
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 03 November 2021
Sec. Family Medicine and Primary Care
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.665023
This article is part of the Research Topic The Biology and Management of Chronic Diseases in Mexican Americans View all 7 articles
 Esperanza M. Garcia-Oropesa1†
Esperanza M. Garcia-Oropesa1† Yoscelina E. Martinez-Lopez2†
Yoscelina E. Martinez-Lopez2† Sonia María Ruiz-Cejudo3,4
Sonia María Ruiz-Cejudo3,4 José Darío Martínez-Ezquerro3,5
José Darío Martínez-Ezquerro3,5 Alvaro Diaz-Badillo6,7
Alvaro Diaz-Badillo6,7 Carlos Ramirez-Pfeiffer7Alejandra Bustamante-Fuentes8Elena B. Lopez-Sosa9Oscar O. Moctezuma-Chavez10
Carlos Ramirez-Pfeiffer7Alejandra Bustamante-Fuentes8Elena B. Lopez-Sosa9Oscar O. Moctezuma-Chavez10 Edna J. Nava-Gonzalez11Adriana L. Perales-Torres12Lucia M. Perez-Navarro13Marisol Rosas-Diaz1Kathleen Carter14Beatriz Tapia15
Edna J. Nava-Gonzalez11Adriana L. Perales-Torres12Lucia M. Perez-Navarro13Marisol Rosas-Diaz1Kathleen Carter14Beatriz Tapia15 Juan C. Lopez-Alvarenga6,7*
Juan C. Lopez-Alvarenga6,7*Mexicans and Mexican Americans share culture, genetic background, and predisposition for chronic complications associated with obesity and diabetes making imperative efficacious treatments and prevention. Obesity has been treated for centuries focused-on weight loss while other treatments on associated conditions like gout, diabetes (T2D), and hypertriglyceridemia. To date, there is no systematic review that synthesizes the origin of obesity clinics in Mexico and the efforts to investigate treatments for obesity tested by randomized clinical trials (RCT). We conducted systematic searches in Pubmed, Scopus, and Web of Science to retrieve anti-obesity RCT through 2019 and without an inferior temporal limit. The systematic review included RCT of anti-obesity treatments in the Mexican adult population, covering alternative medicine, pharmacological, nutritional, behavioral, and surgical interventions reporting metabolism-associated traits such as BMI, weight, waist circumference, triglycerides, glucose, among others. Only the studies with at least 3 months of treatment were included in the meta-analyses in order to reduce placebo effects. We found 634 entries, after removal of duplicates and screening the studies based on eligibility criteria, we analyzed 43 national, and 2 multinational-collaborative studies. Most of the national studies had small sample sizes, and the implemented strategies do not have replications in the population. The nutrition/behavioral interventions were difficult to blind, and most studies have medium-to-high risk of bias. Nutritional/behavioral interventions and medications showed effects on BMI, waist circumference, and blood pressure. Simple measures like pure water instead of sweet beverages decrease triglycerides and systolic blood pressure. Dark chocolate showed the highest effect for BMI and high blood pressure, and treatment with insulin increased weight in those with T2D. The study of obesity in Mexico has been on-going for more than four decades, the interest on RCT just increased until this millennium, but with small sample sizes and lack of replication. The interventions affect different cardiometabolic associated traits, which should be analyzed in detail in the population living near the Mexico-U.S. border; therefore, bi-national collaboration is desirable to disentangle the cultural effects on this population's treatment response.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020221436, identifier: CRD42020221436.
The history of obesity as a clinical entity started with the Obesity Clinic established in 1959 at the Instituto Nacional de Nutrición Salvador Zubirán, by Dr. Luis Domenge, Dr. Carmen Ramos, and Dr. Jorge Gonzalez-Barranco. They, as expert physicians, considered obesity as an aesthetic but also a medical problem. The so-called epidemiologic transition, from infectious to chronic degenerative diseases, moved slowly from the 70s and 80s derived from an evolution of treating obesity as a medical problem, promoted by Dr. Gonzalez-Barranco based on scientific research and clinical trials with medications in the 90s.
The first attempt to classify obesity was using the Metropolitan Life Insurance Company (MLIC) which developed standard tables for “ideal” (MLIC 1942) and then “desirable” weight (MLIC 1959) based on the observed association of body weight with mortality. These standard tables were the platform for developing the current definition for underweight, normal, overweight, and obese individuals based on the body mass index (BMI) cut-offs (1).
The use of BMI as a reliable measurement started with the NHANES from 1988 to 2016. These studies demonstrated the age-adjusted prevalence of obesity in the United States increased progressively: from 22.9 to 39.6 percent. The main issue of concern in regard to BMI involves the growing obesity epidemic and the increasing population with high BMI numbers (2).
Since 1993 a series of population surveys have been conducted systematically in Mexico using the BMI. The first National Survey on Chronic Diseases (ENEC from Spanish: Encuesta Nacional de Enfermedades Crónicas) highlighted obesity as a national public health problem. The prevalence of obesity in Mexico has increased substantially since the 1980s, and currently affects over 30% of the adult population (3). The epidemiological transition from undernourishment and infectious diseases to emergent chronic diseases were well-documented in the ENEC. A sequel of undernourishment in presence of an obesogenic environment is homeorrhexis as an adaptive response to undernourishment. Homeorrexis or homeorhesis comes from the Greek homós, “equal;” and rhéxis, “violent rupture,” and refers to regulatory mechanisms that allow the body to change from one homeostatic, stable condition to another in a programmed fashion, e.g., growth during childhood or the onset of lactation (4). A combination of genetic and socioeconomic strata were conditions affecting stature. From North to South Mexico the ENEC data show a decrease in stature by expenses of the lower body segment (Figure 1), the sitting height is almost similar across regions. The stature can modify body composition despite BMI (5) and can be an indicator of socioeconomic inequality (6).
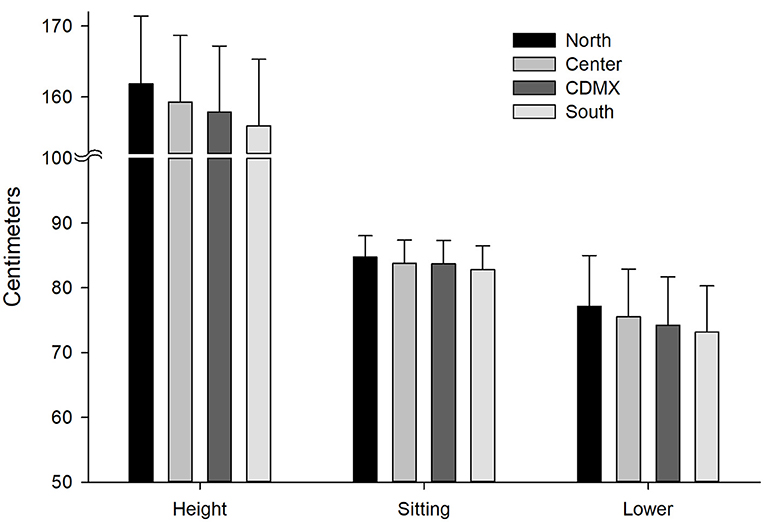
Figure 1. Height measurement standing up, sitting, and the lower body segment. From North to South, height is lower at the expenses of the lower body segment (p < 0.0001, adjusted by Bonferroni for all regions). Sitting height reflects the upper body segment and shows small differences between regions. Means and standard deviations. Data obtained from the ENEC 1993. CDMX, Mexico City; Sitting, sitting height; Lower, Lower segment of the body (Height-sitting height).
The First Obesity meeting in Mexico with the NAASO and the Pan-American Endocrine Meetings were held in Cancun in 1997. These meetings were a landmark achievement for the study of obesity in Mexico with the first NOM (Mexican Official Norm) for obesity management, published in 1998 (7). Since this new millennium, there has been a spread of interest in obesity in other hospitals and Mexican states. Close collaboration with the Diabetes Division at the University of Texas San Antonio Health Science Center (UTSAHSC) and the South Texas Diabetes and Obesity Institute (STDOI) at the UTRGV has been done since then.
In the United States, Mexican Americans are considered part of the Hispanic Americans or Latino group. The U.S.-Mexico border represents this minority with active immigration, and a rapid increase in population. One of the Healthy People 2020 goals was to improve the health of all groups, requiring an understanding of the Hispanic culture, and health care needs for health promotion (8).
Mexican Americans are spread all over the United States, the National Health and Nutrition Examination Surveys 1988–1994 showed children aged 4 to 17 years who were born abroad had significantly lower prevalence of overweight / obesity compared to Mexican American children born in the U.S. (PR = 0.77, 95% CI: 0.61, 0.96). In contrast, during 2005–2014, there was no evidence of a difference in overweight / obesity at birth (PR = 0.95; 95% CI: 0.84, 1.07) and no differences with newer immigrants (<5 years living in the U.S.) compared with those born in the U.S. (9).
Regarding the diet quality, Yoshida et al. (10) reported age differences in diet quality influenced by acculturation (customary adoption of a new culture): older Mexican Americans had higher scores in Healthy Eating Index (HEI) indicating a better diet quality. For vegetables, fruits, and proteins, middle-aged adults had higher scores compared to young adults. Concerning HEI components, a 1-unit increase of acculturation was associated with 10 to 20% lower odds of attaining better scores for vegetables, fruits, dairy, sodium, and empty calories in almost all ages.
Some pharmacokinetics determinants of many drugs depend on the body size; for instance, obesity modifies the volume of distribution, and drug clearance, probably due to increased activity of cytochrome P450 2E1 and possible modifications on tubular reabsorption (11).
However, not only biology can explain the variability of losing weight, other factors are associated with the feasibility of following medical recommendations affected by cultural environment. The importance of lifestyle was defined in early times of weight loss intervention but was debated by the use of medication.
Numerous international published guidelines for anti-obesity treatment consider the local disparities and cultural differences of each geographic region. The management of obesity relies on diverse medical specialists, health professionals and government decisions. Primary prevention of obesity is fundamental and requires policies for favoring spaces for physical activity and a healthy environment. Harmonization on treatment cannot be global but can help to tailor weight loss treatments, and metabolic improvement for prevention of complications (12, 13).
Since 2000 guidelines from the former North American Association for Study of Obesity (nowadays The Obesity Society—TOS) and the NIH Working Group were mainly based on dietary therapy, physical activity, and behavioral therapy, and guided on the appropriate use of pharmacological and surgical interventions. The weight loss recommendation was for patients with BMI >30 and those with BMI between 25 and ≤ 30 with two or more complications. They suggested that pharmacotherapy should be used only in the context of a treatment program with diet, physical activity, and behavioral therapy. Once the guide was published, only two drugs were approved for weight loss: sibutramine and orlistat (12).
The European guidelines also made emphasis on lifestyle modifications including nutrition and physical activity. The goals are risk reduction (even with modest weight loss i.e., 5–10% of initial body weight), attention on waist circumference and management of complications. They increase the number of drug treatments for obesity approved by FDA (Food and Drug Administration) and EMA (European Medicines Agency): orlistat, lorcaserin (only for FDA), phentermine/topiramate (only for FDA), bupropion/naltrexone and liraglutide. They recommend drug discontinuation if the patient does not reach 5% loss of initial weight after 12 weeks of treatment. This guide discusses metabolic surgery focusing on metabolic effects as primary outcomes instead being limited to weight loss (13).
The Endocrine Society in 2015 published the guideline for pharmacological management of obesity (14) implementing diet, exercise, and behavioral modification and suggesting drugs may amplify adherence to behavior change, especially for patients with a clinical history of failure in non-medication treatments.
The nutritional health status in Mexico was affected by government policies, the first supermarket chains selling American processed food in Mexico started in the 1940s. The government eliminated the subsidy of corn tortillas in 1999 with the objective to improve competitiveness in the global economy. This action loaded in the closure of local tortilla factories not able to compete. The transition epidemiology from infectious to chronic diseases was rampant in this period. In 2008 the import tariffs on maize, bean, sugar, and mill were eliminated. In response to the nutritional problems and increase in obesity, in 2010 the Ministries of Public Education and of Health published the General Guidelines for Dispensing or Distribution of Foods and Beverages at School Food Establishments (SFEs). After a mass media campaign to reduce consumption of high caloric food, the Mexican congress, in 2014, excised a tax on high energy dense food (15).
The aim of our study was to perform a systematic review with meta-analyses to synthesize and evaluate the evidence of anti-obesity interventions on BMI and other cardiometabolic associated traits performed in Mexican adults with overweight and obesity. These treatments include pharmaceutical, behavioral, surgical, nutritional, and alternative interventions designed as controlled clinical trials, to compare results within and between interventions.
The protocol was registered in PROSPERO on 11/17/2020 and assigned the registry number CRD42020221436 (16).
The PICO Structure is as follows:
Participants/population: Mexican adults classified as overweight or obese by WHO criteria included in controlled clinical trials for anti-obesity interventions and randomly allocated to treatment groups.
Interventions: Approaches conducted in the Mexican population to treat obesity, including alternative medicine, pharmacological, nutritional, behavioral, and surgical interventions reporting BMI as.
Comparisons: Within and between studies comparison of anti-obesity interventions on BMI, in addition to cardiometabolic associated traits, in which control groups were placebo or active treatments. Studies with at least 3 months of treatment were included in the meta-analyses in order to reduce the placebo effect.
Outcomes: Biometric markers associated with obesity such as BMI, waist circumference, triglycerides, glucose, HDL-C, diastolic, and systolic pressure.
The search strategies included Pubmed, Scopus, and Web of Science databases to obtain published literature up to 2019 to include randomized controlled clinical trials for obesity conducted in Mexico. To identify additional studies and gray literature, we contacted Medical Societies such as the Endocrinology Society from Mexico and researchers from academic institutions such as UNAM. For inclusion in the meta-analysis, all interventions had to be conducted for at least 3 months—as a strategy to control for placebo effects—and report both baseline and final BMI. The query was focused on all interventions with overweight or obese participants who underwent weight loss treatment. We included nutritional/behavioral treatments, with knowledge that many of these interventions cannot be blinded, therefore we assessed the possibility of bias using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (17). Medications, alternative medicine and surgical interventions were included in the review finished in December 2020.
An example of a search strategy performed in Pubmed without time period limits:
[(“obesity”[MeSH Terms] OR “obesity”[All Fields]) AND (“therapy”[Subheading] OR “therapy”[All Fields] OR “treatment”[All Fields] OR “therapeutics”[MeSH Terms] OR “therapeutics”[All Fields])] AND (“mexico”[MeSH Terms] OR “mexico”[All Fields]) AND Clinical Trial[ptyp].
The systematic review included Mexican adult overweight or obese participants in controlled clinical trials subjected to pharmaceutical, behavioral, surgical, nutritional, or alternative interventions. Weight loss was the primary or secondary outcome, besides, we included cardiometabolic traits outcomes when available. We included studies published in English or Spanish at any time, conducted in Mexican centers and multicentric international studies with Mexican participants. For inclusion in the meta-analysis, treatments had to be conducted for at least 3 months and indicate baseline and final BMI. When available, we analyzed obesity-related cardiometabolic components (i.e., serum concentration of glucose, HDL-C, triglycerides, systolic and diastolic blood pressure, and waist circumference). We followed these criteria for the articles' peer-screening and conducted a third final group review to resolve disagreements applying an online Delphi method due to confinement in times of COVID-19 (18). We contacted the corresponding authors to clarify doubts and obtain additional information when necessary.
We recovered 634 studies from three databases: Pubmed (n = 180), Scopus (n = 238), and Web of Science (n = 216). After eliminating duplicate studies and applying the eligibility criteria, 589 studies were eliminated. The flux of the analyzed studies is described in Figure 2. Of the 45 included studies data were extracted using the Cochrane tool and quality assessed with the Jadad scale. There were 45 studies included in the qualitative synthesis and 25 in the meta-analysis. There were 55 interventions in the studies included for the qualitative synthesis: 25 with medications, 27 with nutrition and exercise, and 3 with surgical treatment (Table 1).
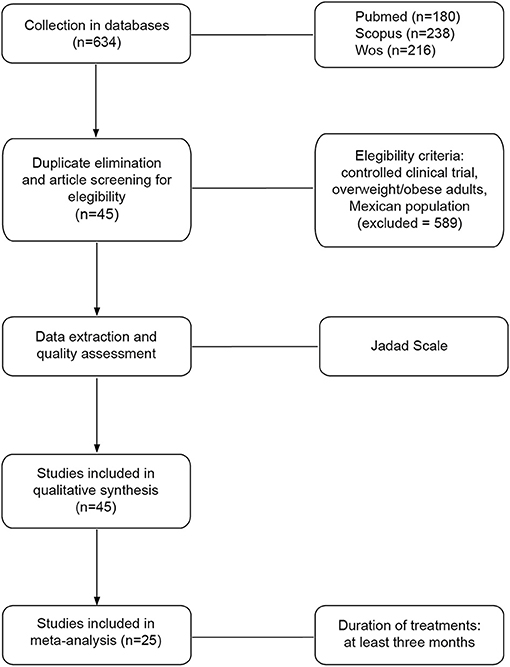
Figure 2. Study framework for systematic review with meta-analyses. The flowchart shows the processes of collection, screening, quality assessment, data extraction, and analysis.
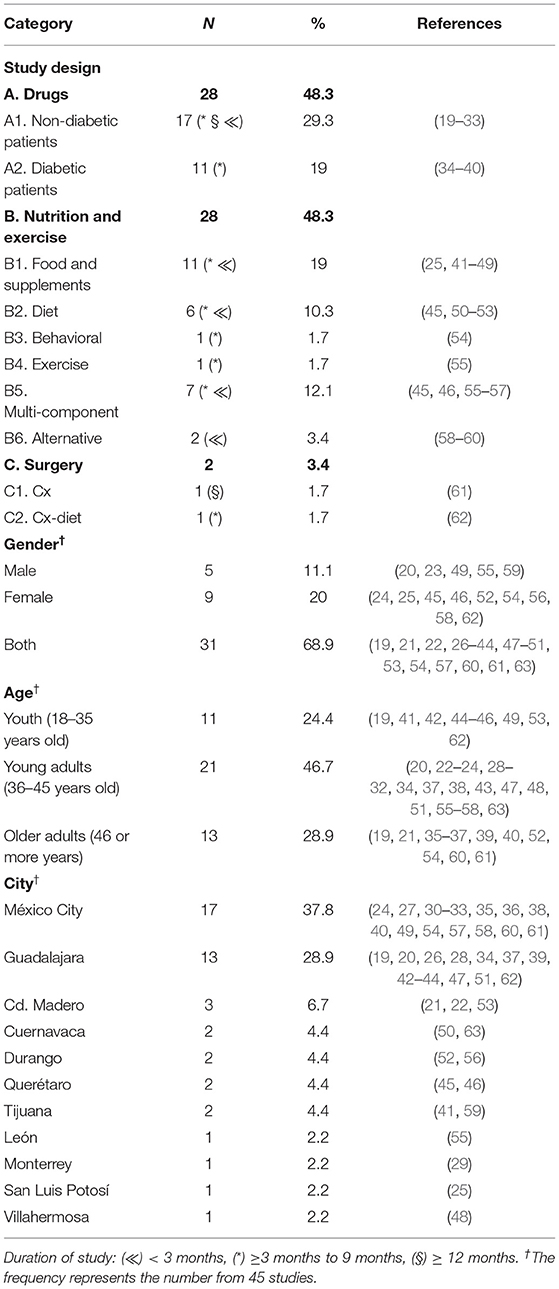
Table 1. Characteristics of the analyzed interventions (n = 58).
The data extraction from the studies was done, by a team of 13 researchers, with a modified Cochrane tool for data collection form to obtain detailed information: type of intervention (nutritional programs, behavioral treatments, use of drugs, surgical interventions or alternative medicine), age of intervention (childhood, adult), duration of treatments, year of the study development, sample size, groups of intervention and control, blindness of the treatment and the size of effects obtained in each study (Cohen's d). Data extraction was performed in duplicate, and cases of discrepancy were re-analyzed in groups of 4 investigators. When necessary, the authors were contacted to collect additional information. The main outcome was related to the reduction of BMI, waist circumference or percentage of body fat and biochemical parameters associated with metabolism such as glucose, total cholesterol, triglycerides, HDL-c, blood pressure, HOMA-IR and Matsuda. We used meta-regression to analyze the source of heterogeneity with mean age, mean BMI, location of the study (represented as latitude of the city of recruitment), sex distribution, and duration of the study. Adverse effects were also analyzed.
The quality assessment of the studies was done using the Jadad scale (64) and the risk of bias was assessed with GRADE checklist (17) with the following assessment guidelines:
Low risk studies were treated with unpredictable allocation: A central office for allocation by phone, web, and pharmacy. Use of sequentially numbered, sealed, opaque envelopes. The drug containers are sequentially numbered and identical. Meanwhile high risk is predictable allocation, like staff know the random sequence in advance. Another high risk of bias was the use of envelopes or packaging without safeguards or non-random, predictable sequence. The attrition bias can be considered if there was a poor description on how much data was missing from each group, or the lack of reasons for missing data and how they were considered in the analysis. We were also interested in whether researchers used intention to treat analysis, imputation of missing values, or just per protocol analysis.
Both the scanning and selection of the studies, as well as the data extraction with the Cochrane tool and the quality assessment using the Jadad scale were procedures performed in a paired manner by the investigators to avoid bias, and each step was discussed prior to the next using an online Delphi method due to COVID-19 confinement.
Sample size, means, and standard deviation were retrieved from the data of the included studies. The summary of contrasts between treatments was computed with Cohen's-d differences. All models were analyzed with Restricted maximum likelihood (REML) random effects models, and the pooled effects were described with 95% confidence intervals (95% CI). Heterogeneity was assessed with I2 statistics, and we use meta-regression to analyze the heterogeneity. The Egger test was performed on the slopes in the weighted regression of the effect size. These statistical analyses were conducted with Stata 16.0 (StataCorp, College Station TX).
The network meta-analysis was computed for studies with medication only, because the designs of nutrition/behavior studies did not allow us to construct networks. This analysis was performed with Stata 16.0 and CINeMA to define the network geometry, and effects comparisons. We did not have enough samples of studies to perform a rankogram.
We collected 634 studies from databases and after duplicate removal identified 64 controlled clinical trials conducted in Mexico from PubMed, 27 from Scopus, and 15 from Web of Science.
For the systematic review, we included 45 anti-obesity national and multinational collaborative controlled clinical trials involving overweight and obese Mexican adults (>18 years) subjected to distinct weight-loss interventions: pharmaceutical (25 studies), nutrition and behavioral (15 studies), surgical (2 studies), and alternative (3 studies) interventions (Table 1). A total of 15 interventions were composed exclusively by women, 5 by men, and 35 by both sexes.
With regard to participant cities, Mexico City had the highest frequency of studies (38%, n = 17), followed by Guadalajara (29%, n = 13). There were 11 out of 32 states in the included studies, three of which are on the Mexico-U.S. border: Nuevo Leon, Tamaulipas, and Baja California. The details are described in Table 1.
We performed a quality assessment at the intervention level. The Jadad mean value for nutritional/behavioral interventions was 3.6 (min 3, max 5), and for drug treatments was 3.7 (min 2, max 5). The nutrition/behavioral interventions had medium risk of bias (by GRADE) in 95% (n = 18/19) and high risk of bias in 5% (n = 1/19). Physical activity was difficult to blind. The use of medication as intervention had very low risk of bias in 32% (n = 7/22), medium 55% (n = 12/22) and high risk in 14% (n = 3/22). No differences in bias were found for interventions that included participants with T2D (Fisher's exact test = 0.286).
This systematic review and meta-analysis included data from 2,074 participants in nutrition/behavioral interventions and 5,086 participants with medication. Excluding multicentric international studies, there were 1,525 participants from studies conducted exclusively in Mexico. The main outcomes from individual studies are described in Tables 2–4. Forest plots with the pooled analysis are in Figures 3–10.
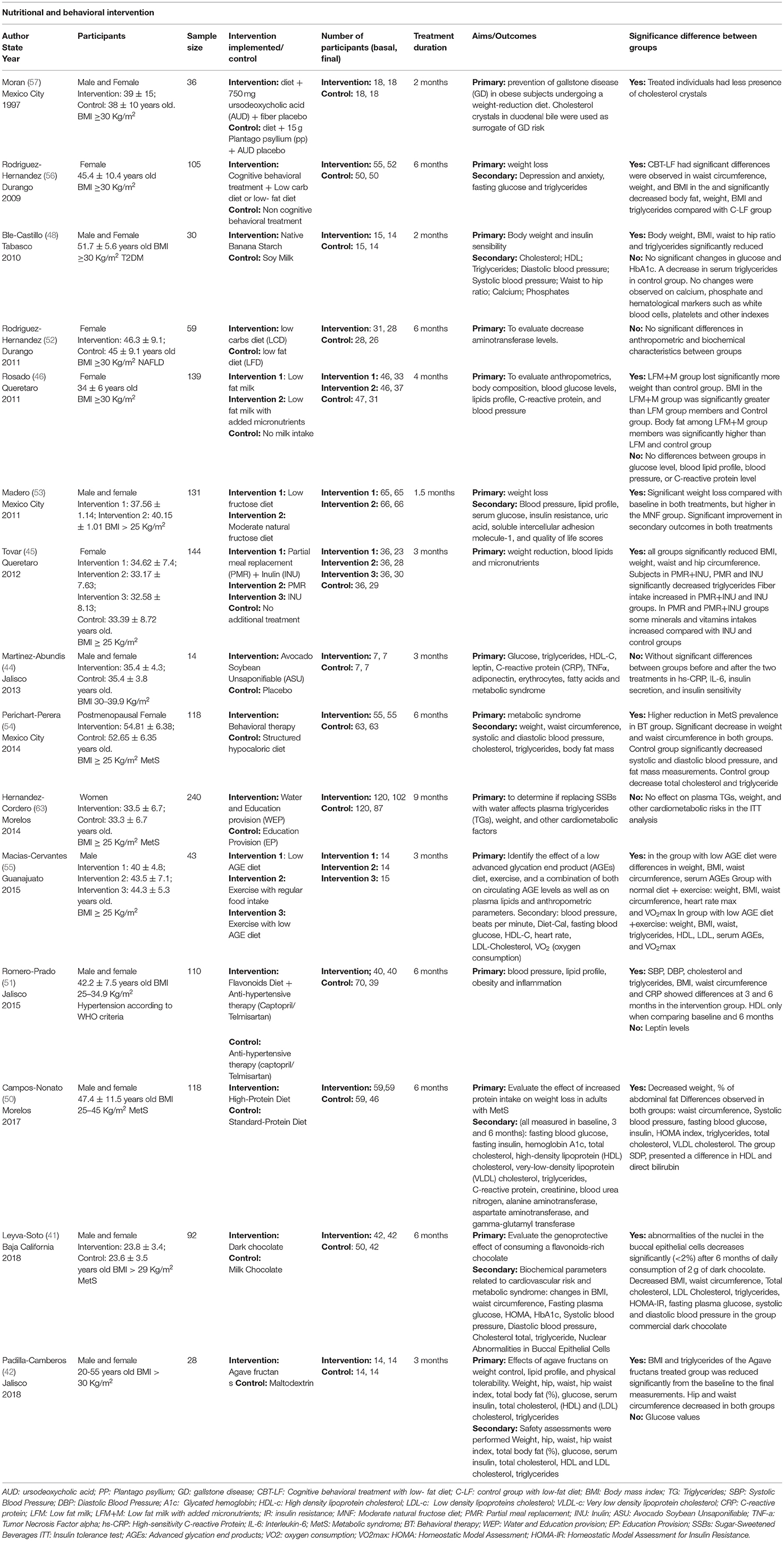
Table 2. Descriptive characteristics and assessment of nutrition/behavioral interventions.
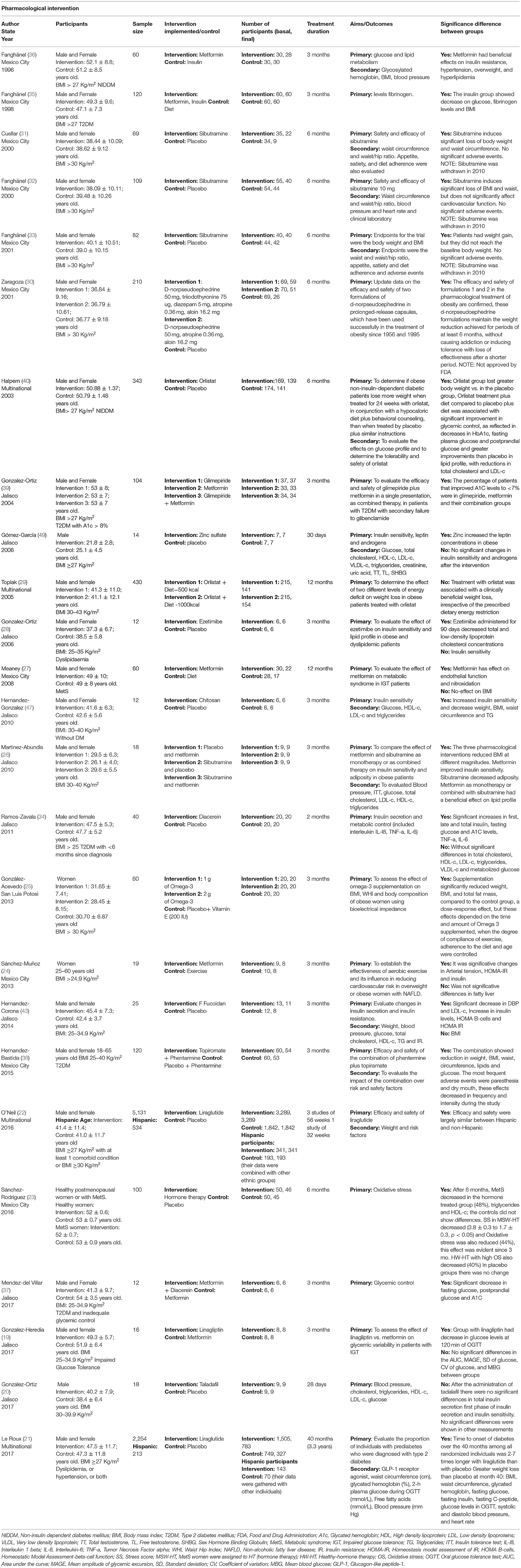
Table 3. Descriptive characteristics and assessment of medications.
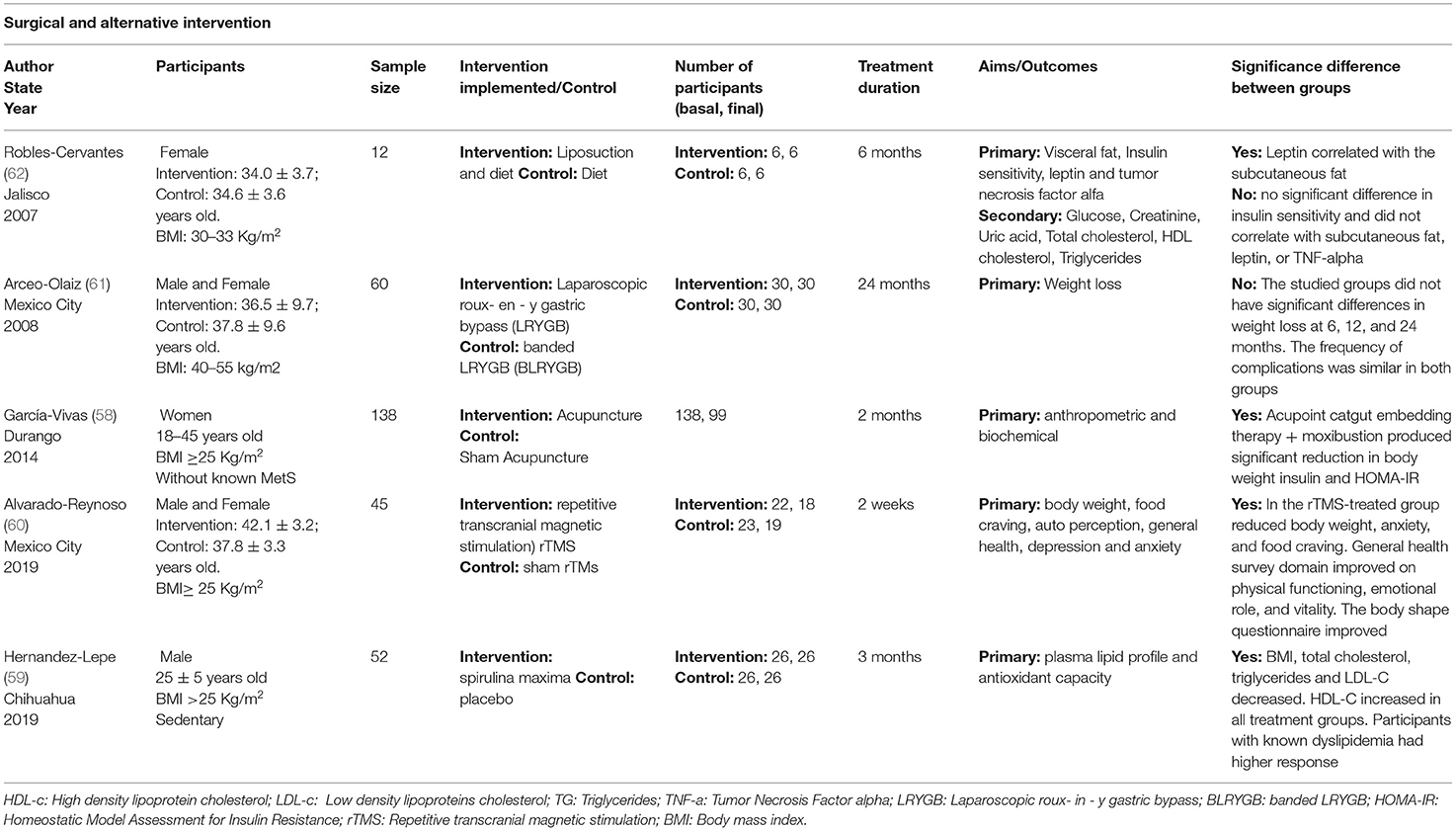
Table 4. Descriptive characteristics and assessment of medications.
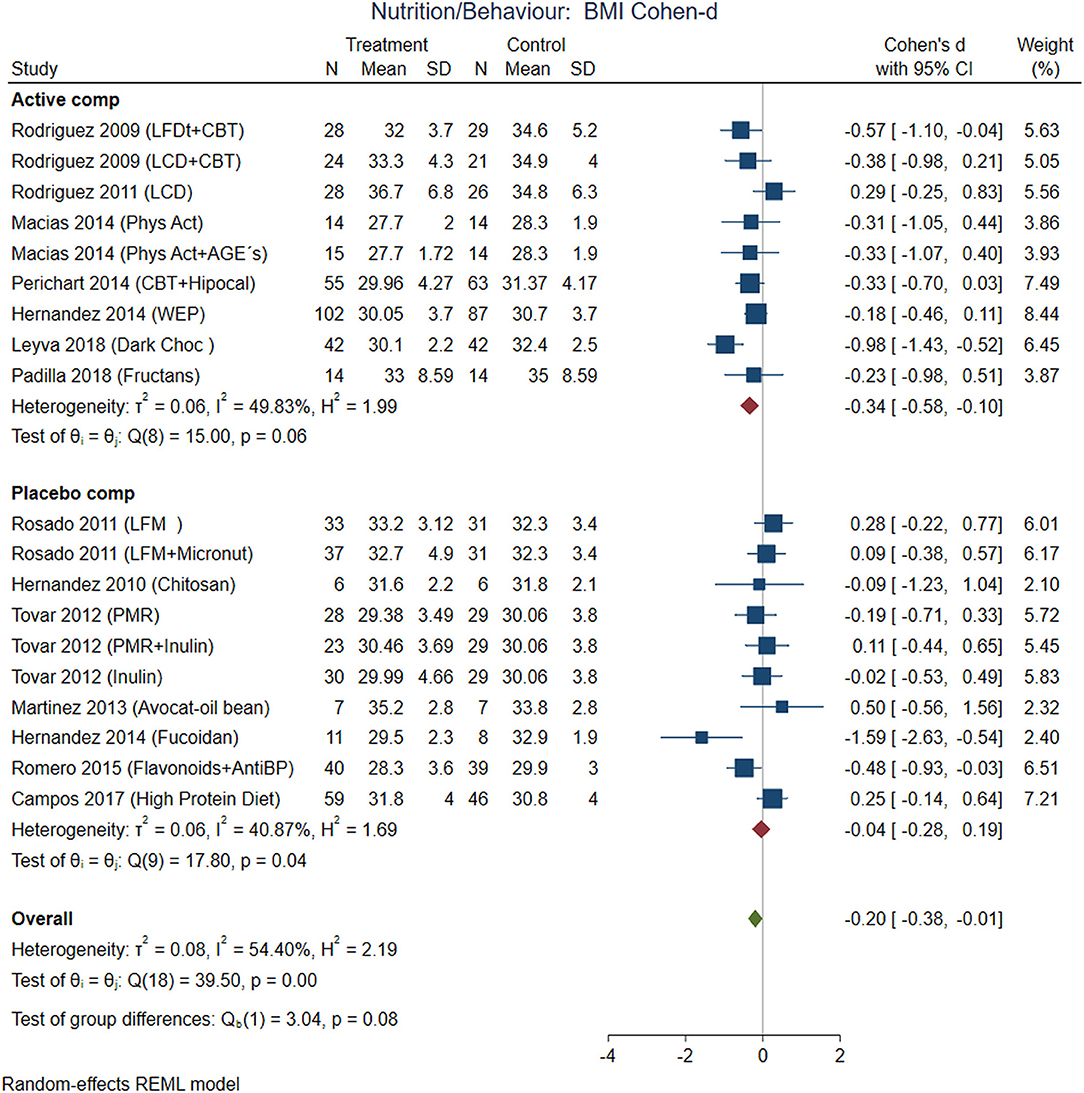
Figure 3. Pooled analysis of Cohen's d-weighted effect size on BMI reduction with nutritional and behavioral interventions. The analysis was stratified by placebo or active comparator. LFDT, Low fat diet; LCD, Low carbohydrate diet; CBT, Cognitive-behavioral therapy; Phys Act, Physical activity; Dark Choc, Dark chocolate; AGE, Advanced glycation end-product; Hipocal, Hypocaloric diet; WEP, Water and Education Provision; LFM, Low fat milk; Micronut, Micronutrients; PMR, Partial meal replacement; AntiBP, Antihypertensive medication; REML, Restricted maximum likelihood.
The comparisons between active nutrition/behavioral interventions with placebo showed improvement for BMI (Cohen-d, 95% CI, Figure 3) 0.2 (0.01, 0.38), waist circumference 0.27 (0.01, 0.53, Figure 4), triglycerides 0.34 (−0.02, 0.71; Figure 5), and systolic blood pressure 0.21 (−0.07, 0.49, Figure 6). The lowest heterogeneity was for BMI (I2 = 41%) and the highest for triglycerides (I2 = 88%). Only one intervention with physical activity showed an effect on BMI (Cohen-d of 0.3), increase on HDL-c (Cohen-d 0.16), but with wide confidence intervals. Most of these studies excluded T2D individuals, therefore the glucose levels did not show difference between compared groups.
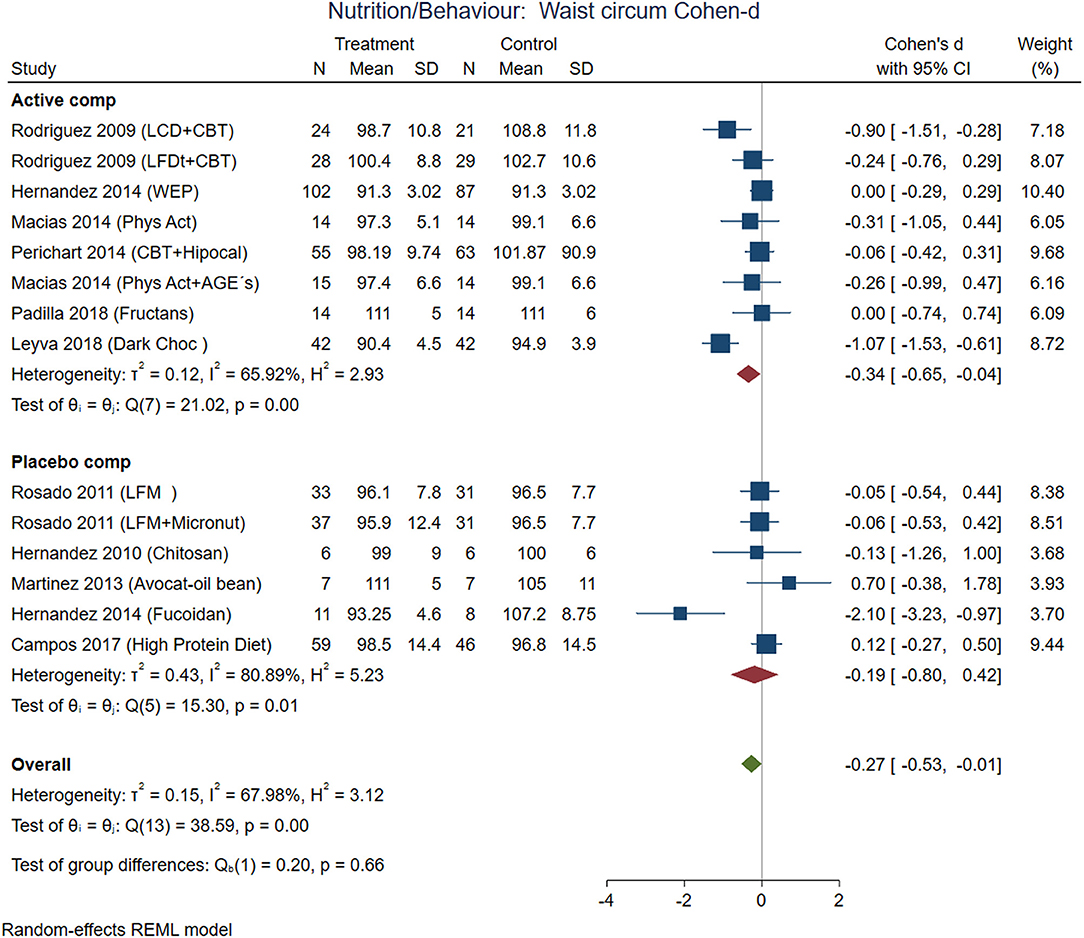
Figure 4. Pooled analysis of Cohen's d-weighted effect size on waist circumference with nutritional and behavioral interventions. The analysis was stratified by placebo or active comparator. LFDT, Low fat diet; LCD, Low carbohydrate diet; CBT, Cognitive-behavioral therapy; Phys Act, Physical activity; Dark Choc, Dark chocolate; AGE, Advanced glycation end-product; Hipocal, Hypocaloric diet; LFM, Low fat milk; Micronut, Micronutrients; PMR, Partial meal replacement; REML, Restricted maximum likelihood.
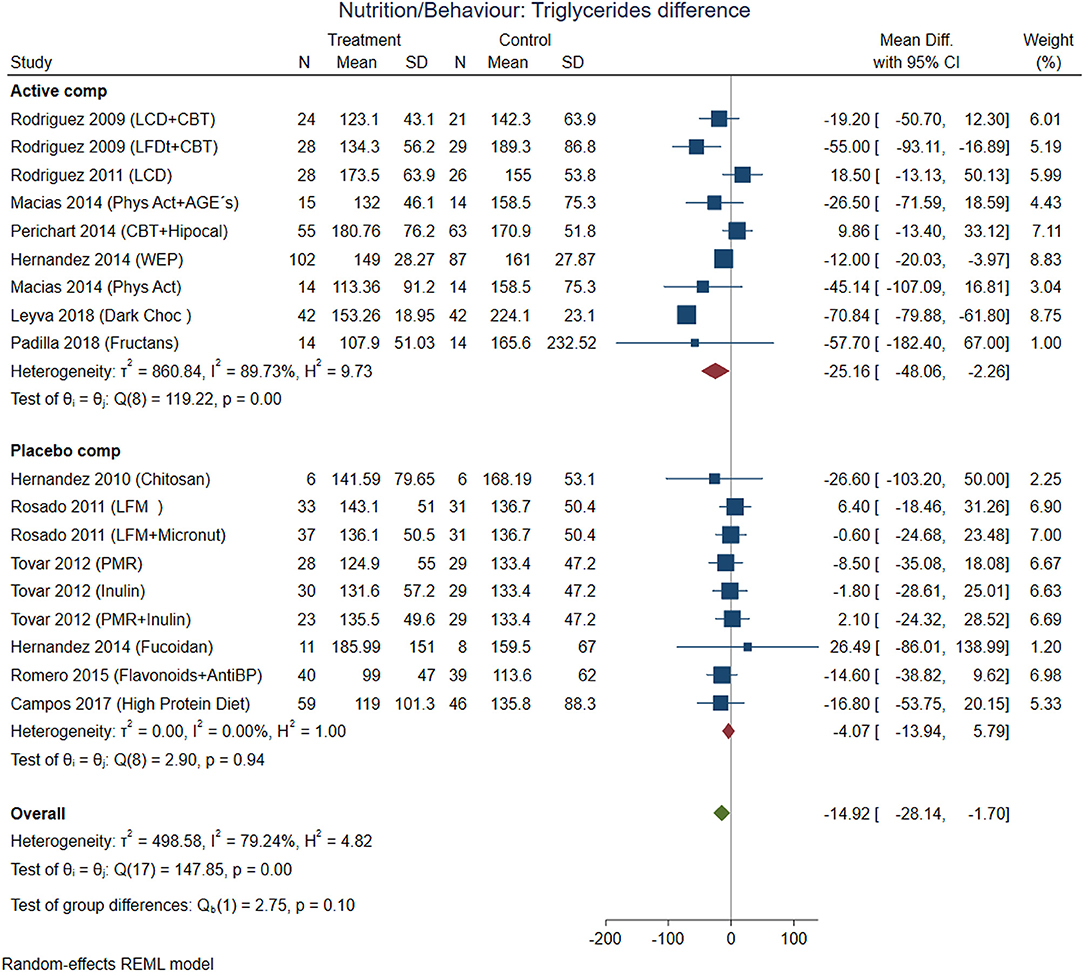
Figure 5. Pooled analysis of Cohen's d-weighted effect size on serum triglycerides concentration with nutritional and behavioral interventions. The analysis was stratified by placebo or active comparator. LFDT, Low fat diet; LCD, Low carbohydrate diet; CBT, Cognitive-behavioral therapy; Phys Act, Physical activity; Dark Choc, Dark chocolate; AGE, Advanced glycation end-product; Hipocal, Hypocaloric diet; WEP, Water and Education Provision; LFM, Low fat milk; Micronut, Micronutrients; PMR, Partial meal replacement; AntiBP, Antihypertensive medication; REML, Restricted maximum likelihood.
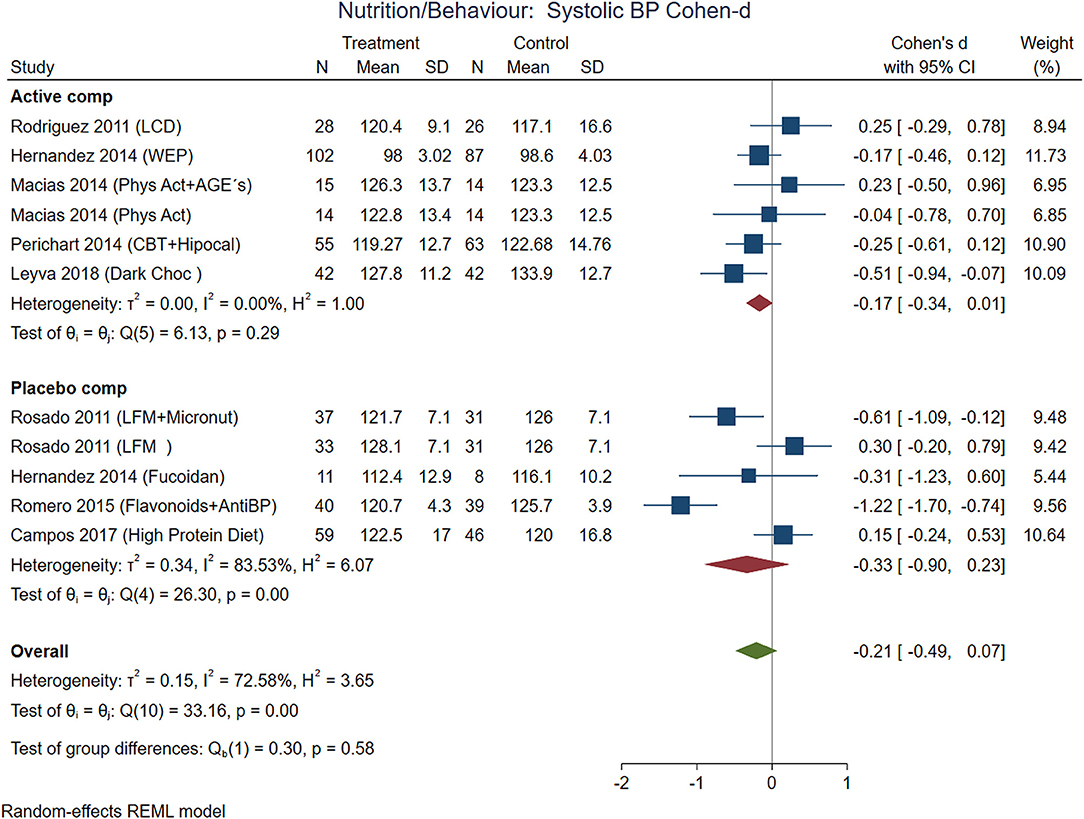
Figure 6. Pooled analysis of Cohen's d-weighted effect size on systolic blood pressure with nutritional and behavioral interventions. The analysis was stratified by placebo or active comparator. LCD, Low carbohydrate diet; CBT, Cognitive-behavioral therapy; Phys Act, Physical activity; Dark Choc, Dark chocolate; AGE, Advanced glycation end-product; Hipocal, Hypocaloric diet; WEP, Water and Education Provision; LFM, Low fat milk; Micronut, Micronutrients; AntiBP, Antihypertensive medication; REML, Restricted maximum likelihood.
Combining cognitive-behavioral therapy (CBT; goal setting, problem-solving, and stimulus control) to either a low-fat diet (21% fat, ≤ 10% saturated fat, 25% protein, 54% carbohydrates), or a low-carbohydrate diet (27% protein, 28% fat, 45% carbohydrate) produced significantly greater short-term weight loss compared to diet alone. The use of antioxidants with flavonoids contained in dark chocolate showed favorable changes in biochemical parameters (total cholesterol, triglycerides, and LDL-cholesterol level in blood) and anthropometrical parameters (waist circumference) the pooled analysis with Cohen-d supported additionally loss of BMI and decrease in systolic blood pressure (Figure 6).
Finally, the avoid of sugar-sweetened beverages (SSB) by water substitution showed positive effect on plasma triglycerides, and systolic blood pressure.
According to effect size, pharmacological treatments from studies that included participants with T2D showed improvements in BMI (Figure 7), waist circumference (Figure 8), and glucose (Figure 9) in non-T2D individuals compared with patients with T2D. BMI reduction in the T2D group had a Cohen-d of 0.24 (0.13, 0.66) compared with non-T2D reduction of 0.53 (0.27, 0.80); the waist circumference had a Cohen-d of 0.22 (0.72, 1.16) compared with non-T2D 0.55 (0.03, 1.07); diastolic blood pressure 0.18 (0.3, 1.42) vs. 0.87 (0.33, 2.06), respectively. As expected, the treatment had a large effect on glucose lowering in individuals with T2D compared to non-T2D participants (Cohen-d 0.7 vs. 0.26, respectively).
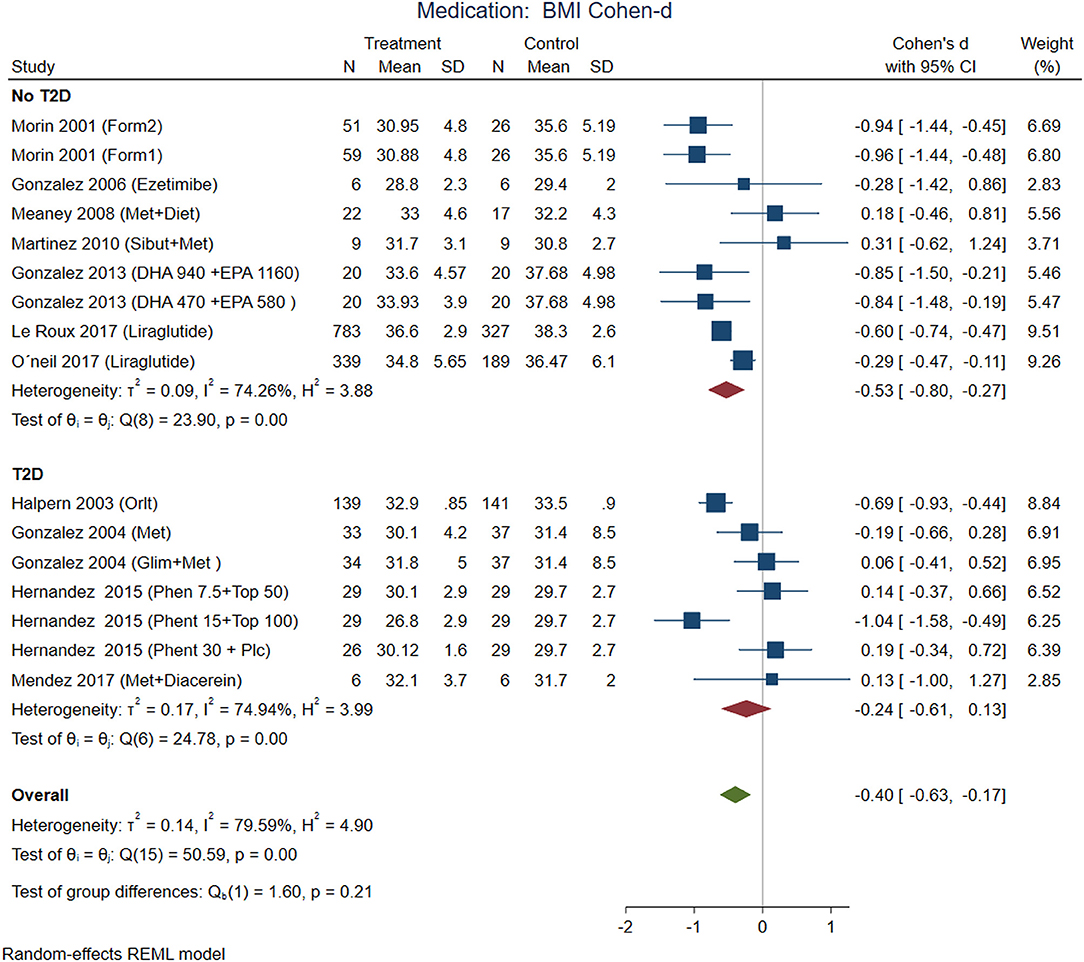
Figure 7. Pooled analysis of Cohen's d-weighted effect size on BMI reduction loss with drug (medication) treatment. The analysis was stratified by T2D status. The Form1 and Form2 are described in the text, they are not approved by FDA. Met, Metformin; Sibut, Sibutramine; DHA, Docosahexaenoic acid; EPA, Eicosapentaenoic acid; Orlit, Orlistat; Glim, Glimepiride; Phent, Phentermine; Top, Topiramate. REML, Restricted maximum likelihood.
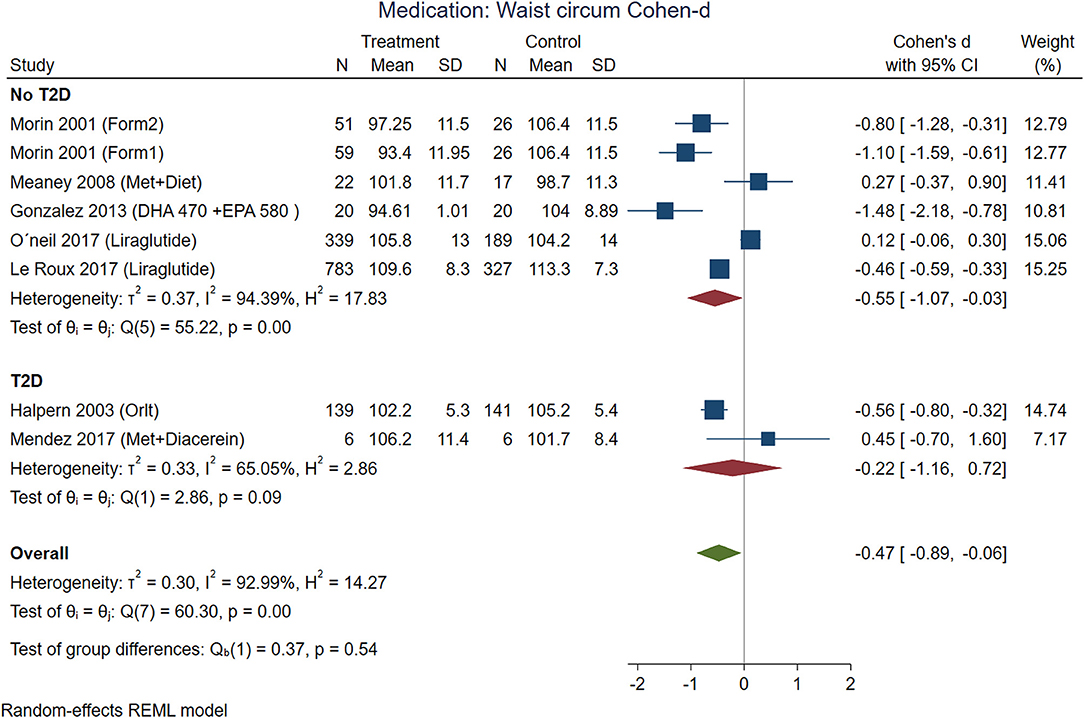
Figure 8. Pooled analysis of Cohen's d-weighted effect size on waist circumference with drug (medication) treatment. The analysis was stratified by T2D status. The Form1 and Form2 are described in the text, they are not approved by FDA. Met, Metformin; Sibut, Sibutramine; DHA, Docosahexaenoic acid; EPA, Eicosapentaenoic acid; Orlit, Orlistat; Glim, Glimepiride; Phent, Phentermine; Top, Topiramate; REML, Restricted maximum likelihood.
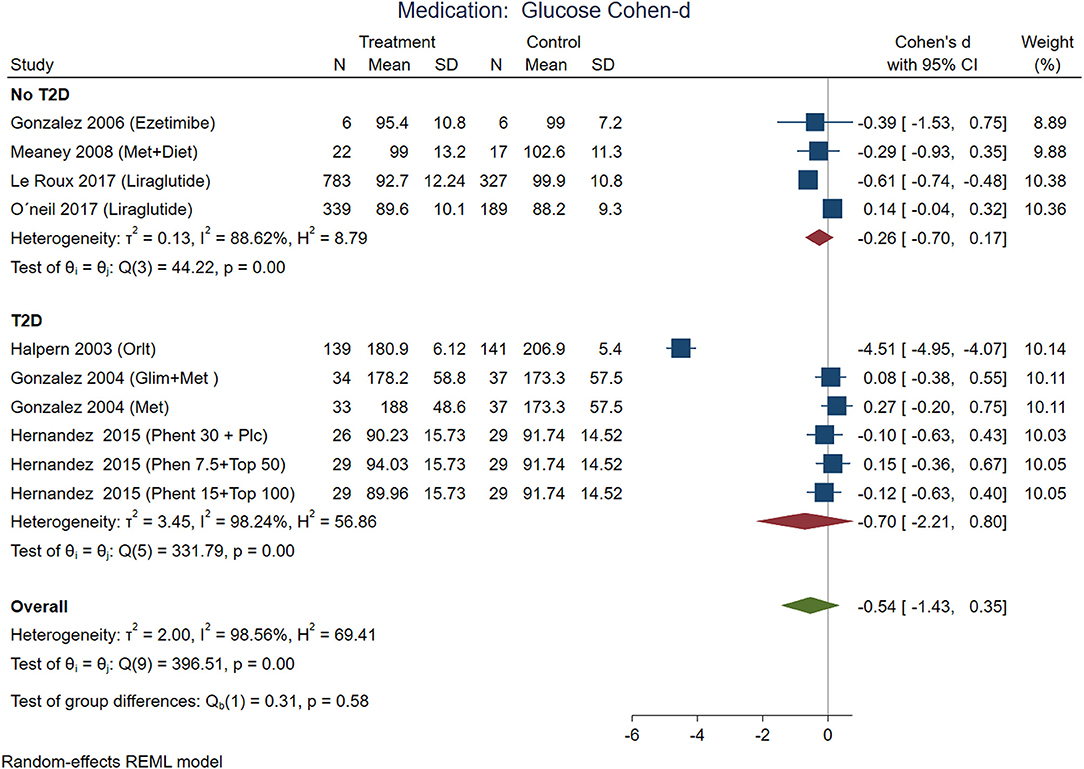
Figure 9. Pooled analysis of Cohen's d-weighted effect size on serum glucose serum concentration with drug (medication) treatment. The analysis was stratified by T2D status. Met, Metformin; Orlit, Orlistat; Glim, Glimepiride; Phent, Phentermine; Top, Topiramate, REML, Restricted maximum likelihood.
Some medications used in Mexico had a large effect on weight reduction (Figures 7, 8) in participants without T2D (Cohen-d about 0.9). For instance, the use of DHA (docosahexanoic acid) 470 or 940 mg combined with EPA (eicosapentanoic acid) 580 or 1,160 mg, compared with placebo, and the use of two different formulations (Formula 1: d-norpseudoephedrine 50 mg, triiodothyronine 75 ug, diazepam 5 mg, atropine 0.36 mg, aloin 16.2 mg; and formula 2: d-norpseudoephedrine 50 mg, atropine 0.36 mg, aloin 16.2 mg.) for 6 months compared with placebo. These medications are not approved for treatment of obesity by FDA, and the formulations are not legally available for purchase in the US, however, reports in US found thyroid intoxication (65). The effect of liraglutide was between 0.3 and 0.6 including participants from international samples. Participants with T2D showed the use of phentermine 15 mg and topiramate 100 mg had higher effect compared with phentermine 7.5 mg and placebo. There was no replication for any of these studies, the Egger test on a random model showed no small study effects on BMI for 18 interventions on nutrition/behavioral (p = 0.43), nor for 19 interventions on medication (p = 0.22).
It is interesting that systolic blood pressure was modified by non-pharmacological treatments, meanwhile, diastolic blood pressure was modified in non-T2D participants treated with medications (Figure 10). From the five analyzed studies with medications, three of them included patients with hypertension (prevalence of hypertension between 24 and 42%). The blood pressure decreases with weight loss, the Trial of Hypertension Prevention had a weight loss intervention arm, resulting in reduction of both, systolic and diastolic, measurements (66).
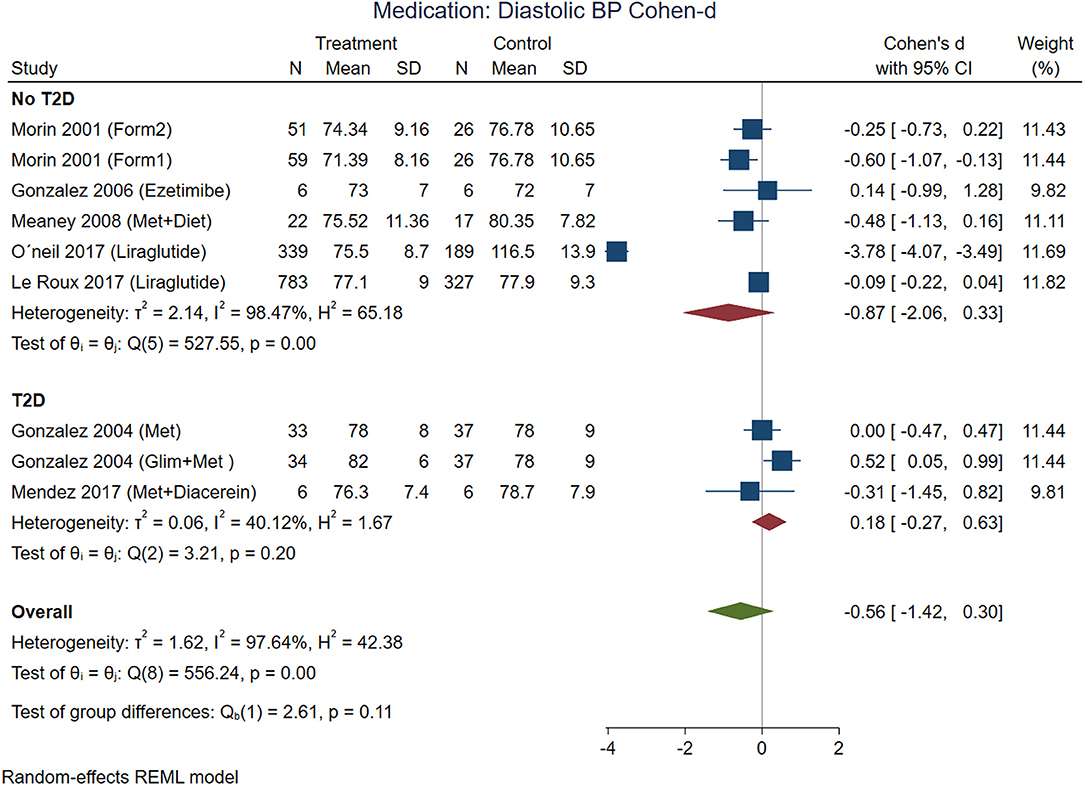
Figure 10. Pooled analysis of Cohen's d-weighted effect size onof effect by Cohen-d in diastolic blood pressure with drug (medication) treatment. The analysis was stratified by T2D status. The Form1 and Form2 are described in the text, they are not approved by FDA but approved by its Mexican counterpart, COFEPRIS. Met, Metformin; Sibut, Sibutramine; Orlit, Orlistat; Glim, Glimepiride; Phent, Phentermine; Top, Topiramate; REML, Restricted maximum likelihood.
We made multiple Meta-Analyses clustering the studies into stratum by type of intervention, T2D status, and group of comparison. Additionally, we did meta regression analyzing the mean age, BMI, months of treatment, comparison with placebo and geographical location measured by latitude. Those confounders that reached statistical significance for HDL-c serum levels were the duration of the intervention [b = 1.07 (se 0.49) p = 0.03, b: beta value, se: standard error] and the comparison vs. placebo [b = 4.4 (se 2.1) p = 0.04]. The triglyceride serum levels showed effects from the mean age of the study [b = 1.3 (se 0.59) p = 0.03] and the geographic location [b = −2.7 (se 1.3) p = 0.04]. However, the geographic location was closely related with the type of intervention, for example, studies located close to the Mexico-U.S. border used physical activity interventions; meanwhile the South regions used nutritional supplements. The diastolic blood pressure was modified by the BMI [b = −0.49 (se 0.27) p = 0.067] and geographical location [b = −0.9 (se 0.44) p = 0.04], however these variables were influenced by the treatment with liraglutide (Supplementary Figures 1, 2).
A network meta-analysis of drug treatments and T2D status was performed for BMI, diastolic blood pressure (DBP), and glucose. The network meta-analysis included direct comparisons constructed with connections between treatments, and indirect comparisons using all possible connections between treatments. All networks had the principles of coherence, transitivity, and consistency. This analysis was not feasible for nutritional/behavioral interventions due to the design and the small number of studies. Supplementary Figure 3 illustrates two networks for studies with T2D patients, examining the efficacy of pharmacological interventions on the studied variables, one network for each comparison between treatments and placebo (Supplementary Figure 3A) and with metformin (Supplementary Figure 3B). These network diagrams provide a graphical representation of how each intervention connects to any other direct comparisons. Table 5 (matrix A and B) and Supplementary Tables 1, 2 detail the complete matrix of results, in which the comparative effects between drugs are shown in terms of differences in standardized means.
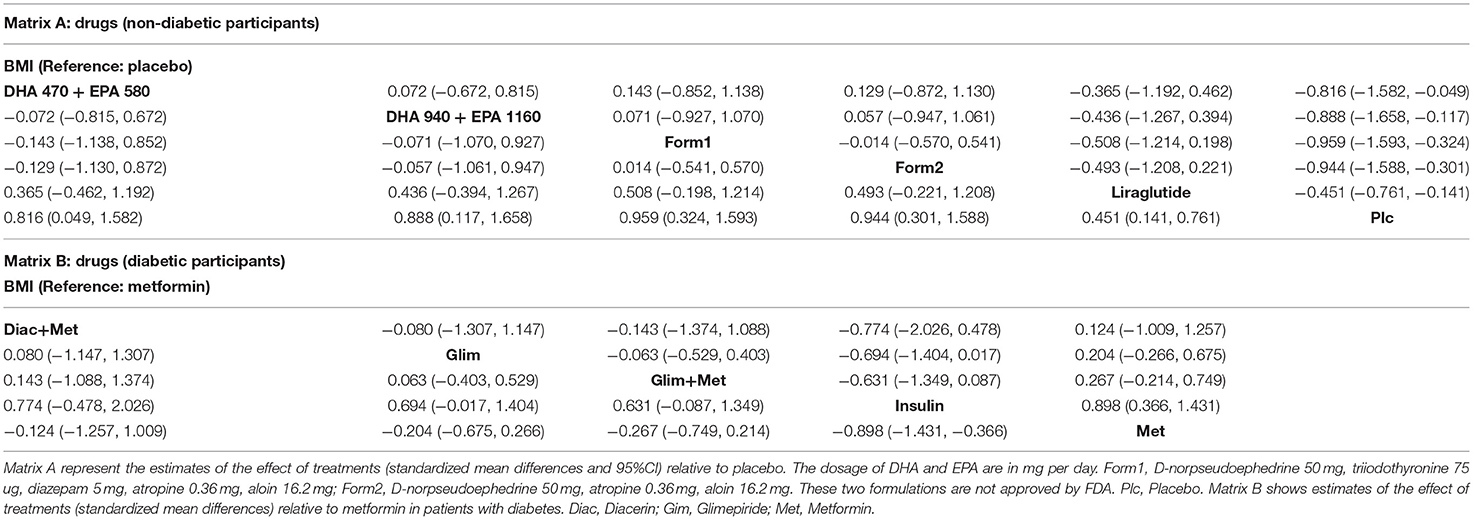
Table 5. Network meta-analysis results matrix.
The contrast matrix between pharmacological treatments with placebo showed a decrease on BMI in every pharmacological intervention, for instance, DHA 470 + EPA 580 mg was 0.816 (CI: 0.049, 1.582); DHA 940 + EPA 1,160 mg: 0.888 (CI: 0.117, 1.658); Formulation 1: 0.959 (CI: 0.324, 1.593); Formulation 2: 0.944 (CI: 0.301, 1.588); Liraglutide: 0.451 (CI: 0.141, 0.761). On the other hand, the status of T2D consistently supported metformin alone or in combinations was the most effective intervention for reducing BMI compared to insulin: −0.898 (CI: −1.431, −0.366). Regarding glucose, the intervention with insulin was more effective in reducing serum glucose levels compared to metformin: −1.506 (CI: −2.084, −0.928); Glimepiride + metformin: −1.332 (CI: −2.083, −0.581) and Glimepiride: −1.332 (CI: −2.077, −0.587). In summary, the interventions with the greatest contribution to the reduction of DBP were metformin: −0.507 (CI: −0.994, −0.020) compared to Glimepiride + metformin, and Glimepiride: −0.507 (−0.980, −0.033) compared to Glimepiride + metformin. Monotherapy interventions had greater efficacy on DBP compared to dual therapies.
This systematic review and multiple meta-analyses by strata summarize the existing evidence of weight loss as primary or secondary aims in the adult population. Besides, we analyzed the cardiometabolic risk traits affected by the proposed strategies and clustered by the type of intervention, control group and T2D status. Our analysis was limited to randomized clinical studies conducted in Mexico or from international multicentric studies with Mexican participants involving nutrition, behavior, medication, or alternative medicine interventions. Some interventions of interest were compared with another active strategy (medication, behavior, physical activity or any other than placebo). This strategy can blunt the effect size of the intervention, because of the effect of active comparators in metabolic and anthropometric variables. We found that all studied interventions were better than placebo, or better than the selected comparator, and many of the published papers made individual paired contrasts between final and basal values. However, we decided to contrast treatments and reported the size of effects by cardiometabolic risk traits. With this strategy we had the advantage of computing the effect size over a maneuver the researchers considered the best comparator. The results should be interpreted considering these control groups defined by the researchers.
The 55 analyzed interventions (from 45 studies) were categorized as nutritional/behavioral with a total sample of 1,407 participants. Pharmacological interventions in Mexico included 1,134; and multinational interventions added 1,307 participants (Hispanics). Surgical procedures were 72, while alternative treatments included 235 individuals. We obtained a total of 4,155 participants from these trials.
The nutritional/behavioral strategies included supplemental, flavonoids, manipulation of macronutrient content diets (low fat, low carb, high protein) with caloric restriction, water consumption and physical activities. CBT combined with a low-calorie diet showed beneficial effects on BMI and waist circumference while combined with a low-fat diet decreased glucose and triglycerides. A cardioprotective structured hypocaloric diet is more effective than the CBT approach in reducing metabolic syndrome (54). Daily flavonoid-rich chocolate (70% cocoa) intake improves fasting plasma glucose levels and insulin resistance parameter (HOMA-IR) and the lipid and glucose metabolism (41). The physical activity showed benefic but small and non-significant effects for the analyzed variables, due to the lack of enough sample size. Other systematic reviews focused on physical activity showed Hispanics had less leisure-time compared with other groups in the U.S., the most common activity was walking, but the most significant results were those with moderate to vigorous physical activity (67). It will be crucial to increase legislative policies to build environments that increase available opportunities for physical activities, particularly for this fast-growing population group.
Adherence to diet and exercise programs (45–60 min/d, 5 days per week) are part of the nutritional/behavioral interventions. Other studies reporting that water consumption habit (2–3 L/day) and partially decreasing sugar-sweetened beverage (SSB) intake of at least 250 kcal/d, with nutritional counseling was effective in increasing water intake (63), and additionally reduces cardiometabolic risks of drinking or eating less sugar in the diet promoting health benefits, although we found positive effect on plasma triglycerides and systolic blood pressure in our analysis, perhaps a consequence of the reduction of the SSB consumption.
The drug treatment in groups of participants with T2D, showed small effect size on improvement on BMI, waist circumference and triglycerides compared with larger effects for non-T2D. The orlistat group in T2D showed weight loss (BMI and waist circumference) lower level of glucose, triglycerides, and systolic blood pressure. Comparing these findings with other studies made in Mexican Americans living in the border shows the difficulty of losing weight with programs on self-management education, but the HbA1c improved (68).
Medication showed larger size of effects on BMI for combined formulations like orlistat, phentermine with topiramate, both approved by regulatory agencies. Other formulations like the combination of triiodothyronine with phentermine (non-approved by FDA but approved by its Mexican counterpart, COFEPRIS—Federal Committee for Protection from Sanitary Risks), and combination of DHA and EPA showed effect on BMI. The authors of the formulations did not show the result on serum glucose neither reported any adverse effect. There was no replication for any of these treatments. We found a couple of sibutramine trials. This is a retired medication because the cardiovascular risk was greater than the benefits (69), especially for the difficulty to identify patients with silent cardiovascular disease (70).
Surgical intervention is the most effective treatment for patients with morbid obesity (71). The percentage of body weight loss with this intervention ranges between 33 and 77% in a period of 24 months, thus demonstrating its effectiveness (72, 73). However, in our surgical papers, no significant differences were found in the percentage of weight loss, this due to the fact that both the intervention group and the control group had equivalent surgeries (74). One of the studies compared banded vs. unbanded laparoscopic roux-en-Y gastric bypass and follow up weight changes for 24 months (61), in a second analysis, no differences were found between these procedures after 5 years of follow-up (75).
In general, many of the studied interventions are challenging to blind for obvious reasons. For example, a comparison of nutritional interventions vs. exercise or CBT cannot be blind. However, there is a possibility to blind the evaluators, but no studies explicitly describe this strategy. We found that heterogeneity of the results was partially attributable to basal differences between contrasting groups, for example in the study of Rosado et al. (46) the diastolic and systolic blood pressure were significantly different between the studied low fat milk groups compared with controls. Some surgical studies for weight loss made in the Instituto de Nutrición Salvador Zubirán in Mexico City blinded the abdominal wall for patients and evaluators when they compared the open abdominal approach vs. the laparoscopic method. The risk of bias can be lessened but still can compromise the results of the studies. The difficulty in addressing nutritional or behavioral interventions is manifest in studies analyzing racial/ethnic disparities. Multilevel church-based interventions considering socio-ecological influence showed a greater impact if they consider program interventions tailored to specific communities.
The most important limitations are the lack of replication studies with the same medications, and the small sample size in most of the studies. There was a wide variety for the selection criteria of participants (i.e., some studies had too specific eligibility criteria for sex, age and BMI compared with other studies with wide range of options), and, despite similar genetic background, the participants live in sites embedded in cultural diversity (i.e., Mexico City's environment problems differ from those in States close to the Mexico-U.S. border). We address a broad question regarding the cardiometabolic traits and found a considerable heterogeneity of the studies. We addressed this problem using meta-regression to statistically weight the main confounders across studies and the use of a network Meta-Analysis to compute the magnitude of contrasts between treatment effects. Due to these limitations the obtention of unstable coefficients is possible, therefore, these analyses should be repeated in the future with a greater number of studies.
The small sample sizes from many of the included studies resulted in low statistical power for contrasting between treatment, and the lack of replication studies increased the standard error for the analysis. The new medications approved by FDA have been tested scarcely in the Mexican population. About 44% of the studies were performed in the limit time of placebo effects (about 12 weeks), but those with more time showed effects on the HDL cholesterol levels.
Southern states of Mexico are experiencing an epidemiological transition toward mortality causes, like T2D, toward the Northern states (76). The Studies we gathered do not have information regarding the socioeconomic strata of the patients, we do not have data to analyze if social determinants affect the adherence or the response to the treatments. This issue should be considered in coming studies for being analyzed.
Future new and replication studies should consider larger periods for treatments to reduce placebo effects. Future reviews and Meta-Analysis should analyze anti-obesity interventions in children and adolescents as well as in old age populations. These suggestions agree with the Healthy People 2030 recommendation on study effective strategies to diminish obesity in children and adolescents (77).
The Mexican states in which research on anti-obesity interventions was conducted involved only 10 of the 32 states. The Mexico-U.S. border has sister states: California-Baja California, Arizona-Sonora, New Mexico-Chihuahua, Texas with Chihuahua, Coahuila, Nuevo León, and Tamaulipas. There is a lack of Meta-Analysis in the Mexican-American population for anti-obesity and anti-diabetic treatments or their influence on cardiometabolic traits. Future studies are needed to fulfill this gap. On the other hand, the Binational initiative should improve the collaborative studies in the U.S.-Mexico border to address interventions in this growing population. The programs from this initiative address environmental protection, communication committees in particular communities (78). The U.S.,-Mexico Border Health Commission has agreements with the Secretary of Health from both countries, and this agency supports initiatives in health security (79). The programs include prevention and wellness using guidelines for eating healthy, physical activity, and drug misuse and abuse prevention.
Clinical experience of researchers on obesity began in 1959 in Mexico City, yet publications on obesity interventions in randomized clinical trials studies in Mexico did not appear until 1996, mainly focused on pharmaceutical, nutritional, or physical activity interventions. Adult participants included in these studies were predominantly from the central and northern Mexican states, with a clear absence from the costal and southern states. Anti-obesity studies in the Mexican population include small samples and reduced time for interventions. A strategy to improve the statistical power for the studies is to conduct multicentric studies, and a compromise from the State or private industries to provide sufficient financial resources.
A national research network is feasible for answering relevant questions regarding anti-obesity interventions and its metabolic consequences. It is clear that not all cardiometabolic traits have the same response to the intervention. The inclusion of Mexican Americans and Mexican immigrants living in the U.S., would be desirable to clarify the importance of different approaches to tackle this problem.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
EG-O, JM-E, AD-B, AP-T, and JL-A supervised the findings and with YM-L, SR-C, AB-F, EL-S, OM-C, EN-G, and MR-D contributed to data collection, extraction, and analysis. CR-P, KC, BT, and JL-A made critical contributions and final approval of the manuscript. EG-O, YM-L, AD-B, SR-C, LP-N, and JL-A performed the statistical analysis and with JM-E developed the theory. All authors discussed the results and contributed to the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Dr. Beatriz Tapia, Office of Faculty Affairs and Department of Pediatrics, School of Medicine, The University of Texas Rio Grande Valley, Harlingen, Texas, United States; and Dr. Edith Cantú de Luna, Principal of the Universidad Mexico-Americana del Norte, Reynosa, Tamaulipas, Mexico, for their generous support in this paper publication. We also thank Dr. Victoria Valles from the National Institute of Medical Sciences and Nutrition Dr. Salvador Zubiran (INCMNSZ) for the share of invaluable experience about the ENEC-93. Last, we would like to pay our gratitude and our respects to Dr. Gonzalez-Barranco. He was a pioneer in obesity research since the 1970s, Dr. Gonzalez-Barranco passed away in December of 2020.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.665023/full#supplementary-material
Supplementary Figure 1. Meta- regression of nutritional/behavioral effects on the mean difference in HDL-C (A) and triglycerides (B) concentrations, adjusted by mean age, BMI, duration of treatment (months), geographical latitude, and use of placebo or active comparator. The gray zone represents the 95% CI of the regression. Liraglutide was used in participants with the highest obesity and in geographic locations in northern Mexico. AGE's, Advanced glycation end-product; AntiBP, Antiblood pressure medication; CBT, Cognitive-behavioral therapy; Dark Choc, Dark chocolate, Hipol; LCD, Low carbohydrate diet; LFDt, Low fat diet; LFM, Low fat milk, Micronut; Phys Act, Physical activity; PMR, Partial meal replacement; WEP, Water and education provision.
Supplementary Figure 2. Meta regression of medication effects on the mean difference in diastolic blood pressure adjusted by mean age, BMI, duration of treatment (months), geographical latitude, and use of placebo or active comparator. The (A) shows the effect of BMI and the (B) the geographical location. The gray zone represents the 95%CI of the regression. Liraglutide was used in participants with the highest obesity and in geographical locations in northern Mexico. The Form1 and Form2 are described in the text, they are not approved by FDA. Met, Metformin; Sibut, Sibutramine; Orlit, Orlistat; Glim, Glimepiride; Phent, Phentermine; Top, Topiramate.
Supplementary Figure 3. Network meta-analysis of studies examining the efficacy of drug treatments in patients with obesity on (A) BMI in non-diabetic patients compared to placebo, (B) BMI in patients with diabetes compared to metformin. The colors of the edges and nodes refer to the risk of bias: low (green), moderate (yellow), and high (red). DHA and EPA doses are in mg per day. Met, Metformin; Diac+Met, Diacerin + Metformin. The Form1 and Form2 are described in the text, they are not approved by FDA but approved by its Mexican counterpart, COFEPRIS. Plc, Placebo.
Supplementary Table 1. Network meta-analysis results matrix. Estimates of the effect of treatments (standardized mean differences with 95% CI) relative to placebo (Plc). The Form1 and Form2 are described in the text, they are not approved by FDA.
Supplementary Table 2. Network meta-analysis results matrix. Estimates of the effect of treatments (standardized mean differences with 95% CI) relative to metformin in patients with diabetes. The Form1 and Form2 are described in the text, they are not approved by FDA.
1. Komaroff M. For researchers on obesity: historical review of extra body weight definitions. J Obes. (2016) 2016:2460285. doi: 10.1155/2016/2460285
2. Weir CB, Jan A. BMI Classification Percentile and Cut Off Points. Treasure Island, FL: Stat Pearls Publishing (2020).
3. Rtveladze K, Marsh T, Barquera S, Sanchez Romero LM, Levy D, Melendez G, et al. Obesity prevalence in Mexico: impact on health and economic burden. Public Health Nutr. (2014) 17:233–9. doi: 10.1017/S1368980013000086
4. Kondrup J. Basic concepts in nutrition: energy and protein balance. e-SPEN. (2008) 3:e117–20. doi: 10.1016/j.eclnm.2008.02.003
5. Lopez-Alvarenga JC, Montesinos-Cabrera RA, Velazquez-Alva C, Gonzalez-Barranco J. Short stature is related to high body fat composition despite body mass index in a Mexican population. Arch Med Res. (2003) 34:137–40. doi: 10.1016/S0188-4409(03)00002-X
6. Castro-Porras LV, Rojas-Russell ME, Aedo-Santos A, Wynne-Bannister EG, Lopez-Cervantes M. Stature in adults as an indicator of socioeconomic inequalities in Mexico. Rev Panam Salud Publica. (2018) 42:e29. doi: 10.26633/RPSP.2018.29
7. Secretaría de Salud. Norma Oficial Mexicana Nom-174-Ssa1-1998, Para El Manejo Integral De La Obesidad (1998).
8. United States Department of Health and Human Services. Healthy People 2020. United States Department of Health and Human Services, Washington, DC (2010). Available online at: https://www.healthypeople.gov/2020/About-Healthy-People
9. Maldonado LE, Albrecht SS. Does the immigrant advantage in overweight/obesity persist over time in Mexican American youth? NHANES 1988−1994 to 2005–2014. Obesity. (2018) 26:1057–62. doi: 10.1002/oby.22178
10. Yoshida Y, Scribner R, Chen L, Broyles S, Phillippi S, Tseng TS. Role of age and acculturation in diet quality among Mexican Americans - findings from the national health and nutrition examination survey, 1999–2012. Prev Chronic Dis. (2017) 14:E59. doi: 10.5888/pcd14.170004
11. Hanley MJ, Abernethy DR, Greenblatt DJ. Effect of obesity on the pharmacokinetics of drugs in humans. Clin Pharmacokinet. (2010) 49:71–87. doi: 10.2165/11318100-000000000-00000
12. Initiative NOE. The Practical Guide. Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. NIH publication Number 00-4084 (2000).
13. Yumuk V, Tsigos C, Fried M, Schindler K, Busetto L, Micic D, et al. European guidelines for obesity management in adults. Obes Facts. (2015) 8:402–24. doi: 10.1159/000442721
14. Apovian CM, Aronne LJ, Bessesen DH, McDonnell ME, Murad MH, Pagotto U, et al. Pharmacological management of obesity: an endocrine Society clinical practice guideline. J Clin Endocrinol Metab. (2015) 100:342–62. doi: 10.1210/jc.2014-3415
15. Ehara T. Mexico and its Obesity Epidemic. Global Food Cultures. (2018). Available online at: https://wp.nyu.edu/steinhardt-gfcmexico2018/2018/04/11/mexico-and-its-obesity-epidemic/ (accessed January 4, 2021).
16. Garcia-Oropesa EM, Bustamante-Fuentes A, Carter K, Diaz-Badillo A, Lopez-Alvarenga JC, Lopez-Sosa EB, et al. Clinical Randomized Trials for Anti-Obesity Interventions in the Mexican Population: A Systematic Review With Meta-Analysis. PROSPERO 2020 CRD42020221436. Available online at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020221436 (accessed September 10, 2021).
17. Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev. (2014) 3:82. doi: 10.1186/2046-4053-3-82
18. Martínez-Ezquerro JD, Ruiz-Cejudo SM, Bustamante-Fuentes A, Díaz-Badillo Á, García-Oropesa EM, López-Sosa EB, et al. Consenso experto en tiempos de COVID-19: aplicaciones del método Delphi en materia de salud. Cir Cir. (2020) 89:120–9. doi: 10.24875/CIRU.20000936
19. Gonzalez-Heredia T, Hernandez-Corona DM, Gonzalez-Ortiz M, Martinez-Abundis E. Effect of linagliptin versus metformin on glycemic variability in patients with impaired glucose tolerance. Diabetes Technol Ther. (2017) 19:471–5. doi: 10.1089/dia.2017.0020
20. Gonzalez-Ortiz M, Martinez-Abundis E, Hernandez-Corona DM, Ramirez-Rodriguez AM. Effect of tadalafil administration on insulin secretion and insulin sensitivity in obese men. Acta Clin Belg. (2017) 72:326–30. doi: 10.1080/17843286.2017.1293759
21. le Roux CW, Astrup A, Fujioka K, Greenway F, Lau DCW, Van Gaal L, et al. 3 years of liraglutide versus placebo for type 2 diabetes risk reduction and weight management in individuals with prediabetes: a randomised, double-blind trial. Lancet. (2017) 389:1399–409. doi: 10.1016/S0140-6736(17)30069-7
22. O'Neil PM, Garvey WT, Gonzalez-Campoy JM, Mora P, Ortiz RV, Guerrero G, et al. Effects of liraglutide 3. 0 mg on weight and risk factors in hispanic versus non-hipanic populations: subgroup analysis from scale randomized trials. Endocr Pract. (2016) 22:1277–87. doi: 10.4158/EP151181.OR
23. Sanchez-Rodriguez MA, Zacarias-Flores M, Castrejon-Delgado L, Ruiz-Rodriguez AK, Mendoza-Nunez VM. Effects of hormone therapy on oxidative stress in postmenopausal women with metabolic syndrome. Int J Mol Sci. (2016) 17:1388. doi: 10.3390/ijms17091388
24. Sanchez-Munoz V, Salas-Romero R, Del Villar-Morales A, Martinez-Coria E, Pegueros-Perez A, Franco-Sanchez JG. [Decrease of liver fat content by aerobic exercise or metformin therapy in overweight or obese women]. Rev Invest Clin. (2013) 65:307–17.
25. Gonzalez-Acevedo O, Hernandez-Sierra JF, Salazar-Martinez A, Mandeville PB, Valadez-Castillo FJ, De La Cruz-Mendoza E, et al. [Effect of Omega 3 fatty acids on body female obese composition]. Arch Latinoam Nutr. (2013) 63:224–31.
26. Martínez-Abundis E, Valera-Gonzalez I, Hernandez-Salazar E, Gonzalez-Ortiz M. Effect of metformin and sibutramine on insulin sensitivity and adiposity in obese patients. Obes Metab. (2010) 6:100–4.
27. Meaney E, Vela A, Samaniego V, Meaney A, Asbun J, Zempoalteca JC, et al. Metformin, arterial function, intima-media thickness and nitroxidation in metabolic syndrome: the mefisto study. Clin Exp Pharmacol Physiol. (2008) 35:895–903. doi: 10.1111/j.1440-1681.2008.04920.x
28. Gonzalez-Ortiz M, Martinez-Abundis E, Kam-Ramos AM, Hernandez-Salazar E, Ramos-Zavala MG. Effect of ezetimibe on insulin sensitivity and lipid profile in obese and dyslipidaemic patients. Cardiovasc Drugs Ther. (2006) 20:143–6. doi: 10.1007/s10557-006-7805-x
29. Toplak H, Ziegler O, Keller U, Hamann A, Godin C, Wittert G, et al. X-PERT: weight reduction with orlistat in obese subjects receiving a mildly or moderately reduced-energy diet: early response to treatment predicts weight maintenance. Diabetes Obes Metab. (2005) 7:699–708. doi: 10.1111/j.1463-1326.2005.00483.x
30. Zaragoza RM, Lonngi G, Ortiz RA, Huerta DR. Comparison of two formulations of d-norpseudoephedrine and placebo in obese patients treated during six months [Comparación de dos formulaciones de d-norpseudoefedrina y placebo en pacientes obesos tratados durante seis meses]. Med Int Mex. (2001) 17:260–71.
31. Cuellar GE, Ruiz AM, Monsalve MC, Berber A. Six-month treatment of obesity with sibutramine 15 mg; a double-blind, placebo-controlled monocenter clinical trial in a Hispanic population. Obes Res. (2000) 8:71–82. doi: 10.1038/oby.2000.10
32. Fanghanel G, Cortinas L, Sanchez-Reyes L, Berber A. A clinical trial of the use of sibutramine for the treatment of patients suffering essential obesity. Int J Obes Relat Metab Disord. (2000) 24:144–50. doi: 10.1038/sj.ijo.0801098
33. Fanghanel G, Cortinas L, Sanchez-Reyes L, Berber A. Second phase of a double-blind study clinical trial on Sibutramine for the treatment of patients suffering essential obesity: 6 months after treatment cross-over. Int J Obes Relat Metab Disord. (2001) 25:741–7. doi: 10.1038/sj.ijo.0801592
34. Ramos-Zavala MG, Gonzalez-Ortiz M, Martinez-Abundis E, Robles-Cervantes JA, Gonzalez-Lopez R, Santiago-Hernandez NJ. Effect of diacerein on insulin secretion and metabolic control in drug-naive patients with type 2 diabetes: a randomized clinical trial. Diabetes Care. (2011) 34:1591–4. doi: 10.2337/dc11-0357
35. Fanghanel G, Silva U, Sanchez-Reyes L, Sisson D, Sotres D, Torres EM. Effects of metformin on fibrinogen levels in obese patients with type 2 diabetes. Rev Invest Clin. (1998) 50:389–94.
36. Fanghanel G, Sanchez-Reyes L, Trujillo C, Sotres D, Espinosa-Campos J. Metformin's effects on glucose and lipid metabolism in patients with secondary failure to sulfonylureas. Diabetes Care. (1996) 19:1185–9. doi: 10.2337/diacare.19.11.1185
37. Villar MM, Martinez-Abundis E, Preciado-Marquez RO, Gonzalez-Ortiz M. Effect of diacerein as an add-on to metformin in patients with type 2 diabetes mellitus and inadequate glycemic control. Arch Endocrinol Metab. (2017) 61:188–92. doi: 10.1590/2359-3997000000242
38. Hernandez-Bastida A. Phentermine and topiramato vs phentermine plus placebo in patients with overweight or obesity class I or II [Fentermina y topiramato contra fentermina más placebo en pacientes con sobrepeso u obesidad clase I o II]. Med Int Mex. (2015) 31:125–36.
39. Gonzalez-Ortiz M, Martinez-Abundis E. Grupo para el Tratamiento de la Diabetes Mellitus con C. [Efficacy and safety of glimepiride plus metformin in a single presentation, as combined therapy, in patients with type 2 diabetes mellitus and secondary failure to glibenclamide, as monotherapy]. Rev Invest Clin. (2004) 56:327–33.
40. Halpern A, Mancini MC, Suplicy H, Zanella MT, Repetto G, Gross J, et al. Latin-American trial of orlistat for weight loss and improvement in glycaemic profile in obese diabetic patients. Diabetes Obes Metab. (2003) 5:180–8. doi: 10.1046/j.1463-1326.2003.00262.x
41. Leyva-Soto A, Chavez-Santoscoy RA, Lara-Jacobo LR, Chavez-Santoscoy AV, Gonzalez-Cobian LN. Daily consumption of chocolate rich in flavonoids decreases cellular genotoxicity and improves biochemical parameters of lipid and glucose metabolism. Molecules. (2018) 23:2220. doi: 10.20944/preprints201807.0399.v1
42. Padilla-Camberos E, Barragan-Alvarez CP, Diaz-Martinez NE, Rathod V, Flores-Fernandez JM. Effects of agave fructans (agave tequilana weber var. azul) on body fat and serum lipids in obesity. Plant Foods Hum Nutr. (2018) 73:34–9. doi: 10.1007/s11130-018-0654-5
43. Hernandez-Corona DM, Martinez-Abundis E, Gonzalez-Ortiz M. Effect of fucoidan administration on insulin secretion and insulin resistance in overweight or obese adults. J Med Food. (2014) 17:830–2. doi: 10.1089/jmf.2013.0053
44. Martinez-Abundis E, Gonzalez-Ortiz M, Mercado-Sesma AR. Reynoso-von-Drateln C, Moreno-Andrade A. Effect of avocado soybean unsaponifiables on insulin secretion and insulin sensitivity in patients with obesity. Obes Facts. (2013) 6:443–8. doi: 10.1159/000355720
45. Tovar AR, Caamano Mdel C, Garcia-Padilla S, Garcia OP, Duarte MA, Rosado JL. The inclusion of a partial meal replacement with or without inulin to a calorie restricted diet contributes to reach recommended intakes of micronutrients and decrease plasma triglycerides: a randomized clinical trial in obese Mexican women. Nutr J. (2012) 11:44. doi: 10.1186/1475-2891-11-44
46. Rosado JL, Garcia OP, Ronquillo D, Hervert-Hernandez D, Caamano Mdel C, Martinez G, et al. Intake of milk with added micronutrients increases the effectiveness of an energy-restricted diet to reduce body weight: a randomized controlled clinical trial in Mexican women. J Am Diet Assoc. (2011) 111:1507–16. doi: 10.1016/j.jada.2011.07.011
47. Hernandez-Gonzalez SO, Gonzalez-Ortiz M, Martinez-Abundis E, Robles-Cervantes JA. Chitosan improves insulin sensitivity as determined by the euglycemic-hyperinsulinemic clamp technique in obese subjects. Nutr Res. (2010) 30:392–5. doi: 10.1016/j.nutres.2010.06.005
48. Ble-Castillo JL, Aparicio-Trapala MA, Francisco-Luria MU, Cordova-Uscanga R, Rodriguez-Hernandez A, Mendez JD, et al. Effects of native banana starch supplementation on body weight and insulin sensitivity in obese type 2 diabetics. Int J Environ Res Public Health. (2010) 7:1953–62. doi: 10.3390/ijerph7051953
49. Gomez-Garcia A, Hernandez-Salazar E, Gonzalez-Ortiz M, Martinez-Abundis E. [Effect of oral zinc administration on insulin sensitivity, leptin and androgens in obese males]. Rev Med Chil. (2006) 134:279–84. doi: 10.4067/S0034-98872006000300002
50. Campos-Nonato I, Hernandez L, Barquera S. Effect of a high-protein diet versus standard-protein diet on weight loss and biomarkers of metabolic syndrome: a randomized clinical trial. Obes Facts. (2017) 10:238–51. doi: 10.1159/000471485
51. de Jesus Romero-Prado MM, Curiel-Beltran JA, Miramontes-Espino MV, Cardona-Munoz EG, Rios-Arellano A, Balam-Salazar LB. Dietary flavonoids added to pharmacological antihypertensive therapy are effective in improving blood pressure. Basic Clin Pharmacol Toxicol. (2015) 117:57–64. doi: 10.1111/bcpt.12360
52. Rodriguez-Hernandez H, Cervantes-Huerta M, Rodriguez-Moran M, Guerrero-Romero F. Decrease of aminotransferase levels in obese women is related to body weight reduction, irrespective of type of diet. Ann Hepatol. (2011) 10:486–92. doi: 10.1016/S1665-2681(19)31517-0
53. Madero M, Arriaga JC, Jalal D, Rivard C, McFann K, Perez-Mendez O, et al. The effect of two energy-restricted diets, a low-fructose diet versus a moderate natural fructose diet, on weight loss and metabolic syndrome parameters: a randomized controlled trial. Metabolism. (2011) 60:1551–9. doi: 10.1016/j.metabol.2011.04.001
54. Perichart-Perera O, Balas-Nakash M, Munoz-Manrique C, Legorreta-Legorreta J, Rodriguez-Cano A, Mier-Cabrera J, et al. Structured hypocaloric diet is more effective than behavioral therapy in reducing metabolic syndrome in Mexican postmenopausal women: a randomized controlled trial. Menopause. (2014) 21:711–20. doi: 10.1097/GME.0000000000000160
55. Macias-Cervantes MH, Rodriguez-Soto JM, Uribarri J, Diaz-Cisneros FJ, Cai W, Garay-Sevilla ME. Effect of an advanced glycation end product-restricted diet and exercise on metabolic parameters in adult overweight men. Nutrition. (2015) 31:446–51. doi: 10.1016/j.nut.2014.10.004
56. Rodriguez-Hernandez H, Morales-Amaya UA, Rosales-Valdez R, Rivera-Hinojosa F, Rodriguez-Moran M, Guerrero-Romero F. Adding cognitive behavioural treatment to either low-carbohydrate or low-fat diets: differential short-term effects. Br J Nutr. (2009) 102:1847–53. doi: 10.1017/S0007114509991231
57. Moran S, Uribe M, Prado ME, de la Mora G, Munoz RM, Perez MF, et al. [Effects of fiber administration in the prevention of gallstones in obese patients on a reducing diet A clinical trial]. Rev Gastroenterol Mex. (1997) 62:266–72.
58. Garcia-Vivas JM, Galaviz-Hernandez C, Becerril-Chavez F, Lozano-Rodriguez F, Zamorano-Carrillo A, Lopez-Camarillo C, et al. Acupoint catgut embedding therapy with moxibustion reduces the risk of diabetes in obese women. J Res Med Sci. (2014) 19:610–6.
59. Hernandez-Lepe MA, Wall-Medrano A, Lopez-Diaz JA, Juarez-Oropeza MA, Hernandez-Torres RP, Ramos-Jimenez A. Hypolipidemic effect of arthrospira (spirulina) maxima supplementation and a systematic physical exercise program in overweight and obese men: a double-blind, randomized, and crossover controlled trial. Mar Drugs. (2019) 17:250. doi: 10.3390/md17050270
60. Alvarado-Reynoso B, Ambriz-Tututi M. Effects of repetitive transcranial magnetic stimulation in combination with a low-carbohydrate diet in overweight or obese patients. A randomized controlled trial. Obes Med. (2019) 14:100095. doi: 10.1016/j.obmed.2019.100095
61. Arceo-Olaiz R, Espana-Gomez MN, Montalvo-Hernandez J, Velazquez-Fernandez D, Pantoja JP, Herrera MF. Maximal weight loss after banded and unbanded laparoscopic Roux-en-Y gastric bypass: a randomized controlled trial. Surg Obes Relat Dis. (2008) 4:507–11. doi: 10.1016/j.soard.2007.11.006
62. Robles-Cervantes JA, Martinez-Abundis E, Gonzalez-Ortiz M, Cardenas-Camarena L, Hernandez-Salazar E, Olvera-Ozuna R. Behavior of insulin sensitivity and its relation to leptin and tumor necrosis factor-alpha in obese women undergoing liposuction: 6-month follow-up. Obes Surg. (2007) 17:1242–7. doi: 10.1007/s11695-007-9213-0
63. Hernandez-Cordero S, Barquera S, Rodriguez-Ramirez S, Villanueva-Borbolla MA, Gonzalez de, Cossio T, Dommarco JR, et al. Substituting water for sugar-sweetened beverages reduces circulating triglycerides and the prevalence of metabolic syndrome in obese but not in overweight Mexican women in a randomized controlled trial. J Nutr. (2014) 144:1742–52. doi: 10.3945/jn.114.193490
64. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. (1996) 17:1–12. doi: 10.1016/0197-2456(95)00134-4
65. Cantrell L. Redotex(R) revisited: intentional overdose with an illegal weight loss product. J Emerg Med. (2012) 43:e147–8. doi: 10.1016/j.jemermed.2011.07.023
66. Whelton PK, Appel L, Charleston J, Dalcin AT, Ewart C, Fried L, et al. The effects of nonpharmacologic interventions on blood pressure of persons with high normal levels. Results of the trials of hypertension prevention, phase I. JAMA. (1992) 267:1213–20. doi: 10.1001/jama.267.9.1213
67. Loya JC. Systematic review of physical activity interventions in hispanic adults. Hisp Health Care Int. (2018) 16:174–88. doi: 10.1177/1540415318809427
68. Brown SA, Garcia AA, Kouzekanani K, Hanis CL. Culturally competent diabetes self-management education for Mexican Americans: the starr county border health initiative. Diabetes Care. (2002) 25:259–68. doi: 10.2337/diacare.25.2.259
70. Curfman GD, Morrissey S, Drazen JM. Sibutramine–another flawed diet pill. N Engl J Med. (2010) 363:972–4. doi: 10.1056/NEJMe1007993
71. Peterli R, Wolnerhanssen BK, Peters T, Vetter D, Kroll D, Borbely Y, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic roux-en-y gastric bypass on weight loss in patients with morbid obesity: the SM-BOSS randomized clinical trial. JAMA. (2018) 319:255–65. doi: 10.1001/jama.2017.20897
72. Buchwald H, Buchwald JN, McGlennon TW. Systematic review and meta-analysis of medium-term outcomes after banded Roux-en-Y gastric bypass. Obes Surg. (2014) 24:1536–51. doi: 10.1007/s11695-014-1311-1
73. Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. (2017) 376:1492. doi: 10.1056/NEJMc1701944
74. Stanford FC, Alfaris N, Gomez G, Ricks ET, Shukla AP, Corey KE, et al. The utility of weight loss medications after bariatric surgery for weight regain or inadequate weight loss: a multi-center study. Surg Obes Relat Dis. (2017) 13:491–500. doi: 10.1016/j.soard.2016.10.018
75. Zarate X, Arceo-Olaiz R, Montalvo Hernandez J, Garcia-Garcia E, Pablo Pantoja J, Herrera MF. Long-term results of a randomized trial comparing banded versus standard laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. (2013) 9:395–7. doi: 10.1016/j.soard.2012.09.009
76. Manzanares-Rivera JL. Mortalidad por diabetes tipo 2 en las fronteras de Mexico. Población y Salud en Mesoamérica. (2017) 14:1–19. doi: 10.15517/psm.v14i2.27028
77. Promotion OoDPaH. Overweight and Obesity. (2020). Available online at: https://health.gov/healthypeople/objectives-and-data/browse-objectives/overweight-and-obesity (accessed January 11, 2021).
78. United States Environmental Protection Agency. What Is Border 2020? (2020). Available online at: https://www.epa.gov/usmexicoborder/what-border-2020 (accessed September 1–January 4 2020–2021).
79. U.S. Department of Health & Human Services. U.S.-Mexico Border Health Commission. (2020). Available online at: https://www.hhs.gov/about/agencies/oga/about-oga/what-we-do/international-relations-division/americas/border-health-commission/index.html
Keywords: anti-obesity agents, abdominal obesity metabolic syndrome, systematic review and meta-analysis, randomized clinical trials, type 2 diabetes
Citation: Garcia-Oropesa EM, Martinez-Lopez YE, Ruiz-Cejudo SM, Martínez-Ezquerro JD, Diaz-Badillo A, Ramirez-Pfeiffer C, Bustamante-Fuentes A, Lopez-Sosa EB, Moctezuma-Chavez OO, Nava-Gonzalez EJ, Perales-Torres AL, Perez-Navarro LM, Rosas-Diaz M, Carter K, Tapia B and Lopez-Alvarenga JC (2021) Looking for Crumbs in the Obesity Forest: Anti-obesity Interventions and Obesity-Associated Cardiometabolic Traits in the Mexican Population. History and Systematic Review With Meta-Analyses. Front. Med. 8:665023. doi: 10.3389/fmed.2021.665023
Received: 06 February 2021; Accepted: 24 September 2021;
Published: 03 November 2021.
Edited by:
Belinda Reininger, University of Texas Health Science Center at Houston, United StatesReviewed by:
Nicolas Musi, The University of Texas Health Science Center at San Antonio, United StatesCopyright © 2021 Garcia-Oropesa, Martinez-Lopez, Ruiz-Cejudo, Martínez-Ezquerro, Diaz-Badillo, Ramirez-Pfeiffer, Bustamante-Fuentes, Lopez-Sosa, Moctezuma-Chavez, Nava-Gonzalez, Perales-Torres, Perez-Navarro, Rosas-Diaz, Carter, Tapia and Lopez-Alvarenga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan C. Lopez-Alvarenga, anVhbi5sb3BlemFsdmFyZW5nYUB1dHJndi5lZHU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.