 Eric Denes
Eric Denes Fabrice Fiorenza2
Fabrice Fiorenza2- 1Infectious Diseases Department, ELSAN Polyclinique de Limoges, Limoges, France
- 2Orthopaedic Surgery Department, Limoges Teaching Hospital, Limoges, France
- 3Bacteriology Laboratory, Limoges Teaching Hospital, Limoges, France
Background: Immunity against Pasteurella spp. is not well-known for humans.
Methods: We've tested T CD8+ lymphocytes in a patient with a chronic prosthetic joint infection due to Pasteurella spp. to search for a deficit which could have favored her infection. As this deficit was found, we've searched for such a deficit in other patients with Pasteurella spp. Infections, either acute or subacute.
Results: Eight patients were tested and all had a persistent T CD8+ lymphocytes deficit. This is striking as these cells are involved in the response to this type of infection in animal models.
Conclusion: The authors suggest that a deficit in CD8+ T lymphocytes can be one of the causes for the onset of infections with P. multocida.
Introduction
Pasteurella spp. is widely found in animal's mouths and is transmitted to humans by bites (1). One of the main diseases caused by this bacterium is hand tendon sheath infections. Clinical symptoms are usually acute in the first 24 h (2). Orthopedic prosthesis infections due to this bacterium are scarce and <35 cases have been reported in the literature (3).
Case Report
We took in charge a 77-year-old patient with a total hip prosthetic infection due to P. multocida. Interestingly, a cat bite occurred 1 year prior to diagnosis and the patient had been complaining of pain in her left hip after the bite. Infection was treated using a two-stage surgery associated with a 6 weeks course of antibiotics (ceftriaxone and ciprofloxacin). With this management, after a follow-up of 2 years, we've conclude to a cure of this infection. This unusual chronic presentation led us to look for a possible unknown immune deficit. As we previously described a case of chronic wound skin infection due to Rhodococcus equi facilitated by a CD8+ T lymphocytes deficit (4), we looked for the same kind of deficit for this patient. Analyses revealed a CD8+ T lymphocytes deficit for both the percentage (15.5% - normal range: 31–40%) and the absolute value (205/mm3 – normal range: 500–900/mm3). As a CD8+ T lymphocyte deficit can be the consequence of infections, a control was performed 4 months later, when the clinical evolution was favorable and antibiotics had been stopped for 2.5 months. The deficit was still noticeable (absolute value: 220/mm3 and percentage: 17%). We then wondered if this deficit could play a role in the occurrence of this usually acute infection. Therefore, in a preliminary study, we performed T CD8+ lymphocytes analysis for other patients with acute Pasteurella spp. infection (all patients gave their consent for this analysis). First, we randomly picked up two patients who previously presented an acute hand tendon sheath infection among patients who presented this type of infection during the past 4 years. In addition, during the same period of time, several patients were hospitalized and presented acute and sub-acute infections due to animal bites. The characteristics of these consecutive patients are summarized in Table 1. Two of them (patients 7 & 8) with negative bacteriology samples, were treated with antibiotics (amoxicillin—clavulanate acid) prior to surgery, but clinical presentation was compatible with Pasteurella spp. infection with an acute onset in the first few hours after the bite. All patients with Pasteurella spp. infections had a CD8+ T lymphocytes deficit in percentage and 6 out of 8 had a deficit in absolute value. None of them presented a deficit in total lymphocytes count. The other biological parameters such as white blood cells, liver and renal function, inflammatory parameters were normal at the time of evaluation. None of them had a history of unusual infections.
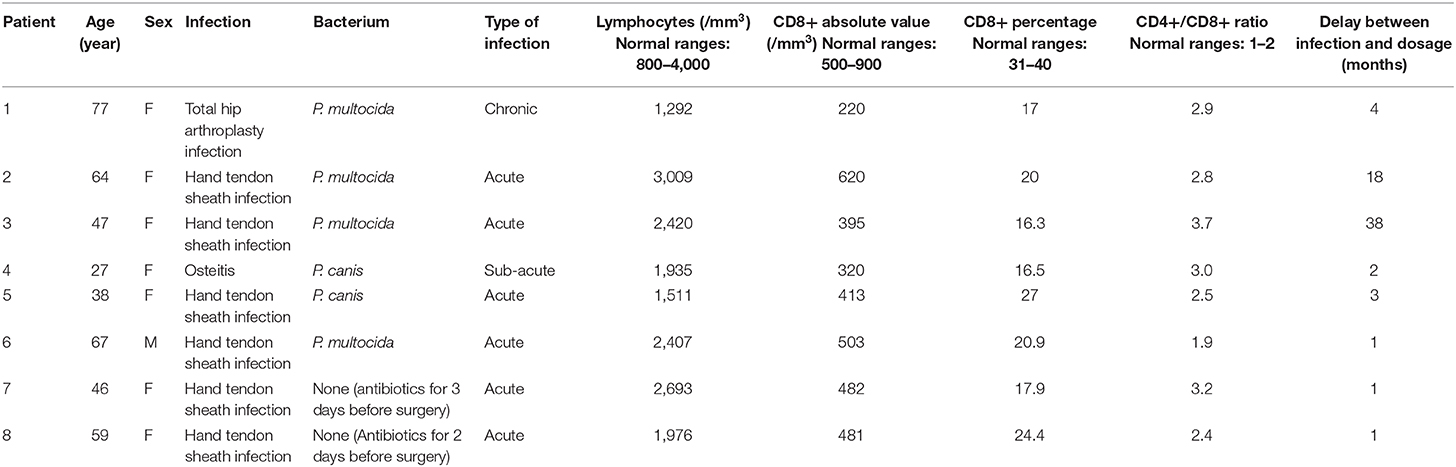
Table 1. Summary of patient's characteristics.
Discussion
Although pathogenicity of P. multocida relies on several virulence factors among which its capsule, adhesins or toxins (5), immunity against Pasteurella spp. is not well-known in humans (2, 6). Antibody secretion was demonstrated against capsular and somatic antigens, however its real impact is not well-established (7). In veterinary medicine an increase of CD8+ T lymphocytes after a challenge with P. multocida has been demonstrated (8–10). These studies were performed with lung infection models in three different types of animals: swine (8), calves (9) and pigs (10). These studies indicate that at least concerning animals, the inflammatory response is mediated via lymphocytes activation and particularly CD8 + T cells.
P. multocida is the most commonly isolated pathogen after dogs or cats' bites; however it is unusual to develop an infection. Nevertheless, it is difficult to assess whether people are not infected because of their immune system (efficient CD8+ T lymphocytes for example) or because of local treatment, antibiotics or the absence of such bacteria in animals' mouth.
However, it is striking to note that 8 patients with an unusual infection (prosthetic infection), randomly chosen or consecutively treated for classical infection presentation present the same type of immune deficit. The analogy with animal models seems difficult to establish but it appears logical to think that partially missing or inefficient cells involved in immune response to an aggression by Pasteurella spp. will favor infection. As in animal models, an increased CD8+ T lymphocytes count should be observed in humans, in reaction to bacterium. However, it is only possible if these cells are sufficient in number and with the possibility to react. Unfortunately, we were not able to challenge CD8+ T cells of patients with their bacterial strain, to observe an activation of these latter.
In conclusion, we are aware that this study does not demonstrate the link between T CD8+ lymphocytes deficit and the occurrence of infection with Pasteurella spp., but our observations question the nature of immunity against Pasteurella spp. and the likely role of CD8+ T cell lymphocytes. Yet, other studies will be necessary to understand whether only people with a deficit can develop such an infection and to study the exact role of CD8+ T lymphocytes. However, such a study is difficult as many factors are involved such as antibiotic use before cares and bacteriological samples, the presence/absence of the bacteria in animals' mouth and its transmission.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Author Contributions
ED: proposed the CD8+ T lymphocyte dosage, analyse patient's files, drafted the manuscript, and approved the final version. FF and MA: did the surgery and approved the final version. CM: performed bacterial culture, retrieved patient with previous Pasteurella spp. infection, and approved the final version. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Talan DA, Citron DM, Abrahamian FM, Moran GJ, Goldstein EJ. Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med. (1999) 340:85–92. doi: 10.1056/NEJM199901143400202
2. Zurlo J. Pasteurella species. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Elsevier (2005). 2687–91.
3. Ding DY, Orengo A, Alaia MJ, Zuckerman JD. Pasteurella multocida infection in a primary shoulder arthroplasty after cat scratch: case report and review of literature. J Shoulder Elb Surg. (2015) 24:e159–63. doi: 10.1016/j.jse.2015.03.005
4. Denes E, Peignon-Orsoni D, Terrade F-X. Nonhealing wound due to Rhodococcus equi in an apparently immunocompetent patient, revealing CD8+ T-lymphocyte deficiency. J Clin Microbiol. (2010) 48:4658–60. doi: 10.1128/JCM.01469-10
5. Harper M, Boyce JD, Adler B. Pasteurella multocida pathogenesis: 125 years after Pasteur. FEMS Microbiol Lett. (2006) 265:1–10. doi: 10.1111/j.1574-6968.2006.00442.x
6. Kubatzky KF. Pasteurella multocida and immune cells. Curr Top Microbiol Immunol. (2012) 361:53–72. doi: 10.1007/82_2012_204
7. Choudat D, Paul G, Legoff C, Choudat L, Philippon A, Perreau P, et al. Specific antibody response to Pasteurella multocida. Scand J Infect Dis. (1987) 19:453–7. doi: 10.3109/00365548709021678
8. Berndt A, Muller G. Occurrence of T lymphocytes in perivascular regions of the lung after intratracheal infection of swine with Pasteurella multocida. Vet Immunol Immunopathol. (1995) 49:143–59. doi: 10.1016/0165-2427(95)05457-H
9. Mathy NL, Mathy JPD, Lee RP, Walker J, Lofthouse S, Meeusen ENT. Pathological and immunological changes after challenge infection with Pasteurella multocida in naive and immunized calves. Vet Immunol Immunopathol. (2002) 85:179–88. doi: 10.1016/S0165-2427(01)00427-5
Keywords: Pasteurela multocida, CD8 lymphocytes +, deficit, infection - immunology, dog bite, cat bite
Citation: Denes E, Fiorenza F, Armendariz M and Martin C (2021) Case Report: CD8+ T-Lymphocyte Deficit: A Prerequisite for Pasteurella spp. Infection? Front. Med. 8:668976. doi: 10.3389/fmed.2021.668976
Received: 17 February 2021; Accepted: 30 March 2021;
Published: 27 April 2021.
Edited by:
Claudio Fenizia, University of Milan, ItalyReviewed by:
Zhong Peng, Huazhong Agricultural University, ChinaNengzhang Li, Southwest University, China
Lawan Adamu, University of Maiduguri, Nigeria
Copyright © 2021 Denes, Fiorenza, Armendariz and Martin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eric Denes, ZGVuZXMuZXJpY0BnbWFpbC5jb20=; orcid.org/0000-0001-5321-3171