
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med., 17 April 2019
Sec. Hematology
Volume 6 - 2019 | https://doi.org/10.3389/fmed.2019.00080
This article is part of the Research TopicProceedings of KININ2018CLE, Cleveland, Ohio, June 18-20, 2018: A Compendium of the PresentationsView all 15 articles
 Camila Lopes Veronez1
Camila Lopes Veronez1 Régis Albuquerque Campos2Rosemeire Navickas Constantino-Silva3
Régis Albuquerque Campos2Rosemeire Navickas Constantino-Silva3 Priscila Nicolicht1
Priscila Nicolicht1 João Bosco Pesquero1
João Bosco Pesquero1 Anete Sevciovic Grumach3*
Anete Sevciovic Grumach3*Abdominal pain due to intestinal swellings is one of the most common manifestations in hereditary angioedema (HAE). Bowel swellings can cause severe abdominal pain, nausea, vomiting, and diarrhea, which may lead to misdiagnosis of gastrointestinal disorders. In rare cases, HAE abdominal attacks can be accompanied by acute pancreatitis. Here, we report 3 patients with HAE and acute pancreatitis and present a literature review of similar cases. Patients with confirmed diagnosis of HAE secondary to C1-inhibitor (C1-INH) deficiency (n = 2) and HAE with normal C1-INH and F12 mutation (F12-HAE) (n = 1) were included. Pancreatitis was diagnosed based on clinical symptoms and high lipase and amylase levels. Three HAE patients were diagnosed with acute pancreatitis based on increased amylase levels during severe abdominal swelling episodes. Two were previously diagnosed with HAE type I and one with F12-HAE. Pancreatitis was efficiently treated in two patients using Icatibant, with pain relief within hours. When conservatively treated, pancreatitis pain took longer time to resolve. Eighteen pancreatitis cases in HAE with C1-INH deficiency were previously reported and none in F12-HAE. Most patients (12/18) underwent invasive procedures and/or diagnostic methods. Although rare, severe abdominal HAE attacks could cause pancreatitis; HAE-specific treatments may be efficient for HAE-associated pancreatitis. HAE should be considered as a differential diagnosis of acute idiopathic pancreatitis. To our knowledge, this is the first report of HAE-associated pancreatitis in a F12-HAE patient treated with Icatibant.
Hereditary angioedema (HAE) is an autosomal dominant disease caused mostly by deleterious mutations in the gene encoding the C1-inhibitor (C1-INH) (C1-INH-HAE). It occurs in quantitative and functional C1-INH deficiency (type I) or functional C1-INH deficiency (type II) (OMIM #106100) (1). Another group of patients present with clinical characteristics of HAE with normal C1-INH (2). In these cases, HAE can be caused by specific mutations in F12 gene (F12-HAE) (OMIM #610618) (2). Recently, HAE with normal C1-INH has been linked to mutations in genes encoding plasminogen (3) and angiopoietin 1 (4), however, there are still patients with unknown genetic cause.
The characteristic symptoms are nonpruritic and nonpitting swelling of submucosal or subcutaneous tissues involving the face, hands, feet, arms, legs, intestines, genitourinary tract, and upper airways, which can be life threatening (5). HAE symptoms generally last 2–5 days before resolving spontaneously without treatment; the most common trigger factors include emotional stress, infections, trauma, medical and surgical procedures, and estrogens (1, 5).
Abdominal pain is one of the most common manifestations of HAE (5, 6). Bowel swellings can cause severe abdominal pain, nausea, vomiting, and diarrhea. These symptoms may lead to misdiagnosis of gastrointestinal disorders; consequently, patients are frequently submitted to invasive procedures and unnecessary surgeries (5–7). In rare cases, HAE abdominal attacks can be accompanied by acute pancreatitis; this association is not fully understood and/or documented. Herein, we described 3 patients with HAE who presented with pancreatitis and abdominal attacks concomitantly and a review of other cases previously described in the literature.
This study was carried out in accordance with the recommendations of ethical standards of the 1964 Declaration of Helsinki. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee in Research of Universidade Federal de São Paulo (n°56522). Written informed consent for publication was obtained from all the participants of this case report.
A 21-year-old male patient presented to the emergency with severe abdominal pain of 7 h and 8 vomiting episodes. The first test showed normal amylase (93 U/L; normal 30-110 U/L) and slightly augmented lipase levels (332 U/L; normal 23-300 U/L). Analgesics were administered with partial improvement of pain. The second test performed 8 h after patient's admission revealed increase in levels of amylase to 292 U/L and lipase to 1,159 U/L, indicating acute pancreatitis. An increased volume of pancreatic tail, but no gallbladder, was observed through endoscopic retrograde cholangiopancreatography (ERCP) and magnetic resonance imaging (MRI) showed intestinal swelling. Two years before this episode of pancreatitis, he had been diagnosed with HAE type I, characterized by low C1-INH and C4 levels. The onset of HAE occurred at 1 year of age and consisted of facial edema triggered by trauma. Since then, he has been presenting with intermittent and irregular swelling episodes of the hands and feet, abdominal pain, and 3 episodes of upper airway edema. Due to HAE diagnosis, Icatibant (30 mg) was administered 19 h after admission, and the pain significantly reduced within 3 h. Amylase (69 U/L; normal 30–110 U/L) and lipase (165 U/L; normal 23–300 U/L) normalized 18 h after Icatibant injection and the patient was discharged the next day.
A 47-year-old female patient with C1-INH-HAE diagnosed 8 years earlier, presented to the emergency department with distended abdomen and severe abdominal pain lasting 24 h . The first test revealed increased amylase 210 U/L (normal 28–100 U/L), which considering a longer duration of abdominal pain indicated the development of pancreatitis. Since the hospital located in the North of Brazil had no vacancy, a single dose of Icatibant (30 mg) provided by the patient was administered and she was subsequently discharged. The next day, she presented with almost complete relief from the abdominal pain; in a total of 7 days, amylase and lipase reduced to normal levels. This patient has been presenting with recurrent angioedema attacks in the abdomen, face, limbs, and a few episodes in the upper airways, since she was 28-year-old. At that age, she underwent appendectomy and was misdiagnosed with Familial Mediterranean Fever. Only after 11 years, was she correctly diagnosed with C1-INH-HAE, confirmed using low C4 (6 mg/dL; normal 10–40 mg/dL) and C1-INH plasma levels (2 mg/dL; normal 19–40 mg/dL). She was treated with a prophylactic use of plasma-derived C1-INH and Icatibant during the attacks.
A 52-year-old female patient with F12-HAE (mutation p.Thr328Lys) had the onset of angioedema attacks at 16 years of age, during her first pregnancy. Symptoms were edema affecting the face, hands, and feet and abdominal pain. Currently, angioedema episodes occur monthly despite tranexamic acid prophylaxis (500 mg/day), mostly affecting gastrointestinal tract. Recently, one abdominal attack required 4 days of hospitalization. Pancreatitis was diagnosed using acute abdominal pain, high serum amylase levels (391 U/L; normal 25–125 U/L), and pathological signs at abdominal ultrasonography (US). She had normal leucocyte and platelet counts, total bilirubin, and aspartate aminotransferase. She was conservatively treated for pancreatitis due to the lack of the specific medication for HAE.
Acute pancreatitis is diagnosed if a patient presents with at least two of the following characteristics: (a) severe and persistent acute abdominal pain, (b) high serum lipase and/or amylase (3 times the normal upper limit), (c) and/or characteristic findings of pancreatitis on imaging tests (computed tomography, MRI, or US) (8). In addition, if the major and minor risk factors for acute pancreatitis is absent, like gallstones and alcohol misuse, and hereditary or drug-induced pancreatitis, other uncommon causes must be considered for an effective management (9).
The first report of pancreatitis associated with HAE is from 1986, which describes 3 C1-INH-HAE patients with recurrent abdominal attacks found to develop idiopathic chronic pancreatitis (10). In the sequence, more 12 independent cases have been reported, all are C1-INH-HAE (11–22) (Table 1). Although abdominal attacks are quite frequent among the different types of HAE, monitoring pancreatic enzymes is not routinely performed. Aksoy et al. (20) described a male patient diagnosed with HAE type I only after presenting with 4–5 episodes of abdominal pain and pancreatitis, despite that swelling of the face, lips, and tongue had occurred in the first attack (20). In another report, a 6-year-old boy with acute pancreatitis was diagnosed with HAE only after 10 hospitalizations in a period of 18 months. Within this period, this patient underwent cholecystectomy, however, no gallstones were found (16).
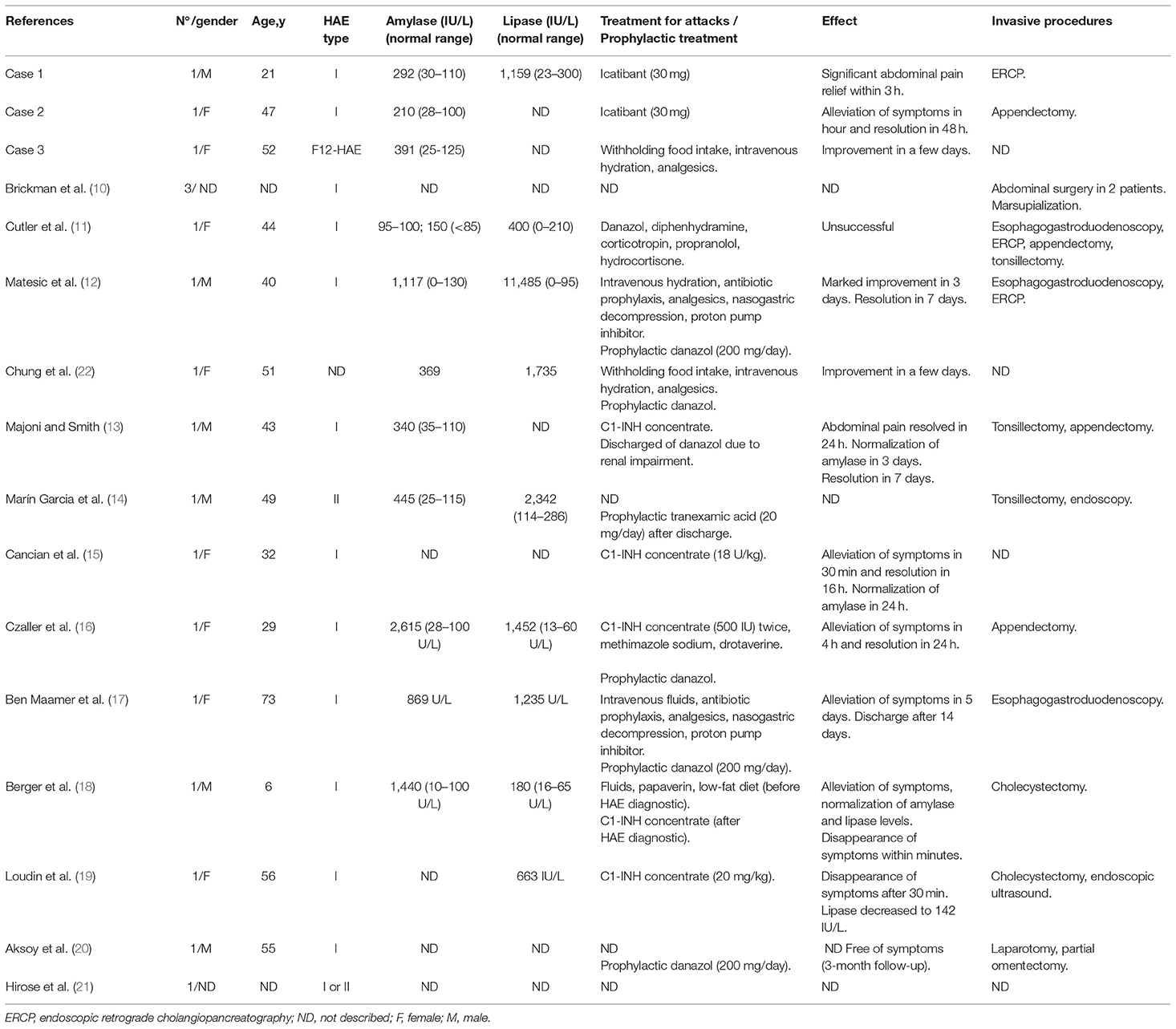
Table 1. Case reports of pancreatitis in HAE patients.
Not only is pancreatitis underdiagnosed, HAE patients frequently undergo invasive or improper diagnostic methods and treatments (5, 23), especially when they present with isolated or predominantly abdominal swellings. Patient 2 underwent appendectomy and spent years relying on a wrong diagnosis. In Case 1, the patient was submitted to an ERCP during the pancreatitis investigation. Likewise, in the other 15 published cases, 7 invasive diagnostic procedures and 12 surgeries possibly related to HAE had been done (Table 1). These include 3 appendectomies and 3 tonsillectomies, 2 cholecystectomies, 2 non-specified abdominal surgeries, 1 laparotomy, 1 omentectomy, and 1 marsupialization (Table 1). In a prospective study, one Japanese patient presented with acute abdomen with intestinal edema; acute pancreatitis was newly diagnosed with C1-INH-HAE (21).
Patients with HAE and normal C1-INH present with similar clinical manifestations as HAE-C1-INH ones. Some authors described facial edema as the most frequent event among F12-HAE (24), nevertheless, we observed that more than 60% of these patients had recurrent abdominal swellings (6). Here, we report the first patient with pancreatitis associated with HAE attack.
During HAE attacks, the obstruction of pancreatic duct or ampulla of Vater can result from duodenal edema, the most probable cause of pancreatitis in this situation. Pancreatic edema itself is not reported in HAE. Aksoy et al. (20) reported mild pancreatic duct dilation and side duct ectasia using magnetic resonance cholangiopancreatography during an HAE-associated pancreatitis episode, supporting the hypothesis that obstruction of pancreatic duct is responsible for pancreatitis in HAE (20); however, in other case reports, pancreatic duct presented normal (12, 17, 19). The obstruction of pancreatic duct causes the blockage of pancreatic secretion, leading to zymogen granules fusion with lysosomes, trypsinogen activation, and autodigestive injury of acinar cells, stimulating inflammatory response (9).
Since angioedema attacks resolve spontaneously in 2–5 days, HAE-associated acute pancreatitis should also disappear within a few days. This was observed in Case 3, and in the reviewed cases in which pancreatitis was treated conservatively (11, 12, 17, 18). However, we cannot establish if the episode described in Case 3 is a pancreatitis associated with an HAE swelling, or a single acute pancreatitis, since no specific medication was administered. Indeed, as well as HAE abdominal attacks are frequently misdiagnosed and mistreated, a comprehensive evaluation of abdominal pain in HAE patients unsuccessfully treated with specific medication should be performed.
When specific treatment for acute HAE attacks was administered (C1-INH replacement), the alleviation and resolution of symptoms was remarkably faster, within hours to a maximum of 1 day (13, 15, 16, 18, 19). C1-INH administration was beneficial in different experimental animal models of pancreatitis (25–27), but ineffective in others (28). Although the benefits of C1-INH therapy are questionable in general pancreatitis, the cases here reviewed indicate good efficacy in HAE-associated pancreatitis.
For the first time, we observed improvement of clinical symptoms caused by abdominal pain and pancreatitis with the administration of Icatibant, a specific antagonist of bradykinin B2 receptor, in Cases 1 and 2. B2 receptor antagonists were shown to diminish pain associated to pancreatitis (29), to reduce pancreatic plasma extravasation, and pancreatic neutrophil influx (30), and to reduce serum amylase and lipase (31) in different pancreatitis-induced models. Although a direct activation of B2 receptors in pancreatitis pathogenesis can be speculated (by both circulating or local bradykinin released by tissue kallikrein), the role of the kinin system in pancreatitis is still unknown.
To our knowledge, other treatments available for acute HAE attacks have not reported for pancreatitis yet. In addition to patient from Case 1, six of the reported patients were under prophylactic treatment with danazol, an attenuated androgen which increases the production of hepatic C1-INH. On the other side, danazol can also be associated with pancreatitis development (9, 32), but in this case, pancreatitis should not resolve spontaneously. Moreover, elevated liver enzymes, a common sign of steroid injury, had been described in only one of the patients presenting pancreatitis and taking danazol (12). One of our patients (case 3) presented with high gamma-glutamyl transferase and slightly high alanine aminotransferase, but she was under long-term prophylaxis with tranexamic acid, a plasmin inhibitor, and not steroids. Moreover, we could not find a causative association between danazol prophylaxis and HAE-associated pancreatitis in any of the 18 cases described.
In conclusion, we present here the first description of HAE-associated acute pancreatitis in a F12-HAE patient and the first cases treated with icatibant. Although HAE attacks are rarely associated with pancreatitis, our findings and the review of literature suggest to investigate HAE in idiopathic pancreatitis. Likewise, pancreatitis signs should be searched for in severe abdominal attacks in HAE patients to avoid further complications. The efficient response to C1-INH replacement and B2 receptor antagonist (Icatibant) indicates that specific drugs for HAE attacks can be useful options for HAE-associated pancreatitis in addition to the conservative treatment.
This study was carried out in accordance with the recommendations of ethical standards of the 1964 Declaration of Helsinki with written informed consent from all subjects. The protocol was approved by the Ethics Committee in Research of Universidade Federal de São Paulo (n°56522).
CV, RC-S, and PN performed the analysis and reviewed the literature. CV conceptualized and drafted the manuscript. RAC and AG performed the data collection instruments, and coordinated data collection. AG and JP conceptualized the study, coordinated and supervised data collection. All the authors drafted, reviewed and approved the manuscript.
This work received grants from Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP–grants numbers 2013/02661-4, 2014/27198-8, and 2015/25494-1) and from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq–grant number 407714/2018-9).
AG and CV received grants from Shire International GmbH (Investigator Initiated Research–IST-BRA-000778 and IIR-BRA-002232).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Dr. Fernanda Gontijo Minafra Silveira Santos from the Universidade Federal de Minas Gerais for helpful discussion on clinical cases.
1. Maurer M, Mager M, Ansotegui I, Aygören-Pürsün E, Betschel S, Bork K, et al. The international WAO/EAACI guideline for the management of hereditary angioedema—the 2017 revision and update. Allergy. (2018) 73:1575–96. doi: 10.1111/all.13384
2. Zuraw BL. Hereditary angioedema with normal C1 inhibitor: four types and counting. J Allergy Clin Immunol. (2018) 141:884–5. doi: 10.1016/j.jaci.2018.01.015
3. Bork K, Wulff K, Steinmüller-Magin L, Braenne I, Staubach-Renz P, Witzke G, et al. Hereditary angioedema with a mutation in the plasminogen gene. Allergy. (2018) 73:442–50. doi: 10.1111/all.13270
4. Bafunno V, Firinu D, D'Apolito M, Cordisco G, Loffredo S, Leccese A, et al. Mutation of the angiopoietin-1 gene (ANGPT1) associates with a new type of hereditary angioedema. J Allergy Clin Immunol. (2018) 141:1009–17. doi: 10.1016/j.jaci.2017.05.020
5. Cicardi M, Aberer W, Banerji A, Bas M, Bernstein JA, Bork K, et al. Classification, diagnosis, and approach to treatment for angioedema: consensus report from the Hereditary Angioedema International Working Group. Allergy. (2014) 69:602–16. doi: 10.1111/all.12380
6. Veronez CL, Moreno AS, Constantino-Silva RN, Maia LSM, Ferriani MPL, Castro FFM, et al. Hereditary angioedema with normal C1 inhibitor and F12 mutations in 42 brazilian families. J Allergy Clin Immunol Pract. (2018) 6:1209–16.e8. doi: 10.1016/j.jaip.2017.09.025
7. Grumach AS, Valle SO, Toledo E, de Moraes Vasconcelos D, Villela MM, Mansour E, et al. Hereditary angioedema: first report of the Brazilian registry and challenges. J Eur Acad Dermatol Venereol. (2013) 27:e338–44. doi: 10.1111/j.1468-3083.2012.04670.x
8. Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis-−2012: revision of the Atlanta classification and definitions by international consensus. Gut. (2013) 62:102–11. doi: 10.1136/gutjnl-2012-302779
9. Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet. (2015) 386:85–96. doi: 10.1016/S0140-6736(14)60649-8
10. Brickman CM, Tsokos GC, Balow JE, Lawley TJ, Santaella M, Hammer CH, et al. Immunoregulatory disorders associated with hereditary angioedema. I. Clinical manifestations of autoimmune disease. J Allergy Clin Immunol. (1986) 77:749–57.
11. Cutler AF, Yousif EA, Blumenkehl ML. Hereditary angioedema associated with pancreatitis. South Med J. (1992) 85:1149–50.
12. Matesic D, Fernández Pérez ER, Vlahakis NE, Hagan JB. Acute pancreatitis due to hereditary angioedema. Ann Allergy Asthma Immunol. (2006) 97:611–4. doi: 10.1016/S1081-1206(10)61089-7
13. Majoni SW, Smith SR. Membranous nephropathy in a patient with hereditary angioedema: a case report. J Med Case Rep. (2008) 2:328. doi: 10.1186/1752-1947-2-328
14. Marín García D, Ceballos Torres A, Ruiz Serrato A, García Ordóñez MÁ. Acute pancreatitis associated with hereditary angioedema. Gastroenterol Hepatol. (2010) 33:633–7. doi: 10.1016/j.gastrohep.2010.07.005
15. Cancian M, Vettore G, Realdi G. An uncommon cause of acute pancreatitis. Hereditary angioedema-induced acute pancreatitis. Gastroenterology. (2011) 140:33,370. doi: 10.1053/j.gastro.2010.02.064
16. Czaller I, Molnár K, Csuka D, Varga L, Farkas H. Successful outcome using C1-inhibitor concentrate in acute pancreatitis caused by hereditary angioedema. Gastroenterol Nurs. (2011) 34:60–3. doi: 10.1097/SGA.0b013e31820b269c
17. Ben Maamer A, Zaafouri H, Haoues N, Cherif A. Acute pancreatitis due to hereditary angioedema. Tunis Med. (2011) 89:579–80.
18. Berger TD, Garty BZ. Hereditary angioedema presenting as recurrent acute pancreatitis. Pediatrics. (2016) 137:e20150620. doi: 10.1542/peds.2015-0620
19. Loudin M, Modiano N, Sallay S. Rapid improvement of pancreatitis secondary to hereditary angioedema with C1 inhibitor administration. Am J Med. (2016) 129:e75–6. doi: 10.1016/j.amjmed.2016.02.045
20. Aksoy EK, Koklu S, Ozturk O, Koklu H, Karcaaltincaba M, Sezgin O. Hereditary angioedema: a rare cause of pancreatitis. Clin Res Hepatol Gastroenterol. (2016) 40:e48–9. doi: 10.1016/j.clinre.2016.02.002
21. Hirose T, Kimbara F, Shinozaki M, Mizushima Y, Yamamoto H, Kishi M, et al. Screening for hereditary angioedema (HAE) at 13 emergency centers in Osaka, Japan: a prospective observational study. Medicine. (2017) 96:e6109. doi: 10.1097/MD.0000000000006109
22. Chung D, Busse P, Oh M. Hereditary angioedema and Pancreatitis. J Allergy Clin Immunol. (2007) 119:S273. doi: 10.1016/j.jaci.2006.12.438
23. Giavina-Bianchi P, Arruda LK, Aun MV, Campos RA, Chong-Neto HJ, Constantino-Silva RN, et al. Brazilian guidelines for hereditary angioedema management - 2017 update part 1: definition, classification and diagnosis. Clinics. (2018) 73:e310. doi: 10.6061/clinics/2018/e310
24. Bork K, Wulff K, Witzke G, Hardt J. Hereditary angioedema with normal C1-INH with versus without specific F12 gene mutations. Allergy. (2015) 70:1004–12. doi: 10.1111/all.12648
25. Ruud TE, Aasen AO, Pillgram-Larsen J, Stadaas JO. Effects on peritoneal proteolysis and hemodynamics of prophylactic infusion with C1 inhibitor in experimental acute pancreatitis. Scand J Gastroenterol. (1986) 21:1018–24.
26. Yamaguchi H, Weidenbach H, Luhrs H, Lerch MM, Dickneite G, Adler G. Combined treatment with C1 esterase inhibitor and antithrombin III improves survival in severe acute experimental pancreatitis. Gut. (1997) 40:531–5.
27. Vesentini S, Benetti L, Bassi C, Bonora A, Campedelli A, Zamboni G, et al. Effects of cholinesterase inhibitor in experimental acute pancreatitis in rats. Preliminary results. Int J Pancreatol. (1993) 13:217–20.
28. Niederau C, Brinsa R, Niederau M, Lüthen R, Strohmeyer G, Ferrell LD. Effects of C1-esterase inhibitor in three models of acute pancreatitis. Int J Pancreatol. (1995) 17:189–96.
29. Chen Q, Vera-Portocarrero LP, Ossipov MH, Vardanyan M, Lai J, Porreca F. Attenuation of persistent experimental pancreatitis pain by a bradykinin B2 receptor antagonist. Pancreas. (2010) 39:1220–5. doi: 10.1097/MPA.0b013e3181df1c90
30. Camargo EA, Ferreira T, Ribela MT, de Nucci G, Landucci EC, Antunes E. Role of substance P and bradykinin in acute pancreatitis induced by secretory phospholipase A2. Pancreas. (2008) 37:50–5. doi: 10.1097/MPA.0b013e3185d9b9b
31. Hirata M1, Hayashi I, Yoshimura K, Ishii K, Soma K, Ohwada T, et al. Blockade of bradykinin B(2) receptor suppresses acute pancreatitis induced by obstruction of the pancreaticobiliary duct in rats. Br J Pharmacol. (2002) 135:29–36. doi: 10.1038/sj.bjp.0704462
Keywords: hereditary angioedema, acute pancreatitis, abdominal swelling, C1-inhibitor deficiency, F12 mutation
Citation: Veronez CL, Campos RA, Constantino-Silva RN, Nicolicht P, Pesquero JB and Grumach AS (2019) Hereditary Angioedema-Associated Acute Pancreatitis in C1-Inhibitor Deficient and Normal C1-Inhibitor Patients: Case Reports and Literature Review. Front. Med. 6:80. doi: 10.3389/fmed.2019.00080
Received: 19 December 2018; Accepted: 01 April 2019;
Published: 17 April 2019.
Edited by:
Evi X. Stavrou, Case Western Reserve University, United StatesReviewed by:
Coen Maas, University Medical Center Utrecht, NetherlandsCopyright © 2019 Veronez, Campos, Constantino-Silva, Nicolicht, Pesquero and Grumach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anete Sevciovic Grumach, YXNncnVtYWNoQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.