 Qiuyue Huang
Qiuyue Huang Xiaofen Jia
Xiaofen Jia Yingming Chu
Yingming Chu Xuezhi Zhang
Xuezhi Zhang Hui Ye
Hui Ye
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 30 September 2021
Sec. Geriatric Medicine
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.713908
This article is part of the Research Topic Impacts of Common Geriatric Syndromes and their Interaction with Chronic Diseases on Health View all 33 articles
Helicobacter pylori (H. pylori) has so far infected more than half the global population. It is the most important and controllable risk factor for gastric cancer. The elderly, who are at a higher incidence of the infection, are also commonly found to develop antibiotic resistance. The symptoms, diagnosis, clinical features (of gastric or extra-digestive diseases), and treatment of H. pylori infection in the elderly, are different from that in the non-elderly. Health conditions, including comorbidities and combined medication have limited the use of regular therapies in elderly patients. However, they can still benefit from eradication therapy, thus preventing gastric mucosal lesions and gastric cancer. In addition, new approaches, such as dual therapy and complementary therapy, have the potential to treat older patients with H. pylori infection.
Aging is an inexorable process in the human life cycle. According to the World Health Organization, population aging is an evident phenomenon in all developed countries and some developing countries (1). Poor health of the elderly and the increasing disease burden have led to a great demand for medical care and social services (2, 3). Aging widely affects the functioning of various organs. Disrupted functioning of the digestive organs can lead to indigestion symptoms. A survey in Italy involving over 3,000 outpatients aged ≥60 years showed that over 40% of them had experienced gastrointestinal symptoms (4). Aging-related changes in the upper digestive system is mainly reflected in anatomical and physiological changes, such as gastric mucosa atrophy, decreased motility of the esophagus and stomach, reduced secretion of gastric acid and bile, decreased mucosal blood flow, and reduced digestive enzyme activity. Moreover, depending on factors such as infections, comorbidities, nutrition, and medications [e.g., non-steroidal anti-inflammatory drugs (NSAIDs)], aging can cause digestive disorders or further progression of diseases acquired in youth.
Among aged people, Helicobacter pylori (H. pylori), the most common infectious pathogen in the stomach, is the main risk factor for gastric cancer (5). Although H. pylori affects individuals of different age groups, the elderly have a higher prevalence of H. pylori infection, and risk of developing atrophic gastritis, and stomach cancer (6–8). As per a previous study, the effect of H. pylori eradication therapy in decreasing gastric cancer deaths varied among different age groups (failing in patients aged ≥80 years), but most of the aged patients with H. pylori infection could still benefit from the treatment (9). The eradication of H. pylori in elderly patients could be tricky due to decline in bodily functions, complications of other disease like renal failure, drug combinations, etc. (10). The use of mainstream therapies have to face more competing situations in older patients. The Fifth Chinese National Consensus Report on H. pylori infection has focused on geriatric patients, but it lacks information and treatment strategies specific to such patients (11). There is substantial scope to improve health care for elderly patients with H. pylori-related diseases. Therefore, this article aims to review the current knowledge on H. pylori infection in the geriatric population and the promising new approaches in this regard (Figure 1).
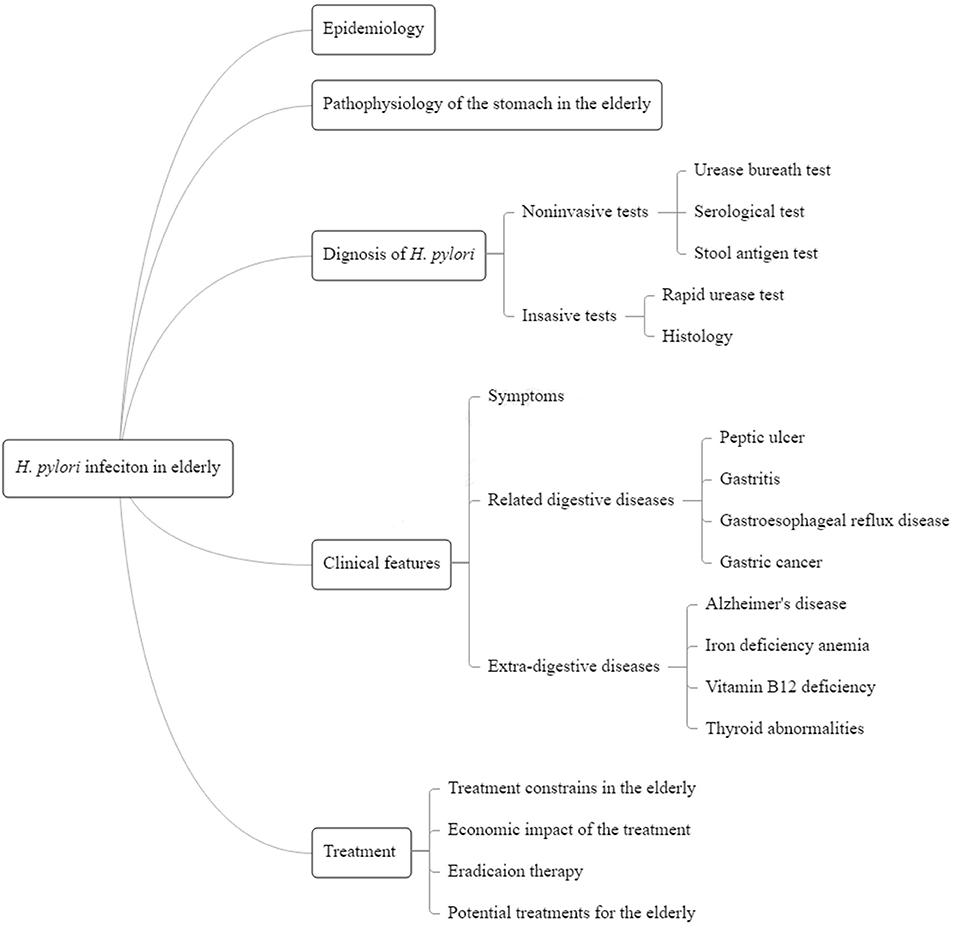
Figure 1. Summary figure of the review.
Approximately 50% of the global population is infected with H. pylori. The infection rate varies with age, socioeconomic class, and geographic area. H. pylori infection is usually acquired during childhood, and chronic infection lasts a lifetime if untreated. Due to improvement in sanitary conditions, the prevalence of H. pylori infection has gradually decreased in recent years, especially among the younger generation in the developed countries (12). However, in poor and developing countries and regions, the prevalence of H. pylori infection remains high in children. Decades later, these children might get affected by H. pylori-related diseases when they age (13, 14). The total H. pylori infection rate among the elderly in Beijing, China, according to a seroepidemiological investigation 15 years ago, was 83.4% (15), while in a recent study using the 13C-urea breath test, it was found to be 46.5% (16). Our previous study retrospectively collected the results of the 13C-urea breath test performed in our department from 2013 to 2019, in which the prevalence of H. pylori infection in people aged <20 years was 22.0%, and in those aged >60 years, it was 39.4% (17). The geriatric population in developing countries such as China is still facing the challenge of a high incidence of H. pylori infection. In addition, antibiotic resistance is more severe in the elderly population. A study conducted in China revealed that the antibiotic resistance rates to clarithromycin, levofloxacin, and metronidazole were 17.76, 19.66, and 95.5%, respectively in the entire patients; the highest antibiotic resistance rate was observed in patients aged 71–80 years (18). A larger study found that younger patients exhibited lower antibiotic resistance rates compared to patients aged ≥40 years (19). Thus, the epidemiology of H. pylori infection in elderly patients is characterized by high prevalence and drug resistance.
Compared with normal stomach, the stomach of the elderly exhibits functional and structural abnormalities, which lead to a series of biological responses, including impaired nuclear-mitochondrial communication (20), hypoxia (21), apoptosis (22), and increased levels of reactive oxygen species. The common characteristics of aging stomachs include slowing of gastric emptying, and dyspepsia (23). It also results in ‘anorexia of aging' (24) and post-prandial hypotension (25). Further, aging also contributed to a decrease in microbial diversity in stomach. In H. pylori-uninfected gastric corpus mucosa, the abundance and the microbial diversity of Firmicutes (Streptococcus, and Veillonella), Fusobacteria (Fusobacterium), Actinobacteria (Rothia), and Bacteroidetes (Prevotella) both decreased with age (26). In addition, atrophy of the gastric glands and the decrease in gastric mucosal blood flow weaken the gastric mucosal defense. The atrophy of the gastric glands induces the reduction of bicarbonate and prostaglandin production in the stomach and impairs the mucosal barrier. Gastric blood vessels are important for facilitating blood flow and preserving gastric mucosal morphology (27). They maintain the mucosal barrier, provide nutrients and oxygen, and defend the gastric mucosa against injury (28). As reported in a study, in elderly people, the mucosal blood flow decreases by >60%, causing profound hypoxia in all mucosal cells (29). The fundamental process of angiogenesis is impaired in aging gastric mucosa (30). These changes lead to increased susceptibility to injuries, such as the NSAID. H. pylori infection induces overproduction of nitric oxide, upregulates endothelial nitric oxide synthase expression, and induces angiogenesis (31), thus leading to obstruction of oxygen and blood flow.
H. pylori infection causes stomach mucosal lesions, atrophy, and microcirculation dysfunction in older people. Eradication therapy for H. pylori infection in geriatric patients can potentially prevent gastric cancer (32). The testing for H. pylori should be performed in aspirin and NSAID users (33). H. pylori eradication can prevent gastric mucosal injury induced by antiplatelet drugs (34). However, due to the complicated comorbidities, history of medications, and poor adherence to eradication therapy among the older patients, further efforts are required to develop appropriate treatment strategies for them.
Non-invasive tests include the urea breath test (UBT), H. pylori stool antigen test, and serological tests (35, 36). UBT is considered the gold standard of non-invasive methods for H. pylori diagnosis (37). It is the first choice for treating outpatients because of its wide availability and high accuracy (96%). In a previous study, the mean UBT values were found to significantly increase with age (38). The manufacturer-recommended cut-off values for UBT are not applicable in every setting. The 13C-UBT might have higher threshold values in subjects aged >60 years due to impairment in gastric emptying or lower endogenous CO2 production, compared to younger people (39). Severe gastric mucosal atrophy and intestinal metaplasia are independent risk factors for false positivity of UBT (40) because of the resultant lowered H. pylori density in the stomach (41). Thus, the UBT cut-off values should take age of the patient into account (42).
As per a study, the sensitivity, specificity, and diagnostic accuracy of serological tests in elderly patients were 74.4, 59, and 67%, respectively (43). The combined use of serological tests with UBT may further increase the sensitivity and specificity of H. pylori detection. However, the H. pylori antibody test may often yield false negative results because of spontaneous disappearance of H. pylori with advanced gastric mucosal atrophy, particularly in individuals aged ≥65 years (44).
H. pylori stool antigen test can effectively compensate for the drawbacks of UBT in the elderly. Detection of bacterial antigens was not affected by atrophic gastritis, ulceration, or intestinal metaplasia. In a study that evaluated the diagnostic efficiency of H. pylori stool antigen test in elderly subjects (≥65 years old), the accuracy (91.5%) and specificity (97.6%) were both high for all participants. However, the sensitivity was only 68.7%. Further, it was found that constipation and colorectal polyps were negatively and positively associated with its sensitivity, respectively (45).
Rapid urease test (RUT) is the preferred method for invasive detection of H. pylori, with a sensitivity of up to 95% and specificity of 85–95% (46). The sensitivity of RUT performed on antral biopsies of patients aged ≥60 years (57%) was lower than that performed on younger patients (75%) (47). Histological diagnosis of H. pylori can be performed at the same time as the pathological diagnosis in the gastric mucosa. For patients with high risk of gastric cancer, histological detection is recommended, which is of great significance for the evaluation of prognosis and the formulation of treatment measures. Upper gastrointestinal endoscopy is often necessary for the diagnosis of H. pylori infection in older adults with varying abdominal symptoms because of the high prevalence of severe stomach disorders in this age group (48). Bacterial culture performed on gastric biopsy specimens is mainly used for scientific research and is not a routine method for H. pylori detection. It showed low sensitivity (53.3%) and high specificity (100%) (49).
H. pylori infection is associated with the occurrence of peptic ulcers, chronic atrophic gastritis, gastric cancer etc. (50). With increasing age, the incidence and severity of most upper gastrointestinal diseases increase. The clinical features of H. pylori infection range from asymptomatic gastritis to gastrointestinal malignancy (51). Symptoms such as nausea, vomiting, epigastric pain, and belching are also common in acute H. pylori infection. However, most symptoms improve or disappear gradually in persistent chronic infection. In case of old patients, long-term H. pylori infection usually has no or mild digestive symptoms. These non-specific symptoms are often confused with those of other diseases, especially in case of H. pylori-induced gastritis. Patients with treatment-resistant H. pylori infections show more severe gastrointestinal symptoms (52). Further, older people with a history of treatment failure and excessive antibiotic exposure might also have more prominent symptoms.
H. pylori infection is strongly associated with peptic ulcer disease (PUD) (53). As the population ages, the incidence of cardiovascular and musculoskeletal diseases increases, as does the use of aspirin and NSAIDs. Aspirin, NSAIDs, and H. pylori are independent risk factors for PUD and its complications (54–56). The incidence of PUD increases with age, with most ulcers occurring between the ages of 25 and 64 (57). The most common and serious complication of PUD is bleeding, and people aged >60 years are at the highest risk of suffering from it (58). Treatment for H. pylori-associated PUD is mainly directed toward the eradication of infection. In cases of NSAID-induced ulcers, H. pylori eradication alone did not impair ulcer healing; and the use of proton pump inhibitors (PPI), H2 receptor antagonists, and misoprostol are recommended before using NSAIDs, in order to protect the gastric mucosa and prevent PUD and its complications (33, 55, 58). Early eradication of H. pylori in patients with PUD can reduce the risk of gastric cancer (59).
Chronic atrophic gastritis (CAG) is a disease characterized by atrophy of the gastric glands and/or intestinal metaplasia, which is mainly caused by prolonged persistence of H. pylori infection. Studies on the prevalence of CAG in different parts of the world have found that CAG is relatively common among the elderly (7). A study from Germany found that the prevalence of chronic atrophic gastritis increased from 4.8% in the 50–54 age group to 8.7% in the 70–74 age group (6). CAG is also a precancerous lesion of gastric cancer, especially when accompanied by intestinal metaplasia. All H. pylori-positive individuals should receive eradication therapy unless there are competing considerations (60). The eradication of H. pylori can reverse the atrophy of the gastric antrum and gastric body to a certain extent, but it has no observable effect on intestinal metaplasia (61). In the elderly, however, eradication of H. pylori may improve gastric atrophy and prevent the progression of intestinal metaplasia (8). Further, it can also delay the progression of CAG in the elderly, which is of great significance for the prevention of gastric cancer (62).
Gastroesophageal reflux disease (GERD) is a multifactorial disease that causes reflux of acidic stomach contents into the esophagus, causing tissue damage. Under normal conditions, gastric acid secretion does not decrease with age, but factors that cause atrophic gastritis, such as H. pylori infection, reduce gastric acid secretion (36). A case-control study found that compared with young and middle-aged GERD patients, atypical symptoms, low upper esophageal sphincter resting pressure, increased incidence of ineffective esophageal motility, and acid exposure were more significant in the elderly (63). A meta-analysis indicated that the prevalence of GERD was significantly higher in patients with H. pylori eradication than in those without it (64). However, eradication of H. pylori may not affect the healing rates or relapse rates of preexisting GERD (65). For patients with GERD, their condition should be comprehensively evaluated before carefully initiating H. pylori eradication therapy.
Gastric cancer is the fifth most common cancer and the third most common cause of cancer-related deaths worldwide (66). More than 1 million new cases of gastric cancer were reported in 2018, with an estimated 783,000 deaths (equivalent to 1 in 12 deaths worldwide). East Asian countries have a high incidence of gastric cancer (67). H. pylori is the main risk factor for gastric cancer apart from diet, alcohol, and smoking (67). H. pylori eradication may reduce the risk of gastric cancer in healthy, asymptomatic, and gastrointestinal patients (68). Among the high-incidence- and high-risk-population of gastric cancer, screening and eradication of H. pylori are recommended before the development of atrophic gastritis and intestinal metaplasia to prevent gastric cancer (14, 69). Due to the high incidence of gastric mucosal atrophy and intestinal epithelial metaplasia in elderly patients, it was thought in the past that the benefit of H. pylori eradication might be limited to treating gastric cancer. However, a long-term cohort study demonstrated that the risk of gastric cancer was significantly lower in people aged ≥60 years than that in the general population aged ≥10 years, after eradication of H. pylori (32). Moreover, patients at early stages of gastric cancer who received H. pylori eradication therapy had lower rates of metachronous gastric cancer than those who did not (70).
Although the relationship between H. pylori infection and gastric pathology has been established, the effect of this bacterium on the host body as a whole remains to be studied. It is well-known that some pathogens exist locally and may cause systemic pathological effects (71). Studies have found that H. pylori is associated with blood disorders such as vitamin B12 deficiency, iron-deficiency anemia (IDA), primary immune thrombocytopenia, as well as a number of dermatological, eye, metabolic, neurological, and allergic diseases (71). Among these diseases, we will only elaborate on diseases that have a greater impact on the elderly.
Approximately 46.8 million people live with dementia worldwide in 2015 (72). Alzheimer's disease (AD) is the single biggest cause of dementia, and is doubling in prevalence every 5 years after age 65 (73). Epidemiological studies have shown an association between H. pylori infection, mild cognitive impairment, and AD (74). H. pylori may affect the pathophysiology of AD in various ways (74, 75). Selective eradication of potentially curative H. pylori infection is recommended for H. pylori-infected patients with AD, and those who might fulfill the criteria of clinicians (for example, poor response to conventional drugs and complicated gastrointestinal symptoms) (74).
Iron deficiency is a common cause of anemia in the elderly. Many studies have shown a strong link between H. pylori infection and IDA. Compared with uninfected individuals, the prevalence of IDA was higher, and iron levels were significantly lower in those infected with H. pylori (76, 77). Hemorrhage (i.e., bleeding from ulcers) resulting from blood loss and the reduced iron absorption are the main causes of IDA (71). The Maastricht V/Florence Consensus Report recommends that patients with IDA of unknown cause should be diagnosed and treated for H. pylori (33). H. pylori eradication therapy combined with iron supplementation may help improve ferritin and hemoglobin levels (76).
Vitamin B12 deficiency is common in the elderly, and its prevalence increases with age (78, 79). Chronic atrophic gastritis, ingestion of drugs that affect gastric acid secretion or acid (i.e., proton pump inhibitors and antacids), H. pylori infection, overgrowth of intestinal bacteria, inadequate food intake, alcohol abuse, and smoking can all lead to B12 deficiency (79, 80). The clinical manifestations of B12 deficiency are heterogeneous; generally, there are no visible clinical symptoms. Its classical manifestations include Hunter's glossitis, megaloblastic anemia, and subacute combined degeneration of the spinal cord, and are associated with atherosclerotic vascular disease and neuropsychiatric disorders (78). B12 deficiency is particularly difficult to diagnose in elderly individuals. The Maastricht V/Florence Consensus Report recommends that all patients with vitamin B12 deficiency be screened for H. pylori infection, and treated if necessary (33).
Persistent active inflammation induced by H. pylori infection can lead to autoimmune immunopathological reactivity in affected patients, including thyroid abnormalities. The prevalence of anti-thyroid peroxidase antibody positivity is more frequent in subjects with H. pylori infection, and the association was still significant after adjusting other confounding factors (81). H. pylori-mediated chronic inflammation has also been shown to increase the expression of proinflammatory cytokines. And non-thyroidal-illness syndrome may develop on this background of chronic inflammation. A positive association between chronic active H. pylori infection and non-thyroidal-illness syndrome prevalence in elderly male cohort was found (82).
Several clinical guidelines are available for treating H. pylori infection in adults (11, 33, 83–86), children, and adolescents (87, 88). In general, the regimens recommended for adults are effective for older patients. However, a comprehensive benefit/risk assessment should be performed and individualized treatment be given to eradicate H. pylori in elderly patients (11, 34), due to their declining physical conditions, serious comorbidities, side effects and ongoing medications (89). A retrospective study indicated that clinicians might be reluctant to treat very old patients, possibly due to concerns about complications (90). Age, physical health condition, and history of medications are the determining factors for performing H. pylori eradication therapy.
The elderly population is more likely to be resistant to antibiotics because of excessive use in the past (91, 92). A multicenter cohort study showed that people aged >40 years were particularly at risk of developing dual drug resistance to levofloxacin and metronidazole (93). In case of chronic infectious bronchial pneumonia in the elderly, it is important to be wary of levofloxacin resistance, as they may have already been treated with quinolones or fluoroquinolones (94). It is recommended to select antibiotics according to the results of antibiotic susceptibility test. If eradication treatment fails, multidrug resistance may develop, making antibiotic selection more difficult (95, 96).
Aging stomachs are less defensive and more sensitive to stimuli, and the side effects of medications may be more pronounced, which may lead to less compliance to the regimen. Progressive aging of the human body can also change the ecological flora. The core microflora, such as Bacteroidetes, decreases in number, while the colony abundance of subdominant microflora such as Firmicutes, Actinobacteria, and Proteobacteria increases (97). The intestinal flora of the elderly population is more likely to be affected by antibiotic treatment as compared to that of the general population. Using probiotics during or after eradicating H. pylori may prevent or reduce microecological imbalance in elderly patients, thus reducing the occurrence of adverse effects (98, 99).
In addition to physiological senility, elderly people often suffer from a variety of diseases, such as hypertension, diabetes, liver and kidney dysfunction, etc. These diseases limit the use of certain drugs. For instance, the doses of amoxicillin and clarithromycin may have to be adjusted in patients with renal insufficiency or severe liver impairment. Further, comorbidities in the elderly patients result in drug interactions that can cause serious side effects (100). Some PPIs such as omeprazole can easily interact with cardiovascular drugs such as clopidogrel, which are commonly used in the geriatric population (101, 102). Amoxicillin, clarithromycin, metronidazole, and tetracycline may also interact with cardiovascular medications, such as statins, antiarrhythmic drugs, and warfarin (101).
Some economic analyses suggest that H. pylori screening and eradication are cost-effective for preventing gastric cancer, especially in high-risk areas (103–111). A study in Japan found that from 2013 to 2019, H. pylori eradication was economical and reduced the incidence of and mortality caused by gastric cancer in patients aged 20–80 years compared to those not having undergone eradication. Among the patients that had received eradication therapy, those aged 60 years had the highest cost benefits and best health outcomes (110). The use of H. pylori eradication as a strategy for the prevention of gastric cancer can not only save lives, but also greatly reduce the healthcare-related economic burden on the national budget (110).
Triple therapy has been used worldwide for decades and is the standard first-line eradication regimen for H. pylori infection (112). However, increased antibiotic resistance, particularly to clarithromycin, metronidazole, and levofloxacin (113, 114), has reduced the eradication rate of triple therapy (115, 116). A case-control study assessed the efficacy of a standard H. pylori eradication therapy among elderly patients, and concluded that the elderly did not affect efficacy or safety of a clarithromycin-based triple therapy for H. pylori eradication (117). Triple therapy was only recommended in the areas with clarithromycin resistance rate of <15%. Bismuth-containing quadruple therapy, concomitant therapy, sequential therapy, hybrid therapy, levofloxacin triple therapy, and rifabutin triple therapy were developed to overcome the challenge of antibiotic resistance (Table 1). These regimens are recommended by different consensus and guidelines for certain cases of H. pylori infection (33, 83, 84). Few studies have evaluated the efficacy and safety of these therapies in elderly patients. Bismuth-containing quadruple therapy was successful for the initial eradication of H. pylori in elderly patients, but 28% of patients had mild to moderate side effects (118). The sequential treatment regimen achieved significantly higher eradication rates in comparison with standard triple therapy in elderly patients, and there were mild side effects (<12%) of both the regimens (119). A retrospective investigation of 1,271 cases of H. pylori infection in elderly patients indicated that the rate of side effects with both the first and second treatment using triple therapy was <10%, suggesting that clinicians need not withhold treatment strictly based on old age (90).
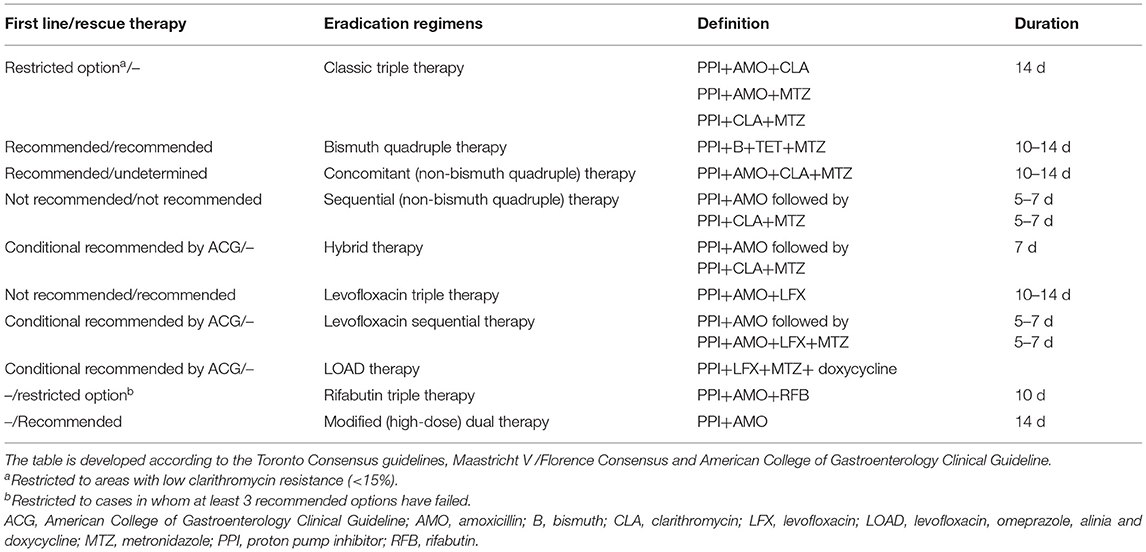
Table 1. Current mainstream regimens.
High-dose dual therapy consisting of amoxicillin and a PPI has drawn much attention recently because of the low resistance to amoxicillin and simpler drug composition as compared to the quadruple therapies. It has been recommended by the ACG Clinical Guidelines as a salvage regimen (84). A systematic review and meta-analysis indicated that the efficacy and compliance of modified dual therapy was comparable with the current mainstream first-line regimens for H. pylori infection, with a significantly lower incidence of adverse side effects (120, 121). A retrospective, real-life study demonstrated that modified dual therapy consisting of high-dose amoxicillin and rabeprazole was effective and safe for the first-line treatment of H. pylori infection in elderly patients (122). Although the dosage and frequency are increased in modified dual therapy, the total dose throughout the day remains within the safe range. Dual therapy reduces the use of antibiotics and bismuth, which is a promising new approach for the elderly. However, it must be used in patients not allergic to penicillin and those not having renal insufficiency. A randomized controlled clinical trial showed that the cost of medications in the modified dual therapy was lower than that in bismuth-containing quadruple therapy (123).
The development of new drugs has also widened the options for eradication therapy in the elderly population. Vonoprazan, a novel potassium-competitive acid blocker, is more potent and long-acting than traditional PPIs (124, 125). According to a network meta-analysis, vonoprazan-based triple therapy achieved high eradication rates of more than 90% as a first-line empiric treatment. Vonoprazan-based triple therapy is highly effective and well-tolerated, regardless of clarithromycin susceptibility (126). A retrospective cohort study reported that a triple-drug blister-packaged medication with amoxicillin, clarithromycin, and vonoprazan improved the first-line eradication rate of H. pylori in elderly patients (127). Therefore, vonoprazan-based therapy can be a valuable and promising new approach for the treatment of H. pylori infection in elderly.
New treatment strategies, including complementary and alternative medicine, are also being considered. Phytomedicines such as traditional Chinese medicine (TCM) treatment can not only improve the eradication rate of H. pylori, but also alleviate clinical symptoms and reduce adverse effects (128). H. pylori is considered as an “evil qi” in TCM theory. TCM believes that while trying to get rid of the “evil qi,” the “healthy qi” should be strengthened. In other words, it emphasizes on the protection of gastric mucosa and the promotion of immune regulation, which is of great significance in the prevention of H. pylori-related diseases. The Fifth Chinese National Consensus Report on the management of H. pylori infection suggests that the therapeutic effect of Chinese herbal medicines and Chinese patent medicines on H. pylori infection should be studied (11). To date, many studies have been conducted on the efficacy of classical ancient formulas [e.g., Banxia Xiexin decoction (129), Huangqi Jianzhong decoction (130), etc.], empirical prescriptions [Shengjiang Yiyou decoction (131), etc.], and proprietary Chinese medicines [Qingwei Qushi granules (132), Jinghua Weikang capsules (133), etc.] to treat H. pylori infection. For example, a randomized, double-blind, placebo-controlled clinical trial showed that the Burdock complex can ameliorate UBT, enhance antioxidant capacity, and reduce inflammatory response in asymptomatic patients with H. pylori infection (134). Some Chinese herbal medicines, such as Coptidis Rhizoma (Huang Lian) (135, 136), Scutellariae Radix (Huang Qin) (137), and Polygonum capitatum (Tou Hualiao) (138), also have anti-H. pylori effect. The studies have been in-depth and specific to the active components with clear chemical structure, among which berberine, the active component of Coptidis Rhizoma and many other traditional Chinese medicines, has been studied the most. Studies have indicated that berberine exerts antibacterial and anti-inflammatory effects by attenuating the Th17 response triggered by the B cell-activating factor, thus regulating macrophage polarization through the IL-4-STAT6 signaling pathway and suppressing proinflammatory genes and the IRF8-IFN-γ signaling axis (139–141). A meta-analysis has shown that the addition of berberine to standard triple therapy significantly improves H. pylori eradication, relieves clinical symptoms, accelerates ulcer healing, and has fewer side effects comparing to the standard triple therapy (142). As per a previous study, the combination of traditional Chinese and Western medicine may overcome the problem of antibiotic resistance, or be useful as a remedy after the failure of antibiotic-based eradication therapy (143). For elderly patients showing contraindications to the use of antibiotics, TCM may be an appropriate option to suppress gastric mucosal inflammation, delay lesion progression, and improve the quality of life.
H. pylori infection is considered the most common and controllable risk factor for gastric cancer. Screening and employing appropriate treatment strategies in areas with a high incidence of gastric cancer can effectively reduce its risk, ideally before the occurrence of gastric mucosal atrophy and intestinal metaplasia. Eradication therapy can reduce the risk of gastric cancer and prevent NSAID-induced ulcer in elderly patients. However, the degree of benefit depends on the degree of aging and life expectancy. Due to the decline in physical functions, comorbidities, and the presence of certain combined medications, many older adults have difficulty in following the standard treatment regimen recommended for adults.
Eradication therapy should be used to treat elderly patients only after an adequate risk-benefit assessment. The ideal regimen should be safe and effective, with minimal interaction with other drugs. However, the situation of continuous upgrade of the types and duration of eradication therapy, remains not ideal for the elderly patient. By optimizing the doses, reducing the use of antibiotics, or supplementing complementary drugs, the risk of adverse effects and drug interactions can be effectively reduced. The resurgence of dual therapy, especially the current hot topic, high-dose dual therapy, and vonoprazan, provided new directions. It successfully achieved satisfactory efficacy with fewer medications in normal patients. Further evaluation of its efficacy and safety in elderly patients should be conducted to gather more evidence (e.g., ChiCTR2100045059 in https://www.chictr.org.cn/).
Eradication therapy of H. pylori might not benefit all elderly patients. Patients aged >80 years, or those with severe organ function decline, and limited life expectancy, cannot tolerate full dosage and duration of eradication therapy. However, the possible benefits of eradication therapy should not be ignored in case of H. pylori-related diseases. Non-antibiotic treatment, typically involving probiotics and natural products that inhibit H. pylori activity, might be a complementary and alternative therapy. Several herbal medicines show remarkable anti-H. pylori properties (144); however, clinical trials are needed to confirm their effects. In China, integrative medicine is being considered as a new approach for H. pylori treatment in older patients, for which, clinical trials are being conducted (e.g., ChiCTR1900028373 in https://www.chictr.org.cn/).
Considering the progress toward an aging society and the high incidence of gastric cancer, more attention needs to be paid to the rational diagnosis and treatment of H. pylori infection in the elderly. Elderly patients also need to be finely stratified and treated with appropriate individualized eradication regimens or non-antibiotic regimens.
QH and XJ studied the literature and drafted the articles. YC participated in writing. XZ and HY identified the topics, analyzed the literature, presented the outlines, reviewed, and approved the publication of the article. All authors read and approved the final version of the manuscript.
This work was supported by the National Natural Science Foundation of China (Grant Number: 81973615) and the Beijing TCM Science and Technology Foundation (Grant Number: JJ2018-105).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. Arai H, Ouchi Y, Toba K, Endo T, Shimokado K, Tsubota K, et al. Japan as the front-runner of super-aged societies: perspectives from medicine and medical care in Japan. Geriatr Gerontol Int. (2015) 15:673–87. doi: 10.1111/ggi.12450
3. Zhang YS, Strauss JA, Hu P, Zhao Y, Crimmins EM. Links between mortality and socioeconomic characteristics, disease burden, and biological and physical functioning in the aging Chinese population. J Gerontol B Psychol Sci Soc Sci. (2021). doi: 10.1093/geronb/gbab059. [Epub ahead of print].
4. Pilotto A, Maggi S, Noale M, Franceschi M, Parisi G, Crepaldi G. Association of upper gastrointestinal symptoms with functional and clinical charateristics in elderly. World J Gastroenterol. (2011) 17:3020–6. doi: 10.3748/wjg.v17.i25.3020
5. Thrift AP, Nguyen TH. Gastric cancer epidemiology. Gastrointest Endosc Clin N Am. (2021) 31:425–39. doi: 10.1016/j.giec.2021.03.001
6. Weck MN, Stegmaier C, Rothenbacher D, Brenner H. Epidemiology of chronic atrophic gastritis: population-based study among 9444 older adults from Germany. Aliment Pharmacol Ther. (2007) 26:879–87. doi: 10.1111/j.1365-2036.2007.03430.x
7. Weck MN, Brenner H. Prevalence of chronic atrophic gastritis in different parts of the world. Cancer Epidemiol Biomarkers Prev. (2006) 15:1083–94. doi: 10.1158/1055-9965.EPI-05-0931
8. Toyokawa T, Suwaki K, Miyake Y, Nakatsu M, Ando M. Eradication of Helicobacter pylori infection improved gastric mucosal atrophy and prevented progression of intestinal metaplasia, especially in the elderly population: a long-term prospective cohort study. J Gastroenterol Hepatol. (2010) 25:544–7. doi: 10.1111/j.1440-1746.2009.05995.x
9. Asaka M, Kobayashi M, Kudo T, Akino K, Asaka Y, Fujimori K, et al. Gastric cancer deaths by age group in Japan: outlook on preventive measures for elderly adults. Cancer Sci. (2020) 111:3845–53. doi: 10.1111/cas.14586
10. Zendehdel A, Roham M. Role of Helicobacter pylori infection in the manifestation of old age-related diseases. Mol Genet Genomic Med. (2020) 8:e1157. doi: 10.1002/mgg3.1157
11. Liu WZ, Xie Y, Lu H, Cheng H, Zeng ZR, Zhou LY, et al. Fifth Chinese National Consensus Report on the management of Helicobacter pylori infection. Helicobacter. (2018) 23:e12475. doi: 10.1111/hel.12475
12. Watanabe M, Ito H, Hosono S, Oze I, Ashida C, Tajima K, et al. Declining trends in prevalence of Helicobacter pylori infection by birth-year in a Japanese population. Cancer Sci. (2015) 106:1738–43. doi: 10.1111/cas.12821
13. Curado MP, de Oliveira MM, de Araújo Fagundes M. Prevalence of Helicobacter pylori infection in Latin America and the Caribbean populations: a systematic review and meta-analysis. Cancer Epidemiol. (2019) 60:141–48. doi: 10.1016/j.canep.2019.04.003
14. Liou JM, Malfertheiner P, Lee YC, Sheu BS, Sugano K, Cheng HC, et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: the Taipei global consensus. Gut. (2020) 69:2093–112. doi: 10.1136/gutjnl-2020-322368
15. Zhang M, Tang Z, Zhou YZ, Cai L, Tang X. [Seroepidemiology study on Helicobacter pylori (cagA, vacA) infection of elderly people in Beijing]. Zhonghua Liu Xing Bing Xue Za Zhi. (2005) 26:687–9. doi: 10.3760/j.issn:0254-6450.2005.09.016
16. Zhu HM, Li BY, Tang Z, She J, Liang XY, Dong LK, et al. Epidemiological investigation of Helicobacter pylori infection in elderly people in Beijing. World J Clin Cases. (2020) 8:2173–80. doi: 10.12998/wjcc.v8.i11.2173
17. Yang SS, Deng X, Shi ZM, Ye H, Zhang XZ. Helicobacter pylori incidence survey in a general hospital. Beijing Med J. (2020) 42:782–83+86. doi: 10.15932/j.0253-9713.2020.08.022
18. Ji Z, Han F, Meng F, Tu M, Yang N, Zhang J. The Association of Age and antibiotic resistance of Helicobacter Pylori: a study in Jiaxing City, Zhejiang Province, China. Medicine. (2016) 95:e2831. doi: 10.1097/MD.0000000000002831
19. Liu DS, Wang YH, Zeng ZR, Zhang ZY, Lu H, Xu JM, et al. Primary antibiotic resistance of Helicobacter pylori in Chinese patients: a multiregion prospective 7-year study. Clin Microbiol Infect. (2018) 24:780.e5–80.e8. doi: 10.1016/j.cmi.2017.11.010
20. Gomes AP, Price NL, Ling AJ, Moslehi JJ, Montgomery MK, Rajman L, et al. Declining NAD(+) induces a pseudohypoxic state disrupting nuclear-mitochondrial communication during aging. Cell. (2013) 155:1624–38. doi: 10.1016/j.cell.2013.11.037
21. Samoszuk MK, Walter J, Mechetner E. Improved immunohistochemical method for detecting hypoxia gradients in mouse tissues and tumors. J Histochem Cytochem. (2004) 52:837–9. doi: 10.1369/jhc.4B6248.2004
22. Tarnawski AS, Szabo I. Apoptosis-programmed cell death and its relevance to gastrointestinal epithelium: survival signal from the matrix. Gastroenterology. (2001) 120:294–9. doi: 10.1053/gast.2001.21402
23. Soenen S, Rayner CK, Horowitz M, Jones KL. Gastric emptying in the elderly. Clin Geriatr Med. (2015) 31:339–53. doi: 10.1016/j.cger.2015.04.003
24. Landi F, Calvani R, Tosato M, Martone AM, Ortolani E, Savera G, et al. Anorexia of aging: risk factors, consequences, and potential treatments. Nutrients. (2016) 8:69. doi: 10.3390/nu8020069
25. Pham H, Phillips L, Trahair L, Hatzinikolas S, Horowitz M, Jones KL. Longitudinal changes in the blood pressure responses to, and gastric emptying of, an oral glucose load in healthy older subjects. J Gerontol A Biol Sci Med Sci. (2020) 75:244–48. doi: 10.1093/gerona/glz014
26. Shin CM, Kim N, Park JH, Lee DH. Changes in gastric corpus microbiota with age and after Helicobacter pylori eradication: a long-term follow-up study. Front Microbiol. (2020) 11:621879. doi: 10.3389/fmicb.2020.621879
27. Grishina I, Fenton A, Sankaran-Walters S. Gender differences, aging and hormonal status in mucosal injury and repair. Aging Dis. (2014) 5:160–9. doi: 10.14336/AD.2014.0500160
28. Björne HH, Petersson J, Phillipson M, Weitzberg E, Holm L, Lundberg JO. Nitrite in saliva increases gastric mucosal blood flow and mucus thickness. J Clin Invest. (2004) 113:106–14. doi: 10.1172/JCI19019
29. Tarnawski A, Pai R, Deng X, Ahluwalia A, Khomenko T, Tanigawa T, et al. Aging gastropathy-novel mechanisms: hypoxia, up-regulation of multifunctional phosphatase PTEN, and proapoptotic factors. Gastroenterology. (2007) 133:1938–47. doi: 10.1053/j.gastro.2007.08.037
30. Tarnawski AS, Ahluwalia A, Jones MK. Angiogenesis in gastric mucosa: an important component of gastric erosion and ulcer healing and its impairment in aging. J Gastroenterol Hepatol. (2014) 29(Suppl. 4):112–23. doi: 10.1111/jgh.12734
31. Lazaraki G, Kountouras J, Metallidis S, Vrettou E, Tzioufa V, Germanidis G, et al. Helicobacter pylori infection upregulates endothelial nitric oxide synthase expression and induces angiogenesis in gastric mucosa of dyspeptic patients. Eur J Gastroenterol Hepatol. (2008) 20:441–9. doi: 10.1097/MEG.0b013e3282f4c35a
32. Leung WK, Wong IOL, Cheung KS, Yeung KF, Chan EW, Wong AYS, et al. Effects of Helicobacter pylori treatment on incidence of gastric cancer in older individuals. Gastroenterology. (2018) 155:67–75. doi: 10.1053/j.gastro.2018.03.028
33. Malfertheiner P, Megraud F, O'Morain CA, Gisbert JP, Kuipers EJ, Axon AT, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. (2017) 66:6–30. doi: 10.1136/gutjnl-2016-312288
34. Wang JB. [Benefit/risk assessment and issues related to antibiotic use of Helicobacter pylori eradication in elderly individuals]. Zhonghua Yi Xue Za Zhi. (2020) 100:2343–45. doi: 10.3760/cma.j.cn112137-20200524-01640
35. Kamboj AK, Cotter TG, Oxentenko AS. Helicobacter pylori: the past, present, and future in management. Mayo Clin Proc. (2017) 92:599–604. doi: 10.1016/j.mayocp.2016.11.017
36. Pilotto A, Franceschi M. Helicobacter pylori infection in older people. World J Gastroenterol. (2014) 20:6364–73. doi: 10.3748/wjg.v20.i21.6364
37. Goossens H, Glupczynski Y, Burette A, Van den Borre C, DePrez C, Bodenmann J, et al. Evaluation of a commercially available complement fixation test for diagnosis of Helicobacter pylori infection and for follow-up after antimicrobial therapy. J Clin Microbiol. (1992) 30:3230–3. doi: 10.1128/jcm.30.12.3230-3233.1992
38. Eisdorfer I, Shalev V, Goren S, Chodick G, Muhsen K. Sex differences in urea breath test results for the diagnosis of Helicobacter pylori infection: a large cross-sectional study. Biol Sex Differ. (2018) 9:1. doi: 10.1186/s13293-017-0161-7
39. Perets TT, Gingold-Belfer R, Leibovitzh H, Itskoviz D, Schmilovitz-Weiss H, Snir Y, et al. Optimization of (13) C-urea breath test threshold levels for the detection of Helicobacter pylori infection in a national referral laboratory. J Clin Lab Anal. (2019) 33:e22674. doi: 10.1002/jcla.22674
40. Kwon YH, Kim N, Yoon H, Shin CM, Park YS, Lee DH. Effect of citric acid on accuracy of (13)C-urea breath test after Helicobacter pylori Eradication therapy in a region with a high prevalence of atrophic gastritis. Gut Liver. (2019) 13:506–14. doi: 10.5009/gnl18398
41. Chen X, Haruma K, Kamada T, Mihara M, Komoto K, Yoshihara M, et al. Factors that affect results of the 13C urea breath test in Japanese patients. Helicobacter. (2000) 5:98–103. doi: 10.1046/j.1523-5378.2000.00015.x
42. Zevit N, Niv Y, Shirin H, Shamir R. Age and gender differences in urea breath test results. Eur J Clin Invest. (2011) 41:767–72. doi: 10.1111/j.1365-2362.2010.02467.x
43. Pilotto A, Di Mario F, Franceschi M, Leandro G, Soffiati G, Scagnelli M, et al. Cure of Helicobacter pylori infection in the elderly: effects of eradication on gastritis and serological markers. Aliment Pharmacol Ther. (1996) 10:1021–7. doi: 10.1046/j.1365-2036.1996.88260000.x
44. Kato M, Ota H, Okuda M, Kikuchi S, Satoh K, Shimoyama T, et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2016 Revised Edition. Helicobacter. (2019) 24:e12597. doi: 10.1111/hel.12597
45. Han Y, Dai W, Meng F, Gan X, Liu M, Deng X, et al. Diagnosis of Helicobacter pylori infection in the elderly using an immunochromatographic assay-based stool antigen test. Microbiologyopen. (2020) 9:e1102. doi: 10.1002/mbo3.1102
46. Patel SK, Pratap CB, Jain AK, Gulati AK, Nath G. Diagnosis of Helicobacter pylori: what should be the gold standard? World J Gastroenterol. (2014) 20:12847–59. doi: 10.3748/wjg.v20.i36.12847
47. Abdalla AM, Sordillo EM, Hanzely Z, Perez-Perez GI, Blaser MJ, Holt PR, et al. Insensitivity of the CLOtest for H. pylori, especially in the elderly. Gastroenterology. (1998) 115:243–4. doi: 10.1016/S0016-5085(98)70401-9
48. Pilotto A, Franceschi M, Costa MC, Di Mario F, Valerio G. Helicobacter pylori test-and-eradication strategy. Lancet. (2000) 356:1683–4. doi: 10.1016/S0140-6736(05)70386-X
49. Shetty V, Ballal M, Balaraju G, Shetty S, Pai GC, Lingadakai R. Helicobacter pylori in dyspepsia: phenotypic and genotypic methods of diagnosis. J Glob Infect Dis. (2017) 9:131–34. doi: 10.4103/jgid.jgid_52_17
50. de Brito BB, da Silva FAF, Soares AS, Pereira VA, Santos MLC, Sampaio MM, et al. Pathogenesis and clinical management of Helicobacter pylori gastric infection. World J Gastroenterol. (2019) 25:5578–89. doi: 10.3748/wjg.v25.i37.5578
51. Diaconu S, Predescu A, Moldoveanu A, Pop CS, Fierbin?eanu-Braticevici C. Helicobacter pylori infection: old and new. J Med Life. (2017) 10:112–17. PMID:28616085.
52. Nestegard O, Johnsen KM, Sørbye SW, Halvorsen FA, Tønnessen T, Paulssen EJ, et al. Clinical characterization of Helicobacter pylori infected patients 15 years after unsuccessful eradication. PLoS ONE. (2020) 15:e0238944. doi: 10.1371/journal.pone.0238944
53. Graham DY. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer. World J Gastroenterol. (2014) 20:5191–204. doi: 10.3748/wjg.v20.i18.5191
54. Kim BW. Diagnosis and treatment of peptic ulcer disease: present and future perspective. Korean J Gastroenterol. (2016) 67:318–20. doi: 10.4166/kjg.2016.67.6.318
55. Melcarne L, García-Iglesias P, Calvet X. Management of NSAID-associated peptic ulcer disease. Expert Rev Gastroenterol Hepatol. (2016) 10:723–33. doi: 10.1586/17474124.2016.1142872
56. Sarri GL, Grigg SE, Yeomans ND. Helicobacter pylori and low-dose aspirin ulcer risk: a meta-analysis. J Gastroenterol Hepatol. (2019) 34:517–25. doi: 10.1111/jgh.14539
57. Dunlap JJ, Patterson S. Peptic ulcer disease. Gastroenterol Nurs. (2019) 42:451–54. doi: 10.1097/SGA.0000000000000478
58. Malfertheiner P, Chan FK, McColl KE. Peptic ulcer disease. Lancet. (2009) 374:1449–61. doi: 10.1016/S0140-6736(09)60938-7
59. Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology. (2009) 137:1641–8.e1–2. doi: 10.1053/j.gastro.2009.07.060
60. Lahner E, Carabotti M, Annibale B. Treatment of Helicobacter pylori infection in atrophic gastritis. World J Gastroenterol. (2018) 24:2373–80. doi: 10.3748/wjg.v24.i22.2373
61. Rokkas T, Pistiolas D, Sechopoulos P, Robotis I, Margantinis G. The long-term impact of Helicobacter pylori eradication on gastric histology: a systematic review and meta-analysis. Helicobacter. (2007) 12(Suppl. 2):32–8. doi: 10.1111/j.1523-5378.2007.00563.x
62. Chung JW, Hahm KB. Rejuvenation of atrophic gastritis in the elderly. J Gastroenterol Hepatol. (2010) 25:434–5. doi: 10.1111/j.1440-1746.2010.06251.x
63. Shi HX, Wang ZF, Sun XH. [Characteristics of esophageal motility and clinical presentation in gastroesophageal reflux disease patients of different age groups]. Zhonghua Yi Xue Za Zhi. (2021) 101:1015–19. doi: 10.3760/cma.j.cn112137-20200713-02110
64. Mou WL, Feng MY, Hu LH. Eradication of Helicobacter Pylori Infections and GERD: a systematic review and meta-analysis. Turk J Gastroenterol. (2020) 31:853–59. doi: 10.5152/tjg.2020.19699
65. Zhao Y, Li Y, Hu J, Wang X, Ren M, Lu G, et al. The effect of Helicobacter pylori eradication in patients with gastroesophageal reflux disease: a meta-analysis of randomized controlled studies. Dig Dis. (2020) 38:261–68. doi: 10.1159/000504086
66. Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. (2020) 396:635–48. doi: 10.1016/S0140-6736(20)31288-5
67. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
68. Lin Y, Kawai S, Sasakabe T, Nagata C, Naito M, Tanaka K, et al. Effects of Helicobacter pylori eradication on gastric cancer incidence in the Japanese population: a systematic evidence review. Jpn J Clin Oncol. (2021) 51:1158–70. doi: 10.1093/jjco/hyab055
69. Choi IJ. [Helicobacter pylori eradication therapy and gastric cancer prevention]. Korean J Gastroenterol. (2018) 72:245–51. doi: 10.4166/kjg.2018.72.5.245
70. Choi IJ, Kook MC, Kim YI, Cho SJ, Lee JY, Kim CG, et al. Helicobacter pylori therapy for the prevention of metachronous gastric cancer. N Engl J Med. (2018) 378:1085–95. doi: 10.1056/NEJMoa1708423
71. Gravina AG, Priadko K, Ciamarra P, Granata L, Facchiano A, Miranda A, et al. Extra-gastric manifestations of Helicobacter pylori infection. J Clin Med. (2020) 9:3887. doi: 10.3390/jcm9123887
72. Prince MJ. World Alzheimer Report 2015: The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Alzheimer's Disease International (ADI) (2015).
73. Lane CA, Hardy J, Schott JM. Alzheimer's disease. Eur J Neurol. (2018) 25:59–70. doi: 10.1111/ene.13439
74. Doulberis M, Kotronis G, Thomann R, Polyzos SA, Boziki M, Gialamprinou D, et al. Review: impact of Helicobacter pylori on Alzheimer's disease: what do we know so far? Helicobacter. (2018) 23:e12534. doi: 10.1111/hel.12534
75. Albaret G, Sifré E, Floch P, Laye S, Aubert A, Dubus P, et al. Alzheimer's disease and Helicobacter pylori infection: inflammation from stomach to brain? J Alzheimers Dis. (2020) 73:801–09. doi: 10.3233/JAD-190496
76. Hudak L, Jaraisy A, Haj S, Muhsen K. An updated systematic review and meta-analysis on the association between Helicobacter pylori infection and iron deficiency anemia. Helicobacter. (2017). 22:10.1111/hel.12330. doi: 10.1111/hel.12330
77. Demerdash DME, Ibrahim H, Hassan DM, Moustafa H, Tawfik NM. Helicobacter pylori associated to unexplained or refractory iron deficiency anemia: an Egyptian single-center experience. Hematol Transfus Cell Ther. (2018) 40:219–25. doi: 10.1016/j.htct.2018.02.001
78. Wong CW. Vitamin B12 deficiency in the elderly: is it worth screening? Hong Kong Med J. (2015) 21:155–64. doi: 10.12809/hkmj144383
79. Green R, Allen LH, Bjørke-Monsen AL, Brito A, Guéant JL, Miller JW, et al. Vitamin B(12) deficiency. Nat Rev Dis Primers. (2017) 3:17040. doi: 10.1038/nrdp.2017.40
80. Ulasoglu C, Temiz HE, Saglam ZA. The relation of cytotoxin-associated gene-A seropositivity with vitamin B12 deficiency in Helicobacter pylori-positive patients. Biomed Res Int. (2019) 2019:1450536. doi: 10.1155/2019/1450536
81. Choi YM, Kim TY, Kim EY, Jang EK, Jeon MJ, Kim WG, et al. Association between thyroid autoimmunity and Helicobacter pylori infection. Korean J Intern Med. (2017) 32:309–13. doi: 10.3904/kjim.2014.369
82. Sun B, Wang X, McLarnon MED, Ding Y, Liu M, Dai W, et al. Higher prevalence of non-thyroidal-illness syndrome in elderly male patients with active Helicobacter pylori infection. Front Med. (2021) 8:682116. doi: 10.3389/fmed.2021.682116
83. Fallone CA, Chiba N, van Zanten SV, Fischbach L, Gisbert JP, Hunt RH, et al. The toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. (2016) 151:51–69.e14. doi: 10.1053/j.gastro.2016.04.006
84. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol. (2017) 112:212–39. doi: 10.1038/ajg.2016.563
85. El-Serag HB, Kao JY, Kanwal F, Gilger M, LoVecchio F, Moss SF, et al. Houston consensus conference on testing for Helicobacter pylori infection in the United States. Clin Gastroenterol Hepatol. (2018) 16:992–1002.e6. doi: 10.1016/j.cgh.2018.03.013
86. Mahachai V, Vilaichone RK, Pittayanon R, Rojborwonwitaya J, Leelakusolvong S, Maneerattanaporn M, et al. Helicobacter pylori management in ASEAN: the Bangkok consensus report. J Gastroenterol Hepatol. (2018) 33:37–56. doi: 10.1111/jgh.13911
87. Jones NL, Koletzko S, Goodman K, Bontems P, Cadranel S, Casswall T, et al. Joint ESPGHAN/NASPGHAN guidelines for the management of Helicobacter pylori in children and adolescents (Update 2016). J Pediatr Gastroenterol Nutr. (2017) 64:991–1003. doi: 10.1097/MPG.0000000000001594
88. Huang Y. Expert consensus on diagnosis and treatment of Helicobacter pylori infection in children. Chin J Pediatr. (2015) 53:496–98.
89. Norgard NB, Mathews KD, Wall GC. Drug-drug interaction between clopidogrel and the proton pump inhibitors. Ann Pharmacother. (2009) 43:1266–74. doi: 10.1345/aph.1M051
90. Kobayashi S, Joshita S, Yamamoto C, Yanagisawa T, Miyazawa T, Miyazawa M, et al. Efficacy and safety of eradication therapy for elderly patients with Helicobacter pylori infection. Medicine. (2019) 98:e16619. doi: 10.1097/MD.0000000000016619
91. Nguyen CT, Davis KA, Nisly SA, Li J. Treatment of Helicobacter pylori in special patient populations. Pharmacotherapy. (2019) 39:1012–22. doi: 10.1002/phar.2318
92. Boyanova L, Gergova G, Markovska R, Kandilarov N, Davidkov L, Spassova Z, et al. Primary Helicobacter pylori resistance in elderly patients over 20 years: a Bulgarian study. Diagn Microbiol Infect Dis. (2017) 88:264–67. doi: 10.1016/j.diagmicrobio.2017.05.001
93. Lyu T, Cheung KS, Ni L, Guo J, Mu P, Li Y, et al. High prevalence and risk factors of multiple antibiotic resistance in patients who fail first-line Helicobacter pylori therapy in southern China: a municipality-wide, multicentre, prospective cohort study. J Antimicrob Chemother. (2020) 75:3391–94. doi: 10.1093/jac/dkaa315
94. Tandan M, Zimmerman S, Sloane PD, Ward K, Daniels LM, Wretman CJ. Which nursing home residents with pneumonia are managed on-site and which are hospitalized? Results from 2 years' surveillance in 14 US homes. J Am Med Dir Assoc. (2020) 21:1862–68.e3. doi: 10.1016/j.jamda.2020.07.028
95. Liou JM, Lee YC, Wu MS. Treatment of refractory Helicobacter pylori infection-tailored or empirical therapy. Gut Liver. (2021). doi: 10.5009/gnl20330. [Epub ahead of print].
96. Kuo CJ, Lee CH, Chang ML, Lin CY, Lin WR, Su MY, et al. Multidrug resistance: the clinical dilemma of refractory Helicobacter pylori infection. J Microbiol Immunol Infect. (2021). doi: 10.1016/j.jmii.2021.03.006. [Epub ahead of print].
97. Vaiserman AM, Koliada AK, Marotta F. Gut microbiota: a player in aging and a target for anti-aging intervention. Ageing Res Rev. (2017) 35:36–45. doi: 10.1016/j.arr.2017.01.001
98. Zhang M, Zhang C, Zhao J, Zhang H, Zhai Q, Chen W. Meta-analysis of the efficacy of probiotic-supplemented therapy on the eradication of H. pylori and incidence of therapy-associated side effects. Microb Pathog. (2020) 147:104403. doi: 10.1016/j.micpath.2020.104403
99. Tang B, Tang L, Huang C, Tian C, Chen L, He Z, et al. The effect of probiotics supplementation on gut microbiota after Helicobacter pylori eradication: a multicenter randomized controlled trial. Infect Dis Ther. (2021) 10:317–33. doi: 10.1007/s40121-020-00372-9
100. Tomita N, Mizokami F, Kisara S, Arai H. Transdisciplinary approach for potentially harmful drug-drug interaction detection as a part of a comprehensive medication review and geriatric assessment. Geriatr Gerontol Int. (2019) 19:462–63. doi: 10.1111/ggi.13638
101. Anrys P, Petit AE, Thevelin S, Sallevelt B, Drenth C, Soiza RL, et al. An International consensus list of potentially clinically significant drug-drug interactions in older people. J Am Med Dir Assoc. (2021). doi: 10.1016/j.jamda.2021.03.019. [Epub ahead of print].
102. Abrignani MG, Gatta L, Gabrielli D, Milazzo G, De Francesco V, De Luca L, et al. Gastroprotection in patients on antiplatelet and/or anticoagulant therapy: a position paper of National Association of Hospital Cardiologists (ANMCO) and the Italian Association of Hospital Gastroenterologists and Endoscopists (AIGO). Eur J Intern Med. (2021) 85:1–13. doi: 10.1016/j.ejim.2020.11.014
103. Cheng HC, Wang JD, Chen WY, Chen CW, Chang SC, Sheu BS. Helicobacter pylori test-and-treat program can be cost-effective to prevent gastric cancer in Taiwanese adults: referred to the nationwide reimbursement database. Helicobacter. (2015) 20:114–24. doi: 10.1111/hel.12185
104. Teng AM, Kvizhinadze G, Nair N, McLeod M, Wilson N, Blakely T. A screening program to test and treat for Helicobacter pylori infection: cost-utility analysis by age, sex and ethnicity. BMC Infect Dis. (2017) 17:156. doi: 10.1186/s12879-017-2259-2
105. Chen Q, Liang X, Long X, Yu L, Liu W, Lu H. Cost-effectiveness analysis of screen-and-treat strategy in asymptomatic Chinese for preventing Helicobacter pylori-associated diseases. Helicobacter. (2019) 24:e12563. doi: 10.1111/hel.12563
106. Kowada A. Cost-effectiveness of Helicobacter pylori test and eradication versus upper gastrointestinal series versus endoscopy for gastric cancer mortality and outcomes in high prevalence countries. Scand J Gastroenterol. (2019) 54:685–89. doi: 10.1080/00365521.2019.1627408
107. Beresniak A, Malfertheiner P, Franceschi F, Liebaert F, Salhi H, Gisbert JP. Helicobacter pylori “Test-and-Treat” strategy with urea breath test: a cost-effective strategy for the management of dyspepsia and the prevention of ulcer and gastric cancer in Spain-Results of the Hp-Breath initiative. Helicobacter. (2020) 25:e12693. doi: 10.1111/hel.12693
108. Han Y, Yan T, Ma H, Yao X, Lu C, Li Y, et al. Cost-Effectiveness Analysis of Helicobacter pylori eradication therapy for prevention of gastric cancer: a markov model. Dig Dis Sci. (2020) 65:1679–88. doi: 10.1007/s10620-019-05910-1
109. Kowada A. Endoscopy Is Cost-Effective for gastric cancer screening after successful Helicobacter pylori eradication. Dig Dis Sci. (2021). doi: 10.1007/s10620-020-06813-2. [Epub ahead of print].
110. Kowada A, Asaka M. Economic and health impacts of introducing Helicobacter pylori eradication strategy into national gastric cancer policy in Japan: a cost-effectiveness analysis. Helicobacter. (2021) 26:e12837. doi: 10.1111/hel.12837
111. Zheng H, Xie Q, Zhan M, Jin C, Li Q. Cost-effectiveness analysis of Helicobacter pylori eradication therapy in first-degree relatives of patients with gastric cancer. Patient Prefer Adherence. (2021) 15:77–85. doi: 10.2147/PPA.S286860
112. Current European concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. European Helicobacter Pylori Study Group. Gut. (1997) 41:8–13. doi: 10.1136/gut.41.1.8
113. Hu Y, Zhu Y, Lu NH. Primary antibiotic resistance of Helicobacter pylori in China. Dig Dis Sci. (2017) 62:1146–54. doi: 10.1007/s10620-017-4536-8
114. Savoldi A, Carrara E, Graham DY, Conti M, Tacconelli E. Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in World Health Organization Regions. Gastroenterology. (2018) 155:1372–82.e17. doi: 10.1053/j.gastro.2018.07.007
115. Dang BN, Graham DY. Helicobacter pylori infection and antibiotic resistance: a WHO high priority? Nat Rev Gastroenterol Hepatol. (2017) 14:383–84. doi: 10.1038/nrgastro.2017.57
116. Wang B, Lv ZF, Wang YH, Wang H, Liu XQ, Xie Y, et al. Standard triple therapy for Helicobacter pylori infection in China: a meta-analysis. World J Gastroenterol. (2014) 20:14973–85. doi: 10.3748/wjg.v20.i40.14973
117. Durazzo M, Ferro A, Fagoonee S, Staiano MT, Saracco GM, Pellicano R. Helicobacter pylori eradication with a clarithromycin-based triple therapy in elderly patients: a case-control study. Panminerva Med. (2021). doi: 10.23736/S0031-0808.21.04500-6. [Epub ahead of print].
118. Dore MP, Maragkoudakis E, Pironti A, Tadeu V, Tedde R, Realdi G, et al. Twice-a-day quadruple therapy for eradication of Helicobacter pylori in the elderly. Helicobacter. (2006) 11:52–5. doi: 10.1111/j.0083-8703.2006.00370.x
119. Zullo A, Gatta L, De Francesco V, Hassan C, Ricci C, Bernabucci V, et al. High rate of Helicobacter pylori eradication with sequential therapy in elderly patients with peptic ulcer: a prospective controlled study. Aliment Pharmacol Ther. (2005) 21:1419–24. doi: 10.1111/j.1365-2036.2005.02519.x
120. Gao CP, Zhang D, Zhang T, Wang JX, Han SX, Graham DY, et al. PPI-amoxicillin dual therapy for Helicobacter pylori infection: an update based on a systematic review and meta-analysis. Helicobacter. (2020) 25:e12692. doi: 10.1111/hel.12692
121. Huang Q, Shi Z, Cheng H, Ye H, Zhang X. Efficacy and safety of modified dual therapy as the first-line regimen for the treatment of Helicobacter pylori infection: a meta-analysis of randomized controlled trials. J Clin Gastroenterol. (2020). doi: 10.1097/MCG.0000000000001448. [Epub ahead of print].
122. Gao W, Ye H, Deng X, Wang C, Xu Y, Li Y, et al. Rabeprazole-amoxicillin dual therapy as first-line treatment for H. pylori eradication in special patients: a retrospective, real-life study. Helicobacter. (2020) 25:e12717. doi: 10.1111/hel.12717
123. Yang J, Zhang Y, Fan L, Zhu YJ, Wang TY, Wang XW, et al. Eradication efficacy of modified dual therapy compared with bismuth-containing quadruple therapy as a first-line treatment of Helicobacter pylori. Am J Gastroenterol. (2019) 114:437–45. doi: 10.14309/ajg.0000000000000132
124. Graham DY, Dore MP. Update on the use of vonoprazan: a competitive acid blocker. Gastroenterology. (2018) 154:462–66. doi: 10.1053/j.gastro.2018.01.018
125. Ozaki H, Harada S, Takeuchi T, Kawaguchi S, Takahashi Y, Kojima Y, et al. Vonoprazan, a novel potassium-competitive acid blocker, should be used for the Helicobacter pylori eradication therapy as first choice: a large sample study of vonoprazan in real world compared with our randomized control trial using second-generation proton pump inhibitors for Helicobacter pylori eradication therapy. Digestion. (2018) 97:212–18. doi: 10.1159/000485097
126. Okubo H, Akiyama J, Kobayakawa M, Kawazoe M, Mishima S, Takasaki Y, et al. Vonoprazan-based triple therapy is effective for Helicobacter pylori eradication irrespective of clarithromycin susceptibility. J Gastroenterol. (2020) 55:1054–61. doi: 10.1007/s00535-020-01723-6
127. Nishida T, Tsujii Y, Okamoto A, Tomita R, Higaki Y, Osugi N, et al. A triple-drug blister-packaged drug with vonoprazan improves first-line eradication of Helicobacter pylori in elderly patients: a retrospective propensity score-matched cohort study. Digestion. (2020) 101:608–14. doi: 10.1159/000501608
128. Li Y, Li X, Tan Z. An overview of traditional Chinese medicine therapy for Helicobacter pylori-related gastritis. Helicobacter. (2021) 26:e12799. doi: 10.1111/hel.12799
129. Lin CG. Clinical effect and effective effect analysis of banxia xiexin decoction in the treatment of Helicobacter pylori-positive chronic gastritis. China Foreign Med Treat. (2019) 38:155–57+63. doi: 10.16662/j.cnki.1674-0742.2019.21.155
130. Yao MW, Xu L, Huang GH. Observation on the effect of Huangqi Jianzhong Decoction combined with moxibustion of matching of he-sea point and front Mu point on H. pylori positive chronic atrophic gastritis of type of spleen and stomach deficiency-cold. Mod J Integr Tradit Chin West Med. (2020) 29:124–28. doi: 10.3969/j.issn.1008-8849.2020.02.003
131. Li JS, Lin GB, Chen ZL, Zou KW, Cheng HH, Chen HJ. Clinical observation of shengjiang yiyou decoction in treating chronic gastritis with Helicobacter pylori infection of spleen-stomach damp-heat type. J Guangzhou Univ Tradit Chin Med. (2019) 36:787–90. doi: 10.13359/j.cnki.gzxbtcm.2019.06.004
132. Wu SH, Ge Y, Zeng J, Tan WF. Clinical observation of Qingwei Qushi qranules combined with bismuth containing quadruple in treating Helicobacter pylori positive chronic non-atrophic gastritis with spleen-stomach damp-heat syndrome. Chin J Integr Tradit West Med Dig. (2019) 27:260–63. doi: 10.3969/j.issn.1671-038X.2019.04.05
133. Dai MS, Cheng XH. Clinical study on Jinghua Weikang soft capsules for chronic gastritis caused by Helicobacter pylori. J New Chin Med. (2019) 51:110–12. doi: 10.13457/j.cnki.jncm.2019.11.032
134. Yen CH, Chiu HF, Huang SY, Lu YY, Han YC, Shen YC, et al. Beneficial effect of Burdock complex on asymptomatic Helicobacter pylori-infected subjects: a randomized, double-blind placebo-controlled clinical trial. Helicobacter. (2018) 23:e12469. doi: 10.1111/hel.12469
135. Li C, Xie J, Chen X, Mo Z, Wu W, Liang Y, et al. Comparison of Helicobacter pylori urease inhibition by rhizoma coptidis, cortex phellodendri and berberine: mechanisms of interaction with the sulfhydryl group. Planta Med. (2016) 82:305–11. doi: 10.1055/s-0035-1558229
136. Chen X, Wang R, Bao C, Zhang J, Zhang J, Li R, et al. Palmatine ameliorates Helicobacter pylori-induced chronic atrophic gastritis by inhibiting MMP-10 through ADAM17/EGFR. Eur J Pharmacol. (2020) 882:173267. doi: 10.1016/j.ejphar.2020.173267
137. Yu XD, Zheng RB, Xie JH, Su JY, Huang XQ, Wang YH, et al. Biological evaluation and molecular docking of baicalin and scutellarin as Helicobacter pylori urease inhibitors. J Ethnopharmacol. (2015) 162:69–78. doi: 10.1016/j.jep.2014.12.041
138. Song X, He Y, Liu M, Yang Y, Yuan Y, Yan J, et al. Mechanism underlying Polygonum capitatum effect on Helicobacter pylori-associated gastritis based on network pharmacology. Bioorg Chem. (2021) 114:105044. doi: 10.1016/j.bioorg.2021.105044
139. Yang T, Wang R, Zhang J, Bao C, Zhang J, Li R, et al. Mechanism of berberine in treating Helicobacter pylori induced chronic atrophic gastritis through IRF8-IFN-γ signaling axis suppressing. Life Sci. (2020) 248:117456. doi: 10.1016/j.lfs.2020.117456
140. Yang T, Wang R, Liu H, Wang L, Li J, Wu S, et al. Berberine regulates macrophage polarization through IL-4-STAT6 signaling pathway in Helicobacter pylori-induced chronic atrophic gastritis. Life Sci. (2021) 266:118903. doi: 10.1016/j.lfs.2020.118903
141. Wu X, Li X, Dang Z, Jia Y. Berberine demonstrates anti-inflammatory properties in Helicobacter pylori-infected mice with chronic gastritis by attenuating the Th17 response triggered by the B cell-activating factor. J Cell Biochem. (2018) 119:5373–81. doi: 10.1002/jcb.26681
142. Hu Q, Peng Z, Li L, Zou X, Xu L, Gong J, et al. The efficacy of berberine-containing quadruple therapy on Helicobacter Pylori eradication in China: a systematic review and meta-analysis of randomized clinical trials. Front Pharmacol. (2019) 10:1694. doi: 10.3389/fphar.2019.01694
143. Huang YQ, Huang GR, Wu MH, Tang HY, Huang ZS, Zhou XH, et al. Inhibitory effects of emodin, baicalin, schizandrin and berberine on hefA gene: treatment of Helicobacter pylori-induced multidrug resistance. World J Gastroenterol. (2015) 21:4225–31. doi: 10.3748/wjg.v21.i14.4225
Keywords: Helicobacter pylori, eradication therapy, stomach cancer, dual therapy, complementary therapy, elderly
Citation: Huang Q, Jia X, Chu Y, Zhang X and Ye H (2021) Helicobacter pylori Infection in Geriatric Patients: Current Situation and Treatment Regimens. Front. Med. 8:713908. doi: 10.3389/fmed.2021.713908
Received: 10 July 2021; Accepted: 03 September 2021;
Published: 30 September 2021.
Edited by:
Andrea P. Rossi, Integrated University Hospital Verona, ItalyReviewed by:
Claudio de Lucia, Sapienza University of Rome, ItalyCopyright © 2021 Huang, Jia, Chu, Zhang and Ye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuezhi Zhang, emhhbmcueHVlemhpQDI2My5uZXQ=; Hui Ye, YnJpZ2h0bGVhZjcyM0AxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.