 Borja Hernández-Breijo1*†
Borja Hernández-Breijo1*† Chamaida Plasencia-Rodríguez1,2‡
Chamaida Plasencia-Rodríguez1,2‡ Victoria Navarro-Compán1,2
Victoria Navarro-Compán1,2 Carlota García-Hoz3†
Carlota García-Hoz3† Israel Nieto-Gañán3
Israel Nieto-Gañán3 Cristina Sobrino4Javier Bachiller-Corral4Mariana Díaz-Almirón5Ana Martínez-Feito1,6Teresa Jurado1Paloma Lapuente-Suanzes3Gema Bonilla2Cristina Pijoán-Moratalla4Garbiñe Roy3Mónica Vázquez-Díaz4
Cristina Sobrino4Javier Bachiller-Corral4Mariana Díaz-Almirón5Ana Martínez-Feito1,6Teresa Jurado1Paloma Lapuente-Suanzes3Gema Bonilla2Cristina Pijoán-Moratalla4Garbiñe Roy3Mónica Vázquez-Díaz4 Alejandro Balsa1,2
Alejandro Balsa1,2 Luisa M. Villar3Dora Pascual-Salcedo1Eulalia Rodríguez-Martín3‡
Luisa M. Villar3Dora Pascual-Salcedo1Eulalia Rodríguez-Martín3‡- 1Immuno-Rheumatology Research Group, Hospital La Paz Institute for Health Research-IdiPAZ, Madrid, Spain
- 2Rheumatology, La Paz University Hospital, Madrid, Spain
- 3Immunology, Ramón y Cajal Institute for Health Research, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 4Rheumatology, Ramón y Cajal Institute for Health Research, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 5Biostatistics Unit, Hospital La Paz Institute for Health Research-IdiPAZ, Madrid, Spain
- 6Immunology, La Paz University Hospital, Madrid, Spain
Biological therapies, such as TNF inhibitors (TNFi), are increasing remission (REM) rates in rheumatoid arthritis (RA) patients, although these are still limited. The aim of our study was to analyze changes in the profile of peripheral blood mononuclear cells (PBMC) in patients with RA treated with TNFi in relation to the clinical response. This is a prospective and observational study including 78 RA patients starting the first TNFi. PBMC were analyzed by flow cytometry both at baseline and at 6 months. Disease activity at the same time points was assessed by DAS28, establishing DAS28 ≤ 2.6 as the criteria for REM. Logistic regression models were employed to analyze the association between the changes in PBMC and REM. After 6 months of TNFi treatment, 37% patients achieved REM by DAS28. Patients who achieved REM showed a reduction in the percentage of naive B cells, but only when patients had received concomitant methotrexate (MTX) (OR: 0.59; 95% CI: 0.39–0.91). However, no association was found for patients who did not receive concomitant MTX (OR: 0.85; 95% CI: 0.63–1.16). In conclusion, PBMC, mainly the B-cell subsets, are modified in RA patients with TNFi who achieve clinical REM. A significant decrease in naive B-cell percentage is associated with achieving REM after 6 months of TNFi treatment in patients who received concomitant therapy with MTX.
Introduction
Tumor necrosis factor inhibitors (TNFi) are widely used for the treatment of patients with rheumatoid arthritis (RA), who do not respond to conventional synthetic disease-modifying antirheumatic drugs (csDMARDs). However, 20–40% of patients do not achieve an adequate clinical response to TNFi (1). Moreover, despite the continuous advances in the understanding of the molecular mechanisms underlying the effect of TNFi therapy, there is still a lack of objective parameters associated with clinical response to TNFi in RA (2, 3).
It is well-known that different types of immune cells such as monocytes and natural killer (NK), T, and B cells are involved in the development of inflammation and autoimmunity in the RA pathogeny (4–6). Although these cells are recruited to inflamed synovium, peripheral blood mononuclear cells (PBMC) may be reflecting the local inflammation, thus providing useful information about the disease status. Accordingly, several publications have reported that TNFi treatment could modify the proportion of the different PBMC subsets (7–9). The effect of TNFi on B cells has not been extensively studied and controversial results have been reported. On the one hand, published data showed that TNFi treatment may increase the frequency of CD27+ memory B cells in responders (10). On the other hand, other studies described reduced CD27+ or double negative IgD− CD27− memory B cells as a consequence of TNFi therapy (11, 12). In a different study, the frequency of IL-10 producing regulatory B cells (B10 cells) appears to be increased by TNFi treatment in responders (9). We have recently published that patients who did not achieve remission by Disease Activity Score-28 (DAS28) after 6 months of TNFi therapy showed lower percentages of total and naive B cells at baseline than remission (REM) subjects. However, to deepen into this field, more studies are needed (13).
In this study, we aimed to analyze whether treatment with TNFi modulates PBMC in relation to clinical response in patients with RA.
Materials and Methods
Patients
This was a prospective, observational, longitudinal bi-center pilot study, including 78 patients with RA starting a first TNFi [infliximab (n = 14), adalimumab (n = 3), etanercept (n = 37), golimumab (n = 8), or certolizumab (n = 16)] according to national recommendations and followed-up for 6 months (14). Forty-five patients were from La Paz University Hospital and 33 patients from Ramón y Cajal University Hospital, in Madrid, Spain. All included patients were adults (age over 18), fulfilled the ACR/EULAR 2010 classification criteria for RA, and had moderate or high disease activity (DAS28 > 3.2) (15). Approvals were obtained from the Institutional Ethics Committees from both centers (PI-018/17; PI-2618) in accordance with the Helsinki Declaration. All patients signed an informed consent document before inclusion.
Clinical Data
Disease activity was assessed by DAS28 at baseline (before starting TNFi) and after 6 months of treatment. REM was defined as DAS28 ≤ 2.6 after 6 months of TNFi therapy. The achievement of REM was established as our clinical outcome in responder patients (16). In addition, disease activity was assessed by the Simple Disease Activity Index (SDAI), and REM was defined as SDAI ≤ 3.3 for the sensitivity analysis (17).
Isolation of PBMC From Human Peripheral Blood
Blood samples were collected at baseline and after 6 months of TNFi treatment. For baseline samples, blood was collected from patients just before starting TNFi. For samples at 6 months, blood was collected within 24 h before TNFi administration. PBMC were purified from heparinized venous blood by Ficoll®-Paque PREMIUM (GE Healthcare, Chicago, IL, USA) density gradient centrifugation, and cells were subsequently cryopreserved (10% DMSO) in liquid N2 in aliquots of 5 × 106 cells until studied (18). Basal and 6-month samples were studied simultaneously to avoid interassay variability. We recorded for every leukocyte subset total cell counts per ml of blood calculated by measuring total lymphocyte and monocyte numbers by a Coulter counter and the percentages of every subset over total mononuclear cells.
Flow Cytometry Analysis
PBMC were thawed and resuspended (106 cells/ml) in RPMI 1,640 medium (Life Technologies, Carlsbad, CA, USA) supplemented with 10% heat-inactivated fetal bovine serum (Life Technologies), 1% L-glutamine, and 1% penicillin–streptomycin at the time of analysis. PBMC were subsequently incubated with specific monoclonal antibodies for membrane antigen staining during 20 min at 4°C in the dark and then washed with PBS. Then, PBMC were acquired on a FACSCanto II cytometer (BD Biosciences, San Diego, CA, USA). Data were analyzed using FACSDiva software, version 8.0.1 (BD Biosciences). Mean autofluorescence values were set using appropriate negative isotype controls.
Monocyte and lymphocyte populations were studied. The following monoclonal antibodies were used: CD4-FITC, CD14-FITC, CD197-PE (CCR7-PE), CD3-PerCP, CD19-PE-Cy7, CD56-PE-Cy7, CD45RO-APC, CD27-APC, CD8-APC-H7, CD3-BV421, and CD45-V500-C (all from BD Biosciences). According to the differential expression of several antigens, CD4+ and CD8+ T cells were classified as naive (CCR7+ CD45RO−), central memory (CCR7+ CD45RO+), effector memory (CCR7− CD45RO+), or terminally differentiated effector memory (CCR7− CD45RO−). B cells were classified as total CD19+ B cells, naive (CD19+ CD27−), or memory (CD19+ CD27+). CD56+ cells were subdivided into NK cells (CD56dim CD3−), natural killer T (NKT) cells (CD56dim CD3+), and NK regulatory cells (CD3− CD56bright). Monocytes were classified as CD14+ cells. Gating strategies are described in Supplementary Figures 1, 2. A gate including lymphocytes and monocytes, but excluding debris, duplets, and apoptotic cells, was established. Viable CD45+ cells were confirmed by nonstaining with 7-AAD (Supplementary Figure 1, gate R6). A minimum amount of 100,000 events concerning viable CD45+ cells was analyzed.
Statistical Analyses
Descriptive analyses were performed for the demographic and clinical variables. The results were shown as mean and SD [or median and interquartile range (IQR)] for continuous variables and absolute numbers and relative frequencies for categorical variables. The frequency data were compared using Fisher's exact tests. Comparisons of unpaired continuous data were conducted using the unpaired t-test or Mann–Whitney U-test, depending on data distribution. Comparisons of paired continuous data were conducted using the paired t-test or Wilcoxon, depending on data distribution. In a previous study conducted by our group including the same cohort of patients, the correction of multiple comparisons using the Benjamini–Hochberg (BH) method with a predefined value FDR = 0.25 was applied (free software used MEV 2.0). This analysis demonstrated that the associations of either total or naive B lymphocytes with REM were not due to chance (13). Therefore, clinical follow-up analyses after initiation of TNFi therapy have been performed in these two subpopulations.
The associations between either the clinical/serological variables or the percentage of change (Δ, 6–0 months) within each PBMC subset and REM at 6 months were evaluated by uni- and multivariable logistic regression (odds ratio; 95% CI). The presence of possible interactions with covariates was tested, stratifying the results if significant. In case of no significant interaction, the model was later adjusted for these covariates.
A p-value < 0.05 was considered as statistically significant. The Statistical Package for the Social Sciences version 24 (SPSS, Chicago, IL, USA) was used for the analyses. The GraphPad Prism version 7 (GraphPad Software, San Diego, CA, USA) was used to prepare the graphs.
Patient and Public Involvement
Patients did not cooperate with us in the design of the study. However, it was explained to them prior to inclusion, and they all agreed to participate.
Results
Patients' Characteristics
Demographic and clinical baseline characteristics are shown in Table 1. The mean baseline disease activity (DAS28) was 4.9. Forty-one (53%) patients were treated with TNFi monoclonal antibodies (infliximab, adalimumab, golimumab, certolizumab) and 37 (47%) patients with a TNFi fusion protein (etanercept). Concomitant MTX was administered in 58 (74%) patients. After 6 months of TNFi therapy, 29 (37%) patients achieved REM by DAS28. According to clinical REM achievement (DAS28 ≤ 2.6) after 6 months of TNFi treatment, differences at baseline between REM and non-REM patients were analyzed. Overall, no differences between baseline characteristics in both groups were found, except for DAS28. Baseline DAS28 was lower in patients who attained REM (4.2 ± 0.9 vs. 5.3 ± 0.9; p < 0.001).
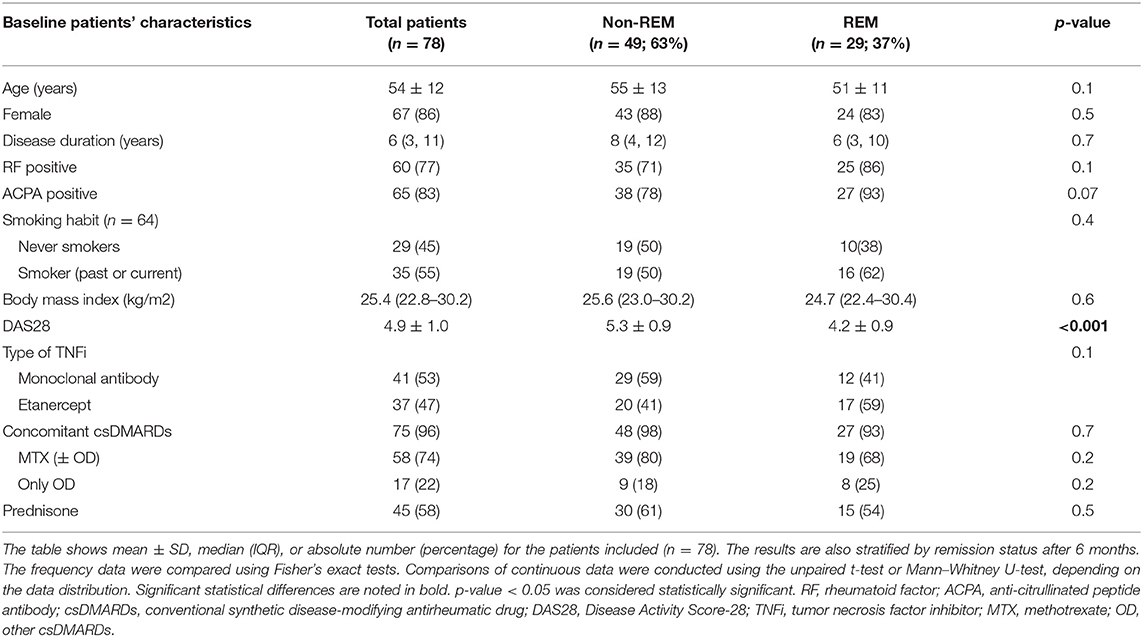
Table 1. Baseline characteristics of patients included in the study.
Univariable analyses were performed to investigate the association between REM and the baseline patients' characteristics. A significant association was found for lower baseline DAS28 (OR: 0.28; 95% CI: 0.19–0.51). Associations of REM with other baseline patients' characteristics, such as age (OR: 0.97; 95% CI: 0.94–1.01), rheumatoid factor (RF) positivity (OR: 2.50; 95% CI: 0.73–8.50), anti-citrullinated protein antibody (ACPA) positivity (OR: 3.91; 95% CI: 0.80–19.07), or the type of TNFi (reference fusion protein, etanercept) used (OR: 2.05; 95% CI: 0.81–5.22) were also found, although they were not significant (Table 2). Therefore, further analyses were adjusted by the patients' and disease's characteristics with a p < 0.1 in the univariable analysis (ACPA and baseline DAS28) as well by the type of TNFi used.
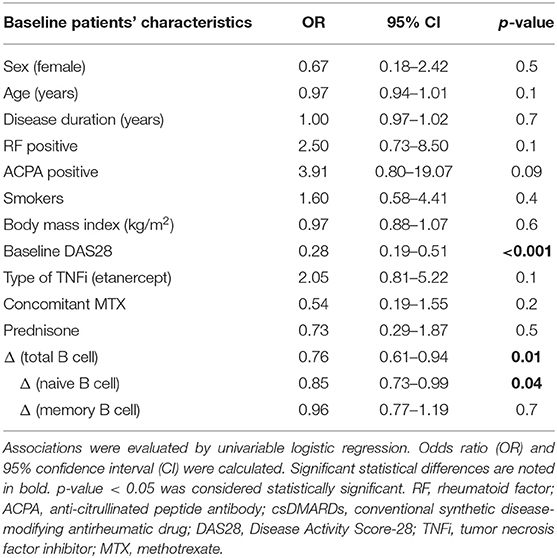
Table 2. Association between patients' characteristics and clinical remission (DAS28 ≤ 2.6) after 6 months of TNFi treatment.
PBMC Subset Changes After 6 Months of TNFi Treatment
Different PBMC subsets were analyzed at baseline and after 6 months of TNFi treatment, in order to identify whether PBMC profile changes after TNFi therapy (Δ, 6–0 months). A previous analysis in our cohort of patients showed that a higher percentage of baseline B cells (especially naive B cells) was associated with attaining REM after 6 months of TNFi treatment (13).
The present results showed a significant reduction in the percentage of total B cells in patients who achieved REM compared with non-REM patients, after 6 months of TNFi treatment (p = 0.01). It was mainly due to a reduction of naive B cells in REM patients (p = 0.04). No differences in percentage for any other PBMC subset analyzed were observed (Supplementary Table 1). In addition, the analysis of the absolute cell number was performed; however, no differences were found for none of the PBMC subset evaluated (Supplementary Table 4).
Association Between PBMC Subset Changes and Clinical Remission
In The Univariable analysis, a significant association between REM achievement and a reduction of total B-cell percentage (OR: 0.76; 95% CI: 0.61–0.94) was found. After evaluating B-cell subtypes, it was observed that this association was mainly due to a reduction in naive B cells (OR: 0.85; 95% CI: 0.73–0.99) (Table 2). No significant associations were found for the other analyzed PBMC subsets (Supplementary Table 2).
The presence of interactions between the change of naive B cells (Δ naive B cells) and REM achievement after 6 months of TNFi therapy was tested. A significant interaction between the change in the percentage of naive B cells and the use of concomitant MTX was found (Wald chi-square value = 4.56; p = 0.03). Therefore, further analyses over the association between the Δ naive B cells and REM were stratified according to the use of concomitant MTX. No significant interactions with other variables were found (Supplementary Table 3).
Fifty-eight (74%) patients received concomitant MTX. Interestingly, the results of the multivariable analysis showed that a reduction in the percentage of naive B cell was independently associated with REM after 6 months of treatment with TNFi only in the group of patients who received concomitant MTX (OR: 0.59; 95% CI: 0.39–0.91). No association was found for the group of patients who did not receive concomitant MTX (OR: 0.85; 95% CI: 0.63–1.16). However, a lower DAS28 at baseline was also independently associated with REM, regardless of the use of concomitant MTX (Table 3).
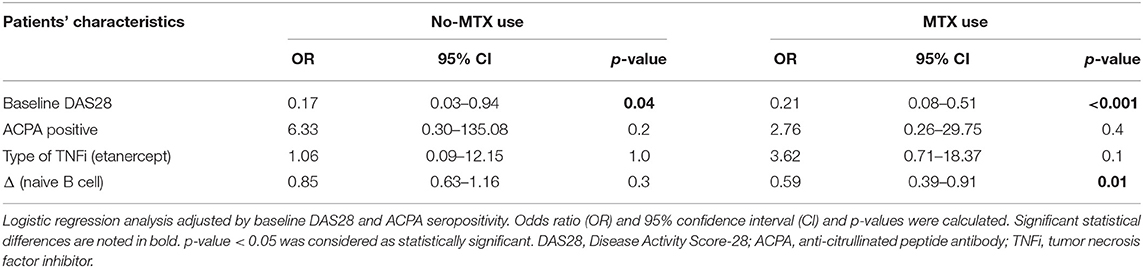
Table 3. Analysis of the association between Δ (naive B cell) and clinical remission (DAS28 ≤ 2.6) after 6 months of TNFi treatment, stratified by the concomitant use of MTX.
In order to confirm our results, a sensitivity analysis was performed employing the SDAI definition for clinical REM (SDAI ≤ 3.3). Out of the 78 patients, 17% (n = 13) achieved clinical remission according to this criterion. The results were consistent with the evaluation through DAS28, finding that a reduction in the percentage of naive B cells was associated with REM after 6 months of treatment with TNFi, mainly in the group of patients who received concomitant MTX (OR: 0.45; 95% CI: 0.24–0.88). However, no association was found for the group of patients who did not receive concomitant MTX (OR: 0.84; 95% CI: 0.66–1.08).
Discussion
In this study, we aimed to investigate how peripheral blood cell profile can be modified after TNFi treatment, according to the clinical response in patients with RA. The results showed that a reduction in the percentage of peripheral naive B cells was associated with attaining REM in patients with RA treated with TNFi, mainly in combination with MTX.
The latest breakthroughs in the physiopathology of RA highlighted the activation of naive B cells as the trigger of the joint flare initiation and, therefore, gave them a central role in the pathogenesis of the disease (19, 20). Although the mechanism of this B-cell activation remains unknown, several investigations have pointed out that defects on B-cell receptor (BCR) signaling may cause breakdown of B-cell tolerance. This may lead to maturation of autoreactive B cells, associated to the development of autoimmunity (21, 22) and to the subsequent RF and ACPA production (23–25). Moreover, it has been demonstrated that activated B cells can act as antigen-presenting cells by the processing and presenting of antigenic peptides to CD4+ T cells (26). This presentation ability promotes or triggers the proinflammatory environment that is found in RA (27). Furthermore, this B-cell ability would be enhanced in RF-positive patients, given that B cells can capture antigen–Ig immune complexes via their membrane immunoglobulin receptors and react with the IgG Fc part of antibody molecules. Then, antigen is processed and presented to CD4+ T cells, initiating the immune response (28).
Although it is still unclear and controversial, some publications have suggested that B cells could play a relevant role in the response to TNFi. This controversy may be related to the variability within the different RA cohorts (age, disease duration, seropositivity, disease activity, treatment with TNFi and/or csDMARDs) and the different criteria used to assess clinical response (10, 29). These cofounders should be taken into account when differences between cell populations are analyzed. Moura et al. suggested, in a study with a small number of patients, that treatment with TNFi restores the frequency of a subtype of peripheral memory B cells to normal levels, regardless of the clinical response (12). Moreover, Daien et al. reported that a high baseline level of CD27+ memory B cells was associated with good clinical response to TNFi (10). In addition, a different B-cell subpopulation that could be affected by TNFi treatment is IL-10-producing memory B cells (B10). Bankó et al. suggested that B10 increases after TNFi treatment in responding RA patients (9). In our study, in which all the analyses were adjusted by confounders, a significant decrease in the percentage of B cells in REM patients after 6 months of TNFi therapy, mainly due to naive B cells, was found. These results could suggest that this reduction is related to the fact that patients in REM had lower production of cytokines such as interleukin-6 (IL-6), TNFα, interleukin-12 (IL-12), or granulocyte macrophage-colony stimulating factor (GM-CSF), by different PBMC subsets (30, 31). In consequence, it is hypothesized that the reduction in the frequency of naive B cells in patients who achieved remission is mainly due to the improvement of inflammatory activity, regardless of the type of drug itself. To confirm this hypothesis, it would be highly interesting to evaluate it with other bDMARDs, or even with targeted synthetic DMARDs or csDMARDs.
A novel and interesting finding of our study is that the association between the reduction in the percentage of naive B cells and the achievement of REM was mainly observed in the group of patients who received TNFi concomitantly with MTX. Therefore, because of MTX mechanism of action, T cells would reduce the production of cytokines such as TNFα, IL-6, or GM-CSF (32). The diminished IL-6 and GM-CSF production may have as a consequence lesser development and survival of B cells (33, 34). Consequently, their reduction by MTX may be impairing the development of B cells (35). A recent study from our research group reported that patients with early RA who responded to MTX therapy had significantly decreased circulating transitional B cells, supporting also the impairment of B-cell development (36). Although the effect of MTX would seem enough potent to improve the clinical manifestations of the disease, our cohort showed that the proportion of patients using concomitant MTX was no different between REM and non-REM groups. In this sense, it is relevant to take into account that the activity indices to control RA include both inflammatory (swollen joints and acute phase reactants) and others less dependent on inflammation (tender joints and patient global assessment) parameters. Indeed, there may be patients in clinical REM who persist having tender and/or swollen joints, as well as elevation of acute phase reactants. It would be very interesting to conduct further studies to investigate whether the co-administration of TNFi and MTX produces a synergistic effect on the immunological expression of inflammatory molecules that translates into greater clinical remission of the disease.
Currently, the core principles of the treat-to-target (T2T) strategy in RA are shared decision-making and regular patient review with a target of REM or, failing that, low disease activity to ensure optimal outcomes (37, 38). Therefore, objective parameters of REM are necessary to achieve a successful outcome following the T2T strategy. In this study, we identify that naive B-cell subset is modulated after TNFi therapy in patients who achieve REM. At the moment, we do not know whether this may have implications with long-term outcome measurements and therefore could be useful to monitor TNFi therapy. In addition, independent to the reduction in the percentage of naive B cells after 6 months of TNFi treatment, a low baseline DAS28 was also associated with REM achievement. This result was in agreement with previous investigations. Aletaha et al. demonstrated that lower baseline disease activity is associated with achieving clinical REM (39).
One of the limitations of our study was the population included; however, sample size calculation (before starting the patient recruitment) showed that 78 patients naive to TNFi would be enough to demonstrate statistical differences in the proposed clinical outcomes. The other limitation of the study was that patients who attained REM after 6 months of TNFi treatment showed lower baseline DAS28 than patients who did not attain it. However, baseline disease activity did not interact with the association between the reduction of the percentage of naive B cells and REM, both parameters remaining independently associated. On the other hand, as it was previously described (12), CD19+ CD27− cells are mostly naive B cells, but a small proportion of them are memory B cells. However, due to our gating strategy that did not include IgD, it was not possible to discriminate this small subset of double negative memory B cells defined as CD19+ CD27− IgD−. Another limitation of our study was not performing in vitro functional evaluation to analyze in detail the mechanism of TNFi (± MTX) in reducing the percentage of naive B cells. Finally, another interesting aspect to consider in future studies would be to add a group with only MTX and evaluate if similar changes on naive B cells occur in patients who achieved clinical remission.
Our future research agenda, following this line of work, will include an in-depth study into this research field through evaluation of differences in the intracellular cytokine production that could help to better understand the changes in PBMC, according to the clinical response.
In conclusion, our study suggests that PBMC (principally the B-cell subsets) are modulated in patients with RA in clinical REM after 6 months of TNFi therapy. A significant decrease in naive B-cell percentage is associated with achieving REM, mainly in patients who received concomitant MTX. However, further research studies with other cohorts of patients need to be performed before implementing the results of this study.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics committees of Ramón y Cajal (PI-018/17) and La Paz University Hospitals (PI-2618), Madrid. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CP-R, LV, DP-S, and ER-M planned the study. BH-B, CG-H, IN-G, TJ, and PL-S collected the samples and performed flow cytometry experiments. BH-B wrote the manuscript draft. ER-M and LV supervised flow cytometry studies. BH-B, CP-R, VN-C, and MD-A performed and supervised statistical studies. CP-R, VN-C, CS, JB-C, GB, CP-M, MV-D, and AB visited RA patients and collected clinical data. ER-M and CP-R had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors were involved in revising the manuscript critically for important intellectual content, approved the final version to be published, and contributed to the manuscript and approved the submitted version.
Funding
This work was supported by Fondo para la Investigación Sanitaria, Instituto de Salud Carlos III (PI16/01092 and PI16/00474), Programa Estatal de Investigación Orientada a los Retos de la Sociedad, en el marco del Plan Estatal de Investigación Científica y Técnica y de Innovación 2013–2016, Ministerio de Economía y Competitividad, Spain, and FEDER Una manera de hacer Europa.
Conflict of Interest
CP-R has received research grants/honoraria from AbbVie, Lilly, Novartis, Pfizer, Sanofi, Biogen and UCB. VN-C reports speaker fees and grants from Abbvie, Janssen, Lilly, MSD, Novartis, Pfizer and UCB during the conduct of the study. AB reports grants, consultancies and speaker fees from Abbvie, BMS, Nordic, Novartis, Pfizer, Sandoz, Sanofi, Roche and UCB during the conduct of the study. DP-S reports speaker fees and grants from Abbvie, Grifols, Menarini, Novartis, Pfizer and Takeda during the conduct of the study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The results derived from this study were partially presented in the ACR Convergence 2020 conference (40). The authors thank the nurses from the Departments of Rheumatology and the laboratory technicians of the Immunology Units for their help and for contributing to a good working environment as well as Dr. Marta Galán for the linguistic assistance. We also acknowledge the Rheumatology Society in Madrid (SORCOM) for granting CP-R.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.683990/full#supplementary-material
References
1. Souto A, Maneiro JR, Gómez-Reino JJ. Rate of discontinuation and drug survival of biologic therapies in rheumatoid arthritis: a systematic review and meta-analysis of drug registries and health care databases. Rheumatology. (2016) 55:523–34. doi: 10.1093/rheumatology/kev374
2. Smolen JS, Landewé R, Bijlsma J, Burmester G, Chatzidionysiou K, Dougados M, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. (2017) 76:960–77. doi: 10.1136/annrheumdis-2016-210715
3. Xie X, Li F, Li S, Tian J, Chen JW, Du JF, et al. Application of omics in predicting anti-TNF efficacy in rheumatoid arthritis. Clin Rheumatol. (2018) 37:13–23. doi: 10.1007/s10067-017-3639-0
4. Malmström V, Catrina AI, Klareskog L. The immunopathogenesis of seropositive rheumatoid arthritis: from triggering to targeting. Nat Rev Immunol. (2017) 17:60–75. doi: 10.1038/nri.2016.124
5. Scrivo R, Di Franco M, Spadaro A, Valesini G. The immunology of rheumatoid arthritis. Ann N Y Acad Sci. (2007) 1108:312–22. doi: 10.1196/annals.1422.033
6. Chen SJ, Lin GJ, Chen JW, Wang KC, Tien CH, Hu CF, et al. Immunopathogenic mechanisms and novel immune-modulated therapies in rheumatoid arthritis. Int J Mol Sci. (2019) 20:1332. doi: 10.3390/ijms20061332
7. Nakayamada S, Kubo S, Yoshikawa M, Miyazaki Y, Yunoue N, Iwata S, et al. Differential effects of biological DMARDs on peripheral immune cell phenotypes in patients with rheumatoid arthritis. Rheumatology. (2018) 57:164–74. doi: 10.1093/rheumatology/kex012
8. Dulic S, Vásárhelyi Z, Sava F, Berta L, Szalay B, Toldi G, et al. T-Cell subsets in rheumatoid arthritis patients on long-term anti-TNF or IL-6 receptor blocker therapy. T-Cell Subsets in Rheumatoid Arthritis Patients on Long-Term Anti-TNF or IL-6 Receptor Blocker Therapy. Med Inflamm. (2017) 2017:6894374. doi: 10.1155/2017/6894374
9. Bankó Z, Pozsgay J, Gáti T, Rojkovich B, Ujfalussy I, Sármay G. Regulatory B cells in rheumatoid arthritis: alterations in patients receiving anti-TNF therapy. Clin Immunol. (2017) 184:63–9. doi: 10.1016/j.clim.2017.05.012
10. Daien CI, Gailhac S, Mura T, Combe B, Hahne M, Morel J. High levels of memory B cells are associated with response to a first tumor necrosis factor inhibitor in patients with rheumatoid arthritis in a longitudinal prospective study. Arthritis Res Ther. (2014) 16:R95. doi: 10.1186/ar4543
11. Anolik JH, Ravikumar R, Barnard J, Owen T, Almudevar A, Milner EC, et al. Cutting edge: anti-tumor necrosis factor therapy in rheumatoid arthritis inhibits memory B lymphocytes via effects on lymphoid germinal centers and follicular dendritic cell networks. J Immunol. (2008) 180:688–92. doi: 10.4049/jimmunol.180.2.688
12. Moura RA, Quaresma C, Vieira AR, Gonçalves MJ, Polido-Pereira J, Romão VC, et al. B-cell phenotype and IgD-CD27- memory B cells are affected by TNF-inhibitors and tocilizumab treatment in rheumatoid arthritis. PLoS ONE. (2017) 12:e0182927. doi: 10.1371/journal.pone.0182927
13. Rodríguez-Martín E, Nieto-Gañán I, Hernández-Breijo B, Sobrino C, García-Hoz C, Bachiller J, et al. Blood lymphocyte subsets for early identification of non-remission to TNF inhibitors in rheumatoid arthritis. Front Immunol. (2020) 11:1913. doi: 10.3389/fimmu.2020.01913
14. Sanmartí R, García-Rodríguez S, Álvaro-Gracia JM, Andreu JL, Balsa A, Cáliz R, et al. 2014 update of the Consensus Statement of the Spanish Society of Rheumatology on the use of biological therapies in rheumatoid arthritis. Reumatol Clin. (2015) 11:279–94. doi: 10.1016/j.reumae.2015.05.002
15. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 rheumatoid arthritis classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. (2010) 62:2569–81. doi: 10.1002/art.27584
16. Fransen J, Creemers MCW, Van Riel PLCM. Remission in rheumatoid arthritis: agreement of the disease activity score (DAS28) with the ARA preliminary remission criteria. Rheumatology. (2004) 43:1252–5. doi: 10.1093/rheumatology/keh297
17. Aletaha D, Ward MM, Machold KP, Nell VP, Stamm T, Smolen JS. Remission and active disease in rheumatoid arthritis: defining criteria for disease activity states. Arthritis Rheum. (2005) 52:2625–36. doi: 10.1002/art.21235
18. Böyum A. Isolation of leucocytes from human blood. Further observations. Methylcellulose, dextran, and ficoll as erythrocyte aggregating agents. Scand J Clin Lab Invest Suppl. (1968) 97:31–50.
19. Gravallese EM, Robinson WH. PRIME time in rheumatoid arthritis. N Engl J Med. (2020) 383:278–9. doi: 10.1056/NEJMe2018218
20. Orange DE, Yao V, Sawicka K, Fak J, Frank MO, Parveen S, et al. RNA identification of PRIME cells predicting rheumatoid arthritis flares. N Engl J Med. (2020) 383:218–28. doi: 10.1056/NEJMoa2004114
21. Rubin SJS, Bloom MS, Robinson WH. B cell checkpoints in autoimmune rheumatic diseases. Nat Rev Rheumatol. (2019) 15:303–15. doi: 10.1038/s41584-019-0211-0
22. Meffre E, Wardemann H. B-cell tolerance checkpoints in health and autoimmunity. Curr Opin Immunol. (2008) 20:632–8. doi: 10.1016/j.coi.2008.09.001
23. Moura RA, Graca L, Fonseca JE. To B or not to B the conductor of rheumatoid arthritis orchestra. Clin Rev Allergy Immunol. (2012) 43:281–91. doi: 10.1007/s12016-012-8318-y
24. Shlomchik MJ. Sites and stages of autoreactive B cell activation and regulation. Immunity. (2008) 28:18–28. doi: 10.1016/j.immuni.2007.12.004
25. Lu DR, McDavid AN, Kongpachith S, Lingampalli N, Glanville J, Ju CH, et al. T cell-dependent affinity maturation and innate immune pathways differentially drive autoreactive b cell responses in rheumatoid arthritis. Arthritis Rheumatol. (2018) 70:1732–44. doi: 10.1002/art.40578
26. Roosnek E, Lanzavecchia A. Efficient and selective presentation of antigen-antibody complexes by rheumatoid factor B cells. J Exp Med. (1991) 173:487–9. doi: 10.1084/jem.173.2.487
27. Panayi GS. B cells: a fundamental role in the pathogenesis of rheumatoid arthritis? Rheumatology. (2005) 44(Suppl. 2) ii3–7. doi: 10.1093/rheumatology/keh616
28. Aarvak T, Natvig JB. Cell-cell interactions in synovitis: antigen presenting cells and T cell interaction in rheumatoid arthritis. Arthritis Res. (2001) 3:13–7. doi: 10.1186/ar135
29. Leandro MJ. Anti-tumour necrosis factor therapy and B cells in rheumatoid arthritis. Arthritis Res Ther. (2009) 11:128. doi: 10.1186/ar2809
30. Degboé Y, Rauwel B, Baron M, Boyer JF, Ruyssen-Witrand A, Constantin A, et al. Polarization of rheumatoid macrophages by TNF targeting through an IL-10/STAT3 mechanism. Front Immunol. (2019) 10:3. doi: 10.3389/fimmu.2019.00003
31. Davignon JL, Rauwel B, Degboé Y, Constantin A, Boyer JF, Kruglov A, et al. Modulation of T-cell responses by anti-tumor necrosis factor treatments in rheumatoid arthritis: a review. Arthritis Res Ther. (2018) 20:229. doi: 10.1186/s13075-018-1725-6
32. Witte T. Methotrexate as combination partner of TNF inhibitors and tocilizumab. What is reasonable from an immunological viewpoint? Clin Rheumatol. (2015) 34:629–34. doi: 10.1007/s10067-015-2861-x
33. Srirangan S, Choy EH. The Role of Interleukin 6 in the Pathophysiology of Rheumatoid Arthritis. Ther Adv Musculoskelet Dis. (2015) 2:247–56. doi: 10.1177/1759720X10378372
34. Lotfi N, Thome R, Rezaei N, Zhang GX, Rezaei A, Rostami A, et al. Roles of GM-CSF in the pathogenesis of autoimmune diseases: an update. Front Immunol. (2019) 10:1265. doi: 10.3389/fimmu.2019.01265
35. Wicks IP, Roberts AW. Targeting GM-CSF in inflammatory diseases. Nat Rev Rheumatol. (2016) 12:37–48. doi: 10.1038/nrrheum.2015.161
36. Fortea-Gordo P, Villalba A, Nuño L, Santos-Bórnez MJ, Peiteado D, Monjo I, et al. Circulating CD19+CD24hiCD38hi regulatory B cells as biomarkers of response to methotrexate in early rheumatoid arthritis. Rheumatology. (2020) 59:3081–91. doi: 10.1093/rheumatology/keaa186
37. Benham H, Rutherford M, Kirby S, Stebbings S, White D, Sim D, et al. Treat-to-target in rheumatoid arthritis: evaluating the patient perspective using the patient opinion real-time anonymous liaison system: the RA T2T PORTAL study. Int J Rheum Dis. (2019) 22:874–9. doi: 10.1111/1756-185X.13514
38. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. (2018) 320:1360–72. doi: 10.1001/jama.2018.13103
39. Aletaha D, Funovits F, Keystone EC, Smolen JS. Disease activity early in the course of treatment predicts response to therapy after one year in rheumatoid arthritis patients. Arthritis Rheum. (2007) 56:3226–35. doi: 10.1002/art.22943
40. Hernandez-Breijo B, Plasencia C, Navarro-Compán V, Nieto-Gañán I, Sobrino C, Martínez-Feito A, et al. Reduction in peripheral CD19+ CD27− naïve B cells is associated with clinical remission in patients with rheumatoid arthritis receiving combined treatment with methotrexate and TNF inhibitors. Arthritis Rheumatol. (2020) 72(Suppl. 10):1–4231. doi: 10.1002/art.41538
Keywords: rheumatoid arthritis, autoimmunity, B cells, remission, TNF inhibitors
Citation: Hernández-Breijo B, Plasencia-Rodríguez C, Navarro-Compán V, García-Hoz C, Nieto-Gañán I, Sobrino C, Bachiller-Corral J, Díaz-Almirón M, Martínez-Feito A, Jurado T, Lapuente-Suanzes P, Bonilla G, Pijoán-Moratalla C, Roy G, Vázquez-Díaz M, Balsa A, Villar LM, Pascual-Salcedo D and Rodríguez-Martín E (2021) Remission Induced by TNF Inhibitors Plus Methotrexate is Associated With Changes in Peripheral Naïve B Cells in Patients With Rheumatoid Arthritis. Front. Med. 8:683990. doi: 10.3389/fmed.2021.683990
Received: 22 March 2021; Accepted: 24 May 2021;
Published: 17 June 2021.
Edited by:
Maria Leandro, University College London Hospitals NHS Foundation Trust, United KingdomReviewed by:
Rita A. Moura, University of Lisbon, PortugalMarcia Alwina Friedman, Oregon Health and Science University, United States
Copyright © 2021 Hernández-Breijo, Plasencia-Rodríguez, Navarro-Compán, García-Hoz, Nieto-Gañán, Sobrino, Bachiller-Corral, Díaz-Almirón, Martínez-Feito, Jurado, Lapuente-Suanzes, Bonilla, Pijoán-Moratalla, Roy, Vázquez-Díaz, Balsa, Villar, Pascual-Salcedo and Rodríguez-Martín. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Borja Hernández-Breijo, Ym9yamEuaGVybmFuZGV6QGlkaXBhei5lcw==
†These authors have contributed equally to this work
‡These authors share senior authorship