
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med., 07 May 2020
Sec. Rheumatology
Volume 7 - 2020 | https://doi.org/10.3389/fmed.2020.00141
This article is part of the Research TopicImaging In Inflammatory Rheumatic Diseases - Recent AdvancesView all 17 articles
 Garifallia Sakellariou1
Garifallia Sakellariou1 Carlo Alberto Scirè2,3*
Carlo Alberto Scirè2,3* Antonella Adinolfi4Alberto Batticciotto5
Antonella Adinolfi4Alberto Batticciotto5 Alessandra Bortoluzzi2Andrea Delle Sedie6
Alessandra Bortoluzzi2Andrea Delle Sedie6 Orazio De Lucia7
Orazio De Lucia7 Christian Dejaco8,9Oscar Massimiliano Epis4Emilio Filippucci10
Christian Dejaco8,9Oscar Massimiliano Epis4Emilio Filippucci10 Luca Idolazzi11
Luca Idolazzi11 Andrea Picchianti Diamanti12
Andrea Picchianti Diamanti12 Alen Zabotti13Annamaria Iagnocco14
Alen Zabotti13Annamaria Iagnocco14 Georgios Filippou2 on behalf of the Musculoskeletal Ultrasound Study Group of the Italian Society of Rheumatology
Georgios Filippou2 on behalf of the Musculoskeletal Ultrasound Study Group of the Italian Society of RheumatologyBackground: Differential diagnosis in early arthritis is challenging, especially early after symptom onset. Several studies applied musculoskeletal ultrasound in this setting, however, its role in helping diagnosis has yet to be clearly defined. The purpose of this work is to systematically assess the diagnostic applications of ultrasonography in early arthritis in order to summarize the available evidence and highlight possible gaps in knowledge.
Methods: In December 2017, existing systematic literature reviews (SLR) on rheumatoid arthritis (RA), osteoarthritis (OA), psoriatic arthritis (PsA), polymyalgia rheumatica (PMR), calcium pyrophosphate deposition disease (CPPD), and gout were retrieved. Studies on ultrasound to diagnose the target conditions and detecting elementary lesions (such as synovitis, tenosynovitis, enthesitis, bone erosions, osteophytes) were extracted from the SLRs. The searches of the previous reviews were updated and data from new studies fulfilling the inclusion criteria extracted. Groups of reviewers worked separately for each disease, when possible diagnostic accuracy (sensitivities, specificities) was calculated from primary studies. When available, the reliability of ultrasound to detect elementary lesions was extracted.
Results: For all the examined disease, recent SLRs were available. The new searches identified 27 eligible articles, with 87 articles included from the previous SLRs. The diagnostic performance of ultrasound in identifying diseases was addressed by 75 studies; in most of them, a single elementary lesion was used to define diagnosis, except for PMR. Only studies on RA included consecutive patients with new onset of arthritis, while studies on gout and CPPD often focused on subjects with mono-arthritis. Most of the remaining studies enrolled patients with a defined diagnosis. Synovitis was the most frequently detected lesion; clinical diagnosis was the most common reference standard. The diagnostic performance of ultrasound across different conditions was extremely variable. Ultrasound to identify elementary lesions was assessed in 38 studies in OA, gout and CPPD. Its performance in OA was very variable, with better results in CPPD and gout. The reliability of ultrasound was moderate to good for most lesions.
Conclusions: Although a consistent amount of literature investigated the diagnostic application of ultrasound, in only a minority of cases its additional value over clinical diagnosis was tested. This SLR underlines the need for studies with a pragmatic design to identify the placement of ultrasound in the diagnostic pathway of new-onset arthritis.
With effective treatment strategies for inflammatory arthropathies becoming extensively available, in the last decade a prompt diagnosis, allowing intervention within the window of opportunity, has become a critical point in the management of early arthritis (1). However, in rheumatology diagnosis can be achieved with certainty in a minority of cases, and this is particularly true when patients are assessed at very early stages of diseases. While in some cases the presence of valuable biomarkers, such as anticyclic citrullinated peptides antibodies (ACPA), drives the diagnostic process, in seronegative early arthritis the degree of uncertainty remains high. Moreover, the current classification criteria for the main rheumatic diseases, which are often inappropriately used to help diagnosis, require differential diagnosis to be performed before they are applied (2). This difficulty in the correct definition of diagnoses at early stages might lead to inappropriate management, delaying the start of effective treatment but also exposing patients to useless and potentially toxic drugs. In addition, also in a research setting, an imprecise diagnosis implies the impossibility to measure reliably the effect of innovative treatments in early phases. In this context, there is a great interest in the research of new biomarkers and new tools to help the diagnostic process.
Musculoskeletal ultrasonography has been widely applied in rheumatic diseases, demonstrating to be a valid and reproducible tool in both inflammatory and non-inflammatory pathologies. The relevance of this instrument has also been recognized by the European League Against Rheumatism (EULAR), that recommends ultrasound among the imaging which can be considered to help the clinical management of several conditions (3–5). The applications of ultrasound cover the areas of diagnosis, assessment of prognosis, follow-up of diseases and guide for intra-articular and peri-tendinous procedures. In the field of diagnosis, most of the studies on ultrasound investigated the frequency of elementary lesions characteristics of diseases, thus providing information on the diagnostic performance of this tool to detect single abnormalities or on the performance of single lesions to diagnose a disease. On the other hand, only a minority of studies tests the diagnostic value of combinations of lesions, assessed at the same time. Moreover, in this context elementary lesions are not selected based on their diagnostic properties and specificity for a certain condition. Only a minority of studies, in which the added value of ultrasound is tested jointly with clinical evaluation (6, 7), apply a pragmatic design that reproduces the clinical context. The lack of information on the application of ultrasound in a realistic clinical process of diagnosis translates into the limited weight given to this imaging in classification criteria. For instance, the only role for ultrasound in Rheumatoid Arthritis (RA) classification is the possible confirmation of the presence of synovitis (2), while to date the only classification criteria including ultrasound are those for polymyalgia rheumatica (PMR) (8).
Given the limited availability of methodologically sound studies to address the diagnostic performance of ultrasound in a realistic clinical context of differential diagnosis of inflammatory arthropathies, the Ultrasound Study Group of the Italian Society for Rheumatology (SIR) prioritized its research on this subject. The present study represents the first step of such project. The aim of the present work was the evaluation of the available literature on the diagnostic application of ultrasound in inflammatory arthropathies.
As a first step, the most relevant differential diagnoses in patients with suspected inflammatory arthropathies were identified, including also osteoarthritis (OA) as a relevant differential diagnosis. We afterwards individuated two research questions, rephrased following the PICOs (Patient, Intervention, Comparator, Outcome, Study type) methodology to provide inclusion and exclusion criteria (Table 1). On this basis, we planned separate systematic literature reviews (SLR) to assess the diagnostic performance of ultrasound to diagnose OA, RA, psoriatic arthritis (PsA), PMR, gout, calcium pyrophosphate deposition disease (CPPD). The SLRs were not registered, but a common protocol was available for all researchers before the beginning of the process. The diagnostic performance of ultrasound in detecting elementary lesions was also addressed. If studies on diagnostic performance reported also data on intra and inter-reader reliability on elementary lesions, that information was also extracted. Working groups composed by supervisors and fellows were created to work separately on each topic, participants were selected based on the expertise on the specific disease and on SLR methodology to create uniform groups. The most recent SLRs on ultrasound in the same diseases were first sought in electronic databases (5, 9–13). Some of the authors involved in the present project were also co-authors of these SLR and could provide background material (AA, ABa, AI, AZ, CS, EF, GF, GS). Since many of the existing SLR had a broader focus, only primary studies focusing on the diagnostic use of ultrasound were taken into account for the present work.
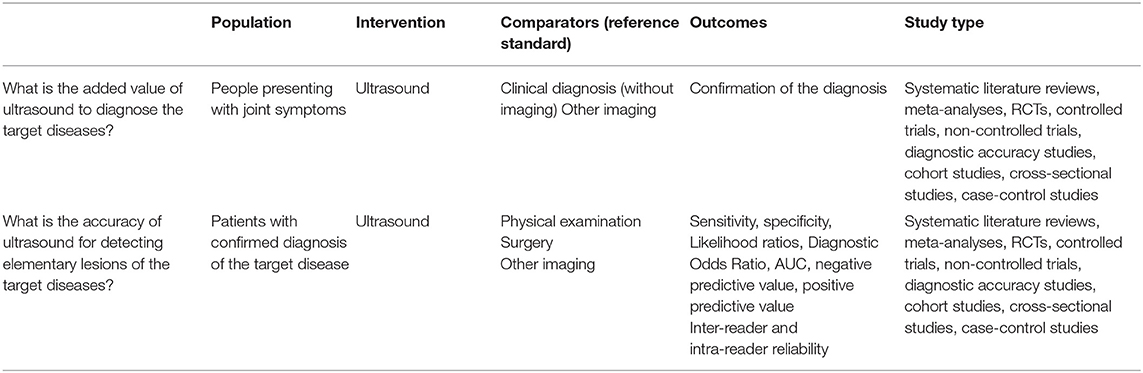
Table 1. Inclusion criteria for research questions.
The search strategies of the previous SLR were applied in PubMed and Embase, starting from the date of the last search of the previous reviews (5, 9–13). Searches were last run on November 30th 2017. The search on PubMed and Embase was selected because we expected that all the relevant literature would be retrieved, and we did not expect to find further evidence including other databases. The records retrieved from the new searches were transferred into a bibliographic manager software (Zotero, RRID:SCR_013784) and libraries shared with each working group. The titles and abstracts of the retrieved records were evaluated by pairs of reviewers to assess the eligibility for full-text review according to the pre-specified criteria. Full-texts were afterwards evaluated by the same criteria and data from the included studies extracted into a standardized form, including 2 × 2 tables of diagnostic performance. A flow-chart describing the selection process was separately generated for each SLR. Results were summarized through summary of findings tables, describing both studies included in the previous reviews and those identified by the present ones.
In total, all search strategies retrieved 943 references since the date of the last search of the previous SLRs. The higher number of references belonged to the fields of PsA and gout (Additional Online File). After reviewing the abstracts, 27 papers were finally included, together with 87 articles from previous SLRs meeting the inclusion criteria, for a total of 114 papers included in the present SLR (Table 2). The PRISMA flow-chart of the SLR for each disease is available in the Additional Online File, as well as the full results, presented through summary of findings tables.

Table 2. Features of the SLRs used as a basis for the present work.
Information regarding the value of ultrasound to diagnose diseases could be extracted from 75 studies. The greatest amount of evidence was available for PsA, with 29 studies assessing the diagnostic performance of ultrasound.
There were meaningful differences in terms of enrolled populations across different diseases. In fact, in studies addressing PsA and OA, the primary aim was mostly to report the prevalence of different lesions. The frequency of each lesion was compared in patients with already known PsA or OA and healthy controls or patients with other definite diseases. A realistic clinical scenario of consecutive patients referred for suspicion of inflammatory arthropathy was rarely available (6).
Conversely, studies on RA evaluated the added value of ultrasound over classification criteria (14–17), the added value for diagnosis on top of clinical findings (18–20) or its prognostic value over the future development of RA (21–25) by cross-sectional or longitudinal study design.
Studies dealing with PMR mostly included populations of consecutive patients with shoulder pain (8, 13, 26) and some of them evaluated the additional value of ultrasound on the diagnostic performance of the 2012 classification criteria (8, 26, 27).
In the fields of both gout and CPPD, most of the studies included patients presenting with mono-arthritis and with suspect crystal-related arthritis.
Despite these discrepancies across different conditions, there were only a few studies, mainly focused on RA, that enrolled a population of consecutive patients with joint pain (6, 16–20, 22, 24, 28).
The interventions used to help diagnosis were also variable. Since most of the studies did not have diagnostic accuracy as primary objective, data on the diagnosis of disease were based on single elementary lesions. A relevant exception was represented by PMR, for which some studies addressed different lesions (tenosynovitis, bursitis and synovitis) in combination (8, 26, 27). Graph 1 summarizes all the different lesions used to define diagnosis.

Graph 1. Number of studies using each single elementary lesion to establish diagnoses, alone or in combination. CPP, calcium pyrophosphate; MSU, monosodium urate.
The confirmation of the diagnosis was based on a variety of reference standards, which depended on the diagnostic suspicion, as expected. While clinical diagnosis was frequently considered in RA and PMR, for PsA the confirmation of diagnosis mostly relied on clinical diagnosis and classification criteria, while synovial fluid analysis was frequently considered in crystal-related arthropathies (Graph 2).
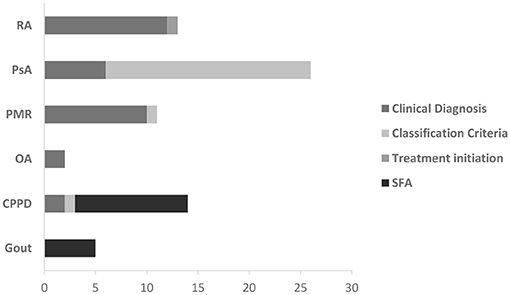
Graph 2. Reference standards adopted to confirm diagnoses. PMR, polymyalgia rheumatica; CPPD, calcium pyrophosphate deposition disease; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SFA, synovial fluid analysis.
The study design adopted to define diagnostic accuracy was also widely variable. While studies aiming to diagnose RA were mainly cohort studies (15–24, 28), in the field of PsA emerged a significant prevalence of studies with a case-control design; controls were represented mostly by patients with RA (29–37), while in some studies also healthy controls were included (29, 31, 33, 38–43). For the remaining diseases, the type of study was more variable (Graph 3).
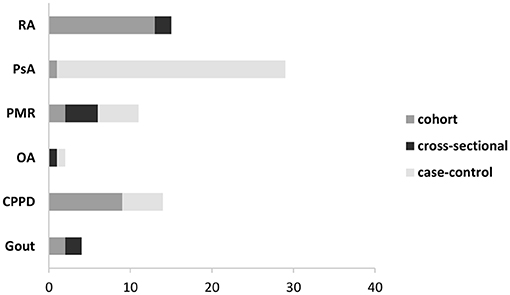
Graph 3. Study design of the included studies, depending on the assessed disease. PMR, polymyalgia rheumatica; CPPD, calcium pyrophosphate deposition disease; OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SFA: synovial fluid analysis.
In OA, adding ultrasound information to the clinical evaluation increased the certainty of the diagnosis made by the clinician (6), while the likelihood of OA, compared to being healthy, increased with the finding of bone erosions (44).
In the field of RA, some studies supported the possibility to integrate clinical and ultrasound findings to reclassify undifferentiated arthritis (14–17, 21), while in other studies ultrasound information was applied to confirm a diagnosis of RA or tested against a clinical diagnosis (18–20), leading in general to an increase in diagnostic performance. The prognostic value of ultrasound in predicting the future development of the disease or the need for specific treatment has also been tested, once again with positive results supporting this application (22–24, 28) (Tables 3, 4). The most specific lesion to diagnose RA were bone erosions, with the specificity of 1 reported by a single study (19), although also the specificity of PD positive synovitis was high (ranging from 0.88 to 0.93).

Table 3. Performance of ultrasound to detect RA by elementary lesions and reliability.
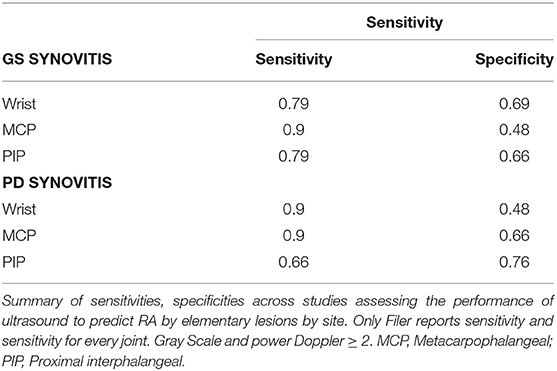
Table 4. Performance of ultrasound to predict RA by elementary lesions by site.
Despite a higher number of studies with a focus on PsA, in this area there was a greater variability, due to many different lesions, tissues and sites assessed. Many studies (14 studies) focused on the assessment of entheseal abnormalities (30, 34, 35, 39, 40, 42, 45–52) and the joints (6 studies) (29, 32, 33, 38, 41, 53), while only a few studies assessed the fingers (considering joints, tendons, soft tissues and entheses) (31, 36, 37) or the nails (43, 54, 55). The primary aim of the included studies rarely addressed the diagnostic accuracy. In fact, most of the studies compared the prevalence of lesions in PsA and other diseases. Also, for this, the diagnostic performance of ultrasound findings, which were usually considered alone and not in combination or in addition to clinical findings, was extremely variable across lesions and sites (Table 5). Among the tested lesions, those proving to be more specific to detect PsA were those at the level of the entheses. In fact, the specificity of entheseal PD ranged from 0.33 to 0.99, of enthesophytes from 0.52 to 1 and of calcifications from 0.86 to 0.97. Peritenonitis was also very specific (from 0.95 to 1 when PD signal was present).

Table 5. Performance of ultrasound lesions to detect PsA and reproducibility.
Studies focusing on ultrasound of the hips and the shoulders in PMR had a more variable design. In fact, along with some older studies with a case-control design (8, 56–59) several cohort studies, including that on which the current classification criteria are based (8), included consecutive patients with shoulder pain (34, 60). Moreover, several recent studies provided external validation for the classification criteria (26). Again, in terms of accuracy, studies yielded very heterogeneous results (Table 6). In general, bilateral findings seemed to be more specific for PMR. The specificity of bilateral subacromiodeltoid bursitis ranged from 0.68 to 0.99, while for bilateral long head of the biceps tenosynovitis ranged from 0.62 to 0.98.

Table 6. Performance of ultrasound lesions to detect PMR.
Studies in CPPD evaluated several different sites, including the knees (61–68), the wrist (69, 70), the affected joint or all joints (71). Study design was variable, including both case-control and cohort studies. The diagnosis of CPPD was confirmed more frequently by synovial fluid analysis, while in some cases a clinical diagnosis (70, 71) or histology (68) were used as references. In general, ultrasound seemed to perform well in identifying this condition, especially at the knee and the wrist. The specificity to confirm CPPD at the knee (considering all the assessed sites) ranged from 0.66 to 1, while at the wrist from 0.81 to 0.91.
In the field of gout, the type of joint under investigation was widely variable, all studies (72–74) but two (75, 76) adopted synovial fluid analysis as reference standard to diagnose the disease. 4/6 studies had a cross-sectional design, while the two remaining were a prospective (73) and a retrospective (72) study. While 4 studies reported a satisfactory performance of ultrasound (73–75, 77), for 2 studies sensitivity was low (72, 76). Considering the combination of all possible elementary lesions (e.g., double contour, aggregates, tophi), the specificity of ultrasound to diagnose gout ranged from 0.42 to 0.87.
Data on the accuracy of ultrasound to detect elementary lesions were extracted only for OA, CPPD and gout, with 20 (78–96), 12 (68–70, 97–104), and 6 (105–110) studies addressing this aspect, respectively (Tables 7–10).
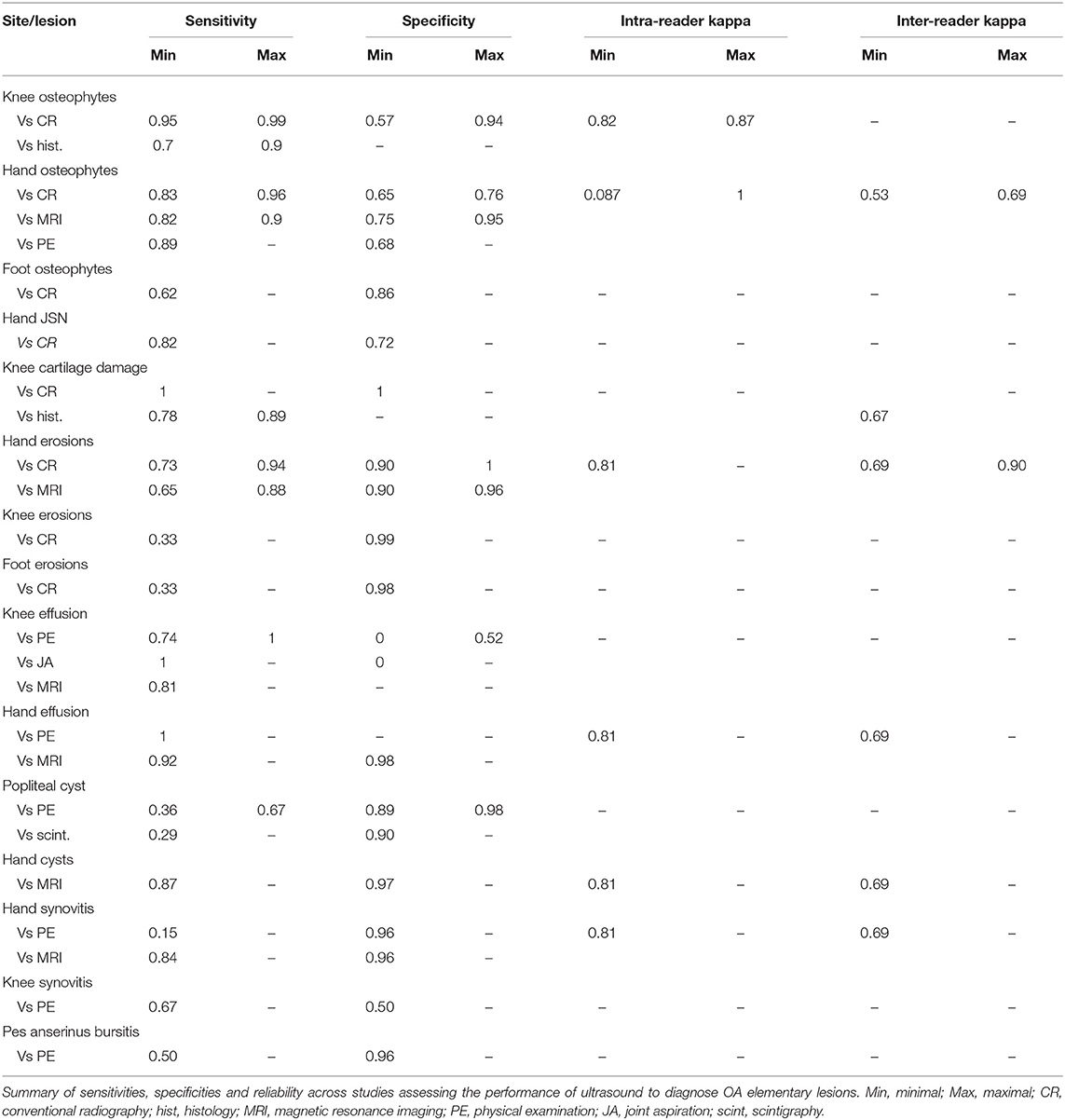
Table 7. Performance of ultrasound to detect osteoarthritis elementary lesions and reliability.

Table 8. Performance of ultrasound to detect CPPD elementary lesions and reproducibility.
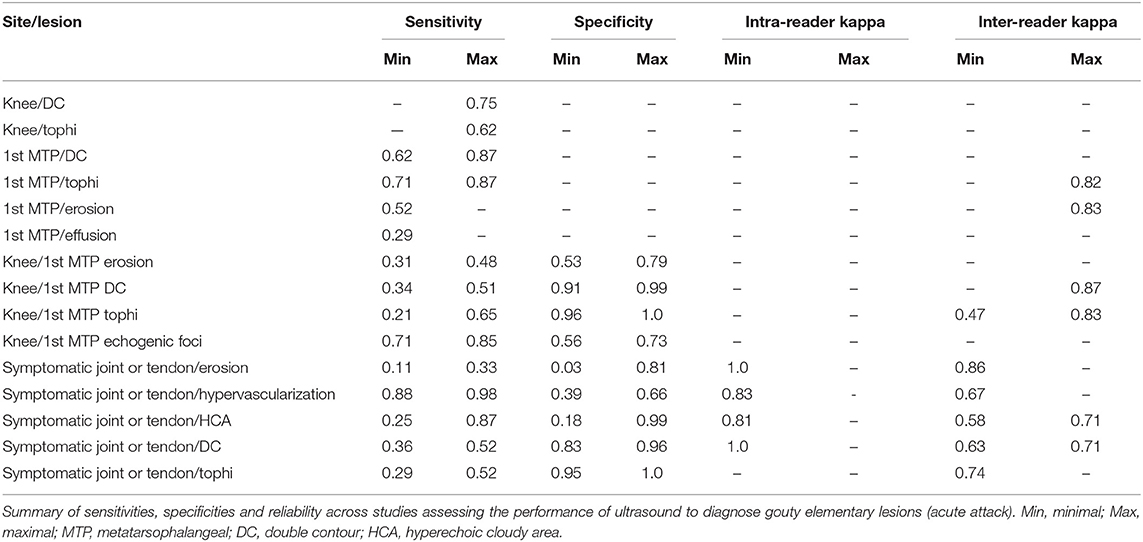
Table 9. Performance of ultrasound to detect gout elementary lesions and reproducibility (acute attack).
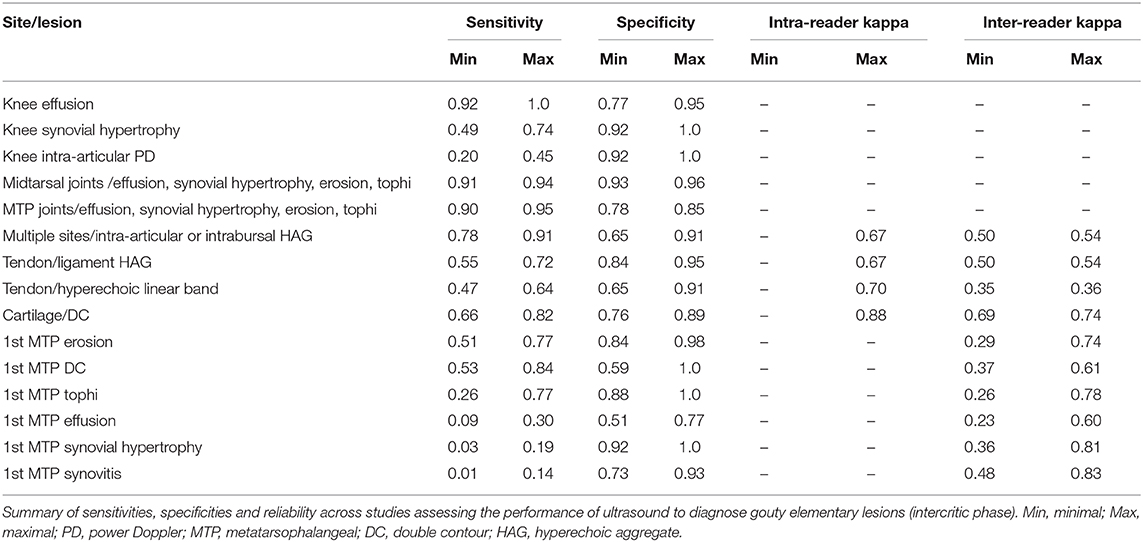
Table 10. Performance of ultrasound to detect gout elementary lesions and reproducibility (intercritic phase).
The typical population enrolled was represented by subjects with confirmed disease, in which ultrasound was compared to a reference standard to confirm the presence of a lesion.
As expected, also the reference standard was variable, in particular for OA. For CPPD, the only assessed target lesion was CPP deposition, which was evaluated by conventional radiography (2 studies), synovial fluid analysis (6 studies), microscopic analysis (2 studies). All studies on gout but one (107), in which conventional radiography was used, adopted synovial fluid analysis as reference standard.
Most of the studies assessing ultrasound to detect elementary lesions had a cross-sectional design, in particular, all the studies on OA, 4 (74–77) and 9 (62, 69, 70, 99–101, 103) studies for gout and CPPD, respectively, while the remaining studies for these two conditions had a cohort design.
In OA, results on the performance of ultrasound were once again widely variable across studies. This was also due to the variability of the reference standards adopted to define each separate lesion and the assessment of different anatomical areas.
Most of the studies on CPPD reported good performance of ultrasound to detect deposits, and this was true especially for specificity. The same conclusions can be drawn from the included articles on gout.
Most of the studies on OA in which reliability data were presented reported good reliability for the assessment of osteophytes, erosions, effusion, cartilage damage, synovitis and cysts (Table 7).
In RA, the available evidence supported a good intra-reader and inter-reader reliability for erosions, GS and PD synovitis across all the assessed sites (Tables 3, 4).
There was less information about reliability in the ultrasound assessment of PsA; entheseal PD, synovial hypertrophy and bursitis were the only lesions for which reliability was available. Inter-reader reliability was good for synovial hypertrophy and bursitis, as well as intra-reader for entheseal PD and bursitis (Table 5).
Among the included studies on PMR, none reported information on the reliability for the assessed lesions.
For CPPD, some studies reported a good inter-reader reliability to assess both the meniscal fibrocartilage and the hyaline cartilage at the level of the knee (Table 8). In gout during acute attacks, very good intra-reader reliability was reported for double contour, aggregates, erosions and hypervascularisation. Inter-reader reliability was assessed for tophi, erosions, double contour, hypervascularisation and aggregates, still with good values (Table 9). The reliability on the same lesions was also assessed in the intercritical phases, with still good, although in general lower, results (Table 10).
The aim of our SLR was that of retrieving all the available evidence to support future studies on the integration of the information provided by ultrasound in the diagnostic process. Several groups had already focused on this aspect, since recent SLRs were available for all of the conditions of our interest (5, 9, 11, 13, 104). The existing reviews presented a summary of the diagnostic use of ultrasound deriving from a relevant number of studies for each considered disease. Despite all the reviews being relatively recent, we found additional studies in the subsequent literature from which we could retrieve further evidence. The number of SLRs and eligible studies represents a clue of the interest that ultrasound as diagnostic tool has raised. The easier availability of high-end ultrasound equipment, the accessibility to training and the possibility to apply directly the information provided by ultrasound during a routine visit are likely the features that have driven the enthusiasm about the technique. However, when analyzing in depth the available literature, there is an evident gap between the interest in the diagnostic applications of ultrasound and the quality of the studies produced so far in this field. In fact, with some important exceptions, the main objective of the studies was that of describing the prevalence of different lesions and comparing groups of patients in terms of ultrasound findings. Although information on diagnostic accuracy can be retrieved also from such study design, these results cannot be generalized to external populations, since a realistic clinical setting is not reproduced.
Many studies, in fact, included patients with definite and longstanding diagnosis and adopted a case-control design, with controls that were unlikely to be very similar to the true differential diagnoses of disease. This is particularly true for PsA, for which most of the studies had a case-control design.
There was limited evidence regarding the diagnosis of OA (6), while for RA and PMR the studies reproduced a more pragmatic context. In fact, in RA, some studies evaluated patients with new-onset arthralgia and tested the ability of ultrasound to help confirm diagnosis (19), while some others integrated ultrasound on top of classification criteria (16, 17). There were also some studies testing the prognostic value of ultrasound on the future development of RA (22).
In the context of PMR, some older studies still adopted a case-control design (56), however, since the development of the new classification criteria (8), the interest has shifted to the evaluation of the additional impact of ultrasound on classification (26). The performance of US in this context was highly variable. Such heterogeneous results might be due to the disease, which may present with variable abnormalities, thus affecting the US sensitivity. Bilateral pathologic conditions appear to be the most specific US findings.
In the field of crystal-related arthropathies, several studies evaluated both patients during the acute presentation and the inter-critical periods. The population of interest was that of patients presenting with monoarthritis, representing a realistic clinical scenario for this diagnostic suspicion, although quite specific.
The ability of ultrasound to correctly identify elementary lesions typical of each disease seemed to be good, and this was especially true for inflammatory lesions. When a suboptimal performance was achieved, it must be kept in mind that in several studies the reference standard adopted to define a lesion (e.g., physical examination) could not be considered the optimal one for the specific lesion.
Although this was not the primary objective of this SLR, we extracted information on intra and inter-reader reliability, if available. The information from the primary studies supported good reliability of ultrasound to identify inflammatory lesions, as well as signs of damage, at the level of joints and entheses, as well as deposition of crystals. It must however be considered that rheumatologists taking part in ultrasound studies might have greater expertise on a specific lesion or disease than average, so that such reliabilities could not be reproduced in a clinical setting.
The present SLR has some limitations. First, only two databases were searched, and, although probably the greatest part of the literature has been covered, we cannot exclude the presence of further studies, even among gray literature. Due to the clinical heterogeneity of the results, we did not perform a pooled estimate of the diagnostic performance. Moreover, a formal assessment of quality and risk of bias was not performed. However, the present work is, to our knowledge, the first one to provide a comprehensive overview on the diagnostic use of ultrasound in arthritis, with a focus on the general question and without concentrating on a single disease.
What emerges from the overview of the results of our SLR is that a very few studies (6, 16, 19, 22, 24) investigated the additional impact of ultrasound findings in making a diagnosis in consecutive patients presenting with joint symptoms, which is indeed the typical scenario of every day's rheumatologist work.
In most studies, clinical and ultrasound assessments were performed separately, and ultrasound findings were not evaluated on top of clinical findings but validated against clinical diagnosis. With this being almost the only evidence available today, it is of no surprise that so far, the relevance of ultrasound in recommendations on the diagnosis and management of rheumatic diseases and in classification criteria is so limited. This happens despite ultrasound being an ideal tool in this context: adequate ultrasound equipment can now be easily accessible, they can be used during scheduled visits and provide immediately helpful information. Multiple sites can be assessed at the same time with good acceptability by the patients. Several other modern imaging have been applied in the setting of early arthritis, such as magnetic resonance imaging (MRI), positron emission tomography (PET) od dual energy CT (DECT), however they present a limited feasibility compared to ultrasound, limited availability, higher costs and, in some cases, limited data in the clinical setting. Since the accuracy of ultrasound in detecting elementary lesions has been established and the increasing ultrasound expertise across rheumatologists allows at least some findings to be detected reliably, the time has come to test the real potentialities of ultrasound during the first evaluation for the suspicion of inflammatory arthropathy. The Musculoskeletal ultrasound Study Group of the Italian Society for Rheumatology has recently focused on the design of such study, which implies the definition of the ideal combination of joints to be assessed based on the clinical suspicion and confirming diagnoses after a follow-up. Before the application of ultrasound, an initial set of differential diagnoses should be defined for each patient, based on clinical features. The additional value of an ultrasound examination, targeted on the clinical suspicion, would afterwards be tested in terms of correct and timely diagnosis. We expect that these results will help clarify the real role of ultrasound through the process of diagnosis and help giving a new insight into its correct placement in the management of inflammatory arthropathies.
The datasets generated for this study are available on request to the corresponding author.
GS, SC, GF, and AI conceived the study and supervised its conduction. SC performed the searches in the electronic databases. AA, ABa, ABo, AD, OD, CD, OE, EF, LI, AP, AZ, and GS performed the systematic literature review. GS drafted the manuscript. All authors revised critically the article, read and approved its final version for submission.
This work was supported by the Italian Society of Rheumatology by affording the open access fees.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Authors would like to thank Cecilia Agnes, Irene Azzolin, Emanuela Bellis, Nicola Boffini Marco Canzoni, Marta Caprioli, Linda Carli, Francesco Cavatorta, Giovanni Ciancio, Giovanna Cuomo, Andrea Di Matteo, Ilaria Farina, Matteo Filippini, Valentina Foschi, Alessandra Gabba, Ariela Hoxha, Federica Martinis, Claudio Mastaglio, Augusta Ortolan, Simone Parisi, Marco Piras, Francesco Porta, Bernd Raffeiner, Roberta Ramonda, Daniela Rossi, Silvia Rossi, Crescenzio Scioscia, Palma Scolieri, Teodora Serban, Riccardo Terenzi, Giulia Tesei, Ilaria Tinazzi, Carmela Toscano, Carlo Venditti, and Gentiana Vukatana for contributing to the SLR.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2020.00141/full#supplementary-material
1. Smolen JS, Breedveld FC, Burmester GR, Bykerk V, Dougados M, Emery P, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. (2016) 75:3–15. doi: 10.1136/annrheumdis-2015-207524
2. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. (2010) 69:1580–8. doi: 10.1136/ard.2010.138461
3. Mandl P, Navarro-Compan V, Terslev L, Aegerter P, van der Heijde D, D'Agostino MA, et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann Rheum Dis. (2015) 74:1327–39. doi: 10.1136/annrheumdis-2014-206971
4. Colebatch AN, Edwards CJ, Østergaard M, van der Heijde D, Balint PV, D'Agostino M-A, et al. EULAR recommendations for the use of imaging of the joints in the clinical management of rheumatoid arthritis. Ann Rheum Dis. (2013) 72:804–14. doi: 10.1136/annrheumdis-2012-203158
5. Sakellariou G, Conaghan PG, Zhang W, Bijlsma JWJ, Boyesen P, D'Agostino MA, et al. EULAR recommendations for the use of imaging in the clinical management of peripheral joint osteoarthritis. Ann Rheum Dis. (2017) 76:1484–94. doi: 10.1136/annrheumdis-2016-210815
6. Matsos M, Harish S, Zia P, Ho Y, Chow A, Ioannidis G, et al. Ultrasound of the hands and feet for rheumatological disorders: influence on clinical diagnostic confidence and patient management. Skeletal Radiol. (2009) 38:1049–54. doi: 10.1007/s00256-009-0738-2
7. D'Agostino M-A, Saraux A, Chary-Valckenaere I, Marcelli C, Guis S, Gaudin P, et al. Can we improve the diagnosis of spondyloarthritis in patients with uncertain diagnosis? The EchoSpA prospective multicenter French cohort. Joint Bone Spine Rev Rhum. (2012) 79:586–90. doi: 10.1016/j.jbspin.2012.02.007
8. Dasgupta B, Cimmino MA, Maradit-Kremers H, Schmidt WA, Schirmer M, Salvarani C, et al. 2012 Provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. (2012) 71:484–92. doi: 10.1016/j.ymed.2012.09.009
9. Zabotti A, Bandinelli F, Batticciotto A, Scirè CA, Iagnocco A, Sakellariou G, et al. Musculoskeletal ultrasonography for psoriatic arthritis and psoriasis patients: a systematic literature review. Rheumatology. (2017) 56:1518–32. doi: 10.1093/rheumatology/kex179
10. Filippou G, Adinolfi A, Iagnocco A, Filippucci E, Cimmino M.A, Bertoldi I, et al. Ultrasound in the diagnosis of calcium pyrophosphate dihydrate deposition disease. a systematic literature review and a meta-analysis. Osteoarthr Cartil. (2016) 24:973–81. doi: 10.1016/j.joca.2016.01.136
11. Chen J, Liao M, Zhang H, Zhu D. Diagnostic accuracy of dual-energy CT and ultrasound in gouty arthritis: a systematic review. Z Rheumatol. (2017) 76:723–9. doi: 10.1007/s00393-016-0250-8
12. Lage-Hansen PR, Lindegaard H, Chrysidis S, Terslev L. The role of ultrasound in diagnosing rheumatoid arthritis, what do we know? an updated review. Rheumatol Int. (2017) 37:179–87. doi: 10.1007/s00296-016-3587-z
13. Mackie SL, Koduri G, Hill CL, Wakefield RJ, Hutchings A, Loy C, et al. Accuracy of musculoskeletal imaging for the diagnosis of polymyalgia rheumatica: systematic review. RMD Open. (2015) 1:e000100. doi: 10.1136/rmdopen-2015-000100
14. Filer A, De Pablo P, Allen G, Nightingale P, Jordan A, Jobanputra P, et al. Utility of ultrasound joint counts in the prediction of rheumatoid arthritis in patients with very early synovitis. Ann Rheum Dis. (2011) 70:500–7. doi: 10.1136/ard.2010.131573
15. Kawashiri SY, Suzuki T, Okada A, Yamasaki S, Tamai M, Nakamura H, et al. Musculoskeletal ultrasonography assists the diagnostic performance of the 2010 classification criteria for rheumatoid arthritis. Mod Rheumatol. (2013) 23:36–43. doi: 10.3109/s10165-012-0628-7
16. Nakagomi D, Ikeda K, Okubo A, Iwamoto T, Sanayama Y, Takahashi K, et al. Ultrasonographic assessment of synovitis improves the accuracy of 2010 american college of rheumatology/European league against rheumatism classification criteria for rheumatoid arthritis to predict development of a methotrexate-requiring disease. Ann Rheum Dis. (2013) 65:890–8.
17. Ji L, Deng X, Geng Y, Song Z, Zhang Z. The additional benefit of ultrasonography to 2010 ACR/EULAR classification criteria when diagnosing rheumatoid arthritis in the absence of anti-cyclic citrullinated peptide antibodies. Clin Rheumatol. (2017) 36:261–7. doi: 10.1007/s10067-016-3465-9
18. Minowa K, Ogasawara M, Murayama G, Gorai M, Yamada Y, Nemoto T, et al. Predictive grade of ultrasound synovitis for diagnosing rheumatoid arthritis in clinical practice and the possible difference between patients with and without seropositivity. Mod Rheumatol. (2015) 3:1–6. doi: 10.3109/14397595.2015.1069457
19. Broll M, Albrecht K, Tarner I, Müller-Ladner U, Strunk J. Sensitivity and specificity of ultrasonography and low-field magnetic resonance imaging for diagnosing arthritis. Clin Exp Rheumatol. (2012) 30:543–7.
20. Rezaei H, Torp-Pedersen S, Af Klint E, Backheden M, Kisten Y, Györi N, et al. Diagnostic utility of musculoskeletal ultrasound in patients with suspected arthritis–a probabilistic approach. Arthritis Res Ther. (2014) 16:448. doi: 10.1186/s13075-014-0448-6
21. Salaffi F, Ciapetti A, Gasparini S, Carotti M, Filippucci E, Grassi W. A clinical prediction rule combining routine assessment and power doppler ultrasonography for predicting progression to rheumatoid arthritis from early-onset undifferentiated arthritis. Clin Exp Rheumatol. (2010) 28:686–94.
22. Navalho M, Resende C, Rodrigues AM, Alberto Pereira DSJ, Fonseca JE, Campos J, et al. Bilateral evaluation of the hand and wrist in untreated early inflammatory arthritis: A comparative study of ultrasonography and magnetic resonance imaging. J Rheumatol. (2013) 40:1282–92. doi: 10.3899/jrheum.120713
23. Ozgul A, Yasar E, Arslan N, Balaban B, Taskaynatan MA, Tezel K, et al. The comparison of ultrasonographic and scintigraphic findings of early arthritis in revealing rheumatoid arthritis according to criteria of American College of Rheumatology. Rheumatol Int. (2009) 29:765–8. doi: 10.1007/s00296-008-0765-7
24. Platt PN, Pratt A. The predictive value of musculoskeletal ultrasound in unselected early arthritis clinic patients with polyarthralgia. Rheumatology. (2013) 52:i65.
25. Tămaş MM, Rednic N, Felea I, Rednic S. Ultrasound assessment for the rapid classification of early arthritis patients. J Investig Med. (2013) 61:1184–91. doi: 10.2310/JIM.0000000000000005
26. Macchioni P, Boiardi L, Catanoso M, Pazzola G, Salvarani C. Performance of the new 2012 EULAR/ACR classification criteria for polymyalgia rheumatica: Comparison with the previous criteria in a single-centre study. Ann Rheum Dis. (2014) 73:1190–3. doi: 10.1136/annrheumdis-2013-204167
27. Weigand S, Ehrenstein B, Fleck M, Hartung W. Joint involvement in patients with early polymyalgia rheumatica using high-resolution ultrasound and its contribution to the EULAR/ACR 2012 classification criteria for polymyalgia rheumatica. J Rheumatol. (2014) 41:730–4. doi: 10.3899/jrheum.130946
28. Zufferey P, Rebell C, Benaim C, Ziswiler HR, Dumusc A, So A. Ultrasound can be useful to predict an evolution towards rheumatoid arthritis in patients with inflammatory polyarthralgia without anticitrullinated antibodies. Joint Bone Spine. (2017) 84:299–303. doi: 10.1016/j.jbspin.2016.05.011
29. Gutierrez M, Filippucci E, Salaffi F, Di Geso L, Grassi W. Differential diagnosis between rheumatoid arthritis and psoriatic arthritis: the value of ultrasound findings at metacarpophalangeal joints level. Ann Rheum Dis. (2011) 70:1111–4. doi: 10.1136/ard.2010.147272
30. Iagnocco A, Spadaro A, Marchesoni A, Cauli A, de Lucia O, Gabba A, et al. Power doppler ultrasonographic evaluation of enthesitis in psoriatic arthritis. a multi-center study. Joint Bone Spine. (2012) 79:324–5. doi: 10.1016/j.jbspin.2011.10.005
31. Lin Z, Wang Y, Mei Y, Zhao Y, Zhang Z. High-Frequency ultrasound in the evaluation of psoriatic arthritis: a clinical study. Am J Med Sci. (2015) 350:42–6. doi: 10.1097/MAJ.0000000000000504
32. Melchiorre D, Calderazzi A, Maddali Bongi S, Cristofani R, Bazzichi L, Eligi C, et al. A comparison of ultrasonography and magnetic resonance imaging in the evaluation of temporomandibular joint involvement in rheumatoid arthritis and psoriatic arthritis. Rheumatology. (2003) 42:673–6. doi: 10.1093/rheumatology/keg181
33. Wiell C, Szkudlarek M, Hasselquist M, Moller JM, Vestergaard A, Norregaard J, et al. Ultrasonography, magnetic resonance imaging, radiography, and clinical assessment of inflammatory and destructive changes in fingers and toes of patients with psoriatic arthritis. Arthritis Res Ther. (2007) 9:R119. doi: 10.1186/ar2327
34. Falsetti P, Frediani B, Fioravanti A, Acciai C, Baldi F, Filippou G, et al. Sonographic study of calcaneal entheses in erosive osteoarthritis, nodal osteoarthritis, rheumatoid arthritis and psoriatic arthritis. Scand J Rheumatol. (2003) 32:229–34. doi: 10.1080/03009740310003721
35. Falsetti P, Frediani B, Filippou G, Acciai C, Baldi F, Storri L, et al. Enthesitis of proximal insertion of the deltoid in the course of seronegative spondyloarthritis. an atypical enthesitis that can mime impingement syndrome. Scand J Rheumatol. (2002) 31:158–62. doi: 10.1080/713798352
36. Fournié B, Margarit-Coll N, Champetier de Ribes TL, Zabraniecki L, Jouan A, Vincent V, et al. Extrasynovial ultrasound abnormalities in the psoriatic finger. Prospective comparative power-doppler study versus rheumatoid arthritis. Joint Bone Spine. (2006) 73:527–31. doi: 10.1016/j.jbspin.2006.01.019
37. Zabotti A, Salvin S, Quartuccio L, De Vita S. Differentiation between early rheumatoid and early psoriatic arthritis by the ultrasonographic study of the synovio-entheseal complex of the small joints of the hands. Clin Exp Rheumatol. (2016) 34:459–65.
38. Turner DE, Hyslop E, Barn R, McInnes IB, Steultjens MPM, Woodburn J. Metatarsophalangeal joint pain in psoriatic arthritis: a cross-sectional study. Rheumatology. (2014) 53:737–40. doi: 10.1093/rheumatology/ket435
39. Woodburn J, Hyslop E, Barn R, McInnes IB, Turner DE. Achilles tendon biomechanics in psoriatic arthritis patients with ultrasound proven enthesitis. Scand J Rheumatol. (2013) 42:299–302. doi: 10.3109/03009742.2012.747626
40. Eder L, Jayakar J, Thavaneswaran A, Haddad A, Chandran V, Salonen D, et al. Is the madrid sonographic enthesitis index useful for differentiating psoriatic arthritis from psoriasis alone and healthy controls? J Rheumatol. (2014) 41:466–72. doi: 10.3899/jrheum.130949
41. Ciancio G, Volpinari S, Fotinidi M, Furini F, Farina I, Bortoluzzi A, et al. Involvement of the inconstant bursa of the fifth metatarsophalangeal joint in psoriatic arthritis: a clinical and ultrasonographic study. BioMed Res Int. (2014) 2014:174841 doi: 10.1155/2014/174841
42. Bandinelli F, Prignano F, Bonciani D, Bartoli F, Collaku L, Candelieri A, et al. Ultrasound detects occult entheseal involvement in early psoriatic arthritis independently of clinical features and psoriasis severity. Clin Exp Rheumatol. (2013) 31:219–24.
43. Aydin SZ, Castillo-Gallego C, Ash ZR, Abignano G, Marzo-Ortega H, Wittmann M, et al. Potential use of optical coherence tomography and high-frequency ultrasound for the assessment of nail disease in psoriasis and psoriatic arthritis. Dermatol Basel Switz. (2013) 227:46–51. doi: 10.1159/000351702
44. Zayat AS, Ellegaard K, Conaghan PG, Terslev L, Hensor EM, Freeston JE, et al. The specificity of ultrasound-detected bone erosions for rheumatoid arthritis. Ann Rheum Dis. (2015) 745:897–903. doi: 10.1136/annrheumdis-2013-204864
45. Freeston JE, Coates LC, Helliwell PS, Hensor EM, Wakefield RJ, Emery P, et al. Is there subclinical enthesitis in early psoriatic arthritis? A clinical comparison with power doppler ultrasound. Arthritis Care Res. (2012) 64:1617–21. doi: 10.1002/acr.21733
46. Marchesoni A, de Lucia O, Rotunno L, de Marco G, Manara M. Entheseal power doppler ultrasonography: a comparison of psoriatic arthritis and fibromyalgia. J Rheumatol. (2012) 39:29–31. doi: 10.3899/jrheum.120238
47. Acquacalda E, Albert C, Montaudie H, Fontas E, Danre A, Roux CH, et al. Ultrasound study of entheses in psoriasis patients with or without musculoskeletal symptoms: a prospective study. Joint Bone Spine. (2015) 82:267–71. doi: 10.1016/j.jbspin.2015.01.016
48. Falcao S, de Miguel E, Castillo-Gallego C, Peiteado D, Branco J, Martín Mola E. Achilles enthesis ultrasound: the importance of the bursa in spondyloarthritis. Clin Exp Rheumatol. (2013) 31:422–7.
49. Ezzat Y, Gaber W, Abd ELRSF, Ezzat M, El Sayed M. Ultrasonographic evaluation of lower limb enthesis in patients with early spondyloarthropathies. Egypt Rheumatol. (2013) 35:29–35. doi: 10.1016/j.ejr.2012.09.004
50. Aydin SZ, Ash ZR, Tinazzi I, Castillo-Gallego C, Kwok C, Wilson C, et al. The link between enthesitis and arthritis in psoriatic arthritis: a switch to a vascular phenotype at insertions may play a role in arthritis development. Ann Rheum Dis. (2013) 72:992–5. doi: 10.1136/annrheumdis-2012-201617
51. Farouk HM, Mostafa AAA, Youssef SS, Elbeblawy MMS, Assaf NY, Elokda ESE. Value of entheseal ultrasonography and serum cartilage oligomeric matrix protein in the preclinical diagnosis of psoriatic arthritis. Clin Med Insights Arthritis Musculoskelet Disord. (2010) 3:7–14. doi: 10.4137/CMAMD.S4461
52. Groves C, Chandramohan M, Chew NS, Aslam T, Helliwell PS. Clinical examination, ultrasound and MRI imaging of the painful elbow in psoriatic arthritis and rheumatoid arthritis: which is better, ultrasound or MR, for imaging enthesitis? Rheumatol Ther. (2017) 4:71–84. doi: 10.1007/s40744-017-0053-7
53. De Simone C, Caldarola G, D'Agostino M, Carbone A, Guerriero C, Bonomo L, et al. Usefulness of ultrasound imaging in detecting psoriatic arthritis of fingers and toes in patients with psoriasis. Clin Dev Immunol. (2011) 2011:390726. doi: 10.1155/2011/390726
54. Aydin SZ, Castillo-Gallego C, Ash ZR, Marzo-Ortega H, Emery P, Wakefield RJ, et al. Ultrasonographic assessment of nail in psoriatic disease shows a link between onychopathy and distal interphalangeal joint extensor tendon enthesopathy. Dermatology. (2012) 225:231–5. doi: 10.1159/000343607
55. Mendonça JA. [Differences of spectral doppler in psoriatic arthritis and onychomycosis]. Rev Bras Reumatol. (2014) 54:490–3. doi: 10.1016/j.rbre.2014.03.028
56. Ruta S, Rosa J, Navarta DA, Saucedo C, Catoggio LJ, Monaco RG, et al. Ultrasound assessment of new onset bilateral painful shoulder in patients with polymyalgia rheumatica and rheumatoid arthritis. Clin Rheumatol. (2012) 31:1383–7. doi: 10.1007/s10067-012-2016-2
57. Cantini F, Salvarani C, Olivieri I, Niccoli L, Padula A, Macchioni L, et al. Shoulder ultrasonography in the diagnosis of polymyalgia rheumatica: a case-control study. J Rheumatol. (2001) 28:1049–55.
58. Cantini F, Niccoli L, Nannini C, Padula A, Olivieri I, Boiardi L, et al. Inflammatory changes of hip synovial structures in polymyalgia rheumatica. Clin Exp Rheumatol. (2005) 23:462–8.
59. Coari G, Paoletti F, Iagnocco A. Shoulder involvement in rheumatic diseases. sonographic findings. J Rheumatol. (1999) 26:668–73.
60. Lange U, Piegsa M, Teichmann J, Neeck G. Ultrasonography of the glenohumeral joints–a helpful instrument in differentiation in elderly onset rheumatoid arthritis and polymyalgia rheumatica. Rheumatol Int. (2000) 19:185–9. doi: 10.1007/s002960000051
61. Catay E, Ruta S, Rosa J, Navarta DA, Scolnik M, Garcia-Monaco R, et al. Knee effusion: Sensitivity and specificity of ultrasound for the identification of calcium pyrophosphate crystals. Arthritis Rheum. (2013) 65:S367.
62. Juge PA, Ottaviani S, Aubrun A, Palazzo E, Dieudé P. Sensitivity and reproducibility of ultrasonography in calcium pyrophosphate crystal deposition: a case-control study. Ann Rheum Dis. (2014) 73:492–509. doi: 10.1136/annrheumdis-2014-eular.3849
63. Ottaviani S, Juge PA, Aubrun A, Palazzo E, Dieudé P. Sensitivity and reproducibility of ultrasonography in calcium pyrophosphate crystal deposition in knee cartilage: a cross-sectional study. J Rheumatol. (2015) 42:1511–3. doi: 10.3899/jrheum.141067
64. Salcion A, Kozyreff-Meurice M, Richette P, Avenel G, Bisson-Vaivre A, Trouvin A.-P. Assessment of the ultrasonography's efficiency as a diagnostic tool for calcium pyrophosphate crystal deposition disease. Ann Rheum Dis. (2015) 74:538. doi: 10.1136/annrheumdis-2015-eular.4964
65. Adinolfi A, Picerno V, Scanu A, Toscano C, Scirè C, Carrara G, et al. Diagnostic performance of the new omeract criteria for CPPD identification by us: correlation with synovial fluid analysis. Ann Rheum Dis. (2017) 2017:730–1. doi: 10.1136/annrheumdis-2017-eular.5164
66. Filippou G, Frediani B, Gallo A, Menza L, Falsetti P, Baldi F, et al. A ‘new' technique for the diagnosis of chondrocalcinosis of the knee: sensitivity and specificity of high-frequency ultrasonography. Ann Rheum Dis. (2007) 66:1126–8. doi: 10.1136/ard.2007.069344
67. Ellabban AS, Kamel SR, Abo Omar HAS, El-Sherif AMH, Abdel-Magied RA. Ultrasonographic diagnosis of articular chondrocalcinosis. Rheumatol Int. (2012) 32:3863–8. doi: 10.1007/s00296-011-2320-1
68. Filippou G, Bozios P, Gambera D, Lorenzini S, Bertoldi I, Adinolfi A, et al. Ultrasound detection of calcium pyrophosphate dihydrate crystal deposits in menisci: a pilot in vivo and ex vivo study. Ann Rheum Dis. (2012) 71:1426–7. doi: 10.1136/annrheumdis-2011-201001
69. Forien M, Combier A, Gardette A, Palazzo E, Dieudé P, Ottaviani S. Comparison of ultrasonography and radiography of the wrist for diagnosis of calcium pyrophosphate deposition. Joint Bone Spine. (2018) 85:615–8. doi: 10.1016/j.jbspin.2017.09.006
70. Di Matteo A, Filippucci E, Salaffi F, Carotti M, Carboni D, Di Donato E, et al. Diagnostic accuracy of musculoskeletal ultrasound and conventional radiography in the assessment of the wrist triangular fibrocartilage complex in patients with definite diagnosis of calcium pyrophosphate dihydrate deposition disease. Clin Exp Rheumatol. (2017) 35:647–52.
71. Contant E, Ornetti P, Bohm A, Fortunet C, Maillefert JF. Interest of musculoskeletal ultrasound in the diagnosis of calcium pyrophosphate dihydrate deposition disease. Ann Rheum Dis. (2014) 73:775 doi: 10.1136/annrheumdis-2014-eular.3533
72. Lai KL, Chiu YM. Role of ultrasonography in diagnosing gouty arthritis. J Med Ultrasound. (2011) 19:7–13. doi: 10.1016/j.jmu.2011.01.003
73. Huppertz A, Hermann KGA, Diekhoff T, Wagner M, Hamm B, Schmidt WA. Systemic staging for urate crystal deposits with dual-energy CT and ultrasound in patients with suspected gout. Rheumatol Int. (2014) 34:763–71. doi: 10.1007/s00296-014-2979-1
74. Elsaman AM, Muhammad EMS, Pessler F. Sonographic findings in gouty arthritis: diagnostic value and association with disease duration. Ultrasound Med Biol. (2016) 42:1330–6. doi: 10.1016/j.ultrasmedbio.2016.01.014
75. Basaric MM, Radunovic G, Damjanov N, Perovic-Radak M. Sensitivity and specificity of ultrasound score for the diagnosis of gout. Ann Rheum Dis. (2016) 75:863–4. doi: 10.1136/annrheumdis-2016-eular.3750
76. Gruber M, Bodner G, Rath E, Supp G, Weber M, Schueller-Weidekamm C. Dual-energy computed tomography compared with ultrasound in the diagnosis of gout. Rheumatol. (2014) 53:173–9. doi: 10.1093/rheumatology/ket341
77. Pascal Z, Valcov R, Fabreguet I, Dumusc A, Omoumi P, So A. A prospective evaluation of ultrasound as a diagnostic tool in acute microcrystalline arthritis. Arthritis Res Ther. (2015) 17:188 doi: 10.1186/s13075-015-0701-7
78. Iagnocco A, Filippucci E, Ossandon A, Ciapetti A, Salaffi F, Basili S, et al. High resolution ultrasonography in detection of bone erosions in patients with hand osteoarthritis. J Rheumatol. (2005) 32:2381–3.
79. Keen HI, Lavie F, Wakefield RJ, D'Agostino MA, Berner Hammer H, Hensor EMA, et al. The development of a preliminary ultrasonographic scoring system for features of hand osteoarthritis. Ann Rheum Dis. (2008) 67:651–5. doi: 10.1136/ard.2007.077081
80. Koutroumpas AC, Alexiou IS, Vlychou M, Sakkas LI. Comparison between clinical and ultrasonographic assessment in patients with erosive osteoarthritis of the hands. Clin Rheumatol. (2010) 29:511–6. doi: 10.1007/s10067-009-1348-z
81. Hammer HB, Mathiessen A, Iagnocco A, Filippucci E, Gandjbakhch F, Kortekaas MC, et al. High reliability was found for ultrasound scoring of osteophytes in patients with hand osteoarthritis using an atlas as reference; an omeract initiative. Arthritis Rheum. (2013) 65:S728–9.
82. Vlychou M, Koutroumpas A, Malizos K, Sakkas LI. Ultrasonographic evidence of inflammation is frequent in hands of patients with erosive osteoarthritis. Osteoarthr Cartil. (2009) 17:1283–7. doi: 10.1016/j.joca.2009.04.020
83. Vlychou M, Koutroumpas A, Alexiou I, Fezoulidis I, Sakkas LI. High-resolution ultrasonography and 3.0 T magnetic resonance imaging in erosive and nodal hand osteoarthritis: high frequency of erosions in nodal osteoarthritis. Clin Rheumatol. (2013) 32:755–62. doi: 10.1007/s10067-013-2166-x
84. Wittoek R, Carron P, Verbruggen G. Structural and inflammatory sonographic findings in erosive and non-erosive osteoarthritis of the interphalangeal finger joints. Ann Rheum Dis. (2010) 69:2173–6. doi: 10.1136/ard.2010.128504
85. Wittoek R, Jans L, Lambrecht V, Carron P, Verstraete K, Verbruggen G. Reliability and construct validity of ultrasonography of soft tissue and destructive changes in erosive osteoarthritis of the interphalangeal finger joints: a comparison with MRI. Ann Rheum Dis. (2011) 70:278–83. doi: 10.1136/ard.2010.134932
86. Iagnocco A, Coari G. Usefulness of high resolution US in the evaluation of effusion in osteoarthritic first carpometacarpal joint. Scand J Rheumatol. (2000) 29:170–3. doi: 10.1080/030097400750002049
87. Akgul O, Guldeste Z, Ozgocmen S. The reliability of the clinical examination for detecting Baker's cyst in asymptomatic fossa. Int J Rheum Dis. (2014) 17:204–9. doi: 10.1111/1756-185X.12095
88. Chatzopoulos D, Moralidis E, Markou P, Makris V, Arsos G. Baker's cysts in knees with chronic osteoarthritic pain: a clinical, ultrasonographic, radiographic and scintigraphic evaluation. Rheumatol Int. (2008) 29:141–6. doi: 10.1007/s00296-008-0639-z
89. Eşen S, Akarirmak U, Aydin FY, Unalan H. Clinical evaluation during the acute exacerbation of knee osteoarthritis: the impact of diagnostic ultrasonography. Rheumatol Int. (2013) 33:711–7. doi: 10.1007/s00296-012-2441-1
90. Ike RW, Somers EC, Arnold EL, Arnold WJ. Ultrasound of the knee during voluntary quadriceps contraction: a technique for detecting otherwise occult effusions. Arthritis Care Res. (2010) 62:725–9. doi: 10.1002/acr.20047
91. Pendleton A, Millar A, O'Kane D, Wright GD, Taggart AJ. Can sonography be used to predict the response to intra-articular corticosteroid injection in primary osteoarthritis of the knee? Scand J Rheumatol. (2008) 37:395–7. doi: 10.1080/03009740802050738
92. Song IH, Althoff CE, Hermann KG, Scheel AK, Knetsch T, Burmester GR, et al. Contrast-enhanced ultrasound in monitoring the efficacy of a bradykinin receptor 2 antagonist in painful knee osteoarthritis compared with MRI. Ann Rheum Dis. (2009) 68:75–83. doi: 10.1136/ard.2007.080382
93. Yoon CH, Kim HS, Ju JH, Jee WH, Park SH, Kim HY. Validity of the sonographic longitudinal sagittal image for assessment of the cartilage thickness in the knee osteoarthritis. Clin Rheumatol. (2008) 27:1507–16. doi: 10.1007/s10067-008-0956-3
94. Okano T, Filippucci E, Carlo M. D., Draghessi A, Carotti M, Salaffi F, et al. Ultrasonographic evaluation of joint damage in knee osteoarthritis: Feature-specific comparisons with conventional radiography. Rheumatol UK. (2016) 55:2040–9. doi: 10.1093/rheumatology/kew304
95. Camerer M, Ehrenstein B, Hoffstetter P, Fleck M, Hartung W. High-resolution ultrasound of the midfoot: sonography is more sensitive than conventional radiography in detection of osteophytes and erosions in inflammatory and non-inflammatory joint disease. Clin Rheumatol. (2017) 36:2145–9. doi: 10.1007/s10067-017-3658-x
96. Mortada M, Zeid A, Abd El-Hamid Al-Toukhy M, Ezzeldin N, Elgawish M. Reliability of a proposed ultrasonographic grading scale for severity of primary knee osteoarthritis. Clin Med Insights Arthritis Musculoskelet Disord. (2016) 9:161–6. doi: 10.4137/CMAMD.S38141
97. Ellabban AS, Kamel SR, Omar HASA, El-Sherif AMH, Abdel-Magied RA. Ultrasonographic findings of Achilles tendon and plantar fascia in patients with calcium pyrophosphate deposition disease. Clin Rheumatol. (2012) 31:697–704. doi: 10.1007/s10067-011-1911-2
98. Ottaviani S. Ultrasonography in crystal-related diseases. Rev Rhum Monogr. (2015) 82:181–6. doi: 10.1016/j.monrhu.2015.04.005
99. Foldes K. Knee chondrocalcinosis: an ultrasonographic study of the hyalin cartilage. Clin Imaging. (2002) 26:194–6. doi: 10.1016/S0899-7071(01)00385-0
100. Falsetti P, Frediani B, Acciai C, Baldi F, Filippou G, Prada EP, et al. Ultrasonographic study of achilles tendon and plantar fascia in chondrocalcinosis. J Rheumatol. (2004) 31:2242–50.
101. Filippucci E, Gutierrez Riveros M, Georgescu D, Salaffi F, Grassi W. Hyaline cartilage involvement in patients with gout and calcium pyrophosphate deposition disease. An ultrasound study. Osteoarthritis Cartilage. (2009) 17:178–81. doi: 10.1016/j.joca.2008.06.003
102. Barskova VG, Kudaeva FM, Bozhieva LA, Smirnov AV, Volkov AV, Nasonov EL. Comparison of three imaging techniques in diagnosis of chondrocalcinosis of the knees in calcium pyrophosphate deposition disease. Rheumatology. (2013) 52:1090–4. doi: 10.1093/rheumatology/kes433
103. Gutierrez M, Di Geso L, Salaffi F, Carotti M, Girolimetti R, de Angelis R, et al. Ultrasound detection of cartilage calcification at knee level in calcium pyrophosphate deposition disease. Arthritis Care Res. (2014) 66:69–73. doi: 10.1002/acr.22190
104. Filippou G, Adinolfi A, Lorenzini S, Bertoldi I, Di Sabatino V, Picerno V, et al. Ultrasound versus X-rays versus synovial fluid analysis for the diagnosis of calcium pyrophosphate dihydrate deposition disease: Is it CPPD? Arthritis Rheumatol. (2014) 66:S77–8.
105. de Miguel E, Puig JG, Castillo C, Peiteado D, Torres RJ, Martín-Mola E. Diagnosis of gout in patients with asymptomatic hyperuricaemia: a pilot ultrasound study. Ann Rheum Dis. (2012) 71:157–8. doi: 10.1136/ard.2011.154997
106. Rettenbacher T, Ennemoser S, Weirich H, Ulmer H, Hartig F, Klotz W, et al. Diagnostic imaging of gout: comparison of high-resolution US versus conventional X-ray. Eur Radiol. (2008) 18:621–30. doi: 10.1007/s00330-007-0802-z
107. Naredo E, Uson J, Jiménez-Palop M, Martínez A, Vicente E, Brito E, et al. Ultrasound-detected musculoskeletal urate crystal deposition: which joints and what findings should be assessed for diagnosing gout? Ann Rheum Dis. (2014) 73:1522–8. doi: 10.1136/annrheumdis-2013-203487
108. Lamers-Karnebeek FBG, van Riel PLCM, Jansen TL. Additive value for ultrasonographic signal in a screening algorithm for patients presenting with acute mono-/oligoarthritis in whom gout is suspected. Clin Rheumatol. (2014) 33:555–9. doi: 10.1007/s10067-014-2505-6
109. Pattamapaspong N, Vuthiwong W, Kanthawang T, Louthrenoo W. Value of ultrasonography in the diagnosis of gout in patients presenting with acute arthritis. Skeletal Radiol. (2017) 46:759–67. doi: 10.1007/s00256-017-2611-z
Keywords: early arthritis, ultrasonography, diagnosis, systematic review, imaging
Citation: Sakellariou G, Scirè CA, Adinolfi A, Batticciotto A, Bortoluzzi A, Delle Sedie A, De Lucia O, Dejaco C, Epis OM, Filippucci E, Idolazzi L, Picchianti Diamanti A, Zabotti A, Iagnocco A, Filippou G and on behalf of the Musculoskeletal Ultrasound Study Group of the Italian Society of Rheumatology (2020) Differential Diagnosis of Inflammatory Arthropathies by Musculoskeletal Ultrasonography: A Systematic Literature Review. Front. Med. 7:141. doi: 10.3389/fmed.2020.00141
Received: 22 January 2020; Accepted: 31 March 2020;
Published: 07 May 2020.
Edited by:
Helena Canhao, New University of Lisbon, PortugalReviewed by:
Konstantinos Triantafyllias, ACURA Rheumatology Clinic, GermanyCopyright © 2020 Sakellariou, Scirè, Adinolfi, Batticciotto, Bortoluzzi, Delle Sedie, De Lucia, Dejaco, Epis, Filippucci, Idolazzi, Picchianti Diamanti, Zabotti, Iagnocco and Filippou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlo Alberto Sciré, Yy5zY2lyZUByZXVtYXRvbG9naWEuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.