 Likke Prawidya Putri
Likke Prawidya Putri Deborah Jane Russell
Deborah Jane Russell Belinda Gabrielle O'Sullivan
Belinda Gabrielle O'Sullivan Rebecca Kippen
Rebecca Kippen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 13 May 2021
Sec. Family Medicine and Primary Care
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.594695
This article is part of the Research Topic Effective Strategies To Develop Rural Health Workforce In Low and Middle-Income Countries (LMICs) View all 15 articles
Background: Doctor shortages in remote areas of Indonesia are amongst challenges to provide equitable healthcare access. Understanding factors associated with doctors' work location is essential to overcome geographic maldistribution. Focused analyses of doctors' early-career years can provide evidence to strengthen home-grown remote workforce development.
Method: This is a cross-sectional study of early-career (post-internship years 1–5) Indonesian doctors, involving an online self-administered survey on demographic characteristics, and; locations of upbringing, medical clerkship (placement during medical school), internship, and current work. Multivariate logistic regression was used to test factors associated with current work in remote districts.
Results: Of 3,176 doctors actively working as clinicians, 8.9% were practicing in remote districts. Compared with their non-remote counterparts, doctors working in remote districts were more likely to be male (OR 1.5,CI 1.1–2.1) or unmarried (OR 1.9,CI 1.3–3.0), have spent more than half of their childhood in a remote district (OR 19.9,CI 12.3–32.3), have completed a remote clerkship (OR 2.2,CI 1.1–4.4) or internship (OR 2.0,CI 1.3–3.0), currently participate in rural incentive programs (OR 18.6,CI 12.8–26.8) or have previously participated in these (OR 2.0,CI 1.3–3.0), be a government employee (OR 3.2,CI 2.1–4.9), or have worked rurally or remotely post-internship but prior to current position (OR 1.9,CI 1.2–3.0).
Conclusion: Our results indicate that building the Indonesian medical workforce in remote regions could be facilitated by investing in strategies to select medical students with a remote background, delivering more remote clerkships during the medical course, deploying more doctors in remote internships and providing financial incentives. Additional considerations include expanding government employment opportunities in rural areas to achieve a more equitable geographic distribution of doctors in Indonesia.
More than 90% of the population in the Asia Pacific region live in low- and middle-income countries (LMICs). Of these, nearly two-thirds reside in rural areas. Many of these countries have fewer than one doctor per 1,000 population (1). This, compounded by significant geographical maldistribution of doctors, means that the doctor-to-population ratios in some rural or remote regions is 10–75% lower than in urban areas of the same country (2–6). As doctor shortages negatively affect access to care, the World Health Organization (WHO) has recommended policies to increase health-workforce supply in rural and remote areas around four key dimensions: (1) educational, including interventions aimed at the medical training phase; (2) regulatory, including mandated rural postings and expanding the authorities of rural health workers; (3) financial incentive provisions; and (4) personal and professional supports, including strategies to provide various living amenities and facilitate professional development of the rural health workforce (7).
Studies highlight successful rural pathway initiatives in increasing rural doctor supply, that expand from medical student selection processes, offering rural medical training, and extend to providing exposure to rural clinical settings (8–13). Selection of at least 25% of medical students from a rural background and providing at least a year of rural clinical training during medical school have been successful in increasing the proportion of doctors working rurally in Australia (9, 10, 14–16). Thailand's comprehensive strategies to recruit medical students from rural regions, clinical clerkships in rural settings and provide scholarships tied to compulsory return-of-service, have jointly led to higher rural doctor retention (17, 18). China's rural-oriented tuition-waived medical education (RTME), which combines targeted recruitment of medical students from rural areas and obligatory rural service at the end of the qualification, was associated with a 12% increase in the number of rural physicians within 4 years (19).
Studies also emphasized the importance of intervention beyond medical education to recruit more doctors working rurally. The initial job upon graduation has been found to be critical in influencing work turnover among doctors in India (20). Internship, as a physician's first job, has potential to sustain the rural pathway of medical education. Doctors with an internship in non-metropolitan areas were more likely to practice in the same areas subsequently (21, 22). Compulsory or voluntary rural postings in Chile and the Philippines, mainly targeting junior doctors, also have potential to influence future practice locations of medical graduates (23).
This study focuses on Indonesia, a country with 1 doctor for every 4,300 people (24), substantially below the WHO recommendation of 1 per 1,000 (25). Eleven per cent of Indonesia's population resides in 122 government-defined remote districts (26). On average, remote districts have a doctor-to-population ratio of 1 per 6,180 population, and a doctor-to-area ratio of 1 per 170 km2, which contrasts with non-remote districts which are much better supplied, having average ratios of 1 doctor per 4,150 population and 1 doctor per 20 km2 (24). Besides the limited infrastructure and lack of health facilities, such geographically imbalanced distribution may be influenced by the decentralization systems that give district governments the authority to hire and fire health workers (27, 28).
As of 2020, Indonesia had 88 medical schools—59% of which are privately owned—producing around 10,000 graduates annually. Undergraduate medical education in Indonesia involves 3–4 years of basic medical science (mostly in a classroom setting) and 1–2 years of clerkship or clinical placements in teaching hospitals and the community. After completing medical school, doctors complete a one-year-long medical internship which involves them practicing under supervision in hospitals and primary healthcare facilities (29). This mandated year of internship was introduced in 2010 in selected districts, then rolled out nationally in 2014. Upon completion of the internship, doctors can obtain registration to practice as a general practitioner without any further training required. An additional 3–5 years of post-graduate fellowship is required to pursue other specializations. These fellowships are mostly located in teaching and teaching-affiliated hospitals in urban areas.
In Indonesia, strategies to improve the geographic distribution of doctors have been implemented since the 1980s. Two are ongoing. The first is an opt-in post-internship rural program with a financial incentive (referred to as the “rural incentive program”). The programs run for 1–2 years with the possibility of extension, and are managed by either the national government (Nusantara Sehat, with an average 100 places annually) or district governments (Pegawai Tidak Tetap/PTT or voluntary contractual employment, annual national number of places undocumented). Nusantara Sehat requires doctors to be unmarried and younger than 35 years. It provides doctors with around IDR11,000,000 (USD782) of monthly income from the national government, while the PTT doctors' monthly incomes vary from IDR4,000,000 to IDR20,000,000 (USD284-1422). These incomes are higher than the base salary for government-employed doctors of IDR2,700,000 (USD192) (30). The second strategy is the expansion of the medical internship program to include more districts for intern postings. This has resulted in 46% of interns being deployed to rural districts, and 14% to remote districts (29).
There are some early signs that geographic distribution of doctors has improved since these strategies were implemented. From 2014 to 2018, the doctor-to-population ratio in Indonesia's remote districts increased from an average of 1 per 7,060 to 1 per 6,180 population, reflecting remote-population growth of 4% and a 19% increase in the number of remotely located doctors (31, 32). However, the factors that specifically relate to better geographic distribution remain under-researched. While location of origin has been revealed as one of the reasons for doctors working in rural or remote Indonesia (33, 34), no study has explored the association between location of undergraduate education and subsequent work. Dasman et al. (35) reported that poor experience during rural internship demotivated young doctors from continuing to work in rural areas (35), yet, the study was limited to one Indonesian province.
This paper addresses the evidence gap by investigating factors associated with Indonesian doctors working in remote districts. The focus is on doctors within 5 years post-internship, as this is a period when the Indonesian government uses strategies to improve doctors' geographic distribution. In addition, location choices made at the key formative early-career stage may impact subsequent work location preferences (20, 36). Understanding these factors would inform future design of effective policies and programs.
A cross-sectional nationwide online survey was administered to Indonesian early-career doctors who, at the time of data collection, were at post-internship years 1–5. Because surveys among physicians generally have low response rates, especially when done online (37, 38), we invited the entire cohort of medical graduates who completed their internship between 2015 and 2018 to participate (referred to hereafter as the “MoH internship population”), offering vouchers in a raffle to improve participation. The email invitations to participate in the survey were sent by the Indonesian Ministry of Health (MoH), which holds medical graduates' contact information collected at the time of internship application. The survey was anonymous, administered using Qualtrics™ and in the Indonesian language, with informed opt-in consent from all participating doctors. Ethics approval for the survey was obtained from the Monash University Human Research Ethics Committee, approval number 16922.
Survey questions were drawn from national-scale medical workforce surveys in other countries, including Australia's MABEL survey (Medicine in Australia: Balancing Employment and Life) (39), the Community Service Officers Exit Survey in South Africa (40), a medical students survey in China (41) and several LMICs surveys (42, 43). These were adapted to the Indonesian context, based on a comprehensive literature review that specifically sought to hypothesize factors associated with rural practice in the Asia-Pacific LMICs context.
The survey questions, wording, and structure were extensively discussed and revised by the research team of experienced rural health workforce researchers. The team also consulted with 2 Indonesian MoH staff with experience in medical workforce and 3 Indonesian academics in health workforce policy, to inform the brevity and accuracy of the survey, relative to the research question. Two survey pilots were conducted in December 2018 to January 2019, and May 2019, with volunteer early-career Indonesian doctors. Pilot feedback was used to further refine the survey instrument, including reducing the length—from 48 to 34 questions—and rewording some questions. The final administered survey (see Supplementary Material) covered: undergraduate training and internship; location of upbringing; current and past work experiences; and demographic characteristics. The survey was online for 5 weeks between August and September 2019, and extended for 2 weeks in October 2019.
We used summary statistics to describe respondent characteristics, and multivariate logistic regression to estimate associations between a range of factors of interests (independent variables) and the key outcome (dependent variable) which was “currently working in remote district”. Remote districts referred to those classified as underdeveloped by Presidential Regulation 131/2015, based on measures of geographic characteristics, socioeconomic status, human resources, built infrastructure, fiscal capacity, accessibility, and vulnerabilities to natural disaster (44). On average, remote districts have significantly worse doctor-to-population and doctor-to-area ratios than do non-remote districts. Remote districts are also targeted for affirmative policies, including for allocation of special funds and targeting of educational and health programs (45, 46).
To further explore the effects of locational independent variables—including location(s) of the doctors' upbringing, medical school, medical clerkships and internship—non-remote districts were further classified into rural and urban. Non-remote districts were classified as rural if they had at least 50% of residents living in rural villages, while the remainder were classified as urban (47). The use of this urban-rural taxonomy is widely-applied in Indonesian studies, with rural areas more likely to have poorer health service quality and utilization (48, 49). In total, there are 122 remote districts, 264 rural districts, and 128 urban districts in Indonesia (Figure 1).
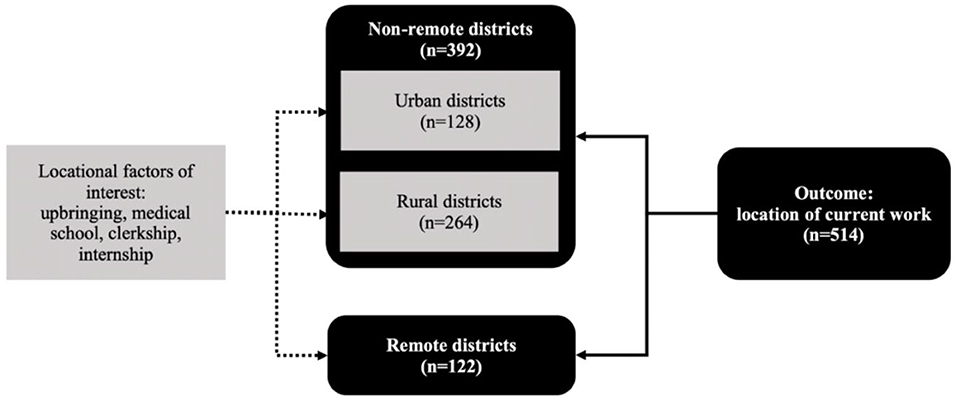
Figure 1. Classifications of outcome and locational factors of interest.
Location of upbringing was classified based on the response to the question “In what province, district, and sub-district did you live the longest up to the age of 18?”. Medical school location was based on the response to “In what medical school in Indonesia did you complete your basic medical degree?” For clerkship location, respondents were asked to list up to three sites (province and district) where their clerkships were based. These locations were coded as remote, rural or urban.
Respondents were asked whether they were participating in specific workforce programs (Nusantara Sehat/PTT/company doctor/others). Those in Nusantara Sehat and PTT were classified as “currently in a rural incentive program” and others as “currently not in a rural incentive program.” We also collected information on: previous post-internship work in any rural or remote location (Nusantara Sehat/PTT/Others), whether they were government employees (Yes/No), gender (Female/Male/Other), and relationship status (Unmarried/Married with children/Married with no children).
StataIC-v13 (StataCorp) was used for all statistical analyses. We performed univariate analyses to investigate associations between the outcome and each of the factors of interest. To identify potential collinearity, univariate regression was also performed between the factors of interest; those with weak association with the outcome (p-value > 0.05) were excluded in the multivariate model, except for age. Missing responses were categorized as “unknown” to retain them in the final modeling, which used listwise deletion. To investigate sample representativeness, data on gender, medical school type, internship location, and Nusantara Sehat participation of the respondents were compared with aggregate data on the MoH internship population.
Of 31,510 emails sent to the MoH internship population, 17,981 were opened (57% contact rate). The email announcement and WhatsApp announcement yielded 5,199 responses downloadable via Qualtrics (29% of the contact rate), with 4,432 responses (25% of contacted respondents) from doctors who had completed their internship between 2015 and 2018 and who provided information on their internship location. The number of responses meets the minimum of required sample estimation with the known proportion of doctors working in remote districts 7.5%, total MoH internship population 31,510, 95% confidence interval and 0.01 precision (minimum sample size 2,459). Compared to the target population, survey respondents were representative by gender (61.8% female, survey respondents; 63.2% female, MoH internship population). The proportion of respondents who graduated from private medical schools (47.1%), and who completed internships in remote districts (11.6%), were slightly lower than for the MoH internship population (51.3 and 14.6%, respectively). The proportion of surveyed respondents participating in Nusantara Sehat (2.6%), however, was higher than that of MoH internship population (1.5%).
Of 4,432 respondents, 3,176 were working as clinicians at the time of the survey, and were included in analyses. Of these, 8.9% were working in remote districts when surveyed. Excluding unknown or missing information, 61.8% of respondents were female, 53.4% were unmarried, and the age range was 24 to 38 years (mean 27.7, SD 3.2). Doctors with a remote upbringing, remote clerkship, or remote internship, comprised 4.6, 2.5 and 11.9%, respectively of respondents (Table 1). More than half of the respondents were within 24-month of completing internship, while 21.6% mentioned that they had worked in a rural or remote location before commencing their current work.
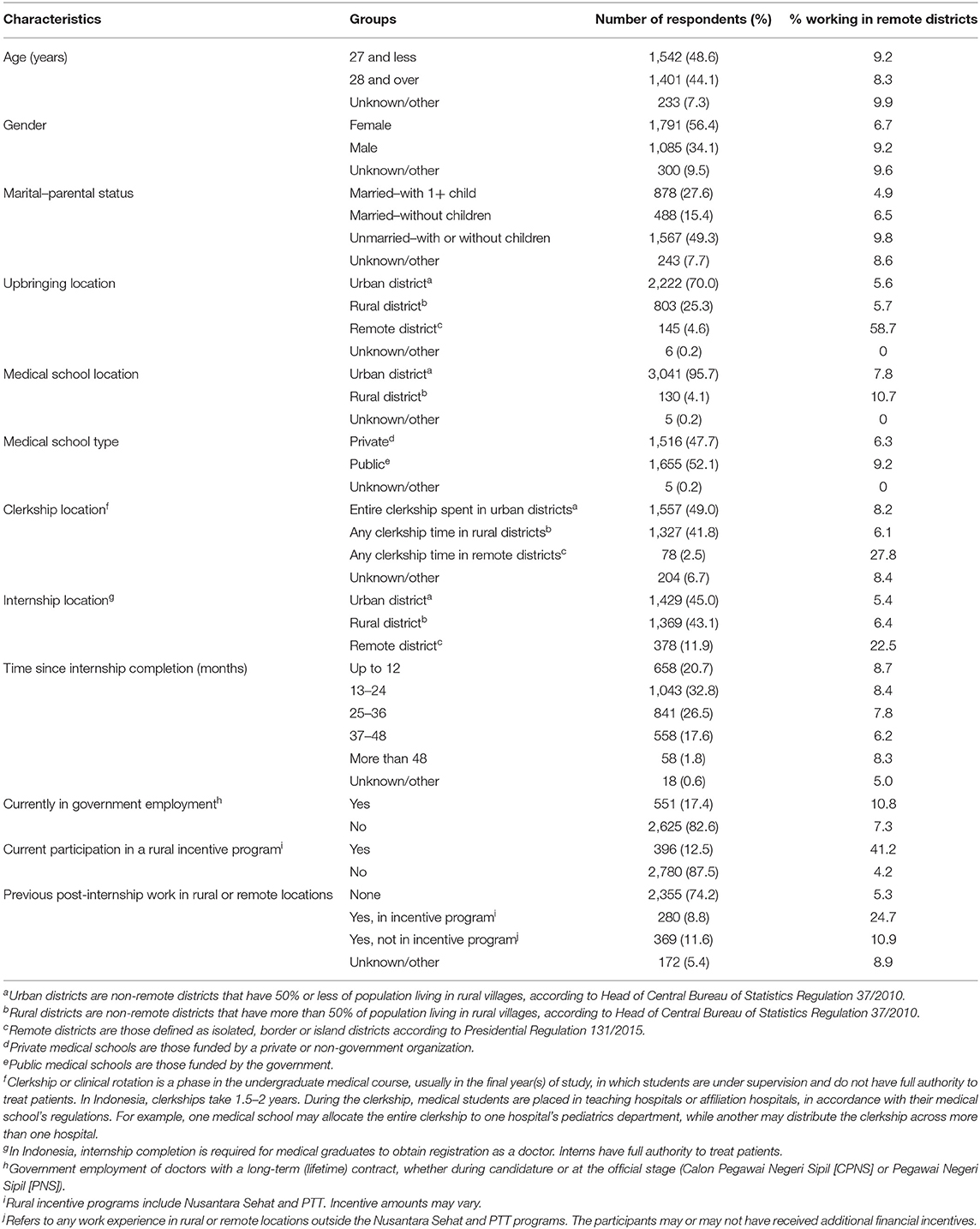
Table 1. Sociodemographic characteristics of respondents.
Of those who grew up in remote districts (n = 145), 58.7% were practicing in remote districts, compared to 5.6 and 5.7% of those growing up in urban and rural districts, respectively. Out of 378 doctors undertaken a remote internship, 22.5% were working in a remote district when surveyed (Table 1).
Multivariate logistic regression showed that doctors working in a remote district were more likely to: be male (OR 1.5, CI 1.1–2.1); be unmarried (OR 1.9, CI 1.3–3.0); have grown up in a remote district (OR 19.9, CI 12.3–32.3); have a clerkship in a remote district (OR 2.2, CI 1.1–4.4); have undertaken an internship in a remote district (OR 2.0, CI 1.3–3.0); be enrolled in the rural incentive program when surveyed (OR 18.6, CI 12.8–26.8); and be a government employee (OR 3.2, CI 2.1–4.9). Strong associations were also found between previous post-internship work in any rural or remote district (OR 1.9, CI 1.2–3.0) and past participation in a rural incentive program (OR 2.0, CI 1.3–3.0) with current work in remote districts. Univariate analyses showed no association between working in a remote district and age, years of post-internship, or medical school location. The odds of working in a remote district were similar for married doctors with children and those without children. An association between attending a public medical school and remote work was evident in the univariate model but was not significant in the multivariate model (Table 2).
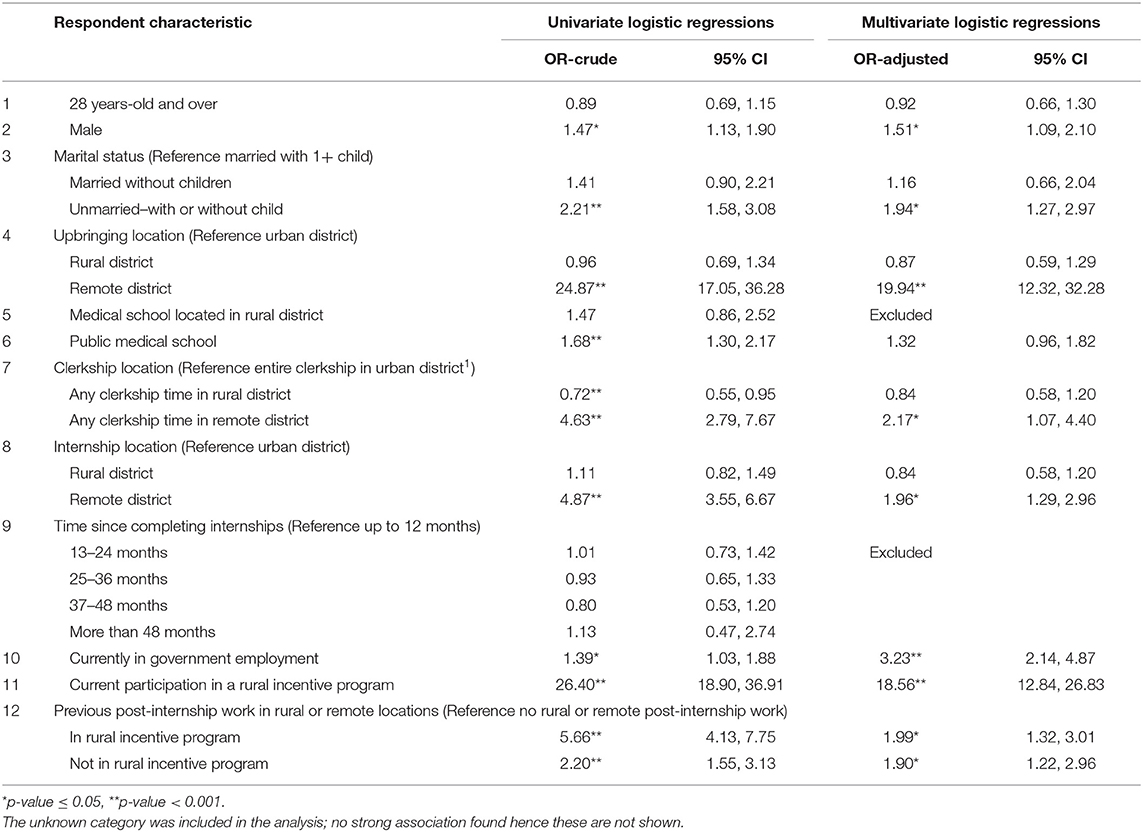
Table 2. Odds ratio of working in remote districts (n = 3,176).
To our knowledge, this is the first national quantitative study exploring factors associated with doctors' work locations in remote districts in Indonesia. Nine percent of early-career doctors surveyed (up to 5 years post-internship) were working in remote districts. This compares to 11% of Indonesia's population who live in these areas (26). Critically, our study identified factors strongly associated with working in remote districts. These include growing up in a remote district; undertaking a remote clerkship during medical school; undertaking a remote internship; working as a government employee; participation in a rural incentives program; being male; unmarried; and previously having worked in any rural or remote area. The first three of these listed factors are all rural pathway factors, suggesting that workforce strategies which select students into medical school from remote areas, train them in those rural and remote locations and then employ them in rural and remote locations immediately upon graduation are key to Indonesia's future remote medical workforce.
Strong relationships between doctors' intentions or actual work in rural areas and rural background, location of secondary schooling, and having a spouse or family living in a rural area have been widely recognized by many previous LMIC studies in the Asia Pacific (3, 4, 41–43, 50–59). Importantly, this research is the first quantitative evidence confirming such strong associations with Indonesian doctors' actual work locations. Our study is also the first to show that, of all the factors of interest, a remote upbringing has the strongest association with remote practice—increasing the odds of remote practice by a substantial 20 times. In contrast, there was no difference in the odds of remote work between doctors who grew up in urban and those who grew up in rural areas. This suggests that exposure to remote places during training, and perhaps to specific remote regions with which doctors may already have a connection, may be effective strategies to encourage remote work choices (60, 61). According to our findings, remote students are proportionally underrepresented in Indonesian medical schools, comprising <5% of students. Without intervention, it is possible that the already low proportion of students who come from remote areas could reduce over time, as has happened, for example, in the United States (62). Given these circumstances, policies and programs that support recruiting undergraduate medical students from remote districts, specifically, are recommended.
Doctors who participated in remote clerkships as medical students had twice the odds of working in a remote district compared to those who only had urban clerkships. This finding indicates that existing evidence, drawn from other countries, of associations between rural clinical placements and rural work preference is relevant for Indonesia (10, 14, 63, 64). This is the case even though Indonesian medical students are assigned by their medical school to rural and remote clerkships; students in many other countries can self-select into these clerkships (64, 65). Given this evidence, increasing the number of remote hospitals and health services which are affiliated with Indonesian medical schools and expanding the number of remote clerkship training weeks during medical school may further improve remote medical workforce outcomes.
Our findings are consistent with other evidence of a positive association between having completed rural internships and subsequent rural work (21, 66, 67). In Indonesia, there are a limited number of internship positions in urban-located hospitals. This forces some interns to choose between doing rural or remote internships or delaying their internship in the hope of getting an urban internship in a subsequent round of internship allocations. The financial assistance for interns' salary provided by the MoH is higher in remote posts, and non-financial support such as, supervisor training and program standardization are also provided (68). This program needs to be expanded to increase the number of doctors working in Indonesian rural locations. Other countries may consider investing in rural internship program as a part of the rural pathway to strengthen efforts to build rural medical workforce.
We found that the opt-in Nusantara Sehat and PTT incentive programs are positively associated with current work in remote Indonesia, consistent with earlier studies demonstrating that opt-in rural incentive programs help address rural doctor shortages (23, 69). We also found that doctors who had ever participated in those programs were more likely to be currently working in remote districts. This suggests that the rural experiences gained through the Nusantara Sehat and PTT programs could be an important part of a pathway to rural practice. This extends beyond the internship year, since these programs are associated with subsequent rural work even after the program incentives are no longer being received.
The strong association that we identified between being a government employee and practicing in remote districts is interesting. Although the positions for government employment are equally available in remote and non-remote districts, the competition may be tougher in the non-remote districts. Further, working in remote areas as a government employee may provide an additional advantage for priority access to scholarships for non-general practice training, for early career doctors wanting to be a specialist. Other evidence has shown that the opportunity for government employment is an incentive for doctors to work in remote locations (70). Indonesian government employees are more likely to be eligible for continuing education scholarships, which are very attractive to medical graduates (71). Also, government employees are permitted to earn additional income from second or third jobs, which is similarly attractive (58, 72, 73). These findings suggest that the longer-term success of stand-alone strategies such as rural incentive programs at the early-career stage could be consolidated by simultaneously increasing opportunities for government appointments in the hardest-to-staff remote locations, or by expanding private job opportunities in remote areas. Concern that government employees with second or third jobs may provide a lower quality of service in government health facilities needs to be managed (74, 75).
Our findings indicate that district governments could have a greater role in developing a home-grown medical workforce—an important highlight for a decentralized nation like Indonesia. Since a remote upbringing has the strongest association with remote work for early-career doctors in Indonesia, remote-district governments could facilitate the entry of local students to medical school, by establishing collaborations with the schools, or providing bonded scholarships. Such collaborations could extend to nominating their district hospitals as sites for clerkships and internships. Remote-district governments could also prioritize government employment for doctors. However, support from the national government should be continued, especially in attracting more doctors to rural and remote locations with its rural financial incentive program and the nationwide internship program.
This study is exploratory and could be extended through ongoing research. First, further research could explore aspects of rural “place” classifications at a more nuanced level, rather than the binary outcome (remote/non-remote) used in this study. Second, the association between duration or design of any rurally-enhanced program and doctors' subsequent work location should be explored in more detail. This includes considering whether a longer duration of clerkship or internship experience, or whether longer exposures in community settings, are more strongly associated with remote or rural workforce outcomes, as has been shown in other countries (76, 77). Third, exploring elements of the internship program that may be more strongly associated with remote practice after the internship would provide more information for future program improvement. Fourth, understanding the long-term retention of doctors in remote areas beyond the internship or rural financial incentive program is essential to identify further efforts required to increase sustainability of the remote medical workforce. It is possible that for retention, working conditions and ongoing training or up-skilling opportunities become imperative (78).
We acknowledge some limitations in this study. This was a self-administered survey with retrospective recollection of details about past characteristics including geographic locations, hence, self-selection and recall bias may occur. As the invitation to the survey was announced through email and online platforms, clinicians not regularly using them may have been under-represented amongst respondents. As described in the Results section, several characteristics of the doctor population were assessed for representativeness. Respondents participating in Nusantara Sehat, one of the rural incentive programs, were overrepresented, which may have led to overestimation of its association with remote practice. However, the odds ratio was high (18.9) with a small p-value (p < 0.001); thus, a type-I error is unlikely in this case. Public medical school graduates were also overrepresented. However, in multivariate analysis this characteristic showed no association with remote practice, and thus did not affect interpretation of the results. Finally, this study did not adjust for other predictors of rural preference found in other studies such as job-related factors (i.e., quality of relationships with colleagues, access to specialist consultations, health facility infrastructure and equipment) (79–81), and locational factors (i.e., access to transportation, socioeconomic development, population density, and health insurance coverage) (82–85).
Our study identifies strong associations between working in remote districts and multiple factors related to rural training pathways (selection, rural training and exposure, professional support, and type of employment). These results indicate that building the Indonesian medical workforce in remote regions could be facilitated by investing in strategies to select medical students with a remote background, delivering more remote clerkships during training, employing more doctors in remote internships, and providing financial incentives for remote work. This would require establishing a more extensive network of remote clerkships for medical students by broadening medical school networks with affiliated-teaching hospitals and community practices. Additional policies include expanding highly sought-after government employment opportunities in rural and remote areas. These strategies are strongly tied to the issue of developing a connected rural pathway to “grow your own,” consistent with the 2010 WHO global policy recommendations about increasing access to health workers.
The data presented in this article are not readily available because they are subject to the requirements of the Monash University Human Research Ethics Committee that they cannot be shared publicly. Requests to access the datasets should be directed to Likke Prawidya Putri: bGlra2UucHV0cmlAdWdtLmFjLmlk or bGlra2VwcEBnbWFpbC5jb20=.
This study was reviewed and approved by the Monash University Human Research Ethics Committee. Informed opt-in consent was given by all participants in accordance with the requirements of the study's ethics approval.
LP, DR, BO'S, and RK designed the study. LP analyzed the data and wrote up the initial draft. DR, BO'S, and RK guided the analysis and interpretation of the results, and drafting of the paper. RK was the principal supervisor overseeing the study. All authors contributed to the article and approved the submitted version.
The research was funded by LPDP (Endowment Fund for Education) Indonesia and the Monash University Student Support Fund. The first author received a PhD scholarship from LPDP Indonesia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor is currently organizing a Research Topic with one of the authors BO'S.
The authors thank dr. Maxi Rein Rondonewu, DHSM, MARS, dr. Mawari Edy, M. Epid, Tumpal Pardomuan Hendriyanto, S. Kom, M.Sc (PH), and Ananta Dwi Saputra, S. Kom from BPPSDM MoH and Dr. dr. Andreasta Meliala, DPH, M. Kes, MAS from Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada for support in conducting this survey. We also thank the survey participants for their time and sharing their experiences.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.594695/full#supplementary-material
1. The World Bank Group. World Bank Open Data United States. (2019). Available online at: https://data.worldbank.org/ (accessed August 1, 2020)
2. Anderson I, Meliala A, Marzoeki P, Pambudi E. (2014). The Production, Distribution, and Performance of Physicians, Nurses, and Midwives in Indonesia: An Update. Health, Nutrition and Population Discussion Paper. Washington DC: The World Bank. p. 1–56.
3. Vujicic M, Shengelia B, Alfano M, Thu HB. Physician shortages in rural Vietnam: using a labor market approach to inform policy. Soc Sci Med. (2011) 73:970–7. doi: 10.1016/j.socscimed.2011.06.010
4. Liu J, Zhu B, Mao Y. Association between rural clinical clerkship and medical students' intentions to choose rural medical work after graduation: A cross-sectional study in western China. PloS ONE. (2018) 13:e0195266. doi: 10.1371/journal.pone.0195266
5. Wibulpolprasert S, Pengpaibon P. Integrated strategies to tackle the inequitable distribution of doctors in Thailand: four decades of experience. Hum Resour Health. (2003) 1:12. doi: 10.1186/1478-4491-1-12
6. Indonesian Health Profile 2017 (Data dan Informasi Profil Kesehatan Indonesia 2017). Jakarta: Indonesian Ministry of Health (2018).
7. World Health Organization. Increasing Access to Health Workers in Remote and Rural Areas Through Improved Retention: Global Policy Recommendations. World Health Organization (2010).
8. Laven G, Wilkinson D. Rural doctors and rural backgrounds: how strong is the evidence? A systematic review. Aust J Rural Health. (2003) 11:277–84. doi: 10.1111/j.1440-1584.2003.00534.x
9. McGirr J, Seal A, Barnard A, Cheek C, Garne D, Greenhill J, et al. The Australian Rural Clinical School (RCS) program supports rural medical workforce: evidence from a cross-sectional study of 12 RCSs. Rural Remote Health. (2019) 19:4971. doi: 10.22605/RRH4971
10. Kwan MM, Kondalsamy-Chennakesavan S, Ranmuthugala G, Toombs MR, Nicholson GC. The rural pipeline to longer-term rural practice: General practitioners and specialists. PloS ONE. (2017) 12:1–15. doi: 10.1371/journal.pone.0180394
11. Schwartz MR. The physician pipeline to rural and underserved areas in Pennsylvania. J Rural Health. (2008) 24:384–9. doi: 10.1111/j.1748-0361.2008.00185.x
12. Matsumoto M, Inoue K, Kajii E, Takeuchi K, Inoue M. Retention of physicians in rural Japan: concerted efforts of the government, prefectures, municipalities and medical schools. Rural Remote Health. (2010) 10:1432. Available online at: https://www.rrh.org.au/journal/article/1432
13. Rabinowitz HK, Diamond JJ, Markham FW, Santana AJ. Retention of rural family physicians after 20-25 years: outcomes of a comprehensive medical school rural program. J Am Board Fam Med. (2013) 26:24–7. doi: 10.3122/jabfm.2013.01.120122
14. O'Sullivan B, McGrail M, Major L, Woodfield M, Holmes C. Rural work outcomes of medical students participating in a contracted Extended Rural Cohort (ERC) program by course-entry preference. Medical Teach. (2019) 41:703–10. doi: 10.1080/0142159X.2019.1569755
15. Playford D, Ngo H, Atkinson D, Puddey IB. Graduate doctors' rural work increases over time. Medical Teach. (2019) 41:1073–80. doi: 10.1080/0142159X.2019.1621278
16. Walters LK, McGrail MR, Carson DB, O'Sullivan BG, Russell DJ, Strasser RP, et al. Where to next for rural general practice policy and research in Australia? Med J Austr. (2017) 207:56–8. doi: 10.5694/mja17.00216
17. Pagaiya N, Kongkam L, Sriratana S. Rural retention of doctors graduating from the rural medical education project to increase rural doctors in Thailand: a cohort study. Human Resources Health. (2015) 13:10. doi: 10.1186/s12960-015-0001-y
18. Techakehakij W, Arora R. Rural retention of new medical graduates from the Collaborative Project to Increase Production of Rural Doctors (CPIRD): a 12-year retrospective study. Health Policy Planning. (2017) 32:809–15. doi: 10.1093/heapol/czx026
19. Hou J, Liang Y, Tong L, Kolars JC, Wang M. Targeted enrollment of medical students for rural China: prospects and challenges. Adv Med Educ Pract. (2019) 10:1021–30. doi: 10.2147/AMEP.S227028
20. Purohit B, Martineau T. Initial posting—a critical stage in the employment cycle: lessons from the experience of government doctors in Gujarat, India. Human Resources Health. (2016) 14:41. doi: 10.1186/s12960-016-0138-3
21. Peach HG, Trembath M, Fensling B. A case for more year-long internships outside metropolitan areas? Medical J Aust. (2004) 180:106–9. doi: 10.5694/j.1326-5377.2004.tb05829.x
22. Straume K, Sondena MS, Prydz P. Postgraduate training at the ends of the earth - a way to retain physicians? Rural Remote Health. (2010) 10:1356. Available online at: www.rrh.org.au/journal/article/1356
23. Peña S, Ramirez J, Becerra C, Carabantes J, Arteaga O. The Chilean Rural Practitioner Programme: a multidimensional strategy to attract and retain doctors in rural areas. Bull World Health Organ. (2010) 88:371–8. doi: 10.2471/BLT.09.072769
24. The World Bank Group. Indonesia Database for Policy and Economic Research. (2020). Available online at: https://databank.worldbank.org/reports.aspx?source=1266 (accessed March, 10 2020).
25. World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals: Human Resources for Health Observer Series No 17. Switzerland: World Health Organization (2016).
26. Bureau of Statistics Indonesia. Population Census 2010 (Sensus Penduduk 2010) (2010). Available online at: https://sp2010.bps.go.id/ (accessed March 10, 2020).
27. Rokx C, Giles J, Satriawan E, Marzoeki P, Harimurti P, Yavuz E. New Insights Into the Provision of Health Services in Indonesia: A Health Workforce Study. Washington DC: World Bank Publications (2010). doi: 10.1596/978-0-8213-8298-1
28. Rakmawati T, Hinchcliff R, Pardosi JF. District-level impacts of health system decentralization in Indonesia: a systematic review. Int J Health Plann Manag. (2019) 34:e1026–e1053. doi: 10.1002/hpm.2768
29. Minister of Health Regulation Number 39 Year 2017 on Effectuation of Internship Program for Doctor and Dentist in Indonesia (Peraturan Menteri Kesehatan Republik Indonesia Nomor 39 Tahun 2017 tentang Penyelenggaraan Program Internsip Dokter dan Dokter Gigi Indonesia). Jakarta: Indonesian Ministry of Health (2017).
30. Minister of Health Regulation Number 33 Year 2018 on Special Assignment for Health Workers for Nusantara Sehat Program (Peraturan Menteri Kesehatan nomor 33 tahun 2018 tentang Penugasan khusus tenaga kesehatan dalam mendukung program Nusantara Sehat). Indonesian Ministry of Health (2018).
31. Bureau of Statistics Indonesia. Village Census of Indonesia 2014 (Pendataan Potensi Desa Indonesia 2014). Jakarta: Bureau of Statistics Indonesia (2014).
32. Bureau of Statistics Indonesia. Village Census of Indonesia 2018 (Pendataan Potensi Desa Indonesia 2018). Jakarta: Bureau of Statistics Indonesia (2018).
33. Handoyo NE, Prabandari YS, Rahayu GR. Identifying motivations and personality of rural doctors: a study in Nusa Tenggara Timur, Indonesia. Educ Health. (2018) 31:174–7. doi: 10.4103/efh.EfH_106_14
34. Tjung L, Meliala A, Trisnantoro L. Physician engagement at Eka Hospital BSD-City and Pekanbaru (Keterlekatan Dokter Spesialis di Eka Hospital Bsd-city dan Pekanbaru). Jurnal Manajemen Pelayanan Kesehatan. (2012) 15:115–23. Available online at: https://jurnal.ugm.ac.id/jmpk/article/view/2476
35. Dasman H, Mwanri L, Martini A. Indonesian rural medical internship: The impact on health service and the future workforce. Indian J Public Health Res Dev. (2018) 9:231–6. doi: 10.5958/0976-5506.2018.00646.0
36. McGrail MR, Russell DJ, Campbell DG. Vocational training of general practitioners in rural locations is critical for the Australian rural medical workforce. Med J Aust. (2016) 205:216–21. doi: 10.5694/mja16.00063
37. Scott A, Jeon S-H, Joyce CM, Humphreys JS, Kalb G, Witt J, et al. A randomised trial and economic evaluation of the effect of response mode on response rate, response bias, and item non-response in a survey of doctors. BMC Med Res Methodol. (2011) 11:1–12. doi: 10.1186/1471-2288-11-126
38. Dykema J, Jones NR, Piche T, Stevenson J. Surveying clinicians by web: current issues in design and administration. Eval Health Prof . (2013) 36:352–81. doi: 10.1177/0163278713496630
39. Joyce CM, Scott A, Jeon S-H, Humphreys J, Kalb G, Witt J, et al. The “Medicine in Australia: Balancing Employment and Life (MABEL)” longitudinal survey-Protocol and baseline data for a prospective cohort study of Australian doctors' workforce participation. BMC Health Serv Res. (2010) 10:50. doi: 10.1186/1472-6963-10-50
40. Hatcher AM, Onah M, Kornik S, Peacocke J, Reid S. Placement, support, and retention of health professionals: National, cross-sectional findings from medical and dental community service officers in South Africa. Hum Resour Health. (2014) 12:1–13. doi: 10.1186/1478-4491-12-14
41. Chuenkongkaew WL, Negandhi H, Lumbiganon P, Wang W, Mahmud K, Cuong PV. Attitude towards working in rural area and self-assessment of competencies in last year medical students: a survey of five countries in Asia. BMC Med Educ. (2016) 16:238. doi: 10.1186/s12909-016-0719-9
42. Silvestri DM, Blevins M, Afzal AR, Andrews B, Derbew M, Kaur S, et al. Medical and nursing students' intentions to work abroad or in rural areas: a cross-sectional survey in Asia and Africa. Bull World Health Organ. (2014) 92:750–9. doi: 10.2471/BLT.14.136051
43. Silvestri DM, Blevins M, Wallston KA, Afzal AR, Alam N, Andrews B, et al. Nonacademic attributes predict medical and nursing student intentions to emigrate or to work rurally: an eight-country survey in Asia and Africa. Am J Trop Med Hyg. (2017) 96:1512–20. doi: 10.4269/ajtmh.16-0756
44. Presidential Regulation Number 131 Year 2015 on Determination of Remote Area 2015-2019 (Peraturan Presiden Nomor 131 Tahun 2015 tentang Penetapan Daerah Tertinggal Tahun 2015-2019). Presiden of Republic Indonesia (2015).
45. LPDP. List of LPDP Scholarship Affirmation Areas 2019 (Daftar Daerah Afirmasi LPDP 2019). Jakarta: Lembaga Pengelola Dana Pendidikan (2019).
46. Decree of the Minister of Health Number HK 02.02/Menkes/367/2015 on 48 Targeted Districts and 124 Puskesmas as the National Health Service Priorities in Border Areas (Surat Keputusan Menteri Kesehatan Nomor HK 02.02/Menkes/367/2015 tentang 48 Kabupaten/Kota dan 124 Puskesmas Sasaran Program Prioritas Nasional Pelayanan Kesehatan di Daerah Perbatasan tahun 2015-2019). Jakarta: Indonesian Ministry of Health (2015).
47. Head of Central Bureau of Statistics Regulation Number 37 Year 2010 (Peraturan Kepala Badan Pusat Statistik Nomor 37 Tahun 2010). Jakarta: Indonesian Central Bureau of Statistics (2010).
48. Nasution SK, Mahendradhata Y, Trisnantoro L. Can a national health insurance policy increase equity in the utilization of skilled birth attendants in indonesia? a secondary analysis of the 2012 to 2016 national socio-economic survey of Indonesia. Asia Pac J Public Health. (2020) 32:19–26. doi: 10.1177/1010539519892394
49. Diana A, Hollingworth SA, Marks GC. Quality of physical resources of health facilities in Indonesia: a panel study 1993–2007. Int J Qual Health Care. (2013) 25:488–96. doi: 10.1093/intqhc/mzt057
50. Hou J, Xu M, Kolars JC, Dong Z, Wang W, Huang A, et al. Career preferences of graduating medical students in China: a nationwide cross-sectional study. BMC Med Educ. (2016) 16:136. doi: 10.1186/s12909-016-0658-5
51. Liu J, Zhang K, Mao Y. Attitude towards working in rural areas: a cross-sectional survey of rural-oriented tuition-waived medical students in Shaanxi, China. BMC Med Educ. (2018) 18:91. doi: 10.1186/s12909-018-1209-z
52. Nallala S, Swain S, Das S, Kasam SK, Pati S. Why medical students do not like to join rural health service? An exploratory study in India. J Family Commun Med. (2015) 22:111–7. doi: 10.4103/2230-8229.155390
53. Saini NK, Sharma R, Roy R, Verma R. What impedes working in rural areas? A study of aspiring doctors in the National Capital Region, India. Rural Remote Health. (2012) 12:1967. Available online at: www.rrh.org.au/journal/article/1967
54. Sinha RK. Perception of young doctors towards service to rural population in Bihar. J Indian Med Assoc. (2012) 110:530–4. Available online at: https://europepmc.org/article/med/23741816
55. Huntington I, Shrestha S, Reich NG, Hagopian A. Career intentions of medical students in the setting of Nepal's rapidly expanding private medical education system. Health Policy Plan. (2012) 27(5):417–28. doi: 10.1093/heapol/czr052
56. Sapkota BP, Amatya A. What factors influence the choice of urban or rural location for future practice of Nepalese medical students? A cross-sectional descriptive study. Human Resour Health. (2015) 13:84. doi: 10.1186/s12960-015-0084-5
57. Zimmerman M, Shakya R, Pokhrel BM, Eyal N, Rijal BP, Shrestha RN, et al. Medical students' characteristics as predictors of career practice location: retrospective cohort study tracking graduates of Nepal's first medical college. BMJ. (2012) 345:e4826. doi: 10.1136/bmj.e4826
58. Farooq U, Ghaffar A, Narru IA, Khan D, Irshad R. Doctors perception about staying in or leaving rural health facilities in District Abbottabad. J Ayub Med Coll Abbottabad. (2004) 16:64–9. Available online at: https://www.jamc.ayubmed.edu.pk/jamc/index.php/jamc/article/view/4057
59. Syahmar I, Putera I, Istatik Y, Furqon MA, Findyartini A. Indonesian medical students' preferences associated with the intention toward rural practice. Rural Remote Health. (2015) 15:3526. Available online at: https://www.rrh.org.au/journal/article/3526
60. Woolley T, Sen Gupta T, Murray R, Hays R. Predictors of rural practice location for James Cook University MBBS graduates at postgraduate year 5. Aust J Rural Health. (2014) 22:165–71. doi: 10.1111/ajr.12106
61. McGrail MR, O'Sullivan BG, Russell DJ. Rural training pathways: the return rate of doctors to work in the same region as their basic medical training. Hum Resour Health. (2018) 16:1–10. doi: 10.1186/s12960-018-0323-7
62. Shipman SA, Wendling A, Jones KC, Kovar-Gough I, Orlowski JM, Phillips J. The decline in rural medical students: a growing gap in geographic diversity threatens the rural physician workforce. Health Affairs. (2019) 38:2011–8. doi: 10.1377/hlthaff.2019.00924
63. Playford D, Ngo H, Gupta S, Puddey IB. Opting for rural practice: the influence of medical student origin, intention and immersion experience. Med J Aust. (2017) 207:154–8. doi: 10.5694/mja16.01322
64. Johnson GE, Wright FC, Foster K. The impact of rural outreach programs on medical students' future rural intentions and working locations: a systematic review. BMC Med Educ. (2018) 18:196. doi: 10.1186/s12909-018-1287-y
65. Jones M, Bushnell J, Humphreys J. Are rural placements positively associated with rural intentions in medical graduates? Med Educ. (2014) 48:405–16. doi: 10.1111/medu.12399
66. Sen Gupta T, Woolley T, Murray R, Hays R, McCloskey T. Positive impacts on rural and regional workforce from the first seven cohorts of James Cook University medical graduates. Rural Remote Health. (2014) 14:1–13. Available online at: https://www.rrh.org.au/journal/article/2657
67. Straume K, Shaw DM. Internship at the ends of the Earth–a way to recruit physicians. Rural Remote Health. (2010) 10:1–10. Available online at: https://www.rrh.org.au/journal/article/1366
68. Circular of the Ministry of Health Number HK 03.03 Year 2016 on Contribution to Living Expenses for Internship Doctor (Surat Edaran Kementerian Kesehatan Nomor HK 03.03 Tahun 2016 tentang Bantuan Biaya Hidup Dokter Internsip). Jakarta: Indonesian Ministry of Health (2016).
69. Pereira L, Santos W, Oliveira A, Rattner D. Mais Médicos program: provision of medical doctors in rural, remote and socially vulnerable areas of Brazil, 2013-2014. Rural Remote Health. (2016) 16:1–12. Available online at: www.rrh.org.au/journal/article/3616
70. Arifandi Meliala A. Factors affecting recruitment of physicians at primary health care in the work area of public health office of Buol in 2016 (Faktor yang Mempengaruhi Rekrutment Dokter di Puskesmas Wilayah Kerja Dinas Kesehatan Kabupaten Buol Tahun 2016). Jurnal Kebijakan Kesehatan Indonesia JKKI. (2017) 6:103–14. doi: 10.22146/jkki.v6i3.29659
71. Efendi F, Chen C-M, Nursalam N, Andriyani NWF, Kurniati A, Nancarrow SA. How to attract health students to remote areas in Indonesia: a discrete choice experiment. Int J Health Plan Manag. (2016) 31:430–45. doi: 10.1002/hpm.2289
72. Meliala A, Hort K, Trisnantoro L. Addressing the unequal geographic distribution of specialist doctors in indonesia: the role of the private sector and effectiveness of current regulations. Social Sci Med. (2013) 82:30–4. doi: 10.1016/j.socscimed.2013.01.029
73. Darkwa EK, Newman MS, Kawkab M, Chowdhury ME. A qualitative study of factors influencing retention of doctors and nurses at rural healthcare facilities in Bangladesh. BMC Health Serv Res. (2015) 15:1–12. doi: 10.1186/s12913-015-1012-z
74. Socha KZ, Bech M. Physician dual practice: a review of literature. Health Policy. (2011) 102:1–7. doi: 10.1016/j.healthpol.2010.10.017
75. Macq J, Ferrinho P, De Brouwere V, Van Lerberghe W. Managing health services in developing countries: between ethics of the civil servant and the need for moonlighting: managing and moonlighting. Human Res Health Dev J. (2001) 5:17–24.
76. O'Sullivan B, McGrail M, Russell D, Walker J, Chambers H, Major L, et al. Duration and setting of rural immersion during the medical degree relates to rural work outcomes. Med Educ. (2018) 52:803–15. doi: 10.1111/medu.13578
77. Boonluksiri P, Tumviriyakul H, Arora R, Techakehakij W, Chamnan P, Umthong N. Community-based learning enhances doctor retention. Educ Health. (2018) 31:114–8. doi: 10.4103/efh.EfH_153_17
78. O'Sullivan B, Chater B, Bingham A, Wynn-Jones J, Couper I, Hegazy NN, et al. A Checklist for implementing rural pathways to train, develop and support health workers in low and middle-income countries. Front Med. (2020) 7:594728. doi: 10.3389/fmed.2020.594728
79. Lehmann U, Dieleman M, Martineau T. Staffing remote rural areas in middle-and low-income countries: a literature review of attraction and retention. BMC Health Ser Res. (2008) 8:10. doi: 10.1186/1472-6963-8-19
80. Bonenberger M, Aikins M, Akweongo P, Wyss K. The effects of health worker motivation and job satisfaction on turnover intention in Ghana: a cross-sectional study. Human Resour Health. (2014) 12:1–12. doi: 10.1186/1478-4491-12-43
81. Behera MR, Prutipinyo C, Sirichotiratana N, Viwatwongkasem C. Living conditions, work environment, and intention to stay among doctors working in rural areas of Odisha state, India. Ann Trop Med Public Health. (2018) 17:S809. doi: 10.4103/ATMPH.ATMPH_338_17
82. Scholz S, von der Schulenburg J-MG, Greiner W. Regional differences of outpatient physician supply as a theoretical economic and empirical generalized linear model. Human Resour Health. (2015) 13:85. doi: 10.1186/s12960-015-0088-1
83. Russo G, Ferrinho P, de Sousa B, Conceição C. What influences national and foreign physicians' geographic distribution? An analysis of medical doctors' residence location in Portugal. Human Resour Health. (2012) 10:12. doi: 10.1186/1478-4491-10-12
84. De Costa A, Al-Muniri A, Diwan VK, Eriksson B. Where are healthcare providers? Exploring relationships between context and human resources for health Madhya Pradesh province, India. Health Policy. (2009) 93:41–7. doi: 10.1016/j.healthpol.2009.03.015
Keywords: rural health services, physician practice, low- and middle-income countries, health workforce maldistribution, career choice, professional practice location
Citation: Putri LP, Russell DJ, O'Sullivan BG and Kippen R (2021) Factors Associated With Working in Remote Indonesia: A National Cross-Sectional Study of Early-Career Doctors. Front. Med. 8:594695. doi: 10.3389/fmed.2021.594695
Received: 14 August 2020; Accepted: 26 March 2021;
Published: 13 May 2021.
Edited by:
Pratyush Kumar, Patna Medical College and Hospital, IndiaReviewed by:
Diantha Soemantri, University of Indonesia, IndonesiaCopyright © 2021 Putri, Russell, O'Sullivan and Kippen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Likke Prawidya Putri, bGlra2VwcEBnbWFpbC5jb20=; bGlra2UucHV0cmlAdWdtLmFjLmlk
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.