
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 26 February 2021
Sec. Nuclear Medicine
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.628179
This article is part of the Research TopicArtificial Intelligence in Positron Emission TomographyView all 13 articles
 Pierre Pinochet1
Pierre Pinochet1 Florian Eude1
Florian Eude1 Stéphanie Becker1,2
Stéphanie Becker1,2 Vijay Shah3Ludovic Sibille3Mathieu Nessim Toledano1
Vijay Shah3Ludovic Sibille3Mathieu Nessim Toledano1 Romain Modzelewski1,2
Romain Modzelewski1,2 Pierre Vera1,2
Pierre Vera1,2 Pierre Decazes1,2*
Pierre Decazes1,2*Introduction: Our aim was to evaluate the performance in clinical research and in clinical routine of a research prototype, called positron emission tomography (PET) Assisted Reporting System (PARS) (Siemens Healthineers) and based on a convolutional neural network (CNN), which is designed to detect suspected cancer sites in fluorine-18 fluorodeoxyglucose (18F-FDG) PET/computed tomography (CT).
Method: We retrospectively studied two cohorts of patients. The first cohort consisted of research-based patients who underwent PET scans as part of the initial workup for diffuse large B-cell lymphoma (DLBCL). The second cohort consisted of patients who underwent PET scans as part of the evaluation of miscellaneous cancers in clinical routine. In both cohorts, we assessed the correlation between manually and automatically segmented total metabolic tumor volumes (TMTVs), and the overlap between both segmentations (Dice score). For the research cohort, we also compared the prognostic value for progression-free survival (PFS) and overall survival (OS) of manually and automatically obtained TMTVs.
Results: For the first cohort (research cohort), data from 119 patients were retrospectively analyzed. The median Dice score between automatic and manual segmentations was 0.65. The intraclass correlation coefficient between automatically and manually obtained TMTVs was 0.68. Both TMTV results were predictive of PFS (hazard ratio: 2.1 and 3.3 for automatically based and manually based TMTVs, respectively) and OS (hazard ratio: 2.4 and 3.1 for automatically based and manually based TMTVs, respectively). For the second cohort (routine cohort), data from 430 patients were retrospectively analyzed. The median Dice score between automatic and manual segmentations was 0.48. The intraclass correlation coefficient between automatically and manually obtained TMTVs was 0.61.
Conclusion: The TMTVs determined for the research cohort remain predictive of total and PFS for DLBCL. However, the segmentations and TMTVs determined automatically by the algorithm need to be verified and, sometimes, corrected to be similar to the manual segmentation.
Positron emission tomography (PET) with fluorine-18 (18F) fluorodeoxyglucose (FDG) has an important contribution in the diagnosis and the management of oncological pathologies by highlighting regions with a high glucidic metabolism (1).
PET can establish an initial staging of tumor lesions (2), enable treatment optimization, and evaluate treatment effectiveness or possible relapse (3–8). It also provides prognostic parameters in certain types of cancer, in particular in onco-hematology, such as the Deauville score, which evaluates the therapeutic response and is used in clinical routine, or the total metabolic tumor volume (TMTV) (9).
TMTV represents, generally on FDG PET, the volume of the entire cancerous disease. It is obtained by segmenting each diagnosed lesion. TMTV has been shown to be an independent prognostic factor in lymphoma (10). Recently, Albano et al. have shown its predictive nature on progression-free survival (PFS) in elderly Hodgkin's lymphoma (11) and mantle cell lymphoma (12), but also on total and PFS in Burkitt lymphoma (13) and cerebral lymphoma (14). However, this parameter has some limitations. The first is that the measurement is time-consuming to make, explained by the fact that each lesion must be segmented individually, a task that cannot be performed manually in clinical practice. The second is the absence of a standard method for the segmentation of hypermetabolic lesions, which is responsible for some variability in the determination of TMTV. Thus, a fixed threshold of SUVmax (for example 41% for lymphomas) for each lesion is frequently used (15). However, this may not be appropriate for all pathological foci, particularly in the case of heterogeneous tumor fixation and adjacent physiological volume with high uptake (16).
A problem frequently encountered during the interpretation and segmentation of the images is differentiating between benign physiological (e.g., brain, heart, liver, kidney, and bladder) or inflammatory foci, and pathological foci suspicious for cancerous lesions. This is particularly true for malignant tumors with a low avidity for glucose, unusual location, or small size or in the presence of attenuation and/or motion artifacts (17). Moreover, inflammatory or infectious foci, or even foci with a high physiological consumption of glucose may have a sufficiently high FDG uptake to make it not possible to eliminate a cancerous origin (18, 19).
Intra- and interobserver interpretation of FDG PET/computed tomography (CT) findings has a high level of agreement in studies involving single site and experienced readers for lymphoma, lung, and head and neck cancers (20–22). Widespread adoption of TMTV would be facilitated by tools to assist image interpretation and standardize results. Automatic segmentation has also proven to be a prerequisite for certain studies, particularly in the field of radiomics.
In recent years, several automatic segmentation methods have been developed. They can be divided into two main groups. The first is based on an ROI placed manually by the physician within which a threshold relative to SUVmax is applied (23–25). The resulting segmentation depends on the defined ROI and is generally not optimal. A second approach, which is less time-consuming and observer-independent, uses supervised machine learning to analyze PET/CT images (26). A research software prototype called PET Assisted Reporting System (PARS), based on convolutional neural networks (CNNs), has recently been developed by Siemens Healthineers to classify hypermetabolic foci into benign and malignant and to provide parameters such as TMTV, total lesion glycolysis (TLG), and Deauville score (27). With this algorithm, PET volumes of interest are first segmented by using a fixed thresholding algorithm. Each volume of interest is then evaluated independently by using a combination of PET and CT multiplanar reconstructions, PET maximum intensity projections (MIPs), and atlas positions to predict the anatomic localization of FDG foci. These are input to a CNN that determines whether a focus is suspicious for malignancy. The training and validation sets were carried out on cohorts of patients with either lung cancer or lymphoma. A first, internal evaluation of this tool showed good accuracy of the automatic segmentation of FDG positive foci, and also good sensitivity and specificity of the classification in staging patients with lung cancer and lymphoma compared with manual segmentation (27).
The aim of this study was to verify the performance of PARS in order to determine its usefulness in research and clinical routine.
This retrospective monocentric study included patients treated at the Henri Becquerel Cancer Center, Rouen, France. Two patient cohorts were analyzed: a first clinical research cohort composed of patients with diffuse large B-cell lymphoma (DLBCL), as TMTV is a well-known prognostic factor for this disease (10), and a second clinical routine cohort composed of patients selected at random and followed up for miscellaneous cancers to evaluate if an automatic measurement of TMTV can be performed in routine. All patients were over 18 years of age. The baseline PET/CT was analyzed for the DLBCL clinical research cohort. For the routine clinical cohort, including patients with suspected or confirmed cancer, a baseline or a follow-up PET/CT was analyzed. The study was approved by the institutional review board (no. 1901B). Patients were informed about the use of anonymized data for research and their right to oppose this use. Fully anonymized data were used, and explicit consent was waived.
Concerning the research cohort, 119 patients followed up for DLBCL were included between November 2004 and September 2014, and their initial FDG PET/CT was analyzed.
PET/CT scans were acquired on a Biograph 16 (Siemens Healthineers, Knoxville, TN, USA). Patients fasted for at least 4 h and were injected with FDG at an activity of 3.5 MBq/kg of body weight. Images were acquired 60 min after injection at 2.5 min per bed position. The manual segmentation of lesions was performed using semiautomatic software (Planet Onco, version 2.0, DOSIsoft®, Cachan, France). A volume of interest was set around each lesion on the PET images. Then a fixed threshold value of 41% of SUVmax was applied to define the volume for each segmented lesion. The volumes of all suspicious lesions in a particular patient were added to compute the TMTV. The manual segmentation was performed by two nuclear physicians for each patient (MT and FE). One of the manual segmentations (MT), chosen arbitrarily, was used for the calculation of the Dice scores. The average of the two TMTVs was used for all other calculations.
Five-year follow-up, including PFS and overall survival (OS), was available for this cohort.
Concerning the routine cohort, 430 patients referred for cancer assessment underwent routine thoraco-abdomino-pelvic or whole body PET/CT (according to the indication), and with at least one tumoral uptake, were included between August 2018 and February 2020.
PET/CT scans were acquired on GE 710 (General Electric, Milwaukee, WI, USA) or Biograph Vision 600 (Siemens Healthineers, Knoxville, TN, USA). Patients fasted for at least 4 h and were injected with FDG at a dose of 3.0 MBq/kg of body weight. Images were acquired 60 min after injection at 2 min per bed position (GE 710) or by continuous bed motion (Biograph Vision).
The manual segmentation of lesions was performed using another semiautomatic software (PET VCAR, General Electric®) during routine clinical activity by two different nuclear medicine physicians (PD and PP). A volume of interest was set around each lesion on the PET images according to an adaptive thresholding (28), manually adapted if necessary according to medical advice. After the database was gathered, a second reading was done in order to check and confirm the suspicious character of the different segmented foci. These values were added to compute the TMTV.
Data of the two cohorts of patients are summarized in Table 1.
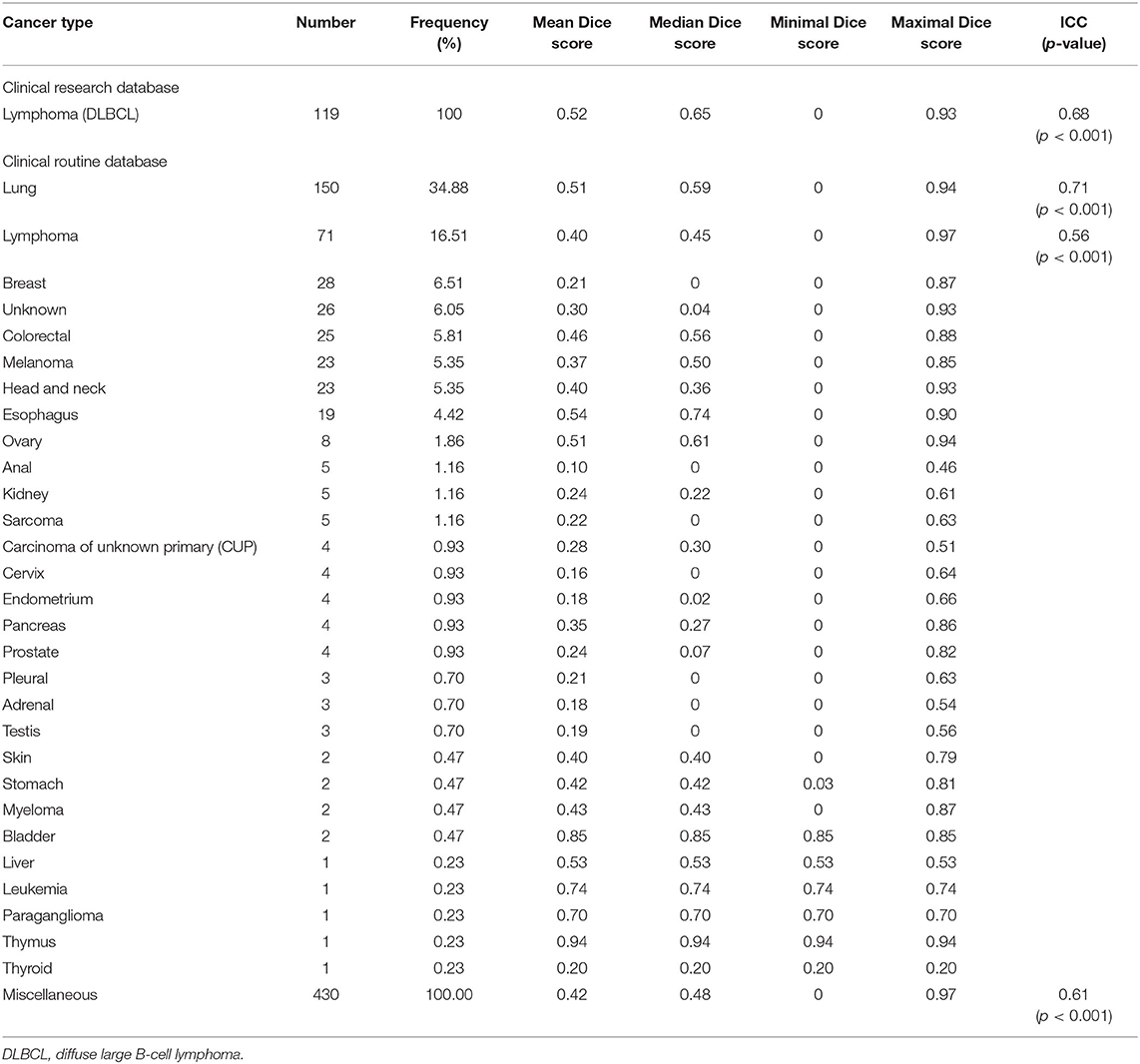
Table 1. Summary results from two patient cohorts.
PET/CT images were analyzed using a software prototype called PARS (Siemens Healthineers, Knoxville, TN, USA). A cylindrical reference region was automatically placed in the center of descending thoracic aorta to measure the mean blood pool uptake (SUVBP). Regions on PET images with SUVpeak greater than SUVBP + 2 stdSUVBP were identified and segmented using 42% of local SUVmax. Only segmentations with volumes over 2 ml (research cohort) or 1 ml (routine cohort) were selected to be processed by the CNN, which specifies location and physiological or suspicious character of the different foci.
For both cohorts, agreement between automatic and manual segmentations was characterized using the Dice score. Differences between TMTVs from PARS and manual segmentation were determined using intraclass correlation coefficient (ICC), notably for subgroups of more than 30 patients. Comparisons were also made by way of Bland–Altman plots.
The prognostic value for PFS and OS for both automatic and manual TMTVs was analyzed in the research cohort. Hazard ratios were calculated on continuous data. Receiver operating characteristic (ROC) curves were used to determine TMTV cutoff thresholds by Youden's index. Survival functions were computed by Kaplan–Meier analyses and used to estimate survival time statistics for low and high TMTV groups with log-rank tests.
Concerning the research cohort, 119 patients were included in the analysis. The median age was 65.8 years. Ninety-three patients had stage 3 or 4 DLBCL according to the Ann Arbor classification. Thirty received first-line treatment with R-ACVBP (doxorubicin, cyclophosphamide, vindesine, bleomycin, prednisone regimen) and 89 with R-CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone regimen). The ICC between the two manual TMTVs was 0.86 (p < 0.001), confirming the reproducibility of the segmentations. The median Dice score across all patients between the set of PARS ROI's labeled as suspicious and the set of manual ROI's was 0.65. The average Dice score was 0.52. The median TMTVPARS was 194.79 ml, maximum 1,821 ml, and minimum 0 ml. The median TMTVmanual was 313.34 ml, maximum 3,304 ml, and minimum 8 ml (Table 1 and Supplementary Figure 1). The ICC between PARS and manual TMTVs was 0.68 (Table 1). Concerning the Bland–Altman plot, the deviation from the mean between TMTVmanual and TMTVPARS was +204 ml with a confidence interval of −554 to +963 ml (see Figure 1A).
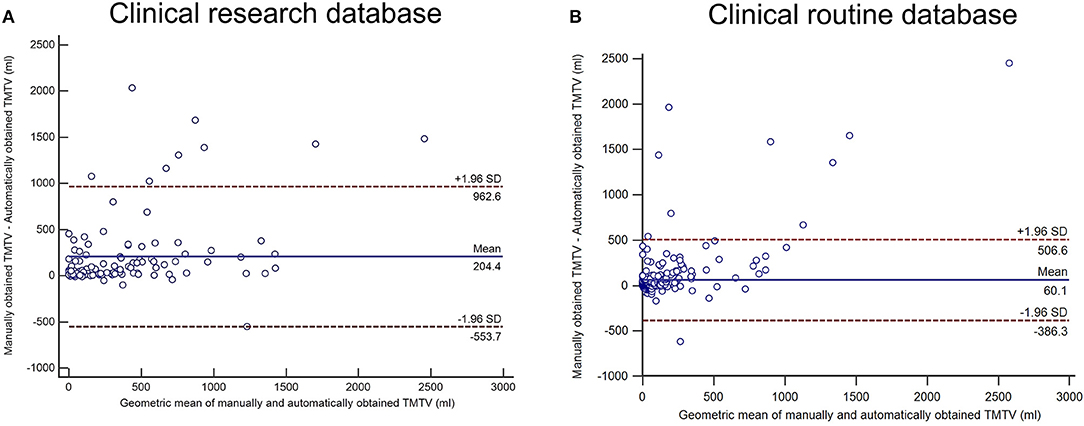
Figure 1. Bland–Altman analysis between manually and automatically obtained total metabolic tumor volumes (TMTVs) for the clinical research cohort (A) and the clinical routine database (B).
After a median follow-up of 5 years, 60 patients presented a recurrence of the disease and 54 deceased. The 5-year survival rates were 49.6% for PFS and 54.6% for OS.
The area under the ROC curve for predicting PFS was 0.62 for TMTVPARS and 0.71 for TMTVmanual (Figures 2A,B). The optimal cutoffs for predicting PFS were 223.09 ml for TMTVPARS and 327.14 ml for TMTVmanual. The 5-year PFS rates were 61.5 and 35.2% for the low- and high-TMTVPARS groups and 69.8% and 26.8% for the low- and high-TMTVmanual groups, respectively (Figures 3A,B). The log-rank test indicated a significantly longer PFS time in the low-TMTV group for both TMTV estimation methods (p = 0.0034 for TMTVPARS and p < 0.0001 for TMTVmanual). Hazard ratios (high-TMTV group vs. low-TMTV group) were 2.1 (range 1.3–3.5) for TMTVPARS and 3.3 (range 2.0–5.6) for TMTVmanual.
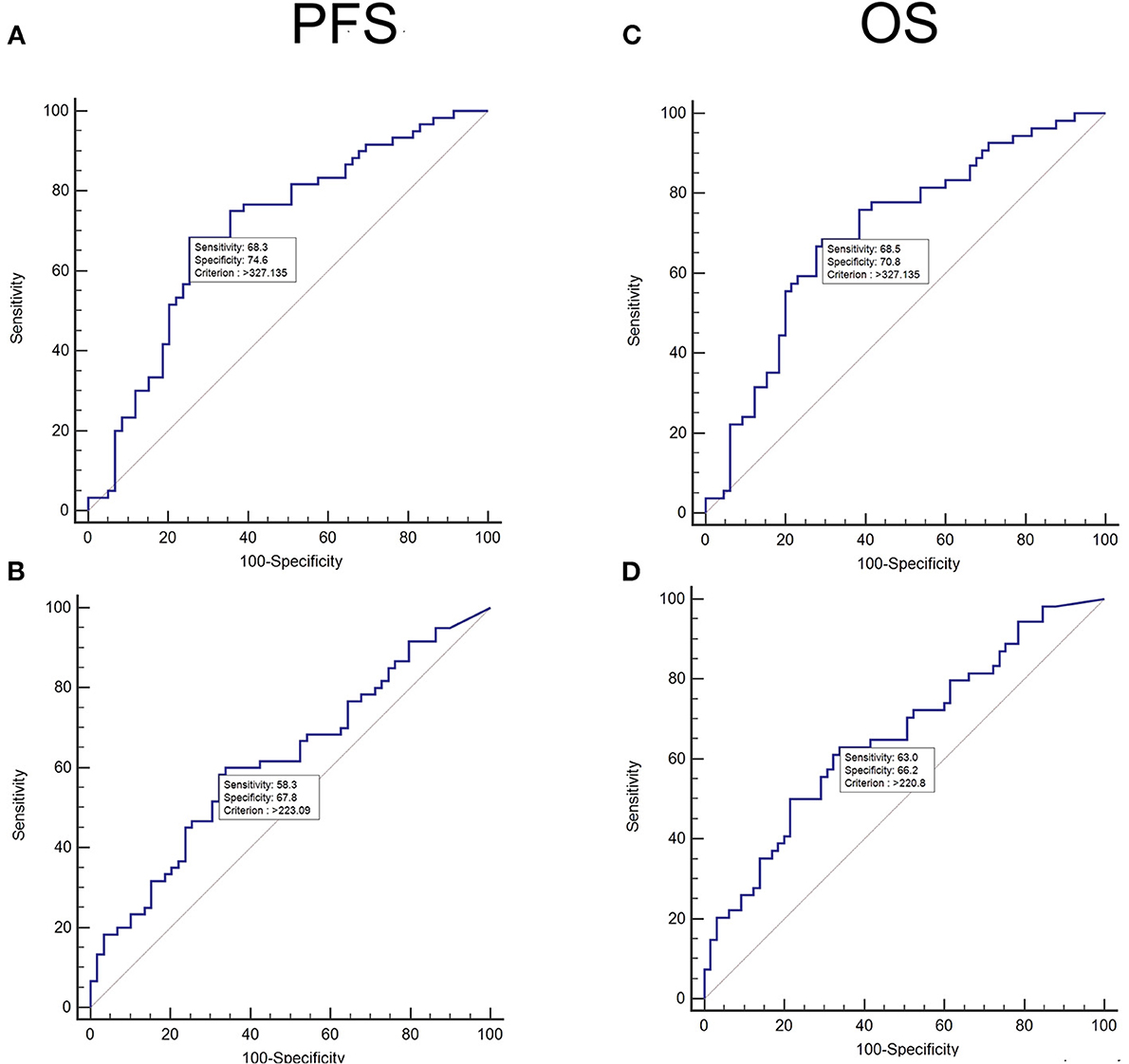
Figure 2. Receiver operating characteristic (ROC) curve analysis of the population of diffuse large B-cell lymphomas (clinical research database) for progression-free survival (PFS) for manually obtained total metabolic tumor volumes (TMTVs) (A) and automatically obtained TMTVs (B) and for overall survival (OS) for manually obtained TMTVs (C) and automatically obtained TMTVs (D).
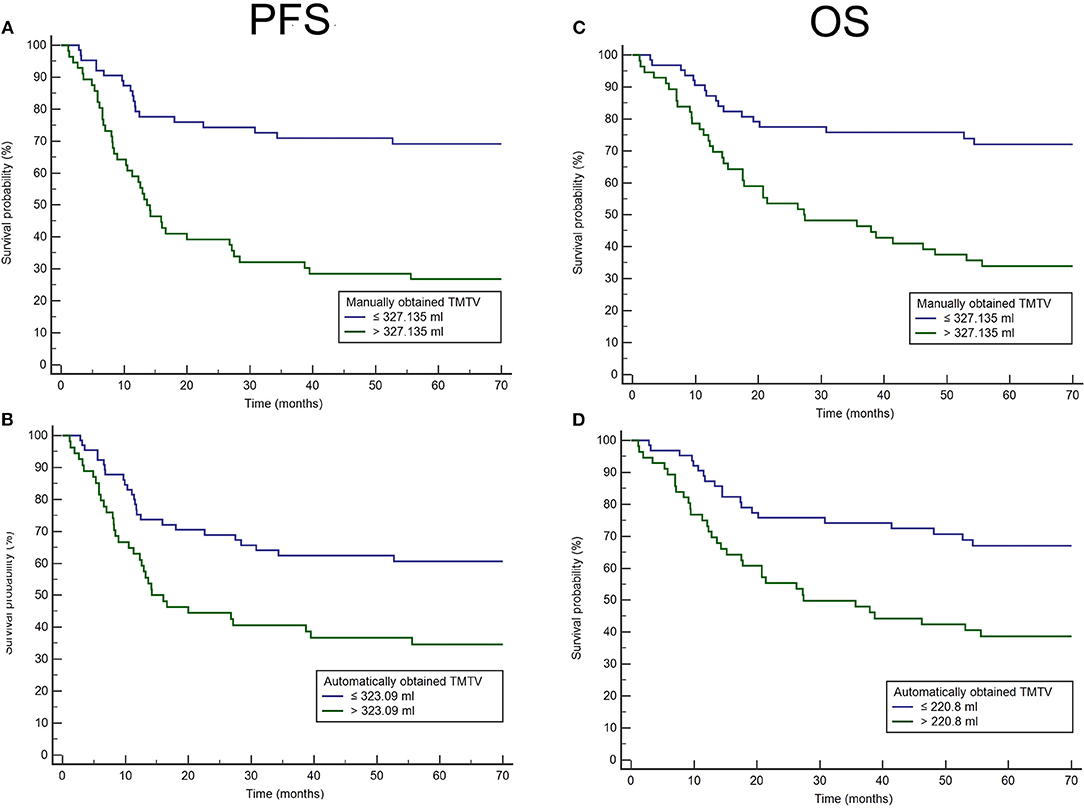
Figure 3. Kaplan–Meier analysis of the population of diffuse large B-cell lymphomas (clinical research database) for progression-free survival (PFS) for manually obtained total metabolic tumor volumes (TMTVs) (A) and automatically obtained TMTVs (B) and for overall survival (OS) for manually obtained TMTVs (C) and automatically obtained TMTVs (D).
For OS, the area under the ROC curve was 0.66 for TMTVPARS and 0.71 for TMTVmanual (Figures 2C,D). The optimal cutoffs for predicting OS were 220.80 ml for TMTVPARS and 327.14 ml for TMTVmanual. The 5-year OS rates were 68.3 and 39.3% for the low- and high-TMTVPARS groups and 73.0% and 33.9% for the low- and high-TMTVmanual groups, respectively (Figures 3C,D). The log-rank test indicated a significantly longer PFS time in the low-TMTV group for both TMTV estimation methods (p = 0.0016 for TMTVPARS and p = 0.0001 for TMTVmanual). Hazard ratios (high-TMTV group vs. low-TMTV group) were 2.4 (range 1.4–4.1) for TMTVPARS and 3.1 (range 1.8–5.3) for TMTVmanual.
Concerning the routine cohort, 430 patients were analyzed; 35% of them had lung cancer, 17% lymphoma, 7% breast cancer, 6% colorectal cancer, 5% melanoma, 5% head and neck cancer, 4% esophageal cancer, and 15% another cancer. In 6% of the cases, the patients were followed up in another center, and we did not have the proven cancer origin.
The median Dice score across all patients between the suspicious PARS ROIs and the manual ROIs was 0.48. The average Dice score was 0.42. For automatic segmentation, median TMTV was 7.37 ml, maximum TMTV was 1,626.97 ml, and minimum TMTVs was 0.00 ml. For manual segmentation, median TMTV was 20.09 ml, maximum TMTV was 4,076.63 ml, and minimum TMTV was 1.00 ml (Table 1 and Supplementary Figure 1). The intraclass coefficient between PARS and manual TMTV was 0.61 (Table 1). Concerning Bland–Altman plot, the deviation from the mean between TMTVmanual and TMTVPARS was +60 ml with a confidence interval of −386 to +506 ml (see Figure 1B).
We analyzed an automatic segmentation software prototype using CNN in PET to distinguish hypermetabolic foci suspicious for cancer from nonsuspicious foci in two distinct cohorts of patients.
The first of these cohorts consisted of 119 patients with DLBCL, a disease used for the training of the model and for which the prognostic value of TMTV is well known (10). The median overlapping score of automatic and manual segmentation estimated by the Dice coefficient was 0.65. The ICC between automatically and manually determined TMTVs was 0.68. As follow-up was available for this cohort, survival analysis based on volume thresholds determined by the ROC curves showed that automatically determined TMTVs remained a predictive factor for PFS and OS, but hazard ratios were however lower than for manually determined TMTVs.
The second cohort consisted of 430 patients with a variety of cancers who were referred for PET/CT evaluation. The aim of the analysis of this cohort was to determine the possible utility of the algorithm for clinical routine, in terms of speed and reliability of the analysis of the different foci, and the estimation of the TMTVs. The median overlapping score of automatic and manual segmentation estimated by the Dice coefficient was 0.48. The ICC between automatically and manually determined TMTVs was 0.61.
The scanner type and acquisition parameters were different between the two cohorts. However, the results obtained were relatively similar despite these differences. Moreover, the manual segmentation methods differed (fixed threshold for the clinical research cohort and adaptive threshold for the routine cohort), but this did not greatly influence the results. The use of the 41% SUVmax thresholding method has been published in the context of DLBCLs and is a standard in clinical research (15), although much discussed (16). In particular, this method is difficult to use in clinical routine where tumor lesions are often smaller than those observed in DLBCL where a threshold of 41% of the SUVmax becomes unsuitable because of the partial volume effect for small lesions (29).
Finally, in the PARS configuration, to limit the computation time without impacting the TMTV measurement, only segmentations with volumes over 1 ml in the routine cohort were analyzed, as potentially small tumors were observed while the limit of 2 ml was used in the research cohort, as DLBCLs present generally large tumors.
In recent years, a number of algorithms have been developed that focus on PET segmentation, mainly in lymphoma, using different branches of artificial intelligence (30–32). In particular, machine learning using CNNs is a major advance in medical imaging. In PET, this technology stands to assist the nuclear physician's interpretation by facilitating, or even refining, the analysis. Concerning lymphomas, and DLBCL particularly, TMTV is usually not calculated during pretherapeutic PET/CT because it takes too long to determine using manual segmentation. Automatic or semiautomatic determination of TMTV could enable clinicians to integrate it in the determination of prognosis and therapeutic adaptation.
PARS is among the first published and validated CNN algorithms for PET/CT lesion classification (21). It was developed to detect FDG foci, and to predict the anatomic location and the expert classification (i.e., suspicious or not suspicious for cancer). It was trained on 380 examinations of patients with lung cancer or lymphoma with a validation set of 126 examinations and a test set of 123 patients (21).
In a recent study (33), the PARS software prototype was tested on a cohort of 280 patients with DLBCL. As with this study, we have established the ability to determine the prognosis of DLBCL using automatic segmentation. The authors however obtained a better lymphomatous lesion recovery coefficient (Dice) of 0.73 and a better TMTV correlation of 0.76. The automatically determined TMTVs were, as in our study, predictive of total and PFS with hazard ratios of 2.8 and 2.4, respectively. The difference in Dice coefficients and TMTV correlation could be explained by the difference in the populations.
Our results are consistent with a recent study (34), in which the performances of a CNN model, based on nnU-Net, were investigated to automatically segment TMTV in patients with DLBCL. A first cohort of 639 patients with pretherapeutic FDG PET/CT was used to train the model. In this cohort, the mean Dice score and Jaccard coefficients for manual and automatic segmentations were 0.73 and 0.68, respectively. There was a mean underestimation of automatic TMTV by 12 ml (p = 0.27). An external validation was done on a second cohort of 94 patients. In this testing set, the mean underestimation of automatically determined TMTV was 116 ml, which was statistically significant (p = 0.01).
Concerning the clinical routine database, we chose to analyze the examinations of patients followed for any cancerous pathology, whereas the model was trained only on lung cancer and lymphomas. This approach corresponds well to the clinical routine where the pathology is variable, and the results remain consistent with those of the research cohort. Nevertheless, the results are more similar to those obtained for the research cohort, which is closer to the training conditions of the algorithm.
Although promising, the PARS software prototype tends, in this study, to underestimate the number of cancerous foci, leading to some false-negative cases (see Figure 4). For both clinical research and clinical routine cohorts, the results obtained suggest that a manual check is still needed after the automatic segmentation.
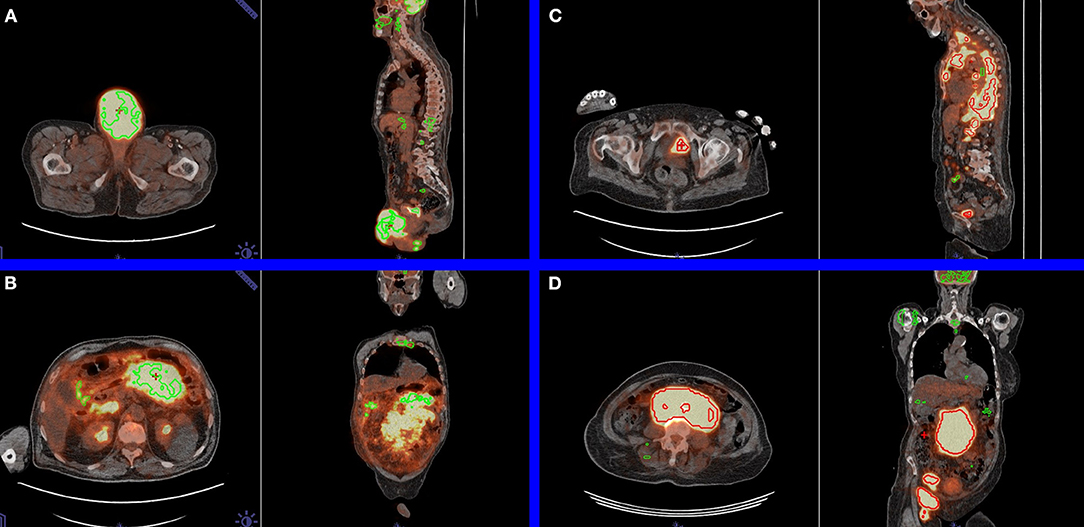
Figure 4. Examples in axial and sagittal views of limitations of the automatic segmentation. (A) Pathological testicular mass labeled as physiological by positron emission tomography Assisted Reporting System (PARS) (false negative). For this patient, the manually and automatically obtained total metabolic tumor volumes (TMTVs) were 281.18 and 5.18 ml, respectively. (B) Pathological mesenteric mass was erroneously labeled as physiological by PARS (false negative). For this patient, the manually and automatically obtained TMTVs were 2,125.38 and 89.35 ml, respectively. (C) Physiological urinary bladder focus was erroneously labeled as pathological by PARS (false positive). For this patient, the manually and automatically obtained TMTVs were 816.94 and 661.08 ml, respectively. (D) Pathological mesenteric mass was correctly labeled as pathological by PARS (true positive). For this patient, the manually and automatically obtained TMTVs were 1,369.19 and 1,343.88 ml, respectively.
The purpose of our study was to evaluate the software prototype PARS, which applies CNNs to detect carcinologically suspicious foci of hypermetabolism in FDG PET scans. The total tumor metabolic volumes determined by PARS were predictive of OS and PFS for patients belonging to the DLBCL research cohort. The segmentations and TMTVs determined automatically by the algorithm need to be verified and, sometimes, corrected to be similar to the manual segmentation in both clinical research and clinical routine.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by Henri Becquerel Center Internal Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
PD is the guarantor of the paper. PD, PV, RM, and PP designed the study. PD, SB, PP, and MT ensured inclusion and follow-up of patients. PP, FE, MT and PD managed imaging procedures. PP, PD and PV analyzed the data. LS and VS developed the software prototype. All authors contributed in drawing up the manuscript.
LS and VS are employees of the company Siemens Healthineers.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.628179/full#supplementary-material
Supplementary Figure 1. Boxplot showing the distribution of the Dice scores for the research cohort (DLBCL) and for the routine cohort (miscellaneous, lung cancer, and lymphoma).
1. Kostakoglu L, Agress H, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer patients. RadioGraphics. (2003) 23:315–40. doi: 10.1148/rg.232025705
2. El-Galaly TC, Gormsen LC, Hutchings M. PET/CT for staging; past, present, and future. Sem Nucl Med Medicine. (2018) 48:4–16. doi: 10.1053/j.semnuclmed.2017.09.001
3. Oyen WJ, Bussink J, Verhagen AF, Corstens FH, Bootsma GP. Role of FDG-PET in the diagnosis and management of lung cancer. Exp Rev Anticancer Ther. (2004) 4:561–7. doi: 10.1586/14737140.4.4.561
4. Kandathil A, Iii RCS, Subramaniam RM. Lung cancer recurrence: 18 F-FDG PET/CT in clinical practice. Am J Roentgenol. (2019) 213:1136–44. doi: 10.2214/AJR.19.21227
5. Szyszko TA, Cook GJR. PET/CT and PET/MRI in head and neck malignancy. Clin Radiol. (2018) 73:60–9. doi: 10.1016/j.crad.2017.09.001
6. Kemppainen J, Hynninen J, Virtanen J, Seppänen M. PET/CT for evaluation of ovarian cancer. Sem Nucl Med Medicine. (2019) 49:484–92. doi: 10.1053/j.semnuclmed.2019.06.010
7. Gandy N, Arshad MA, Park W-HE, Rockall AG, Barwick TD. FDG-PET imaging in cervical cancer. Sem Nucl Med Medicine. (2019) 49:461–70. doi: 10.1053/j.semnuclmed.2019.06.007
8. Ulaner GA. PET/CT for patients with breast cancer: where is the clinical impact? Am J Roentgenol. (2019) 213:254–65. doi: 10.2214/AJR.19.21177
9. Cheson BD. PET/CT in lymphoma: current overview and future directions. Sem Nucl Med. (2018) 48:76–81. doi: 10.1053/j.semnuclmed.2017.09.007
10. Guo B, Tan X, Ke Q, Cen H. Prognostic value of baseline metabolic tumor volume and total lesion glycolysis in patients with lymphoma: a meta-analysis. PLoS ONE. (2019) 14:e0210224. doi: 10.1371/journal.pone.0210224
11. Albano D, Mazzoletti A, Spallino M, Muzi C, Zilioli VR, Pagani C, et al. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in elderly HL: a two-center experience in 123 patients. Ann Hematol. (2020) 99:1321–1330. doi: 10.1007/s00277-020-04039-w
12. Albano D, Bosio G, Bianchetti N, Pagani C, Re A, Tucci A, et al. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in mantle cell lymphoma. Ann Nucl Med. (2019) 33:449–58. doi: 10.1007/s12149-019-01354-9
13. Albano D, Bosio G, Pagani C, Re A, Tucci A, Giubbini R, et al. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in Burkitt lymphoma. Eur J Nucl Med Mol Imaging. (2019) 46:87–96. doi: 10.1007/s00259-018-4173-2
14. Albano D, Bertoli M, Battistotti M, Rodella C, Statuto M, Giubbini R, et al. Prognostic role of pretreatment 18F-FDG PET/CT in primary brain lymphoma. Ann Nucl Med. (2018) 32:532–41. doi: 10.1007/s12149-018-1274-8
15. Meignan M, Sasanelli M, Casasnovas RO, Luminari S, Fioroni F, Coriani C, et al. Metabolic tumour volumes measured at staging in lymphoma: methodological evaluation on phantom experiments and patients. Eur J Nucl Med Mol Imaging. (2014) 41:1113–22. doi: 10.1007/s00259-014-2705-y
16. Ilyas H, Mikhaeel NG, Dunn JT, Rahman F, Møller H, Smith D, et al. Defining the optimal method for measuring baseline metabolic tumour volume in diffuse large B cell lymphoma. Eur J Nucl Med Mol Imaging. (2018) 45:1142–54. doi: 10.1007/s00259-018-3953-z
17. Griffeth LK. Use of Pet/Ct scanning in cancer patients: technical and practical considerations. Baylor Univ Med Center Proc. (2005) 18:321–30. doi: 10.1080/08998280.2005.11928089
18. Vaidyanathan S, Patel CN, Scarsbrook AF, Chowdhury FU. FDG PET/CT in infection and inflammation—current and emerging clinical applications. Clin Radiol. (2015) 70:787–800. doi: 10.1016/j.crad.2015.03.010
19. Rahman WT, Wale DJ, Viglianti BL, Townsend DM, Manganaro MS, Gross MD, et al. The impact of infection and inflammation in oncologic 18F-FDG PET/CT imaging. Biomed Pharm. (2019) 117:109168. doi: 10.1016/j.biopha.2019.109168
20. Hofman MS, Smeeton NC, Rankin SC, Nunan T, O'Doherty MJ. Observer variation in interpreting 18F-FDG PET/CT findings for lymphoma staging. J Nuclear Med. (2009) 50:1594–597. doi: 10.2967/jnumed.109.064121
21. Hofman MS, Smeeton NC, Rankin SC, Nunan T, O'Doherty MJ. Observer variation in FDG PET-CT for staging of non-small-cell lung carcinoma. Eur J Nucl Med Mol Imaging. (2009) 36:194–9. doi: 10.1007/s00259-008-0946-3
22. Senft A, de Bree R, Golding RP, Comans EFI, Van Waesberghe J-HTM, Kuik JD, et al. Interobserver variability in chest ct and whole body FDG-PET screening for distant metastases in head and neck cancer patients. Mol Imaging Biol. (2011) 13:385–90. doi: 10.1007/s11307-010-0354-5
23. Black QC, Grills IS, Kestin LL, Wong C-YO, Wong JW, Martinez AA. Defining a radiotherapy target with positron emission tomography. Int J Rad Oncol Biol Phys. (2004) 60:1272–82. doi: 10.1016/j.ijrobp.2004.06.254
24. Tylski P, Stute S, Grotus N, Doyeux K, Hapdey S, Gardin I, et al. Comparative assessment of methods for estimating tumor volume and standardized uptake value in 18F-FDG PET. J Nucl Med. (2010) 51:268–76. doi: 10.2967/jnumed.109.066241
25. Vauclin S, Doyeux K, Hapdey S, Edet-Sanson A, Vera P, Gardin I. Development of a generic thresholding algorithm for the delineation of 18 FDG-PET-positive tissue: application to the comparison of three thresholding models. Phys Med Biol. (2009) 54:6901–16. doi: 10.1088/0031-9155/54/22/010
26. Yasaka K, Akai H, Kunimatsu A, Kiryu S, Abe O. Deep learning with convolutional neural network in radiology. Jpn J Radiol. (2018) 36:257–72. doi: 10.1007/s11604-018-0726-3
27. Sibille L, Seifert R, Avramovic N, Vehren T, Spottiswoode B, Zuehlsdorff S, Schäfers M. 18 F-FDG PET/CT uptake classification in lymphoma and lung cancer by using deep convolutional neural networks. Radiology. (2020) 294:445–52. doi: 10.1148/radiol.2019191114
28. Doyeux K, Vauclin S, Hapdey S, Daouk J, Edet-Sanson A, Vera P, et al. Reproducibility of the adaptive thresholding calibration procedure for the delineation of 18F-FDG-PET-positive lesions. Nucl Med Commun. (2013) 34:432–8. doi: 10.1097/MNM.0b013e32835fe1f4
29. Berthon B, Marshall C, Edwards A, Evans M, Spezi E. Influence of cold walls on PET image quantification and volume segmentation: A phantom study: Influence of cold walls on PET image quantification and volume segmentation. Med Phys. (2013) 40:082505. doi: 10.1118/1.4813302
30. Yu Y, Decazes P, Gardin I, Vera P, Ruan S. 3D lymphoma segmentation in PET/CT images based on fully connected CRFs. In: Cardoso MJ, Arbel T, Gao F, Kainz B, van Walsum T, Shi K, Bhatia KK, Peter R, Vercauteren T, Reyes M, editors. Molecular Imaging, Reconstruction Analysis of Moving Body Organs. Cham: Springer International Publishing (2017). p. 3–12. doi: 10.1007/978-3-319-67564-0_1
31. Hu H, Decazes P, Vera P, Li H, Ruan S. Detection and segmentation of lymphomas in 3D PET images via clustering with entropy-based optimization strategy. Int J CARS. (2019) 14:1715–24. doi: 10.1007/s11548-019-02049-2
32. Yu Y, Decazes P, Lapuyade-Lahorgue J, Gardin I, Vera P, Ruan S. Semi-automatic lymphoma detection and segmentation using fully conditional random fields. Comp Med Imag Grap. (2018) 70:1–7. doi: 10.1016/j.compmedimag.2018.09.001
33. Capobianco N, Meignan MA, Cottereau A-S, Vercellino L, Sibille L, Spottiswoode B, et al. Deep learning FDG uptake classification enables total metabolic tumor volume estimation in diffuse large B-cell lymphoma. J Nucl Med. (2021). 62:30–6. doi: 10.2967/jnumed.120.242412
34. Blanc-Durand P, Jégou S, Kanoun S, Berriolo-Riedinger A, Bodet-Milin C, Kraeber-Bodéré F, et al. Fully automatic segmentation of diffuse large B cell lymphoma lesions on 3D FDG-PET/CT for total metabolic tumour volume prediction using a convolutional neural network. Eur J Nucl Med Mol Imaging. (2020). doi: 10.1007/s00259-020-05080-7. [Epub ahead of print].
Keywords: positron emission tomography, convolutional neural network, diffuse large B cell lymphoma (DLBCL), artificial intelligence-AI, fluorodeoxyglucose (18F-FDG)
Citation: Pinochet P, Eude F, Becker S, Shah V, Sibille L, Toledano MN, Modzelewski R, Vera P and Decazes P (2021) Evaluation of an Automatic Classification Algorithm Using Convolutional Neural Networks in Oncological Positron Emission Tomography. Front. Med. 8:628179. doi: 10.3389/fmed.2021.628179
Received: 11 November 2020; Accepted: 25 January 2021;
Published: 26 February 2021.
Edited by:
Xiaoli Lan, Huazhong University of Science and Technology, ChinaReviewed by:
Domenico Albano, University of Brescia, ItalyCopyright © 2021 Pinochet, Eude, Becker, Shah, Sibille, Toledano, Modzelewski, Vera and Decazes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre Decazes, cGllcnJlLmRlY2F6ZXNAY2hiLnVuaWNhbmNlci5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.