
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 15 June 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.657977
This article is part of the Research Topic Coronavirus Disease (COVID-19): Pathophysiology, Epidemiology, Clinical Management and Public Health Response, Volume II View all 165 articles
 Eduardo Gutiérrez-Abejón1,2*†
Eduardo Gutiérrez-Abejón1,2*† Débora Martín-García3†Eduardo Tamayo4,5,6
Débora Martín-García3†Eduardo Tamayo4,5,6 F. Javier Álvarez1,4,7‡Francisco Herrera-Gómez1,4,8,9‡
F. Javier Álvarez1,4,7‡Francisco Herrera-Gómez1,4,8,9‡Introduction: One of the worst clinical outcomes of the coronavirus disease 2019 (COVID-19) pandemic was acute kidney injury (AKI).
Methods: This manuscript presents results from a population-based registry study assessing treatment, comorbidities, and predictors of hospital death among COVID-19 patients with AKI from March 1st to May 31th, 2020. Death, oxygen delivery and ventilation, acute dialysis need, use of medications, and various clinical outcomes, in addition to the length of stay in the hospital and intensive care unit (ICU), were evaluated.
Results: In Castile and Leon, the largest region of Spain, 10.87% of the patients admitted for COVID-19 (n = 7,307) developed AKI. These patients were known by having hypertension (57.93%), cardiovascular disease (48.99%), diabetes (26.7%) and chronic kidney disease (14.36%), and they used antibiotics (90.43%), antimalarials (60.45%), steroids (48.61%), antivirals (33.38%), anti-systemic inflammatory response syndrome (SIRS) drugs (9.45%), and tocilizumab (8.31%). Mortality among patients with AKI doubled that observed in patients without AKI (46.1 vs. 21.79%). Predictors of hospital death in COVID-19 patients with AKI were ventilation needs (OR = 5.9), treatment with steroids (OR = 1.7) or anti-SIRS (OR = 2.4), severe acute respiratory syndrome (SARS) occurrence (OR = 2.8), and SIRS occurrence (OR = 2.5).
Conclusions: Acute kidney injury is a frequent and serious complication among COVID-19 patients, with a very high mortality, that requires more attention by treating physicians, when prescribing medications, by looking for manifestations particular to the disease, such as SARS or SIRS.
Acute kidney injury (AKI) continues to affect between 10 and 40% of in-hospital coronavirus disease 2019 (COVID-19) patients (1–4). Since the beginning of the COVID-19 pandemic, mostly elderly individuals with many comorbidities have developed AKI and died (5, 6). The adaptation of mechanisms to the kidneys that respond to hemodynamic changes, inflammation, and other stress-inducing situations, perform worse in cases of previous kidney affectation, diabetes, heart failure, etc. Furthermore, in COVID-19 patients, systemic inflammatory response syndrome (SIRS) and severe acute respiratory syndrome (SARS) may exhaust kidney function capacities, leading to the appearance of AKI (4).
Acute kidney injury is a direct result of COVID-19 infection (7) and is common in critically ill patients, being one of the poor clinical outcomes with a negative prognosis for survival (4, 8).
In addition, AKI incidence and death rates are changing throughout the regions of world, probably in relation to the characteristics of the individuals in those regions. In this sense, we report our pharmacological, clinical, and epidemiological findings related to the in-hospital COVID-19 patients with AKI.
The main aim of this study was to describe the pharmacological treatment and the clinical baselines of the in-hospital COVID-19 patients affected by AKI (March 1st to May 31th, 2020), in Castile and Leon, the largest region of Spain. Furthermore, we have analyzed the risk factors associated with deaths of COVID-19 patients with AKI. Finally, the influence of AKI on the survival of the in-hospital COVID-19 patients was analyzed.
This article presents findings from an epidemiological analysis carried out following a population-based registry study design, with the collection of clinical and administrative data. The Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) recommendations (9) and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) standards (10) were adhered to. Ethics committee approval reference and date: PI 20-1863, June 11th, 2020.
This study evaluated cross-sectionally clinical findings, treatment, and outcomes from a population of COVID-19 patients with AKI. These study participants were selected from the total COVID-19 patient population with a recorded stay in public Castile and Leon hospitals between March 1st and May 31th, 2020. COVID-19 was diagnosed by in-hospital treating physicians who decided on hospitalizing the patients on the basis of clinical or radiological findings defining SARS (Supplementary Table 1). A positive result on the COVID-19 real-time reverse transcription polymerase chain reaction (rRT-PCR) test for qualitative detection of the nucleic acid from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was not required to formally diagnose the disease. SIRS was diagnosed following the proper criteria (Supplementary Table 1) (11).
Acute kidney injury was diagnosed in the hospital by treating physicians using the Kidney Disease Improving Global Outcomes (KDIGO) criteria (12) and, following these recommendations, by calculating glomerular filtration rate (GFR) with the Modification of Diet in Renal Disease (MDRD) study equation, or the Chronic Kidney Disease EPIdemiology Collaboration (CKD-EPI) equation (Supplementary Table 1): briefly, an increase in serum creatinine (SCr) by ≥0.3 mg/dL within 48 h or ≥1.5 times within the prior 7 days, in addition to an urine volume <0.5 ml/kg/h for 6 h, was required.
These patients may have chronic kidney disease (CKD), categories 3–5, defined by an estimated GFR of 60 ml/min or lower (13): the MDRD or CKD-EPI equations were used for following up the kidney function of patients with visits to Nephrology units, and the Cockcroft-Gault formula was used for patients with visits to primary healthcare centers depending on public Castile and Leon hospitals. Dialysis patients were excluded.
Cardiovascular disease was defined by the occurrence of major adverse cardiovascular events (MACE), which included all non-fatal coronary events, including revascularization procedures, and all cerebrovascular events, including transient ischemic attacks (TIA). Peripheral artery disease and decompensated heart failure (HF) were considered indicative of cardiovascular disease. Diabetes, hypertension, and other well-known cardiovascular risk factors were also considered.
Access to registries containing EHR information from the Castile and Leon hospitals and associated primary healthcare centers (Jimena and Medora, https://www.saludcastillayleon.es/sanidad/cm), hospital pharmaceutical care information in our region (Concylia, http://www.saludcastillayleon.es/portalmedicamento/es/indicadoresinformes/concylia) and hospital discharges information in Castile and Leon (Pestadistico, https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/N/rae-cmbd/rae-cmbd), was obtained.
The main outcome during the study period was death (March 1st to May 31th, 2020). Other outcomes were stays in the hospital and intensive care unit (ICU) (length in days), the need for acute dialysis, SARS, SIRS, disseminated intravascular coagulation (DIC), cardiomyopathy, and bacterial and fungal superinfection.
The use of medications to treat COVID-19 according to the Spanish national recommendations (14, 15) (Supplementary Table 2) during the study period (i.e., antibiotics, antimalarials, steroids, antivirals, tocilizumab, and other anti-SIRS), was assessed through dispensaries in public hospitals in Castile and Leon. Anatomical Therapeutic Chemical (ATC) classification was used to evaluate medication consumption (Supplementary Table 3). Data on the use of oxygen delivery using low-flow systems (nasal cannula and simple face masks) and high-flow systems (high-flow nasal cannula, venturi masks, and rebreather masks), non-invasive pressure positive ventilation (NIPPV), and invasive ventilation (IV), was also assessed.
Statistical analysis was carried out considering age and gender distributions and an age cut-off at 65 years of age. A 15-day period analysis was performed for all measurements and consideration of all clinical outcomes (March 1–14 to May 15–31, 2020). Frequencies (in percentages) and their corresponding 95% confidence intervals (95% CI) and means or medians with, respectively, their standard deviations (SD) or interquartile ranges (IQR), are presented, as appropriate.
Comparisons were performed using the Student t-test or the Mann-Whitney U-test (for continuous variables), after confirmation of normal distribution of data in a given variable (Kolmogorov-Smirnov-test), and using Pearson's chi-square-test or Fisher's exact-test (categorical variables).
Multiple logistic regression, with a forward selection approach, was performed for in-hospital COVID-19 patients with or without AKI, who died, as opposed to those who did not die. The odds ratio (OR) and a 95% CI were presented. The following variables were included in the analysis: age (>65 years), gender, comorbidities (hypertension, diabetes, cardiovascular disease, CKD), obesity (BMI ≥ 30 kg/m2), need for ventilation, acute dialysis need (only in patients developing AKI), medications used (antibiotics, antimalarials, steroids, antivirals, tocilizumab, or anti-SIRS), occurrence of SARS, SIRS, DIC, cardiomyopathy, and bacterial and fungal superinfections.
The survival of COVID-19 patients with and without AKI was performed using the Kaplan-Meier approach and the log-rank-test for comparison between groups.
The level of significance was set at p < 0.05. All statistical analyses were performed by using the Statistical Package for the Social Sciences (SPSS) software version 24.0. (SPSS Inc., Chicago, IL).
From a total population of 7,307 in-hospital COVID-19 patients for which data were available, the findings presented here describe 794 patients with AKI (10.87%), most of them males aged 65 years or more. Around half of the patients had hypertension or cardiovascular disease (Table 1). Many of these patients also had diabetes mellitus (26.7%) and CKD categories 3–5 (14.36%).
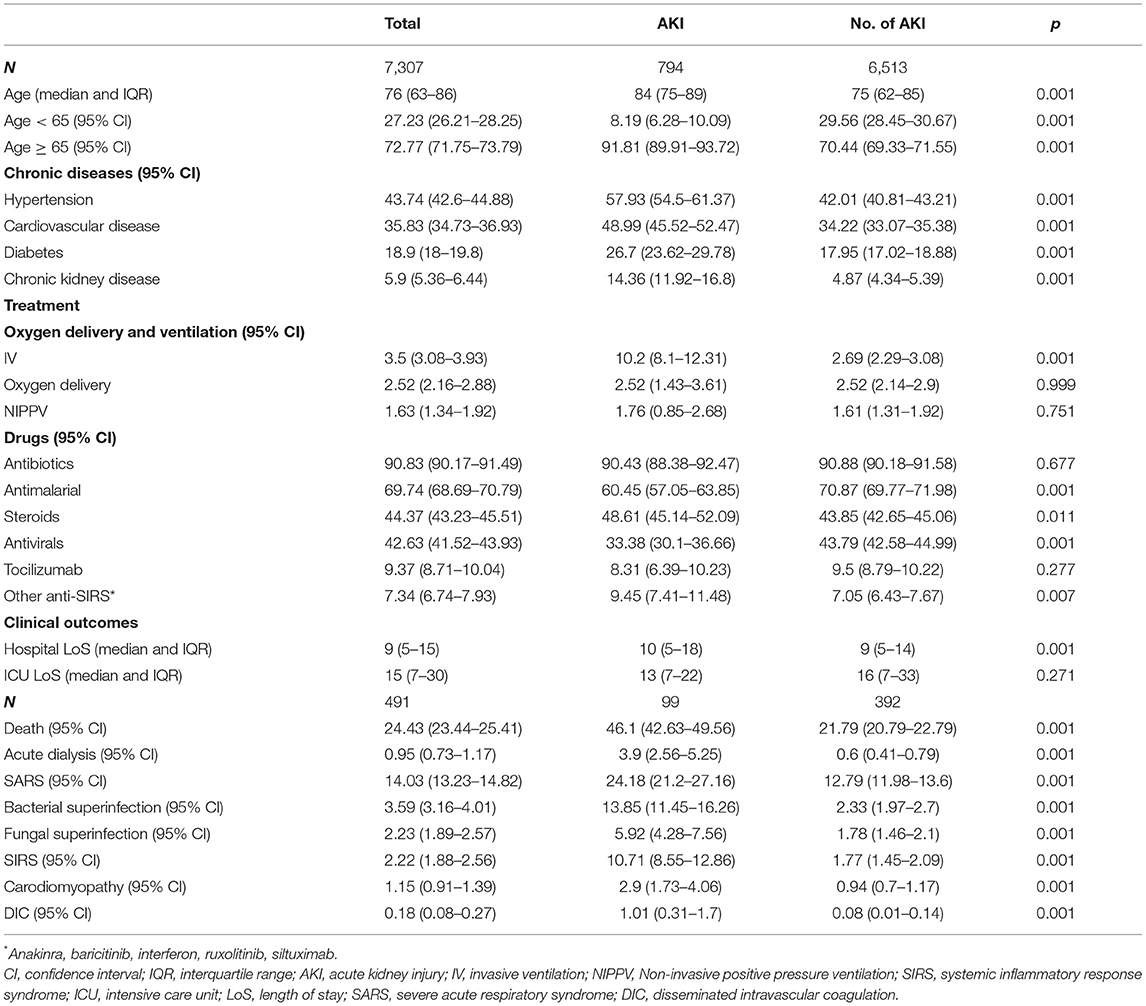
Table 1. Baseline characteristics, treatment, and clinical outcomes of in-hospital COVID-19 patients with acute kidney injury in Castile and Leon (Spain) (March 1st–May 3th 2020).
Into the group of COVID-19 patients presenting AKI, there were no differences in comorbidities between the two gender groups. Nevertheless, compared with females, twice as many male patients needed IV and three times as many male patients needed at least one session of acute dialysis, even if NIPPV and oxygen delivery were used similarly by both genders (Table 1). Males also had SARS and cardiomyopathy more commonly, and their hospital length of stay (median 10 days) was more prolonged, compared with that of females. In addition to antibiotics, male patients also used more antimalarials, steroids, antivirals, other anti-SIRS, and tocilizumab, compared with females (Table 1).
In addition, within the first 15-day period the mortality rate was very high (75%), while decreasing to 44.12% in the last 15-day period. The same trend applies to the length of hospital stay (Figure 1 and Supplementary Table 4). The peak of AKI incidence was reached between April 15th and May 14th (about 14%). COVID-19 patients with AKI needed to stay in the ICU more frequently in the second half of March 2020 (27.2%) (Supplementary Table 4).
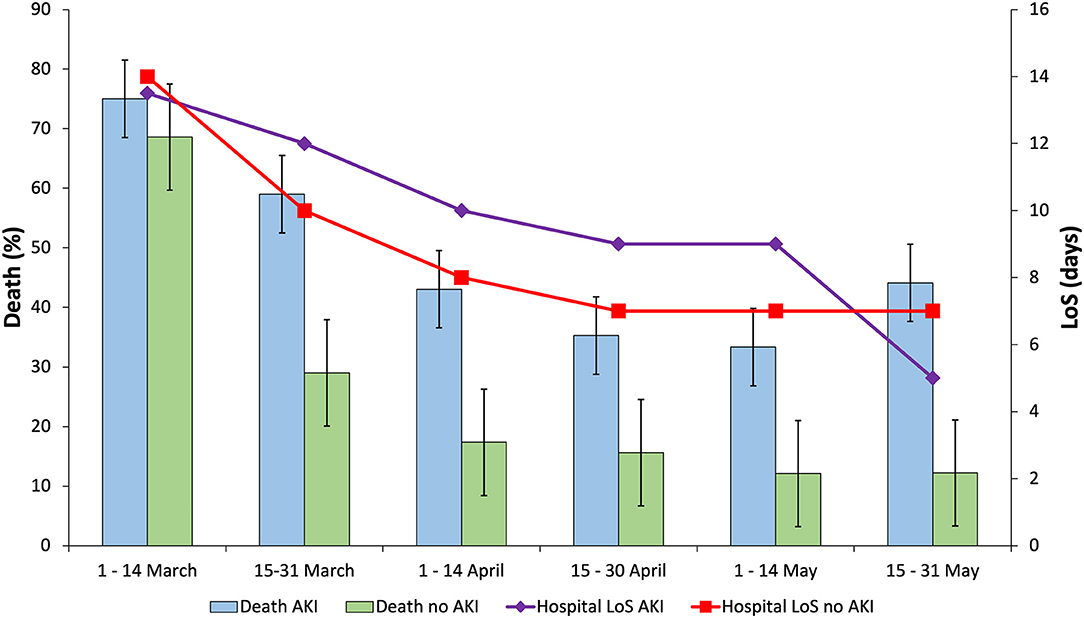
Figure 1. Death and hospital length of stay (LoS) corresponding to the in-hospital COVID-19 patients with or without acute kidney injury (AKI) in Castile and Leon (Spain) (March 1st–May 31th, 2020).
While the use of antibiotics and steroids, to some extent, remains stable throughout the time, the use of rest of the medications decreased during the study period (Figure 2 and Supplementary Table 4).
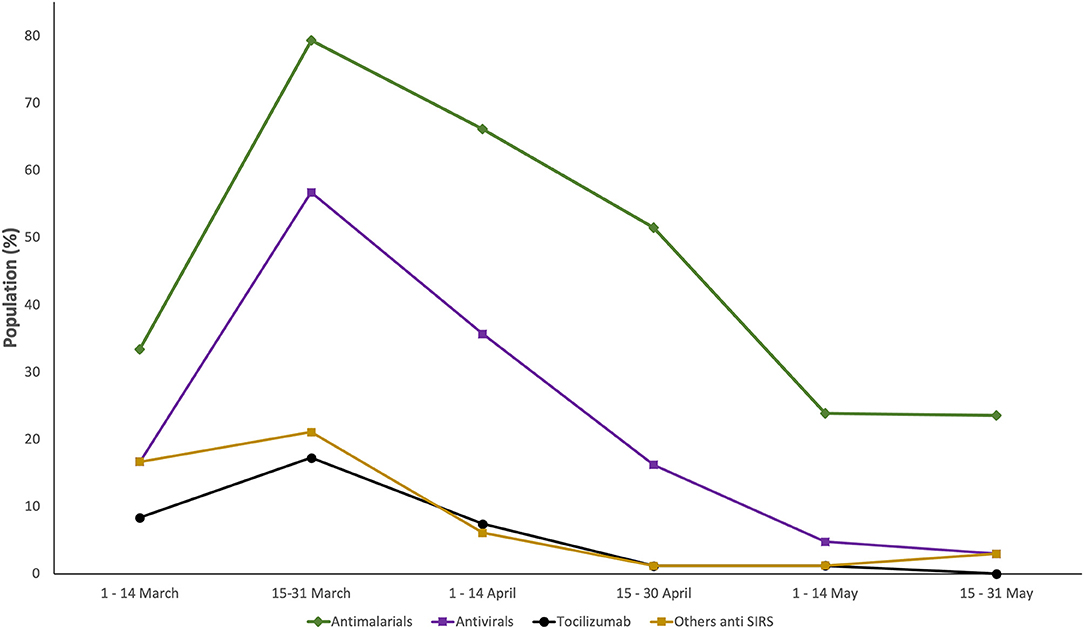
Figure 2. Trends in the use of the medications used by in-hospital COVID-19 patients with acute kidney injury (AKI) in Castile and Leon (Spain) (March 1st–May 31th, 2020).
Table 2 shows the medication received by COVID-19 patients with AKI who died or survived: significantly lower use of antibiotics and greater use of beta interferon (another anti-SIRS drug category) were noted in those who died compared with those patients who did not die.
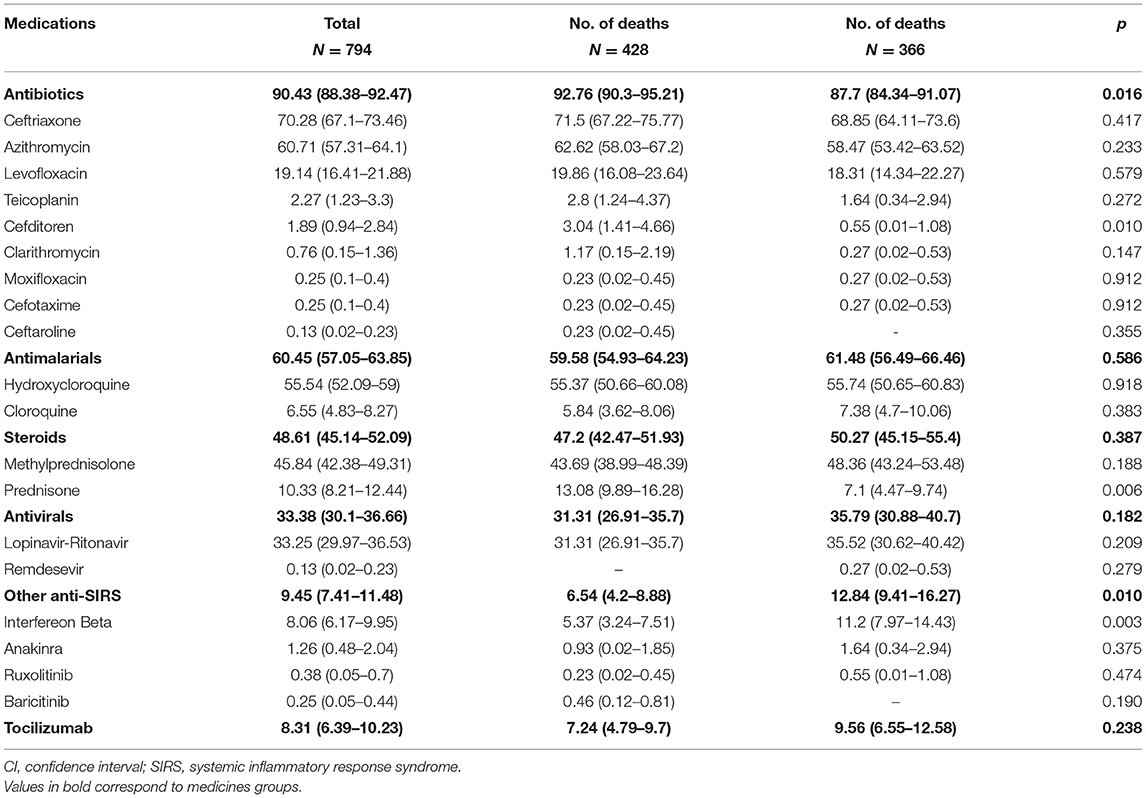
Table 2. Medications used by in-hospital COVID-19 patients with acute kidney injury (AKI) in Castile and Leon (Spain) (March 1st–May 31th 2020).
No impact on survival in patients with or without AKI was observed (median survival: 12 vs. 12 days; p = 0.55) (Supplementary Figure 1). However, multiple logistic regression analysis for all in-hospital COVID-19 patients shows the impact of AKI on death (OR: 2.6; 95% CI: 1.73–2.45), as well as comorbidities, such as cardiovascular disease (1.56, 1.37–1.76), diabetes mellitus (1.18, 1.01–1.36), and particularly having an age of 65 years or more (7.34, 5.93–9.08). Furthermore, among the COVID-19 patients with AKI, death was more likely to occur in those requiring ventilation, without distinguishing between invasive and non-invasive modalities (OR: 5.89; 95% CI: 3.13–11.06), in those treated with steroids (1.73, 1.24–2.41) or anti-SIRS drugs (2.38, 1.27–4.44), and in those who developed SARS (2.75, 1.83–4.14) or SIRS (2.52, 1.46–4.34).
This study shows that AKI was present in 1 out of 10 in-hospital COVID-19 patients (March 1st to May 31th, 2020) and that 9 out of 10 cases occurred in people aged more than 65 years, with a mortality around 50%. Ventilation, the use of some medications (steroids, anti-SIRS), and SARS and SIRS incidence may be present in COVID-19 patients with AKI who have an increased risk of death. In addition, AKI had no impact on median survival (in days) compared with in-hospital COVID-19 patients who did not develop AKI. However, mortality among patients with AKI was twice that observed in patients without AKI (46.1 vs. 21.79%) (16), and it is higher than in other studies (17).
Surprisingly, obesity had no influence on death of the patients both with AKI and without AKI, contrary to other studies (18, 19). Probably, lower rates of obesity (in patients with or without AKI, 21.16 and 18.58%, respectively) compared with other cohorts, may be an explanation (20).
Meta-analyses assessing COVID-19 patients from all over the world with AKI confirm that the incidence of AKI was greater in our region compared with Asia (4.3%) but lower than in North America (22.6%) and similar to that of other European countries (11.6%) (3, 8, 21, 22). Surprisingly, the mortality rate in Castile and Leon, Spain, was higher than in all of them. It is difficult to establish which factors are associated with this high mortality rate, which probably is related to the aging of the population in Castile and Leon, but also to other factors, such as the “collapse” of the Spanish public health system, the limited expertise of physicians in treating COVID-19 patients at such a moment, professional extenuation, etc. In this sense, there were differences with respect to other cohorts having an elevated percentage of patients aged 65 years or older, as in our region, which obliging to define the prognosis of the COVID-19 patient with AKI (21): AKI itself seems to have an impact on death, as demonstrated by our analysis and according to findings in other studies (8, 22); however, the impact from other factors should be characterized and considered for different world regions. However, it seems clear that mortality is higher in patients with chronic kidney disease who develop AKI (23).
Our study shows that ventilation, the use of some medicines (steroids, anti-SIRS), the occurrence of SARS or SIRS may depict a patient with a poor prognosis: Physicians should understand that such an individual has an elevated risk of dying, and they should consider these factors in order to assist COVID-19 patients with AKI now and in the future. Importantly, previous clinical conditions, such as age and gender, as well as the need for acute dialysis, seem to have no influence on the change in patients, but the use of some medications (steroids, anti-SIRS) and the severity of COVID-19 (SARS occurrence, signs of SIRS), should lead to more intensive interventions.
This study provides real-world evidence of risk factors associated with the deaths of COVID-19 patients with AKI in the largest region of Spain. As in other healthcare settings (24), assessing data that come from the actual clinical practice has contributed to the characterization of a population suffering bad outcomes. Nevertheless, questions about the quality of the evidence may arise. The findings presented here may be considered to belong to “emerging sources” from outside classic research environments (25).
This real-world data study presents a comprehensive analysis from the COVID-19 pandemic in Castile and Leon, the largest region of Spain, with a population of 2,323,770 inhabitants and a network of public hospitals with a total capacity of 7,141 beds (14 hospitals). Our findings thus cover all in-hospital COVID-19 patients (n = 7,307), of whom those presenting with AKI are presented here (n = 794).
This study has limitations that should be mentioned. First, although all extracted COVID-19 cases were recorded in the health administration registries accessed as COVID-19 patients, in one third of the cases, COVID-19 diagnosis was clinical or radiological, without microbiological confirmation, as tests were not available for all and because clinical judgment was the only tool at that time. Therefore, risk of selection bias should invite prudence in interpreting the results of this article. Second, due to the collapse of the health system, errors in the clinical data register during the first COVID-19 wave have been observed, which may explain study attrition. Furthermore, selection bias is suspected in the figures of CKD prevalence as not all CKD patients in KDIGO GFR categories 3–5 return to general practitioners after the first consultation in nephrology departments, and not all patients in those CKD categories are sent by general practitioners to the nephrologist. The Angiotensin-Converting Enzyme Inhibitors (ACE)/Angiotensin II Receptor Antagonists (ARB) ratio could be related to the COVID patients' survival; unfortunately, that information was not available, which may be a limitation. Over 8 months have elapsed since the collection of the data, which may be a limitation; however, AKI is still one of the COVID-19 outcomes with the worst prognosis. Finally, other medications not included in Spanish guidelines (14, 15) were not taken into account in this study.
In conclusion, AKI was observed in one 1 out of 10 COVID-19 patients, and almost half of them died before discharge, which demonstrates a mortality rate higher than that observed in other regions including Spain (3, 4, 26–29).
With respect to the pharmacological treatment of these patients, with the exception of antibiotics and steroids, the use of the medications analyzed decreased throughout the study period, either due to their availability or that of other medications not used in our studio. Our study has characterized the subjects hospitalized with COVID-19 and highlighted the use of medicines to treat systemic inflammation, and this situation has not changed up to now.
Lastly, AKI is a serious complication of COVID-19, and it must be taken into account by physicians in order to pay better attention to patients' treatment and to the occurrence of manifestations such as SARS or SIRS associated with a poor prognosis.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by East Valladolid Health Area Ethics Committee (reference: PI 20–1863).
EG-A, ET, and FÁ: conceptualization. EG-A, FH-G, DM-G, and FÁ: methodology, validation, and investigation. EG-A and ET: software. EG-A, FH-G, ET, and FÁ: formal analysis. FÁ: resources, supervision, project administration, and funding acquisition. EG-A: data curation and visualization. EG-A, FH-G, and FÁ: writing—original draft preparation. EG-A, FH-G, ET, DM-G, and FÁ: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
This research was funded by the Gerencia Regional de Salud (Grant Number GRS COVID 10/A/20).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank the Gerencia Regional de Salud de Castilla y León for access to JIMENA, MEDORA, and CONCYLIA database.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.657977/full#supplementary-material
1. Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. (2020) 98:209–18. doi: 10.1016/j.kint.2020.05.006
2. Zahid U, Ramachandran P, Spitalewitz S, Alasadi L, Chakraborti A, Azhar M, et al. Acute kidney injury in COVID-19 patients: an inner city hospital experience and policy implications. Am J Nephrol. (2020) 51:786–96. doi: 10.1159/000511160
3. Portolés J, Marques M, López-Sánchez P, de Valdenebro M, Muñez E, Serrano ML, et al. Chronic kidney disease and acute kidney injury in the COVID-19 Spanish outbreak. Nephrol Dial Transplant. (2020) 35:1353–61. doi: 10.1093/ndt/gfaa189
4. Ronco C, Reis T, Husain-Syed F. Management of acute kidney injury in patients with COVID-19. Lancet Respir Med. (2020) 8:738–42. doi: 10.1016/S2213-2600(20)30229-0
5. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
6. Miller J, Fadel RA, Tang A, Perrotta G, Herc E, Soman S, et al. The impact of sociodemographic factors, comorbidities and physiologic response on 30-day mortality in COVID-19 patients in metropolitan detroit. Clin Infect Dis. (2020) ciaa1420. doi: 10.1093/cid/ciaa1420. [Epub ahead of print].
7. Yang X, Jin Y, Li R, Zhang Z, Sun R, Chen D. Prevalence and impact of acute renal impairment on COVID-19: a systematic review and meta-analysis. Crit Care. (2020) 24:356. doi: 10.1186/s13054-020-03065-4
8. Shao M, Li X, Liu F, Tian T, Luo J, Yang Y. Acute kidney injury is associated with severe infection and fatality in patients with COVID-19: a systematic review and meta-analysis of 40 studies and 24,527 patients. Pharmacol Res. (2020) 161:105107. doi: 10.1016/j.phrs.2020.105107
9. Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. (2015) 12:e1001885. doi: 10.1371/journal.pmed.1001885
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. (2008) 61:344–9. doi: 10.1016/j.jclinepi.2007.11.008
11. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. (1992) 101:1644–55. doi: 10.1378/chest.101.6.1644
12. KDIGO AKI Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. (2012) 2:1–138. doi: 10.1038/kisup.2012.1
13. Stevens PE, Levin A, Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. (2013) 158:825–30. doi: 10.7326/0003-4819-158-11-201306040-00007
14. Spanish Ministry of Health. Clinical Management of COVID-19. (2020). Available online at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Protocolo_manejo_clinico_ah_COVID-19.pdf (accessed November 16, 2020).
15. Spanish Agency for Medicine and Health Products. Available Treatments for the Management of Respiratory Infection by SARS-CoV-2. (2020). Available online at: https://www.aemps.gob.es/laAEMPS/docs/medicamentos-disponibles-SARS-CoV-2-22-5-2020.pdf?x57200 (accessed November 16, 2020).
16. Gutiérrez-Abejón E, Tamayo E, Martín-García D, Álvarez FJ, Herrera-Gómez F. Clinical profile, treatment and predictors during the first COVID-19 wave: a population-based registry analysis from castile and Leon hospitals. Int J Environ Res Public Health. (2020) 17:9360. doi: 10.3390/ijerph17249360
17. Gupta S, Coca SG, Chan L, Melamed ML, Brenner SK, Hayek SS, et al. AKI treated with renal replacement therapy in critically ill patients with COVID-19. J Am Soc Nephrol. (2021) 32:161–76. doi: 10.1681/ASN.2020060897
18. Simpson AHR, Simpson CJ, Frost H, Welburn SC. COVID-19: obesity, deprivation and death. J Glob Health. (2020) 10:020389. doi: 10.7189/jogh.10.020389
19. Rottoli M, Bernante P, Belvedere A, Balsamo F, Garelli S, Giannella M, et al. How important is obesity as a risk factor for respiratory failure, intensive care admission and death in hospitalised COVID-19 patients? Results from a single Italian centre. Eur J Endocrinol. (2020) 183:389–97. doi: 10.1530/EJE-20-0541
20. Petrilli CM, Jones SA, Yang J, Rajagopalan H, O'Donnell L, Chernyak Y, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. (2020) 369:m1966. doi: 10.1136/bmj.m1966
21. Lin L, Wang X, Ren J, Sun Y, Yu R, Li K, et al. Risk factors and prognosis for COVID-19-induced acute kidney injury: a meta-analysis. BMJ Open. (2020) 10:e042573. doi: 10.1136/bmjopen-2020-042573
22. Hansrivijit P, Qian C, Boonpheng B, Thongprayoon C, Vallabhajosyula S, Cheungpasitporn W, et al. Incidence of acute kidney injury and its association with mortality in patients with COVID-19: a meta-analysis. J Investig Med. (2020) 68:1261–70. doi: 10.1136/jim-2020-001407
23. Flythe JE, Assimon MM, Tugman MJ, Chang EH, Gupta S, Shah J, et al. Characteristics and outcomes of individuals with pre-existing kidney disease and COVID-19 admitted to intensive care units in the United States. Am J Kidney Dis. (2021) 77:190–203.e1. doi: 10.1053/j.ajkd.2020.09.003
24. Richesson RL, Hammond WE, Nahm M, Wixted D, Simon GE, Robinson JG, et al. Electronic health records based phenotyping in next-generation clinical trials: a perspective from the NIH health care systems collaboratory. J Am Med Inform Assoc. (2013) 20:e226–31. doi: 10.1136/amiajnl-2013-001926
25. Sherman RE, Anderson SA, Dal Pan GJ, Gray GW, Gross T, Hunter NL, et al. Real-world evidence—what is it and what can it tell us? N Engl J Med. (2016) 375:2293–7. doi: 10.1056/NEJMsb1609216
26. Berenguer J, Ryan P, Rodríguez-Baño J, Jarrín I, Carratalà J, Pachón J, et al. Characteristics and predictors of death among 4035 consecutively hospitalized patients with COVID-19 in Spain. Clin Microbiol Infect. (2020) 26:1525–36. doi: 10.1016/j.cmi.2020.07.024
27. Casas-Rojo JM, Antón-Santos JM, Millán-Núñez-Cortés J, Lumbreras-Bermejo C, Ramos-Rincón JM, Roy-Vallejo E, et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: results from the SEMI-COVID-19 Registry. Rev Clin Esp. (2020) 220:480–94. doi: 10.1016/j.rce.2020.07.003
28. Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. (2020) 323:2052–9. doi: 10.1001/jama.2020.6775
Keywords: SARS-CoV-2, COVID-19, acute kidney injury, chronic kidney disease, treatment, mortality
Citation: Gutiérrez-Abejón E, Martín-García D, Tamayo E, Álvarez FJ and Herrera-Gómez F (2021) Clinical Profile, Pharmacological Treatment, and Predictors of Death Among Hospitalized COVID-19 Patients With Acute Kidney Injury: A Population-Based Registry Analysis. Front. Med. 8:657977. doi: 10.3389/fmed.2021.657977
Received: 24 January 2021; Accepted: 29 March 2021;
Published: 15 June 2021.
Edited by:
Susan Christina Welburn, University of Edinburgh, United KingdomReviewed by:
Lili Chan, Icahn School of Medicine at Mount Sinai, United StatesCopyright © 2021 Gutiérrez-Abejón, Martín-García, Tamayo, Álvarez and Herrera-Gómez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Gutiérrez-Abejón, ZWd1dGllcnJlemFAc2FsdWRjYXN0aWxsYXlsZW9uLmVz
†These authors share first authorship
‡These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.