
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Lupus, 14 May 2024
Sec. Clinical Research and Treatment in Lupus
Volume 2 - 2024 | https://doi.org/10.3389/flupu.2024.1386256
This article is part of the Research TopicShowcase of Key Advances and Challenges in LupusView all 8 articles
 Maria Alexandra Bandehkhoda Wegener1,2Sören Möller3,4Mads Nikolaj Olesen1,2,5,6,†
Maria Alexandra Bandehkhoda Wegener1,2Sören Möller3,4Mads Nikolaj Olesen1,2,5,6,† Jonna Skov Madsen2,7
Jonna Skov Madsen2,7 Grith Lykke Sorensen5,6,8Anne Voss3,9,10
Grith Lykke Sorensen5,6,8Anne Voss3,9,10 Nasrin Asgari1,2,3,5*
Nasrin Asgari1,2,3,5*
Objectives: Central nervous system (CNS) proteins such as neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP) are released into the body fluids following CNS injury. Microfibrillar-associated protein 4 (MFAP4) is an extracellular matrix protein. Recently we reported expression of MFAP4 in CNS and alteration of levels in patients with acute neuroinflammation. We aimed to determine the levels of MFAP4 in a predominantly population-based cohort of systemic lupus erythematosus (SLE) patients, including neuropsychiatric SLE (NPSLE), and to evaluate MFAP4 as a marker of inflammation.
Methods: In total 208 SLE patients, 44 of those with NPSLE, and 50 age- and sex-matched healthy controls (HC) were recruited. MFAP4 was measured using AlphaLISA immunoassay. NfL, GFAP and a panel of inflammatory mediators were measured using Simoa HD-1 digital ELISA or a Luminex 200 instrument.
Results: MFAP4 levels were elevated in patients with NPSLE compared to patients with non-NPSLE (p = 0.031), more prominent in NPSLE patients with CNS involvement (p = 0.017). NfL and GFAP were higher in the total SLE cohort (p < 0.001, p < 0.001, respectively) as well as NPSLE subgroup (p < 0.001, p < 0.001, respectively), and in the subgroup of NPSLE patients with CNS involvement (p < 0.001, p < 0.001), compared to HC. NfL and GFAP levels correlated positively with MFAP4 in the NPSLE as well as the non-NPSLE subgroup (ρ = 0.44, p = 0.003, ρ = 0.25, p = 0.004). VEGF was reduced in NPSLE patients compared to HC (p = 0.015). MMP-9 was elevated in NPSLE compared to non-NPSLE (p = 0.048). Inflammatory markers including IFN-α, IL-6, IL-10 and TNF-α, were elevated in the NPSLE group compared to HC (p < 0.001, p = 0.0026, p = 0.042, p = 0.007, respectively). In NPSLE patients the levels of MFAP4 correlated with TNF-α (p = 0.016) and IL-17 (p = 0.0044) and with markers of blood brain barrier (BBB) disruption MMP-7 (p = 0.005) and VEGF (p < 0.001). In NPSLE patients with CNS manifestations MMP-3 and VEGF correlated with MFAP4 (p = 0.011, p = 0.0004, respectively).
Conclusion: Levels of MFAP4 correlated with NfL, GFAP and proinflammatory cytokines and in NPSLE additionally with markers of BBB disruption, suggesting that MFAP4 is a marker of inflammation and vascular re-organization. Correlation of NfL and GFAP with MFAP4 may reflect CNS tissue damage.
Systemic lupus erythematosus (SLE) is an autoimmune, systemic inflammatory disorder with a heterogeneous clinical presentation (1, 2). It affects multiple tissue and organ systems such as skin, joints, serosa, blood vessels, kidneys and nervous system (1–3). In Denmark the estimated prevalence of SLE is 45.2 per 100.000 but globally up to 517.5 cases per 100.000 have been reported (4, 5). Certain genetic polymorphisms in combination with environmental exposures are believed to induce and maintain the disease (1, 3, 6). This interplay between genetic factors and environment leads to activation of both innate and adaptive immune system components (1), resulting in production of proinflammatory cytokines e.g., type 1 interferons (IFN), synthesis of autoantibodies that recognize the patients' own DNA or RNA, immune complex formation, and amplification of autoreactive lymphocytes (1, 3, 7). These mechanisms lead to a loss of tolerance to self-antigens and eventually lead to irreversible tissue and organ damage (1, 3).
Neuropsychiatric systemic lupus erythematosus (NPSLE) contributes considerably to morbidity and mortality in patients with SLE (8). NPSLE encompasses manifestations from both the central nervous system (CNS) and the peripheral nervous system (PNS) and may give rise to both neurological and psychiatric symptoms (8, 9). In 1999, the American College of Rheumatology (ACR) summarized these NPSLE manifestations and outlined 19 neuropsychiatric syndromes, 12 connected to the CNS and 7 to the PNS, that can appear in patients with SLE (8, 9). These manifestations were further subdivided into focal NPSLE such as stroke and non-focal/diffuse NPSLE such as psychosis, cognitive dysfunction and affective disorders (8, 9).
The exact prevalence of NPSLE is unknown but data indicates that more than 50% of SLE patients have CNS involvement with the most frequent manifestations being headache, mood disorders and cognitive dysfunction (8, 10, 11). Several studies have proposed different potential mechanisms to explain the pathogenesis of NPSLE involving proinflammatory cells, autoantibodies, cytokines, chemokines, complement and other molecules (8, 12, 13). Notably, type 1 IFNs have been found to be elevated in both serum and the hippocampus of SLE patients (8, 14). One specific effect of IFN-α is the production of several cytokines, including the proinflammatory interleukin (IL)-6 (13). IL-6 is found to be elevated in the serum and the CSF of NPSLE patients (13–15) and has been suggested to play a role in the breakdown of the blood-brain-barrier (BBB) in NPSLE (15). Disruption of the BBB is proposed as the common foundation for development of NPSLE as it may lead to entry of proinflammatory cells, cytokines and autoantibodies into the CNS causing neuroinflammation (8, 13, 16, 17). Thus, markers that mirror BBB disruption may be indicators of NPSLE (9) and also elucidate disease pathogenesis. In addition, neuronal and astrocytic damage as reflected in high intrathecal levels of neurofilament light chains (NfL) and glial fibrillary acidic protein (GFAP) have been reported in NPSLE with CNS involvement (18, 19).
Microfibrillar-associated protein 4 (MFAP4) is an extracellular matrix (ECM) protein belonging to the fibrinogen-related domain (FReD) family that includes different proteins engaged in tissue homeostasis and innate immunity (20–22). MFAP4 has binding affinity for the ECM components elastin and collagen that forms elastic and collagen fibers, and MFAP4 is found to play an active role in elastic fiber formation (20, 21, 23). Elastic fibers are ECM macromolecules that have the biomechanical properties of elasticity and resilience (20, 24). These properties are crucial for the structural integrity of the ECM and hence for the function of connective tissue e.g., in arteries, lungs, and skin (20, 24, 25). MFAP4 is measurable in serum, serum levels increase in specific conditions characterized by aberrant tissue remodeling (26) while ECM-bound MFAP4 is predominantly located in arteries and arterioles in most tissues (17). Very recently our group reported data on expression of MFAP4 in the CNS and alteration of the levels of soluble MFAP4 in cerebrospinal fluid (CSF) in patients with acute neuroinflammation and relapse (27). These data suggest that MFAP4 may serve as a potential biomarker of disease activity. Nonetheless, the potential role of MFAP4 in BBB integrity in patients with NPSLE is so far unexplored.
We propose that levels of MFAP4 in serum (a) may differ between SLE patients with and without NPSLE as well as healthy controls (HCs) and (b) may act as a biomarker for inflammation. Hence, this study aimed at measuring serum MFAP4 in a predominantly population based SLE cohort as well as healthy controls (HC), and correlate this to clinical characteristics, cytokines, and markers of BBB disruption.
Patients: A clinical database with associated biobank was established for SLE patients diagnosed in the period 1995–2016 in the Region of Southern Denmark (28–30). A total of 208 SLE patients were included, with 124 cases originating from a population-based cohort from Funen and 84 cases from a clinic-based cohort from the rest of the Region of Southern Denmark as described previously (28, 30). All 208 patients, primarily white Europeans (98%) aged 18–70 years at present and with a female to male ratio of 6.4:1, were included in this cross-sectional study (28, 30). As described previously patients with NPSLE were classified in this SLE cohort (30) in accordance with the ACR nomenclature and case definitions for neuropsychiatric SLE syndromes (31–34, 35), and 44 NPSLE patients were included in the present study, 37 of 44 (84.1%) with CNS involvement (30). Patients not classified with NPSLE are denoted as non-NPSLE in this study. Clinical characteristics and treatment status reported was collected between 2010 and 2012 except patients’ NPSLE status which was classified in 2017. Each patient was diagnosed with SLE by the occurrence of multisystem disease, autoantibodies, and exclusion of other diseases according to Fries & Holman (28, 31) and was classified according to the 1997 revised ACR criteria (28, 32, 33). At the time of inclusion patients had to be 18 years or older, and patients with primary antiphospholipid syndrome and drug induced SLE were excluded from the study (28, 29). Disease activity was monitored using the SLE Disease Activity Index 2000 (SLEDAI-2K) (36). Cumulative disease damage was calculated using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index for SLE, SLICC (28, 33, 37, 38) reflecting both damage due to disease and treatment of SLE (33, 37, 38). The clinical profile of the SLE cohort is comparable to other Western European study populations and has previously been described (28–30).
Controls: Serum from fifty self-reported healthy anonymized blood donors aged 18–65 years was obtained from the blood bank at the Department of Clinical Immunology, Odense University Hospital, Odense, Denmark, in January 2021. Healthy controls (HCs) were from the same geographical background population as the SLE cohort and were matched with regard to age and sex.
The study complies with the Declaration of Helsinki. The clinical data material and blood samples were collected in a study approved by The Regional Committee on Biomedical Research Ethics (Ref. no. S-20100015). Before donation each blood donor approved the use of their blood for research purposes in line with relevant national guidelines (Standards in Transfusion Medicine).
Patient serum was obtained from blood samples taken from 2010 to 2012. Blood samples were collected using standard venipuncture and allowed to clot at room temperature for 30 min before centrifuged for 10 min, serum was transferred into cryo-tubes and stored at −80°C until laboratory analysis. Blood samples from HC were taken in 2021 by venipuncture and stored overnight for coagulation at 4°C before being centrifuged, aliquoted and stored at −80°C. This cold overnight storage has been shown not to affect levels of various cytokines (39).
Serum MFAP4 was measured using AlphaLISA immunoassay (Perkin Elmer, MA, USA) as formerly described (20). Samples were run in duplicates, and occasional samples with coefficient of variation (CV) > 10% (2/208 samples 0.96%) were re-analyzed to obtain a valid measurement for every sample.
Inflammatory mediators in serum were measured on a Luminex 200 instrument (Luminex Corporation, TX, USA, custom designed panel) using a 7-plex kit for interleukin (IL)-6, -10, 17, matrix metalloproteinase (MMP)-3, -7, vascular endothelial growth factor (VEGF) and tumor necrosis factor (TNF)-α and 2-plex for MMP-2 and −9 according to manufacturer's instructions (premixed Human Magnetic Luminex Assay, R&D Systems, MN, USA) (40). Due to limited materiale available MMP-2 and -9 were analysed in 176 out of the 208 SLE patients. All Luminex analyses were done at the Department of Clinical Immunology, Odense University Hospital, Denmark, in February and March 2021.
Serum concentrations of IFN-α, NfL and GFAP were analyzed at the Department of Biochemistry and Immunology, Lillebaelt Hospital, Vejle using the commercial available 2-plex assay for the Single molecule array (Simoa) HD-X Analyzer (Quanterix, Billerica, MA, USA, NfL and GFAP no. 1035209, IFN-α, no.100860), according to manufacturer's instructions (41, 42). The total analytical variation for the included controls were 10%–16% for NfL and 8%–14% for GFAP.
In-house quality controls consisting of pooled anonymous sera were used as inter-run quality control in Luminex (CV: 32% for IL-6, 15% for IL-17, 31% for TNF-α, 10% for VEGF, 1% for MMP-2, 16% for MMP-3, 10% for MMP-7, 3% for MMP-9).
The laboratory staff was blinded with regard to the NPSLE status of patients during the analyses process, and SLE patient and healthy donor samples were randomized across assay layouts.
Statistical calculations were carried out using Stata16 (StataCorp, College Station, TX). Numerical participant characteristics were reported as means with standard deviation (SD), while categorical characteristics were reported as counts and proportions. For comparisons of patient groups within each cohort, normality of variables was assessed using quantile-quantile plots. Approximation of MFAP4 and inflammatory biomarkers to normal distribution was achieved by log10 transformation before further statistical analysis. For comparisons between groups linear regression of log10-transformed measurements with Tukey's multiple testing correction was used. For SLICC and SLEDAI scores, groups were compared using Kruskal–Wallis test. Categorical data were compared using Fisher's exact test. Seven IFN-α measurements were below limits of detection (LOD) and were ignored as missing data to allow usage of parametric tests. This in one way makes detection of significant changes in IFN-a levels difficult but is compensated by the increased power of parametric analyses. A p-value of <0.05 was used as limit of statistical significance. Pairwise associations between MFAP4, clinical variables, treatment status, cytokines or markers of BBB disruption were investigated using Spearman's correlation method or linear regression. We found no correlation (as an indication of degradation with long-term storage) between MFAP4 and time stored in freezer. When comparing NPSLE subgroups (CNS vs. PNS manifestations), the four patients with mixed CNS and PNS manifestations were excluded from analyses.
Of 208 patients in the SLE cohort 44 patients (21%) were previously identified with NPSLE (24) while the rest (79%) are denoted as non-NPSLE in this study.
Only four patients (1.9%) were treatment naive at the time of blood sampling. Further baseline demographics, clinical characteristics, and treatment status of the total SLE cohort, NPSLE and non-NPSLE patients and HC are presented in Table 1.
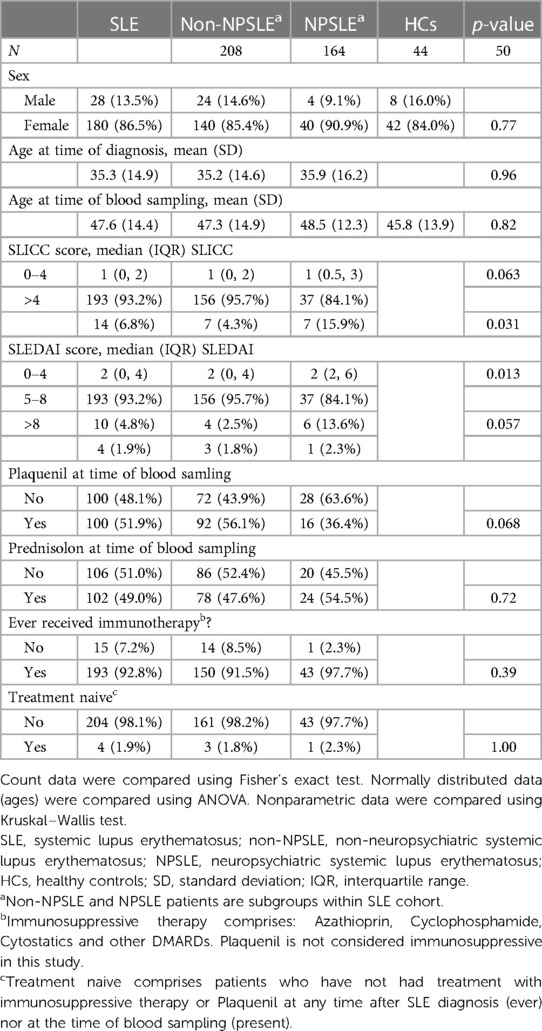
Table 1. Baseline demographics, clinical and treatment status of SLE cohort, NPSLE and non-NPSLE patients and healthy controls.
No difference was found between MFAP4 levels and sex within the total SLE cohort (p = 0.87) nor within the NPSLE group of patients (p = 0.50). Overall, a positive association was found between MFAP4 levels and patients' age at blood sampling (ρ = 0.35, p < 0.001). This positive association with age was also observed in healthy controls (ρ = 0.30, p = 0.032). When NPSLE/non-NPSLE was used as independent variables, this revealed an accelerated age-dependent increase in NPSLE (ρ = 0.51, p < 0.001) compared to non-NPSLE (ρ = 0.31, p < 0.001) (p = 0.008). This age-dependent increase in MFAP4 levels was even more prominent in CNS-group (ρ = 0.59, p < 0.001) compared to non-NPSLE (ρ = 0.31, p < 0.001) (p = 0.014).
A positive association was found between NfL levels and patients' age at blood sampling in healthy controls (ρ = 0.75, p < 0.001) as well as in the NPSLE (ρ = 0.53, p < 0.001) and non-NPSLE subgroups (ρ = 0.36, p = 0.020). When NPSLE/non-NPSLE was used as independent variables, this did not reveal an age-accelerated increase for NfL (p = 0.962).
A positive association was found between GFAP levels and patients' age at blood sampling in healthy controls (ρ = 0.59, p < 0.001) as well as NPSLE (ρ = 0.46, p < 0.001), however not within the non-NPSLE subgroup (ρ = 0.25, p = 0.138). When NPSLE/non-NPSLE was used as independent variables, this did not reveal an age-accelerated increase for GFAP (p = 0.570).
MFAP4 levels were significantly elevated in patients with NPSLE compared to patients with non-NPSLE (p = 0.031), independent of age, more prominent in the NPSLE subgroup with CNS involvement (p = 0.017) (Figures 1A,B). No significant differences were found in MFAP4 between the total SLE cohort and HC (p = 0.77), nor between NPSLE (p = 0.47) and non-NPSLE compared to HC (p = 0.73).
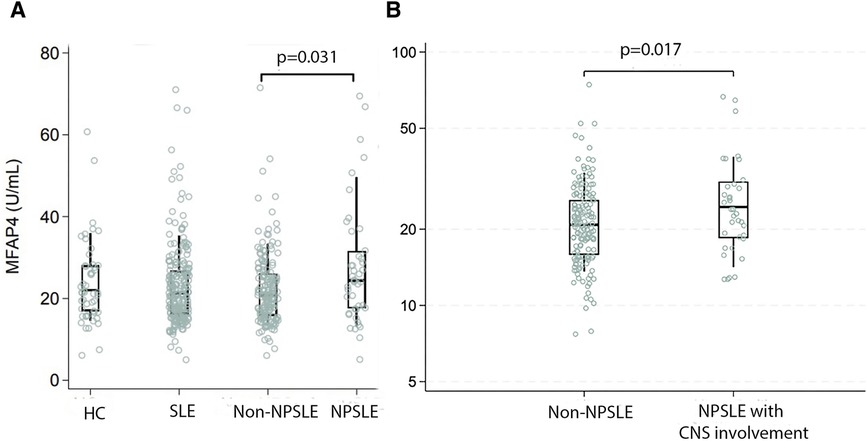
Figure 1. MFAP4 levels in total SLE cohort, non-NPSLE and NPSLE patients and healthy controls. Non-NPSLE and NPSLE patients are subgroups within the SLE cohort. MFAP4 was found significantly elevated in NPSLE (A) and more prominent in NPSLE patients with CNS involvement (B) compared to non-NPSLE patients. HC, healthy controls; SLE, systemic lupus erythematosus; NPSLE, neuropsychiatric systemic lupus erythematosus; Non-NPSLE, non-neuropsychiatric systemic lupus erythematosus; MFAP4, microfibrillar-associated protein 4.
NfL and GPAP levels may be released into blood following CNS tissue damage. In this study NfL and GFAP were found to be significantly higher in the total SLE cohort as well as in the NPSLE subgroup compared to HC (all p < 0.001) (Table 2). NfL and GFAP were found to be significantly higher in the NPSLE subgroup with CNS manifestations compared to HC (p < 0.001, p < 0.001) (Figures 2A,B). No significant difference was found between NPSLE and non-NPSLE (data not shown), neither between the subgroup of NPSLE with CNS involvement and non-NPSLE (data not shown).
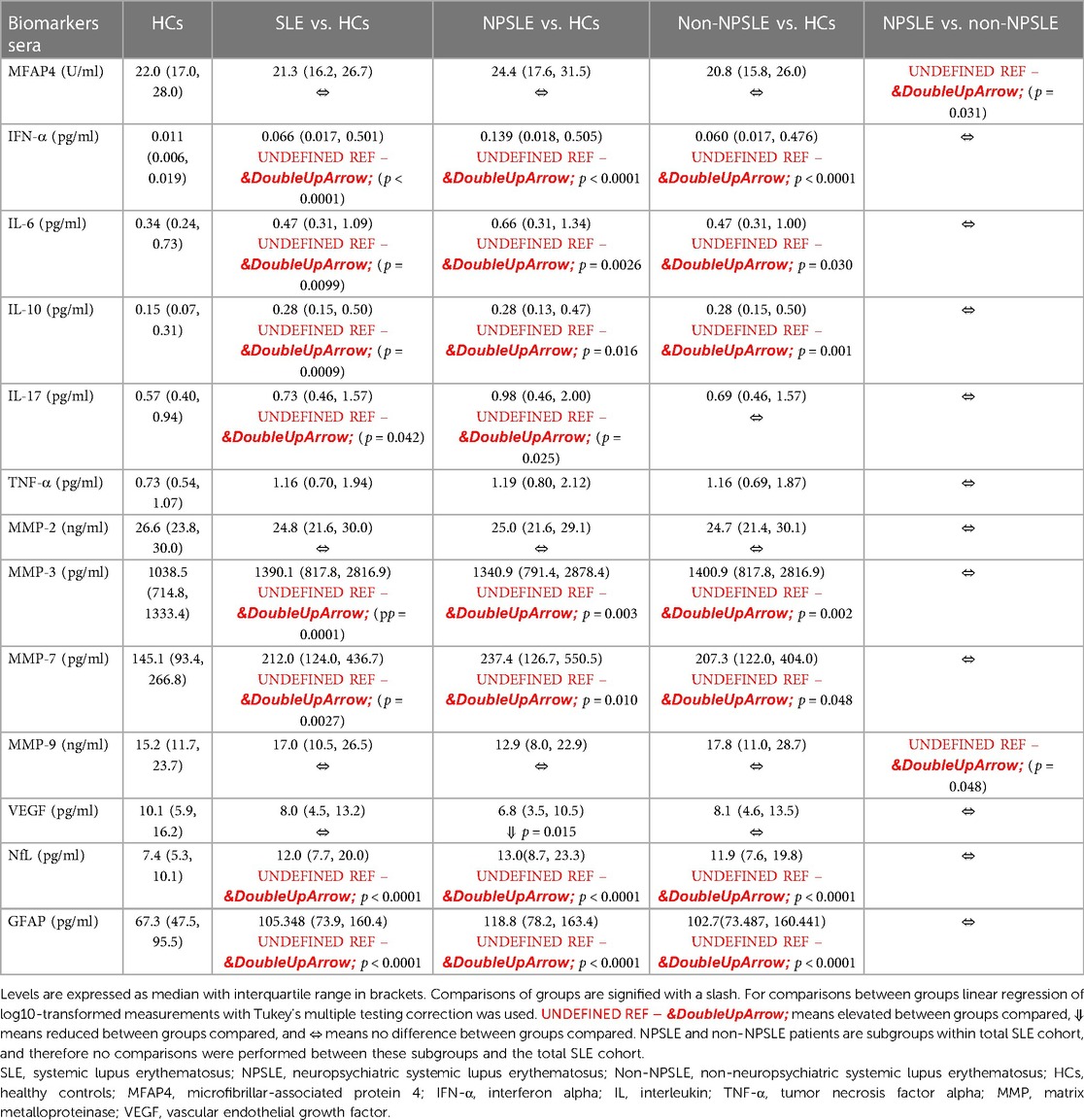
Table 2. Levels of MFAP4, cytokines, MMPs and VEGF in SLE, NPSLE, non-NPSLE and healthy controls.
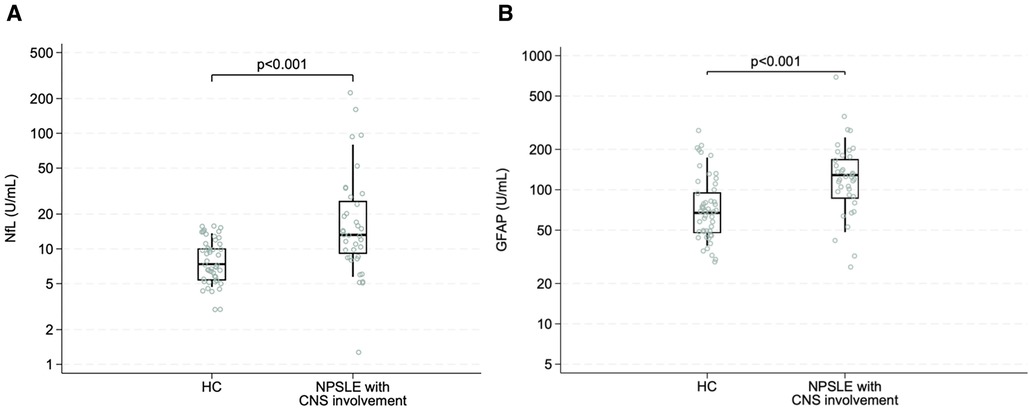
Figure 2. NfL and GFAP levels in NPSLE patients with CNS involvement compared to healthy controls. NfL (A) and GFAP (B) levels were significantly elevated in NPSLE patients with CNS involvement compared to healthy controls.
Markers indicative of BBB disruption may serve as surrogate markers of NPSLE disease activity. Therefore, we examined MMPs (MMP-2, -3, -7, -9) and VEGF. A significant elevation in MMP-3 and MMP-7 levels was found in the total SLE cohort compared to HC (p = 0.001, p = 0.0027, respectively) and in NPSLE patients compared with HC (p = 0.003, p = 0.010). MMP-9 was elevated when comparing NPSLE and non-NPSLE (p = 0.048). Additionally, MMP-2 was significantly elevated in NPSLE patients with CNS manifestations compared to PNS manifestations (p = 0.010). VEGF was significantly reduced in NPSLE patients compared to HC (p = 0.015) (Table 2).
We determined the serum levels of inflammatory markers, also presented in Table 2 for the NPSLE- and non-NPSLE-patients and HC. A significant elevation of IFN-α, IL-10, TNF-α, IL-6 and IL-17 was found in the total SLE cohort compared to HC (p < 0.001, p = 0.0009, p = 0.0022, p = 0.0099, p = 0.042, respectively). IFN-α, IL-10 and TNF-α were significantly elevated in NPSLE (p < 0.001, p = 0.042, p = 0.007, respectively) and in non-NPSLE compared to HC (p < 0.001, p = 0.003, p = 0.004). Also, a significant elevation in IL-6 and IL-17 was observed in the NPSLE compared to HC (p = 0.0026, p = 0.025), and for IL-6 also in non-NPSLE compared to HCs (p = 0.030).
Association between MFAP4, NfL and GFAP and inflammatory markers are shown in Supplementary Table S1.
In brief, a positive association was found between NfL and MFAP4 in the NPSLE as well as the non-NPSLE subgroup (ρ = 0.44, p = 0.003, ρ = 0.25, p = 0.004). This positive association with MFAP4 was also found for GFAP in the NPSLE as well as in non-NPSLE subgroup (ρ = 0.33, p = 0.031, ρ = 0.31, p < 0.001) (Figures 3A,B and Supplementary Table S1).
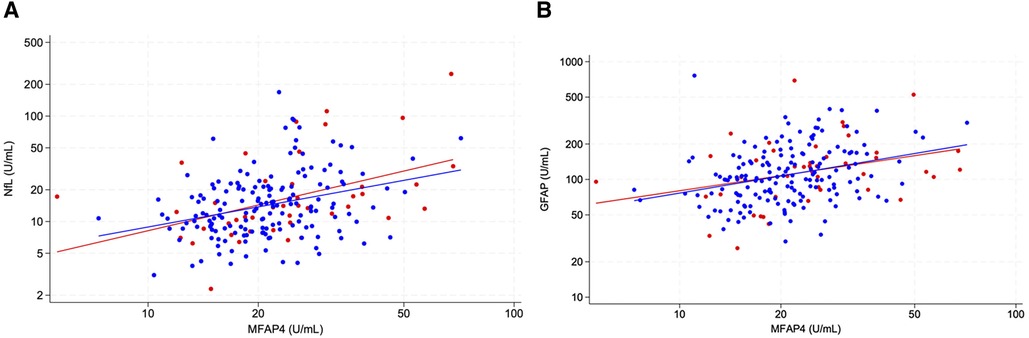
Figure 3. Correlation between NfL and MFAP4 (A) and GFAP and MFAP4 (B) in the NPSLE subgroup (red) and non-NPSLE subgroup (blue). A positive association was found between NfL and MFAP4 and GFAP and MFAP4 in the NPSLE as well as the non-NPSLE.
In the NPSLE-subgroup MMP-2 and MFAP4 was found to be significantantly associated (ρ = 0.39, p = 0.014), however this was not the case for MMP-9 (ρ = −0.25, p = 0.256). An association was found between MMP-7 and VEGF and MFAP4 in NPSLE patients (ρ = 0.43, p = 0.023, ρ = 0.52, p < 0.001, respectively) (Figure 4). No association was found between MMP-7 and VEGF and MFAP4 in non-NPSLE patients (ρ = −0.003, p = 0.967, ρ = −0.062, p = 0.302, respectively). An association was found between MMP-3 and VEGF and MFAP4 in NPSLE patients only with CNS manifestations (ρ = 0.29, p = 0.023, ρ = 0.53, p = 0.001, respectively), however not in the non-NPSLE subgroup (ρ = −0.02, p = 0.836).
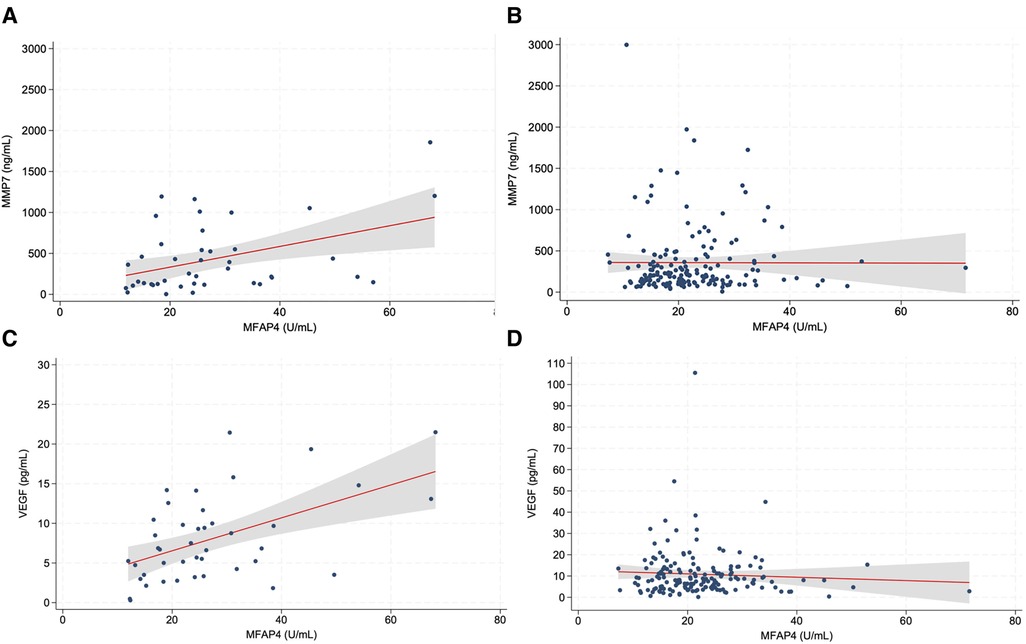
Figure 4. Correlation of MFAP4 with MMP-7 and VEGF in NPSLE subgroup and non-NPSLE subgroup. A significant association was found between MMP-7 and MFAP4 within NPSLE patients (A). Likewise, a significant association was found between VEGF and MFAP4 within NPSLE patients (C). No association was found between MMP-7 and MFAP4 (B) nor between VEGF and MFAP4 (D) in the non-NPSLE subgroup. Grey zone, confidence band. MFAP4, microfibrillar-associated protein 4; MMP-7, matrix metalloproteinase 7; VEGF, vascular endothelial growth factor; SLE, systemic lupus erythematosus; NPSLE, neuropsychiatric systemic lupus erythematosus.
Additionally, an association was found between IL-17 and MFAP4 and between TNF-α and MFAP4 in the NPSLE subgroup (ρ = 0.43, p = 0.006, ρ = 0.36, p = 0.021, respectively), which was not the case in the non-NPSLE subgroup (ρ = −0.09, p = 0.245, ρ = −0.05, p = 0.507, respectively (Figure 5).
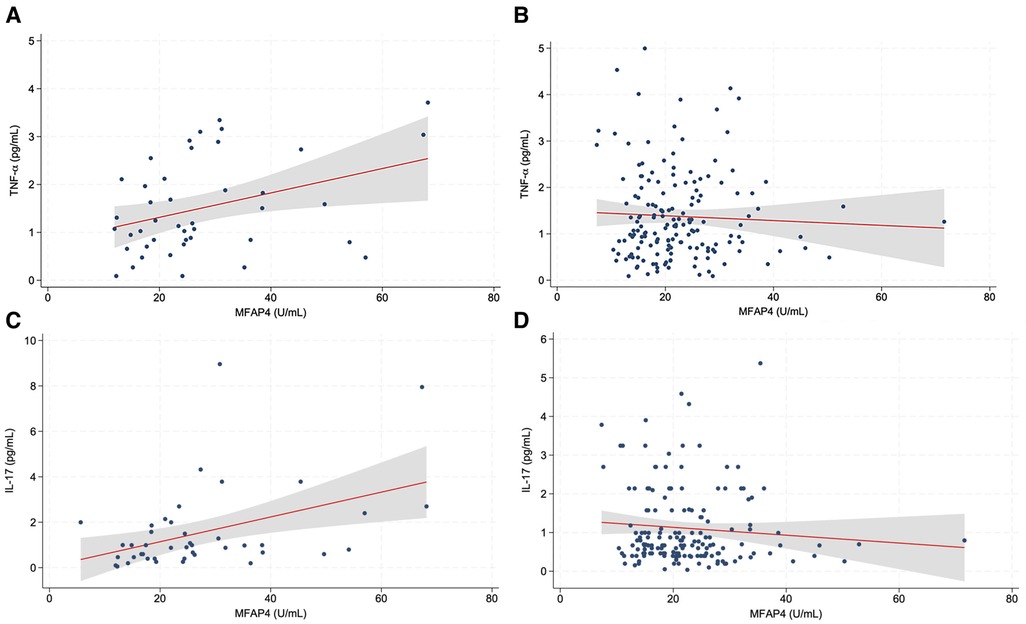
Figure 5. Correlation of MFAP4 with TNF-α and IL-17 in the NPSLE subgroup and non-NPSLE subgroup. A significant association was found between MFAP4 levels and TNF-α within the NPSLE subgroup (A). Furthermore, a significant association was found between MFAP4 levels and IL-17 within NPSLE subgroup (C). No association was found between TNF-α and MFAP4 (B) nor between IL-17 and MFAP4 (D) in the non-NPSLE subgroup. Grey zone, confidence band MFAP4, microfibrillar-associated protein 4; TNF-α, tumor necrosis factor alpha; IL-17, interleukin 17; SLE, systemic lupus erythematosus; NPSLE, neuropsychiatric systemic lupus erythematosus.
A significant association between MFAP4 levels and SLICC score (accumulated disease damage) was found in the non-NPSLE subgroup (ρ = 0.18, p = 0.003). However, no association was found between MFAP4 levels and SLICC score when looking at the NPSLE subgroup (p = 0.19). No significant association was found between MFAP4 and SLEDAI score (present disease activity) neither in the total SLE cohort (p = 0.83) nor the NPSLE subgroup (p = 0.89).
In this predominantly population-based cohort study of SLE with a longitudinal clinical follow-up, the main finding was that MFAP4 levels in the NPSLE subgroup were elevated compared to patients with non-NPSLE, more prominent in NPSLE patients with CNS involvement. In line with this observation markers of neuronal and astrocyte injury (NfL, GFAP) were significantly higher in the NPSLE subgroup with CNS manifestations compared to HC. A significant increase of inflammatory and BBB disruption markers was found in NPSLE subgroup. Remarkably, a positive correlation was found between MFAP4 levels and markers for neuronal (NfL) and astrocyte (GFAP) damage, BBB disruption (MMP-7 and VEGF) and inflammatory markers (TNF-α and IL-17). These data suggest that MFAP4, concurrent with MMPs and VEGF, is a marker for BBB disruption, and like cytokines may act as a marker for inflammation. A positive correlation between MFAP4 and NfL and GFAP may reflect tissue damage. These findings may contribute to the understanding of the pathogenesis of non-NPSLE as well as NPSLE.
The pathogenesis of NPSLE is complex and the precise mechanisms remain elusive (12, 35). BBB disruption is believed to be central in the pathogenesis of NPSLE (8, 13, 16). The BBB is a dynamic, non-absolute barrier that is highly regulated via the interactions between ECM proteins and ECM receptors such as integrin receptors (43). Thus, changes in the ECM components result in alterations of the functions of the BBB cells and leads to increased permeability of the BBB seen in pathological conditions of the CNS such as stroke, multiple sclerosis and Alzheimer's disease (12, 43). MFAP4 is an ECM protein that is located in the vascular ECM in most tissues (20, 21) and is measurable in serum (26). MFAP4 may directly affect the functions of the cells in the BBB as the primary cellular receptor for MFAP4 is integrin αVβ3 (44). Activation of vascular endothelial αVβ3 integrin results in disruption of VE-cadherin localized at the endothelial adherends junctions resulting in increased vascular permeability (43, 45). MMPs, one of the main proteolytic enzyme systems involved in ECM protein degradation during remodeling, is upregulated in pathological conditions such as stroke (43). MFAP4 has been linked with ECM remodeling during vascular injury (20, 44, 46, 47). We recently describe the expression of the MFAP4 in healthy human CNS, in connective tissue spaces of the brain including the meninges and the vascular/perivascular spaces. Notably, in autopsy samples from patients with acute multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD), we observed a downregulation of MFAP4 immunoreactivity at sites of active inflammation documented by the presence of inflammatory infiltrates. In line with these pathology data, cerebrospinal fluid (CSF) MFAP4 levels were reduced in active disease stages (27). The data suggested that inflammation changes the composition of ECM, perhaps due to the secretion of proteolytic enzymes e.g., MMPs in inflammatory conditions. In the present study, we found MFAP4 to be upregulated in NPSLE patients compared to non-NPSLE patients. MMP-3 and MMP-7 were upregulated in NPSLE compared to HC. MMP-2 was upregulated in NPSLE patients with CNS manifestations compared to PNS manifestations. Furthermore, our data showed MFAP4 to be associated with markers of BBB disruption, MMP-7 and VEGF, in patients with NPSLE. MMP-3 and VEGF were found associated with MFAP4 within NPSLE patients only with CNS manifestations. This leads us to suggest that serum MFAP4 levels may reflect the BBB remodeling as a consequence of BBB disruption during CNS inflammation.
In this study higher levels of CNS-proteins, NfL and GFAP, were found in the total SLE cohort as well as NPSLE subgroup compared to HC. Notably, NfL and GFAP were significantly higher in the NPSLE subgroup with CNS manifestations compared to HC. This finding is in accordance with previous studies that reported that in NPSLE patients with CNS involvement, intrathecal levels of NFL and GFAP were increased (18, 19). Remarkably, in our study NfL and GFAP levels correlated positively with MFAP4, which may reflect CNS tissue damage.
Notably in NPSLE, IFN-α has been suggested to directly damage neurons and stimulate microglial engulfment of neurons after BBB disruption, and also to stimulate microglial production of proinflammatory cytokines, like IL-6 and IL-8 (13). IL-6 is believed to increase B-cell activation and survival (13) and may also play a role in BBB breakdown in NPSLE (14). IL-10 and TNF-α are also both thought to be regulators of the immune response in patients with NPSLE (13). IL-6 is furthermore considered to induce the production of IL-17 through T cell differentiation (48). IL-17 is a proinflammatory cytokine that plays a vital role in the pathogenesis of SLE (6, 48). In line with these events the present study shows that IFN-α, IL-6, IL-10, IL-17 and TNF-α were elevated in the total SLE cohort compared to HC. Furthermore, IFN-α, IL-6, IL-10 and TNF-α were significantly elevated in NPSLE compared to HC. Notably, IL-17 and MFAP4 were associated both in the total SLE cohort and in the NPSLE subgroup, and TNF-α was associated with MFAP4 in the NPSLE subgroup. Cytokines have been linked to clinical characteristics of SLE and NPSLE as cytokines drive the inflammatory cascade and lead to disease damage (1, 2, 8, 13, 48).
The study has several strengths. A large predominantly population-based cohort was used, including a significant number of patients with NPSLE. Secondly, analysis was done in a blinded fashion with detailed clinical information. A limitation of the study is the cross-sectional design. Furthermore, the relationship between MFAP4 levels and the type and degree of neuropsychiatric involvement cannot be established in this study due to the limited sample size. Experimental studies suggest that MFAP4 immune reactivity is increased in cardiovascular disorders, asthma and liver fibrosis (26, 49, 50). Moreover, in patients with asthma MFAP4 levels in serum were increased (50). SLE is a systemic autoimmune disease with various organ involvement. More data is required on the effects of different disease manifestations on MFAP4 levels. One may also argue that CSF reflects CNS pathology in a more direct and specific way compared to serum. We acknowledge the need to confirm the results in a prospective preferably multicenter study with longitudinal follow-up and with paired CSF and serum samples taken prior to treatment.
In conclusion, this study points to a potential role for MFAP4 in NPSLE additionally correlated with markers of BBB disruption and proinflammatory cytokines, suggesting that MFAP4 is a marker of inflammation and vascular re-modelling. Furthermore, data show that MFAP4 may act as a marker for tissue damage in CNS in line with NfL and GFAP in NPSLE with CNS involvement. These findings may contribute to the understanding of the pathogenesis of SLE as well as NPSLE. Further studies, preferably longitudinal, multicenter and with multiple ethnicities, on MFAP4 are warranted to validate the value of MFAP4 as a potential biomarker for NPSLE and SLE.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Regional Southern of Denmark. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MW: Investigation, Methodology, Formal Analysis, Data curation, Writing – original draft. SM: Data curation, Formal Analysis, Methodology, Software, Writing – review & editing. MO: Methodology, Formal Analysis, Writing – review & editing, Investigation. JM: Formal Analysis, Investigation, Writing – review & editing, Methodology. GS: Formal Analysis, Investigation, Methodology, Writing – review & editing, Data curation. AV: Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing, Software, Supervision. NA: Formal Analysis, Investigation, Methodology, Supervision, Writing – review & editing, Conceptualization, Funding acquisition, Validation.
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the Danish Rheumatism Association (R193-A6886, R196-A6887).
We would like to thank for guidance and collaboration, Søren Lillevang for ensuring healthy controls for the study, Tine Drud Lüttge Rasmussen, Cancer and Inflammation Research at the Department of Molecular Medicine, University of Southern Denmark, and Dorte Aalund Olsen, Department of Biochemistry & Immunology, Vejle Hospital, for assistance in analysis of biomarkers.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/flupu.2024.1386256/full#supplementary-material
1. Liu Z, Davidson A. Taming lupus-a new understanding of pathogenesis is leading to clinical advances. Nat Med. (2012) 18(6):871–82. doi: 10.1038/nm.2752
2. Duarte-Delgado NP, Vásquez G, Ortiz-Reyes BL. Blood-brain barrier disruption and neuroinflammation as pathophysiological mechanisms of the diffuse manifestations of neuropsychiatric systemic lupus erythematosus. Autoimmun Rev. (2019) 18(4):426–32. doi: 10.1016/j.autrev.2018.12.004
3. Crow MK. Pathogenesis of systemic lupus erythematosus: risks, mechanisms and therapeutic targets. Ann Rheum Dis. (2023) 82(8):999–1014. doi: 10.1136/ard-2022-223741
4. Hermansen ML, Lindhardsen J, Torp-Pedersen C, Faurschou M, Jacobsen S. Incidence of systemic lupus erythematosus and lupus nephritis in Denmark: a nationwide cohort study. J Rheumatol. (2016) 43(7):1335–9. doi: 10.3899/jrheum.151221
5. Carter EE, Barr SG, Clarke AE. The global burden of SLE: prevalence, health disparities and socioeconomic impact. Nat Rev Rheumatol. (2016) 12(10):605–20. doi: 10.1038/nrrheum.2016.137
6. Relle M, Weinmann-Menke J, Scorletti E, Cavagna L, Schwarting A. Genetics and novel aspects of therapies in systemic lupus erythematosus. Autoimmun Rev. (2015) 14(11):1005–18. doi: 10.1016/j.autrev.2015.07.003
7. Bennett L, Palucka AK, Arce E, Cantrell V, Borvak J, Banchereau J, et al. Interferon and granulopoiesis signatures in systemic lupus erythematosus blood. J Exp Med. (2003) 197(6):711–23. doi: 10.1084/jem.20021553
8. Schwartz N, Stock AD, Putterman C. Neuropsychiatric lupus: new mechanistic insights and future treatment directions. Nat Rev Rheumatol. (2019) 15(3):137–52. doi: 10.1038/s41584-018-0156-8
9. ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature. The American college of rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. (1999) 42(4):599–608. doi: 10.1002/1529-0131(199904)42:4%3C599::AID-ANR2%3E3.0.CO;2-F
10. Borowoy AM, Pope JE, Silverman E, Fortin PR, Pineau C, Smith CD, et al. Neuropsychiatric lupus: the prevalence and autoantibody associations depend on the definition: results from the 1000 faces of lupus cohort. Semin Arthritis Rheum. (2012) 42(2):179–85. doi: 10.1016/j.semarthrit.2012.03.011
11. Unterman A, Nolte JE, Boaz M, Abady M, Shoenfeld Y, Zandman-Goddard G. Neuropsychiatric syndromes in systemic lupus erythematosus: a meta-analysis. Semin Arthritis Rheum. (2011) 41(1):1–11. doi: 10.1016/j.semarthrit.2010.08.001
12. Hanly JG, Kozora E, Beyea SD, Birnbaum J. Review: nervous system disease in systemic lupus erythematosus: current Status and future directions. Arthritis Rheumatol. (2019) 71(1):33–42. doi: 10.1002/art.40591
13. Deijns SJ, Broen JCA, Kruyt ND, Schubart CD, Andreoli L, Tincani A, et al. The immunologic etiology of psychiatric manifestations in systemic lupus erythematosus: a narrative review on the role of the blood brain barrier, antibodies, cytokines and chemokines. Autoimmun Rev. (2020) 19(8):102592. doi: 10.1016/j.autrev.2020.102592
14. Rönnblom L. The type 1 interferon system in the etiopathogenesis of autoimmune diseases. Upsala J Med Sci. (2011) 116:227–37. doi: 10.3109/03009734.2011.624649
15. Hirohata S, Kikuchi H. Role of Serum IL-6 in neuropsychiatric systemic lupus erythematosus. ACR Open Rheumatol. (2021) 3(1):42–9. doi: 10.1002/acr2.11217
16. Moore E, Huang MW, Putterman C. Advances in the diagnosis, pathogenesis and treatment of neuropsychiatric systemic lupus erythematosus. Curr Opin Rheumatol. (2020) 32(2):152–8. doi: 10.1097/BOR.0000000000000682
17. Mackay M, Vo A, Tang CC, Small M, Anderson EW, Ploran EJ, et al. Metabolic and microstructural alterations in the SLE brain correlate with cognitive impairment. JCI Insight. (2019) 4(1):e124002. doi: 10.1172/jci.insight.124002
18. Trysberg E, Nylen K, Rosengren LE, Tarkowski A. Neuronal and astrocytic damage in systemic lupus erythematosus patients with central nervous system involvement. Arthritis Rheum. (2003) 48(10):2881–7. doi: 10.1002/art.11279
19. Tjensvoll AB, Lauvnes MB, Zetterberg H, Kvaløy JT, Kvivik I, Maroni SS, et al. Neurofilament light is a biomarker of brain involvement in lupus and primary Sjögren’s syndrome. J Neurol. (2021) 268(4):1385–94. doi: 10.1007/s00415-020-10290-y
20. Wulf-Johansson H, Lock Johansson S, Schlosser A, Trommelholt Holm A, Rasmussen LM, Mickley H, et al. Localization of microfibrillar-associated protein 4 (MFAP4) in human tissues: clinical evaluation of serum MFAP4 and its association with various cardiovascular conditions. PLoS One. (2013) 8(12):e82243. doi: 10.1371/journal.pone.0082243
21. Pilecki B, Holm AT, Schlosser A, Moeller JB, Wohl AP, Zuk AV, et al. Characterization of microfibrillar-associated protein 4 (MFAP4) as a tropoelastin- and fibrillin-binding protein involved in elastic fiber formation. J Biol Chem. (2016) 291(3):1103–14. doi: 10.1074/jbc.M115.681775
22. Kanaan R, Medlej-Hashim M, Jounblat R, Pilecki B, Sorensen GL. Microfibrillar-associated protein 4 in health and disease. Matrix Biol. (2022) 111:1–25. doi: 10.1016/j.matbio.2022.05.008
23. Kasamatsu S, Hachiya A, Fujimura T, Sriwiriyanont P, Haketa K, Visscher MO, et al. Essential role of microfibrillar-associated protein 4 in human cutaneous homeostasis and in its photoprotection. Sci Rep. (2011) 1:164. doi: 10.1038/srep00164
24. Kielty CM, Sherratt MJ, Shuttleworth CA. Elastic fibres. J Cell Sci. (2002) 115(Pt 14):2817–28. doi: 10.1242/jcs.115.14.2817
25. Holm AT, Wulf-Johansson H, Hvidsten S, Jorgensen PT, Schlosser A, Pilecki B, et al. Characterization of spontaneous air space enlargement in mice lacking microfibrillar-associated protein 4. Am J Physiol Lung Cell Mol Physiol. (2015) 308(11):L1114–24. doi: 10.1152/ajplung.00351.2014
26. Madsen BS, Thiele M, Detlefsen S, Sørensen MD, Kjaergaard M, Møller LS, et al. Prediction of liver fibrosis severity in alcoholic liver disease by human microfibrillar-associated protein 4. Liver Int. (2020) 40(7):1701–12. doi: 10.1111/liv.14491
27. Samadzadeh S, Olesen MN, Wirenfeldt M, Möller S, Misu T, Soelberg K, et al. Microfibrillar-associated protein as a potential marker of acute relapse in inflammatory demyelinating diseases of the central nervous system: pathological and clinical aspects. Mult Scler. (2023) 29(14):1721–35. doi: 10.1177/13524585231200720
28. Voss A, Green A, Junker P. Systemic lupus erythematosus in Denmark: clinical and epidemiological characterization of a county-based cohort. Scand J Rheumatol. (1998) 27(2):98–105. doi: 10.1080/030097498440958
29. Laustrup H, Voss A, Green A, Junker P. Occurrence of systemic lupus erythematosus in a Danish community: an 8-year prospective study. Scand J Rheumatol. (2009) 38(2):128–32. doi: 10.1080/03009740802419073
30. Asgari N, Jarius S, Laustrup H, Skejoe HP, Lillevang ST, Weinshenker BG, et al. Aquaporin-4-autoimmunity in patients with systemic lupus erythematosus: a predominantly population-based study. Mult Scler. (2018) 24(3):331–9. doi: 10.1177/1352458517699791
31. Fries JF, Holman HR. Systemic lupus erythematosus: a clinical analysis. Major Probl Intern Med. (1975) 6:v-199.1177502
32. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. (1982) 25(11):1271–7. doi: 10.1002/art.1780251101
33. Hochberg MC. Updating the American college of rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. (1997) 40(9):1725. doi: 10.1002/art.1780400928
34. Panush RS, Greer JM, Morshedian KK. What is lupus? What is not lupus? Rheum Dis Clin North Am. (1993) 19(1):223–34. doi: 10.1016/S0889-857X(21)00178-2
35. Hanly JG. Diagnosis and management of neuropsychiatric SLE. Nat Rev Rheumatol. (2014) 10(6):338–47. doi: 10.1038/nrrheum.2014.15
36. Gladman DD, Ibañez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29(2):288–91. PMID: 11838846.11838846
37. Stoll T, Stucki G, Gordon C, Isenberg DA. A damage index for lupus patients–where are we now? Lupus. (1997) 6(3):219–22. doi: 10.1177/096120339700600301
38. Dayal NA, Gordon C, Tucker L, Isenberg DA. The SLICC damage index: past, present and future. Lupus. (2002) 11(4):261–5. doi: 10.1191/0961203302lu190sa
39. Aziz N, Detels R, Quint JJ, Li Q, Gjertson D, Butch AW. Stability of cytokines, chemokines and soluble activation markers in unprocessed blood stored under different conditions. Cytokine. (2016) 84:17–24. doi: 10.1016/j.cyto.2016.05.010
40. Vignali DA. Multiplexed particle-based flow cytometric assays. J Immunol Methods. (2000) 243(1-2):243–55. doi: 10.1016/S0022-1759(00)00238-6
41. Wilson DH, Rissin DM, Kan CW, Fournier DR, Piech T, Campbell TG, et al. The simoa HD-1 analyzer: a novel fully automated digital immunoassay analyzer with single-molecule sensitivity and multiplexing. J Lab Autom. (2016) 21(4):533–47. doi: 10.1177/2211068215589580
42. Rissin DM, Kan CW, Campbell TG, Howes SC, Fournier DR, Song L, et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat Biotechnol. (2010) 28(6):595–9. doi: 10.1038/nbt.1641
43. Baeten KM, Akassoglou K. Extracellular matrix and matrix receptors in blood-brain barrier formation and stroke. Dev Neurobiol. (2011) 71(11):1018–39. doi: 10.1002/dneu.20954
44. Schlosser A, Pilecki B, Hemstra LE, Kejling K, Kristmannsdottir GB, Wulf-Johansson H, et al. MFAP4 promotes vascular smooth muscle migration, proliferation and accelerates neointima formation. Arterioscler Thromb Vasc Biol. (2016) 36(1):122–33. doi: 10.1161/ATVBAHA.115.306672
45. Alghisi GC, Ponsonnet L, Rüegg C. The integrin antagonist cilengitide activates alphaVbeta3, disrupts VE-cadherin localization at cell junctions and enhances permeability in endothelial cells. PLoS One. (2009) 4(2):e4449. doi: 10.1371/journal.pone.0004449
46. Modrego J, López-Farré AJ, Martínez-López I, Muela M, Macaya C, Serrano J, et al. Expression of cytoskeleton and energetic metabolism-related proteins at human abdominal aortic aneurysm sites. J Vasc Surg. (2012) 55(4):1124–33. doi: 10.1016/j.jvs.2011.10.033
47. de la Cuesta F, Alvarez-Llamas G, Maroto AS, Donado A, Zubiri I, Posada M, et al. A proteomic focus on the alterations occurring at the human atherosclerotic coronary intima. Mol Cell Proteomics. (2011) 10(4):M110.003517. doi: 10.1074/mcp.M110.003517
48. Crispín JC, Liossis SN, Kis-Toth K, Lieberman LA, Kyttaris VC, Juang YT, et al. Pathogenesis of human systemic lupus erythematosus: recent advances. Trends Mol Med. (2010) 16(2):47–57. doi: 10.1016/j.molmed.2009.12.005
49. Hemstra LE, Schlosser A, Lindholt JS, Sorensen GL. Microfibrillar-associated protein 4 variation in symptomatic peripheral artery disease. J Transl Med. (2018) 16(1):159. doi: 10.1186/s12967-018-1523-6
Keywords: systemic lupus erythematosus, neuropsychiatric SLE, inflammation, microfibrillar-associated protein 4, accumulated disease damage
Citation: Wegener MAB, Möller S, Olesen MN, Madsen JS, Sorensen GL, Voss A and Asgari N (2024) Microfibrillar-associated protein 4 interaction with inflammation and clinical characteristics in neuropsychiatric systemic lupus erythematosus. Front. Lupus 2:1386256. doi: 10.3389/flupu.2024.1386256
Received: 14 February 2024; Accepted: 29 April 2024;
Published: 14 May 2024.
Edited by:
Luís Pedro Sousa Inês, Coimbra Hospital and University Center, PortugalReviewed by:
Rahul Kakalij, University of Nebraska Medical Center, United States© 2024 Wegener, Möller, Olesen, Madsen, Sorensen, Voss and Asgari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nasrin Asgari, bmFzZ2FyaUBoZWFsdGguc2R1LmRr
†Present Address: Mads Nikolaj Olesen, Lundbeck A/S, Copenhagen, Denmark
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.