
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 09 November 2020
Sec. Geriatric Medicine
Volume 7 - 2020 | https://doi.org/10.3389/fmed.2020.609359
 Laura Lorenzo-López*
Laura Lorenzo-López* Julia Blanco-Fandiño
Julia Blanco-Fandiño Nuria Cibeira
Nuria Cibeira Ana Buján
Ana Buján Rocío López-López
Rocío López-López Ana Maseda
Ana Maseda José Carlos Millán-Calenti
José Carlos Millán-CalentiPhysical frailty is closely associated with cognitive impairment. We aim to investigate the neuropsychological profiles of prefrail and non-frail dementia-free community-dwelling older adults using a comprehensive neuropsychological evaluation, and to examine the association between specific frailty criteria and clinical and neuropsychological scores. Participants completed a comprehensive standardized neuropsychological evaluation (covering cognitive domains such as memory, executive functions, language and attention), and frailty assessment. Frailty was assessed according to biological criteria: unintentional weight loss, exhaustion, low physical activity, slowness, and weakness. The sample comprised 60 dementia-free community-dwelling adults, aged 65 years or older (range 65–89 years; 60.0% women). Forty-two participants were classified as robust (no frailty criteria present), and 18 as prefrail (1 or 2 frailty criteria present). We explored neurocognitive differences between the groups and examined the association between specific criteria of frailty phenotype and clinical and neuropsychological outcomes with bivariate tests and multivariate models. Prefrail participants showed poorer cognitive performance than non-frail participants in both memory and non-memory cognitive domains. However, delayed episodic memory was the only cognitive subdomain that remained significant after controlling for age, gender, and educational level. Gait speed was significantly associated with general cognitive performance, immediate memory, and processing speed, while grip strength was associated with visual episodic memory and visuoconstructive abilities. Both gait speed and grip strength were negatively associated with depressive scores. Our results suggest that prefrailty is associated with cognitive dysfunction. The fact that specific cognitive domains may be susceptible to subclinical states of physical frailty may have important clinical implications. Indeed, early detection of specific cognitive dysfunctions may allow opportunities for reversibility.
Frailty is a common clinical syndrome in older adults due to age-related cumulative decline in multiple physiological systems, associated with negative health outcomes, including deterioration of daily living activities, disability, institutionalization, morbidity, and mortality (1). Cross-sectional and longitudinal research has demonstrated that older adults with physical frailty exhibit poorer cognitive performance and greater risk of cognitive decline and dementia than individuals without frailty (2–15), and that individuals with cognitive decline or dementia show a higher risk of physical frailty (16–18). It has also been demonstrated that the coexistence of physical frailty and cognitive impairment (cognitive frailty), ranging from 1 to 5% in community-dwelling older adults (19), increases the risk of mortality (20–25), functional disability (26), and incident neurocognitive disorders (9, 27) in later life. Importantly, the rates of change of frailty and cognition over time are strongly correlated and associated with the same brain pathologies, such as the presence of macroinfarcts, Alzheimer's disease pathology, and nigral neuronal loss (28). Thus, consideration of both factors is required for the identification of vulnerable older adults at risk of adverse health outcomes (20, 26). With increasing life expectancy, frailty and cognitive disorders, which are increasingly prevalent with advancing age, are being recognized as major healthcare priorities.
Although a growing number of studies are focusing on the relationship between physical frailty and cognitive impairment, most of the researches adopted only a measure of general cognitive functioning to assess cognition or a limited number of cognitive tests (2, 3, 9, 12, 14, 21, 26, 29–35). Moreover, few previous studies have focused on the relationship between prefrailty and cognitive function (35–39), with conflicting results. Some studies reported that prefrailty was not associated with poor cognitive performances (36) and others revealed significant poor performances in several cognitive domains (35, 37–39), but it is unclear whether prefrailty is associated with memory or non-memory cognitive domains, or both. Prefrailty is an intermediate and potentially reversible state between non-frailty and frailty, which has been considered an optimal target for preventive interventions. It has been demonstrated that cognitive performance progressively declines across the continuum from robustness to frailty (40) and that prefrail individuals present more prominent neuroimaging evidence of diffuse cortical or subcortical brain damage than non-frail individuals (41). Because it is unclear whether the associations between frailty and cognitive function are different according to the level of frailty, it is important to identify the cognitive characteristics of prefrailty status. In the present paper, we investigated the neuropsychological profiles of prefrail and non-frail dementia-free community-dwelling older adults using a comprehensive neuropsychological evaluation to identify the cognitive domains most altered by prefrailty. We also examined the association between specific components of frailty phenotype and clinical and neuropsychological scores. Exploring specific cognitive functions and describing neuropsychological correlates of prefrailty may shed light on the understanding of the syndrome, contributing to the investigation of cognitive frailty, and may help to implement intervention strategies for prevention and treatment.
This study used a cross-sectional design. Participants were recruited from community centers for older adults located in Galicia (Northwestern Spain), and through distribution of informative leaflets and emails. Talks were given at the centers explaining the purpose, procedures, and assessments to be carried out. Participants were invited to participate in the project and were involved in a voluntary basis. Ninety-one community-dwelling older adults were assessed for eligibility, of which 60 participants without dementia diagnosis (aged 65–89 years, mean age 72.5 ± 6.1 years, 60.0% females) were included in the study and analyzed (18 met the criteria for prefrailty). All participants were 65 years and older, right-handed, free of major physical or psychiatric conditions, and reporting having normal or corrected-to-normal vision and hearing. Participants were excluded from the study if they were taking psychoactive medications based on prescribed medication history, including antipsychotics, antiepileptics, and antidepressants, which could affect cognitive functioning. Institutional review board approval was obtained from the Autonomic Research Ethics of Galicia Committee, Spain (code 2018/049), and research was conducted consistent with the Declaration of Helsinki. Written informed consent was obtained from all participants, who were individually assessed by qualified professionals trained in clinical evaluation.
The sociodemographic characteristics analyzed were age, gender, and education. Clinical data were collected, including weight and height. Body mass index (BMI) was calculated as weight in kilograms (kg) divided by the square of height in meters (m). Depressive symptoms were determined by the Spanish version of the Geriatric Depression Scale-15 items (GDS-SF) (42, 43).
Participants were screened for physical frailty using Fried's criteria (1), including unintentional weight loss ≥ 4.5 kg of body weight in the last year; self-reported exhaustion; low muscle strength (JAMAR hand-grip hydraulic dynamometer), adjusted for gender and BMI; reduced walking speed, assessed by the time (in seconds) needed to walk a distance of 4.57 m, adjusted for gender and height; and low physical activity level, measured by the amount of weekly energy spent (in kilocalories), stratified by gender. Cut-off points of the standardized version of the Fried's criteria were used according to the phenotypic characteristics of the Spanish population (44). Participants who met 1–2 of these criteria were allocated into the prefrail group.
A neuropsychological battery of tests was administered. The battery involved the assessment of global cognitive function using the Spanish version (45) of the Mini-Mental State Examination (MMSE) (46), and the Montreal Cognitive Assessment test (MoCA) (47). Specific cognitive domains were also explored: episodic memory, attention, executive functioning, naming, and visuospatial function. To assess episodic memory, the immediate memory subscale of the Luria battery for Neuropsychological Diagnosis of Adults was used (Luria-NDA) (48). Visual episodic memory and visuoconstructive abilities were assessed with the Benton Visual Retention Test (BVRT) (49) administration A (immediate recall) and D (short-term retention, with a 15-s interval between the encoding phase and the visual stimulus reproduction), recording the number of correctly reproduced visual stimulus. Visual scanning, psychomotor speed, divided attention, and cognitive shifting were assessed with the Trail Making Test (TMT-A and B) (50). TMT-A is a measure of simple attention and speeded processing and TMT-B is a speeded measure of cognitive flexibility and executive functioning. The time taken to complete each part of the test was recorded in seconds. Visual confrontation naming function was evaluated using the short 15-item version of the Boston Naming Test (BNT) (51), recording the number of correct responses, and excluding perseverations and intrusion errors. Finally, to assess attentional function, the attentional control subscale of the Luria battery for Neuropsychological Diagnosis of Adults (Luria-NDA) (48) was used.
All variables were checked for normality with the Shapiro-Wilk test. Non-normal continuous dependent variables are reported as median (interquartile range, IQR), normal continuous variables are presented as mean and standard deviations (SD), and categorical variables are expressed as count (percentage). A Mann-Whitney U-test was conducted to compare differences between groups in the non-normally distributed continuous variables, and an independent t-test was conducted for the variables distributed normally. We reported Cohen's r or d effect (52, 53) for the Mann-Whitney and t-tests, respectively (0.1 to <0.3 small, 0.3 to <0.5 medium, and 0.5 to 1 large effect sizes). For categorical variables, we used the chi-squared (χ2) test. We performed multivariate linear regression models to further explore the relationship between frailty and neuropsychological scores while controlling for demographics (age, gender, and education), as these variables have been previously identified as risk factors for cognitive impairment. Specifically, we estimated separate models for neuropsychological scores that were significant according to univariate analyses, in which the cognitive performance was the dependent variable and a dichotomous variable for frailty (non-frailty and prefrailty) was entered as an independent variable with the covariates. Spearman's Rho partial correlation coefficients adjusted by age were used to assess the relationship between neuropsychological test performance and performance-based frailty criteria; gait speed and hand-grip strength, for the whole sample. These two variables were used as continuous variables to analyze their correlation with cognitive function. Specifically, the time (in seconds) taken to walk 4.57 m at the usual pace was converted to gait speed (meters per second, m/s). Regarding hand-grip strength, three successive readings were taken from the dominant hand in the standardized position, and the highest values (measured in kg) were used in the correlation analysis. Statistical analyses were performed with the statistical software IBM SPSS Statistics, version 25.0. The statistic level of significance was set as p < 0.05.
Of the 60 participants, 18 (30.0%) meet the criteria for prefrailty and 42 (70.0%) did not meet any frailty criteria. Table 1 displays the sociodemographic characteristics and cognitive scores of prefrail and non-frail groups. Participants had a mean age of 72.5 years (SD = 6.1), and 34 (60.0%) were females. Prefrail participants were slightly older than robust participants (p = 0.049, Cohen's r = −0.25). No significant differences in years of formal education (p = 0.092) or gender (p = 0.206) were observed. Although no significant differences were observed between groups in overall cognitive performance assessed by the MMSE (U = 345.5, z = −0.542, p = 0.588), bivariate tests indicated that prefrail participants showed worse scores in Benton Visual Retention Test, both in immediate (U = 216.5, z = −2.537, p = 0.011, r = −0.33) and delayed (U = 167.5, z = −3.297, p = 0.001, r = −0.43) applications, poor scores on the Luria-NDA immediate memory subscale (U = 226.0, z = −2.453, p = 0.014, r = −0.32), and worse scores in part B of Trail Making Test (U = 183.0, z = −2.646, p = 0.008, r = −0.34), compared to non-frail participants. Significant differences were found between the groups in the MoCA scores (p = 0.032, r = −0.28), with worse scores in the prefrail group. As shown in the Table 1, no significant differences were observed between prefrail and non-frail groups in the naming function (BNT), visual scanning (TMT-A), and attentional control (Luria-NDA- attentional control). Multivariate regression models revealed that delayed episodic memory was the only cognitive subdomain that remained significantly associated with frail status after controlling for age, gender and educational level (see Table 2).
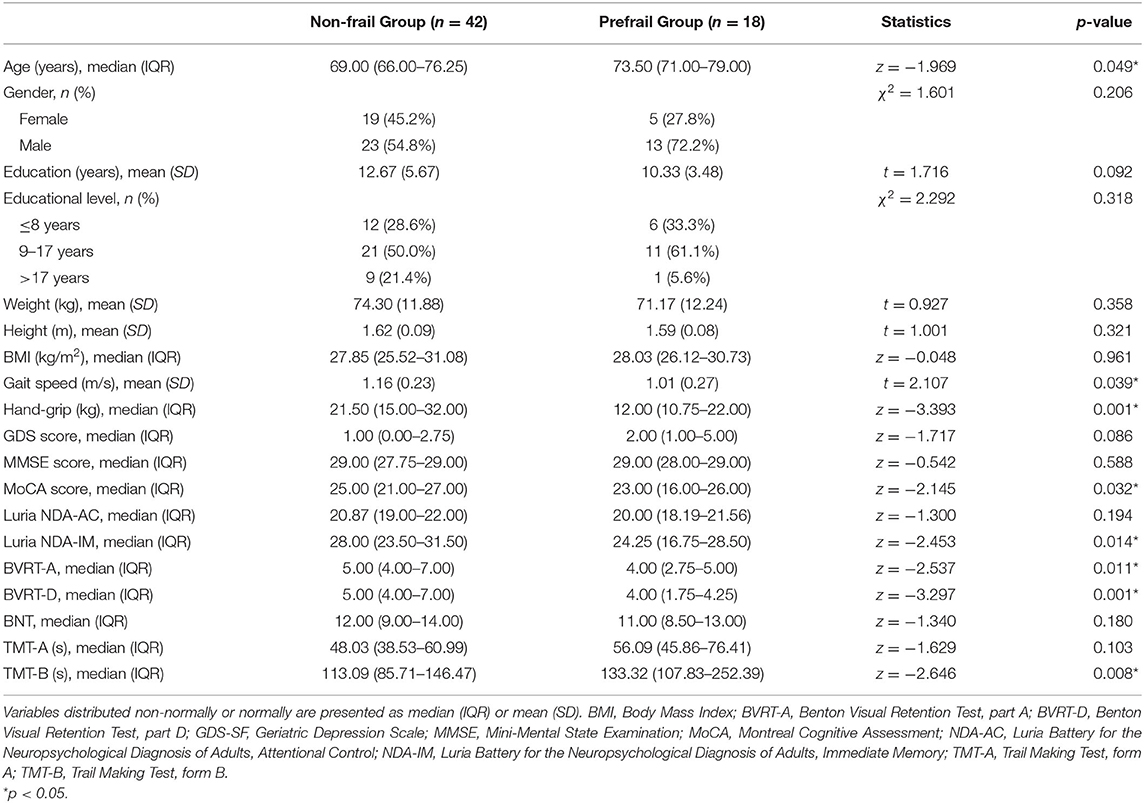
Table 1. Clinical characteristics and neuropsychological performance of participants according to their frailty status.
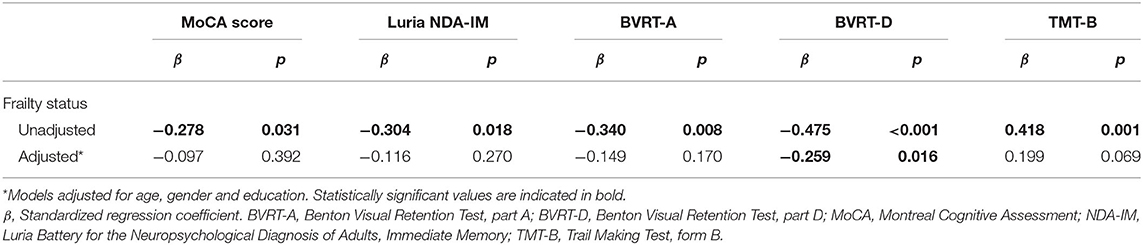
Table 2. Effect of frailty status on neuropsychological scores.
Figures 1, 2 present the scatter plots showing the results of partial correlation coefficients adjusted by age between the gait speed and hand-grip strength, and the clinical and neuropsychological tests, respectively. Rho coefficients (ρ) indexed positive lineal correlations between gait speed (m/s) and cognitive performance in the MoCA test (ρ = 0.258, p = 0.048), the Luria-NDA immediate memory subscale (ρ = 0.286, p = 0.028), and negative correlations between gait speed and TMT-A (ρ = −0.270, p = 0.039) scores. Negative values of the ρ in TMT scores indicate a negative correlation because these scores reflect the time to complete the task and a higher time indicates worse performance. Importantly, gait speed was negatively correlated with GDS-SF scores (ρ = −0.376, p = 0.003). Hand-grip strength (kg) was positively correlated with the delayed BVRT (ρ = 0.322, p = 0.015) and negatively correlated with GDS-SF scores (ρ = −0.343, p = 0.008).
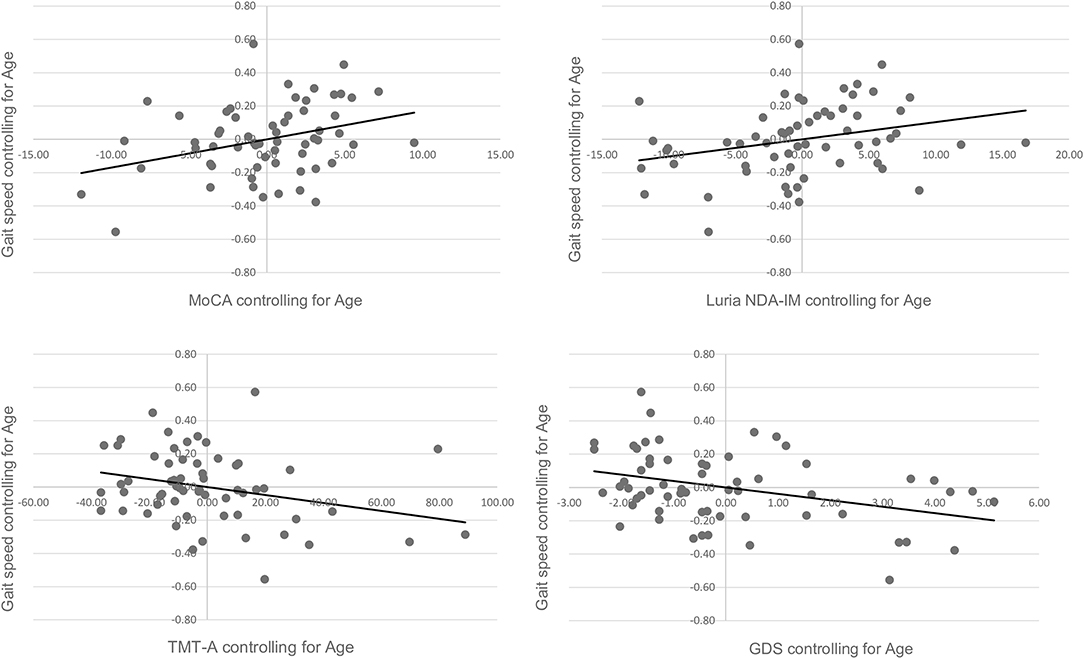
Figure 1. Scatter plots showing the partial correlation between gait speed (m/s) and clinical and cognitive performance, controlled for age. Values on the x-axis represent residuals from regressing MoCA scores, Luria NDA-IM scores, TMT-A scores, and GDS scores on age, respectively. Values on the y-axis represent residuals from regressing gait speed on age.
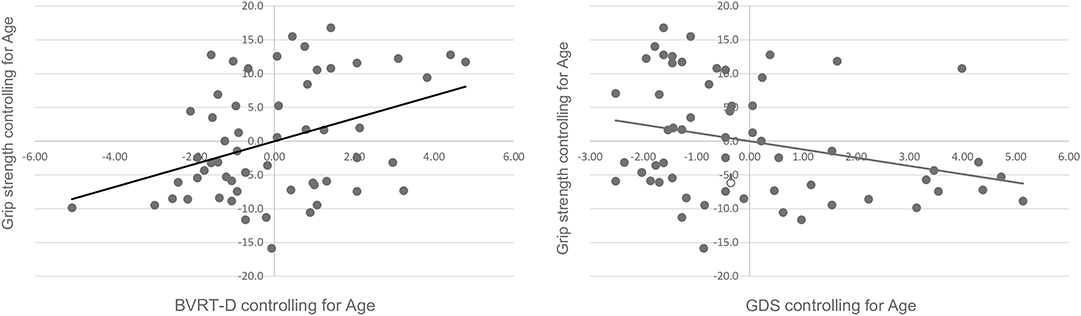
Figure 2. Scatter plots showing the partial correlation between hand-grip strength (kg) and clinical and cognitive performance, controlled for age. Values on the x-axis represent residuals from regressing BVRT-D scores, and GDS scores on age, respectively. Values on the y-axis represent residuals from regressing grip strength on age.
The primary aim of the present study was to examine neuropsychological correlates of prefrailty in dementia-free community-dwelling older adults and to examine the association between specific components of the frailty phenotype and clinical and neuropsychological performance.
Our findings associate prefrailty with the presence of specific neuropsychological impairments. Indeed, in the simple comparisons prefrail participants demonstrated significantly poorer cognitive functions, including executive function, verbal and visual immediate memory, and visuospatial function than non-frail participants with the same level of education. It is important to note, however, that only visual episodic memory domain remained significantly associated with frailty status when controlling for demographic characteristics. In recent research, poor results on delayed memory and processing speed were observed in prefrail older adults with cognitive complaints (38). It has been previously shown that prefrail older adults with no diagnosis of cognitive impairment present poor global cognitive function than non-frail older adults (30, 37). In a study exploring the neuropsychological profiles of cognitive frailty, it was observed that cognitively frail individuals had significant impairments in memory and visuospatial domains than those with cognitive impairment with no physical frailty (54). Comorbid prefrailty and cognitive impairment have been previously associated with future frailty and mortality (21, 35), and with an increased risk for dementia (9).
The poor performance on the BVRT, which assess episodic visual memory, reveals potential different patterns of visual scanning and fixation in the prefrail participants. Poorer performances (longer times) in the TMT-B may suggest problems in divided attention and cognitive shifting in prefrail participants. However, this difference was not significant after controlling for demographics. This is a speeded measure of cognitive flexibility involving mental tracking and switching between letter-number sets, evaluating the executive function. A significant correlation between frailty and TMT-B was previously observed (55). Previous studies have also reported a significant impairment of sustained attention (56) and executive function in prefrail (39) and frail (55, 57–60) older adults.
No significant differences were observed between prefrail and non-frail groups in the naming function, assessed by the BNT, in the present work, in contrast to previous studies (39, 61). Because prefrailty is an intermediate state of frailty syndrome, some authors (61) hypothesized that language impairment could contribute to a more rapid progression of the syndrome. Because no relationship was found between frailty state and performance on language tests in our study (40, 60), our results do not support this hypothesis (61).
No significant differences were found between the groups in attentional control assessed by the Luria-NDA subscale. This subscale includes five items assessing selective and sustained attention function. This finding suggests that the mechanisms of attentional control seem preserved in prefrail older adults.
As stated in the introduction, in the literature it is unclear whether prefrailty status is associated with memory or non-memory cognitive domains, or both. Some previous cross-sectional studies focusing on prefrailty, revealed differences in both memory and non-memory cognitive domains (37, 38), and other study found differences only in non-memory domains (39). In general, our findings provide evidence of the susceptibility of the memory cognitive domain to prefrailty status in relatively healthy participants with the same level of education and free of dementia or cognitive complaints. Although we also observed poor performance in other non-memory cognitive domains, adjustments diminished the statistical significance other than delayed visual memory. Thus, our findings contradict studies showing that non-memory domains seem to be influenced first in the prefrail status (39). Importantly, it has been pointed out that not all cognitive subdomains may become impaired simultaneously but may be impaired depending on the specific frailty criteria present and age (37), and this may partially explain the differences among studies. To our knowledge, only one longitudinal study investigated the effects of combinations of cognitive impairment and prefrailty on cognitive outcomes (35), revealing that prefrail participants with cognitive impairments (cognitive prefrailty) had poorer delayed recall at 4-years follow-up. However, only a measure of general cognitive status was used in this study (35). Given the inconsistencies in the results, future longitudinal studies are needed to further explore the association between prefrailty and cognition including neuroimaging findings. Identifying cognitive differences between non-frail and prefrail older adults will be useful for future intervention studies, assisting in the establishment of optimal multimodal strategies.
It is important to note that no significant differences in global cognition evaluated by the MMSE were observed between prefrail and non-frail groups in the present study. However, cognitive differences between the groups were sensitively captured by using the MoCA. This finding suggests that there may be cognitive performance problems related to frailty that are not detectable by the global measurement of the MMSE alone. In this sense, efforts to detect and further understand frailty should include a consistent measurement of specific cognitive domains employing comprehensive neuropsychological testing.
Individual criteria of physical frailty have been previously associated with cognition. In the present paper, we explored the association between objectively measured physical capacity criteria (low grip strength and slow gait speed) and cognitive performance, because they are more prevalent than physiological markers (self-reported exhaustion, unintentional weight loss, and low physical activity) in the prefrail Galician population (62), and they have shown a better ability to predict future disability (63). Moreover, the components most strongly associated with cognitive function among older adults are grip strength and gait speed (6, 17, 34, 37, 39, 64, 65), and weakness and slowness have been shown the first emerging components of physical frailty (66). The rates of change over time of both gait speed and grip strength is strongly correlated with the rate of change in cognition (28). Slow gait speed is a predictor of transitions between mild and severe cognitive decline and mortality (67). Both motor skills (gait and grip strength) contributing to physical frailty and cognition depends on the integrity of the central nervous system (68). A recent neuroimaging study revealed a significant association between gait speed and brain amyloid-β accumulation in the temporal cortex, parietal cortex, precuneus/posterior cingulate cortex, and basal ganglia, and a significant association between weakness and a general brain amyloid-β accumulation (69).
Self-reported fatigue or exhaustion has been also significantly associated with poor global cognition (30, 37) and a higher risk of incident mild cognitive impairment (6) and dementia (33).
The present study demonstrated an association between gait speed and general cognitive performance assessed by the MoCA, immediate memory, and processing speed. Slower gait speed has been previously associated with worse scores in attention, executive function (37), memory tests (70), slow processing speed (37, 38, 71, 72), and verbal fluency (34, 72). Importantly, the combination of slow gait speed and cognitive impairment has been associated with a high risk for progression to dementia (32). However, a more regular and predictable gait pattern, but not gait speed, was previously correlated with cognitive decline in other studies (73). Performance on the TMT-B has been previously associated with performance on usual gait speed tests in older adults with cognitive impairment (74). In our study, gait speed was negatively associated with the performance on the TMT-A reflecting processing speed, but not in the TMT-B associated with executive functions.
Hand-grip strength was positively correlated with visual episodic memory and visuoconstructive abilities in the present study. Low hand-grip strength has been previously associated with reduced cognitive performance over time (68), and with a higher risk of developing mild cognitive impairment (6). Grip-strength has been associated with performance on the MMSE (34, 75), and executive function (37). In a longitudinal study, grip strength performance was associated with a change in verbal ability, spatial ability, processing speed and memory after age 65 years (76). Weakness was the most common initial manifestation in prefrail women (66). Because gender-related differences may exist in both grip-strength and cognitive function, future studies focusing in these differences are needed to get a better understanding of their association.
Our findings may have specific clinical implications since hand-grip is a simple and modifiable factor that can be useful for the monitoring of the progression of cognitive impairment (68).
Finally, it is important to note that in our study, both gait speed and grip strength negatively correlated with depressive symptomatology (GDS-SF score). The relationship between physical frailty and depression has been previously reported (33, 77, 78). It has been shown that frail depressed older adults show worse performance than non-frail depressed in speed-dependent executive functions and verbal fluency (79), and that the severity of physical frailty was associated with poor verbal memory, slower processing speed and decreased working memory (71). These findings suggest that depression seems to be an important condition to take into account when disentangling the association between prefrailty and cognitive impairment. Thus, future research is needed to further explore the mechanisms underlying associations among physical frailty, cognitive dysfunction, and depressive symptoms. Future work should also explore the longitudinal relationships between hand-grip strength and gait speed and cognitive performance.
The main strengths of this preliminary study were the comprehensive neuropsychological evaluation and the focus on the prefrailty status. The main limitation, however, was the small sample size, which may increase the variability of the data and reduce the statistical power. The cross-sectional design and the slight age difference between the groups limited our ability to interpret the cause-effect relationship of the association between physical prefrailty and cognitive performance, since cognitive changes occur over the life span. Future longitudinal studies including comprehensive neuropsychological testing and neuroimaging information are needed to further explore the dynamic nature of both frailty/prefrailty and cognition and the influence of genetic and environmental factors in their relationship.
Our findings confirm that memory cognitive domain may be susceptible to a subclinical state of physical frailty or prefrailty. Knowledge about specific cognitive deficits associated with prefrailty is important as such markers may help early identification of persons at risk of frailty and dementia. We conclude that the comprehensive assessment for cognitive impairment may be effective for identifying prefrail older adults at higher risk of frailty, dementia, and mortality. This may have important clinical implications since prefrail older adults with cognitive impairments are targets for preventive interventions. Both physical and cognitive therapy should be recommended for the prevention and treatment of frailty.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Autonomic Research Ethics of Galicia Committee, Spain (code 2018/049). The patients/participants provided their written informed consent to participate in this study.
LL-L and JM-C: study concept and design. AB, RL-L, NC, and JB-F: acquisition of data. LL-L, AB, and JB-F: analysis and interpretation of data. LL-L and JB-F: drafting of the manuscript. LL-L, AB, AM, JB-F, RL-L, NC, and JM-C: critical revision of the manuscript for important intellectual content. All authors: contributed to the article and approved the submitted version.
This work was supported by Xunta de Galicia (ED431C 2017/49, ED431F 2017/09). LL-L was supported by the Ramon y Cajal Postdoctoral Senior Grant (RYC-2015-18394) from the Spanish Ministry of Economy, Industry and Competitiveness, co-financed by the European Social Fund. JB-F was supported by a predoctoral grant from the Autonomous Government of Galicia (ED481A-2017/219), and the European Union (European Social Fund).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank the Gerontological Complex La Milagrosa for providing access to their facilities and psychophysiological laboratory. We specially thank all the voluntary participants and the staff of the participating centers for their time and dedication (Espazo+60 A Coruña—AFundación, Universidad Senior de A Coruña, Asociación Provincial de Jubilados y Pensionistas UDP de A Coruña, Parroquia de Nuestra Señora de Los Rosales de A Coruña, Asociación Provincial de Amas de Casa, Consumidores y Usuarios de A Coruña).
1. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:146–56. doi: 10.1093/gerona/56.3.M146
2. Alencar MA, Domingues-Dias JM, Costa-Figueirido L, Corrêa-Dias R. Frailty and cognitive impairment among community-dwelling elderly. Arq Neuropsiquiatr. (2013) 71:362–7. doi: 10.1590/0004-282X20130039
3. Auyeung TW, Lee JSW, Kwok T, Woo J. Physical frailty predicts future cognitive decline-a four year prospective study in 2737 cognitively normal older adults. J Nutr Health Aging. (2011) 15:690–4. doi: 10.1007/s12603-011-0110-9
4. Armstrong JJ, Godin J, Launer LJ, White LR, Mitnitski A, Rockwood K, et al. Changes in frailty predict changes in cognition in older men: the honolulu-asia aging study. J Alzheimers Dis. (2016) 53:1003–13. doi: 10.3233/JAD-151172
5. Borges MK, Cezar NO, Santos-Siqueira S, Yassuda M, Cesari M, Aprahamian I. The relationship between physical frailty and mild cognitive impairment in the elderly: a systematic review. J Frailty Aging. (2019) 8:192–7.
6. Boyle PA, Buchman AS, Wilson RS, Leurgans SE, Bennett DA. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J Am Geriatr Soc. (2010) 58:248–55. doi: 10.1111/j.1532-5415.2009.02671.x
7. Buchman A, Boyle PA, Wilson RS, Tang Y, Bennet DA. Frailty is associated with incident Alzheimer's disease and cognitive decline in the elderly. Psychosom Med. (2007) 69:483–9. doi: 10.1097/psy.0b013e318068de1d
8. Chen S, Honda T, Narazaki K, Chen T, Kishimoto H, Haeuchi Y, et al. Physical frailty is associated with longitudinal decline in global cognitive function in non-demented older adults: a prospective study. J Nutr Health Aging. (2017) 22:82–8. doi: 10.1007/s12603-017-0924-1
9. Feng L, Nyunt MSZ, Gao Q, Feng L, Yap KB, Ng TP. Cognitive frailty and adverse health outcomes: findings from the Singapore Longitudinal Ageing Studies (SLAS). J Am Med Dir Assoc. (2017) 18:252–8. doi: 10.1016/j.jamda.2016.09.015
10. Gifford KA, Bell SP, Liu D, Neal JE, Turchan M, Shah AS, et al. Frailty is related to subjective cognitive decline in older women without dementia. J Am Geriatr Soc. (2019) 67:1803–11. doi: 10.1111/jgs.15972
11. Gray SL, Anderson ML, Hubbard RA, LaCroix A, Crane PK, McCornick W, et al. Frailty and incident dementia. J Gerontol A Biol Sci Med Sci. (2013) 68:1083–90. doi: 10.1093/gerona/glt013
12. Han ES, Lee Y, Kim J. Association of cognitive impairment with frailty in community-dwelling older adults. Int Psychogeriatr. (2013) 26:155–63. doi: 10.1017/S1041610213001841
13. Rogers NT, Steptoe A, Cadar D. Frailty is an independent predictor of incident dementia: evidence from the english longitudinal study of ageing. Sci Rep. (2017) 7:15746. doi: 10.1038/s41598-017-16104-y
14. Samper-Ternent R, Al Snih S, Raji MA, Markides KS, Ottenbacher KJ. Relationship between frailty and cognitive decline in older Mexican Americans. J Am Geriatr Soc. (2008) 56:1845–52. doi: 10.1111/j.1532-5415.2008.01947.x
15. Solfrizzi V, Scafato E, Frisardi V, Seripa Logroscino, Maggi, et al. Frailty syndrome and the risk of vascular dementia: The Italian longitudinal study of aging. Alzheimers Dement. (2013) 9:113–22. doi: 10.1016/j.jalz.2011.09.223
16. Borda MG, Soennesyn H, Steves CJ, Vik-Mo AO, Pérez-Zepeda MU, Aarsland D. Frailty in older adults with mild dementia: dementia with Lewy bodies and Alzheimer's disease. Dement Geriatr Cogn Disord. (2019) 9:176–83. doi: 10.1159/000496537
17. Fougère B, Daumas M, Lilamand M, Sourdet S, Delrieu J, Vellas B, et al. Association between frailty and cognitive impairment: cross-sectional data from Toulouse frailty day hospital. J Am Med Dir Assoc. (2017) 18:990. doi: 10.1016/j.jamda.2017.06.024
18. Robertson GM, Savva R, Kenny A. Frailty and cognitive impairment—a review of the evidence and causal mechanisms. Ageing Res Rev. (2013) 12:840–51. doi: 10.1016/j.arr.2013.06.004
19. Arai H, Satake S, Kozaki K. Cognitive frailty in geriatrics. Clin Geriatr Med. (2018) 34:667–75. doi: 10.1016/j.cger.2018.06.011
20. Aliberti MJR, Cenzer IS, Smith AK, Lee SJ, Yaffe K, Covinsky KE. Assessing risk for adverse outcomes in older adults: the need to include both physical frailty and cognition. J Am Geriatr Soc. (2018) 67:477–83. doi: 10.1111/jgs.15683
21. Downer B, Snih SA, Howrey BT, Raji MA, Markides KS, Ottenbacher J. Combined effects of cognitive impairment and pre-frailty on future frailty and death in older Mexican Americans. Aging Ment Health. (2018) 23:1405–12. doi: 10.1080/13607863.2018.1493719
22. Esteban-Cornejo I, Cabanas-Sánchez V, Higueras-Fresnillo S, Ortega FB, Kramer AF, Rodríguez-Artalejo F, et al. Cognitive frailty and mortality in a national cohort of older adults: the role of physical activity. Mayo Clin Proc. (2019) 94:1180–9. doi: 10.1016/j.mayocp.2018.10.027
23. Hao Q, Dong B, Yang M, Dong B, Wei Y. Cognitive impairment in predicting mortality among oldest-old people. Front Aging Neurosci. (2018) 10:295. doi: 10.3389/fnagi.2018.00295
24. Lee WJ, Peng LN, Liang CK, Loh CH, Chen LK. Cognitive frailty predicting all-cause mortality among community-living older adults in Taiwan: a 4-year nationwide population-based cohort study. PLoS ONE. (2018) 13:e0200447. doi: 10.1371/journal.pone.0200447
25. St. John PD, Tyas S, Griffith LE, Menec V. The cumulative effect of frailty and cognition on mortality-results of a prospective cohort study. Int Psychogeriatr. (2016) 29:535–43. doi: 10.1017/S1041610216002088
26. Ávila-Funes JA, Amieva H, Barberger-Gateau P, Le Goff M, Raoux N, Ritchie K, et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: the three-city study. J Am Geriatr Soc. (2009) 57:453–61. doi: 10.1111/j.1532-5415.2008.02136.x
27. Grande G, Haaksma ML, Rizzuto D, Melis RJF, Marengoni A, Onder G, et al. Co-occurrence of cognitive impairment and physical frailty, and incidence of dementia: systematic review and meta-analysis. Neurosci Biobehav Rev. (2019) 107:96–103. doi: 10.1016/j.neubiorev.2019.09.001
28. Buchman AS, Yu L, Wilson RS, Boyle PA, Schneider JA, Bennett DA. Brain pathology contributes to simultaneous change in physical frailty and cognition in old age. J Gerontol A Biol Sci Med Sci. (2014) 69:1536–44. doi: 10.1093/gerona/glu117
29. Jacobs JM, Cohen A, Ein-Mor E, Maaravi Y, Stessman J. Frailty, cognitive impairment and mortality among the oldest old. J Nutr Health Aging. (2011) 15:678–82. doi: 10.1007/s12603-011-0096-3
30. Ma L, Zhang L, Sun F, Li Y, Tang Z. Cognitive function in prefrail and frail community-dwelling older adults in China. BMC Geriatrics. (2019) 19:53. doi: 10.1186/s12877-019-1056-8
31. Macuco C, Batistoni S, Lopes A, Cachioni M, Da Silva Falcão D, et al. Mini-Mental State examination performance in frail, pre-frail, and non-frail community dwelling older adults in Ermelino Matarazzo, São Paulo, Brazil. Int Psychogeriatr. (2012) 24:1725–31. doi: 10.1017/S1041610212000907
32. Montero-Odasso MM, Barnes B, Speechley M, Hunter Muir SW, Doherty TJ, Duque G, et al. Disentangling cognitive-frailty: results from the gait and brain study. J Gerontol A Biol Sci Med Sci. (2016) 71:1476–82. doi: 10.1093/gerona/glw044
33. Panagiotakis SH, Simos P, Zaganas I, Basta M, Perynisaki GS, Fountoulakis N, et al. Self-reported fatigue as a risk index for dementia diagnosis. Eur Geriatr Med. (2018) 9:211–7. doi: 10.1007/s41999-017-0020-4
34. Yassuda MS, Lopes A, Cachioni M, Falcao DVS, Batistoni SST, Guimaraes VV, et al. Frailty criteria and cognitive performance are related: data from the FIBRA study in Ermelino Matarazzo, São Paulo, Brazil. J Nutr Health Aging. (2012) 16:55–61. doi: 10.1007/s12603-012-0003-6
35. Yu R, Morley JE, Kwok T, Leung J, Cheung O, Woo J. The effects of combinations of cognitive impairment and pre-frailty on adverse outcomes from a prospective community-based cohort study of older Chinese people. Front Med. (2018) 6:50. doi: 10.3389/fmed.2018.00050
36. Nishiguchi S, Yamada M, Fukutani N, Adachi D, Tashiro Y, Hotta T, et al. Differential association of frailty with cognitive decline and sarcopenia in community-dwelling older adults. J Am Med Dir Assoc. (2015) 16:120–4. doi: 10.1016/j.jamda.2014.07.010
37. Robertson DA, Savva GM, Coen RF, Kenny RA. Cognitive function in the prefrailty and frailty syndrome. J Am Geriatr Soc. (2014) 62:2118–24. doi: 10.1111/jgs.13111
38. Umegaki H, Makino T, Shimada H, Hayashi T, Cheng XW, Kuzuya M. Cognitive dysfunction in urban-community dwelling prefrail older subjects. J Nutr Health Aging. (2018) 22:549–54. doi: 10.1007/s12603-018-1017-5
39. Wu Y, Liu L, Chen W, Lee L, Peng L, Wang P, et al. Cognitive function in individuals with physical frailty but without dementia or cognitive complaints: results from the I-Lan longitudinal aging study. J Am Med Dir Assoc. (2015) 16:899.e9–16. doi: 10.1016/j.jamda.2015.07.013
40. Rosado-Artalejo C, Carnicero JA, Losa-Reyna J, Guadalupe-Grau A, Castillo-Gallego C, Gutiérrez-Ávila G, et al. Cognitive performance across 3 frailty phenotypes: toledo study for healthy aging. J Am Med Dir Assoc. (2017) 18:785–90. doi: 10.1016/j.jamda.2017.04.008
41. Del Brutto OH, Mera RM, Cagino K, Fanning KD, Milla-Martínez MF, Nieves J, et al. Neuroimaging signatures of frailty: a population-based study in community-dwelling older adults (the Atahualpa Project). Geriatr Gerontol Int. (2017) 17:270–6. doi: 10.1111/ggi.12708
42. Martínez de la Iglesia J, Onís Vilches MC, Dueñas Herrero R, Albert Colomer C, Aguado Taberné C, Luque-Luque R. Versión española del cuestionario de Yesavage abreviado (GDS) para el despistaje de depresión en mayores de 65 años: adaptación y validación. [The Spanish version of the Yesavage abbreviated questionnaire (GDS) to screen depressive dysfunctions in patients older than 65 years]. MEDIFAM. (2002) 12:620–30. doi: 10.4321/S1131-57682002001000003
43. Sheikh JI, Yesavage JA. Geriatric depression scale (GDS). Recent evidence and development of a shorter version. Clin Gerontol. (1986) 5:165–73. doi: 10.1300/J018v05n01_09
44. Bouzón CA, Carnicero JA, Gonzáles-Turín J, García-García FJ, Esteban A, Rodríguez-Mañas L. The standardization of frailty phenotype criteria improves its predictive ability: the toledo study for healthy aging. J Am Med Dir Assoc. (2017) 18:402–8. doi: 10.1016/j.jamda.2016.11.003
45. Blesa R, Pujol M, Aguilar M, Santacruz P, Bertran-Serra I, Hernández G, et al. Clinical validity of the 'Mini-Mental State' for Spanish speaking communities. Neuropsychologia. (2001) 39:1150–7. doi: 10.1016/S0028-3932(01)00055-0
46. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
47. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
48. Manga D, Ramos F. Luria DNA: Diagnóstico Neuropsicológico de Adultos [Luria Adults Neuropsychological Diagnosis]. 2nd Edn. Madrid, España: TEA Ediciones SA (2007).
49. Benton AL. Test de Retención Visual de Benton [Benton Visual Retention Test]. Madrid, España: TEA Ediciones SA (2011).
50. Reitan RM. Validity of the trail making test as an indication of organic brain damage. Percept Mot Skills. (1958) 8:271–6. doi: 10.2466/pms.1958.8.3.271
51. Kaplan E, Goodglass H, Weintraub S. Test de vocabulario de boston [boston naming test]. In: Goodglass H, Kaplan E, García Albea J, editors. Evaluación de la afasia y de los trastornos relacionados [Aphasia assessment and related disorders]. Madrid, España: Médica Panamericana (2005).
52. Cohen J. Cohen, Statistical Power Analysis for the Behavioural Sciences. 2nd Edn. Hillsdale, NJ: Erlbaum (1988).
53. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. (2012) 141:2–18. doi: 10.1037/a0024338
54. Delrieu J, Pahor M, Cantet C, Cesari M, Ousset PJ, Voisin T, et al. Neuropsychological profile of “cognitive frailty” subjects in MAPT study. J Prev Alzheimer's Dis. (2016) 3:151–9. doi: 10.14283/jpad.2016.94
55. Canevelli M, Cesari M, Raganato R, Trentin F, Valleta M, Salati E, et al. Role of frailty in the assessment of cognitive functioning. Mech Ageing Dev. (2019) 181:42–6. doi: 10.1016/j.mad.2019.111122
56. O'Halloran AM, Finucane C, Savva GM, Robertson IH, Kenny RA. Sustained attention and frailty in the older adult population. J Gerontol B Psychol Sci Soc Sci. (2014) 69:147–56. doi: 10.1093/geronb/gbt009
57. Amanzio M, Palermo S, Zucca M, Rosato R, Rubino E, Leotta D, et al. Neuropsychological correlates of pre-frailty in neurocognitive disorders: a possible role for metacognitive dysfunction and mood changes. Front Med. (2017) 15:199. doi: 10.3389/fmed.2017.00199
58. Bunce D, Batterman PJ, Mackinnon AJ. Long-term associations between physical frailty and performance in specific cognitive domains. J Gerontol B Psychol Sci. (2018) 74:919–26. doi: 10.1093/geronb/gbx177
59. Canevelli M, Cesan M, van Kan GA. Frailty and cognitive decline: how do they relate? Clin Nutr Metab Care. (2015) 18:43–50. doi: 10.1097/MCO.0000000000000133
60. Ginsberg TB, Powell L, Patel A, Emrani S, Chopra A, Cavalieti T, et al. Frailty phenotype and neuropsychological test performance: a preliminary analysis. J Am Osteopath Assoc. (2017) 117:683–7. doi: 10.7556/jaoa.2017.134
61. Fabricio D, Da Silva Alexandre T, Nisihara Chagas MH. Frailty and cognitive performance in older adults living in the community: a cross-sectional study. Arch Clin Psychiatry. (2019) 46:151–5. doi: 10.1590/0101-60830000000216
62. Lorenzo-López L, López-López R, Maseda A, Diego-Diez C, Gómez-Caamaño S, Millán-Calenti JC. Prevalence and clinical characteristics of pre-frailty in elderly population: differences by degree of urbanization. J Am Geriatr Soc. (2016) 64:221–3. doi: 10.1111/jgs.13908
63. Romero-Ortuno R, Scarlett S, O'Halloran AM, Kenny RA. Is phenotypical prefrailty all the same? a longitudinal investigation of two prefrailty subtypes in TILDA. Age Ageing. (2019) 49:39–45. doi: 10.1093/ageing/afz129
64. Brigola AG, Rossetti ES, Rodrigues dos Santos B, Neri AL, Zazzeta S, Inouye K, et al. Relationship between cognition and frailty in elderly. Dement Neuropsychol. (2015) 9:110–9. doi: 10.1590/1980-57642015DN92000005
65. Kang JY, Kim CH, Sung EJ, Shin HC, Shin WJ, Jung KH. The association between frailty and cognition in elderly women. Korean J Fam Med. (2016) 37:164–70. doi: 10.4082/kjfm.2016.37.3.164
66. Xue QL, Bandeen-Roche K, Varadhan R, Zhou J, Fried LP. Initial manifestations of frailty criteria and the development of frailty phenotype in the Women's health and aging study II. J Gerontol A Biol Sci Med Sci. (2008) 63A:984–90. doi: 10.1093/gerona/63.9.984
67. Hoogendijk EO, Rijnhart JJM, Skoog J, Robitaille A, Van den Hout A, Ferrucci L, et al. Gait speed as predictor of transition into cognitive impairment: findings from the three longitudinal studies of aging. Exp Gerontol. (2020) 129:110783. doi: 10.1016/j.exger.2019.110783
68. Fritz NE, McCarthy CJ, Adamo DE. Handgrip strength as a means of monitoring progression of cognitive decline- a scoping review. Ageing Res Rev. (2017) 35:122–3. doi: 10.1016/j.arr.2017.01.004
69. Yoon DH, Lee JY, Shin SA, Kim YK, Song W. Physical frailty and amyloid-β deposits in the brains of older adults with cognitive frailty. J Clin Med. (2018) 7:169. doi: 10.3390/jcm7070169
70. McGough EL, Cochrane BB, Pike KC, Logsdon RG, McCurry SM, Teri L. Dimensions of physical frailty and cognitive function in older adults with amnestic mild cognitive impairment. Ann Phys Rehabil Med. (2013) 56:329–41. doi: 10.1016/j.rehab.2013.02.005
71. Arts MHL, Collard RM, Comijs HC, Zuidersma M, Rooij SE, Naarding P, et al. Physical frailty and cognitive functioning in depressed older adults: findings from the NESDO study. J Am Med Dir Assoc. (2016) 17:36–43. doi: 10.1016/j.jamda.2015.07.016
72. Soumaré A, Tavernier B, Alpérovitch A, Tzourio C, Elbaz A. A cross-sectional and longitudinal study of the relationship between walking speed and cognitive function in community-dwelling elderly people. J Gerontol A Biol Sci Med Sci. (2009) 64A:1058–65. doi: 10.1093/gerona/glp077
73. Kikkert LH, Vuillerme N, Van Campen JP, Appels BA, Hortobágyi T, Lamoth CJC. The relationship between gait dynamics and future cognitive decline: a prospective pilot study in geriatric patients. Int Psychogeriatr. (2018) 30:1301–9. doi: 10.1017/S1041610217002770
74. McGough EL, Kelly VE, Logsdon RG, McCurry SM, Cochrane BB, Engel JM, et al. Associations between physical performance and executive function in older adults with mild cognitive impairment: gait speed and the Timed “Up & Go” test. Phys Ther. (2011) 91:1198–207. doi: 10.2522/ptj.20100372
75. Clouston SAP, Brewster P, Richards M, Cooper R, Hardy R, Rubin MS, et al. The dynamic relationships between physical function and cognition in longitudinal aging cohorts. Epidemiol Rev. (2013) 35:33–50. doi: 10.1093/epirev/mxs004
76. Sternäng O, Reynolds CA, Finkel D, Ernsth-Bravell M, Pedersen NL, Dahl Aslan AK. Grip strength and cognitive abilities: associations in old age. J Gerontol. (2016) 71:841–8. doi: 10.1093/geronb/gbv017
77. Lohman M, Dumenci L, Mezuk B. Depression and frailty in late life: evidence for a common vulnerability. J Gerontol Psychol Sci. (2016) 71:630–40. doi: 10.1093/geronb/gbu180
78. Panza F, Lozupone M, Solfrizzi V, Sardone R, Dibello V, Di Lena L, et al. Different cognitive frailty models and health- and cognitive-related outcomes in older age: from epidemiology to prevention. J Alzheimers Dis. (2018) 62:993–1012. doi: 10.3233/JAD-170963
Keywords: aging, prefrailty, neuropsychologial assessment, gait speed, grip strength
Citation: Lorenzo-López L, Blanco-Fandiño J, Cibeira N, Buján A, López-López R, Maseda A and Millán-Calenti JC (2020) Clinical and Neuropsychological Correlates of Prefrailty Syndrome. Front. Med. 7:609359. doi: 10.3389/fmed.2020.609359
Received: 23 September 2020; Accepted: 20 October 2020;
Published: 09 November 2020.
Edited by:
Emanuele Marzetti, Catholic University of the Sacred Heart, ItalyCopyright © 2020 Lorenzo-López, Blanco-Fandiño, Cibeira, Buján, López-López, Maseda and Millán-Calenti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Lorenzo-López, bGF1cmEubG9yZW56by5sb3BlekB1ZGMuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.