L, and ER-C: acquisition, analysis, and interpretation of data. AG-S, ED-D, and AGM-D: drafting the article and revising it critically for important intellectual content. ED-D, AG-S, AGM-D, JC-G, CP-N, JA-S, BJ-M, AB-L, and ER-C: final approval of the version to be published. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cozzolino M, Ureña-Torres P, Vervloet MG, Brandenburg V, Bover J, Goldsmith D, et al. Is chronic kidney disease-mineral bone disorder (CKD-MBD) really a syndrome? Nephrol Dial Transplant. (2014) 29:1815–20. doi: 10.1093/ndt/gft514
2. Taniguchi M, Fukagawa M, Fujii N, Hamano T, Shoji T, Yokoyama K, et al. Serum phosphate and calcium should be primarily and consistently controlled in prevalent hemodialysis patients. committee of renal data registry of the japanese society for dialysis therapy. Ther Apher Dial. (2013) 17:221–8. doi: 10.1111/1744-9987.12030
3. Young EW, Albert JM, Satayathum S, Goodkin DA, Pisoni RL, Akiba T, et al. Predictors and consequences of altered mineral metabolism: the dialysis outcomes and practice patterns study. Kidney Int. (2005) 67:1179–87. doi: 10.1111/j.1523-1755.2005.00185.x
4. Scialla JJ, Kendrick J, Uribarri J, Kovesdy CP, Gutiérrez OM, Jimenez EY, et al. State-of-the-art management of hyperphosphatemia in patients with CKD: An NKF-KDOQI controversies perspective. Am J Kidney Dis. (2021) 77:132–41. doi: 10.1053/j.ajkd.2020.05.025
5. Suki WN, Zabaneh R, Cangiano JL, Reed J, Fischer D, Garrett L, et al. Effects of sevelamer and calcium-based phosphate binders on mortality in hemodialysis patients. Kidney Int. (2007) 72:1130–37. doi: 10.1038/sj.ki.5002466
6. Tzanno-Martins C, Biavo BM, Ferreira-Filho O, et al. Clinical efficacy, safety and anti-inflammatory activity of two sevelamer tablet forms in patients on low-flux hemodialysis. Int J Immunopathol Pharmacol. (2014) 27:25–35. doi: 10.1177/039463201402700105
7. Patel L, Bernard LM, Elder GJ. Sevelamer versus calcium-based binders for treatment of hyperphosphatemia in CKD: a meta-analysis of randomized controlled trials. Clin J Am Soc Nephrol. (2016) 11:232–44. doi: 10.2215/CJN.06800615
8. Komaba H, Wang M, Taniguchi M, Yamamoto S, Nomura T, Schaube DE, et al. Initiation of sevelamer and mortality among hemodialysis patients treated with calcium-based phosphate binders. Clin J Am Soc Nephrol. (2017) 12:1489–97. doi: 10.2215/CJN.13091216
9. Rodríguez-Osorio L, Zambrano DP, Gracia-Iguacel C, Rojas-Rivera J, Ortiz A, Egido J, et al. Use of sevelamer in chronic kidney disease: beyond phosphorus control. Nefrologia. (2015) 35:207–17. doi: 10.1016/j.nefroe.2015.05.011
10. Peres AT, Dalboni MA, Canziani ME, Manfredi SR, Carvalho JTG, Batista MC, et al. Effect of phosphate binders on oxidative stress and inflammation markers in hemodialysis patients. Hemodial Int. (2009) 13:271–77. doi: 10.1111/j.1542-4758.2009.00369.x
11. Liakopoulos V, Roumeliotis S, Gorny X, Dounousi E, Mertens PR. Oxidative stress in hemodialysis patients: a review of the literature. Oxid Med Cell Longev. (2017) 2017:3081856. doi: 10.1155/2017/3081856
12. Ikee R, Tsunoda M, Sasaki N, Sato N, Hashimoto N. Emerging effects of sevelamer in chronic kidney disease. Kidney Blood Press Res. (2013) 37:24–32. doi: 10.1159/000343397
13. Evenepoel P, Selgas R, Caputo F, Foggensteiner L, Heaf JG, Ortiz A, et al. Efficacy and safety of sevelamer hydrochloride and calcium acetate in patients on peritoneal dialysis. Nephrol Dial Transplant. (2009) 24:278–85. doi: 10.1093/ndt/gfn488
15. Gonzalez-Parra E, Tuñón J, Egido J, Ortiz A. Phosphate: a stealthier killer than previously thought? Cardiovasc Pathol. (2012) 21:372–81. doi: 10.1016/j.carpath.2012.02.008
16. Spaia S. Phosphate binders: sevelamer in the prevention and treatment of hyperphosphataemia in chronic renal failure. Hippokratia. (2011) 15:22–6.
17. Rastogi A. Sevelamer revisited: pleiotropic effects on endothelial and cardiovascular risk factors in chronic kidney disease and end-stage renal disease. Ther Adv Cardiovasc Dis. (2013) 7:322–42. doi: 10.1177/1753944713513061
18. Yu-Feng L, Chiang-Ting C, Wei-Chih K. Pleiotropic effects of sevelamer beyond phosphate binding in end-etage renal disease patients A randomized, open-label, parallel-group study. Clin Drug Investig. (2011) 31:257–67. doi: 10.2165/11539120-000000000-00000
19. Nguyen TT, Quan X, Hwang KH, Xu S, et al. Mitochondrial oxidative stress mediates high-phosphate-induced secretory defects and apoptosis in insulin-secreting cells. Am J Physiol Endocrinol Metab. (2015) 308: E933–41. doi: 10.1152/ajpendo.00009.2015
20. Lee J, Bae EH, Ma SK, Kim SW. Altered nitric oxide system in cardiovascular and renal diseases. Chonnam Med J. (2016) 52:81–90. doi: 10.4068/cmj.2016.52.2.81
21. Di Iorio B, Molony D, Bell C, Cucciniello E, Bellizzi V, Russo D, et al. Sevelamer versus calcium carbonate in incident hemodialysis patients: results of an open-label 24-month randomized clinical trial. Am J Kidney Dis. (2013) 62:771–8. doi: 10.1053/j.ajkd.2013.03.023
22. Boaz M, Matas Z, Biro A, Katzir Z, Green M, Fainaru M, et al. Serum malondialdehyde and prevalent cardiovascular disease in hemodialysis. Kidney Int. (1999) 56:1078–83. doi: 10.1046/j.1523-1755.1999.00613.x
23. Ben Omrane Sioud O, El Ati Z, Bouzidi H, Kerkeni M, Hammami M. Lipid and oxidative profile in hemodialysis patients: clinical follow-up for three years. Tunis Med. (2019) 97:551–55.
24. Lucchi L, Iannone A, Bergamini S, Stipo L, Perrone S, Uggeri S, et al. Comparison between hydroperoxides and malondialdehyde as markers of acute oxidative injury during hemodialysis. Artif Organs. (2005) 29:832–37. doi: 10.1111/j.1525-1594.2005.00136.x
25. Kang ES, Tevlin MT, Wang YB, Chiang TM, Cardenas R, Myers LK, et al. Hemodialysis hypotension: interaction of inhibitors, iNOS, and the interdialytic period. Am J Med Sci. (1999) 317:9–21. doi: 10.1097/00000441-199901000-00003
26. Noris M, Benigni A, Boccardo P, Aiello S, Gaspari F, Todeschini M, et al. Enhanced nitric oxide synthesis in uremia: Implications for platelet dysfunction and dialysis hypotension. Kidney Int. (1993) 44:445–50. doi: 10.1038/ki.1993.264
27. Raj DSC, Vincent B, Simpson K, Sato E, Jones KL, Welbourne TC, et al. Hemodynamic changes during hemodialysis: role of nitric oxide and endothelin. Kidney Int. (2002) 61:697–704. doi: 10.1046/j.1523-1755.2002.00150.x
28. McGuire BB, Watson RW, Pérez-Barriocal F, Fitzpatrick JM, Docherty NG. Gender differences in the renin-angiotensin and nitric oxide systems: relevance in the normal and diseased kidney. Kidney Blood Press Res. (2007) 30:67–80. doi: 10.1159/000099150
29. Assmann TS, Brondani LA, Bouças AP, Rheinheimer J, de Souza BM, Canani LH, et al. Nitric oxide levels in patients with diabetes mellitus: a systematic review and meta-analysis. Nitric Oxide. (2016) 69:1–9. doi: 10.1016/j.niox.2016.09.009
30. Tsapenko MV, d'Uscio LV, Grande JP, Croatt AJ, Hernandez MC, Ackerman AW, et al. Increased production of superoxide anion contributes to dysfunction of the arteriovenous fistula. Am J Physiol Renal Physiol. (2012) 303:F1601–7. doi: 10.1152/ajprenal.00449.2012
31. Meyer C, Heiss C, Drexhage C, Kehmeier ES, Balzer J, Mühlfeld A, et al. Hemodialysis-induced release of hemoglobin limits nitric oxide bioavailability and impairs vascular function. J Am Coll Cardiol. (2010) 55:454–9. doi: 10.1016/j.jacc.2009.07.068
32. Moncada S, Higgs EA. The discovery of nitric oxide and its role in vascular biology. Br J Pharmacol. (2006) 147:S193–201. doi: 10.1038/sj.bjp.0706458
33. Gedik CM, Boyle SP, Wood SG, Vaughan NJ, Collins AR. Oxidative stress in humans: validation of biomarkers of DNA damage. Carcinogenesis. (2002) 23:1441–46. doi: 10.1093/carcin/23.9.1441
34. Kasai H. Analysis of a form of oxidative DNA damage, 8-hydroxy-2-deoxyguanosine, as a marker of cellular oxidative stress during carcinogenesis. Mutat Res. (1997) 387:147–63.
35. Xu H, Watanabe M, Qureshi AR, Heimbürger O, Bárány P, Anderstam B, et al. Oxidative DNA damage and mortality in hemodialysis and peritoneal dialysis patients. Perit Dial Int. (2015) 32:206–15. doi: 10.3747/pdi.2013.00259
36. Mastalerz-Migas A, Steciwko A, Pokorski M, Pirogowicz I, Drobnik J, Bunio A, et al. What influences the level of oxidative stress as measured by 8-hydroxy-2'-deoxyguanosine in patients on hemodialysis? J Physiol Pharmacol. (2006) 57:199–205.
37. Tarng DC, Liu TY, Huang TP. Protective effect of vitamin C on 8-hydroxy-2'-deoxyguanosine level in peripheral blood lymphocytes of chronic hemodialysis patients. Kidney Int. (2004) 66:820–31. doi: 10.1111/j.1523-1755.2004.00809.x
38. Pastor S, Coll E, Rodríguez-Ribera L, Stoyanova E, Corredor ZF, Marcos R. Influence of carnicor, venofer, and sevelamer on the levels of genotoxic damage in end-stage renal disease patients. Environ Mol Mutagen. (2018) 59:302–11. doi: 10.1002/em.22170
39. Brønden A, Larsen EL, Karstoft K, Henriksen T, Vilsbøll T, Poulsen HE, et al. Changes in oxidative nucleic acid modifications and inflammation following one-week treatment with the bile acid sequestrant sevelamer: two randomized, placebo-controlled trials. J Diabetes Complications. (2020) 34:107446. doi: 10.1016/j.jdiacomp.2019.107446
40. Bravard A, Vacher M, Gouget B, Coutant A, de Boisferon FH, Stéphanie Marsin, et al. Redox regulation of human OGG1 activity in response to cellular oxidative stress. Mol Cell Biol. (2006) 26:7430–36. doi: 10.1128/MCB.00624-06
41. Tarng DC, Tsai TJ, Chen WT, Liu TY, Wei YH. Effect of human OGG1 1245C–>G gene polymorphism on 8-hydroxy-2'-deoxyguanosine levels of leukocyte DNA among patients undergoing chronic hemodialysis. J Am Soc Nephrol. (2001) 12:2338–47. doi: 10.1681/ASN.V12112338
42. Pan G, Deshpande M, Pang H, Stemmer PM, Carruthers NJ, Shearn CT, et al. 4-Hydroxy-2-nonenal attenuates 8-oxoguanine DNA glycosylase 1 activity. J Cell Biochem. (2020) 121:4887–97. doi: 10.1002/jcb.29814
43. Gutiérrez-Prieto JA, Soto-Vargas J, Parra-Michel R, Pazarín-Villaseñor HL, García-Sánchez A, Miranda-Díaz AG. The Behavior of the type of peritoneal transport in the inflammatory and oxidative status in adults under peritoneal dialysis. Front Med. (2019) 6:210. doi: 10.3389/fmed.2019.00210
44. Fridovich I. Superoxide radical and superoxide dismutases. Annu Rev Biochem. (1995) 64:97–112. doi: 10.1146/annurev.bi.64.070195.000525
45. Kimura F, Hasegawa G, Obayashi H, Adachi T, Hara H, Ohta M, et al. Serum extracellular superoxide dismutase in patients with type 2 diabetes: relationship to the development of micro- and macrovascular complications. Diabetes Care. (2003) 26:1246–50. doi: 10.2337/diacare.26.4.1246
46. Tajbakhsh R, Qorbani M, Mehrpour G, Rahimzadeh M, Azimzadeh MM, Mirmiranpour H. Effect of hemodialysis on oxidants and antioxidant factors in chronic renal failure. Saudi J Kidney Dis Transpl. (2017) 28:507–16. doi: 10.4103/1319-2442.206446
47. Rezaie A, Parker RD, Abdollahi M. Oxidative stress and pathogenesis of inflammatory bowel disease: an epiphenomenon or the cause? Dig Dis Sci. (2007) 52:2015–21. doi: 10.1007/s10620-006-9622-2
48. Yacoub R, Nugent M, Cai W, Nadkarni GN, Chaves LD, Abyad S, et al. Advanced glycation end products dietary restriction effects on bacterial gut microbiota in peritoneal dialysis patients; a randomized open label-controlled trial. PLoS ONE. (2017) 12:e0184789. doi: 10.1371/journal.pone.0184789
49. Yubero-Serrano EM, Woodward M, Poretsky L, Vlassara H, Strike GE. AGE-less Study Group. Effects of sevelamer carbonate on advanced glycation end products and antioxidant/pro-oxidant status in patients with diabetic kidney disease. Clin J Am Soc Nephrol. (2015) 10:759–66. doi: 10.2215/CJN.07750814
50. Ogunleye A, Akinbodewa AA, Adejumo OA, Oluwafemmi TT, Akinfaderin DA. Changes in antioxidant status associated with haemodialysis in chronic kidney disease. Ghana Med J. (2018) 52:29–33. doi: 10.4314/gmj.v52i1.6
51. Arena A, Stassi G, Iannello D, Gazzara D, Calapai M, Bisignano C, et al. Both IL-1β and TNF-α regulate NGAL expression in polymorphonuclear granulocytes of chronic hemodialysis patients. Mediators Inflamm. (2010) 2010:613937. doi: 10.1155/2010/613937
52. Ruggiero B, Trillini M, Tartaglione L, Rotondi S, Perticucci E, Tripepi R, et al. Effects of sevelamer carbonate in patients with CKD and proteinuria: the ANSWER randomized trial. Am J Kidney Dis. (2019) 74:338–50. doi: 10.1053/j.ajkd.2019.01.029
53. Kubotera N, Prokopienko AJ, Garba AO, Pai AB. Endotoxin binding by sevelamer: potential impact on nutritional status. Int J Nephrol. (2013) 2013:954956. doi: 10.1155/2013/954956
54. Perianayagam MC, Jaber BL. Endotoxin-binding affinity of sevelamer hydrochloride. Am J Nephrol. (2008) 285:802–7. doi: 10.1159/000135691
55. Shantouf R, Budoff MJ, Ahmadi N, Tiano J, Flores F, Kalantar-Zadeh K. Effects of sevelamer and calcium-based phosphate binders on lipid and inflammatory markers in hemodialysis patients. Am J Nephrol. (2008) 28:275–79. doi: 10.1159/000111061
56. Navarro-González JF, Mora-Fernández C, Muros de Fuentes M, Dontate-Correa J, Cazaña-Pérez V, García-Pérez J. Effect of phosphate binders on serum inflammatory profile, soluble CD14, and endotoxin levels in hemodialysis patients. Clin J Am Soc Nephrol. (2011) 6:2272–79. doi: 10.2215/CJN.01650211
57. Cachofeiro V, Goicochea M, de Vinuesa SG, Oubiña P, Lahera V, Luño J. Oxidative stress and inflammation, a link between chronic kidney disease and cardiovascular disease. Kidney Int. (2008) 111:S4–9. doi: 10.1038/ki.2008.516
58. Kuo WH, Lee YT, Ng HY, Wang CY, Wu CH, Lee CT. C-reactive protein variability is associated with vascular access outcome in hemodialysis patients. J Clin Lab Anal. (2018) 32:e22213. doi: 10.1002/jcla.22213
Keywords: oxidative stress markers, ESRD, calcium carbonate, antioxidants, sevelamer hydrochloride
Citation: Díaz-De la Cruz EN, Cerrillos-Gutiérrez JI, García-Sánchez A, Prado-Nevárez CG, Andrade-Sierra J, Jalomo-Martínez B, Banda-López A, Rojas-Campos E and Miranda-Díaz AG (2021) The Influence of Sevelamer Hydrochloride and Calcium Carbonate on Markers of Inflammation and Oxidative Stress in Hemodialysis at Six Months of Follow-Up. Front. Med. 8:714205. doi: 10.3389/fmed.2021.714205
Received: 24 May 2021; Accepted: 18 October 2021;
Published: 25 November 2021.
Edited by:
Ekamol Tantisattamo, University of California, Irvine, United StatesReviewed by:
Mateusz Maciejczyk, Medical University of Bialystok, PolandPrasenjit Mitra, Post Graduate Institute of Medical Education & Research (PGIMER), India
Copyright © 2021 Díaz-De la Cruz, Cerrillos-Gutiérrez, García-Sánchez, Prado-Nevárez, Andrade-Sierra, Jalomo-Martínez, Banda-López, Rojas-Campos and Miranda-Díaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alejandra Guillermina Miranda-Díaz, a2luZGFsZXgxQG91dGxvb2suY29t