
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Med. , 25 May 2021
Sec. Geriatric Medicine
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.664681
This article is part of the Research Topic COVID-19, Aging, and Public Health View all 41 articles
 Davide Angioni1,2*†
Davide Angioni1,2*† Camille Nicolay1†
Camille Nicolay1† Frédéric Vandergheynst3Robin Baré1
Frédéric Vandergheynst3Robin Baré1 Matteo Cesari4
Matteo Cesari4 Sandra De Breucker1
Sandra De Breucker1In the autumn of 2020, the second wave of the COVID-19 pandemic hit Europe. In this context, because of the insufficient number of beds in geriatric COVID units, non-geriatric wards were confronted with a significant number of admissions of geriatric patients. In this perspective article, we describe the role of a mobile geriatric team in the framework of the COVID-19 pandemic and specifically how it assisted other specialists in the management of hospitalized geriatric patients by implementing a new approach: the systematic assessment and optimization of Intrinsic Capacity functions. For each patient, assessed by this consultative team, an individualized care plan, including an anticipated end-of-life decision-making process, was established. Intensity of care was most often not stated by considering chronological age but rather the comorbidity burden, the frailty status, and the patient's wishes. Further studies are needed to determine if this mobile geriatric team approach was beneficial in terms of mortality, length of stay, or functional, psychological, and cognitive outcomes in COVID-19 geriatric patients.
In the early autumn of 2020, the second wave of the COVID-19 pandemic hit Europe and the number of hospitalizations rapidly increased in several European countries (1). In October 2020, with about 8,500 new cases per day (considering symptomatic as well as asymptomatic patients) for a population of 11 million inhabitants1, Belgium neared a “coronavirus tsunami.” Age is one of the most critical risk factors for infection and negative outcomes of SARS-CoV-2 (2, 3), thus characterizing a “gero-pandemic” (4). Due to the lack of available geriatric COVID beds, non-geriatric wards were faced with countless hospitalizations of patients with a geriatric profile.
Geriatric patients present specific characteristics like comorbidity, polypharmacy, and physical frailty, making their management challenging for healthcare providers without geriatric training (5, 6). In order to capture the composite of older adult functions in a holistic way, the concept of intrinsic capacity (IC) was introduced in 2015 by the World Health Organization (7). Intrinsic capacity is defined as the composite of all the physical and mental capacities of an individual. Five domains are targeted: cognition, mobility, vitality, mood, and sensory domain (8).
The mobile geriatric team (MGT), initially described in the early eighties and later implemented in several countries, is a consultative team aimed to offer a multidisciplinary geriatric approach to older patients with a geriatric profile admitted in non-geriatric wards. The MGT, referred also in the literature as an inpatient geriatric consultation team or geriatric liaison team, is composed of nurses, occupational therapists, psychologists, speech therapists, dietitians, social workers, and physiotherapists, coordinated by one or more geriatricians (9). The early intervention of an MGT was shown to reduce the length of stay of geriatric inpatients (10) and was associated with a lower mortality rate and less functional decline after hospital discharge (11–13).
In this perspective article, we describe the role of a mobile geriatric team in the context of the emergency situation of the COVID-19 pandemic and specifically how it assisted other specialists in the management of geriatric patients by implementing a new approach: the systematic assessment and optimization of intrinsic capacity functions.
The MGT aimed to systematically assess and optimize intrinsic capacity and support non-geriatrician physicians in implementing an individualized care plan during hospitalization and after hospital discharge (Figure 1). For each patient over 74 years old hospitalized for COVID-19 infection, an alert was generated and managed by the mobile geriatric team nurse coordinator (Figure 1). Because geriatric age is set in Belgium at 75 years old by the Royal Decree defining the standards of geriatric care program and its components, MGT assessed only patients aged 75 years old or older (14).
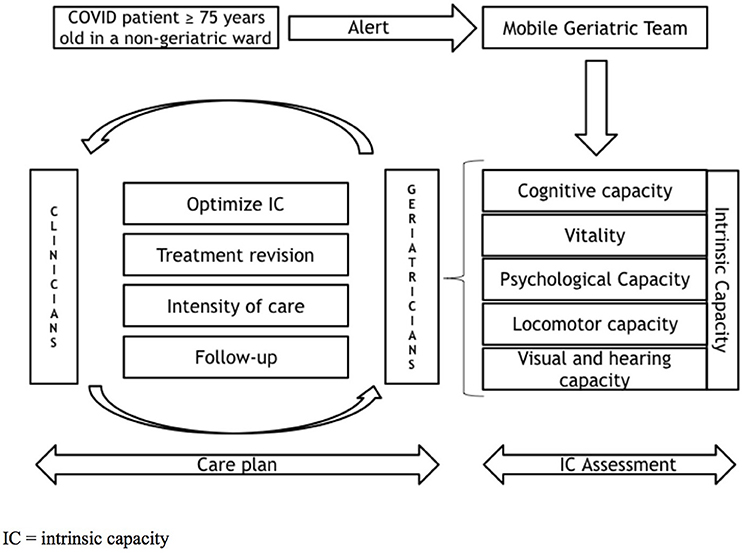
Figure 1. MGT management.
According to the institutional COVID-19 registry, 557 patients with COVID-19 were hospitalized between October 1st and December 4th, in a non-intensive care unit of our academic hospital of 850 beds, the Erasmus Hospital. The mean age was 66.2 (±11.7) years. Two hundred and two patients were 75 years old or more, and among them, 105 (52%) were hospitalized in COVID geriatric units, while 97 (48%) were oriented to COVID medical and surgical non-geriatric units. Among the patients hospitalized in non-geriatric wards, 49 (51%) were assessed by the MGT.
Forty-eight patients (49%) did not benefit from the mobile geriatric team assessment due to the severity of their clinical status (e.g., hemodynamic instability or respiratory distress, end-of-life status, or not able to answer the questions) or because the patient refused the geriatric assessment. Data were extracted from the “COVID-19 Seniors Registry,” the registry of patients aged 75 years old or older hospitalized for COVID-19 infection in our hospital. The local ethics committee (Comité d'Ethique Hospitalo-Facultaire Erasme-ULB) approved this project on June 25, 2020, under the reference number SRB2020/209—P2020/320.
The World Health Organization (WHO) published a handbook guidance called the Integrated Care for Older People (ICOPE), whose ambition is to reduce the number of dependent people in the next decades (15). The objective is to promote healthy aging by optimizing intrinsic capacity functions. In order to achieve this goal, ICOPE proposes a program consisting in five actions called steps: the screening of intrinsic capacity decline, the complete assessment of intrinsic capacity functions, the implementation of a personalized care plan, the monitoring of the care plan, and the integration of the caregivers and the community (16). The importance of assessing intrinsic capacity in the context of COVID-19 has been previously discussed and is justified by the strong impact of COVID-19 infection on the key functions of the aging population (17). The present MGT model was inspired by steps 1 (screening of IC decline) and 2 (complete assessment of IC functions) of ICOPE recommendations (Table 1).
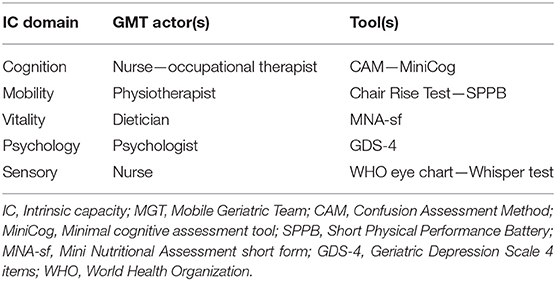
Table 1. Intrinsic capacity assessment by domain.
At the beginning of hospitalization, IC assessment was performed by the different actors of the mobile geriatric team. Every actor discussed his/her workup with the geriatrician, who thereafter delivered MGT recommendations to the clinicians and nurses in charge of the patients orally and by a written note in the patient medical file (accessed by all the members of medical and paramedical team in charge of the patients). During the stay, the MGT continued to follow the patients, the frequency of their interventions varying according to the domain and the clinical situation. During this phase, the MGT actors monitored the evolution, adapted the recommendations proposed, and referred to geriatricians if they considered that a medical advice was needed (e.g., patient who presented a significant weight loss were considered to benefit from a parenteral nutrition). Patients assessed by the MGT were systematically weekly discussed.
Delirium is a common condition in older adults admitted for COVID-19 (18) and is associated with high in-hospital mortality (19). Moreover, COVID-19 has been associated with short-term cognitive decline (20). The assessment of cognitive domains focused on the screening and treatment of delirium and a short cognitive assessment. Recommendations to prevent or manage delirium were proposed to clinicians and nurses in charge of the patient from the day of assessment. An occupational therapist assessed autonomy status (upon admission, during hospitalization, and before hospital discharge) and asked the relatives about previous problems of memory, orientation, speech, language, or any difficulties with performing basic and instrumental daily activities.
Prolonged bed rest has been associated with poor outcomes in older adults hospitalized for infections (21). Frail patients have better outcomes if they receive exercise therapy during hospitalization (22). High inflammatory and hypercatabolic status owing to COVID-19 infection and bed rest lead to an important reduction of functional performances. This may compromise the recovery of functional capacities and induce loss of autonomy. There is evidence that patients with severe COVID-19 need prolonged exercise therapy to prevent or reverse disability (23). Physical therapists assessed mobility upon admission and proposed in-room individualized programs of exercises using an information leaflet for the patients. Thereafter, the physical therapist followed or adapted this program daily during the stay.
COVID-19 patients present a high risk of malnutrition (24) and sarcopenia (25). A poor nutritional status could contribute to increasing the risk of clinical complications (2). According to the current recommendations, all patients were assessed by a dietician upon admission to choose the best nutritional pathway strategy, which was regularly reassessed during hospitalization. If swallowing disorders were suspected, a speech therapist was consulted.
During hospitalization, because of distancing with relatives, room isolation, and visiting ban, older people with COVID-19 fell often abandoned, fearful, and sometimes unable to understand the situation. This contributes to the onset of anxiety and depressive disorders (26, 27). If long-term psychological consequences are still unknown, anxiety, and depressive disorders have been associated with a significant cognitive decline risk (20). For patients able to communicate, a psychological support was provided during hospitalization, and video calls with relatives were organized every day (28).
Vision and hearing impairments are common in older adults and have been associated with an increased risk of delirium and higher mortality during hospitalization (29, 30). Furthermore, during the pandemic, the wearing of masks, visors, and social distancing were major obstacles to communication between patients and healthcare providers. In this context, it was recommended to nurses that patients wore hearing devices and glasses as indicated as possible, and to speak them slowly and clearly.
Geriatricians of the MGT discussed with clinicians about an individualized care plan, taking care not to modify or substitute the routine management of COVID-19 infection, but rather to counsel how to optimize intrinsic capacity as discussed previously, but also how to review medical treatment, define the intensity of care, and organize follow-up (Figure 1). During the COVID-19 pandemic, given the limited number of intensive care beds, a major challenge for healthcare providers was to identify patients who would be the most likely to benefit from intensive care. According to a national survey led by the Belgian Society of Gerontology and Geriatrics in June 2020, one of the most difficult issues for the physicians was the feeling of loneliness while having to make decisions around the intensity of care and the sense of powerlessness in front of a high mortality rate2. Although it is known that mortality rate due to COVID-19 increases with age (31), several studies found that chronological age alone is not a good predictor of COVID-19 lethality in individuals without comorbidities or robust (32, 33). Indeed, chronological age alone does not directly reflect the homeostastic and homeodynamic changes making an individual more susceptible to a poor COVID-19 prognosis (34). Geriatricians frequently discussed with clinicians about reasonable limitations of the therapeutic efforts when needed, or at the contrary, to consider ICU admission for older patients with higher resilience. The decision-making was based on the individual's frailty status, comorbidity, and opinions and wishes rather than chronological age per se. Frailty status was assessed by the Clinical Frailty Scale (35), as proposed by different geriatric societies (36–38). Considering comorbidity burden, geriatricians focused on pathologies and geriatric syndromes that have been associated with a poor prognosis in the context of COVID-19, like dementia, type 2 diabetes, or chronic obstructive pulmonary disease (39). Patients able to communicate and understand the situation were questioned on the intensity of care they wished. When this was not possible, geriatricians enquired about existing advanced directives or patients' wishes by discussing with patients' relatives and their general practitioner.
Due to lockdown restrictions, access to ambulatory care was limited to urgent situations (40). Likewise, for COVID-19 patients admitted in healthcare facilities, hospitalization time was almost exclusively allocated to the treatment of COVID-19 infection. For this reason, chronic diseases and new incident diseases were often not optimally managed or were neglected. In this context, a post-discharge plan was proposed, including consultations in geriatric day hospital and/or referral to other specialists. Persons who have severe COVID-19 infection might take several months to return to normal mobility (41). With this in mind, after a careful reviewing of patients' mobility capacity, MGT considered a transfer to a rehabilitation unit at discharge or a home-based individual physical exercise program.
During the second wave of the COVID-19 pandemic, the admission of geriatric patients in non-geriatric units was widespread and therefore particularly challenging for healthcare providers without geriatric training. In this perspective paper, we proposed the first description of a new approach based on the systematic screening of IC functions by a multidisciplinary mobile geriatric team in a hospital setting. Although we presented a single-center experience, the implementation of this model may promote multidisciplinary management of older adults in non-geriatrics wards and solicit attention to often neglected (but critical) aspects of the individual's health status. By raising awareness about the key functions of the persons, it is possible to obtain a comprehensive assessment of the health status and design adequate interventions for potentially preventing or reversing functional decline, even in emergency situations as the COVID-19 pandemic. Ethical decision-making is a stressful skill task in medical practice and was even more difficult during the COVID-19 crisis. The decision-making process was based on the individual's frailty status, comorbidity burden, and patient's wishes and priorities. The COVID-19 pandemic highlighted the need for markers of resilience capacity in clinical practice. In the future, these markers could be integrated into ethical decision-making algorithms. Further studies are needed to establish if, during the COVID-19 pandemic, a geriatric assessment was beneficial in terms of length of stay and functional, psychological, and cognitive outcomes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité d'Ethique Hospitalo-Facultaire Erasme-ULB. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
DA and CN conceived the project, drafted the article. RB was responsible for data extraction and analysis. FV was involved in the critical appraisal of the manuscript. MC modified the article with important intellectual content. SD conceived the project, drafted the article, was involved in the critical appraisal of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank Thierry Honorez, Najat Benhadi, Marina Tuganova (permanent members of the Geriatric Mobile Team), and Professor Olivier Le Moine (data manager).
COVID, Coronavirus disease; MGT, mobile geriatric team; IC, intrinsic capacity; ICOPE, Integrated Care for Older PEople.
1. ^Available online at: https://covid-19.sciensano.be/fr/covid-19-situation-epidemiologique (accessed December 12, 2019).
2. ^Available online at: https://geriatrie.be/media/2020/10/8.DeBreucker-S-Enquete-COVID-en-geriatrie.pdf (accessed December 12, 2019).
1. Looi MK. Covid-19: is a second wave hitting Europe? BMJ. (2020) 371:m4113. doi: 10.1136/bmj.m4113
2. Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect. (2020) 80:e14–e8. doi: 10.1016/j.jinf.2020.03.005
3. Garg S, Kim L, Whitaker M, O'Halloran A, Cummings C, Holstein R, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 - COVID-NET, 14 States, March 1-30, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:458–64. doi: 10.15585/mmwr.mm6915e3
4. Wister A, Speechley M. COVID-19: pandemic risk, resilience and possibilities for aging research. Can J Aging. (2020) 39:344–7. doi: 10.1017/S0714980820000215
5. Astrone P, Cesari M. Integrated care and geriatrics: a call to renovation from the COVID-19 pandemic. J Frailty Aging. (2021) 10:182–3. doi: 10.14283/jfa.2020.59
6. Cesari M, Proietti M. Geriatric medicine in Italy in the time of COVID-19. J Nutr Health Aging. (2020) 24:459–60. doi: 10.1007/s12603-020-1354-z
7. Belloni G, Cesari M. Frailty and intrinsic capacity: two distinct but related constructs. Front Med (Lausanne). (2019) 6:133. doi: 10.3389/fmed.2019.00133
8. Cesari M, Araujo de Carvalho I, Amuthavalli Thiyagarajan J, Cooper C, Martin FC, Reginster JY, et al. Evidence for the domains supporting the construct of intrinsic capacity. J Gerontol A Biol Sci Med Sci. (2018) 73:1653–60. doi: 10.1093/gerona/gly011
9. Campion EW, Jette A, Berkman B. An interdisciplinary geriatric consultation service: a controlled trial. J Am Gériatrie Soc. (1983) 31:792–96. doi: 10.1111/j.1532-5415.1983.tb03401.x
10. Launay CP, Annweiler C, Delanoe-Telfour L, de Decker L, Kabeshova A, Beauchet O. Mobile geriatric team advice: effect on length of hospital stay in older adults. J Am Geriatr Soc. (2014) 62:390–1. doi: 10.1111/jgs.12677
11. Deschodt M, Flamaing J, Haentjens P, Boonen S, Milisen K. Impact of geriatric consultation teams on clinical outcome in acute hospitals: a systematic review and meta-analysis. BMC Med. (2013) 11:48. doi: 10.1186/1741-7015-11-48
12. Ellis G, Whitehead MA, O'Neill D, Langhorne P, Robinson D. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. (2011) 7:CD006211. doi: 10.1002/14651858.CD006211.pub2
13. Stuck AE, Siu AL, Wieland GD, Adams J, Rubenstein LZ. Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet. (1993) 342:1032–6. doi: 10.1016/0140-6736(93)92884-V
14. Braes T, Flamaing J, Pelemans W, Milisen K. Geriatrics on the run: rationale, implementation, and preliminary findings of a Belgian internal liaison team. Acta Clin Belg. (2009) 64:384–92. doi: 10.1179/acb.2009.064
15. WHO ICOPE Handbook App. Apps on Google Play. Available online at: https://play.google.com/store/apps/details?id=com.universaltools.icope&hl=en (accessed January 10, 2021).
16. Takeda C, Guyonnet S, Sumi Y, Vellas B, Araujo de Carvalho I. Integrated care for older people and the implementation in the INSPIRE care cohort. J Prev Alzheimers Dis. (2020) 7:70–4. doi: 10.14283/jpad.2020.8
17. Nestola T, Orlandini L, Beard JR, Cesari M. COVID-19 and intrinsic capacity. J Nutr Health Aging. (2020) 24:692–5. doi: 10.1007/s12603-020-1397-1
18. O'Hanlon S, Inouye SK. Delirium: a missing piece in the COVID-19 pandemic puzzle. Age Ageing. (2020) 49:497–8. doi: 10.1093/ageing/afaa094
19. Marengoni A, Zucchelli A, Grande G, Fratiglioni L, Rizzuto D. The impact of delirium on outcomes for older adults hospitalised with COVID-19. Age Ageing. (2020) 49:923–6. doi: 10.1093/ageing/afaa189
20. Almeria M, Cejudo JC, Sotoca J, Deus J, Krupinski J. Cognitive profile following COVID-19 infection: Clinical predictors leading to neuropsychological impairment. Brain Behav Immun Health. (2020) 9:100163. doi: 10.1016/j.bbih.2020.100163
21. Angioni D, Hites M, Jacobs F, De Breucker S. Predictive factors of in-hospital mortality in older adults with community-acquired bloodstream infection. J Frailty Aging. (2020) 9:232–7. doi: 10.14283/jfa.2019.45
22. Izquierdo M, Morley JE, Lucia A. Exercise in people over 85. BMJ. (2020) 368:m402. doi: 10.1136/bmj.m402
23. Li J. Effect and enlightenment of rehabilitation medicine in COVID-19 management. Eur J Phys Rehabil Med. (2020). doi: 10.4103/jisprm.jisprm_5_20
24. Azzolino D, Saporiti E, Proietti M, Cesari M. Nutritional considerations in frail older patients with COVID-19. J Nutr Health Aging. (2020) 24:696–8. doi: 10.1007/s12603-020-1400-x
25. Morley JE, Kalantar-Zadeh K, Anker SD. COVID-19: a major cause of cachexia and sarcopenia? J Cachexia Sarcopenia Muscle. (2020) 11:863–5. doi: 10.1002/jcsm.12589
26. Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, Ganz F, Torralba R, Oliveira DV, et al. Impact of social isolation due to COVID-19 on health in older people: mental and physical effects and recommendations. J Nutr Health Aging. (2020) 24:938–47. doi: 10.1007/s12603-020-1500-7
27. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
28. Tsai HH, Cheng CY, Shieh WY, Chang YC. Effects of a smartphone-based videoconferencing program for older nursing home residents on depression, loneliness, and quality of life: a quasi-experimental study. BMC Geriatr. (2020) 20:27. doi: 10.1186/S12877-020-1426-2
29. Ahmed S, Leurent B, Sampson EL. Risk factors for incident delirium among older people in acute hospital medical units: a systematic review and meta-analysis. Age Ageing. (2014) 43:326–3. doi: 10.1093/ageing/afu022
30. Zhang Y, Ge M, Zhao W, Liu Y, Xia X, Hou L, et al. Sensory impairment and all-cause mortality among the oldest-old: findings from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). J Nutr Health Aging. (2020) 24:132–7. doi: 10.1007/s12603-020-1319-2
31. Bonanad C, García-Blas S, Tarazona-Santabalbina F, Sanchis J, Bertomeu-González V, Fácila L, et al. The effect of age on mortality in patients with COVID-19: a meta-analysis with 611,583 subjects. J Am Med Dir Assoc. (2020) 21:915–8. doi: 10.1016/j.jamda.2020.05.045
32. Bello-Chavolla OY, González-Díaz A, Antonio-Villa NE, Fermín-Martínez CA, Márquez-Salinas A, Vargas-Vázquez A, et al. Unequal impact of structural health determinants and comorbidity on COVID-19 severity and lethality in older Mexican adults: considerations beyond chronological aging. J Gerontol A Biol Sci Med Sci. (2020) 76:e52–9. doi: 10.1101/2020.05.12.20098699
33. Marengoni A, Zucchelli A, Vetrano DL, Armellini A, Botteri E, Nicosia F, et al. Beyond chronological age: frailty and multimorbidity predict in-hospital mortality in patients with coronavirus disease 2019. J Gerontol A Biol Sci Med Sci. (2021) 76:e38–e45. doi: 10.1093/gerona/glaa291
34. Vellas C, Delobel P, de Souto Barreto P, Izopet J. COVID-19, virology and geroscience: a perspective. J Nutr Health Aging. (2020) 24:685–91. doi: 10.1007/s12603-020-1416-2
35. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1037/t19726-000
36. COVID-19 Rapid Guideline: Critical Care in Adults; NICE Guideline [NG159] (2020). Available online at: https://www.nice.org.uk/guidance/ng159/chapter/1-Admission-to-hospital (accessed December 20, 2020).
37. Montero-Odasso M, Hogan DB, Lam R, Madden K, MacKnight C, Molnar F, et al. Age alone is not adequate to determine health-care resource allocation during the COVID-19 pandemic. Can Geriatr J. (2020) 23:152–4. doi: 10.5770/cgj.23.452
38. Japan Geriatrics Society Subcommittee on End-of-Life Issues New Coronavirus Coun-termeasure Team, Kuzuya M, Aita K, Katayama Y, Katsuya T, Nishikawa M. The Japan Geriatrics Society consensus statement “recommendations for older persons to receive the best medical and long-term care during the COVID-19 outbreak-considering the timing of advance care planning implementation.” Geriatr Gerontol Int. (2020) 20:1112–9. doi: 10.1111/ggi.14075
39. Atkins JL, Masoli JAH, Delgado J, Pilling LC, Kuo CL, Kuchel GA, et al. Preexisting comorbidities predicting COVID-19 and mortality in the UK Biobank community Co-HORT. J Gerontol A Biol Sci Med Sci. (2020) 75:2224–30. doi: 10.1093/gerona/glaa183
40. Takeda C, Guyonnet S, Ousset PJ, Soto M, Vellas B. Toulouse Alzheimer's clinical research center recovery after the COVID-19 crisis: telemedicine an innovative solution for clinical research during the coronavirus pandemic. J Prev Alzheimers Dis. (2020) 7:301–4. doi: 10.14283/jpad.2020.32
Keywords: COVID-19, older adults, intrinsic capacity, decision-making, mobile geriatric team
Citation: Angioni D, Nicolay C, Vandergheynst F, Baré R, Cesari M and De Breucker S (2021) Intrinsic Capacity Assessment by a Mobile Geriatric Team During the Covid-19 Pandemic. Front. Med. 8:664681. doi: 10.3389/fmed.2021.664681
Received: 05 February 2021; Accepted: 12 April 2021;
Published: 25 May 2021.
Edited by:
Tzvi Dwolatzky, Technion Israel Institute of Technology, IsraelReviewed by:
Marios Kyriazis, National Gerontology Centre, CyprusCopyright © 2021 Angioni, Nicolay, Vandergheynst, Baré, Cesari and De Breucker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Davide Angioni, ZGF2aWRlYW5naW9uaTJAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.