
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 19 August 2021
Sec. Nephrology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.686729
 Frank Lizaraso-Soto1,2†
Frank Lizaraso-Soto1,2† Eduardo Gutiérrez-Abejón1,3†
Eduardo Gutiérrez-Abejón1,3† Juan Bustamante-Munguira4*
Juan Bustamante-Munguira4* Débora Martín-García5María Montserrat Chimeno6Álvaro Nava-Rebollo7Álvaro Maurtua-Briseño-Meiggs8
Débora Martín-García5María Montserrat Chimeno6Álvaro Nava-Rebollo7Álvaro Maurtua-Briseño-Meiggs8 Darío Fernández-Zoppino9Elena Bustamante-Munguira10Félix Jesús de Paz1Jesús Grande-Villoria7Carlos Ochoa-Sangrador11
Darío Fernández-Zoppino9Elena Bustamante-Munguira10Félix Jesús de Paz1Jesús Grande-Villoria7Carlos Ochoa-Sangrador11 Manuel Pascual12
Manuel Pascual12 F. Javier Álvarez1,13‡Francisco Herrera-Gómez1,7,12,14‡
F. Javier Álvarez1,13‡Francisco Herrera-Gómez1,7,12,14‡This manuscript presents findings from the first dichotomous data pooling analysis on clinical trials (CT) regarding the effectiveness of binding potassium. The results emanated from pairwise and network meta-analyses aiming evaluation of response to commercial potassium-binding polymers, that is, to achieve and maintain normal serum potassium (n = 1,722), and the association between this response and an optimal dosing of renin-angiotensin-aldosterone system inhibitors (RAASi) needing individuals affected by heart failure (HF) or resistant hypertension, who may be consuming other hyperkalemia-inducing drugs (HKID) (e.g., β-blockers, heparin, etc.), and frequently are affected by chronic kidney disease (CKD) (n = 1,044): According to the surface under the cumulative ranking area (SUCRA), sodium zirconium cyclosilicate (SZC) (SUCRA >0.78), patiromer (SUCRA >0.58) and sodium polystyrene sulfonate (SPS) (SUCRA <0.39) were different concerning their capacity to achieve normokalemia (serum potassium level (sK+) 3.5–5.0 mEq/L) or acceptable kalemia (sK+ ≤ 5.1 mEq/L) in individuals with hyperkalemia (sK+ >5.1 mEq/L), and, when normokalemia is achieved, patiromer 16.8–25.2 g/day (SUCRA = 0.94) and patiromer 8.4–16.8 g/day (SUCRA = 0.41) can allow to increase the dose of spironolactone up to 50 mg/day in subjects affected by heart failure (HF) or with resistant hypertension needing treatment with other RAASi. The potential of zirconium cyclosilicate should be explored further, as no data exists to assess properly its capacity to optimize dosing of RAASi, contrarily as it occurs with patiromer. More research is also necessary to discern between benefits of binding potassium among all type of hyperkalemic patients, for example, patients with DM who may need treatment for proteinuria, patients with early hypertension, etc.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/, identifier: CRD42020185614, CRD42020185558, CRD42020191430.
Hyperkalemia [serum potassium level (sK+): >5.1 mEq/L] is a life-threatening situation. Individuals with heart failure (HF) may be affected, particularly when they present chronic kidney disease (CKD). Indeed, potassium excretion is impaired in a non-acute manner in such individuals, and physicians are aware of avoiding this situation when estimated glomerular filtration rate (eGFR) falls to 60 ml/min/1.73 m2, that is, in patients into the Kidney Disease–Improving Global Outcomes (KDIGO) GFR categories G3a–G5 (1). HF patients need treatment with angiotensin-converting enzyme inhibitors (ACEi) and/or angiotensin II receptor blockers (ARB), and, in most cases, the addition of a mineralocorticoid receptor antagonist (MRA) is imperative (2).
Treatment with MRA in addition to other renin-angiotensin-aldosterone system inhibitors (RAASi) is also frequently observed among patients with resistant hypertension (i.e., uncontrolled blood pressure when tacking three or more classes of antihypertensive drugs, one of which is a diuretic). Resistant hypertension patients should not be considered as patients with hypertension responding to drugs. These individuals are also affected frequently by CKD, and a sizable proportion of them present some degree of HF (3).
Hyperkalemia is also a concern among individuals with diabetes mellitus (DM), especially with uncontrolled glycemia levels, and for those taking RAASi (e.g., from early hypertension stages, for controlling diabetic proteinuria, etc.), especially when needing other hyperkalemia-inducing drugs (HKID) (e.g., β-blockers, heparin, etc.).
RAASi have demonstrated to improve mortality and other patient-relevant outcomes in HF and resistant hypertension, and substantial benefits in other conditions (e.g., from early hypertension stages patients, to treat diabetic proteinuria, etc.); however, hyperkalemia limits the use of optimal doses of these drugs (4). In figures, hyperkalemia affects globally approximately 23 millions of people having HF and 100 millions of people affected by resistant hypertension (5, 6). In this sense, potassium-binding polymers may allow an optimal treatment with RAASi (7); particularly, new polymers patiromer [Anatomical Therapeutic Chemical (ATC) code: V03AE09] and sodium zirconium cyclosilicate (SZC) (ATC code: V03AE10) face their attractive safety profile compared to classic molecules (8).
Notwithstanding, in order to elucidate the beneficial impact of binding potassium, Bayesian network meta-analysis are necessary to evaluate the capacity of such polymers to facilitate optimal dosing of RAASi, after confirmation of independent effects from all available potassium-binding polymers on correction of hyperkalemia (i.e., efficacy as treatment agent) and on maintaining normal serum potassium (i.e., efficacy as preventive agent) (9).
Individuals along the wide spectrum of CKD should be considered into the evaluation of these nanodrugs, that is, not only patients into KDIGO GFR categories G3a to G5, but also patients with early CKD (KDIGO GFR categories G1 and G2) including subjects with normal kidney function (NKF), as well as dialysis patients and kidney transplant recipients (KTR), as performed in other pharmacometrical studies assessing drugs to treat CKD patients (10).
This manuscript presents findings from pairwise and network meta-analyses aiming evaluation of the efficacy of commercial potassium-binding polymers (i.e., their capacity to achieve and maintain normal serum potassium), and the association between this efficacy and optimal dosing in RAASi-based schemes needing individuals affected by HF or resistant hypertension.
A dichotomous effects meta-analysis following a multiple parallel one-stage systematic review design was performed on clinical trials (CT) having assessed the use of commercial potassium-binding polymers to treat and prevent hyperkalemia. The analysis presented here was not intended to present a summary of continuous data on binding potassium, nor a qualitative systematic review of evidence on these drugs.
Independent study searching, screening, selection, data extraction, and synthesis were carried out in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) recommendations (11), and its extension statement for the reporting of systematic reviews incorporating network meta-analyses of healthcare interventions (12). Such details and those on registration and prospective study updating are consultable online at the site of the International Prospective Register of Systematic Reviews PROSPERO on https://www.crd.york.ac.uk/PROSPERO/ (reference IDs: CRD42020185614, CRD42020185558, CRD42020191430).
Study participants were subjects affected by or at risk of developing hyperkalemia, and they may have HF or resistant hypertension, and may have NKF, CKD into KDIGO GFR categories G1–G5, end-stage kidney disease (ESKD) necessitating dialysis, or received a kidney transplant.
The main intervention was binding potassium either used with the intention to treat or prevent hyperkalemia. Classical and new commercial potassium-binding polymers were considered. Treatment with RAASi, HKID (e.g., β-blockers, heparin, etc.), dietary restriction, diuretics, insulin and other antidiabetic drugs, phosphate-binding drugs, were considered as co-interventions. Comparators were, for randomized controlled trials, placebo and potassium-binding polymers at lower doses, and, for single-arm trials, pre-treatment state.
The same syntaxis of search formulae was used in the three systematic reviews performed. Search formulae was constructed by associating the name of each potassium-binding polymer, including trade names, ATC code, and other names, and the main indication of these drugs, that is, hyperkalemia, considering all possible term variations (e.g., potassium, hyperpotassemia, and hyperkalemia). Searches were not filtered by report type, access type (e.g., open access), or publication year/date. Published studies were searched in MEDLINE (PubMed, Ovid and Web of Science), EMBASE (Elsevier's Scopus), and in Cochrane Controlled Register of Trials (CENTRAL), up to June 2020. Study registries (ClinicalTrials.gov, the EU Clinical Trials Register, and the United Kingdoms' ISRCTN registry) and unpublished study sources (PhD and Master theses, meeting abstracts archives) were also searched. The reference lists of included studies were scanned to identify all relevant studies cited by included studies, so that they did not remain unnoticed.
Risk of bias assessment using the standard tool produced by the Cochrane Collaboration (13) preceded data synthesis.
This meta-analysis presents effect estimates on aggregate data. The first-step analysis assessed the efficacy of binding potassium (i.e., the capacity of commercial potassium-binding polymers to achieve and maintain normal serum potassium) at network and pairwise level. Pooled odds ratios (OR) and 95% credible intervals (95% CrI) for the outcomes of normokalemia (sK+ 3.5 to 5.0 mEq/L) and acceptable kalemia (sK+ ≤ 5.1 mEq/L) corresponding to each of the assessed potassium-binding polymers at all possible doses, were obtained via Bayesian network meta-analysis (Markov chain Monte Carlo simulation on the vague priors random-effects method for “bad” outcomes and zero values correction) with calculation of SUCRA value corresponding to all assessed doses, after verifying convergence (Brooks-Gelman-Rubin method) and inconsistency, using the NetMetaXL software (Canadian Agency for Drugs and Technologies in Health and Cornerstone Research Group) (14). Previously, all potassium-binding polymers as a whole were evaluated via pairwise meta-analysis (Mantel-Haenszel random-effects method) after verifying heterogeneity (χ2, I2) and the presence of reporting bias (visual inspection of funnel plots and calculation of Egger's test value), using the Review Manager software (RevMan) version 5.3 (Cochrane Collaboration) and META-analysis package FOr R (METAFOR) version 2.4 (R project).
In the second-step Bayesian network meta-analysis using the same mathematical assumptions as in the first-step network meta-analysis, calculations present the effects from binding potassium considering the outcome of increase in the dosing of spironolactone up to 50 mg/day in normokalemic patients with HF or resistant hypertension (who were also receiving other RAASi).
Recommendations of the Centre for Reviews and Dissemination (University of York) were followed in qualitative synthesis, that is, to assess all skewed and non-quantitative data (15).
This meta-analysis presents data on 2,279 individuals having participated in 11 clinical trials, of which 82.2% (n = 1,873), 63.5% (n = 1,447), 41.5% (n = 946), and 19.4% (n = 412) were, respectively, under treatment with HKID (e.g., RAASi, β-blockers, heparin, etc.), presented history of DM, had HF, or had resistant hypertension (16–40). Of the study participants, 79.2% (n = 1,805) had CKD into KDIGO GFR categories G3a–G5 and, the rest, NKF/early CKD (KDIGO GFR categories G1 and G2).
All participants in the included trials were either affected by or were at risk of developing hyperkalemia. However, with the exception of AMBER that studied only resistant hypertension patients (40), the rest of CT included patients with HF and other conditions (i.e., patients without known HF but with DM, and patients without HF but taking RAASi and other HKID were included in these trials). Dialysis patients and KTR did not participate in the included trials. Characteristics of the study population and key study details, in addition to the interventions, comparators, and outcomes, are available for readers online (Supplementary Table 1).
The pharmaceutical industry sponsored all these 11 CT, of which eight consisted in the phase 1–3 evaluation of the efficacy of patiromer (16–29), zirconium cyclosilicate (30–35), and sodium polystyrene sulfonate (SPS) (36) to treat hyperkalemia. Hyperkalemic patients may have HF or resistant hypertension or may present other causes for their hyperkalemia (n = 1,801): CKD into KDIGO GFR categories G3a–G5, DM under treatment with insulin and other antidiabetic drugs, or treatment with RAASi and other HKID. The impact of binding potassium as a treatment agent was measured on dichotomous and continuous outcomes centered on the influence on serum potassium levels.
Five phase 2 and 3 trials out of the retrieved 11 CT evaluated patiromer to prevent hyperkalemia, that is, for maintaining normokalemia (sK+ 3.5 to 5.0 mEq/L). Prevention of hyperkalemia was evaluated in these five trials as the impact of facilitating optimal dosing of spironolactone in schemes based on RAASi used by normokalemic patients, who had HF or resistant hypertension, with/without CKD into KDIGO GFR categories G3a to G5 (n = 1,135) (21–29, 37–40). Nevertheless, prevention of hyperkalemia was also measured on continuous outcomes concerning the influence on serum potassium levels.
Two CT out of the five CT on prevention of hyperkalemia, OPAL-HK (21–27) and AMENTHYST-DN (28, 29), were intended to assess patiromer also to treat hyperkalemia. Thus, six CT evaluated binding potassium exclusively to treat hyperkalemia (16–20, 30–36).
Trials included in this analysis were different concerning study design. OPAL-HK (21–27) and AMENTHYST-DN (28, 29) stratified study participants with hyperkalemia into the groups of mild hyperkalemia (sK+ <5.5 mEq/L) and moderate-to-severe hyperkalemia (sK+ <6.5 mEq/L) (21–29), and AMENTHYST-DN (28, 29) stratified participants with normokalemia into the groups of losartan 100 mg/day plus spironolactone and other RAASi plus spironolactone (28, 29). OPAL-HK (21–27), AMENTHYST-DN (28, 29), ZS-003/ZS-005 (31–33), and HARMONIZE (34, 35) were two-stage analyses. OPAL-HK, AMENTHYST-DN, and HARMONIZE contained single-arm explorations considering pre-treatment state as comparison (21–29, 34, 35). AMENTHYST-DN, ZS-003/ZS-005 and HARMONIZE were continued by extension follow-up studies (29, 32, 33, 35).
This analysis assessed two single-arm trials (16, 17, 37, 38) together with randomized trials controlled with placebo (21–27, 31–36, 39, 40) or with active comparisons consisting of standardized dietary restriction (18–20) or low doses of the potassium-binding polymers used as intervention (28, 29, 31–33).
Figure 1 presents the selection procedure followed that takes into account gray literature sources and allow the inclusion of seven unpublished reports (oral or posted communications) that provided important information from the published studies that were retrieved (17, 24–27, 32, 33). Gray literature did not provide new trials in addition to those retrieved from published sources.
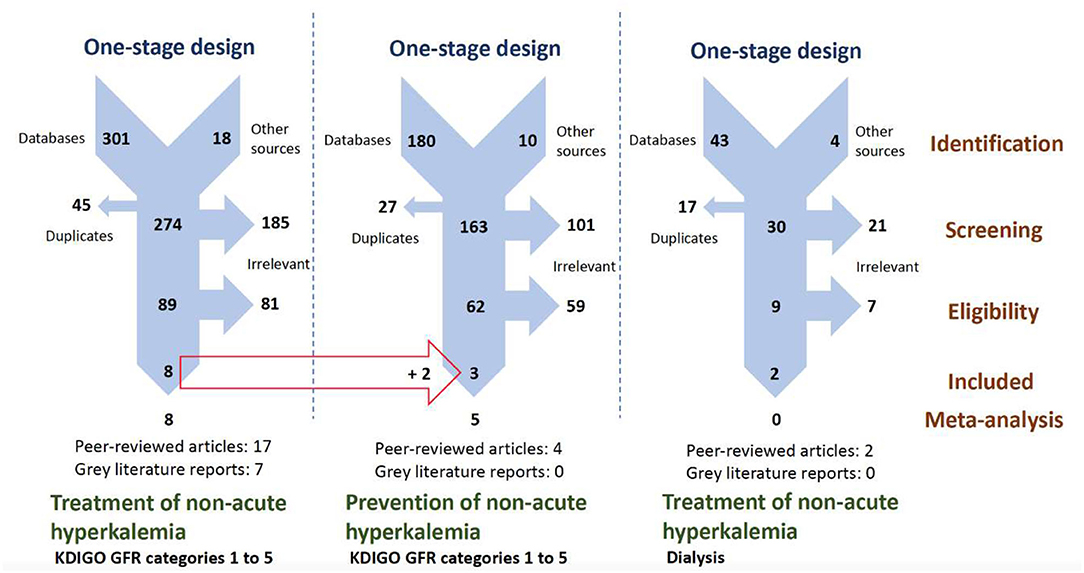
Figure 1. PRISMA flowcharts presenting our parallel one-stage systematic review selection process for retrieving CT providing mathematical data on treatment and prevention of hyperkalemia using potassium-binding polymers. CT, clinical trial; GFR, glomerular filtration rate; KDIGO, kidney disease–improving global outcomes; PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Exclusions for this meta-analysis consisted of editorials and other opinion reports, observational studies that included real-world data evidence, and pre-clinical and clinical trials that did not evaluate our eligible outcomes. However, three and two trials studying calcium polystyrene sulfonate (CPS) and SPS in, respectively, CKD patients into KDIGO GFR categories G3a to G5 (41–43) and dialysis patients, were found (44, 45) but excluded as these CT did not provide the type of numerical data for our planned dichotomous analysis.
Mathematical findings presented here came from moderate- to high-quality studies. Full assessment of risk of bias in the assessed CTs are consultable for readers online (Supplementary Table 2).
Figure 2 presents the league table from multiple-treatment meta-analysis calculations with eight CT studying hyperkalemic patients (n = 1,722) and shows significant positive effects compared to placebo according to the values of ORs and their corresponding 95% CrIs considering normokalemia (sK+ 3.5 to 5.0 mEq/L) and acceptable kalemia (sK+ ≤ 5.1 mEq/L) for patiromer 8.4–25.2 g/day (OR/95% CrI: 0.02/0.01–0.08, 0.02/0.00–0.12) (16–29), patiromer 16.8–33.6 g/day (0.05/0.01–0.34, 0.07/0.00–0.29) (16–29), SZC 15 g/day (0.01/0.00–0.14, 0.00/0.00–0.15) (30–35), SZC 3–10 g/day (0.01/0.00–0.12, 0.00/0.00–0.12) (30–35), and SPS 30 g/day (0.02/0.00–0.13, 0.01/0.00–0.16) (36). Size effects corresponding to such doses did not change when placebo and pre-treatment state were considered together.

Figure 2. League table showing effect estimates in OR and 95% CrI for the outcomes of normokalemia (sK+ 3.5 to 5.0 mEq/L) and acceptable kalemia (sK+ ≤ 5.1 mEq/L) corresponding to all evaluated potassium-binding polymers for each possible (direct and indirect) comparison. CrI, credible intervals; OR, odds ratio; SPS, sodium polystyrene sulfonate; SZC, sodium zirconium cyclosilicate.
The network level forest plot with estimates done on vague prior random-effects (Supplementary Figure 1) that presents a more comprehensive analysis extending our results at the pairwise level (data not shown) confirms effects from the assessed potassium-binding polymers and doses.
Low inconsistency was perceivable at the network level (Supplementary Figure 2), probably as a consequence of statistical heterogeneity observed both in pairwise and network calculations (I2 >65%). Risk for reporting bias [Egger's test (t)/degrees of freedom (df)/p: −2.9135, 21, <0.0001] was also important.
On the basis of the surface under the cumulative ranking area (SUCRA), there were differences between SZC (SUCRA >0.78), patiromer (SUCRA >0.58), and SPS (SUCRA <0.39) regarding their effects on the assessed outcomes. Indeed, mathematically, these molecules were different with respect to their capacity to achieve normokalemia and acceptable kalemia. However, such differences were more perceivable between either SZC or patiromer compared to SPS, so SZC and patiromer, respectively, were the best interventions against hyperkalemia (Table 1).
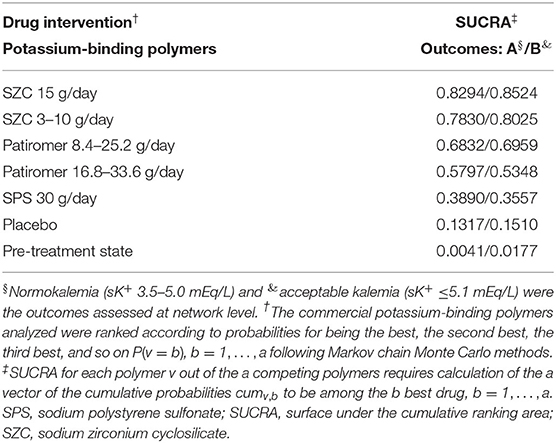
Table 1. SUCRA-based ranking of the evaluated commercial potassium-binding polymers.
Figure 3 shows the Bayesian network diagram corresponding to the main analysis that shows the limited size of CT evidence, both in comparison density (thickness of lines according to the number of CTs in each comparison) and into the evidence for each potassium-binding polymer evaluated (node size according to the number of participants undergoing each polymer).
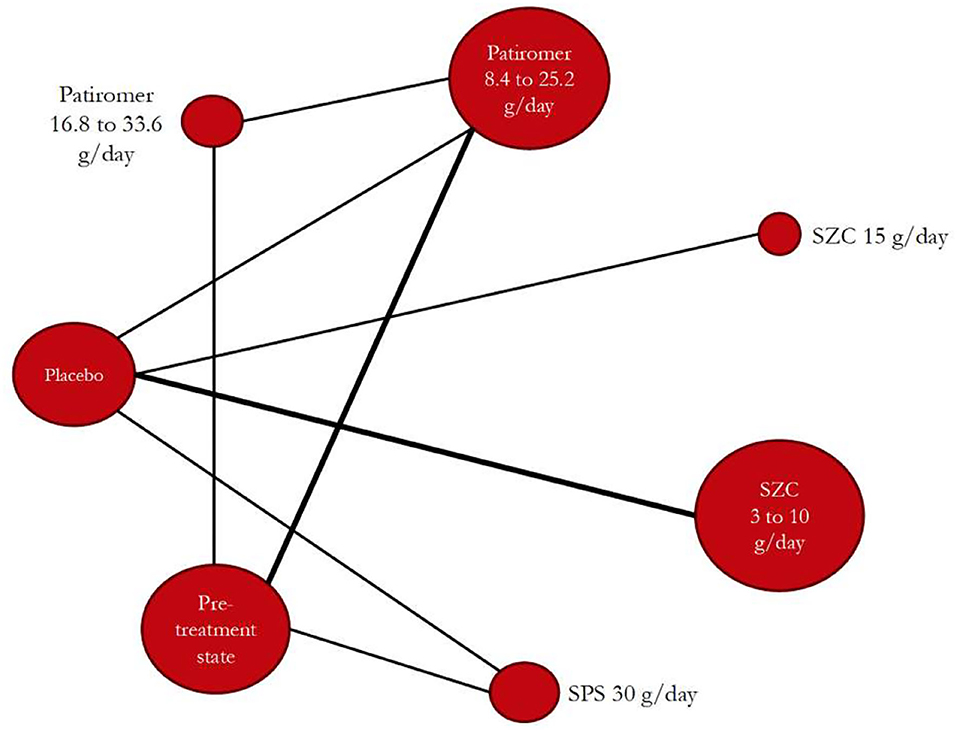
Figure 3. Bayesian network diagram constructed with the retrieved trials after searches and considering all evaluated potassium-binding polymers (nodes) and with showing all comparisons (lines between nodes). SPS, sodium polystyrene sulfonate; SZC, sodium zirconium cyclosilicate.
As depicted in Figure 4, according to the SUCRA value, the dose of spironolactone can be increased up to 50 mg/day in normokalemic patients with HF or resistant hypertension (who may have or not CKD into KDIGO GFR categories G3a–G5, and were also receiving other RAASi), when such individuals (n = 1,044) were treated with patiromer 16.8–25.2 g/day (SUCRA=0.94) or patiromer 8.4–16.8 g/day (SUCRA = 0.41). However, the dose of spironolactone cannot be increased when patiromer was not used (SUCRA = 0.15) (21–29, 37–40).

Figure 4. Vague priors random-effects rankogram for the evaluated patiromer doses allowing spironolactone up-titration up to 50 mg/day in subjects with HF or resistant hypertension (who may have or not CKD into KDIGO GFR categories G3a to G5, and were also receiving other RAASi). CKD, chronic kidney disease; GFR, glomerular filtration rate; KDIGO, kidney disease–improving global outcomes; HF, heart failure; RAASi, renin-angiotensin-aldosterone system inhibitors.
There were no data on SZC to perform calculations as those presented in Figure 4 for patiromer.
According to our findings, there were differences between potassium-binding polymers concerning their capacity to achieve normal or acceptable serum potassium levels in individuals with hyperkalemia (with independence to the safety profile of the studied molecules). When normokalemia was achieved, as a measurable benefit for those using RAASi, current evidence shows association between the use of patiromer for maintaining normokalemia (i.e., as prevention drug against hyperkalemia) and optimal dosing of spironolactone (an increase of up to 50 mg/day) in subjects with HF or resistant hypertension using RAASi and needing the addition of an MRA. Nevertheless, for the moment, such an association for the use of zirconium cyclosilicate was not assessable. The lack of evidence should thus promote more research destined to confirm benefits from this new polymer in order to enlarge the armamentarium for managing patients affected by HF or resistant hypertension. These patients are commonly affected by CKD. In any case, all those needing treatment with RAASi who may be potentially at risk for hyperkalemia (e.g., patients with DM who may need treatment for proteinuria, patients with early hypertension, etc.) may also be included when assessing benefits for binding potassium.
This manuscript gathers and presents clinical trial evidence on the effectiveness of binding potassium. To our knowledge, this is the first dichotomous effects meta-analysis carried out on potassium-binding polymers that confirms findings from other summaries presenting data on conventional continuous outcomes (46–49). With a pharmacometrical perspective, the independent effects from the studied polymers and allowed doses are presented, in addition to the impact on optimizing treatment with RAASi requested by clinicians (50). In any case, even if more research is necessary to discern between benefits among all type of hyperkalemic patients, this study provides hard arguments to improve physicians' decision-making against this situation.
Hyperkalemia is associated with poorer clinical outcomes (51). Mainly caused by using RAASi and other hyperkalemia-inducing drugs such as β-blockers, heparin, etc. (52), hyperkalemia is more common in individuals with HF or resistant hypertension and CKD, especially when having DM (53–55). Therefore, by maintaining normokalemia, potassium-binding polymers may contribute to achieve better outcomes among those necessitating treatment with RAASi. In this sense, our findings show that hyperkalemia related to treatment by the combination of ACEi and/or ARBs with spironolactone is countered efficaciously by patiromer, and probably by zirconium cyclosilicate. Importantly, our analysis did not consider eplerenone, although its potential to induce hyperkalemia is probably similar to spironolactone (56–59), nor the first-in-class angiotensin receptor–neprilysin inhibitor (ARNI) sacubitril/valsartan that may be associated to moderate hyperkalemia in the cases of schemes including an MRA (60).
Hyperkalemia is a complication proper of CKD, as the kidneys are the main regulators of potassium homeostasis (61). In subjects with HF, DM, and in all those needing treatment with RAASi, potassium excretion is impaired in a non-acute manner, such requiring dietary restriction and pharmacological interventions (e.g., potassium-binding polymers, use of drugs with improved hyperkalemic profile, avoidance of other drugs increasing serum potassium levels, etc.) (62). Therefore, given the known safety profile of new polymers, their efficacy against hyperkalemia should from now on be taken into account and, particularly, the benefit elucidated here for patiromer. Such effectiveness is pending to be clarified for SZC.
The benefit of using patiromer will likely to be extended to SZC. Sodium zirconium cyclosilicate was authorized for use by the US Food and Drug Administration (FDA) and the European Medicine Agency (EMA) in 2018. Nevertheless, trial data on this new polymer as those already existing on patiromer are necessary. This analysis is, thus, a starting point and an inspiration of further evaluations on the benefit of these and other nanomolecules with interest by their profile to improve clinical outcomes. In any case, for the moment, results from the ongoing trial DIAMOND (NCT03888066) studying patiromer in 2,388 participants are expected, as they will contribute to clarify findings presented here. Regular updating of analyses like this is very important.
Current recommendations to perform systematic reviews (63) and the standards to present optimally findings from network meta-analysis (64) proposed by the PRISMA research group were followed (14, 15). A multiple parallel one-stage systematic review design was used to retrieve dichotomous data on the studied outcomes. Prospective updating of the three systematic review protocols registered at the International Prospective Register of Systematic Reviews PROSPERO guarantees the transparency of all our methods and the entire analysis (65), confirming non-duplicity of the evaluation (66), and preventing the apparition of undesirable reporting biases (67).
Therefore, conclusions from this first-published dichotomous data pooling analysis can provide strong arguments on the kindness of the drugs assessed. Nevertheless, prudence is requested to readers when interpreting all messages transmitted here, as various limitations should be honestly declared. For the interest of clinicians, there were no data on SZC to perform calculations as those presented for patiromer in order to clarify a clinical impact of SZC on better dosing of MRA. More research will thus provide clinicians of more tools to combat hyperkalemia. Even if strength is the systematic approach, proper limitations of all systematic reviews should also be mentioned. Heterogeneity is an important limitation (66). Hyperkalemia was the common denominator of this analysis, leading to present effect sizes considering patients not only affected by HF or resistant hypertension; however, heterogeneity leads to present a benefit of binding potassium only for a subgroup of 1044 individuals with either HF or resistant hypertension (not for all patients with or at risk for hyperkalemia). A low inconsistency may influence in some degree the reliability of findings presented here, even if it is probably a reflection of heterogeneity (68). Publication bias was also observed and measured, and it is a discouraging finding, leading to overly optimistic conclusions in a meta-analysis (69): It is important to note, however, that our assessments include trials of <1,000 participants, so this study contributes to clarify potential false substantial effects reported by small trials (70). Furthermore, restricted evidence was an important problem to perform calculations that may be noted in effect sizes of overlapping doses of patiromer. In this context, the results obtained in our analysis, considering the outcome definitions that are in accordance to established limits in guidelines and studies (71–80), may change when performing calculations that consider other upper limits of normal (ULN) for serum potassium levels. Finally, non-assessable data on CPS involving patients before dialysis and on CPS and SPS involving patients undergoing dialysis may be considered also as arguments of restricted evidence.
The potential of zirconium cyclosilicate should be explored further, as no data exist to assess properly its capacity to optimize the dosing of RAASi, contrarily as it occurs for patiromer. In any case, considering their safety profile, new potassium-binding polymers may be considered as clinically relevant nanomolecules. In this way, regular intervals updating of evidence will be particularly important to improve the treatment of susceptible patient populations as those involved in this study, which may include observational evidence, if required (81).
Findings presented here correspond only to analyses carried out on clinical trials. This study belongs to an ongoing project aiming to assess clinical trial evidence and observational real-life evidence on the effectiveness of all commercial potassium-binding polymers, as performed by our team in a previous project (82), so further results are pending to be presented.
This manuscript presents findings from the first dichotomous data pooling analysis on the effectiveness of binding potassium. The assessed molecules were different with respect to their capacity to achieve normokalemia (sK+ 3.5–5.0 mEq/L) and acceptable kalemia (sK+ ≤ 5.1 mEq/L) in individuals with hyperkalemia (sK+ >5.1 mEq/L), and current evidence shows that patiromer can lead to the optimal dosing of spironolactone (and probably of other MRA) into schemes based on RAASi used by individuals with HF or resistant hypertension. These patients commonly have CKD. For the moment, there is no evidence to conclude that using zirconium cyclosilicate may allow optimizing treatment with MRA in RAASi-based schemes needing these patients. The lack of evidence should thus promote more research destined to confirm the benefits from this new polymer in order to enlarge options to control hyperkalemia. More research is also necessary to discern between the benefits of binding potassium among all type of hyperkalemic patients, for example, patients with DM who may need treatment for proteinuria, patients with early hypertension, etc. Future meta-analyses for updating findings presented here require more research for more homogenous findings on interventions against hyperkalemia.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
EG-A, FH-G, FÁ, and FL-S developed the hypothesis and study design. ÁM-B-M, ÁN-R, DF-Z, DM-G, EB-M, EG-A, FP, FL-S, JB-M, JG-V, MC, and MP performed the literature searches and/or screened papers. CO-S, FH-G, FÁ, and MC performed the data analyses. All authors contributed to the drafting and critical revision of all manuscript versions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank B. Muñoz (Clinical Epidemiology Support Office, Sanidad de Castilla y León, Zamora, Spain) and Begoña Valdés (Pharmacological Big Data Laboratory, University of Valladolid, Valladolid, Spain) who helped coordinate the data retrieval.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.686729/full#supplementary-material
1. Sarwar CMS, Papadimitriou L, Pitt B, Piña I, Zannad F, Anker SD, et al. Hyperkalemia in heart failure. J Am Coll Cardiol. (2016) 68:1575–89. doi: 10.1016/j.jacc.2016.06.060
2. House AA, Wanner C, Sarnak MJ, Piña IL, McIntyre CW, Komenda P, et al. Heart failure in chronic kidney disease: conclusions from a kidney disease: improving global outcomes (KDIGO) controversies conference. Kidney Int. (2019) 95:1304–17. doi: 10.1016/j.kint.2019.02.022
3. Rossignol P, Massy ZA, Azizi M, Bakris G, Ritz E, Covic A, et al. The double challenge of resistant hypertension and chronic kidney disease. Lancet. (2015) 386:1588–98. doi: 10.1016/S0140-6736(15)00418-3
4. Evans M, Palaka E, Furuland H, Bennett H, Linde C, Qin L, et al. The value of maintaining normokalaemia and enabling RAASi therapy in chronic kidney disease. BMC Nephrol. (2019) 20:31. doi: 10.1186/s12882-019-1228-y
5. Orso F, Fabbri G, Maggioni AP. Epidemiology of heart failure. Handb Exp Pharmacol. (2017) 243:15–33. doi: 10.1007/164_2016_74
6. Noubiap JJ, Nansseu JR, Nyaga UF, Sime PS, Francis I, Bigna JJ. Global prevalence of resistant hypertension: a meta-analysis of data from 3.2 million patients. Heart. (2019) 105:98–105. doi: 10.1136/heartjnl-2018-313599
7. Zannad F, Ferreira JP, Pitt B. Potassium binders for the prevention of hyperkalaemia in heart failure patients: implementation issues and future developments. Eur Heart J Suppl. (2019) 21:A55–A60. doi: 10.1093/eurheartj/suy034
8. Butler J, Khan MS, Anker SD. Novel potassium binders as enabling therapy in heart failure. Eur J Heart Fail. (2019) 21:550–2. doi: 10.1002/ejhf.1474
9. Mills EJ, Thorlund K, Ioannidis JPA. Demystifying trial networks and network meta-analysis. BMJ. (2013) 346:f2914. doi: 10.1136/bmj.f2914
10. Herrera-Gómez F, Chimeno MM, Martín-García D, Lizaraso-Soto F, Maurtua-Briseño-Meiggs Á, Grande-Villoria J, et al. Cholesterol-lowering treatment in chronic kidney disease: multistage pairwise and network meta-analyses. Sci Rep. (2019) 9:8951. doi: 10.1038/s41598-019-45431-5
11. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. (2015) 350:g7647. doi: 10.1136/bmj.g7647
12. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
13. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. (2011). Available online at: www.handbook.cochrane.org (accessed March 10, 2020).
14. Brown S, Hutton B, Clifford T, Coyle D, Grima D, Wells G, et al. A Microsoft-Excel-based tool for running and critically appraising network meta-analyses–an overview and application of NetMetaXL. Syst Rev. (2014) 3:110. doi: 10.1186/2046-4053-3-110
15. Systematic Reviews: Centre for Reviews and Dissemination's (CRD). Guidance for Undertaking Reviews in Health Care. University of York: York, UK. (2008). Available online at: https://york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed March 10, 2020).
16. Bushinsky DA, Williams GH, Pitt B, Weir MR, Freeman MW, Garza D, et al. Patiromer induces rapid and sustained potassium lowering in patients with chronic kidney disease and hyperkalemia. Kidney Int. (2015) 88:1427–33. doi: 10.1038/ki.2015.270
17. Bushinsky DA, Bakris GL, Williams GH, Pitt B, Mayo MR, Garza D, et al. SA-PO153: Patiromer induced a rapid onset of action and sustained K+ lowering throughout the dosing period in CKD patients with hyperkalemia. J Am Soc Nephrol. (2014) 25:669A. Available online at: https://www.asn-online.org/education/kidneyweek/archives/KW14Abstracts.pdf
18. Pergola PE, Spiegel DM, Warren S, Yuan J, Weir MR. Patiromer lowers serum potassium when taken without food: comparison to dosing with food from an open-label, randomized, parallel group hyperkalemia study. Am J Nephrol. (2017) 46:323–32. doi: 10.1159/000481270
19. Bushinsky DA, Spiegel DM, Yuan J, Warren S, Fogli J, Pergola PE. Effects of the potassium-binding polymer patiromer on markers of mineral metabolism. Clin J Am Soc Nephrol. (2019) 14:103–10. doi: 10.2215/CJN.04500418
20. Kloner RA, Gross C, Yuan J, Conrad A, Pergola PE. Effect of patiromer in hyperkalemic patients taking and not taking RAAS inhibitors. J Cardiovasc Pharmacol Ther. (2018) 23:524–31. doi: 10.1177/1074248418788334
21. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al. Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors. N Engl J Med. (2015) 372:211–21. doi: 10.1056/NEJMoa1410853
22. Weir MR, Mayo MR, Garza D, Arthur SA, Berman L, Bushinsky D, et al. Effectiveness of patiromer in the treatment of hyperkalemia in chronic kidney disease patients with hypertension on diuretics. J Hypertens. (2017) 35 (Suppl 1):S57–S63. doi: 10.1097/HJH.0000000000001278
23. Pitt B, Bakris GL, Bushinsky DA, Garza D, Mayo MR, Stasiv Y, et al. Effect of patiromer on reducing serum potassium and preventing recurrent hyperkalaemia in patients with heart failure and chronic kidney disease on RAAS inhibitors. Eur J Heart Fail. (2015) 17:1057–65. doi: 10.1002/ejhf.402
24. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al. FR-PO792: patiromer lowers serum K+ and prevents recurrent hyperkalemia in patients with diabetes and CKD on RAAS inhibitors: subgroup results. J Am Soc Nephrol. (2014) 25:550A–551A. doi: 10.1016/j.amjmed.2017.11.011
25. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al. FR-PO810: patiromer reduced RAASi dose discontinuations in CKD patients with moderate-to-severe hyperkalemia. J Am Soc Nephrol. (2014) 25:555A–556A. doi: 10.1016/j.kisu.2016.01.004
26. Weir MR, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, Wilson DJ, et al. TH-OR035: patiromer lowers serum K+ and prevents recurrent hyperkalemia in CKD patients ≥65 years of age on RAAS inhibitors. J Am Soc Nephrol. (2015) 26:10A. Available online at: https://www.asn-online.org/education/kidneyweek/archives/KW15Abstracts.pdf
27. Weir MR, Mayo MR, Garza D, Stasiv Y, Arthur SA, Berman L, et al. TH-PO658: chronic diuretic therapy does not impair the effectiveness of patiromer in hyperkalemic patients with CKD. J Am Soc Nephrol. (2015) 26:240A. Available online at: https://www.asn-online.org/education/kidneyweek/archives/KW15Abstracts.pdf
28. Bakris GL, Pitt B, Weir MR, Freeman MW, Mayo MR, Garza D, et al. Effect of patiromer on serum potassium level in patients with hyperkalemia and diabetic kidney disease: the AMETHYST-DN randomized clinical trial. JAMA. (2015) 314:151–61. doi: 10.1001/jama.2015.7446
29. Pitt B, Bakris GL, Weir MR, Freeman MW, Lainscak M, Mayo MR, et al. Long-term effects of patiromer for hyperkalaemia treatment in patients with mild heart failure and diabetic nephropathy on angiotensin-converting enzymes/angiotensin receptor blockers: results from AMETHYST-DN. ESC Heart Fail. (2018) 5:592–602. doi: 10.1002/ehf2.12292
30. Ash SR, Singh B, Lavin PT, Stavros F, Rasmussen HS. A phase 2 study on the treatment of hyperkalemia in patients with chronic kidney disease suggests that the selective potassium trap, ZS-9, is safe and efficient. Kidney Int. (2015) 88:404–11. doi: 10.1038/ki.2014.382
31. Packham DK, Rasmussen HS, Lavin PT, El-Shahawy MA, Roger SD, Block G, et al. Sodium zirconium cyclosilicate in hyperkalemia. N Engl J Med. (2015) 372:222–31. doi: 10.1056/NEJMoa1411487
32. Tumlin JA, Kosiborod M, Pergola PE, Qunibi W, Packham DK, Roger SD, et al. SA-PO1101: long-term (52-Week) efficacy and safety of ZS-9 in the treatment of hyperkalemia: Interim results from a phase 3 open-label, multi-center, multi-dose maintenance study. J Am Soc Nephrol. (2015) 26:B6. Available online at: https://www.asn-online.org/education/kidneyweek/archives/KW15Abstracts.pdf
33. Fishbane S, Pergola PE, Packham DK, Roger SD, Lerma E, Butler J, et al. TH-PO1112: efficacy and safety of sodium zirconium cyclosilicate for hyperkalemia: 12-month, open-label, phase 3 study. J Am Soc Nephrol. (2017) 28:390. Available online at: https://www.asn-online.org/education/kidneyweek/archives/KW17Abstracts.pdf
34. Kosiborod M, Rasmussen HS, Lavin P, Qunibi WY, Spinowitz B, Packham D, et al. Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia: the HARMONIZE randomized clinical trial. JAMA. (2014) 312:2223–33. doi: 10.1001/jama.2014.15688
35. Anker SD, Kosiborod M, Zannad F, Piña IL, McCullough PA, Filippatos G, et al. Maintenance of serum potassium with sodium zirconium cyclosilicate (ZS-9) in heart failure patients: results from a phase 3 randomized, double-blind, placebo-controlled trial. Eur J Heart Fail. (2015) 17:1050–6. doi: 10.1002/ejhf.300
36. Lepage L, Dufour A-C, Doiron J, Handfield K, Desforges K, Bell R, et al. Randomized clinical trial of sodium polystyrene sulfonate for the treatment of mild hyperkalemia in CKD. Clin J Am Soc Nephrol. (2015) 10:2136–42. doi: 10.2215/CJN.03640415
37. Pitt B, Bushinsky DA, Kitzman DW, Ruschitzka F, Metra M, Filippatos G, et al. Evaluation of an individualized dose titration regimen of patiromer to prevent hyperkalaemia in patients with heart failure and chronic kidney disease. ESC Heart Fail. (2018) 5:257–66. doi: 10.1002/ehf2.12265
38. Pitt B, Bushinsky D, Halfon S, Kitzman D, Lainscak M, Mathur V, et al. A multicenter study of dose titration of the oral potassium binder rly5016 to maintain normal serum potassium in patients with heart failure and chronic kidney disease treated with renin-angiotensin-aldosterone inhibitors and/or beta-blockers. J Am Coll Cardiol. (2011) 57:E301. doi: 10.1016/S0735-1097(11)60301-X
39. Pitt B, Anker SD, Bushinsky DA, Kitzman DW, Zannad F, Huang I-Z, et al. Evaluation of the efficacy and safety of RLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF) trial. Eur Heart J. (2011) 32:820–8. doi: 10.1093/eurheartj/ehq502
40. Agarwal R, Rossignol P, Romero A, Garza D, Mayo MR, Warren S, et al. Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a phase 2, randomised, double-blind, placebo-controlled trial. Lancet. (2019) 394:1540–50. doi: 10.1016/S0140-6736(19)32135-X
41. Li X, Xu G, Lin H, Hu Z, Yu X, Xing C, et al. MP341: Calcium polystyrene sulfonate in treating hyperkalemia patients with renal insufficiency. Nephrol Dial Transplant. (2013) 28:i405. doi: 10.1093/ndt/gft140
42. Nasir K, Ahmad A. Treatment of hyperkalemia in patients with chronic kidney disease: a comparison of calcium polystyrene sulphonate and sodium polystyrene sulphonate. J Ayub Med Coll Abbottabad. (2014) 26:455–58.
43. Nakayama Y, Ueda K, Yamagishi S-I, Sugiyama M, Yoshida C, Kurokawa Y, et al. Compared effects of calcium and sodium polystyrene sulfonate on mineral and bone metabolism and volume overload in pre-dialysis patients with hyperkalemia. Clin Exp Nephrol. (2018) 22:35–44. doi: 10.1007/s10157-017-1412-y
44. Wang J, Lv M-M, Zach O, Wang L-Y, Zhou M-Y, Song G-R, et al. Calcium-polystyrene sulfonate decreases inter-dialytic hyperkalemia in patients undergoing maintenance hemodialysis: a prospective, randomized, crossover study. Ther Apher Dial. (2018) 22:609–16. doi: 10.1111/1744-9987.12723
45. Gruy-Kapral C, Emmett M, Santa Ana CA, Porter JL, Fordtran JS, Fine KD. Effect of single dose resin-cathartic therapy on serum potassium concentration in patients with end-stage renal disease. J Am Soc Nephrol. (1998) 9:1924–30. doi: 10.1681/ASN.V9101924
46. Meaney CJ, Beccari MV, Yang Y, Zhao J. Systematic review and meta-analysis of patiromer and sodium zirconium cyclosilicate: a new armamentarium for the treatment of hyperkalemia. Pharmacotherapy. (2017) 37:401–11. doi: 10.1002/phar.1906
47. Palaka E, Leonard S, Buchanan-Hughes A, Bobrowska A, Langford B, Grandy S. Evidence in support of hyperkalaemia management strategies: a systematic literature review. Int J Clin Pract. (2018) 72:e13052. doi: 10.1111/ijcp.13052
48. Das S, Dey JK, Sen S, Mukherjee R. Efficacy and safety of patiromer in hyperkalemia: a systematic review and meta-analysis. J Pharm Pract. (2018) 31:6–17. doi: 10.1177/0897190017692921
49. Varallo FR, Trombotto V, Lucchetta RC, Mastroianni P, de C. Efficacy and safety of the pharmacotherapy used in the management of hyperkalemia: a systematic review. Pharm Pract. (2019) 17:1361. doi: 10.18549/PharmPract.2019.1.1361
50. Llubani R, Vukadinović D, Werner C, Marx N, Zewinger S, Böhm M. Hyperkalaemia in heart failure-pathophysiology, implications and therapeutic perspectives. Curr Heart Fail Rep. (2018) 15:390–7. doi: 10.1007/s11897-018-0413-9
51. Kovesdy CP, Matsushita K, Sang Y, Brunskill NJ, Carrero JJ, Chodick G, et al. Serum potassium and adverse outcomes across the range of kidney function: a CKD Prognosis consortium meta-analysis. Eur Heart J. (2018) 39:1535–42. doi: 10.1093/eurheartj/ehy100
52. Ben Salem C, Badreddine A, Fathallah N, Slim R, Hmouda H. Drug-induced hyperkalemia. Drug Saf. (2014) 37:677–92. doi: 10.1007/s40264-014-0196-1
53. Takaichi K, Takemoto F, Ubara Y, Mori Y. Analysis of factors causing hyperkalemia. Intern Med. (2007) 46:823–9. doi: 10.2169/internalmedicine.46.6415
54. Loutradis C, Tolika P, Skodra A, Avdelidou A, Sarafidis PA. Prevalence of hyperkalemia in diabetic and non-diabetic patients with chronic kidney disease: a nested case-control study. Am J Nephrol. (2015) 42:351–60. doi: 10.1159/000442393
55. Belmar Vega L, Galabia ER, Bada da Silva J, Bentanachs González M, Fernández Fresnedo G, Piñera Haces C, et al. Epidemiology of hyperkalemia in chronic kidney disease. Nefrologia. (2019) 39:277–86. doi: 10.1016/j.nefroe.2018.11.014
56. Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. (2003) 348:1309–21. doi: 10.1056/NEJMoa030207
57. Pitt B, Bakris G, Ruilope LM, DiCarlo L, Mukherjee R, EPHESUS Investigators. Serum potassium and clinical outcomes in the eplerenone post-acute myocardial infarction heart failure efficacy and survival study (EPHESUS). Circulation. (2008) 118:1643–50. doi: 10.1161/CIRCULATIONAHA.108.778811
58. Zannad F, McMurray JJV, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. (2011) 364:11–21. doi: 10.1056/NEJMoa1009492
59. Eschalier R, McMurray JJV, Swedberg K, van Veldhuisen DJ, Krum H, Pocock SJ, et al. Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: analyses of the EMPHASIS-HF study subgroups (Eplerenone in Mild Patients Hospitalization And SurvIval Study in Heart Failure). J Am Coll Cardiol. (2013) 62:1585–93. doi: 10.1016/j.jacc.2013.04.086
60. Desai AS, Vardeny O, Claggett B, McMurray JJV, Packer M, Swedberg K, et al. Reduced risk of hyperkalemia during treatment of heart failure with mineralocorticoid receptor antagonists by use of sacubitril/valsartan compared with enalapril: a secondary analysis of the PARADIGM-HF trial. JAMA Cardiol. (2017) 2:79–85. doi: 10.1001/jamacardio.2016.4733
61. De Nicola L, Di Lullo L, Paoletti E, Cupisti A, Bianchi S. Chronic hyperkalemia in non-dialysis CKD: controversial issues in nephrology practice. J Nephrol. (2018) 31:653–64. doi: 10.1007/s40620-018-0502-6
62. Kim G-H. Pharmacologic treatment of chronic hyperkalemia in patients with chronic kidney disease. Electrolyte Blood Press. (2019) 17:1–6. doi: 10.5049/EBP.2019.17.1.1
63. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
64. Hutton B, Salanti G, Chaimani A, Caldwell DM, Schmid C, Thorlund K, et al. The quality of reporting methods and results in network meta-analyses: an overview of reviews and suggestions for improvement. PLoS ONE. (2014) 9:e92508. doi: 10.1371/journal.pone.0092508
65. Stewart L, Moher D, Shekelle P. Why prospective registration of systematic reviews makes sense. Syst Rev. (2012) 1:7. doi: 10.1186/2046-4053-1-7
66. Moher D. The problem of duplicate systematic reviews. BMJ. (2013) 347:f5040. doi: 10.1136/bmj.f5040
67. Kirkham JJ, Altman DG, Williamson PR. Bias due to changes in specified outcomes during the systematic review process. PLoS ONE. (2010) 5:e9810. doi: 10.1371/journal.pone.0009810
68. Donegan S, Williamson P, D'Alessandro U, Tudur Smith C. Assessing key assumptions of network meta-analysis: a review of methods. Res Synth Methods. (2013) 4:291–323. doi: 10.1002/jrsm.1085
69. Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. (2000) 53:1119–29. doi: 10.1016/S0895-4356(00)00242-0
70. Ioannidis JPA. Why most discovered true associations are inflated. Epidemiology. (2008) 19:640–8. doi: 10.1097/EDE.0b013e31818131e7
71. Einhorn LM, Zhan M, Hsu VD, Walker LD, Moen MF, Seliger SL, et al. The frequency of hyperkalemia and its significance in chronic kidney disease. Arch Intern Med. (2009) 169:1156–62. doi: 10.1001/archinternmed.2009.132
72. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart failure society of America. J Am Coll Cardiol. (2017) 70:776–803. doi: 10.1161/CIR.0000000000000509
73. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the european society of cardiology (ESC)developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
74. National Kidney Foundation. Guideline 11: Use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in CKD. In: K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease. (2002). Available online at: https://kidneyfoundation.cachefly.net/professionals/KDOQI/guidelines_bp/guide_11.htm (accessed June 2, 2021).
75. National Institute for Health and Clinical Excellence (NICE) [UK]. Chronic kidney disease (CG73): Early identification and management of chronic kidney disease in adults in primary and secondary care. (2008). Available online at: https://www.nice.org.uk/guidance/cg73 (accessed June 2, 2021).
76. Heart Failure Society of America, Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA. HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. (2010) 16:e1–194. doi: 10.1016/j.cardfail.2010.04.004
77. Weinberg JM, Appel LJ, Bakris G, Gassman JJ, Greene T, Kendrick CA, et al. Risk of hyperkalemia in nondiabetic patients with chronic kidney disease receiving antihypertensive therapy. Arch Intern Med. (2009) 169:1587–94. doi: 10.1001/archinternmed.2009.284
78. Iino Y, Hayashi M, Kawamura T, Shiigai T, Tomino Y, Yamada K, et al. Renoprotective effect of losartan in comparison to amlodipine in patients with chronic kidney disease and hypertension–a report of the Japanese Losartan Therapy Intended for the Global Renal Protection in Hypertensive Patients (JLIGHT) study. Hypertens Res. (2004) 27:21–30. doi: 10.1291/hypres.27.21
79. Miao Y, Dobre D, Heerspink HJL, Brenner BM, Cooper ME, Parving H-H, et al. Increased serum potassium affects renal outcomes: a post hoc analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) trial. Diabetologia. (2011) 54:44–50. doi: 10.1007/s00125-010-1922-6
80. Avapro [package insert]. Bridgewater, NJ: sanofi-aventis U.S. LLC. (2012). Available online at: https://products.sanofi.us/avapro/avapro.pdf (accessed June 2, 2021).
81. O'Neil M, Berkman N, Hartling L, Chang S, Anderson J, Motu'apuaka M, et al. Observational evidence and strength of evidence domains: case examples. Syst Rev. (2014) 3:35. doi: 10.1186/2046-4053-3-35
82. Bernuy-Guevara C, Chehade H, Muller YD, Vionnet J, Cachat F, Guzzo G, et al. The inhibition of complement system in formal and emerging indications: results from parallel one-stage pairwise and network meta-analyses of clinical trials and real-life data studies. Biomedicines. (2020) 8:355. doi: 10.3390/biomedicines8090355
Keywords: hyperkalemia, mineralocorticoid receptor antagonists, nanomedicine, meta-analysis (as topic), potassium-binding polymers
Citation: Lizaraso-Soto F, Gutiérrez-Abejón E, Bustamante-Munguira J, Martín-García D, Chimeno MM, Nava-Rebollo Á, Maurtua-Briseño-Meiggs Á, Fernández-Zoppino D, Bustamante-Munguira E, de Paz FJ, Grande-Villoria J, Ochoa-Sangrador C, Pascual M, Álvarez FJ and Herrera-Gómez F (2021) Binding Potassium to Improve Treatment With Renin-Angiotensin-Aldosterone System Inhibitors: Results From Multiple One-Stage Pairwise and Network Meta-Analyses of Clinical Trials. Front. Med. 8:686729. doi: 10.3389/fmed.2021.686729
Received: 27 March 2021; Accepted: 12 July 2021;
Published: 19 August 2021.
Edited by:
Hoon Young Choi, Yonsei University, South KoreaReviewed by:
Mark Dominik Alscher, Robert Bosch Hospital, GermanyCopyright © 2021 Lizaraso-Soto, Gutiérrez-Abejón, Bustamante-Munguira, Martín-García, Chimeno, Nava-Rebollo, Maurtua-Briseño-Meiggs, Fernández-Zoppino, Bustamante-Munguira, de Paz, Grande-Villoria, Ochoa-Sangrador, Pascual, Álvarez and Herrera-Gómez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Bustamante-Munguira, amJ1c3RhbWFudGVtdW5ndWlyYUBnbWFpbC5jb20=
†These authors share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.