 Stéphane Bonacorsi1*
Stéphane Bonacorsi1* Benoit Visseaux2,3
Benoit Visseaux2,3 Donia Bouzid2,4
Donia Bouzid2,4 Josep Pareja5
Josep Pareja5 Sonia N. Rao6Davide Manissero7Glen Hansen8,9
Sonia N. Rao6Davide Manissero7Glen Hansen8,9 Jordi Vila10
Jordi Vila10- 1Department of Microbiology, Robert Debré University Hospital, AP-HP, Paris, France
- 2Université de Paris, IAME, INSERM, Paris, France
- 3Université de Paris, Laboratoire de Virologie, Hôpital Bichat Claude Bernard, Assistance Publique-Hôpitaux de Paris, Paris, France
- 4Université de Paris, Service d'Accueil des Urgences, Hôpital Bichat Claude Bernard, Assistance Publique-Hôpitaux de Paris, Paris, France
- 5STAT-Dx Life, S.L. (a QIAGEN Company), Medical Affairs, Barcelona, Spain
- 6QIAGEN Inc., Medical Affairs, Germantown, MD, United States
- 7QIAGEN Manchester Ltd, Medical Affairs, Manchester, United Kingdom
- 8Microbiology and Molecular Diagnostics, Hennepin County Medical Center, Department of Infectious Diseases, School of Medicine, University of Minnesota, Minneapolis, MN, United States
- 9Department of Pathology and Laboratory Medicine, School of Medicine, University of Minnesota, Minneapolis, MN, United States
- 10Biomedical Diagnostic Centre, Department of Clinical Microbiology, Institute of Global Health, School of Medicine, Hospital Clinic, University of Barcelona, Barcelona, Spain
Background: Quantitative (q) polymerase chain reaction (PCR) cycle threshold (Ct) values represent the number of amplification cycles required for a positive PCR result and are a proxy of pathogen quantity in the tested sample. The clinical utility of Ct values remains unclear for gastrointestinal infections.
Objectives: This systematic review assesses the global medical literature for associations between Ct values of gastrointestinal pathogens and patient presentation and clinical outcomes.
Data Sources: MEDLINE, EMBASE, Cochrane library databases: searched January 14–17, 2020.
Study Eligibility Criteria: Studies reporting on the presence or absence of an association between Ct values and clinical outcomes in adult and pediatric populations were included. Animal studies, reviews, meta-analyses, and non-English language studies were excluded.
Participants: Humans infected with gastrointestinal pathogens, detected with qPCR.
Interventions: Diagnostics assessing Ct values. Extracted data were reported narratively.
Results: Thirty-three eligible studies were identified; the most commonly studied pathogens were Clostridioides difficile (n = 15), norovirus (n = 10), and rotavirus (n = 9). Statistically significant associations between low C. difficile Ct values and increased symptom severity or poor outcome were reported in 4/8 (50%) studies, and increased risk of death in 1/2 (50%) studies; no significant associations were found between Ct value and duration of symptoms or length of hospital stay. Among studies of norovirus, 5/7 (71%), mainly genogroup II, reported symptomatic cases with significantly lower median Ct values than controls. Significantly lower rotavirus Ct values were also observed in symptomatic cases vs. controls in 3/7 (43%) studies, and associated with more severe symptoms in 2/2 studies. Contradictory associations were identified for non-C. difficile bacterial and parasitic pathogens.
Conclusions: In conclusion, some studies reported clinically useful associations between Ct values and patient or healthcare outcomes; additional, well-designed, large-scale trials are warranted based on these findings.
Systematic Review Registration: [PROSPERO], identifier [CRD42020167239].
Introduction
Gastrointestinal infections contribute significantly to the burden of illness from infectious diseases worldwide (1, 2). Rotavirus is the principal cause of diarrhea mortality, responsible for a high attributable fraction among all age groups (13.9%) (3). Shigella, the second most common cause of diarrhea mortality, is a key contributor to diarrheal death among children younger than 5 years (14.3%), mainly in low income countries (3).
Quantitative (q) polymerase chain reaction (PCR) is a robust and increasingly common methodology for rapid syndromic testing due to its sensitivity and specificity for identification of pathogens. In infectious diseases, qPCR cycle threshold (Ct) values represent the number of amplification cycles required for the fluorescent signal to exceed the basal threshold level. Ct values are inversely related to the number of copies of the target gene in a sample, meaning that lower Ct values correlate with higher pathogen loads. In infectious diseases, qPCR Ct values have potential utility in providing clinicians with information regarding genomic load that may help guide clinical and infection-control decisions. In addition, Ct values may help to clarify diagnostic uncertainty in cases where there is difficulty interpreting binary results, for example when distinguishing between causative infectious pathogen and asymptomatic carriage/colonization (4–6), particularly as identification of multiple pathogens is common (7, 8).
Notably, unprecedented challenges from the COVID-19 pandemic have raised the interest in clinical and diagnostic utility of Ct values (9, 10). However, in a recent systematic review of the utility of Ct values in respiratory infections (parallel to this study), no universal conclusions could be reached [In press: J Antimicrob Chemother 2021]. This systematic review assesses the global medical literature for associations between Ct values of gastrointestinal pathogens and patient or healthcare outcomes.
Methods
This systematic review was undertaken according to the principles outlined in the Cochrane handbook and guidance published by the Center for Reviews and Dissemination. The original protocol was published in the PROSPERO database (CRD42020167239) and included broad search terms unrestricted by pathogen or disease type. This review focuses on gastrointestinal pathogens.
Eligibility Criteria
Literature searches of MEDLINE, EMBASE, and the Cochrane Library using search tools at ncbi.nlm.nih.gov/pubmed, embase.com and cochranelibrary.com were undertaken to identify studies reporting on the presence or absence of an association between qPCR Ct values and patient or healthcare outcomes (see Supplementary Table 1 for the PubMed search strategy). The search strategy comprised three concepts: (real-time [rt]-PCR OR qPCR) AND Ct values AND pathogen. Randomized-controlled, single-arm, non-randomized comparative and observational (retrospective or prospective) studies were included. Animal studies, systematic reviews, non-systematic reviews and meta-analyses were excluded; however, additional publications were identified by manual citation searching of appropriate reviews. Searches were limited to English language studies, for reasons of feasibility.
Study Selection and Data Extraction
Titles and abstracts were screened, based on eligibility criteria, for inclusion by two independent reviewers who then assessed the full texts of relevant studies; a third reviewer resolved conflicts. Key data from all included studies were captured by one reviewer, and subsequently verified by another reviewer. Outcomes were broadly divided into the following categories: mortality, symptomatic vs. asymptomatic, severity of symptoms, duration of symptoms, intensive care unit (ICU) admission, hospitalization and length of stay (LOS).
The quality and risk of bias of each study was assessed using a tool relevant for each study design (Newcastle Ottawa Scale for cross-sectional, cohort, and case-control studies (11).
Results
Overview of Studies Included
Literature searches, conducted January 14–17, 2020, identified 1,029 unique records. Application of distinct screening and restriction parameters specific to gastrointestinal infections identified 33 eligible studies. Most studies reported Ct value association for more than one pathogen; the most commonly studied pathogens were Clostridioides difficile (n = 15), norovirus (n = 10), and rotavirus (n = 9) (Figure 1). All studies identified gastrointestinal pathogens from stool samples. In studies of C. difficile, the majority used genes encoding toxin A or B as PCR targets.
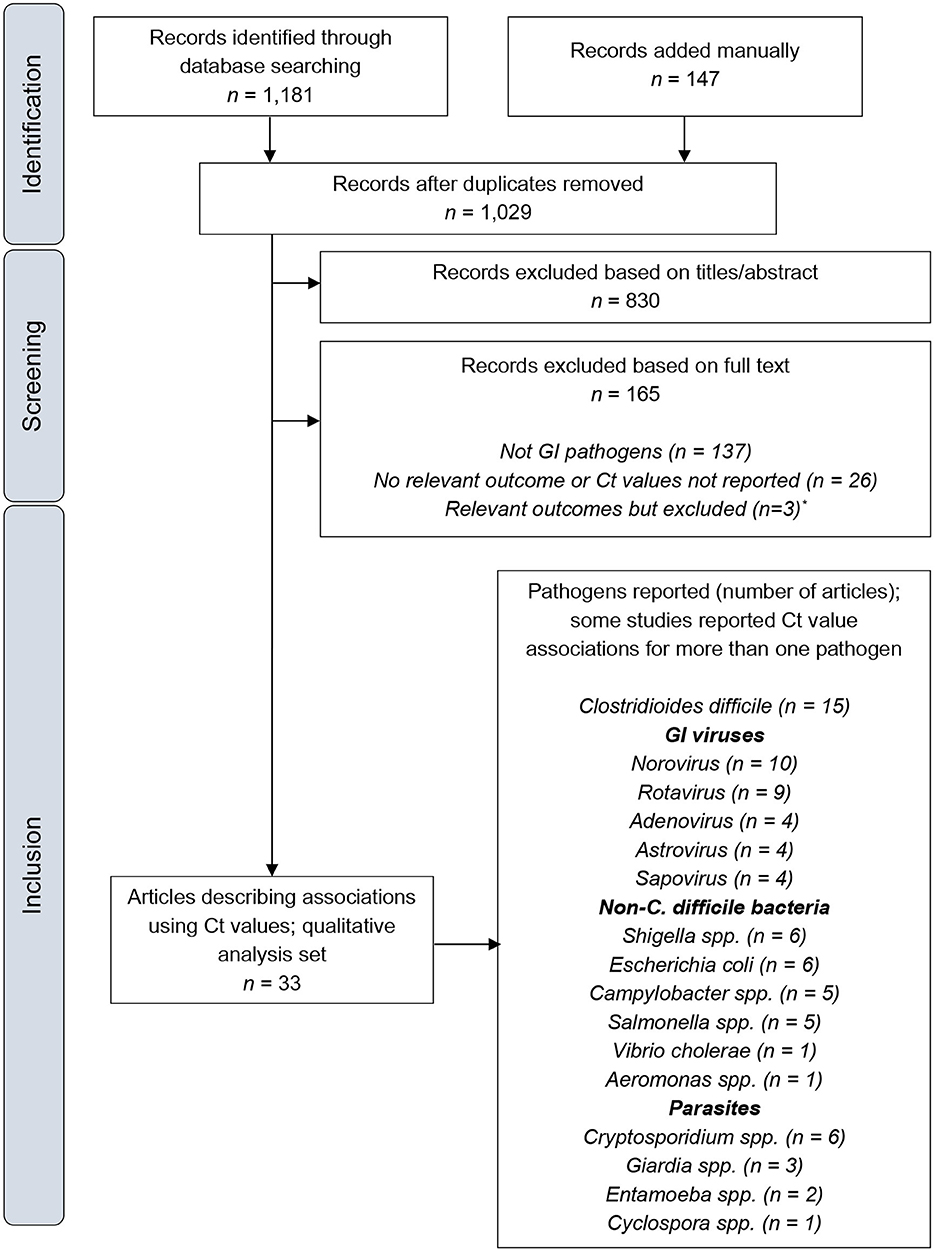
Figure 1. PRISMA flow diagram. Ct, cycle threshold; GI, gastrointestinal. *Details of these publications are provided in the Supplementary Material.
The majority of outcomes reported were related to symptoms, including symptom severity, symptomatic vs. asymptomatic and duration of symptoms. Mortality was assessed by three studies. No studies investigated associations between Ct values and hospitalization and/or ICU admission. The majority (84.8%; 28/33) of studies did not report normalized Ct values. Some (66.7%; 22/33) studies presented Ct value distributions.
Quality and Bias
Using Newcastle-Ottawa scales, all cross-sectional studies, cohort studies and case-control studies were classed as being of poor quality (Supplementary Tables 2–4, respectively). This was generally due to a lack of comparability between groups, insufficient or unjustified sample sizes, the use of non-representative samples (often hospitalized patients or age-specific populations) and a lack of detail regarding patient follow-up or non-response; ascertainment of exposure and outcome was usually appropriate. In an assessment of qPCR methodology, 14/29 (48%) full-length articles were considered to have some or many gaps in the reported methodology (Supplementary Table 5).
Clostridioides difficile
C. difficile was the most commonly reported gastrointestinal pathogen with respect to articles describing associations between Ct values and patient or healthcare outcomes (Table 1). Two studies investigated the association of Ct value with mortality, of which one (N = 1,013) reported no significant associations (12). The second study, conducted by Davies et al. at four UK hospitals, was the largest C. difficile assessment in this systematic review (N = 1,281). The authors reported significantly lower median Ct values for patients who died with C. difficile infection compared with those who survived [25.5 (n = 123) vs. 27.5 (n = 762), respectively; p = 0.021] (13).
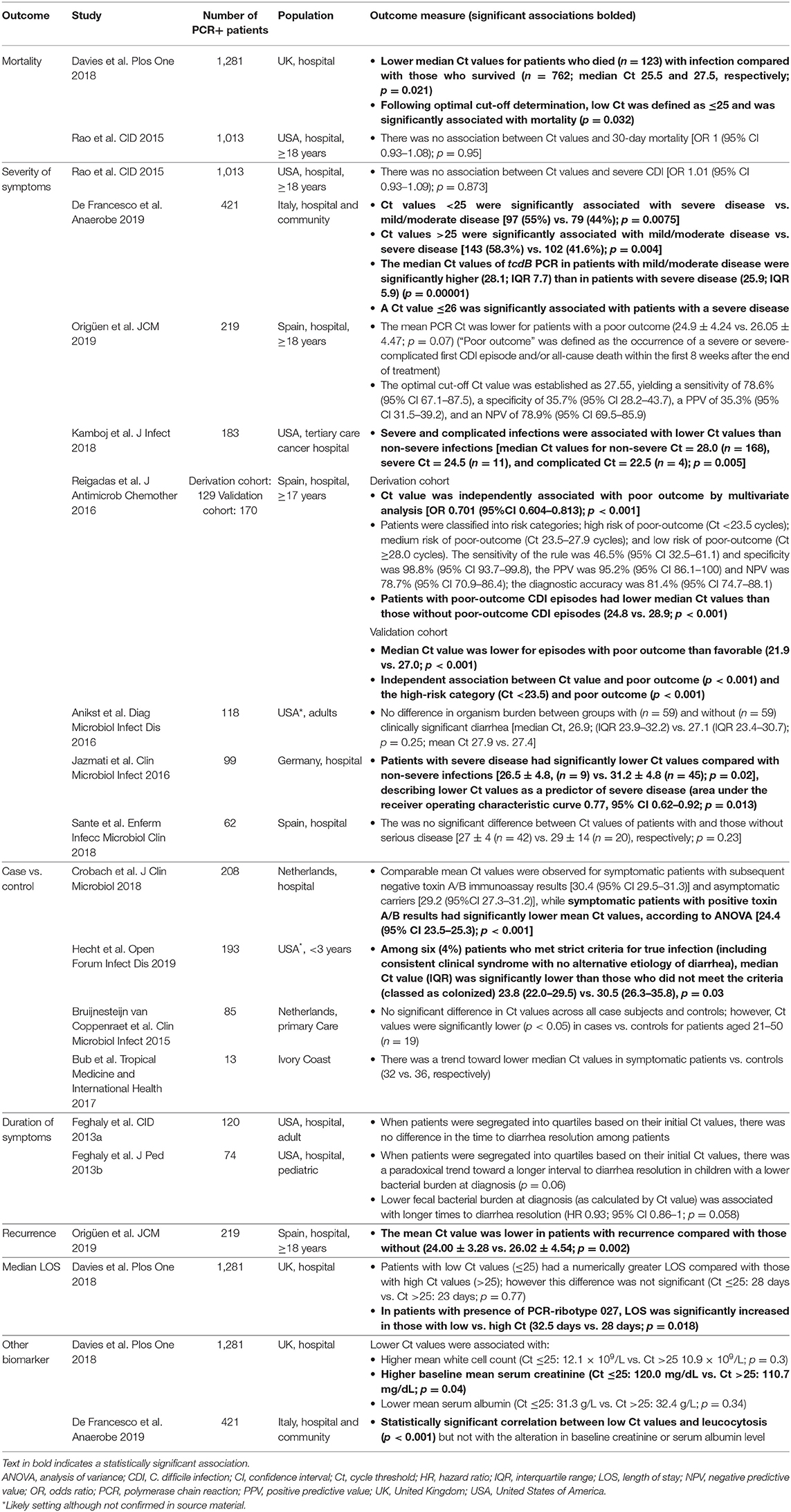
Table 1. Summary of studies that assessed PCR Ct values for C. difficile infections against patient clinical presentation and outcomes.
Among 12 articles reporting associations between Ct values and symptoms, eight investigated severity of symptoms. Three studies reported significantly lower median Ct values in patients with severe or complicated disease vs. those with mild/moderate disease: De Francesco et al. (N = 421) severe 25.9 (n = 199) vs. mild/moderate 28.1 (n = 222), p = 0.00001; Jazmati et al. (N = 99) severe 26.5 vs. mild/moderate 31.2, p = 0.02; Kamboj et al. (N = 183) severe 24.5, complicated 22.5, and non-severe 28.0, p = 0.005 (14–16). Jazmati et al. further described lower Ct values as a predictor of severe disease [area under the receiver operating characteristic curve 0.77, 95% confidence interval (CI) 0.62–0.92; p = 0.013] (14). Reigadas et al. (n = 299) showed that Ct value was independently associated with poor outcome (p < 0.001) and classified patients into risk categories accordingly; high risk of poor outcome (median Ct <23.5); medium risk of poor outcome (median Ct 23.5–27.9); and low risk of poor outcome (median Ct ≥28.0) (17). A further three studies with numbers of PCR-positive patients ranging from 62 to 219, reported lower Ct values in patients with poorer outcomes or more severe disease; however, differences did not reach statistical significance (18–20).
Four studies investigated differences in Ct values in case vs. control subjects. In Crobach et al. (N = 208) mean quantification cycle (Cq) values were significantly lower (p < 0.001) in symptomatic patients who were toxin A/B-positive by enzyme immunoassay (24.4, 95% CI 23.5–25.3) than symptomatic patients who were toxin A/B-negative (30.4, 95% CI 29.5–31.3) and asymptomatic carriers (29.2, 95% CI 27.3–31.2) (5). Similar observations were reported in pediatric patients by Bub et al. (N = 13; median Ct 32 in symptomatic cases vs. 36 in controls, no significance reported) and Hecht et al. (N = 193; median Ct 23.8 in true infections vs. 30.5 in colonized, p = 0.03) (6, 21). In a study (n = 85) by Bruijnesteijn van Coppenraet et al., although no significant difference in Ct values were observed between cases and controls across all subjects, Ct values were significantly lower in cases vs. controls for age group 21–50 years (22).
Two studies (N ≤ 120) investigated association of Ct value with duration of symptoms; no significant associations were reported in either study (23, 24). One large study (N = 1,281) of diarrheal patients in the UK investigated Ct value and LOS; however, no significant associations were reported, except for patients with PCR-ribotype 027, where LOS was significantly increased in those with low vs. high Ct value (32.5 vs. 28 days; p = 0.018) (13).
Gastrointestinal Viruses
Associations between patient or healthcare outcomes and the Ct value of gastrointestinal viruses were investigated in 14 studies, with the most commonly studied viruses being norovirus and rotavirus (n = 10 and n = 9, respectively) (Table 2). The majority of studies (n = 10) investigated the difference in Ct values (or viral load derived from Ct values) between cases and controls (symptomatic and asymptomatic, or patients with or without diarrhea).
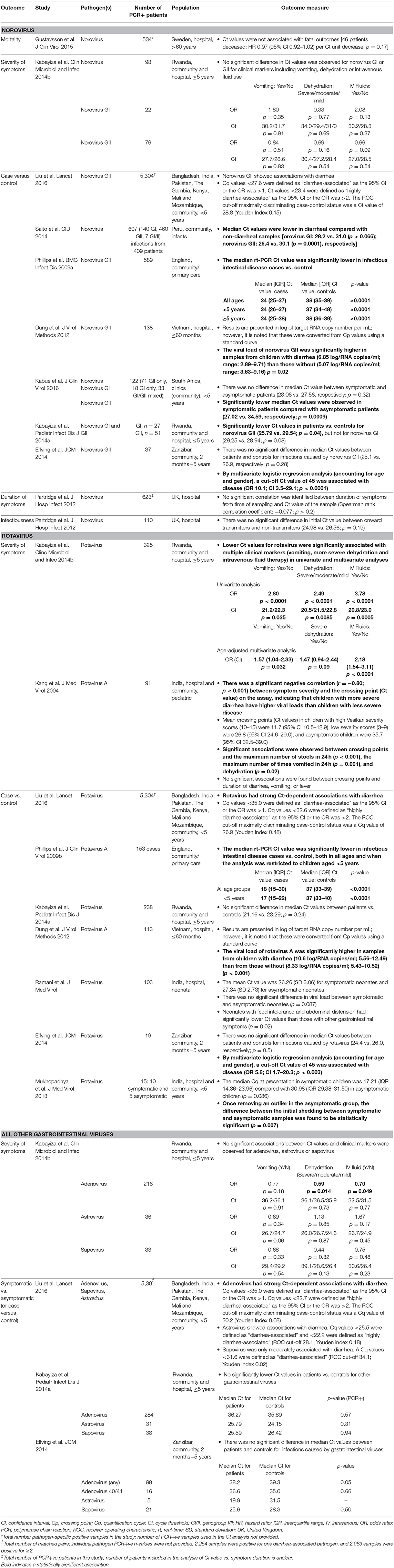
Table 2. Summary of studies that assessed PCR Ct values for gastrointestinal viruses against patient clinical presentation and outcomes.
In general, norovirus, particularly norovirus genogroup II (GII), infections were found to have significantly lower median Ct values in infections vs. controls. Kabue et al. (N = 122) reported that lower median Ct values were observed in symptomatic pediatric patients compared with asymptomatic pediatric patients infected with norovirus GII (n = 104; 27.0 vs. 34.6; p = 0.0009) (25). Similar outcomes were reported in Kabayiza et al. (n = 51; 25.8 vs. 29.5; p = 0.04), Phillips et al. (n = 589; 34 vs. 37; p < 0.0001), Saito et al. (n = 467; 26.4 vs. 30.1; p = 0.0001), and Dung et al. (n = 138; 6.85 log copies/ml vs. 5.07 log copies/ml; p = 0.02) (4, 26–28). Additionally, Liu et al. reported a pathogen quantity-dependent association with diarrhea in children <5 years old (29). Elfving et al. also reported lower median Ct values in patients vs. controls, but the difference was not significant (25.1 vs. 26.9; p = 0.28) (30).
One study investigated Ct values of norovirus GII and fatal outcomes (n = 534) and found no association (31). One other study reported no significant associations between Ct values and symptom duration (n = 623) or infectiousness (n = 110) in patients with infections caused by norovirus (32).
Similar to norovirus, multiple studies showed significantly lower Ct values (or Cq) in cases of symptomatic rotavirus infection vs. controls. Phillips et al. (N = 153) reported lower median Ct values in rotavirus intestinal infections vs. controls (18 vs. 37; p < 0.0001) (33). Dung et al. (n = 113) reported significantly higher median viral loads in children with diarrhea compared with those without (10.6 log copies/ml vs. 8.33 log copies/ml; p < 0.001) (26), and one study in children <5 years by Liu et al. reported strong pathogen quantity-dependent associations with diarrhea (29). Supporting these observations, Kabayiza et al. (n = 325) reported that lower median Ct values were significantly associated with more severe symptoms, including vomiting, severe dehydration and intravenous fluid therapy, in patients with infections caused by rotavirus (27). Kang et al. (N = 91) also reported significant associations between severe diarrhea and low Ct values (reported as “crossing points”) (34). Four further studies also reported lower median Ct values in patients vs. controls/asymptomatic patients, but differences did not reach statistical significance: Elfving et al. (n = 19; 24.4 vs. 26.0; p = 0.50); Kabayiza et al. (n = 238; 21.16 vs. 23.29; p = 0.24); Ramani et al. (n = 103; 26.26 vs. 27.34; p = 0.087) and Mukhopadhya et al. (n = 15; 17.21 vs. 30.98; p = 0.086) (27, 30, 35, 36). Notably, adjustment of an outlier in the study by Mukhopadhya et al. resulted in the difference reaching statistical significance (p = 0.007) (36).
Three studies investigated gastrointestinal viruses other than norovirus and rotavirus. In one study that investigated pathogen quantity and diarrhea in children <5 years old, associations between Ct value and diarrhea were reported for cases of adenovirus and astroviruses (29). No other associations between Ct values and cases vs. controls were identified (27, 30).
Non-C. difficile Bacterial and Parasitic Pathogens
Associations between patient clinical outcomes and the Ct value of non-C. difficile bacterial and parasitic pathogens were investigated in nine studies (Table 3).
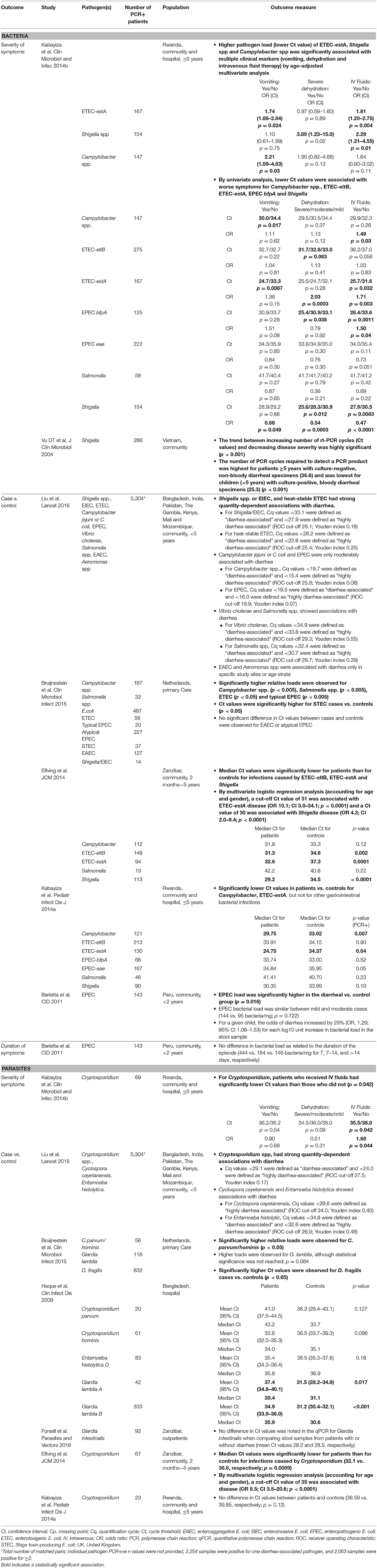
Table 3. Summary of studies that assessed PCR Ct values for non-C. difficile bacterial and parasitic pathogens against patient clinical presentation and outcomes.
Among bacterial studies, the majority investigated associations between quantitative PCR-derived bacterial loads and cases vs. controls (symptomatic vs. asymptomatic, or patients with vs. without diarrhea), and most studies found significant associations. Among five studies reporting differences in Ct values between cases vs. controls, significantly lower median Ct values were reported in cases of enterotoxigenic Escherichia coli (ETEC), enteropathogenic E. coli (EPEC), Campylobacter spp., enteroinvasive E. coli (EIEC)/Shigella spp., and Salmonella spp. (22, 27, 29, 30, 37). However, associations were not consistent across studies, including two reports (n = 9 and n = 46) of no significant difference in cases vs. controls for Salmonella spp. (27, 30). In one study, associations were notably weaker for Campylobacter spp. and typical EPEC (29). In a study (n = 143) of patients with EPEC, a 29% increase in risk of diarrhea was observed for each log10 unit increase (calculated by Ct value) in bacterial load (OR 1.29; 95% CI 1.08–1.53) (37).
Two studies also investigated associations between Ct values and bacterial disease severity. In cases of EIEC/Shigella spp., lower Ct values were significantly associated with higher vs. lower categories of disease severity (n = 286; Ct value 25.3 vs. 36.6), dehydration (n = 154; OR 3.89; p = 0.02), and requirement for intravenous fluids (n = 154; OR 2.29; p = 0.01) (27, 38). Lower Ct values for ETEC-estA were significantly associated with vomiting (n = 167; OR 1.74; p = 0.024) and with intravenous fluids (n = 167; OR 1.81; p = 0.004), and Campylobacter spp. with vomiting (n = 147; OR 2.21; p = 0.03) (27).
One study (n = 143) investigated the effect of EPEC bacterial load on the duration of symptoms; however, no significant association was observed (37).
All studies of parasites investigated associations between Ct values (or Cq) and cases vs. controls (symptomatic vs. asymptomatic, or patients with vs. without diarrhea). In studies including Cryptosporidium spp., two reported significantly lower Ct values in cases vs. controls, including Elfving et al. (n = 67; median Ct 32.1 vs. 36.8; p = 0.0009) (22, 30). One further study also reported lower Ct values in cases vs. controls (n = 23), but did not reach statistical significance (27). Furthermore, and contrary to expected results, Haque et al. reported higher mean Ct values in Cryptosporidium parvum and Cryptosporidium hominus cases than controls, although the differences were not significant (p = 0.127 and 0.098) (39). In a study in children <5 years (n = N/A), strong pathogen quantity-dependent associations with diarrhea were reported in cases of Cryptosporidium spp. (29). Among three studies including Giardia spp. (n = 118, n = 375 and n = 92), none reported statistically significant lower Ct values in cases vs. controls (22, 39, 40). Notably, Haque et al. reported that Giardia lamblia parasite load, as measured by Ct values, was inversely related to diarrhea, which the authors suggest could be related to the primary role played by the immune system in diarrheal illness that results from these infections (39).
Discussion
The objective of this systematic review was to assess the global medical literature for any correlation between Ct values and clincal outcomes of patients with gastrointestinal infections. Lower Ct values correspond with greater quantities of detectible target gene and therefore a higher pathogen load, which may correspond with less favorable clinical outcomes. Here we report outcomes from studies identified that report on gastrointestinal pathogens only. This review gathers data from 33 studies, with the largest number of studies for C. difficile (n = 15). The most common outcomes reported were related to symptoms, including case vs. control, with vs. without diarrhea, and severity of symptoms.
Evidence in this review suggests associations between Ct values and symptomatic C. difficile infections. Four out of eight studies reporting the association between lower Ct values and increased disease severity found the association to be significant, including two studies that reported lower Ct values as a predictor of poor outcome (14, 17). Furthermore, 2/4 case vs. control studies reported significantly lower Ct values in symtomatic cases. Most of the C. difficile studies reported genes encoding toxin A/B as the target for PCR diagnostics, which when detected by other methods, is generally inferred as marker of disease severity (5).
All studies of norovirus and rotavirus reported lower Ct values in cases vs. controls; the majority for norovirus GII and ~50% for rotavirus reported significant differences. Furthermore, two studies of rotavirus infections reported significant associatons between lower Ct values and severity of symptoms, including vomiting, severe dehydration and administering intravenous fluids (27, 34). Notably, the association of Ct values and symptom severity was more pronounced for norovirus GII than norovirus GI (25, 27, 28). One possible explanation for this is the increased virulence observed with GII infection compared with other norovirus genogroups (41), although more investigation is necessary to draw firm conclusions.
This review found less evidence for the clinical utility of Ct values in non-C. difficile bacterial and parasitic infections compared with C. difficile and gastrointestinal viruses. Multiple studies reported significant associations between bacterial loads and symptomatic cases, particularly for Shigella (29, 30). Two studies reported Shigella association with symptom severity (27, 38). Inconsistencies were found in studies of parasitic infections; some studies indicated an association between low Ct values and symptomatic infection in patients with Cryptosporidium spp., however, evidence is limited (22, 29, 30). There is insufficient evidence to draw conclusions for other parasitic infections.
Among the studies included in this review, evidence suggests that Ct values may have utility in defining symptomatic causality, particularly in cases of polymicrobial infection. In one study of norovirus-positive samples, coinfection with rotavirus was observed in 3.7 and 7.4% of asymptomatic and diarrheal samples, respectively; probable etiology was determined based on relative Ct values, highlighting their utility for defining causitive organisms in this setting (28). Ct values may also aid causative diagnosis in patients with C. difficille infection, where asymptomatic colonization (5, 6), and coinfections have been reported (42). C. difficile fecal load is already considered to be of diagnostic utility in distinguishing between infection and colonization (43, 44). However, it is essential to consider Ct values within the context of clinical presentation rather than utilize Ct values as an independent marker of disease.
Despite multiple studies reporting significant associations between high genomic load (low Ct values) and symptomatic infections, particularly for C. difficile, norovirus and rotavirus, statistically significant evidence was inconsistent across studies despite similar trends. A possible explanation for this is the diversity of populations investigated across each study (e.g., hospital vs. community setting, pediatric vs. adult populations); adjusting for similar settings may uncover stronger trends toward Ct value and patient outcomes. Further assessments of associations between Ct values and LOS, hospital/ICU admission, for example, could also aid in understanding the utility of Ct values in the diagnosis of gastrointestinal infections.
When interpreting the studies in this systematic review, consideration must be given to the settings and populations in which they were conducted. Studies for some pathogens, such as norovirus, were conducted primarily in pediatric populations and as such their conclusions may not apply to adult populations. All but one of the studies investigating non-C. difficile bacterial pathogens and parasites were performed in non-industrialized countries; therefore, the clinical impact of Ct values for these pathogens in industrialized countries remains to be determined. Of the seven studies that detected parasites, five investigated a large list of GI pathogens and multiple pathogens were detected for 8–72% patients (22, 27, 29, 30). These studies highlight the utility of syndromic testing in gastrointestinal infection, where multiplex testing is able to detect more pathogens and co-infections than conventional methods (42). It should also be noted that multiplex PCR for GI pathogens does not currently provide a picture of the microbiome, whereas culture-based techniques are able to provide an understanding of dysbiosis resulting from GI infections.
Differences in study methodology and qPCR workflow are likely to impact Ct values, including: specimen source, collection method, transport media type and volume, stability, quality of the sample, time of sampling vs. onset of infection, master mix components, type and concentration of passive reference dye, reaction efficiency, inter- and intravariability in assay platforms, and whether they were single or multiplex systems. Methodologies varied widely between studies and many (39%) had some or many gaps in reporting defined standardized methodologies. Therefore, within-study variability may have limited the ability to detect associations. The majority (84.8%; 28/33) of studies did not report normalized Ct values, which would have provided more accurate estimations of genomic load for each sample. Although outside the scope of our review, we noted not all (66.7%; 22/33) studies presented Ct value distributions. Further studies to understand the distribution of Ct values in relation to patient outcomes across the populations would be necessary if Ct values are to be utilized in clinical decision-making. After data analysis had been completed, we became aware of the Minimum Information for Publication of Quantitative rt-PCR Experiments (MIQE) guidelines (45), which should be applied to laboratory-developed tests. Some of the studies utilized in this review use commercially available assays and, therefore, when implemented in clinical diagnostic routines, applicable validation, and verification using external controls are necessary. Due to the late discovery it was not possible to re-assess the studies using laboratory-developed assays with the MIQE guidelines in mind; however, we believe that assessment of study methodology using these guidelines would not significantly alter the findings of this systematic review.
There were a number of limitations to this systematic review. The protocol restricted articles referring to Ct values as a measure of genomic load, therefore studies which reported genomic load in measures other than Ct value were not picked up in the database searches or excluded from during screening. Furthermore, articles describing Ct values but with no mention of Ct values in the title, abstract or keywords, were not retrieved based on the search parameters used in the database searches. In addition, late in the review we became aware of alternative wording for Ct values, including Cq and “crossing point” [discussed in detail in (45)]; while we have added articles with these terms manually, it is possible that some may have been missed. Another limitation to this review was the assessment of all included studies as poor quality for bias by the Newcastle-Ottawa scale. This is due to the majority of studies reporting Ct values as secondary outputs, as opposed to seeking to compare clinical outcomes against Ct values. Consequently, the studies did not fully align with the risk and bias assessment. There was considerable variability between studies. Given the high heterogeneity between studies, it was not possible to conduct aggregated/meta-analyses, a key limitation in the scope of this review. A number of studies only made comparative analysis between symptomatic and asymptomatic cases, which limits the clinical utility of these studies in defining Ct values as a measure of disease severity. However, Ct values of asymptomatic patients still hold clinical value in order to discriminate between infection and colonization, an observation reported in multiple studies (4–6, 25, 27). A single reviewer conducted the data extraction and a second reviewer checked all the data points. Whilst an acceptable approach, the methodology could have been optimized by double independent reviewer data extraction with a third reviewer for discrepancy resolution. Due to the large number of studies identified as potential data sources for this review, the single-reviewer extraction method ensured that the review remained feasible. Despite these limitations, we believe this review provides insights into the potential clinical utility of gastrointestinal pathogen Ct values. In summary, there is evidence to support relationships between Ct values and clinical outcomes in gastrointestinal infections. Considered alongside clinical presentation, Ct values could help to guide treatment decisions, particularly in cases of C. difficile, where treatment is guided by severity of disease and asymptomatic colonization has been observed (5, 6, 46). This review did not uncover sufficient evidence to draw conclusions on the clinical utility of Ct values for non-C. difficile bacterial and parasitic infections. This systematic review is the first to assess the relationship between Ct values and clinical outcomes in gastrointestinal infections, large-scale clinical trials with endpoints centered on Ct values are warranted to draw definitive evidence.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
BV, DB, JP, SR, DM, GH, and JV were involved in conception and design of the study. All authors contributed to interpretation of the data, manuscript drafting and revision, and approved the submitted version.
Funding
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Isabella Talbot, BSc, of Ashfield MedComms, an Ashfield Health company, and funded by Qiagen Manchester Ltd. This study received funding from QIAGEN Manchester Ltd. The funder had the following involvement with the study: article processing fees and provision of medical writing support.
Conflict of Interest
JP, SR, and DM are employed by Qiagen. BV reports grants, personal fees and non-financial support from Qiagen, personal fees and non-financial support from BioMérieux, personal fees from Hologic, personal fees from Gilead, outside the submitted work. DB reports personal fees from Qiagen, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Qiagen Manchester Ltd. The funder had the following involvement in the study: article processing fees and provision of medical writing support. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.711809/full#supplementary-material
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
2. GBD 2017 Diarrhoeal Disease Collaborators. Quantifying risks and interventions that have affected the burden of diarrhoea among children younger than 5 years: an analysis of the Global Burden of Disease Study 2017. Lancet Infect Dis. (2020) 20:37–59. doi: 10.1016/S1473-3099(19)30401-3
3. GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. (2018) 18:1211–28. doi: 10.1016/S1473-3099(18)30362-1
4. Phillips G, Lopman B, Tam CC, Iturriza-Gomara M, Brown D, Gray J. Diagnosing norovirus-associated infectious intestinal disease using viral load. BMC Infect Dis. (2009) 9:63. doi: 10.1186/1471-2334-9-63
5. Crobach MJT, Duszenko N, Terveer EM, Verduin CM, Kuijper EJ. Nucleic acid amplification test quantitation as predictor of toxin presence in Clostridium difficile infection. J Clin Microbiol. (2018) 56:17. doi: 10.1128/JCM.01316-17
6. Hecht S, Wang H, Everhart K, Watson J, Leber A. Understanding the clinical implications of Clostridium difficile detection in the molecular age: colonization vs infection in children less than 3 years of age. Open Forum Infect Dis. (2019) 6:S812. doi: 10.1093/ofid/ofz360.2036
7. Pouletty M, De Pontual L, Lopez M, Morin L, Poilane I, Pham LL, et al. Multiplex PCR reveals a high prevalence of multiple pathogens in traveller's diarrhoea in children. Arch Dis Child. (2019) 104:141–6. doi: 10.1136/archdischild-2017-314327
8. Boers SA, Peters CJA, Wessels E, Melchers WJG, Claas ECJ. Performance of the QIAstat-Dx gastrointestinal panel for diagnosing infectious gastroenteritis. J Clin Microbiol. (2020) 58:e01737–19. doi: 10.1128/JCM.01737-19
9. Rao SN, Manissero D, Steele VR, Pareja J. A systematic review of the clinical utility of cycle threshold values in the context of COVID-19. Infect Dis Ther. (2020) 9:573–86. doi: 10.1007/s40121-020-00324-3
10. Rabaan AA, Tirupathi R, Sule AA, Aldali J, Mutair AA, Alhumaid S, et al. Viral dynamics and real-time RT-PCR Ct values correlation with disease severity in COVID-19. Diagnostics. (2021) 11:61091. doi: 10.3390/diagnostics11061091
11. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford (accessed September 03, 2021).
12. Rao K, Micic D, Natarajan M, Winters S, Kiel MJ, Walk ST, et al. Clostridium difficile ribotype 027: relationship to age, detectability of toxins A or B in stool with rapid testing, severe infection, and mortality. Clin Infect Dis. (2015) 61:233–41. doi: 10.1093/cid/civ254
13. Davies KA, Planche T, Wilcox MH. The predictive value of quantitative nucleic acid amplification detection of Clostridium difficile toxin gene for faecal sample toxin status and patient outcome. PLoS ONE. (2018) 13:e0205941. doi: 10.1371/journal.pone.0205941
14. Jazmati N, Hellmich M, Licanin B, Plum G, Kaasch AJ. PCR cycle threshold value predicts the course of Clostridium difficile infection. Clin Microbiol Infect. (2016) 22:e7–8. doi: 10.1016/j.cmi.2015.09.012
15. Kamboj M, Brite J, Mcmillen T, Robilotti E, Herrera A, Sepkowitz K, et al. Potential of real-time PCR threshold cycle (CT) to predict presence of free toxin and clinically relevant C. difficile infection (CDI) in patients with cancer. J Infect. (2018) 76:369–75. doi: 10.1016/j.jinf.2017.12.001
16. De Francesco MA, Lorenzin G, Piccinelli G, Corbellini S, Bonfanti C, Caruso A. Correlation between tcdB gene PCR cycle threshold and severe Clostridium difficile disease. Anaerobe. (2019) 59:141–4. doi: 10.1016/j.anaerobe.2019.06.017
17. Reigadas E, Alcala L, Valerio M, Marin M, Martin A, Bouza E. Toxin B PCR cycle threshold as a predictor of poor outcome of Clostridium difficile infection: a derivation and validation cohort study. J Antimicrob Chemother. (2016) 71:1380–5. doi: 10.1093/jac/dkv497
18. Anikst VE, Gaur RL, Schroeder LF, Banaei N. Organism burden, toxin concentration, and lactoferrin concentration do not distinguish between clinically significant and nonsignificant diarrhea in patients with Clostridium difficile. Diagn Microbiol Infect Dis. (2016) 84:343–6. doi: 10.1016/j.diagmicrobio.2015.11.022
19. Sante L, Pedroso Y, Castro B, Lecuona M. Is there a relationship between the polimerase chain reaction cycle threshold and the risk of severe Clostridium difficile infection? Enfermedades Infecciosas Microbiologia Clinica. (2018) 36:600–1. doi: 10.1016/j.eimce.2017.11.022
20. Origuen J, Orellana MA, Fernandez-Ruiz M, Corbella L, San Juan R, Ruiz-Ruigomez M, et al. Toxin B PCR amplification cycle threshold adds little to clinical variables for predicting outcomes in Clostridium difficile infection: a retrospective cohort study. J Clin Microbiol. (2019) 57:e01125–18. doi: 10.1128/JCM.01125-18
21. Bub F, Chatigre JK, Yao JA, Coulibaly JT, Von Mueller L, Polman K, et al. Polymerase chain reaction for the diagnosis of Clostridium difficile infection in patients with persistent digestive disorders and asymptomatic controls in Cote d'Ivoire. Trop Med Internat Health. (2017) 22:3S7.1. doi: 10.1097/MPG.0b013e3182999990
22. Bruijnesteijn Van Coppenraet LES, Dullaert-De Boer M, Ruijs GJHM, Van Der Reijden WA, Van Der Zanden AGM, Weel JFL, et al. Case–control comparison of bacterial and protozoan microorganisms associated with gastroenteritis: application of molecular detection. Clin Microbiol Infect. (2015) 21:592.e599–19. doi: 10.1016/j.cmi.2015.02.007
23. El Feghaly RE, Stauber JL, Deych E, Gonzalez C, Tarr PI, Haslam DB. Markers of intestinal inflammation, not bacterial burden, correlate with clinical outcomes in Clostridium difficile infection. Clin Infect Dis. (2013) 56:1713–21. doi: 10.1093/cid/cit147
24. El Feghaly RE, Stauber JL, Tarr PI, Haslam DB. Intestinal inflammatory biomarkers and outcome in pediatric Clostridium difficile infections. J Pediatr. (2013) 163:1697–704.e1692. doi: 10.1016/j.jpeds.2013.07.029
25. Kabue JP, Meader E, Hunter PR, Potgieter N. Norovirus prevalence and estimated viral load in symptomatic and asymptomatic children from rural communities of Vhembe district, South Africa. J Clin Virol. (2016) 84:12–8. doi: 10.1016/j.jcv.2016.09.005
26. Dung TT, Phat VV, Nga TV, My PV, Duy PT, Campbell JI, et al. The validation and utility of a quantitative one-step multiplex RT real-time PCR targeting rotavirus A and norovirus. J Virol Methods. (2013) 187:138–43. doi: 10.1016/j.jviromet.2012.09.021
27. Kabayiza JC, Andersson ME, Nilsson S, Bergstrom T, Muhirwa G, Lindh M. Real-time PCR identification of agents causing diarrhea in Rwandan children less than 5 years of age. Pediatr Infect Dis J. (2014) 33:1037–42. doi: 10.1097/INF.0000000000000448
28. Saito M, Goel-Apaza S, Espetia S, Velasquez D, Cabrera L, Loli S, et al. Multiple norovirus infections in a birth cohort in a Peruvian Periurban community. Clin Infect Dis. (2014) 58:483–91. doi: 10.1093/cid/cit763
29. Liu J, Platts-Mills JA, Juma J, Kabir F, Nkeze J, Okoi C, et al. Use of quantitative molecular diagnostic methods to identify causes of diarrhoea in children: a reanalysis of the GEMS case-control study. Lancet. (2016) 388:1291–301. doi: 10.1016/S0140-6736(16)31529-X
30. Elfving K, Andersson M, Msellem MI, Welinder-Olsson C, Petzold M, Bjorkman A, et al. Real-time PCR threshold cycle cutoffs help to identify agents causing acute childhood diarrhea in Zanzibar. J Clin Microbiol. (2014) 52:916–23. doi: 10.1128/JCM.02697-13
31. Gustavsson L, Westin J, Lindh M, Andersson LM. Faecal viral load does not predict short-term mortality in norovirus infection. J Clin Virol. (2015) 70:S57. doi: 10.1016/j.jcv.2015.07.135
32. Partridge DG, Evans CM, Raza M, Kudesia G, Parsons HK. Lessons from a large norovirus outbreak: impact of viral load, patient age and ward design on duration of symptoms and shedding and likelihood of transmission. J Hosp Infect. (2012) 81:25–30. doi: 10.1016/j.jhin.2012.02.002
33. Phillips G, Lopman B, Tam CC, Iturriza-Gomara M, Brown D, Gray J. Diagnosing rotavirus A associated IID: Using ELISA to identify a cut-off for real time RT-PCR. J Clin Virol. (2009) 44:242–5. doi: 10.1016/j.jcv.2008.12.001
34. Kang G, Iturriza-Gomara M, Wheeler JG, Crystal P, Monica B, Ramani S, et al. Quantitation of group A rotavirus by real-time reverse-transcription-polymerase chain reaction: correlation with clinical severity in children in South India. J Med Virol. (2004) 73:118–22. doi: 10.1002/jmv.20053
35. Ramani S, Sankaran P, Arumugam R, Sarkar R, Banerjee I, Mohanty I, et al. Comparison of viral load and duration of virus shedding in symptomatic and asymptomatic neonatal rotavirus infections. J Med Virol. (2010) 82:1803–7. doi: 10.1002/jmv.21872
36. Mukhopadhya I, Sarkar R, Menon VK, Babji S, Paul A, Rajendran P, et al. Rotavirus shedding in symptomatic and asymptomatic children using reverse transcription-quantitative PCR. J Med Virol. (2013) 85:1661–8. doi: 10.1002/jmv.23641
37. Barletta F, Ochoa TJ, Mercado E, Ruiz J, Ecker L, Lopez G, et al. Quantitative real-time polymerase chain reaction for enteropathogenic Escherichia coli: a tool for investigation of asymptomatic versus symptomatic infections. Clin Infect Dis. (2011) 53:1223–9. doi: 10.1093/cid/cir730
38. Vu DT, Sethabutr O, Von Seidlein L, Tran VT, Do GC, Bui TC, et al. Detection of Shigella by a PCR assay targeting the ipaH gene suggests increased prevalence of shigellosis in Nha Trang, Vietnam. J Clin Microbiol. (2004) 42:2031–5. doi: 10.1128/JCM.42.5.2031-2035.2004
39. Haque R, Mondal D, Karim A, Molla IH, Rahim A, Faruque AS, et al. Prospective case-control study of the association between common enteric protozoal parasites and diarrhea in Bangladesh. Clin Infect Dis. (2009) 48:1191–7. doi: 10.1086/597580
40. Forsell J, Granlund M, Samuelsson L, Koskiniemi S, Edebro H, Evengard B. High occurrence of Blastocystis sp. subtypes 1-3 and Giardia intestinalis assemblage B among patients in Zanzibar. Tanzania Parasit Vectors. (2016) 9:370. doi: 10.1186/s13071-016-1637-8
41. Huhti L, Szakal ED, Puustinen L, Salminen M, Huhtala H, Valve O, et al. Norovirus GII-4 causes a more severe gastroenteritis than other noroviruses in young children. J Infect Dis. (2011) 203:1442–4. doi: 10.1093/infdis/jir039
42. Stockmann C, Rogatcheva M, Harrel B, Vaughn M, Crisp R, Poritz M, et al. How well does physician selection of microbiologic tests identify Clostridium difficile and other pathogens in paediatric diarrhoea? Insights using multiplex PCR-based detection. Clin Microbiol Infect. (2015) 21:179.e179–15. doi: 10.1016/j.cmi.2014.07.011
43. Leslie JL, Cohen SH, Solnick JV, Polage CR. Role of fecal Clostridium difficile load in discrepancies between toxin tests and PCR: is quantitation the next step in C. difficile testing? Eur J Clin Microb Infect Dis. (2012) 31:3295–9. doi: 10.1007/s10096-012-1695-6
44. Dionne L-L, Raymond F, Corbeil J, Longtin J, Gervais P, Longtin Y. Correlation between Clostridium difficile bacterial load, commercial real-time PCR cycle thresholds, and results of diagnostic tests based on enzyme immunoassay and cell culture cytotoxicity assay. J Clin Microbiol. (2013) 51:3624–30. doi: 10.1128/JCM.01444-13
45. Bustin SA, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. (2009) 55:611–22. doi: 10.1373/clinchem.2008.112797
46. Public Health England. Updated Guidance on the Management and Treatment of Clostridium difficile Infection. (2013). Available online at: https://www.gov.uk/government/publications/clostridium-difficile-infection-guidance-onmanagement-and-treatment (accessed March 31, 2021).
Keywords: cycle threshold, pathogen load, gastrointestinal pathogens, systematic review, qPCR, clinical outcomes
Citation: Bonacorsi S, Visseaux B, Bouzid D, Pareja J, Rao SN, Manissero D, Hansen G and Vila J (2021) Systematic Review on the Correlation of Quantitative PCR Cycle Threshold Values of Gastrointestinal Pathogens With Patient Clinical Presentation and Outcomes. Front. Med. 8:711809. doi: 10.3389/fmed.2021.711809
Received: 26 May 2021; Accepted: 19 August 2021;
Published: 23 September 2021.
Edited by:
Sergio Oscar Angel, CONICET Instituto Tecnológico de Chascomús (INTECH), ArgentinaReviewed by:
Alpha Fardah Athiyyah, Airlangga University, IndonesiaMark Poritz, Idaho Molecular Inc., United States
Graciela Castro Escarpulli, Instituto Politécnico Nacional de México (IPN), Mexico
Copyright © 2021 Bonacorsi, Visseaux, Bouzid, Pareja, Rao, Manissero, Hansen and Vila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stéphane Bonacorsi, c3RlcGhhbmUuYm9uYWNvcnNpQGFwaHAuZnI=