 Cécile Cuvilliers1,2*
Cécile Cuvilliers1,2* Xavier Palard-Novello1,2
Xavier Palard-Novello1,2 Clémence Pontoizeau1Pierre Meneret1,2Anne Devillers1Florence Le Jeune1,2
Clémence Pontoizeau1Pierre Meneret1,2Anne Devillers1Florence Le Jeune1,2 Antoine Girard1,2
Antoine Girard1,2- 1Nuclear Medicine Department, Centre Eugène Marquis, Rennes, France
- 2University of Rennes 1, Rennes, France
Purpose: To evaluate the interest of adding a bloodpool SPECT/CT to standard three-phase bone scintigraphy (BS) for etiological diagnosis of subacute and chronic lower extremity pains.
Methods: We prospectively included patients addressed for pain of lower extremities lasting for at least 6 weeks, without previous surgery. They underwent a standard three-phase BS including late phase SPECT/CT, modified with an additional bloodpool SPECT/CT acquisition. Two independent physicians interpreted the images provided by both protocols. Diagnostic conclusion, diagnostic confidence, and interrater agreements were compared.
Results: One hundred and eighteen lower extremities from 113 patients were analyzed (71 men, median age of 53 years). Adding bloodpool SPECT/CT to standard three-phase BS changed diagnostic conclusions in 24.6% (29/118) of lower extremities. The modified protocol revealed at least one diagnostic conclusion explaining the pain in 89% of extremities, rather than 83.1% with the standard protocol (p = 0.02). Tendinopathies were diagnosed in 12.7% of lower extremities, rather than 4.2% with standard BS (p = 0.002). Adding bloodpool SPECT/CT substantially increased overall confidence of each reader (p < 0.001). Inter-reader agreement was not significantly impacted.
Conclusion: Adding bloodpool SPECT/CT to standard three-phase BS impacted diagnostic conclusion in a quarter of the patients with painful lower extremities, notably by revealing significantly more tendonitis.
Introduction
Subacute and chronic pains of foot and ankle are common reasons for healthcare encounter (1). Many causes can be responsible, such as osseous and articular pathology, as well as tendonitis, ligamentopathy, and complex regional pain syndrome (CRPS) with different therapeutic management. Identifying the underlying etiology of the pain can be challenging, even after detailed clinical examination and initial radiography. This frequently makes further imaging explorations necessary (2). Three-phase bone scintigraphy (3pBS) is an imaging method of choice to establish etiological diagnosis of painful lower extremities (3). The rise of late-phase single photon emission computed tomography (SPECT) has dramatically increased diagnostic performances of bone scintigraphy by enhancing its sensitivity (4), and its localization ability (5). Moreover, with the advent of hybrid imaging, specificity was increased by adding CT to SPECT. These technical developments provided substantial improvement in diagnosis and management of patients with pain, particularly regarding painful lower extremities (6).
Despite the major contribution of bone scintigraphy to diagnose osseous and articular pathologies, the cause of the pain remains unrevealed in many patients (3). To date, only a few studies investigated the role of bone scintigraphy to detect extra-osseous abnormalities, notably concerning foot and ankle pain (7, 8). Based on the standard bloodpool planar images, bone scintigraphy can reveal inflammatory process in extra-osseous tissues (9), while late-phase images appear normal. Verschueren et al. recently reported that bloodpool SPECT outperforms planar imaging in the assessment of painful total knee arthroplasty and improves information on prosthesis outcome (10). Considering the prevalence of extra-osseous pathologies (11) and the particularly complex anatomy of the feet and ankles (11, 12), we assumed that bloodpool SPECT/CT could be of interest when exploring subacute and chronic lower extremities pain and may detect extraosseous pathology unrevealed with standard 3pBS.
The aim of this study was to evaluate the interest of adding a bloodpool SPECT/CT to standard 3pBS for etiological diagnosis of subacute and chronic lower extremities pain, regarding diagnostic conclusion, inter-reader agreement, and diagnostic confidence.
Materials and Methods
Participants
We prospectively included from March 2019 to March 2020 consecutive patients referred to our center to perform a bone scintigraphy who matched the following inclusion criteria: minimum age of 18 years old, subacute (evolving for 6–12 weeks) or chronic (evolving for more than 3 months) foot and/or ankle pain, no previous surgery of the affected lower extremity, affiliation to national healthcare insurance. Exclusion criteria were local anti-inflammatory infiltration within the last month and intake of anti-inflammatory systemic drug within the past week. This study performed in routine care was reviewed and approved by the University Hospital of Rennes ethics committee (approval n°19.99 −2). According to the current regulations of the European Union for prospective observational studies, participants received written information and did not object to participate. Clinical information was obtained from both the examination request letter written by the corresponding practitioner and a standardized questionnaire filled with each patient.
Imaging Procedures
All patients received bone scintigraphy according to the guidelines of the European Association of Nuclear Medicine, consisting of planar 2 min early dynamic and bloodpool acquisitions centered on feet/ankles, and late-phase planar whole-body and SPECT/CT images of the lower extremities. The radiopharmaceutical used was hydroxy-methylene-diphosphonate (HMDP) labeled with 99m-technetium. Bloodpool planar images were acquired systematically in anterior-posterior 5 min projection, and additional projection on request from the nuclear medicine physician. In addition, a bloodpool SPECT/CT centered on feet and ankles was performed 7–14 min after injection. Images were acquired on hybrid SPECT/CT system (Discovery 670, GE Healthcare, or Symbia T16, Siemens Healthineers). Both bloodpool and late-phase SPECT/CT acquisitions were performed with the step-and-shoot acquisition system on the Discovery camera (30 projections of 20 s, yielding a total acquisition time of 10 min) or the continuous acquisition system on the Symbia camera (30 projections of 15 s, total acquisition time of 7 min and 30 s). SPECT data were reconstructed using the Recon Flash 3D on Discovery camera, and an ordered subset expectation maximization on the Symbia camera (128 × 128 matrix, pixel size of 4.4 mm in every axis). A low-dose CT was performed during bloodpool phase (Discovery: voltage 80 kV, 60 mAs, slice thickness and spacing 3,75 mm, iterative reconstruction, Symbia: 80 kV, 35 mAs, Care Dose collimation, slice thickness and spacing 5 mm, with reconstruction of 3 mm) and a diagnostic CT associated with late-phase SPECT (Discovery: 120 kV, maximum of 140 mAs with modulation, slice thickness 0.625 mm and spacing 0.5 mm, iterative reconstruction; Symbia: 130 kV, 120 mAs, slice thickness and spacing of 0.75 mm each 0.5 mm).
Images Interpretation
Two nuclear medicine physicians, aware of clinical information, read independently all the images in two steps. A first interpretation was based on images provided by standard 3pBS (including angiographic phase, bloodpool planar imaging, and late-phase SPECT/CT), then, at least 3 months apart and blinded to prior interpretation, a second reading relied on images obtained with the modified protocol (i.e., with the addition of bloodpool SPECT/CT). In both steps, CT images from hybrid modalities were taken into account in the interpretation. For each interpretation step, each reader provided a description of abnormalities, and a diagnostic conclusion addressing the diagnostic issue with an overall confidence score on a 3-points scale (1: low confidence, 3: high confidence). For each reader, diagnostic conclusions were synthesized as CRPS in hot phase, CRPS in cold phase, fracture (or pseudoarthrosis), arthropathy (from distal tibiofibular joint to toes joints, including accessory sesamoid bones conflicts and osteochondral lesions of the talar dome), ligamentopathy (including ankle and tarsal ligaments and distal tibiofibular syndesmosis), tendinopathy, calcaneal spur, other diagnostic orientation, or no diagnostic orientation. Finally, on each step of interpretation, in case of discrepancy regarding the diagnostic conclusion, a common reading was made until a consensus was reached.
Study Endpoints
The primary endpoint was the diagnostic conclusion provided by bone scintigraphy. The hypothesis of the study was that the use of bloodpool SPECT/CT provides a substantial change in diagnostic conclusion compared to standard 3pBS protocol (reveals more, less, or some other diagnoses). The secondary endpoints were the inter-rater agreement and the overall confidence. The hypotheses were that adding bloodpool SPECT/CT to standard protocol increases inter-rater agreement and overall confidence regarding for the diagnostic conclusions.
Statistical Analysis
Statistical analysis was performed with the MedCalc® version 12.5.0.0 (Medcalc Software, Ostend, Belgium). Distribution of continuous variables were presented as median [Interquartile range (IQR)]. Proportions for each kind of diagnostic conclusion provided by the consensus of experts were compared between standard and modified protocols using the McNemar's t-test. Scores for diagnostic confidence of both readers were compared between standard and modified protocols using a Wilcoxon signed test. Interrater agreements were assessed for each kind of diagnostic orientation using Cohen's kappa coefficient with 95% confidence intervals (95%CI) (values ≤0 as indicating no agreement, 0.01–0.20 as none to slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement). All statistical tests were two-tailed and statistical significance level was set at p < 0.05.
Results
Participants
Two hundred and seventy-one patients were prospectively screened, 79 did not match inclusion criteria, and 79 were excluded. One hundred and eighteen lower extremities from 113 patients [71 men, median age of 53 years (IQR: 37–66)] were finally analyzed. The flowchart of participants is presented in Figure 1. The lower extremity pains lasted for a median duration of 14 weeks (7–40) with an intensity of 5 (4–7) on a 10-points visual analog scale. Thirty-six (31.9%) patients were suspected with CRPS by the corresponding clinician, and 59 (50%) reported a trauma. Characteristics of patients are presented in Table 1.
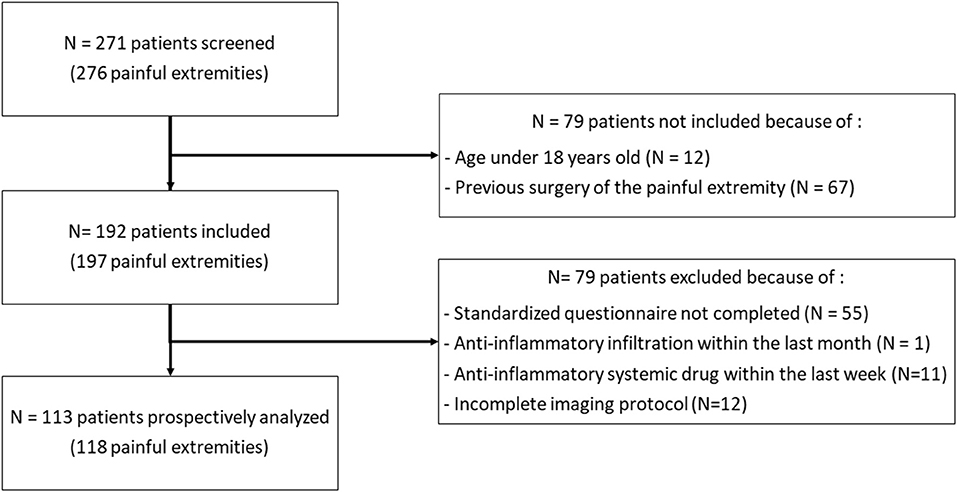
Figure 1. Flowchart of the study.
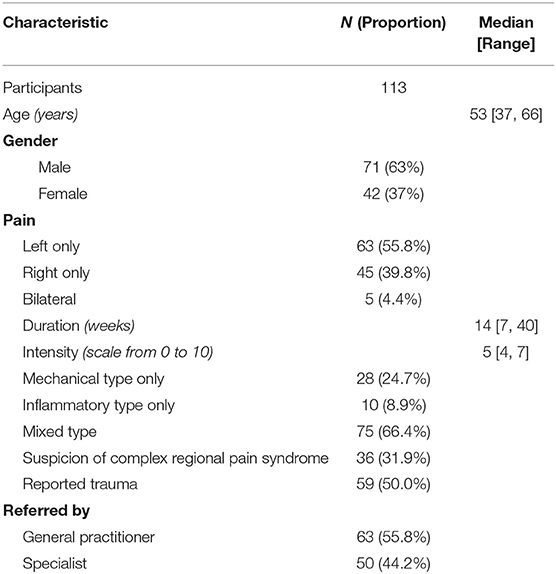
Table 1. Participant characteristics.
Diagnostic Conclusions
Adding bloodpool SPECT/CT substantially impacted diagnostic conclusions in 29 out of 118 (24.6%) lower extremities. Diagnostic conclusions provided by both standard and modified imaging protocols are presented in Table 2. Whereas, 98 (83.1%) lower extremities were found with at least one diagnostic conclusion explaining the symptoms with standard 3pBS including late-phase SPECT/CT, 105 (89.0%) (p = 0.02) showed at least one diagnostic conclusion with the modified imaging protocol including supplementary bloodpool SPECT/CT. The only diagnostic category that detection was significantly impacted by adding bloodpool SPECT/CT was “tendinopathy,” revealed in 15 (12.7%) lower extremities with modified protocol, rather than five (4.2%) with standard 3pBS with late-phase SPECT/CT (p = 0.002). The bloodpool SPECT/CT revealed 12 additional tendons with pathological uptake (including two lower extremities with another tendonitis already visualized with the standard protocol): five posterior tibial tendons, three anterior tibial tendons, three calcaneal tendons, and one fibular tendon (Figure 2).
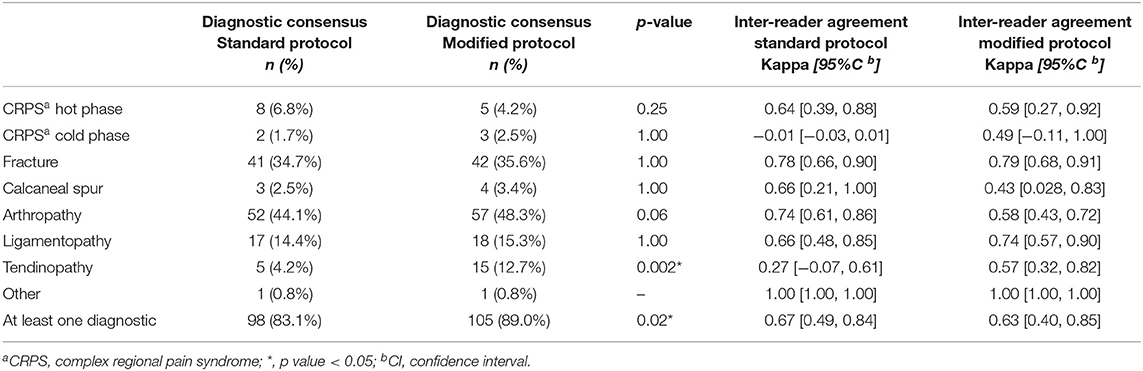
Table 2. Diagnostic conclusions and inter-reader agreement compared between the standard three-phase bone scintigraphy and modified protocol.
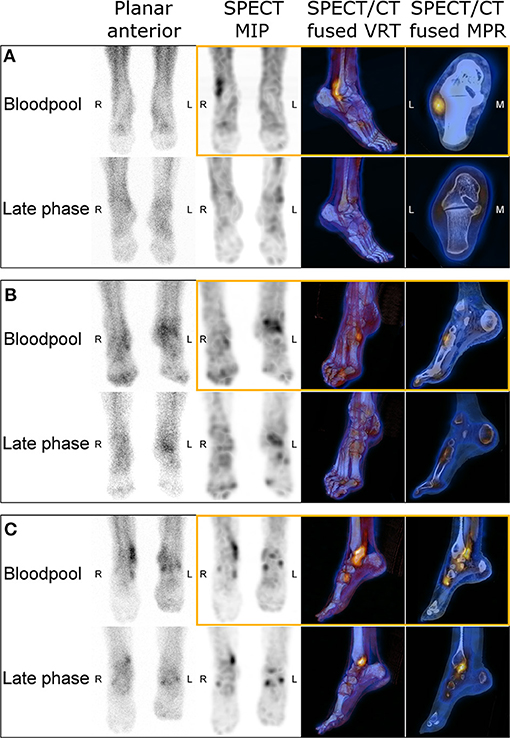
Figure 2. Images of three-phase bone scintigraphy from three patients with right lower extremity pain, including images provided by bloodpool SPECT/CT (in orange boxes). Patient (A) was a 62-year-old man referred for suspicion of right lateral malleolus stress fracture. Bloodpool SPECT/CT revealed intense uptake along peroneal tendons, highly suggesting the diagnosis of right peroneal tendonitis. Patient (B) was an 81-year-old woman with pain of the right ankle and anterior tarsus, suspected with stress fracture. Bloodpool SPECT/CT revealed focal uptake at the insertion of the anterior tibial tendon, leading to set the diagnosis of right tibial anterior tendonitis. Patient (C) was a 60-year-old woman, suffering from right medial ankle pain. Planar bloodpool and late phase SPECT/CT images were compatible with a posterior tibial tendonitis with a low diagnostic confidence. Bloodpool SPECT/CT substantially increased the diagnostic confidence for posterior tibial tendonitis and revealed intense focal uptake at the insertion of the anterior tibial tendon, evocative of associated right tibial anterior tendonitis.
Diagnostic Confidence
Overall confidence of each reader was significantly higher based on the modified protocol including bloodpool SPECT/CT than using the standard 3pBS with late-phase SPECT/CT only. The mean ± standard deviation overall diagnostic confidence was 2.0 ± 0.8 with the standard protocol, and 2.5 ± 0.7 with the addition of bloodpool SPECT/CT (p < 0.0001) for reader 1, and 1.9 ± 0.7 and 2.3 ± 0.8 (p < 0.0001), respectively, for reader 2.
Inter-reader Reproducibility
Inter-reader agreement on diagnostic conclusion are presented in Table 2. The addition of bloodpool SPECT/CT to standard 3pBS did not significantly modify inter-reader reproducibility for any diagnostic conclusion category regarding the Cohen's kappa coefficient.
Bloodpool Imaging Description
To better understand how the addition of bloodpool SPECT/CT impacted the interpretation, here are reported the abnormalities described by the readers based on bloodpool images from the standard and the modified protocol, respectively. A total of 165 abnormalities from 93 lower extremities were described either on planar bloodpool and/or bloodpool SPECT images (Table 3). For 25 lower extremities, no bloodpool abnormality was found, neither on planar nor on SPECT images. One hundred and twelve (67.9%) bloodpool abnormalities from 61 (65.6%) feet or ankles were found on both planar and SPECT images, including 33 out of 112 (29.5%) abnormalities from 31 out of 61 (50.8%) extremities that were differently localized thanks to bloodpool SPECT/CT. The bloodpool SPECT revealed 44 (26.7%) uptake abnormalities from 33 (35.5%) extremities undetected with bloodpool planar images. Inversely, nine (5.4%) abnormalities from nine lower extremities (9.7%) were only reported based on planar images, but unseen with SPECT/CT. Five out of these nine abnormalities (55.6%) were unwell circumscribed increased uptake projecting on median midfoot on planar images. On bloodpool SPECT/CT images, these abnormalities matched linear uptakes following the lateral and deep plantar vessels, without any morphological abnormality (Figure 3).
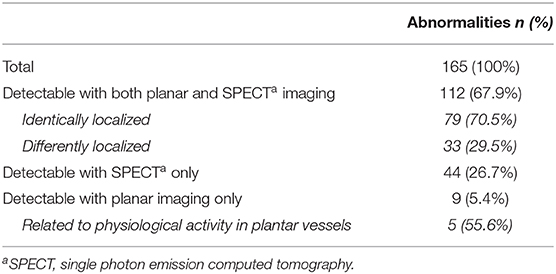
Table 3. Bloodpool imaging description.
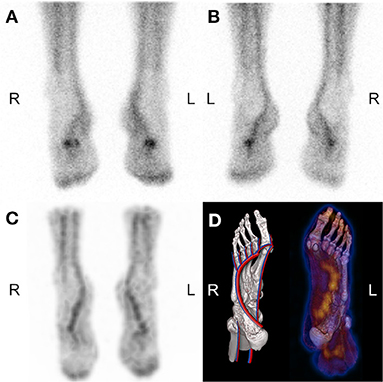
Figure 3. 50-year-old man suffering from pain of third to fifth left metatarsus. Anterior (A) and posterior (B) planar bloodpool images suggested increased uptake in the projection of left and right midfoot. Bloodpool SPECT (C: MIP, D: SPECT fused VRT and anatomical drawing) refuted the “abnormality,” revealing physiological linear uptake on deep plantar arch.
Discussion
In the last decade, the development of hybrid SPECT/CT substantially improved diagnostic performances of bone scintigraphy (13), particularly when imaging the extremities (14). Authors reported that late-phase SPECT/CT has high impact on therapeutic decisions for foot and ankle pain (15), notably if multiple pathologies are coexisting (16). However, to date, the role of bloodpool SPECT/CT has been poorly investigated, especially to explore lower extremities. Recently, authors related that bloodpool SPECT outperforms planar imaging in the assessment of painful total knee arthroplasty, by enhancing the inter-rater agreement and the overall confidence to localize inflammatory regions, and by providing relevant information on prosthesis outcome (10). The value of bloodpool SPECT or SPECT/CT has also been suggested when exploring non-oncological bone pain, improving diagnostic yield compared to planar imaging, showing additional lesions (17), and improving localization of abnormalities (18). Lastly, its benefit has been suggested for viability assessment in mandibular reconstruction (19), painful hip or knee prosthesis (20), and in rheumatoid arthritis (21).
The results of the present study clearly support the role of bloodpool SPECT/CT as a part of 3pBS in the etiological exploration of lower extremity pain. The addition of bloodpool SPECT/CT substantially changed the diagnostic conclusion in 29 out of 118 (24.6%) lower extremities. Using the modified protocol provided significantly less inconclusive exams, revealing at least one diagnostic conclusion explaining the symptoms in 105 out of 118 (89.0%) of painful lower extremities, rather than 98 out of 118 (83.1%) with standard 3pBS. This increased diagnostic yield was mainly explained by a better visualization of tendonitis, which was the only diagnostic category significantly impacted by adding bloodpool SPECT/CT. Modified protocol revealed tendonitis explaining the pain in 15 out of 118 (12.7%) lower extremities, rather 5 out 118 (4.2%) with standard protocol. Besides, the results show that adding bloodpool SPECT significantly improved overall diagnostic confidence of each reader.
Two properties of SPECT/CT compared to planar images can explain the best detection of tendonitis. First, the highest signal-to-noise ratio provided by SPECT may have enable the visualization of tendinous uptake unrevealed by standard bloodpool planar images (22, 23). Moreover, combining SPECT and CT is known to improve localization of scintigraphic abnormalities (16). Hybrid imaging can have led to the diagnosis of tendonitis in patients with slight and/or poorly localized uptake visualized on standard bloodpool planar images, that may initially have been considered non-specific. These observations are in line with those of Verschueren et al. showing a 20% improvement of rater confidence when using bloodpool SPECT compared to planar images, for localizing uptake on bloodpool images in painful total knee arthroplasty (10).
Painful lower extremity is a widespread cause of medical consultation and imaging procedure (1, 22). Extra-osseous pathologies, such as tendon and ligament lesions, are common causes of symptoms (12), for instance ligamentous ankle sprains involves 27,000 patients per day in the US (7, 22). Bone scintigraphy is an imaging procedure performed by almost all nuclear medicine centers across the world, mostly non-expert centers. According to our results, adding bloodpool SPECT/CT to standard 3pBS improves diagnostic yield for tendonitis and enhances overall diagnostic confidence. Thus, expanding this practice could lead to substantially decrease the number of patients with pain remaining unexplained and prevent unnecessary investigation. The time-consuming aspect of adding bloodpool SPECT/CT to standard 3pBS could hamper its use. In the present study, bloodpool SPECT/CT revealed at least as much uptake abnormalities than bloodpool planar images in 94.5% lower extremities, showing more uptake abnormalities in 35.5%. Five out nine (56%) uptakes seen as “abnormal” only on planar images were considered as linked with physiological vascular activity in the plantar vessels on bloodpool SPECT, ruling out some potential pitfalls. These results suggest that bloodpool planar acquisitions might be replaced with SPECT/CT without losing diagnostic value. By doing so, the extra time needed would not exceed 2.5–5 min per patient if only one planar projection was initially planned. When compared to the time spent for several planar projections, performing bloodpool SPECT can even be faster. Moreover, using bloodpool SPECT instead of planar images would prevent the need to perform several planar acquisitions requiring complex foot positioning (24) and thus improve the comfort for patient with painful lower extremities and limit uninterpretable images due to patients' movements. These results are in line with those of Verschueren et al. who recently concluded to a benefit of using bloodpool SPECT instead of planar images (10). Interestingly, in the present study there was no statistically significant difference between standard and modified protocol regarding inter-reader agreement about the diagnostic conclusions. In contrast, Verschueren et al. reported an increased inter-rater agreement for localizing tracer uptake with bloodpool SPECT (10).
Our study has some limitations that need to be considered. First, we did not have a follow-up for any of the patients evaluated since they were addressed by clinicians from other institutions, thus we did not get for any confirmation of diagnostic conclusion provided by the bone scintigraphy. This bias is found in most other studies working on soft tissue pathology, considering the lack of gold standard investigation (12). Nevertheless, all the diagnostic conclusions reported were consistent with the localization and the type of the pain. Secondly, only anterior and posterior projections were systematically acquired regarding planar bloodpool imaging, and acquisition of supplemental projections was left to the discretion of the physician. It could be discussed whether pseudo planar images may have replaced standard planar images. Nevertheless, we considered bone activity to be very low on bloodpool SPECT beginning 7 min after injection, and that it would not impact diagnostic conclusion. Finally, this study was designed to evaluate the interest of bloodpool SPECT/CT in foot and ankle pain. Included patients were selected to constitute a homogeneous sample, and we chose to not include patients with history of previous surgery of the painful lower extremity. We emphasize that bloodpool SPECT/CT might also be particularly useful in this population, that could be investigated in a forthcoming study. As an aside, technical considerations can be discussed since we performed this study using devices with NaI(Tl) scintillation detectors. The use of new devices with CZT semiconductor detectors could improve spatial resolution and sensitivity for both planar and SPECT images (25).
Conclusions
The addition of bloodpool SPECT/CT to standard 3pBS for the exploration of painful lower extremities increased the diagnostic yield and enhanced the diagnostic confidence. No significant impact was observed regarding the inter-reader agreement. To improve its feasibility and the comfort of patients, our results suggest that bloodpool SPECT/CT could be performed instead of bloodpool planar images without missing meaningful information. This last point could be validated in a forthcoming study specially designed for.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by University Hospital of Rennes ethics committee (approval n°19.99 −2). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
AG and CC: study conception and design, screening and inclusion of patients, and bone scintigraphy analysis. CC: data collection. AG: statistical analysis. CC, AG, XP-N, PM, CP, AD, and FL: manuscript editing and reviewing. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ferguson R, Culliford D, Prieto-Alhambra D, Pinedo-Villanueva R, Delmestri A, Ardenet N, et al. Encounters for foot and ankle pain in UK primary care: a population-based cohort study of CPRD data. Br J Gen Pract. (2019) 69:422–9. doi: 10.3399/bjgp19X703817
3. Singh VK, Javed S, Parthipun A, Sott A. The diagnostic value of single photon-emission computed tomography bone scans combined with CT (SPECT-CT) in diseases of the foot and ankle. Foot Ankle Surg. (2013) 19:80–3. doi: 10.1016/j.fas.2012.11.002
4. Han LJ, Au-Yong TK, Tong WCM, Chu KS, Szeto LT, Wong CP. Comparison of bone single-photon emission tomography and planar imaging in the detection of vertebral metastases in patients with back pain. Eur J Nucl Med Mol Imaging. (1998) 25:635–8. doi: 10.1007/s002590050266
5. Gates GF. SPECT bone scanning of the Spine. Semin Nucl Med. (1998) 28:78–94. doi: 10.1016/S0001-2998(98)80020-2
6. Linke R, Kuwert T, Uder M, Forst R, Wuest W. Skeletal SPECT/CT of the peripheral extremities. AJR Am J Roentgenol. (2010) 194:329–35. doi: 10.2214/AJR.09.3288
7. Mandegaran R, Dhillon S, Jen H. Beyond the bones and joints: a review of ligamentous injuries of the foot and ankle on 99m Tc-MDP-SPECT/CT. Br J Radiol. (2019) 92:20190506. doi: 10.1259/bjr.20190506
8. Cuvilliers C, Icard N, Meneret P, Palard-Novello X, Girard A. Blood-Pool SPECT/CT in Chronic ankle tendinopathy. Clin Nucl Med. (2020) 45:e457–8. doi: 10.1097/RLU.0000000000003119
9. Delbeke D, Habibian MR. Noninflammatory entities and the differential diagnosis of positive three phase bone imaging. Clin Nucl Med. (1988) 13:844–51. doi: 10.1097/00003072-198811000-00021
10. Verschueren J, Albert A, Carp L, Ceyssens S, Huyghe I, Stroobants S, et al. Bloodpool SPECT as part of bone SPECT/CT in painful total knee arthroplasty (TKA): validation and potential biomarker of prosthesis biomechanics. Eur J Nucl Med Mol Imaging. (2019) 46:1009–18. doi: 10.1007/s00259-018-4244-4
11. Biersack H-J, Wingenfeld C, Hinterthaner B, Frank D, Sabet A. SPECT-CT of the foot. Nuklearmedizin. (2012) 51:26–31. doi: 10.3413/Nukmed-0421-11-08
12. Chicklore S, Gnanasegaran G, Vijayanathan S, Fogelman I. Potential role of multislice SPECT/CT in impingement syndrome and soft-tissue pathology of the ankle and foot. Nucl Med Commun. (2013) 34:130–9. doi: 10.1097/MNM.0b013e32835c0964
13. Israel O, Pellet O, Biassoni L, De Palma D, Estrada-Lobato E, Gnanasegaran G, et al. Two decades of SPECT/CT - the coming of age of a technology: an updated review of litterature evidence. Eur J Nucl Med Mol Imaging. (2019) 46:1990–2012. doi: 10.1007/s00259-019-04404-6
14. Huellner MW, Strobel K. Clinical applications of SPECT/CT in imaging the extremities. Eur J Nucl Med Mol Imaging. (2014) 41(Suppl. 1):S50–58. doi: 10.1007/s00259-013-2533-5
15. Claassen L, Uden T, Ettinger M, Daniilidis K, Stukenborg-Colsman C, Plaass C. Influence on Therapeutic Decision Making of SPECT-CT for Different Regions of the Foot and Ankle. Biomed Res Int. (2014) 2014:1–5. doi: 10.1155/2014/927576
16. Yoo IR. Bone SPECT/CT of the foot and ankle: potential clinical application for chronic foot pain. Nucl Med Mol Imaging. (2020) 54:1–8. doi: 10.1007/s13139-019-00627-5
17. Gupta SK, Rutherford N, Allen L. SPECT blood pool imaging on bone scintigraphy improves diagnostic yield compared to planar imaging: initial experience. Int J Nucl Medi. (2013) 6:1. Available online at: https://print.ispub.com/api/0/ispub-article/1595
18. Phillips W, Gorzell B, Martinez R, Salman U, Lancaster J, Cooper A. Rapid SPECT/CT blood pool imaging for more accurate localization of infection and inflammation. J Nucl Med. (2017) 58(Suppl. 1):1218. Available online at: https://jnm.snmjournals.org/content/58/supplement_1/1218
19. Aydogan F, Akbay E, Cevik C, Kalender E. Blood-pool SPECT in addition to bone SPECT in the viability assessment in mandibular reconstruction. Eur Rev Med Pharmacol Sci. (2014) 18:587–92.
20. Vaz S, Ferreira TC, Salgado L, Paycha F. Bone scan usefulness in patients with painful hip or knee prosthesis: 10 situations that can cause pain, other than loosening and infection. Eur J Orthop Surg Traumatol. (2017) 27:147–56. doi: 10.1007/s00590-016-1884-6
21. Abdelhafez YG, Hagge RJ, Badawi RD, Raychaudhuri SP, Chaudhari AJ. Early and delayed 99mTc-MDP SPECT/CT findings in rheumatoid arthritis and osteoarthritis. Clin Nucl Med. (2017) 42:480–1. doi: 10.1097/RLU.0000000000001839
22. Işikci NI. Comparison between planar, SPECT and SPECT/computed tomography systems in 99mTc- nanocolloid sentinel lymph node imaging: phantom design and clinical investigations. Nucl Med Commun. (2019) 40:786–91. doi: 10.1097/MNM.0000000000001041
23. Sorensen ES, Zeng GL, Holt B, Scott K, Karen S, Ovard T. Comparison of Planar vs. SPECT Images for Lesion Detectability. Norfolk, VA: IEEE Nuclear Science Symposium Conference Record (2002).
24. Baqer MM, Loutfi I. Optimal imaging positions for 3-phase bone scanning of patients with bony pathology of the feet. J Nucl Med Technol. (2010) 38:69–75. doi: 10.2967/jnmt.109.070771
Keywords: bloodpool SPECT, bone scintigraphy, ankle, foot, early SPECT/CT
Citation: Cuvilliers C, Palard-Novello X, Pontoizeau C, Meneret P, Devillers A, Le Jeune F and Girard A (2021) The Added Value of Bloodpool SPECT/CT in Painful Non-Operated Foot and Ankle Undiagnosed With Standard Three-Phase Bone Scintigraphy. Front. Med. 8:634419. doi: 10.3389/fmed.2021.634419
Received: 27 November 2020; Accepted: 28 January 2021;
Published: 05 March 2021.
Edited by:
Thierry MLB Vander Borght, Catholic University of Louvain, BelgiumReviewed by:
Jeroen Mertens, AZ Maria Middelares, BelgiumDavid John Macfarlane, The University of Queensland, Australia
Copyright © 2021 Cuvilliers, Palard-Novello, Pontoizeau, Meneret, Devillers, Le Jeune and Girard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cécile Cuvilliers, Yy5jdXZpbGxpZXJzQHJlbm5lcy51bmljYW5jZXIuZnI=