
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Med., 10 July 2019
Sec. Regulatory Science
Volume 6 - 2019 | https://doi.org/10.3389/fmed.2019.00157
 Tania Bubela1*
Tania Bubela1* Erika Kleiderman2
Erika Kleiderman2 Zubin Master3,4
Zubin Master3,4 Ubaka Ogbogu5
Ubaka Ogbogu5 Vardit Ravitsky6
Vardit Ravitsky6 Amy Zarzeczny7
Amy Zarzeczny7 Bartha Maria Knoppers2
Bartha Maria Knoppers2Canada's Assisted Human Reproduction Act is long overdue for Parliamentary review. We argue that the current regulation of research using human reproductive materials is not proportionate, not responsive to the uncertain threats posed to human and environmental health and safety, and is not considerate of diverse values in a democratic society. We propose tailored regulatory carve-outs for in vitro research for currently prohibited activities, such as gene editing, and for the exercise of Ministerial Discretion for access by Canadians to experimental in vivo interventions that are currently prohibited, such as mitochondrial replacement therapy. Our recommendations are bounded by constitutional constraints that recognize political and practical challenges in keeping oversight of this research under Federal jurisdiction, whether conducted in academic or private sectors. The proposed nuanced regulatory scheme should be overseen by a new national Agency, modeled on a blend of the Canadian Stem Cell Oversight Committee and Assisted Human Reproduction Canada.
Robust regulation of novel health biotechnologies in morally contentious domains is central to the ethical conduct of research and clinical applications. Such regulation ought to be proportionate, responsive to the uncertain threats posed to human and environmental health and safety, and considerate of diverse values in a democratic society. Proportionality implies an evidence-informed weighing of the risks and benefits, which in the domain of assisted reproductive technologies (ARTs), may bring communities into conflict. Responsiveness implies that a regulatory scheme should not be static, instead employing principled mechanisms to respond to emerging evidence of benefits, threats, and evolving societal values. Uncertainty is addressed over time through the development of an evidence-base on which regulatory frameworks are premised; the evidence base fits the benefit-harm-uncertainty profile of the assets or products the frameworks are designed to oversee.
ARTs raise rights-related questions with human dignity at their core. How should a regulatory scheme balance the respective rights and considerations outlined in the preamble of the 2004 Assisted Human Reproduction Act (AHRA) (1)? These include the interests of researchers and clinicians to advance health/medical innovation, the rights of patients to equitable access to health interventions that have proven to be safe and effective, the rights of women and children to be protected from exploitative practices, as well as consideration of religious freedoms and the “integrity of the human genome.” The question of a balanced regulatory scheme was central to discussions at a multi-stakeholder workshop, convened in Ottawa on December 11, 2018 to deliberate on the Consensus Statement: Gene Editing, Genetic Testing, and Reproductive Medicine in Canada (2). The Consensus Statement derived from a consultation process, supported by the Stem Cell Network, on activities that are currently prohibited by the AHRA (3–6).
The aim of the workshop was to inform proportionate and responsive regulation of research using human reproductive materials and clinical application of ARTs. Workshop participants included 20 experts in law, ethics, science, and reproductive medicine, as well as five representatives and observers from departments and agencies of the Canadian government. Workshop discussions focused on reforms to the AHRA and nuanced regulatory mechanisms that could distinguish between in vitro pre-clinical research, clinical research and clinical practice. Here, we make pragmatic recommendations to address the regulation of ARTs, within the constraints of Canada's legal and political framework. Our discussion focuses on pre-clinical research and access by Canadians to ARTs that are currently prohibited by law and accompanied by penal and monetary sanctions. Our discussion does not consider reimbursement of ARTs by Provincial governments or private payers.
In enacting the AHRA, the Government of Canada employed its criminal law power to prohibit some areas of research and clinical practice that raised societal concerns in the 1990s and early 2000s. This use of the criminal law power was necessitated by peculiarities in Canada's constitutional division of legislative powers between Federal and Provincial governments. The division of powers constrains options for a regulatory environment that is nationally consistent and covers both academic and private-sector actors. Criminal law is within the legislative purview of the Federal Government, while regulation of research, health care delivery, and regulation of medical professionals generally falls within the ambit of Provincial law-making. For pragmatic reasons, therefore, the issue may not be the use of the criminal law power per se, but the lack of an attendant regulatory scheme tailored to research and clinical developments in ARTs. Indeed, the current list of specific prohibitions bans promising avenues of research, while simultaneously allowing some ARTs to escape a similar level of scrutiny, such as pre-implantation genetic diagnosis.
The original intent of the criminal prohibitions contained in the AHRA may have been consistent with accepted norms at the time of its enactment, concerns about safety, and a commitment to striking the right balance between promoting science and a precautionary approach to potential risks. However, these controls need to be supplemented by a regulatory scheme that is nuanced and responsive to current and future developments. This is not to say that the prohibitions are or were immoral or unethical, or that lifting prohibitions on some activities while regulating others would be tantamount to dismissing legitimate concerns. Rather, a move to revisit the prohibitions is consistent with a proportionate, responsive, and considerate approach to regulating science and technologies. It will bring necessary clarity to promising areas of research that have become legally ambiguous in light of emerging techniques. It will provide the public(s) with an assurance that the safety and ethical issues are being seriously attended to within a responsive oversight regime, while providing greater clarity for pre-clinical and clinical researchers, research sponsors, and others with an interest in research outcomes.
That “hard cases make bad law” is a truism. The recent controversy over human germline gene editing in China, therefore, formed a backdrop to the final workshop discussions. In November 2018, Dr. Jiankui He, a biophysicist at the Southern University of Science and Technology in Shenzhen, announced the birth of twin girls whose embryonic genomes he had edited using CRISPR/Cas9 to confer resistance to HIV by removing the CCR5 gene (7). The claim has since been confirmed; the independently wealthy Dr. He had funded the research himself and allegedly side-stepped ethics oversight at his institution (8). At the time of writing, He is under investigation and house arrest, facing allegations of corruption, bribery and contravening research guidelines that ban genetically modified embryos from being implanted into a human in China (9). These research guidelines are enforceable and any violations can lead to penalties and sanctions (10, 11). The global scientific community has condemned Dr. He's actions, and he has been fired by his research institution (12, 13). Given that He faces both monetary penalties and a prison term, it is unlikely that greater criminal sanctions will deter rogue actors (14). While some have called for a moratorium on germline gene editing, in other circles this event has sparked a broader debate on proportionate regulation that enables responsible progress in this field, based on transparency and robust pre-clinical research and a focus on clear medical need (15–17). In response, the Chinese government has issued new draft regulations that would tighten oversight for “high-risk biomedical technologies,” which includes gene editing (18). Canadian regulatory reform discussions should take notice of this event, but not be overly influenced by it (19).
Elsewhere, the authors have argued for a distributed governance model for ARTs and research involving human embryos and reproductive material that engages Federal and Provincial ethics oversight, informed by the 2014 Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (TCPS2) (20), and provincial professional regulation (5). While replacing the AHRA with a new legal framework might be the preferred long-term approach to addressing current issues, we recognize the associated political and practical challenges. Therefore, the consensus of the present workshop was to outline what may be a more feasible way forward in the short term. We focused our discussion on reforms to the AHRA concomitant with the development of regulations and a regulatory agency that would enable unified Federal oversight of research, whether conducted in academic or private sectors. This latter point is significant, because the nationally harmonizing effect of the TCPS2 over ethical conduct of research involving human reproductive materials is limited to institutions that are eligible to receive Tri-Council research funding. Private sector entities, therefore, unless they collaborate with Tri-Council eligible institutions or voluntarily adopt the Policy, do not necessarily fall under the auspices of the TCPS2.
Our focus is on proposing tailored regulatory carve-outs for in vitro research for currently prohibited activities and for the exercise of Ministerial Discretion by the Minister of Health for access by Canadians to experimental in vivo interventions that are currently prohibited under the AHRA [e.g., mitochondrial replacement therapy (MRT)] (4, 21). The latter recommendation is a short-term compromise while researchers determine whether such interventions are safe and effective; thereby demonstrating that a criminal ban is no longer justified, unless social consensus still considers such an intervention as morally reprehensible. Many have argued that such social consensus does not presently exist for many ARTs, even if it may have existed in the period leading up to the enactment of the AHRA (22, 23). Justifying our recommendations requires a foray into the checkered history of the AHRA, as well as Canadian constitutional and administrative law.
The AHRA is long overdue for its Parliamentary Review, mandated within 3 years of the establishment of the Assisted Human Reproduction Agency (the Agency) that was slated to oversee the operations of the AHRA (s. 741–745) (1). The Agency was created shortly after the AHRA came into force. However, it was disbanded shortly thereafter when the Supreme Court of Canada (SCC), in a divided decision with three sets of reasons, struck down most of the provisions of the AHRA after a constitutional challenge over legislative jurisdiction from the Province of Quebec (24). The impugned provisions included those that regulated ARTs in fertility clinics; most of these controlled activities were found to be an unconstitutional incursion into Provincial jurisdiction over health services. However, a majority of justices upheld sections 8, 9, and 12 that regulated surrogacy and donation of human reproductive material as a valid exercise of criminal law. Health Canada has recently held a consultation on regulatory reforms to aspects of these provisions, including the safety of sperm and ova, reimbursement to women for activities associated with surrogacy, and related administration and enforcement (25). This signals the willingness of Health Canada to open regulatory discussions after the only known criminal charges were brought against the operator of a fertility service and her company for remunerating surrogacy and egg donation. The accused plead guilty, so there were no written reasons to clarify the scope of payments allowable for these services (26).
Not challenged as being within Federal jurisdiction were the criminal prohibitions in sections 5–7. Section 5 details prohibited research and clinical activities, including human cloning, creation of embryos for research purposes, human embryonic research beyond 14 days of development, sex selection for non-medical reasons, human genome alterations capable of being transmitted to future generations, transplantation of non-human reproductive material into a human and vice versa, creation of chimera, and creation of human-non-human hybrids for the purposes of reproduction or transplantation into a human. Section 6 prohibits some activities related to surrogacy and section 7 prohibits the purchase and sale of reproductive material and its use without appropriate consent.
We focus our discussion on the prohibitions in section 5 that were not challenged and whose constitutional validity on jurisdictional grounds is therefore presumed based on tangential consideration by the SCC justices, known as obiter. To our knowledge, no legal action has ever been taken to enforce the s. 5 prohibitions. Of particular interest is the judicial reasoning on the scope and relevance of the criminal law in this context. Valid criminal law takes the form of a prohibition backed by a penalty for a legitimate criminal law purpose, including “[p]ublic peace, order, security, health, morality” (p. 50) (27). In considering the legitimacy of the section 5 prohibitions, the three sets of judgments refer to “conduct that is reprehensible” (para. 26) and “reflecting pressing moral concerns” (para. 79) (24). Indeed, “the dominant effect of the prohibitory and administrative provisions is to create a regime that will prevent or punish practices that may offend moral values, give rise to serious public health problems, and threaten the security of donors, donees, and persons not yet born” (para. 32) (24).
On the subject of morality, the Chief Justice stated:
[a]ssisted reproduction raises weighty moral concerns. The creation of human life and the processes by which it is altered and extinguished, as well as the impact this may have on affected parties, lie at the heart of morality. Parliament has a strong interest in ensuring that basic moral standards govern the creation and destruction of life, as well as their impact on persons like donors and mothers. Taken as a whole, the Act seeks to avert serious damage to the fabric of our society by prohibiting practices that tend to devalue human life and degrade participants. This is a valid criminal law purpose, grounded in issues that our society considers to be of fundamental importance (para. 61) (24).
It is not necessary for there to be societal consensus on the morality of specific acts. Rather, “[p]arliament need only have a reasonable basis to expect that its legislation will address a moral concern of fundamental importance, even if hard evidence is unavailable on some points because ‘the jury is still out”' (para. 50) (24).
The AHRA Reference decision suggests that the remaining statutory prohibitions are valid and likely to survive a challenge on jurisdictional grounds. However, the decision also suggests that valid criminal law is capable of supporting a nuanced regulatory scheme that permits “flexibility,” which is “vital in a field of evolving technologies.” Regulations are simpler to reform and therefore more nimble statutory instruments than Acts, which are subject to full Parliamentary review of proposed reforms. Most Acts are operationalized through regulations, which though comprising hard law in the form of subordinate legislation, are made or enacted by the responsible Minister rather than Parliament. Indeed, Health Canada derives its power to regulate drugs, medical devices, and clinical research from the criminal law and protection of public safety (28, 29). For example, the prohibition of the sale of drugs states that “[n]o person shall sell any drug that (a) was manufactured, prepared, preserved, packaged, or stored under unsanitary conditions; or (b) is adulterated” (s. 8) (30). Its comprehensive approach to regulation is done under the umbrella of the Food and Drugs Act (30) and subordinate regulations, such as the Food and Drugs Regulations (31), Cannabis Regulations (32), Medical Devices Regulations (33), Processing and Distribution of Semen for Assisted Conception Regulations (34), Safety of Human Cells, Tissues, and Organs for Transplantation Regulations (35), and Blood Regulations (36). These statutory instruments collectively set out a fulsome regulatory scheme that permits some activities, while imposing penalties for non-compliance.
In numerous arenas, therefore, we have working examples of nuanced regulatory schemes, backed by criminal law powers, capable of protecting public health and safety, without overly restricting health innovation. Working on the assumption that there is limited political will to repeal the AHRA, the consensus of the workshop was to recommend regulatory carve-outs to advance research in the domain of ARTs or using human reproductive materials, without compromising human health and safety. Such an approach has recently been taken, for example, to enable medical assistance in dying (MAiD) in Canada. MAiD had been subject to the criminal prohibition against counseling or aiding suicide and procuring consent to death. Enabling MAiD required amending the Criminal Code of Canada to allow a “carve-out” for patients who meet specified criteria to receive assistance with dying from physicians or nurse practitioners (s. 241) (37). The implementation of MAiD as a health service therefore falls to a distributed governance model between the Federal government and the Provinces under whose jurisdiction falls the delivery of health care through their health authorities as well as the regulation of health professionals through professional associations. A similar regulatory carve-out from criminal prohibitions existed for medicinal marijuana, prior to its legalization in Canada [s. 55(1)] (38). These examples represent the evolution of criminal law as societal values and views of what comprises reprehensible conduct shift over time.
What then would a regulatory carve-out under the statutory prohibitions of the AHRA include that reflects current knowledge and social values? In our view, in vitro pre-clinical research, currently prohibited under the AHRA should be permitted, subject to the 14-day rule for research involving human embryos (see Table 1). Such a regulatory carve-out would protect the safety and interests of Canadians, especially women, and allow Canadians the opportunity to benefit from advances in knowledge in the fields of genomic and regenerative medicine (77, 78). Enabling such research is in the interests of Canadians who carry known mutations for rare diseases, which may benefit from gene editing approaches; currently only pre-implantation genetic diagnosis of carrier embryos is available.
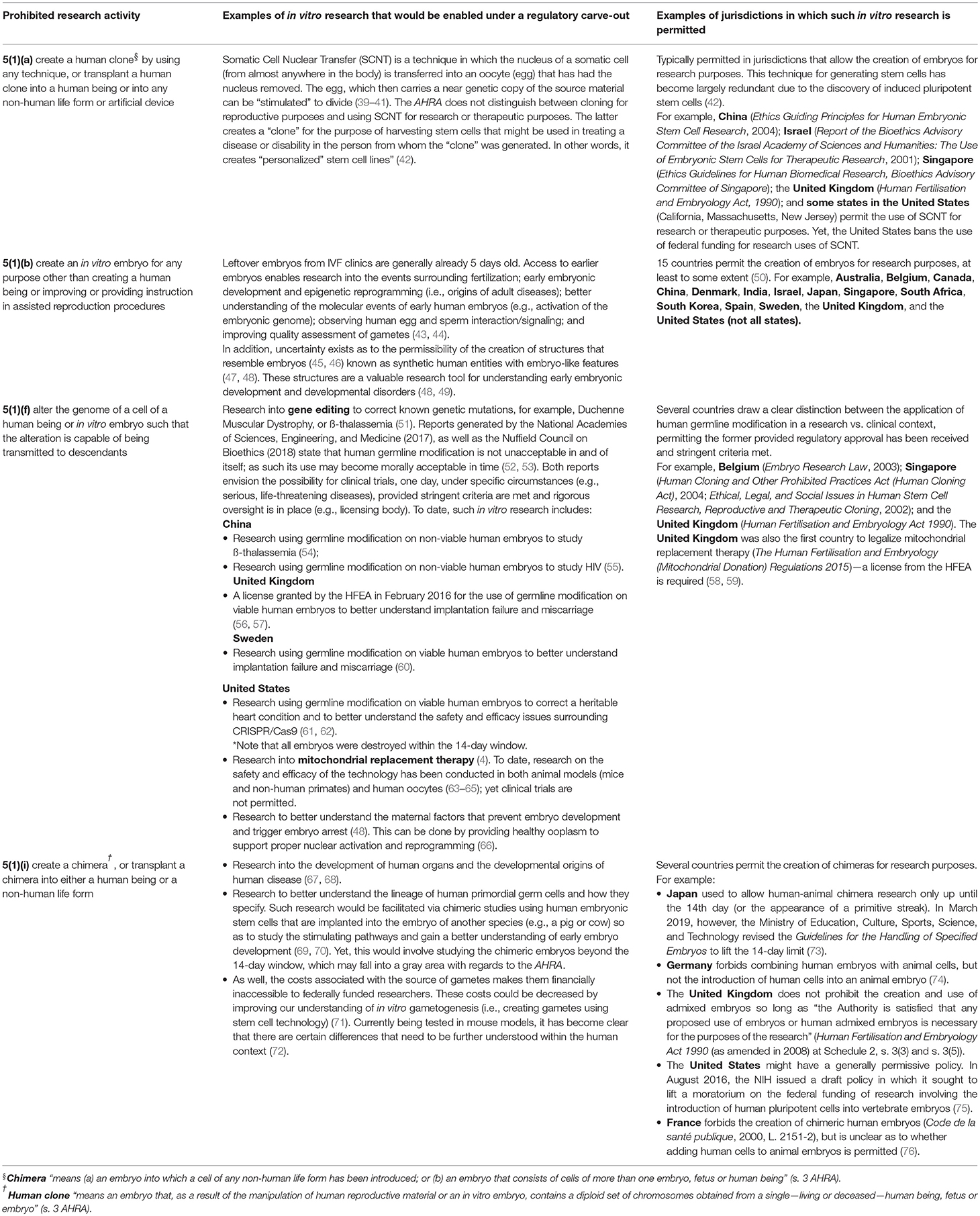
Table 1. Activities that would be enabled under a regulatory carve-out for in vitro research.
Under our proposal, ART research would be overseen by a regulatory agency, modeled on a blend of the national Stem Cell Oversight Committee (SCOC) and Assisted Human Reproduction Canada. Currently, the SCOC oversees research involving pluripotent stem cells, including human embryonic stem cells. The SCOC is administered within the Canadian Institutes of Health Research (CIHR) and oversees compliance of researchers who, by nature of their work affiliation, are required to comply with TCPS2 (5). The SCOC also oversees compliance with the AHRA, whose statutory prohibitions are reflected in TCPS2. For its part, Assisted Human Reproduction Canada was a federal regulatory agency (2006–2013) whose mandate was to “administer and enforce the [AHRA] and related regulations in order to protect and promote the health, safety, dignity and rights of Canadians who use or are born of assisted reproductive technologies” (p. 3) (79).
A new Agency with an expanded mandate under the AHRA and any new regulations would necessarily be charged with oversight of a broader range of research activities by all Canadian researchers, whether subject to TCPS2 or not (see Table 2). Even in its reduced form following the Constitutional challenge, the AHRA retains provisions for an oversight Agency, regulation making power, and general powers for administration and enforcement of the criminal prohibitions. Such an Agency could increase public confidence in its oversight through multi-stakeholder representation, including ethicists and members of the public. In this way, the Agency would follow best practices for citizen participation in regulation and deliberative process (81). An Agency with this mandate would be more likely to be constituted in the current climate, because of the issues at stake and greater confidence in the constitutionality of the remaining provisions of the AHRA.
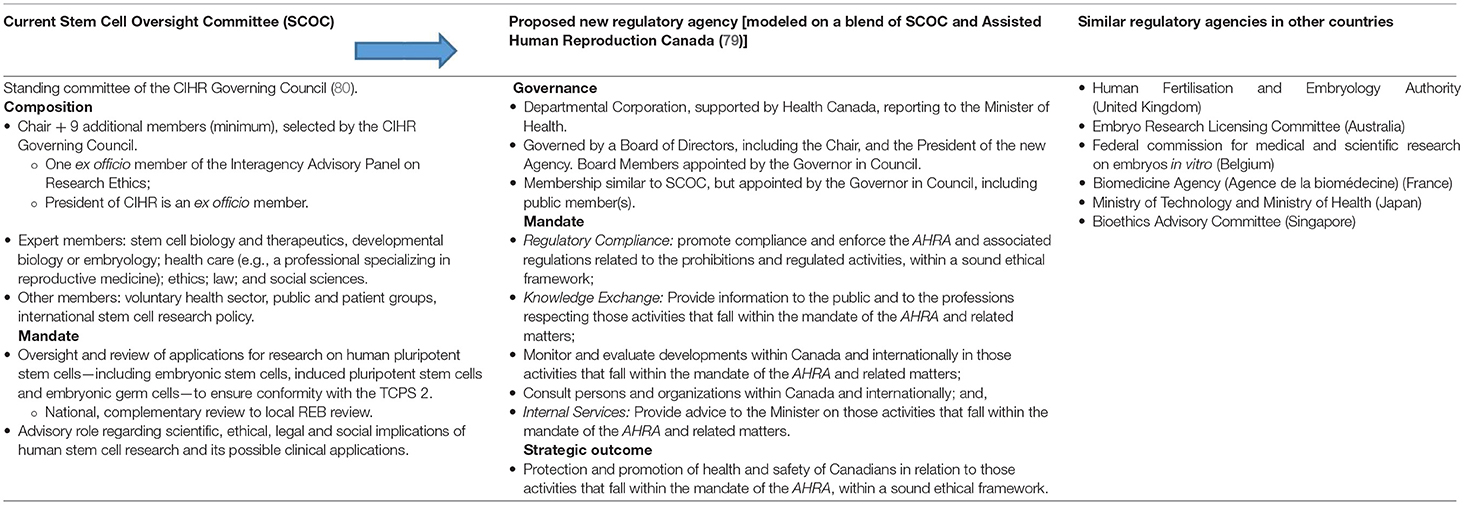
Table 2. Contours of a new regulatory agency to oversee research using ART.
While most of the research activities outlined in Table 1 are not yet ready for clinical application, diagnostic, and therapeutic interventions derived from such research will likely become available in the future. Some, such as MRT, have already been approved for clinical use in other countries, such as the United Kingdom (82). The United Kingdom's Human Fertilization and Embryology Authority (HFEA) has licensed one clinic and has approved the first application for the use of mitochondrial donation to treat patients (58). The clinic has been licensed to perform the technique but must still apply to the HFEA to treat individual patients (83). The latest statistics suggest that 15 babies have been born via MRT in five countries: Ukraine, United States (with MRT performed in Mexico), Israel, Sweden, and Greece (84, 85).
In the Canadian context, it is an open question whether prospective parents could be prosecuted under AHRA if they availed themselves of MRT in a country where the practice is permitted (21). This was the issue in the successful constitutional challenge of the prohibition on assisted suicide (86). The daughter of a Kay Carter, a woman with spinal stenosis, was concerned about being prosecuted upon her return to Canada after assisting her mother to end her life at the Dignitas clinic in Switzerland. She successfully argued, under section 7 of the Canadian Charter of Rights and Freedoms (87) that the prohibition was overly broad and therefore unjustifiably infringed her rights to life, liberty, and security of the person. This avenue of a Charter challenge is open to parents who wish to access MRT as well as to researchers, whose liberty is threatened by the penal sanctions in the AHRA. Indeed, the SCC in considering the constitutionality of the prohibited activities under jurisdictional grounds, left the door open to such a Charter challenge.
Accordingly, is there an available mechanism that might enable controlled access to currently experimental ARTs as their safety and efficacy profiles are ascertained? One option might be to enable a Ministerial Exemption on a case-by-case basis from the operation of the AHRA, following a transparent decision-making process and subject to judicial review. Such a scheme exists, for example, to exempt health practitioners, and other staff of supervised injection facilities from the operation of the Controlled Drugs and Substances Act (CDSA) (38). Section 56(1) of the CDSA. This section enables the Minister to exempt a person from any of the provisions of the CDSA “if, in the opinion of the Minister, the exemption is necessary for a medical or scientific purpose or is otherwise in the public interest.” The CDSA and Regulations then specify the conditions and processes for the exemption, and the Ministerial decision is subject to judicial review, which limits the risk that the decision will be unfair or arbitrary (88).
Recommendations for regulatory reform and ministerial discretion, however, are only practical if they can be implemented. The question is whether the regulatory approaches we have outlined are currently permitted under the AHRA. It could be argued that the general provision, under section 65(1) that “[t]he Governor in Council may make regulations for carrying into effect the purposes and provisions of this Act” is broad enough to create regulatory carve-outs for research purposes. However, the regulatory powers specified in this section refer to repealed sections, or sections other than the statutory prohibitions in section 5. Specifically, regulation-making authority currently rests with the Federal Cabinet (Governor in Council) and covers only the controlled aspects of the AHRA (section 8—“use of reproductive material without consent” and section 12—“reimbursement of expenditures”). The proposed regulatory carve-outs, would therefore, likely require amendments to the AHRA. The Criminal Code (37) similarly was amended to create the regulatory carve-outs for MAiD, including powers to make regulations. However, with broader regulation-making powers, the regulatory carve-out for medicinal marijuana from the CDSA was made under the Access to Cannabis for Medical Purposes Regulations (89), which did not require amendments to its Act.
However, while creating regulations may require a less onerous process than amending an Act, that distinction may be less pronounced with the AHRA. Under section 66, the AHRA takes the unusual step of requiring regulations made under section 65 to be laid before each House of Parliament by the Minister of Health. That process requires a review of the proposed regulation and a report on the findings to the House by the appropriate committee of each house, such as the Standing Committee on Health. These extra steps were required to enhance transparency and public confidence in the operation of the AHRA. Notably, there is no provision for ministerial discretion, which would require reforms to the AHRA itself.
In conclusion, the AHRA is long overdue for Parliamentary review and requires updates to reflect societal changes and scientific progress. Here, we have argued for a proportionate, responsive, and considerate regulatory regime for research using human reproductive materials that are currently prohibited in Canada. Our recommendations are bounded by constitutional constraints that recognize political and practical challenges in keeping oversight of this research under Federal jurisdiction, whether conducted in academic or private sectors. In our view, a nuanced regulatory scheme, overseen by a national Agency, could enable some currently prohibited in vitro research activities, while protecting the safety and interests of Canadians, especially women. Recommended reforms include a regulatory carve-out for some in vitro research activities and exercise of ministerial discretion for promising clinical research, for example, to enable MRT. In the absence of reform or a fulsome societal debate for Parliament to replace the AHRA with a more workable framework, the only recourse for researchers and patients who might benefit, will be through Charter challenges to the remaining provisions of the AHRA. That possible avenue was acknowledged by the SCC in the AHRA reference case (24), but such legal actions are fraught with difficulties and obstacles that researchers and/or patients are unlikely to undertake.
TB, EK, UO, VR, AZ, and BK contributed to the conception and design of the study. TB and EK wrote the first draft of the manuscript. All authors contributed to manuscript revision and acquisition of data, read, and approved the submitted version.
This project was funded by the Stem Cell Network (Impact Research Agreement Program – Public Policy Stream). Funding for TB came from Genome Canada, Genome Alberta, and Alberta Innovates (Government of Alberta) as part of the Precision Medicine Policy Network and the Alberta Precision Health Initiative Development Grant Program. Funding for BK came from the Canada Research Chair in Law and Medicine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to thank Dr. Andrea Jurisicova for her comments and valuable input. We would also like to acknowledge and thank the following workshop participants and observers: Jay Baltz (Ottawa Hospital Research Institute), Cecile Bensimon (Canadian Medical Association), Stanislav Birko (University of Montreal), Jaime Flamenbaum (CIHR Ethics Strategies), Amandeep Kahlon (Health Canada), Katelyn Landon (CIHR Ethics Strategies), Danielle Larouche (ThéCell/LOEX), Arthur Leader (University of Ottawa), Christopher McCabe (Institute of Health Economics), Caroline Mercer (Carlton University), Eric Meslin (Council of Canadian Academies), Jason Min (Canadian Fertility and Andrology Society), Cate Murray (Stem Cell Network), Forough Noohi (McGill University), Alan Peterson (McGill University), Michael Rudnicki (Stem Cell Network), Anu Shukla-Jones (Health Canada), and Susan Zimmerman (Secretariat on Responsible Conduct of Research).
2. Knoppers BM, Ogbogu U, Ravitsky V, Zarzeczny A, Isasi R, Bubela T, et al. Consensus Statement: Gene Editing, Genetic Testing and Reproductive Medicine in Canada. (2017). Available online at: https://stemcellnetwork.ca/wp-content/uploads/2018/02/Consensus-Statement_.pdf
3. Knoppers BM, Isasi R, Caulfield T, Kleiderman E, Bedford P, Illes J, et al. Human gene editing: revisiting Canadian policy. NPJ Regen Med. (2017) 2:3–4. doi: 10.1038/s41536-017-0007-2
4. Knoppers BM, Leader A, Hume S, Shoubridge EA, Isasi R, Noohi F, et al. Mitochondrial replacement therapy: the road to the clinic in Canada. J Obstet Gynaecol Can. (2017) 39:916–8. doi: 10.1016/j.jogc.2017.05.007
5. Ogbogu U, Zarzeczny A, Baltz J, Bedford P, Bijl J, Du J, et al. Research on human embryos and reproductive materials: revisiting Canadian law and policy. Healthc Policy. (2018) 13:10–9. doi: 10.12927/hcpol.2018.25401
6. Ravitsky V, Nguyen MT, Birko S, Kleiderman E, Laberge AM, Knoppers BM. Pre-implantation genetic diagnosis: the road forward in Canada. J Obstet Gynaecol Can. (2019) 41:68–71. doi: 10.1016/j.jogc.2018.08.001
7. Kolata G, Wee S-L, Belluck P. Chinese Scientist Claims to Use CRISPR to Make First Genetically Edited Babies. (2018). Available online at: https://www.nytimes.com/2018/11/26/health/gene-editing-babies-china.html
8. Krimsky S. Ten ways in which He Jiankui violated ethics. Nat Biotechnol. (2019) 37:19. doi: 10.1038/nbt.4337
9. Photopoulos J. Controversial Genome-Editing Scientist Dr. He is Alive and Under Guard. (2019). Available online at: https://www.bionews.org.uk/page_140730
10. Zhang D, Lie RK. Ethical issues in human germline gene editing: a perspective from China. Monash Bioeth Rev. (2018) 36:23–35. doi: 10.1007/s40592-018-0091-0
11. Kleiderman E, Ogbogu U. Realigning gene editing with clinical research ethics: what the “CRISPR Twins” debacle means for Chinese and international research ethics governance. Account Res. (2019) 26:257–64. doi: 10.1080/08989621.2019.1617138
12. Ramzy A, Wee S-L. Scientist Who Edited Babies' Genes is Likely to Face Charges in China. (2019). Available online at: https://www.nytimes.com/2019/01/21/world/asia/china-gene-editing-babies-he-jiankui.html
13. Cyranoski D. CRISPR-baby scientist fired by university. Nature. (2019) 565:402. doi: 10.1038/d41586-019-00246-2
14. Charo RA. Rogues and regulation of germline editing. N Engl J Med. (2019) 380:976–80. doi: 10.1056/NEJMms1817528
15. Lander ES, Baylis F, Zhang F, Charpentier E, Berg P, Bourgain C, et al. Adopt a moratorium on heritable genome editing. Nature. (2019) 567:165–8. doi: 10.1038/d41586-019-00726-5
16. König H. Germline-editing moratorium-why we should resist it. Nature. (2019) 568:458. doi: 10.1038/d41586-019-01292-6
17. Reardon S. World Health Organization panel weighs in on CRISPR-babies debate. Nature. (2019) 567:444–5. doi: 10.1038/d41586-019-00942-z
18. Normile D. China tightens rules on gene editing. Science. (2019) 363:1023. doi: 10.1126/science.363.6431.1023-b
19. Knoppers BM, Kleiderman E. “CRISPR babies”: what does this mean for science and Canada? CMAJ. (2019) 191:E91–E2. doi: 10.1503/cmaj.181657
20. Canadian Institutes of Health Research. Tri-council Policy Statement: Ethical Conduct for Research Involving Humans. Ottawa: Interagency Secretariat on Research Ethics (2014).
21. Cohen IG, Adashi EY, Ravitsky V. How bans on germline editing deprive patients with mitochondrial disease. Nat Biotechnol. (2019) 37:589–92. doi: 10.1038/s41587-019-0145-8
22. Government of Canada. Royal Commission on New Reproductive Technologies. Proceed with Care: Final Report. (1993). Ottawa, ON.
23. Critchley C, Nicol D, Bruce G, Walshe J, Treleaven T, Tuch B. Predicting public attitudes toward gene editing of germlines: the impact of moral and hereditary concern in human and animal applications. Front Genetics. (2018) 9:704. doi: 10.3389/fgene.2018.00704
25. Health Canada. Consultation on Proposed Assisted Human Reproduction Regulations. (2018). Available online at: https://www.canada.ca/en/health-canada/programs/consultation-assisted-human-reproduction-regulations.html
26. Motluk A. First prosecution under Assisted Human Reproduction Act ends in conviction. CMAJ. (2014) 186:E75–6. doi: 10.1503/cmaj.109-4687
40. Caulfield T, Bubela T. Why a criminal ban? Analyzing the arguments against somatic cell nuclear transfer in the Canadian parliamentary debate. Am J Bioeth. (2007) 7:51–61. doi: 10.1080/15265160601109655
41. Hyun I. Policy: regulate embryos made for research. Nat News. (2014) 509:27. doi: 10.1038/509027a
42. Health Canada. Prohibitions Related to Scientific Research and Clinical Applications. Government of Canada (2014). Available online at: https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/legislation-guidelines/assisted-human-reproduction/prohibitions-scientific-research-clinical-applications.html
43. Fraser R, Lin C-J. Epigenetic reprogramming of the zygote in mice and men: on your marks, get set, go! Reproduction. (2016) 152:R211–22. doi: 10.1530/REP-16-0376
44. Alazami AM, Awad SM, Coskun S, Al-Hassan S, Hijazi H, Abdulwahab FM, et al. TLE6 mutation causes the earliest known human embryonic lethality. Genome Biol. (2015) 16:240–7. doi: 10.1186/s13059-015-0792-0
45. Harrison SE, Sozen B, Christodoulou N, Kyprianou C, Zernicka-Goetz M. Assembly of embryonic and extraembryonic stem cells to mimic embryogenesis in vitro. Science. (2017) 356:eaal1810. doi: 10.1126/science.aal1810
46. Warmflash A, Sorre B, Etoc F, Siggia ED, Brivanlou AH. A method to recapitulate early embryonic spatial patterning in human embryonic stem cells. Nat Methods. (2014) 11:847–54. doi: 10.1038/nmeth.3016
47. Aach J, Lunshof J, Iyer E, Church GM. Addressing the ethical issues raised by synthetic human entities with embryo-like features. eLife. (2017) 6:e20674. doi: 10.7554/eLife.27642
48. Rossant J. Gene editing in human development: ethical concerns and practical applications. Development. (2018) 145:dev150888. doi: 10.1242/dev.150888
49. Pera MF, de Wert G, Dondorp W, Lovell-Badge R, Mummery CL, Munsie M, et al. What if stem cells turn into embryos in a dish? Nat Methods. (2015) 12:917–9. doi: 10.1038/nmeth.3586
50. Ishii T, Pera RAR, Greely HT. Ethical and legal issues arising in research on inducing human germ cells from pluripotent stem cells. Cell Stem Cell. (2013) 13:145–8. doi: 10.1016/j.stem.2013.07.005
51. Tremblay JP, Iyombe-Engembe J-P, Duchêne B, Ouellet DL. Gene editing for duchenne muscular dystrophy using the CRISPR/Cas9 technology: the importance of fine-tuning the approach. Mol Ther. (2016) 24:1888–9. doi: 10.1038/mt.2016.191
52. National Academies of Sciences, Engineering, and Medicine. Human Genome Editing: Science, Ethics, and Governance. Washington, DC: The National Academies Press (2017).
53. Nuffield Council on Bioethics. Genome Editing and Human Reproduction: Social and Ethical Issues. London: Nuffield Council on Bioethics (2018).
54. Liang P, Xu Y, Zhang X, Ding C, Huang R, Zhang Z, et al. CRISPR/Cas9-mediated gene editing in human tripronuclear zygotes. Protein Cell. (2015) 6:363–72. doi: 10.1007/s13238-015-0153-5
55. Kang X, He W, Huang Y, Yu Q, Chen Y, Gao X, et al. Introducing precise genetic modifications into human 3PN embryos by CRISPR/Cas-mediated genome editing. J Assist Reprod Genetics. (2016) 33:581–8. doi: 10.1007/s10815-016-0710-8
56. Callaway E. UK scientists gain licence to edit genes in human embryos. Nat News. (2016) 530:18. doi: 10.1038/nature.2016.19270
57. Fogarty NM, McCarthy A, Snijders KE, Powell BE, Kubikova N, Blakeley P, et al. Genome editing reveals a role for OCT4 in human embryogenesis. Nature. (2017) 550:67–73. doi: 10.1038/nature24033
58. Sample I. First UK Licence to Create Three-Person Baby Granted by Fertility Regulator. (2017). Available online at: https://www.theguardian.com/science/2017/mar/16/first-licence-to-create-three-person-baby-granted-by-uk-fertility-regulator
59. Le Page M. UK Becomes First Country to Give Go Ahead to Three-Parent Babies. (2016). Available online at: https://www.newscientist.com/article/2116407-uk-becomes-first-country-to-give-go-ahead-to-three-parent-babies/
60. Reyes AP, Lanner F. Towards a CRISPR view of early human development: applications, limitations and ethical concerns of genome editing in human embryos. Development. (2017) 144:3–7. doi: 10.1242/dev.139683
61. Ma H, Marti-Gutierrez N, Park S-W, Wu J, Lee Y, Suzuki K, et al. Correction of a pathogenic gene mutation in human embryos. Nature. (2017) 548:413–9. doi: 10.1038/nature23305
62. Ledford H. CRISPR fixes disease gene in viable human embryos. Nat News. (2017) 548:13–14. doi: 10.1038/nature.2017.22382
63. Tachibana M, Sparman M, Sritanaudomchai H, Ma H, Clepper L, Woodward J, et al. Mitochondrial gene replacement in primate offspring and embryonic stem cells. Nature. (2009) 461:367–72. doi: 10.1038/nature08368
64. Tachibana M, Amato P, Sparman M, Woodward J, Sanchis DM, Ma H, et al. Towards germline gene therapy of inherited mitochondrial diseases. Nature. (2013) 493:627–31. doi: 10.1038/nature11647
65. Kang E, Wu J, Gutierrez NM, Koski A, Tippner-Hedges R, Agaronyan K, et al. Mitochondrial replacement in human oocytes carrying pathogenic mitochondrial DNA mutations. Nature. (2016) 540:270–5. doi: 10.1038/nature20592
66. Barritt JA, Willadsen S, Brenner C, Cohen J. Cytoplasmic transfer in assisted reproduction. Hum Reprod Update. (2001) 7:428–35. doi: 10.1093/humupd/7.4.428
67. De Los Angeles A, Pho N, Redmond DE Jr. Generating human organs via interspecies chimera formation: advances and barriers. Yale J Biol Med. (2018) 91:333–42.
68. Hayasaki E. Better Living Through CRISPR: Growing Human Organs in Pigs. (2019). Available online at: https://www.wired.com/story/belmonte-crispr-human-animal-hybrid-organs/
69. Kobayashi T, Zhang H, Tang WW, Irie N, Withey S, Klisch D, et al. Principles of early human development and germ cell program from conserved model systems. Nature. (2017) 546:416–20. doi: 10.1038/nature22812
70. Wu J, Platero-Luengo A, Sakurai M, Sugawara A, Gil MA, Yamauchi T, et al. Interspecies chimerism with mammalian pluripotent stem cells. Cell. (2017) 168:473–86. doi: 10.1016/j.cell.2016.12.036
71. Adashi EY, Cohen IG, Hanna JH, Surani AM, Hayashi K. Stem cell-derived human gametes: the public engagement imperative. Trends Mol Med. (2019) 25:165–7. doi: 10.1016/j.molmed.2019.01.005
72. Cohen IG, Daley GQ, Adashi EY. Disruptive reproductive technologies. Sci Transl Med. (2017) 9:372–4. doi: 10.1126/scitranslmed.aag2959
73. Sawai T, Hatta T, Fujita M. Japan significantly relaxes its human-animal chimeric embryo research regulations. Cell Stem Cell. (2019) 24:513–4. doi: 10.1016/j.stem.2019.03.015
74. Ethikrat D. Opinion: Human-Animal Mixtures. (2011). Available online at: https://www.ethikrat.org/fileadmin/Publikationen/Stellungnahmen/englisch/opinion-human-animal-mixtures-in-research.pdf
75. National Institutes of Health. Request for Public Comment on the Proposed Changes to the NIH Guidelines for Human Stem Cell Research and the Proposed Scope of an NIH Steering Committee's Consideration of Certain Human-Animal Chimera Research. (2016). Available online at: https://grants.nih.gov/grants/guide/notice-files/not-od-16--128.html
76. Giquel C, De Vos J, Bourret R, Vialla F, Martinez E, Thonnat-Marin A. La création d'animaux chimères porteurs d'organes humains. Méd Droit. (2016) 2016:37–47. doi: 10.1016/j.meddro.2015.10.005
77. Bubela T, Strotmann A, Adams R, Morrison S. Commercialization and collaboration: competing policies in publicly funded stem cell research? Cell Stem Cell. (2010) 7:25–30. doi: 10.1016/j.stem.2010.06.010
78. Council of Canadian Academies. Building on Canada's Strengths in Regenerative Medicine: Workshop Report. Ottawa, ON (2017).
79. The Honourable Leona Aglukkaq (Minister of Health). Assisted Human Reproduction Canada: Report on Plans and Priorities 2012–13. (2012). Available online at: http://publications.gc.ca/collections/collection_2012/pac-ahrc/H176–1-2012-eng.pdf
80. Canadian Institutes of Health Research. Terms of Reference - Stem Cell Oversight Committee. (2018). Available online at: http://www.cihr-irsc.gc.ca/e/20410.html
81. Stirling A. Risk, precaution and science: towards a more constructive policy debate: talking point on the precautionary principle. EMBO Rep. (2007) 8:309–15. doi: 10.1038/sj.embor.7400953
82. Kmietowicz Z. UK becomes first country to allow mitochondrial donation. BMJ. (2015) 350:h1103. doi: 10.1136/bmj.h1103
83. Sample I. UK Doctors Select First Women to Have ‘Three-Person Babies'. (2018). Available online at: https://www.theguardian.com/science/2018/feb/01/permission-given-to-create-britains-first-three-person-babies
84. Darwin Life Nadiya. Available online at: http://dl-nadiya.com/
85. Wilkinson B. Controversial ‘Three-Person' IVF Used for Baby Boy Born in Greece. (2019). Available online at: https://www.cnn.com/2019/04/11/health/birth-experimental-ivf-greece-scln-intl/index.html
Keywords: assisted reproductive technologies, regulation, criminal law, constitutional law, in vitro research, mitochondrial replacement therapy, germline gene editing, Canada
Citation: Bubela T, Kleiderman E, Master Z, Ogbogu U, Ravitsky V, Zarzeczny A and Knoppers BM (2019) Canada's Assisted Human Reproduction Act: Pragmatic Reforms in Support of Research. Front. Med. 6:157. doi: 10.3389/fmed.2019.00157
Received: 10 May 2019; Accepted: 24 June 2019;
Published: 10 July 2019.
Edited by:
Patrick Legros, Free University of Brussels, BelgiumReviewed by:
Lise Aagaard, Havemann Ltd., DenmarkCopyright © 2019 Bubela, Kleiderman, Master, Ogbogu, Ravitsky, Zarzeczny and Knoppers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tania Bubela, dGJ1YmVsYUBzZnUuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.