 Min Liu
Min Liu Zhijun Zhu
Zhijun Zhu Liying Sun
Liying Sun
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 04 October 2021
Sec. Gastroenterology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.687028
This article is part of the Research Topic Women in Science - Gastroenterology 2021 View all 12 articles
Objectives: Invasive fungal infection (IFI) remains an important cause of mortality in liver transplantation (LT). The objective of this meta-analysis was to identify the risk factors for IFI after LT.
Methods: We searched for relevant studies published up to June 2020 from PubMed, Web of Science, Embase, and the Cochrane Library. Odds ratios (ORs) and their corresponding 95% CIs were used to identify significant differences in the risk factors. Heterogeneity between studies was evaluated by the I2 test, and potential publication bias was assessed with Egger's test. The quality of included studies was evaluated with the Newcastle-Ottawa Scale (NOS).
Results: A total of 14 studies enrolling 4,284 recipients were included in the meta-analysis. Reoperation (OR = 2.18, 95% CI: 1.61–2.94), posttransplantation dialysis (OR = 2.03, 95% CI: 1.52–2.72), bacterial infection (OR = 1.81, 95% CI: 1.33–2.46), live donor (OR = 1.78, 95% CI: 1.20–2.63), retransplantation (OR = 2.45, 95% CI: 1.54–3.89), and fungal colonization (OR = 2.60, 95% CI: 1.99–3.42) were associated with the risk factors of IFI after LT.
Conclusions: Despite some risk factors that have been identified as significant factors for IFI post-LT, which may inform prevention recommendations, rigorous and well-designed studies with adequate sample sizes should be conducted to solve the limitations of this study.
Since the first liver transplantation (LT) by Thomas Starzl in 1963, the prognosis was significantly improved. LT can be considered the most effective therapy for nearly all causes of end-stage liver diseases (ESLDs) (1). The incidence of invasive fungal infections (IFIs) in liver transplant recipients is surpassed only by small bowel and lung transplant recipients (2). IFIs occur in 7–42% of patients with liver transplant (3). Despite the advance in surgical techniques and antifungal prophylactic strategies, IFI is still a major cause of postoperative morbidity and mortality for patients undergoing LT (4). The reported mortality associated with IFI range from 25 to 69% (5).
Several clinical trials have shown that the causative organisms of IFIs are variable. Candida species are the most common causes of IFI post-LT, followed by Aspergillus species (4). Recipients with active or latent infection in the recipient or donor at the time of transplantation, or early graft dysfunction or rejection, are at particularly high risk of developing opportunistic infections (6). Therefore, the incidence of IFI is strongly associated with the hospital microbiological environment, level of immunosuppression, the clinical condition of the patient, surgical factors, complicated transplant operation, and use of high-dose antibiotics (6, 7).
Many studies have reported the risk factors for IFI post-LT, including bacterial infections in the first month and absence of antifungal prophylaxis (7), reoperation, or retransplantation (5). Model for End-Stage Liver Disease (MELD) Score, cytomegalovirus reactivation (8), Roux-en-y anastomosis, and hemodialysis (9). However, because of geographical limitations and sample size, the outcomes of studies of risk factors for IFI post-LT are controversial. For instance, three studies reported that the MELD score was a risk factor for IFI posttransplant (7, 10, 11), but another study reported that the MELD score was not related to IFI post-LT (12). To address the inconsistency in the results, the present meta-analysis measured the quantitative combined effect of all the related studies and increased the power of statistical analysis by merging multiple single studies about the risk factors of IFI in recipients after LT. Finally, this meta-analysis involving 14 studies and provided more reliable evidence for the risk factors of IFI post-LT.
A literature search was performed in PubMed, Web of Science, Embase, the Cochrane Library to identify studies related to risk factors of IFI after LT that were published up to June 2020. The terms searched were “liver transplantation or hepatic transplantation or liver grafting” and “invasive fungal infection or IFI” and “risk factors”.
Studies were selected in accordance with the “Preferred reporting items for systematic reviews and meta-analyses” (PRISMA) statement (13). The inclusion criteria were as follows: (1) the study was related to the risk factors of IFI in recipients post-LT; (2) IFI was defined as proven or probable according to the European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) Criteria (14); (3) the study was a case-control or cohort study in design; (4) availability of the published data; (5) the study was written in English.
The following were the exclusion criteria: (1) duplicate articles; (2) reviews, meeting abstracts, letters, or case reports; (3) no diagnostic or no defined criteria for IFIs; (4) studies were related to the risk factors of IFIs after the organ transplantation but did not report the relevant data on the LT subgroup; (5) studies included data of risk factors for LT infection but did not show the information for IFI.
Relevant information was extracted independently by the two reviewers (ML and LYS). A final check was confirmed by another researcher (ZJZ). The extracted data included the first author, publication year, country of origin, study time and design, number of patients and controls, and risk factors for IFIs with odds ratio (OR) and 95% CI from the multivariate analyses.
The quality of each included study was independently evaluated by the three reviewers (ML, LYS, and ZJZ) based on the Newcastle–Ottawa Scale (NOS) (15). The NOS consists of three domains and a total of nine points: four for selection of study groups, three for outcome and exposure, and two for comparability of the cases. Only studies with scores> 6 were considered as high quality and finally included (16).
Statistical analysis was performed using Review Manager 5.3 and Stata 12.0. Heterogeneity was considered significant with I2 > 50% or P < 0.1 (17). The fixed-effects model was used to calculate the 95% CI and its pooled ORs for the homogeneous data (I2 < 50% or P > 0.05). Otherwise, the random-effects model was used. Sensitivity analysis was conducted by excluding one study at a time. Publication bias was assessed with Egger's test. P < 0.05 suggested that there was a publication bias in this study. The population attributable risk proportion (PARP) was calculated as follows: PARP = Pe (OR−1)/[Pe (OR−1) + 1]. Pe was defined as the pooled exposure rate of controls that represented the overall population exposure rate.
The literature search yielded 2,405 results; most studies were excluded because they were duplicate studies or because they were not relevant to our meta-analysis. Then, 84 studies were excluded after the full-text articles were reviewed because they did not match the criteria. Finally, 14 studies involving 4,284 recipients (533 cases and 3,751 controls) were included in this meta-analysis (7, 10–12, 18–27). The study selection process is shown in Figure 1.
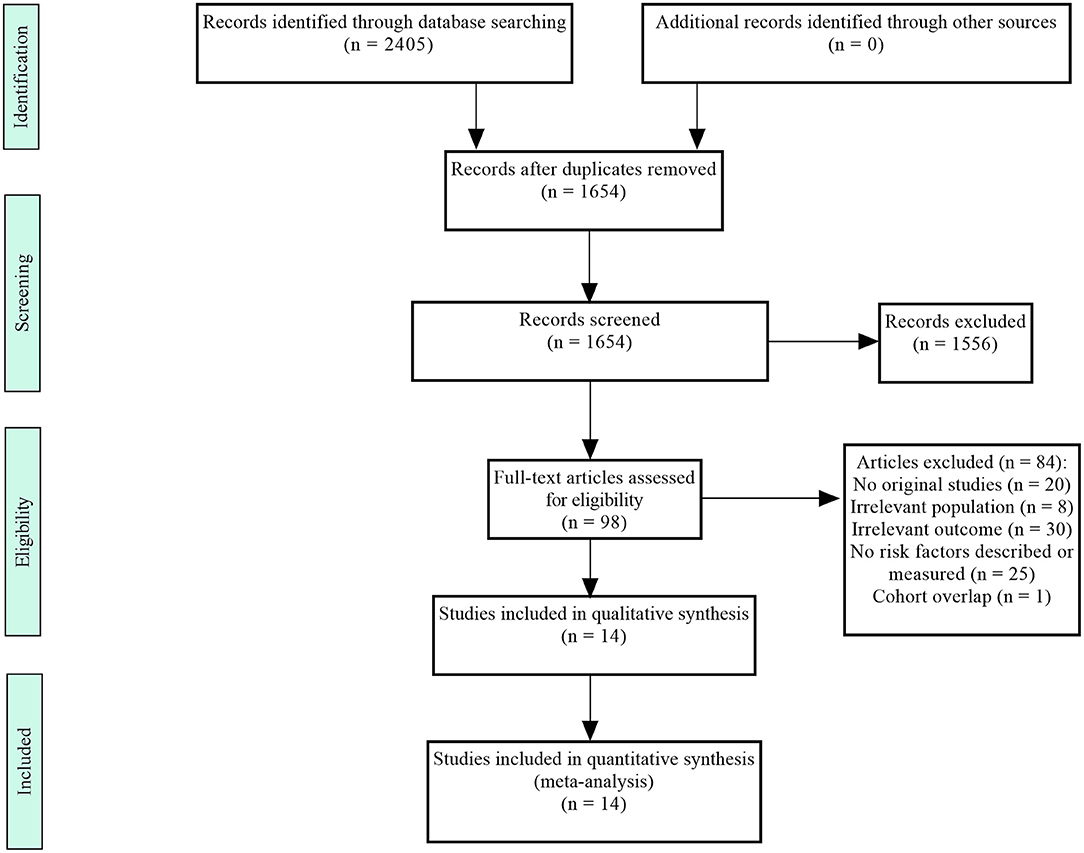
Figure 1. Flowchart of the selection process.
The specific characteristics of the studies included in the meta-analysis are presented in Table 1. These 14 studies were published from 2003 to 2020. They were conducted in the USA (10, 22, 25, 27), Australia (26), China (20), Japan (11, 19, 21), Korea (12), Italy (23, 24), Spain (18), and France (7). A total of seven studies were cohort studies (10, 12, 18, 19, 23, 25, 26) and seven were case–control studies (7, 11, 20–22, 24, 27). All the included studies were evaluated as high quality after being assessed by the NOS.
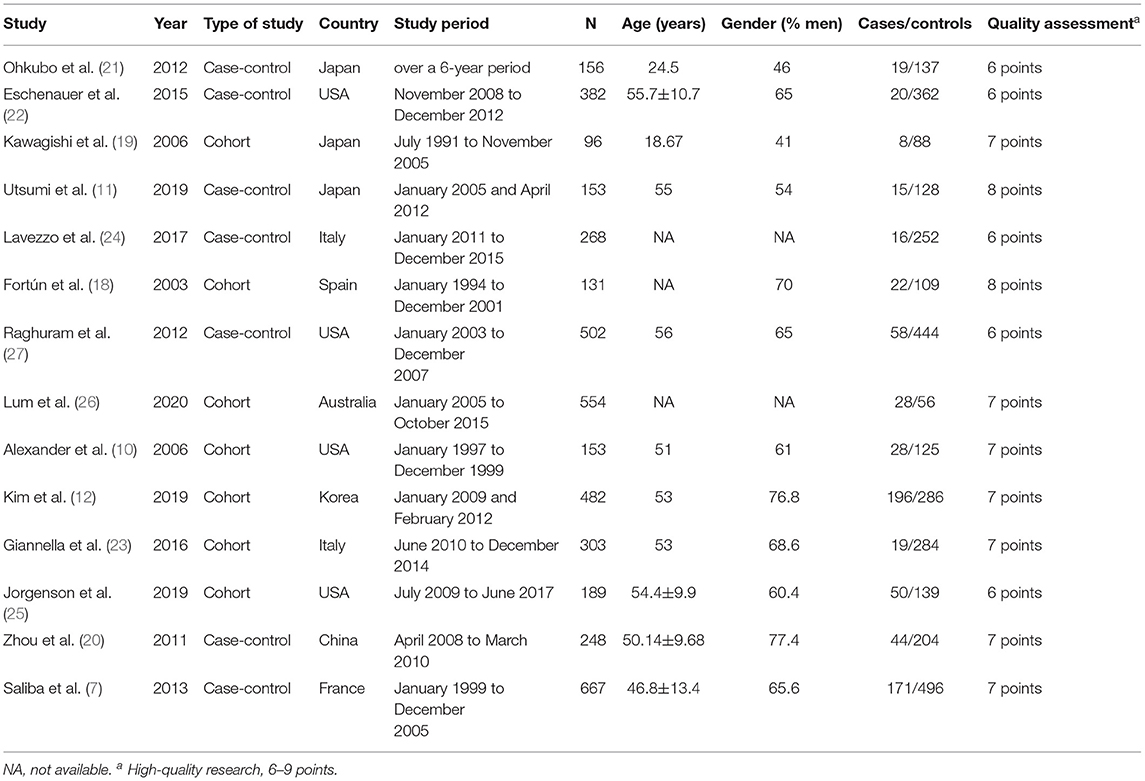
Table 1. Characteristics of studies included in the meta-analysis.
The risk factors for IFI post-LT are shown in Table 2. Several risk factors were identified, including reoperation, post-transplant dialysis, bacterial infection, live donor, the MELD score, retransplantation, fungal colonization, Roux-en-Y anastomosis. The risk factors with significant differences in IFIs after LT were as follows: reoperation (OR = 2.18, 95% CI: 1.61–2.94), posttransplantation dialysis (OR = 2.03, 95% CI: 1.52–2.72), bacterial infection (OR = 1.81, 95% CI: 1.33–2.46), live donor (OR = 1.78, 95% CI: 1.20–2.63), retransplantation (OR = 2.45, 95% CI: 1.54–3.89), and fungal colonization (OR = 2.60, 95% CI: 1.99–3.42). A forest plot describing the association between risk factors for IFIs after LT is presented in Figure 2.
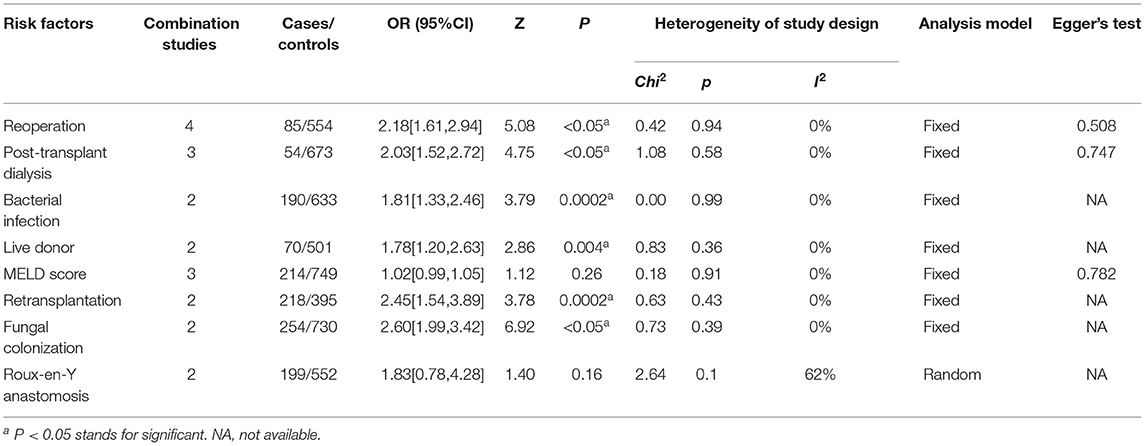
Table 2. Meta-analysis of risk factors of invasive fungal infection in recipients after liver transplantation.
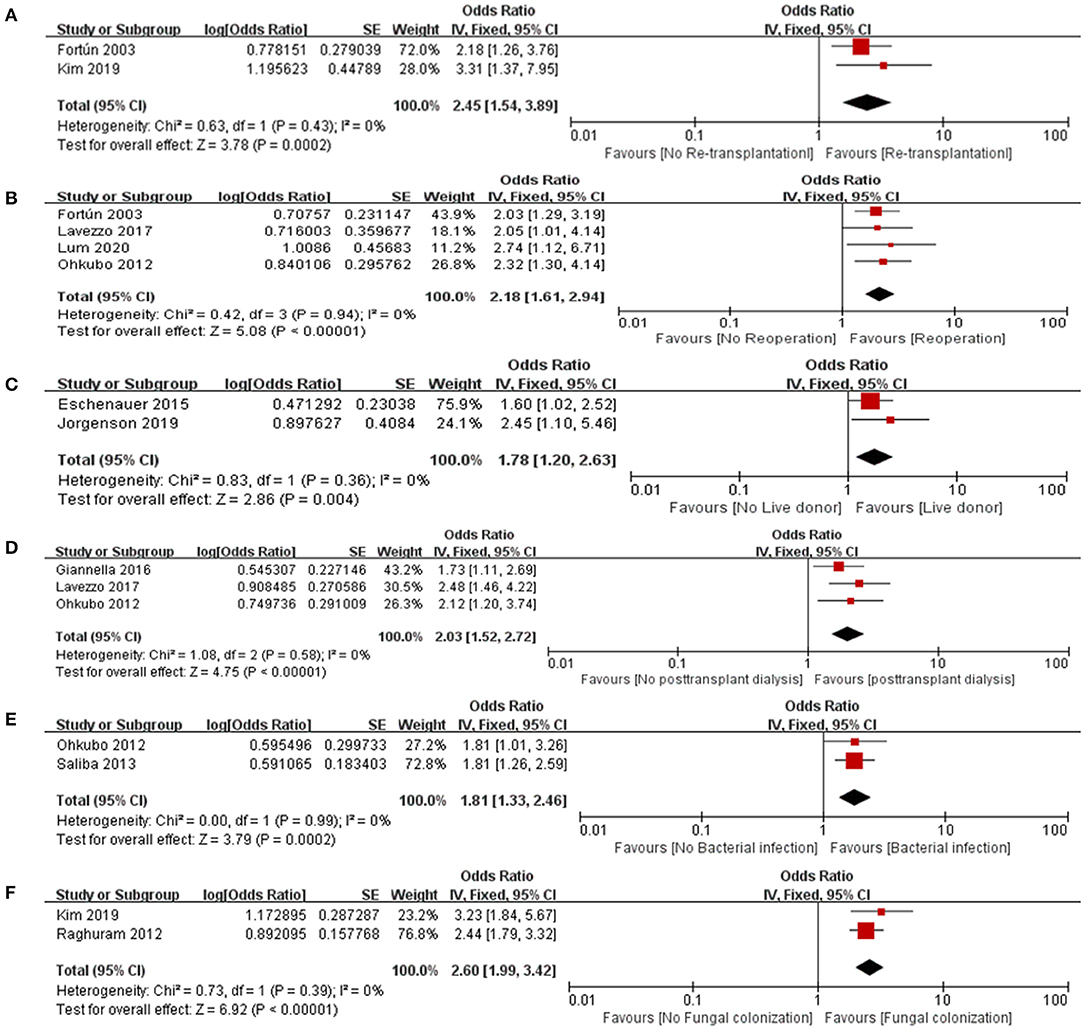
Figure 2. Forest plot for the association between IFI after LT and (A) Retransplantation, (B) Reoperation, (C) Live donor, (D) Posttransplant dialysis, (E) Bacterial infection and (F) Fungal colonization.
Population attributable risk proportion was used to represent the proportion of cases in a population that was attributable to the exposed factor. The PARP of risk factors such as reoperation, posttransplant dialysis, bacterial infection, live donor, fungal colonization, and retransplantation is shown in Table 3. The PARP ranged from 6.3 to 37.5%. Reoperation had the highest PARP, whereas live donor had the lowest. Bacterial infection, reoperation, and fungal colonization were strong risk factors for IFIs after LT.
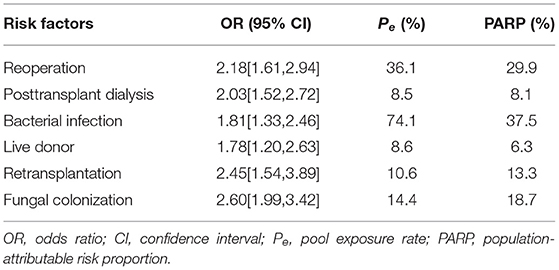
Table 3. Population-attributable risk proportion of risk factors of invasive fungal infections in recipients after liver transplantation.
Sensitivity analysis was used to evaluate the potential effect of heterogeneity conducted by eliminating one study in each turn. Sensitivity analyses manifested no significant changing of heterogeneity when one study was eliminated at a time.
Egger's test was conducted for statistical investigation to evaluate potential publication bias (Table 2). The publication bias was considered to exist for P < 0.05. Egger's test showed that most risk factors did not have a publication bias (P > 0.05).
Invasive fungal infection is associated with poor outcomes in recipients with posttransplant (28). Therefore, identifying risk factors is essential for preventing IFI post-LT. Accordingly, targeted prophylaxis should be performed only in high-risk recipients (22). Several studies have reported potential risk factors for IFI post-LT. However, there has been inconsistency about the risk factors, perhaps because of the different studies using different designs or inclusion criteria. The current meta-analysis was conducted to identify the risk factors for IFI post-LT and provide the best evidence for the clinical applications.
According to the inclusion and exclusion criteria, we identified 14 studies enrolling 4,284 patients. In our meta-analysis, risk factors for IFI after LT included reoperation, posttransplant dialysis, bacterial infection, retransplantation, live donor, and fungal colonization. As summarized in Figure 3, 14 studies identified 506 pathogens that caused IFI post-LT. Candida species were the most common causative organism of IFI among recipients of the LT, and Aspergillus species was the second most common.
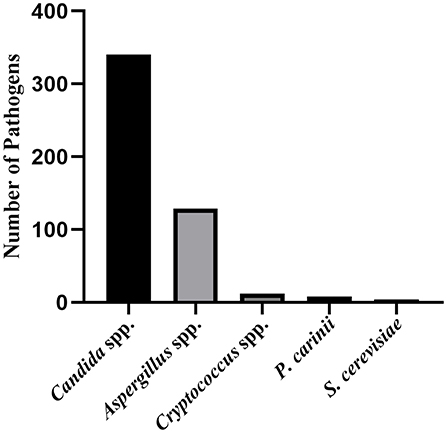
Figure 3. The pathogen composition of IFI after LT. spp, species; P. carinit, Pneumocystis cariniee; S. Cerevisiae, Saccharomyces cerevisiae.
Reoperation and retransplantation, which indicated a more complicated intraoperative and postoperative procedure, were risk factors for IFI. Meta-analysis showed that the risk of IFI in recipients with reoperation was 2.18 times higher than the recipients without reoperation, which was consistent with the results of previous studies (29, 30). However, among the studies included in this meta-analysis, Eschenauer et al. (22) and Utsumi et al. (11) concluded that IFI was not associated with reoperation, but the researchers did not give an explanation for this result. Some included studies reported a higher risk of IFI in recipients who underwent retransplantation (12, 18). Our result was consistent with these studies. Several studies reported that retransplantation was not a significant risk factor (22–24), which was likely due to the small number of recipients who underwent retransplantation. The results showed that Roux-en-y anastomosis was not a risk factor for IFI after LT, possibly because of the small number of patients who underwent retransplantation, which was consistent with the results of a previous study (26).
Recipients of the live donor were at a higher risk of IFI after LT, which was consistent with the previous studies (22, 31). In the case of the living donor liver transplant (LDLT), the graft is smaller than that recovered from a deceased donor, and it involves complex surgery and carries a risk of bile leakage. Therefore, antifungal prophylaxis should be given to patients with LDLT to counter the risks of IFI.
Our study also found that the risk of IFI increased with the posttransplant dialysis that is consistent with the studies of Ohkubo et al. (21), Lavezzo et al. (24), and Giannella et al. (23), but several studies (10, 12, 18, 22) found that the posttransplant dialysis was not a risk factor for IFI post-LT; however, the authors did not give any explanation for this negative outcome.
We used PARP to estimate the percentage of IFI in recipients of LT attributed to one kind of risk factor. We found that the PARP of the bacterial infection and reoperation was high. Thus, we infer that these risk factors were important for IFI post-LT.
Fungal colonization was defined as the presence of fungus before LT without clinical symptoms or evidence of infection. We found that the patients with fungal colonization were at a higher risk of IFI. Several studies have shown that antifungal prophylaxis dramatically reduces fungal colonization, mortality caused by a fungal infection, and the overall incidence of fungal infection (5, 32). Further investigation of pretransplant screening to identify fungal colonization is warranted. Therefore, we recommend that post-LT, the recipients should have targeted antifungal prophylaxis to reduce antibiotic exposure.
There were several limitations to this meta-analysis. First, we only included English language literature from four databases, and there may have been incomplete retrieval. Second, there may have been mistakes in the data conversion because some study data required to be recalculated. Third, because of the limitations of the included date, we did not conduct subgroup analyses and funnel plots. At last, analyses were limited by the sample size included in this meta-analysis, so the combined effect size may have been exaggerated to draw the opposite conclusion.
In conclusion, this meta-analysis identified some risk factors for IFI post-LT and might provide a basis for clinical prevention. However, a well-designed prospective cohort study should be conducted to validate our findings.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
ML and LYS designed the study and wrote the first draft of the manuscript. ML and ZJZ verified data extraction, data analysis, and reviewed the manuscript. LYS and ZJZ supervised the data acquisition, data analysis, and interpretation. All the authors read and approved the final manuscript.
This research was supported by the Beijing Municipal Science & Technology Commission (No. Z181100001718220).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hughes CB, Humar A. Liver transplantation:current and future. Abdom Radiol. (2020) 46:2–8. doi: 10.1007/s00261-019-02357-w
2. Linares L, Garcia-Goez JF, Cervera C, Almela M, Sanclemente G, Cofan F, et al. Early bacteremia after solid organ transplantation. Transplant Proc. (2009) 41:2262–4. doi: 10.1016/j.transproceed.2009.06.079
3. Hadley S, Huckabee C, Pappas PG, Daly J, Rabkin J, Kauffman CA, et al. Outcomes of antifungal prophylaxis in high-risk liver transplant recipients. Transpl Infect Dis. (2009) 11:40–8. doi: 10.1111/j.1399-3062.2008.00361.x
4. Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, Freifeld A, et al. Invasive fungal infections among organ transplant recipients:results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis. (2010) 50:1101–11. doi: 10.1086/651262
5. Eschenauer GA, Lam SW, Carver PL. Antifungal prophylaxis in liver transplant recipients. Liver Transpl. (2009) 15:842–58. doi: 10.1002/lt.21826
6. Welte T, Len O, Munoz P, Romani L, Lewis R, Perrella A. Invasive mould infections in solid organ transplant patients:modifiers and indicators of disease and treatment response. Infection. (2019) 47:919–92. doi: 10.1007/s15010-019-01360-z
7. Saliba F, Delvart V, Ichaï P, Kassis N, Botterel F, Mihaila L, et al. Fungal infections after liver transplantation:outcomes and risk factors revisited in the MELD era. Clin Transplant. (2013) 27:E454–61. doi: 10.1111/ctr.12129
8. Rosenhagen M, Feldhues R, Schmidt J, Hoppe-Tichy T, Geiss HK. A risk profile for invasive aspergillosis in liver transplant recipients. Infection. (2009) 37:313–9. doi: 10.1007/s15010-008-8124-x
9. Gavalda J, Len O, San JR, Aguado JM, Fortun J, Lumbreras C, et al. Risk factors for invasive aspergillosis in solid-organ transplant recipients: a casecontrol study. Clin Infect Dis. (2005) 41:52–9. doi: 10.1086/430602
10. Alexander J, Limaye AP, Ko CW, Bronner MP, Kowdley KV. Association of hepatic iron overload with invasive fungal infection in liver transplant recipients. Liver Transpl. (2006) 12:1799–804. doi: 10.1002/lt.20827
11. Utsumi M, Umeda Y, Yagi T, Nagasaka T, Shinoura S, Yoshida R, et al. Risk analysis for invasive fungal infection after living donor liver transplantation:which patient needs potent prophylaxis? Dig Surg. (2019) 36:59–66. doi: 10.1159/000486548
12. Kim YJ, Kim SI, Choi JY, Yoon SK, Na GH, You YK, et al. Invasive fungal infection in liver transplant recipients in a prophylactic era: a multicenter retrospective cohort study in Korea. Medicine (Baltimore). (2019) 98:e16179. doi: 10.1097/MD.0000000000016179
13. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. Open Med. (2009) 3:e123–30. doi: 10.1371/journal.pmed.1000097
14. Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group. Education and research consortium. Clin Infect Dis. (2020) 71:1367–1376. doi: 10.1093/cid/ciz1008
15. Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS, Hahn S, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. (2013) 66:408–14. doi: 10.1016/j.jclinepi.2012.09.016
16. Margulis AV, Pladevall M, Riera-Guardia N, Varas-Lorenzo C, Hazell L, Berkman ND, et al. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools:the Newcastle-Ottawa, Scale and the RTI item bank. Clin Epidemiol. (2014) 6:359–68 doi: 10.2147/CLEP.S66677
17. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
18. Fortún J, Martín-Davila P, Moreno S, Barcena R, de Vicente E, Honrubia A, et al. Prevention of invasive fungal infections in liver transplant recipients:the role of prophylaxis with lipid formulations of amphotericin B in high-risk patients. J Antimicrob Chemother. (2003) 52:813–9. doi: 10.1093/jac/dkg450
19. Kawagishi N, Satoh K, Enomoto Y, Akamatsu Y, Sekiguchi S, Fujimori K, et al. Risk factors and impact of beta-D glucan on invasive fungal infection for the living donor liver transplant recipients. Tohoku J Exp Med. (2006) 209:207–15. doi: 10.1620/tjem.209.207
20. Zhou T, Xue F, Han LZ, Xi ZF, Li QG, Xu N, et al. Invasive fungal infection after liver transplantation:risk factors and significance of immune cell function monitoring. J Dig Dis. (2011) 12:467–75. doi: 10.1111/j.1751-2980.2011.00542.x
21. Ohkubo T, Sugawara Y, Takayama T, Kokudo N, Makuuchi M The risk factors of fungal infection in living-donor liver transplantation. J Hepatobiliary Pancreat Sci. (2012) 19:382–8. doi: 10.1007/s00534-011-0423-4
22. Eschenauer GA, Kwak EJ, Humar A, Potoski BA, Clarke LG, Shields RK, et al. Targeted versus universal antifungal prophylaxis among liver transplant recipients. Am J Transplant. (2015) 15:180–9. doi: 10.1111/ajt.12993
23. Giannella M, Bartoletti M, Morelli M, Cristini F, Tedeschi S, Campoli C, et al. Antifungal prophylaxis in liver transplant recipients:one size does not fit all. Transpl Infect Dis. (2016) 18:538–44. doi: 10.1111/tid.12560
24. Lavezzo B, Patrono D, Tandoi F, Martini S, Fop F, Ballerini V, et al. A simplified regimen of targeted antifungal prophylaxis in liver transplant recipients: a single-center experience. Transpl Infect Dis. (2018) 20:e12859. doi: 10.1111/tid.12859
25. Jorgenson MR, Descourouez JL, Marka NA, Leverson GE, Smith JA, Andes DR, et al. A targeted fungal prophylaxis protocol with static dosed fluconazole significantly reduces invasive fungal infection after liver transplantation. Transpl Infect Dis. (2019) 21:e13156. doi: 10.1111/tid.13156
26. Lum L, Lee A, Vu M, Strasser S, Davis R. Epidemiology and risk factors for invasive fungal disease in liver transplant recipients in a tertiary transplant center. Transpl Infect Dis. (2020) 22:e13361. doi: 10.1111/tid.13361
27. Raghuram A, Restrepo A, Safadjou S, Cooley J, Orloff M, Hardy D, et al. Invasive fungal infections following liver transplantation:incidence, risk factors, survival, and impact of fluconazole-resistant Candida parapsilosis (2003-2007) Liver Transpl (2012) 18:1100–9. doi: 10.1002/lt.23467
28. Liu X, Ling Z, Li L, Ruan B. Invasive fungal infections in liver transplantation. Int J Infect Dis. (2011) 15:e298–304. doi: 10.1016/j.ijid.2011.01.005
29. Singh N, Paterson DL, Gayowski T, Wagener MM, Marino IR. Preemptive prophylaxis with a lipid preparation of amphotericin B for invasive fungal infections in liver transplant recipients requiring renal replacement therapy. Transplantation. (2001) 71:910–3. doi: 10.1097/00007890-200104150-00016
30. Silveira FP, Husain S. Fungal infections in solid organ transplantation. Med Mycol. (2007) 45:305–20. doi: 10.1080/13693780701200372
31. Suzuki T, Hashimoto T, Nakamura T, Kondo S, Shimizu Y, Nakamura Y, et al. Fungal infection in living related liver transplantation patients. Transplant Proc. (2000) 32:2231–2. doi: 10.1016/S0041-1345(00)01648-1
Keywords: invasive fungal infection, liver transplantation, risk factors, meta-analysis, end-stage liver diseases
Citation: Liu M, Zhu Z and Sun L (2021) Risk Factors of Invasive Fungal Infection in Recipients After Liver Transplantation: A Systematic Review and Meta-Analysis. Front. Med. 8:687028. doi: 10.3389/fmed.2021.687028
Received: 30 March 2021; Accepted: 31 August 2021;
Published: 04 October 2021.
Edited by:
Ang Li, First Affiliated Hospital of Zhengzhou University, ChinaReviewed by:
Yi Huimin, Third Affiliated Hospital of Sun Yat-sen University, ChinaCopyright © 2021 Liu, Zhu and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liying Sun, c3VueGx4QG91dGxvb2suY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.