 Bodo Sahondra Randrianasolo1†
Bodo Sahondra Randrianasolo1† Karoline Jøker2†
Karoline Jøker2† Louise Thomsen Schmidt Arenholt2,3,4
Louise Thomsen Schmidt Arenholt2,3,4 Tiana Onintsoa Oliva Rabozakandraina1
Tiana Onintsoa Oliva Rabozakandraina1 Charles Emile Ramarokoto1
Charles Emile Ramarokoto1 Dorthe Brønnum1
Dorthe Brønnum1 Martin Jensen5
Martin Jensen5 Søren Lundbye Christensen5
Søren Lundbye Christensen5 Jørgen Skov Jensen6
Jørgen Skov Jensen6 Paul Corstjens7
Paul Corstjens7 Govert J. van Dam8
Govert J. van Dam8 Noriko Kobayashi9,10
Noriko Kobayashi9,10 Shinjiro Hamano9,10
Shinjiro Hamano9,10 Peter Derek Christian Leutscher2,4*
Peter Derek Christian Leutscher2,4*- 1Association K’OLO VANONA, Antananarivo, Madagascar
- 2Centre for Clinical Research, Hjoerring, North Denmark Regional Hospital, Hjoerring, Denmark
- 3Department of Gynaecology and Obstetrics, North Denmark Regional Hospital, Hjoerring, Denmark
- 4Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
- 5Research Data and Biostatistics, Aalborg University Hospital, Aalborg, Denmark
- 6Research Unit for Reproductive Microbiology, Bacteria, Parasites and Fungi, Statens Serum Institut, Copenhagen, Denmark
- 7Department of Cell and Chemical Biology, Leiden University Medical Centre, Leiden, Netherlands
- 8Department of Parasitology, Leiden University Medical Centre, Leiden, Netherlands
- 9Department of Parasitology, Institute of Tropical Medicine (NEKKEN), Nagasaki University, Nagasaki, Japan
- 10Graduate School of Biomedical Sciences, Nagasaki University, Nagasaki, Japan
Background: Although a variety of different gynecological manifestations have been reported in women with female genital schistosomiasis (FGS), causality remains to be established. This study aimed to evaluate the gynecological manifestations in women with FGS in accordance with the status of Schistosoma biomarkers, sexually transmitted infections (STIs), and bacterial vaginosis (BV).
Methods: The study was conducted in an endemic Schistosoma haematobium (Sh) area in northern Madagascar in conjunction with a randomized controlled trial investigating the effects and safety of a praziquantel repeated-dosing regimen for women with FGS-associated cervical lesions. Urogenital complaints, pelvic exam abnormalities, and cervical lesion types were assessed in relation to cervicovaginal Schistosoma DNA, circulating anodic antigen (CAA) in serum, and urinary Sh egg count, in addition to STIs and BV.
Results: Among the included 116 women with a median of 26 years (range 15 to 35), the distribution of Schistosoma DNA and CAA outcomes, specified as either positive (+) or negative (-), were as follows: +/+ (18.1%), +/- (0%), -/+ (58.6%), and -/- (23.3%). Of the three Schistosoma biomarkers, only Schistosoma DNA and the urogenital complaint of blood in the urine were significantly associated. None of the biomarkers were significantly associated with pelvic exam abnormalities or cervical lesions. Sixty women (52.6%) were diagnosed with STIs and/or BV. A positive status was not significantly associated with any of the gynecological manifestations, except BV and homogeneous yellow sandy patches.
Conclusion: It remains uncertain whether biomarkers such as cervicovaginal Schistosoma DNA, serum CAA, and Schistosoma eggs in urine adequately cover the full spectrum of gynecological manifestations reported in women with FGS, including urogenital complaints, pelvic exam abnormalities, and cervical lesions. Moreover, it seems difficult to determine the origin of the different manifestations due to the common co-existence of STIs and/or BV as potential confounders.
Introduction
Female genital schistosomiasis (FGS) is a highly prevalent but often underdiagnosed condition, primarily affecting adolescent girls and younger women in sub-Saharan Africa in areas where the waterborne Schistosoma parasite is endemic (1–3). FGS affects the reproductive organs and can lead to a range of signs and symptoms closely mimicking those of sexually transmitted infections (STIs), making accurate diagnosis challenging (4). Several factors contribute to the difficulty in differentiating FGS from STIs and other gynecological conditions affecting reproductive health in adolescent girls and younger women.
Symptoms reported by adolescent girls and younger women with FGS, such as vaginal discharge, lower abdominal pain, and abnormal vaginal bleeding, resemble those of STIs such as trichomonas, gonorrhea, chlamydia, and genital herpes, as well as bacterial vaginosis (BV). This overlap in symptoms often leads to misdiagnosis or delayed diagnosis, as healthcare providers may initially focus on treating or testing for STIs and BV. A recent study conducted in South Africa showed that more than 88% of sexually active women included had one or more STIs or BV, whereas 22.5% had FGS (4). The study also demonstrated that not only do FGS and STIs coexist but there is a tendency toward a higher prevalence of STIs and BV among women also diagnosed with FGS.
Egg-induced cervicovaginal lesions observed in adolescent girls and younger women, such as sandy patches and abnormal blood vessels, in addition to cervicovaginal bleeding in conjunction with the friable mucosal surface, can be mistaken for cervical dysplasia or pre-cancerous changes in the cervix and vice versa (5). The connection between FGS, HPV, and cervical cancer requires further exploration. While a study identified an association between FGS and VIA positivity, another found no correlation between FGS and HPV positivity (5, 6).
Different testing modalities may assist the diagnosis of FGS beyond the symptoms reported by the women and the abnormal findings detected in the pelvic exam. DNA originating from Schistosoma haematobium (Sh) eggs in the vaginal fluid or circulating anodic antigens (CAA) in the serum can be used to indicate FGS in an active disease stage (7, 8). These tests are not always readily available in endemic regions and lack adequate sensitivity and specificity (1, 2, 9). A few studies show that genital self-sampling and following PCR analysis for Schistosoma haematobium DNA may provide a useful, more accessible, and scalable diagnostic tool (10, 11). Histological examination of cervical biopsies from women with FGS typically shows Schistosoma ova surrounded by inflammatory cells. However, this former diagnostic approach is today considered inappropriate due to its invasive nature and increased risk of HIV transmission in the period after taking the biopsy (12, 13).
In spite of the diagnostic challenges being encountered currently, more clinical studies of women with FGS are still needed, with the overall objective of establishing a more robust level of knowledge about the gynecological manifestations being reported and observed in women living in endemic schistosomiasis areas. This knowledge is essential for the further development of evidence-based clinical guidelines in the management of the different manifestations affecting the women. In line with this objective, the aim of this study was to assess urogenital complaints, pelvic exam abnormalities, and cervical lesions in women with FGS living in Madagascar with reference to the panel of Schistosoma biomarkers, in addition to STI pathogens and BV.
Materials and methods
The study was conducted in conjunction with a randomized controlled trial (RCT) investigating the effect and safety of a praziquantel (PZQ) repeated-dosing regimen in women with FGS living in an endemic S. haematobium area in Madagascar (14). The study has been registered on ClinicalTrials.gov under the identifier NCT04115072. The primary ethnic group and language spoken was Sakalava Malagasy. Women from Antsakoamanondro and Antranokarany villages were invited to the local clinic for screening. The inclusion criteria in the RCT were age 15–35 years, with current urogenital complaints and at least one FGS-associated cervical lesion observed during a pelvic exam. Exclusion criteria included virginity, pregnancy, certain medical histories, and recent PZQ treatment. Participation required informed consent. The protocol involved a medical interview, a pelvic exam, and specimen collection. PZQ treatment was administrated at baseline, with one arm receiving additional doses 12 and 24 h after the initial dose, along with subsequent doses after 5 and 10 weeks, and the other arm only received the baseline dose. Both arms were followed up at weeks 5, 10, and 15, although for this study, only data from baseline were analyzed.
Medical interview and pelvic exam
A medical interview and pelvic exam were conducted at baseline (14). Semi-structured questionnaires were used to systematically obtain information from the women about urogenital complaints. To pinpoint FGS-related conditions, we extensively reviewed the literature, selecting only those complaints directly associated with FGS, reported in at least two studies with representative samples. For publication, Sakalava complaints were translated into French using layman’s terms, then literally translated into English.
The following abnormalities were searched for in conjunction with the pelvic exam: bleeding, epithelial disruption (erosions, ulcerations, and/or a friable cervical surface), and tenderness of the cervix, uterus, and adnexa, respectively. Furthermore, a high-resolution Canon EOS M50 camera, equipped with a 100 mm macro-lens and a circular LED light, was used to closely examine FGS-associated lesions. Images of the lesions were captured with autofocus, positioned approximately 30 cm from the cervix. The highest-quality image from each visit was selected for review. These digital images were stored in the REDCap data management system hosted by the North Denmark Regional Hospital.
The digital gridded imaging technique was applied to evaluate images of the cervix for cervical lesion proportion (CLP), grainy sandy patches proportion (GSP), homogenous sandy patches proportion (HSP), abnormal blood vessels proportion (BVP), and rubbery papules count (RPC) (15, 16). Each image had a semi-transparent grid of 424 squares placed over it, with squares containing any FGS-associated lesions manually marked. The marked squares were automatically counted and converted into a percentage, representing the total CLP. Specific lesion types, such as HSP, GSP, and BVP, were also calculated as percentages, whereas RPC was counted as a number.
Laboratory analyses
Various laboratory tests were conducted, encompassing serum CAA, cervicovaginal S. haematobium DNA, and urinary egg count. S. haematobium DNA was measured in vaginal lavage and cervical swab tests. Genomic DNA was extracted from 200 µl of cervical swabs and vaginal lavage fluid using a QIAamp DNA Mini Kit (Qiagen, Germany). The Up-Converting reporter Particle Lateral Flow test was employed to detect CAA. Serum samples underwent testing in SCAA20 and SCAA500 formats, with 20 µl and 500 µl of serum, respectively. Results were expressed as pg CAA/ml serum, with concentrations exceeding 1 pg/ml deemed positive (17). Morning urine samples were collected and filtered through a 14 µm polycarbonate membrane with a volume of 50 ml to detect the presence of S. haematobium eggs. The results, indicating the number of eggs per 50 ml, were evaluated at baseline (18).
Moreover, STI pathogens were also investigated, including Trichomonas vaginalis, Chlamydia trachomatis, Mycoplasma genitalium, and Neisseria gonorrhoea, in addition to BV assessed by detecting abnormal vaginal microbiota. Cervicovaginal swabs were collected in 2 ml of Copan eNat using a regularly flocked swab. Specimens were stored at ambient temperature for less than 12 h before being transferred to −80°C. DNA extraction was performed using 200 µl of the collected swab specimen on a MagNAPure instrument following the Pathogen Universal 200 MagNA Pure protocol. Real-time PCRs were conducted with 5 µl of extracted DNA, each including an internal control for inhibition. Primers targeting the 16S rRNA gene were used for C. trachomatis detection (19), and the N. gonorrhoeae assay targeted the porA pseudogene using a modified TaqMan probe (20). Positive samples were confirmed using an assay targeting the opa gene (21). The T. vaginalis assay targeted a specific repeat sequence, with positive results confirmed by repeating the PCR (22). M. genitalium was detected using primers and probes targeting the major MgPa adhesin (23). BV was diagnosed using a combined assay that detects abnormal vaginal microbiota, including Fannyhessea vaginae (also known as Atopopium vaginae) and Gardnerella species, as described previously. Detection thresholds were set at 10,000 geq/µl template for F. vaginae and 100,000 geq/µl template for Gardnerella spp (24).
Ethics
This study adhered to the principles outlined in the Declaration of Helsinki and followed the Guidelines for Good Clinical Practice. Ethical approval was obtained from the Ethics Committee at the Ministry of Health in Antananarivo (Authorization Number: 098-MSANP/CERBM; Number: 059-MSANP/CERBM; Number: 065 MSANP/SG/-AGMED/CNPV/CERBM).
Data management
Data were entered into the Research Electronic Data Capture (REDCap 13.1.37) system, hosted on the virtual server of the Northern Denmark Regional Hospital. The local team entered the data collected at the investigation site in Madagascar into REDCap. The Danish research team entered additional data obtained from reference laboratory sites into the same server. To ensure data quality, a systematic approach was employed where 10% of the data entries were randomly selected for verification. Access to the database required a personal username and password, with all changes automatically logged. The stored data were accessible only for the authorized team members. Data handling adhered to the data safety and privacy regulations outlined in the General Data Protection Regulation (GDPR) and the Danish Data Protection Act.
Statistics
Analyses were conducted on data from only the baseline visit of the RCT study. Continuous data were described as median [interquartile range (IQR)] and compared among subgroups using the Mann–Whitney U test. Categorical data were described as the number (n) and percentage of patients (%), respectively, and compared between subgroups using Fisher’s exact test. All calculations were carried out using SPSS (IBM SPSS Statistics 29.0.0.0, version 241). P-values <0.05 were considered significant. Owing to the risk of type 1 errors (false positives), Bonferroni correction was additionally calculated, in which all the p-values were multiplied by the number of p-values within a table.
Results
Out of 320 women screened for eligibility to participate in the RCT, 184 were excluded due to the absence of FGS-associated lesions and 20 were excluded due to declining participation or other reasons. Hence, baseline data were evaluated among the 116 women (36.3%) recruited for the RCT. The median age was 26 years (IQR 12; range 15 to 35).
Gynecological manifestations
The most frequently reported urogenital complaint among the 116 women at baseline was lower abdominal pain (56.0%), followed by smelly vaginal discharge (50.9%), itching of the vulva/vagina (50.0%), and pain during sexual intercourse (42.2%). In addition, more than one-third of the women had an abnormal vaginal discharge color, irregular menstruation, and painful micturition (Figure 1).
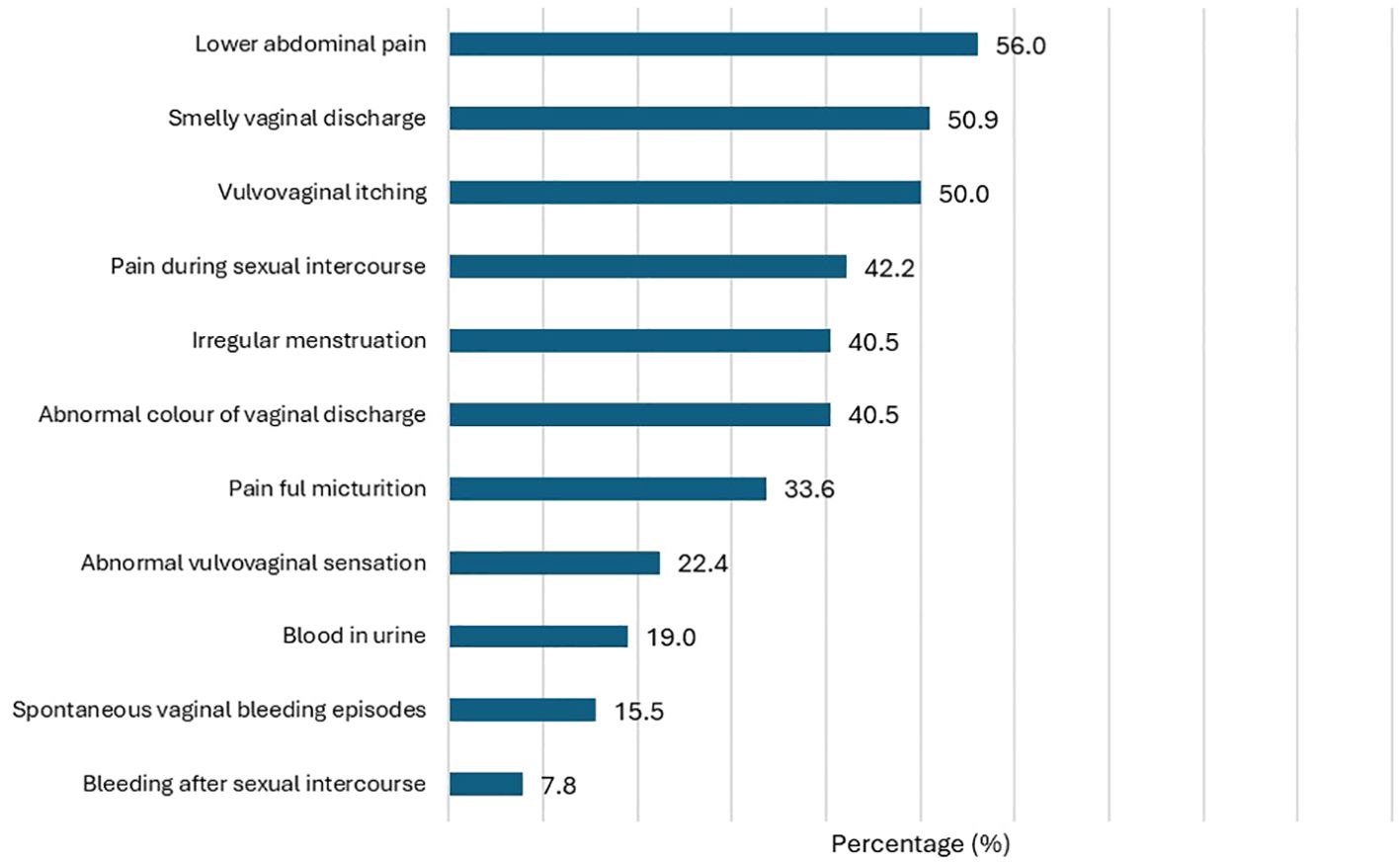
Figure 1. Distribution of urogenital complaints in the study population (N=116).
Cervicovaginal bleeding upon instrumental contact during the pelvic exam was observed in 45 of the 116 women (38.8%), whereas spontaneous bleeding was observed in 7 women (6.0%). Moreover, epithelial disruption was observed in 9 women (7.8%). Forty-seven women (40.5%) reported cervical motion, uterine, and/or adnexal tenderness during the pelvic exam (Figure 2).
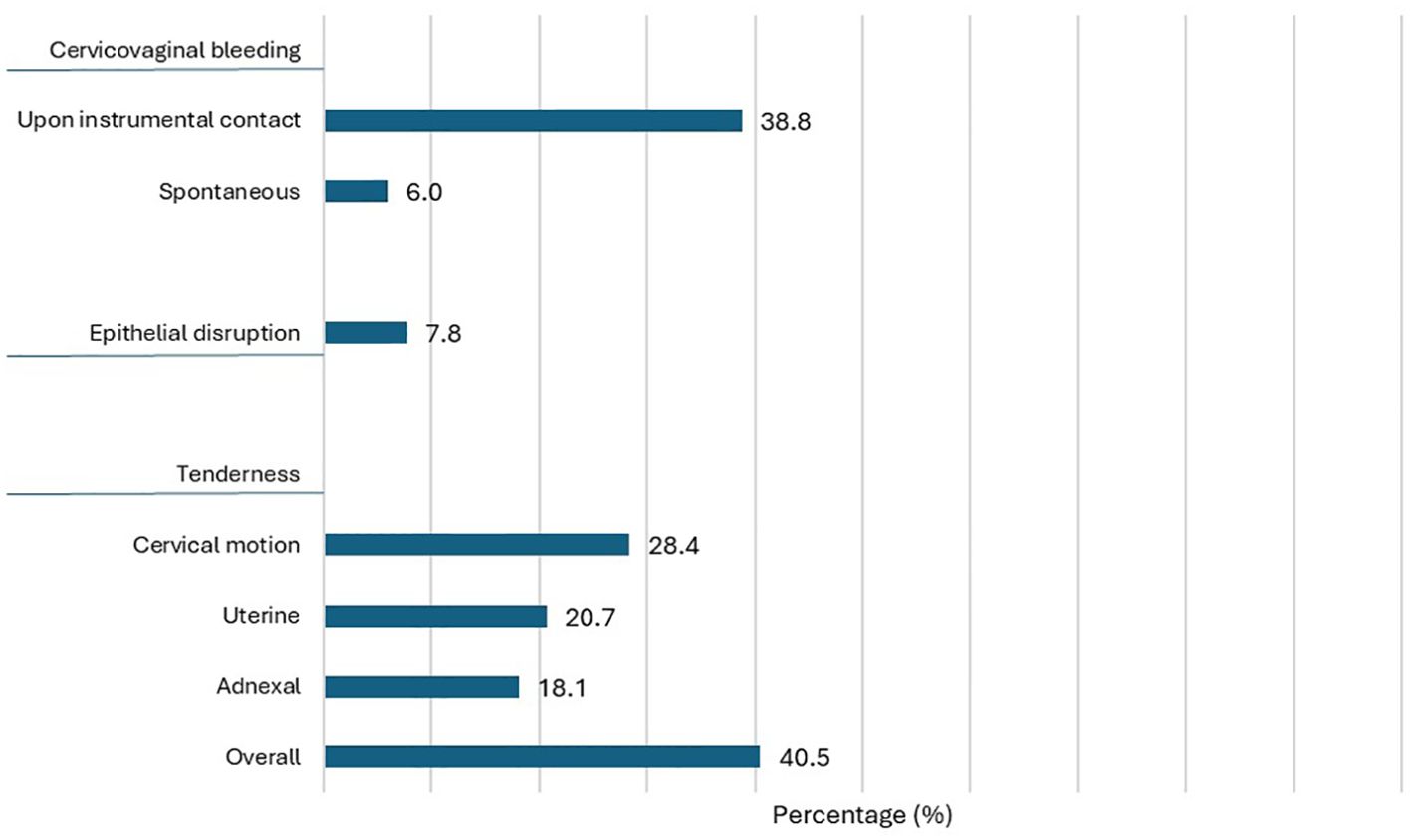
Figure 2. Distribution of pelvic exam abnormalities in the study population (N=116).
At baseline, grainy sandy patches were found in 100% of the 116 women, homogenous yellow sandy patches in 85.7%, abnormal blood vessels in 95.5%, and rubbery papules in 92.9%. The median CLP was 19.8 (IQR 18.2), followed by a median GSP of 17.6 (IQR 13.9), a median HSP of 3.5 (IQR 10.5), and a median BVP of 7.6 (IQR 13.2), in addition to a median RPC of 4.5 (IQR 6.0) (Table 1).
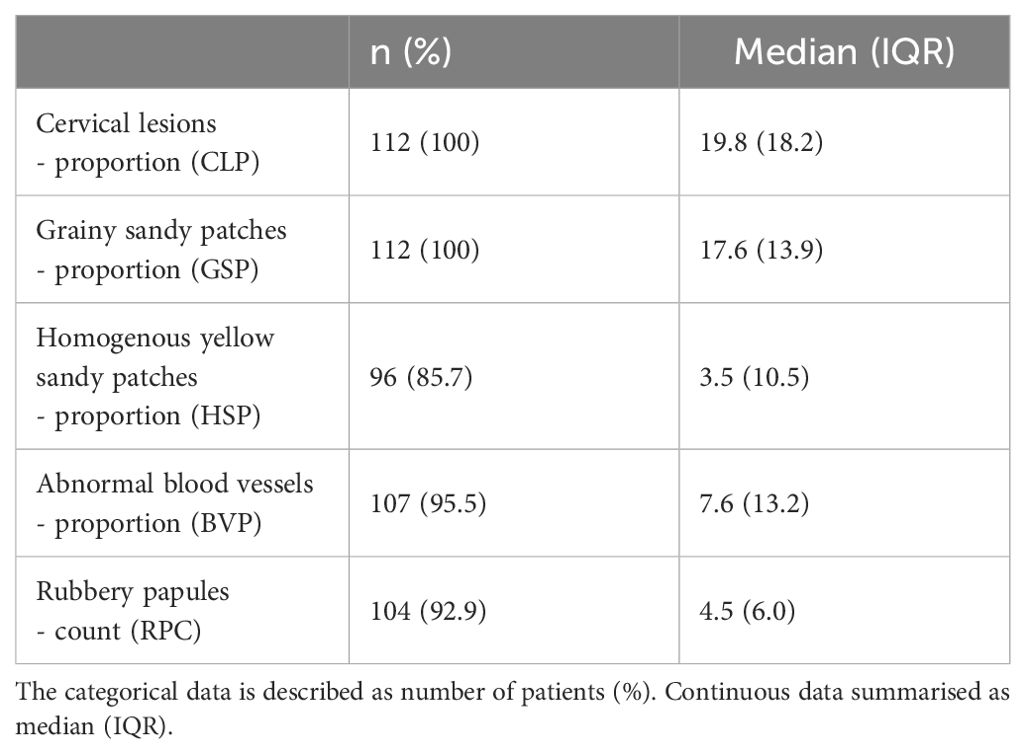
Table 1. Cervical lesions in the study population (N=112).
Coexistence of gynecological manifestations
Different pelvic exam abnormalities were significantly associated with urogenital complaints, including epithelial disruption [smelly vaginal discharge (p=0.03) and abnormally discolored vaginal discharge (p<0.01)] and gynecological tenderness [lower abdominal pain (p<0.001), smelly vaginal discharge (p<0.001), vulvovaginal itching (p<0.01), abnormal vaginal discharge color (p=0.004), painful micturition (p<0.01), and abnormal vulvovaginal sensation (p<0.01)]. However, when applying the Bonferroni correction, gynecological tenderness (uterine and cervical motion specifically) only remained significantly associated with lower abdominal pain (p<0.001) and painful micturition (p<0.001) (Supplementary Table 1A). None of the cervical lesion parameters were significantly associated with any of the reported urogenital complaints, except for a higher mean rank GSP among women with lower abdominal pain and blood in urine, in comparison with women without these urogenital complaints (p<0.01 and p=0.02, respectively) (Supplementary Table 1B). None of the trends were significant when applying the Bonferroni correction.
In the group of 45 women observed with bleeding upon instrumental contact during the pelvic exam, the mean rank HSP was statistically higher than in women without this abnormality (p<0.01) (Supplementary Table 1C). In the group of seven women observed with spontaneous bleeding during the pelvic exam, the mean rank GSP was significantly lower than in women without this abnormality (p<0.001). Moreover, mean rank HSP tended to be higher in women with epithelial disruption than in women without this abnormality (p=0.07). Finally, higher HSP and RPC mean ranks were observed in women who had reported uterine tenderness during the pelvic exam (p=0.01 and p=0.04, respectively). However, upon application of the Bonferroni correction, all the associations were no longer significant.
Cervicovaginal Schistosoma DNA, serum CAA, and eggs in urine
Cervicovaginal Schistosoma DNA was detected in 21 of the 116 (18.1%) women and serum CAA in 89 (76.9%), with a median level of 342.4 pg/ml (IQR 1019.1). S. haematobium eggs were detected in the urine of 86 women (74.1%), with a median count of 8.0 (IQR 62.0).
The distributions of Schistosoma DNA and CAA outcomes, specified as either positive (+) or negative (), were as follows: +/+ (18.1%), +/- (0%), -/+ (58.6%), and -/- (23.3%). Mean rank serum CAA level and mean rank urine egg count were significantly higher among women positive versus negative for cervicovaginal Schistosoma DNA: 451.0 pg/ml (IQR 2,015.2) versus 29.6 pg/ml (IQR 370.9), p<0.001, and 25 eggs/50 ml (IQR 78) versus two eggs/50 ml (IQR 12), p<0.01, respectively.
Among the 86 egg-positive women, 13 (11.2%) were CAA negative. Among the 21 Schistosoma DNA-positive women, 19 were egg-positive in urine and two were egg-negative. Furthermore, a significant positive correlation was observed between serum CAA level and urine egg count (rho=0.46, p<0.001).
Gynecological manifestations in relation to Schistosoma biomarkers
Table 2 presents the three categories of gynecological manifestations in accordance with outcomes of cervicovaginal Schistosoma DNA, serum CAA, and urinary egg count. Blood in urine was the only urogenital complaint positively associated with Schistosoma biomarker detection (Schistosoma DNA p<0.001, CAA p<0.01, and egg in urine p<0.01). Vulvovaginal itching was significantly associated with a urinary egg-negative status (p=0.02) (Table 3). None of the pelvic exam abnormalities were significantly associated with positive cervicovaginal Schistosoma DNA or urine egg status. Of note, uterine tenderness and overall gynecological tenderness were observed in significantly higher proportions of serum CAA-negative women than in positive women (p=0.03 and p<0.01, respectively). Cervical lesions were not associated with positive cervicovaginal Schistosoma DNA, serum CAA, or egg in urine status (Table 2). Additionally, mean BVP was significantly lower in CAA-positive women versus CAA-negative women (p=0.03). In addition, a significant negative correlation was observed between BVP and CAA serum level, as well as urinary egg count (p<0.01 and p=0.04, respectively) (Table 3). When applying the Bonferroni correction, only the association between blood in urine and serum CAA of the observed associations remained significant (Table 2).
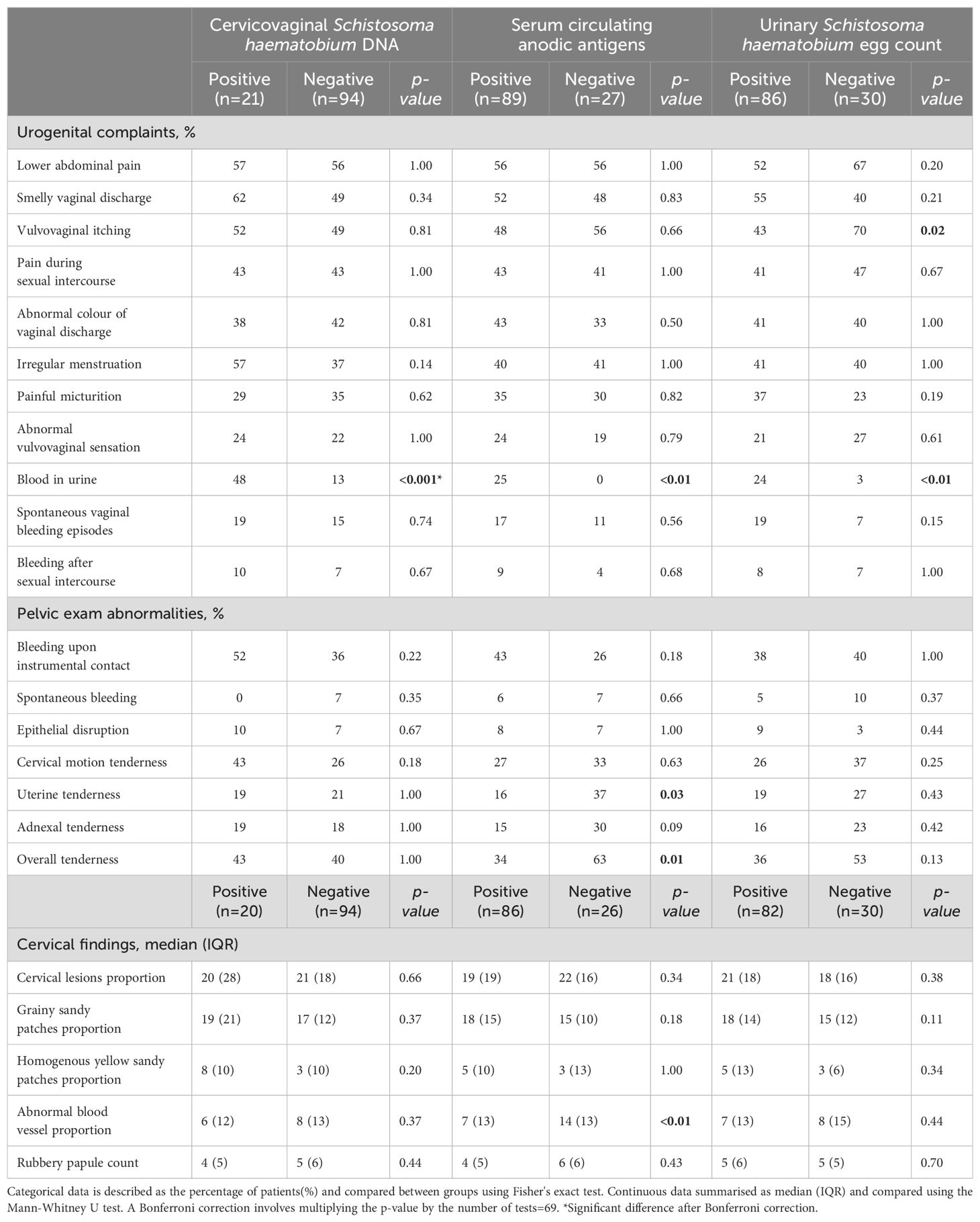
Table 2. Gynecological manifestations by Schistosoma biomarkers.
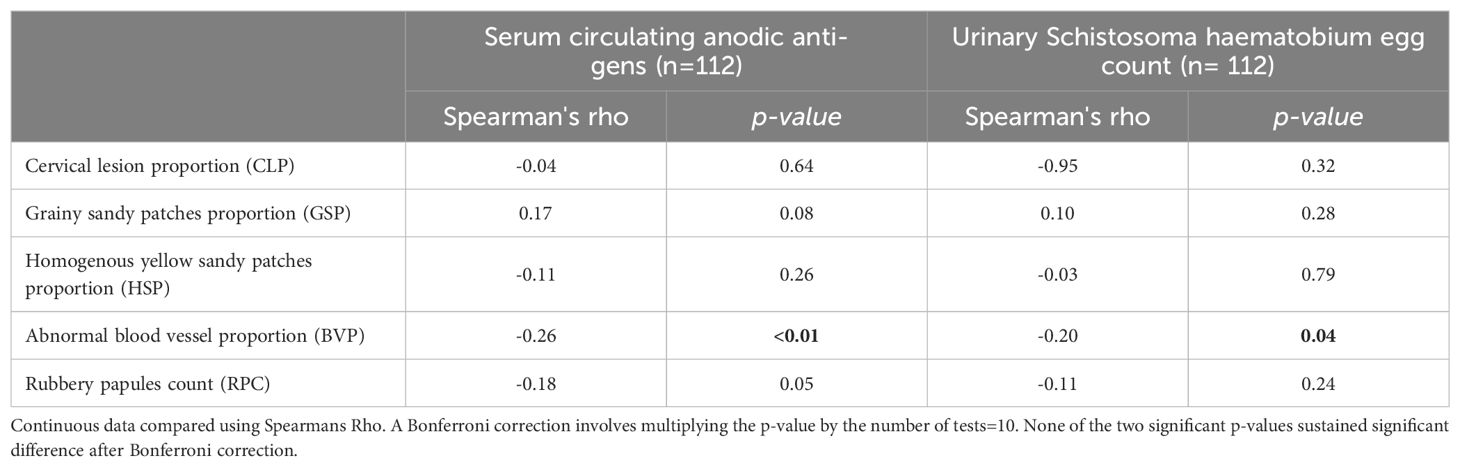
Table 3. Correlation pattern between cervical lesions and Schistosoma biomarkers.
Sexually transmitted infections and bacterial vaginosis in relation to gynecological manifestations
Sixty women (52.6%) were diagnosed with STIs and/or BV at baseline with the following distribution: T. vaginalis (27.8%), M. genitalium (13.9%), C. trachomatis (13.0%), and N. gonorrhoeae (7.8%), in addition to BV (15.8%).
T. vaginalis, C. trachomatis, and N. gonorrhoea, as well as BV, were found to be significantly associated with urogenital complaints, including smelly vaginal discharge, vulvovaginal itching, and irregular menstruation (Supplementary Table 1D). However, none of these associations remained significant after applying the Bonferroni correction. In addition, none of the pelvic exam abnormalities were found to be significantly associated with STIs and BV. Concerning cervical lesions, T. vaginalis was significantly associated with abnormal blood vessels, M. genitalium with rubbery papules, and BV with homogeneous yellow sandy patches, abnormal blood vessels, and rubbery papules.
The positive status of STIs and/or BV was not significantly associated with any of the urogenital complaints or pelvic exam abnormalities (Supplementary Table 1E). Abnormal blood vessels, as the only cervical lesion type, were marginally associated with positive STIs and/or BV status (p=0.05). Bleeding upon instrumental contact was significantly associated with overall positive STIs, BV, and/or Schistosoma biomarker detection status versus overall negative status (n=104 versus n=11). None of the listed associations remained significant after applying the Bonferroni correction, except BV and homogeneous yellow sandy patches.
Discussion
A broad spectrum of different gynecological manifestations was observed among the women with FGS. Furthermore, the manifestations occurred in very complex, and probably also interactive, patterns of urogenital complaints, pelvic exam abnormalities, and specific FGS-associated lesions, as also demonstrated in this study. FGS may, in this context, very well be considered a syndrome of different gynecological manifestations and not a narrowed condition defined merely through the detection of pathognomonic lesions and positive findings of specific Schistosoma biomarkers in the lower genital tract.
In the overall evaluation of the observed gynecological manifestations, the complaint of blood in urine came out as the only manifestation significantly associated with positive Schistosoma biomarker status. However, when applying the Bonferroni correction, only cervicovaginal Sh DNA remained significantly associated with the complaint of blood in the urine. Of interest, a pattern of significant associations between the gynecological manifestations and negative Schistosoma biomarker status was also observed in this study, including complaints of vulvovaginal itching (egg in urine), gynecological tenderness in conjunction with the pelvic exam (serum CAA), and BVP (serum CAA), although none of the manifestations remained in significant association with the biomarkers after the Bonferroni correction.
The three Schistosoma biomarkers applied in the study represent different S. haematobium infection and pathophysiological aspects in this study group of women diagnosed with FGS. Among the three biomarkers, cervicovaginal Sh DNA, as an egg biomarker, exclusively reflects S. haematobium infection activity in the lower genital tract. In this context, it was surprising that 95 (81.9%) out of the 116 women with FGS-associated cervical lesions did not have cervicovaginal Sh DNA. Moreover, it was also observed that Sh DNA neither reflects the different types of cervical lesion proportions nor the RPC level. These findings suggest that cervicovaginal Schistosoma DNA as a biomarker only partially expresses overall S. haematobium infection and pathophysiological aspects in women with FGS, even in the presence of active infection as reflected by positive CAA in the serum and egg in urine detection. The low sensitivity of the assay itself in detecting cervicovaginal Schistosoma DNA could be a possible reason for the observed discrepancy. Another reason could be that Schistosoma DNA is a biomarker of active infection. By contrast, cervical lesions are a testimonial of chronicity due to many years of S. haematobium infection since the women were girls, and therefore, are not necessarily compatible with ongoing active pathophysiology only.
As an adult worm population marker, CAA reflects the dwelling worm burden in the entire pelvic region, mainly the urinary tract system, as a proxy of infection intensity. By contrast, egg in urine reflects infection intensity in relation to the urinary tract system only. Both biomarkers were detected in significantly higher proportions (76.7% and 74.1%, respectively), than cervicovaginal Schistosoma DNA (18.1%) in the study group. Moreover, a significant positive correlation was observed between the serum CAA level and urinary egg count. Of further interest, mean rank values of the two biomarkers were significantly higher among women positive versus negative for cervicovaginal Sh DNA, which may indicate that overall S. haematobium infection intensity in the women is a major determinator of active infection level, and as a result ongoing pathophysiology, in the genital organs. As for cervicovaginal Schistosoma DNA, neither serum CAA nor egg in urine possessed supportive biomarker characteristics in evaluating the observed gynecological manifestations in the study group of women with FGS-associated cervical lesions. This finding contrasts with the findings of Nemungadi et al., who found that grainy sandy patches and abnormal blood vessels were significantly associated with CAA (24). There remains an overall challenge in interpreting the outcomes of the existing Schistosoma biomarkers when evaluating the causality of gynecological manifestations in women with FGS associated with cervical lesions.
Only a few studies have assessed the gynecological manifestations in women with FGS from a broader diagnostic approach through the inclusion of STIs in recognition that both diseases commonly coexist in endemic schistosomiasis areas (3, 4, 25–29). In line with this epidemiological tendency, this study revealed that half of the study population of women with FGS were also diagnosed with N. gonorrhoea, C. trachomatis, M. genitalium, T. vaginalis and/or BV (52.6%). The different sexually transmitted pathogens and BV. cause different gynecological manifestations, as observed in this study, such as pain in the lower abdomen and during sexual intercourse, abnormal discharge characteristics, and vaginal bleeding. From reproductive health clinical and therapeutic perspectives, it is difficult to distinguish the entities of FGS, STIs, and BV from each other, particularly with respect to the clinical interaction and patterns of contribution to the different gynecological manifestations observed among women living in endemic S. haematobium areas in sub-Saharan Africa. This situation supports the rationale for jointly addressing the three gynecological entities in an overall syndromic treatment strategy among these women.
Different limitations were encountered in this study evaluating gynecological manifestations among women with FGS-associated cervical lesions. First, the study was based on an RCT study and was therefore not powered specifically for the analyses conducted as part of the overall evaluation. Hence, the size of the study population was relatively small for performing further in-depth data investigation, including multi-regression analysis aiming to identify different levels of contribution of FGS, STIs, and BV. Second, in evaluating the gynecological manifestations, reference was made to different Schistosoma biomarkers of FGS status, including cervicovaginal Schistosoma DNA, serum CAA, and egg in urine. However, each of the three biomarkers do not seem to cover the full spectrum of S. haematobium infection and pathophysiology in the genital organs adequately, either when used separately or in combination. As a result, evaluating the causality of gynecological manifestations concerning FGS is challenged considerably. Third, the many tests performed increased the risk of type 1 errors (false positives). Arguably, the tests performed were conducted based on hypotheses of associations or correlations. However, additional Bonferroni corrected p-values were calculated per table for further critical assessment of the data. Fourth, using the digital gridded image technique for the quantitative assessment of cervical lesions only does not present the FGS-associated pathology in the lower genital tract in a complete manner to allow for more robust comparative analyses in relation to urogenital complaints and pelvic exam abnormalities. Finally, the RCT team learned that the women in the study area carefully cleaned the vulva and vagina with water regularly. This practice may have interfered with the detection rate of vaginal discharge. Furthermore, the frequency of STIs, BV, and yeast infection might have been underestimated as potential study confounders.
In conclusion, this study failed to demonstrate a statistical causality of gynecological manifestations, whether they were genital complaints or pelvic exam abnormalities in relation to FGS. Larger studies are required to fulfill the essential criteria of adequate statistical power. As a secondary study outcome, it was confirmed that adolescent girls and younger women living in endemic schistosomiasis areas are commonly affected by STIs, BV, and FGS. For that reason, distinguishing FGS from STIs and BV is also a major challenge when determining the pathophysiological etiology behind the reported urogenital complaints and observed pelvic exam abnormalities and choosing a relevant therapeutic strategy. The World Health Organization recommends the syndromic treatment approach in managing women with urogenital complaints when access to diagnostic laboratories and other healthcare facilities is limited in rural areas of sub-Saharan Africa. This approach appropriately targets STIs and other reproductive health disease-evoking agents with a one-size-fits-all rational antibiotic therapy. For women living in endemic schistosomiasis areas, the syndromic treatment strategy could be developed further by adding a single dose of PZQ regimen to the existing anti-STI antibiotic regimens.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Committee of Ethics at the Ministry of Health in Antananarivo (Comité d’Ethique de la Recherche Bio-Médicale auprès du Ministère de la Santé Publique); (Authorization Number: 098-MSANP/CERBM; Number: 059-MSANP/CERBM; Number: 065 MSANP/SG/-AGMED/CNPV/CERBM). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from all participating women (adults and minor). Since girls can be affected by FGS since pre-puberty, and life-threatening sequels of FGS may already occur at an adolescent age, we considered it unethical to exclude women 15-17-years old from the study. To respect confidentiality of these adolescent participants, the informed consent of a third party (parent or legal guardian) was not asked for. The Ethics committee approved this procedure.
Author contributions
BR: Writing – original draft, Writing – review & editing, Conceptualization, Investigation. KJ: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. LA: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. TR: Conceptualization, Investigation, Writing – review & editing. CR: Conceptualization, Investigation, Validation, Writing – review & editing. DB: Data curation, Project administration, Writing – review & editing. MJ: Data curation, Formal analysis, Writing – review & editing. SC: Data curation, Formal analysis, Writing – review & editing. JJ: Data curation, Methodology, Writing – review & editing. PC: Data curation, Methodology, Writing – review & editing. GD: Data curation, Methodology, Writing – review & editing. NK: Data curation, Methodology, Writing – review & editing. SH: Data curation, Methodology, Writing – review & editing. PL: Conceptualization, Writing – review & editing, Funding acquisition, Methodology, Data curation, Formal analysis, Investigation, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study received funding from Merck KGaA, 250 Frankfurters Strasse, 64293, Darmstadt, Germany (Funder’s Study ID Number: MS200157-0021). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors would like to extend their sincere gratitude to the following individuals and organizations for their invaluable contributions and support to this research study: Clara Fabienne Rasoamanamihaja, Paulin Ramasy Manjary, and Bemarivo Jeannoé Assany, Ministry of Health, Antananarivo, Madagascar, and Kristine Brøndbjerg Øby and Maria Jensen, Center for Clinical Research, North Denmark Regional Hospital, Denmark.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1322667/full#supplementary-material
References
1. Le L, Hsieh MH. Diagnosing urogenital schistosomiasis: dealing with diminishing returns. Trends Parasitology. (2017) 33:378–87. doi: 10.1016/j.pt.2016.12.009
2. Kjetland EF, Leutscher PDC, Ndhlovu PD. A review of female genital schistosomiasis. Trends Parasitology. (2012) 28:58–65. doi: 10.1016/j.pt.2011.10.008
3. Orish VN, Morhe EKS, Azanu W, Alhassan RK and Gyapong M. The parasitology of female genital schistosomiasis. Curr Res Parasitol Vector-Borne Diseases. (2022) 2:100093. doi: 10.1016/j.crpvbd.2022.100093
4. Sturt AS, Webb EL, Himschoot L, Phiri CR, Mapani J, Mudenda M, et al. Association of female genital schistosomiasis with the cervicovaginal microbiota and sexually transmitted infections in Zambian women. Open Forum Infect Dis. (2021) 8:ofab438. doi: 10.1093/ofid/ofab438
5. Rafferty H, Sturt AS, Phiri CR, Webb EL, Mudenda M, Mapani J, et al. Association between cervical dysplasia and female genital schistosomiasis diagnosed by genital PCR in Zambian women. BMC Infect Dis. (2021) 21:691. doi: 10.1186/s12879-021-06380-5
6. Kutz JM, Rausche P, Rasamoelina T, Ratefiarisoa S, Razafindrakoto R, Klein P, et al. Female genital schistosomiasis, human papilloma virus infection, and cervical cancer in rural Madagascar: a cross-sectional study. Infect Dis Poverty. (2023) 12:89. doi: 10.1186/s40249-023-01139-3
7. Pillay P, Downs JA, Changalucha JM, Brienen EAT, Ramarokoto CE, Leutscher PDC, et al. Detection of Schistosoma DNA in genital specimens and urine: a comparison between five female African study populations originating from S. haematobium and/or S. mansoni endemic areas. Acta Tropica. (2020) 204:105363. doi: 10.1016/j.actatropica.2020.105363
8. Corstjens PLAM, de Dood CJ, Knopp S, Clements MN, Ortu G, Umulisa I, et al. Circulating anodic antigen (CAA): a highly sensitive diagnostic biomarker to detect active Schistosoma infections—improvement and use during SCORE. Am J Trop Med Hygiene. (2020) 103:50–7. doi: 10.4269/ajtmh.19-0819
9. Galappaththi-Arachchige HN, Holmen S, Koukounari A, Kleppa E, Pillay P, Sebitloane M, et al. Evaluating diagnostic indicators of urogenital Schistosoma haematobium infection in young women: a cross-sectional study in rural South Africa. PloS One. (2018) 13:e0191459. doi: 10.1371/journal.pone.0191459
10. Rutty Phiri C, Sturt AS, Webb EL, Chola N, Hayes R, Shanaube K, et al. Acceptability and feasibility of genital self-sampling for the diagnosis of female genital schistosomiasis: a cross-sectional study in Zambia. Wellcome Open Res. (2020) 5:61. doi: 10.12688/wellcomeopenres.15482.2
11. Ursini T, Scarso S, Mugassa S, Othman JB, Yussuph AJ, Ndaboine E, et al. Assessing the prevalence of female genital schistosomiasis and comparing the acceptability and performance of health worker-collected and self-collected cervical-vaginal swabs using PCR testing among women in North-Western Tanzania: The ShWAB study. PloS Negl Trop Diseases. (2023) 17:e0011465. doi: 10.1371/journal.pntd.0011465
12. Randrianasolo BS, Jourdan PM, Ravoniarimbinina P, Ramarokoto CE, Rakotomanana F, Ravaoalimalala VE, et al. Gynecological manifestations, histopathological findings, and Schistosoma-specific polymerase chain reaction results among women with Schistosoma haematobium infection: a cross-sectional study in Madagascar. J Infect Diseases. (2015) 212:275–84. doi: 10.1093/infdis/jiv035
13. Kjetland EF, Hove RJT, Gomo E, Midzi N, Gwanzura L, Mason P, et al. Schistosomiasis PCR in vaginal lavage as an indicator of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hygiene. (2009) 81:1050–5. doi: 10.4269/ajtmh.2009.09-0081
14. Arenholt LTS, Randrianasolo BS, Rabozakandraina TOO, Ramarokoto CE, Jøker K, Aarøe KK, et al. Efficacy and safety of a repeated praziquantel dosing regimen in treatment of female genital schistosomiasis – a phase 2 randomized controlled trial. Front Trop Dis. (2024). doi: 10.3389/fitd.2024.1322652
15. Arenholt LTS, Aaroe KK, Norderud K, Lumholdt M, Randrianasolo BS, Ramarokoto CE, et al. Cervical lesion proportion measure using a digital gridded imaging technique to assess cervical pathology in women with genital schistosomiasis. PloS Negl Trop Diseases-. (2022) 16:e0009995. doi: 10.1371/journal.pntd.0009995
16. Dragsbæk SJ, Carstens SK, Østergaard IS, Jøker K, Randrianasolo BS, Leutscher PDC, et al. Measurement of cervical grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels proportions in women with female genital schistosomiasis – a clinical validation study of the digital gridded imaging technique. Front Trop Diseases. (2024) 5. doi: 10.3389/fitd.2024.1322696
17. Corstjens PL, De Dood CJ, Kornelis D, Fat EM, Wilson RA, Kariuki TM, et al. Tools for diagnosis, monitoring and screening of Schistosoma infections utilizing lateral-flow based assays and upconverting phosphor labels. Parasitology. (2014) 141:1841–55. doi: 10.1017/S0031182014000626
18. Feldmeier H, Bienzle U, Dietrich M, Sievertsen HJ. Combination of a viability test and a quantification method for Schistosoma haematobium eggs (filtration–trypan blue-staining technique). Tropenmed Parasitol. (1979) 30:417–22.
19. Westh H, Jensen JS. Low prevalence of the new variant of Chlamydia trachomatis in Denmark. Sex Transm Infect. (2008) 84:546–7. doi: 10.1136/sti.2008.031906
20. Hjelmevoll SO, Olsen ME, Sollid JU, Haaheim H, Unemo M and Skogen V. A fast real-time polymerase chain reaction method for sensitive and specific detection of the Neisseria gonorrhoeae porA pseudogene. J Mol Diagn. (2006) 8:574–81. doi: 10.2353/jmoldx.2006.060024
21. Tabrizi SN, Chen S, Tapsall J, Garland SM. Evaluation of opa-based real-time PCR for detection of Neisseria gonorrhoeae. Sex Transm Dis. (2005) 32:199–202. doi: 10.1097/01.olq.0000154495.24519.bf
22. Pillay A, Radebe F, Fehler G, Htun Y, Ballard RC. Comparison of a TaqMan-based real-time polymerase chain reaction with conventional tests for the detection of Trichomonas vaginalis. Sex Transm Infect. (2007) 83:126–9. doi: 10.1136/sti.2006.022376
23. Jensen JS, Björnelius E, Dohn B and Lidbrink P. Use of TaqMan 5' nuclease real-time PCR for quantitative detection of Mycoplasma genitalium DNA in males with and without urethritis who were attendees at a sexually transmitted disease clinic. J Clin Microbiol. (2004) 42:683–92. doi: 10.1128/JCM.42.2.683-692.2004
24. Haahr T, Humaidan P, Elbaek HO, Alsbjerg B, Laursen RJ, Rygaard K, et al. Vaginal microbiota and in vitro fertilization outcomes: Development of a simple diagnostic tool to predict patients at risk of a poor reproductive outcome. J Infect Dis. (2019) 219:1809–17. doi: 10.1093/infdis/jiy744
25. Shukla JD, Kleppa E, Holmen S, Ndhlovu PD, Mtshali A, Sebitloane M, et al. The association between female genital schistosomiasis and other infections of the lower genital tract in adolescent girls and young women: a cross-sectional study in South Africa. J Lower Genital Tract Disease. (2023) 27:291–6. doi: 10.1097/LGT.0000000000000756
26. Yirenya-Tawiah D, Annang TN, Apea-Kubi KA. Chlamydia trachomatis and Neisseria gonorrhoeae prevalence among women of reproductive age living in urogenital schistosomiasis endemic area in Ghana. BMC Res Notes. (2014) 7:349. doi: 10.1186/1756-0500-7-349
27. Søfteland S, Sebitloane M, Galappaththi-Arachchige HN, Kleppa E, Holmen S, Pillay P, et al. Diagnosis of female genital schistosomiasis and other genital infections in young South African women: challenges in the syndromic approach. Front Trop Dis. (2024) 5:1379526. doi: 10.3389/fitd.2024.1379526
28. Nemungadi TG, Kleppa E, van Dam GJ, Corstjens PLAM, Galappaththi-Arachchige HN, Pillay P, et al. Female genital schistosomiasis lesions explored using circulating anodic antigen as an indicator for live Schistosoma worms. Front Trop Dis. (2022) 3:821463. doi: 10.3389/fitd.2022.821463
29. Leutscher PDC, Ramarokoto CE, Hoffmann S, Jensen JS, Ramaniraka V, Randrianasolo B, et al. Coexistence of urogenital schistosomiasis and sexually transmitted infection in women and men living in an area where Schistosoma haematobium is endemic. Clin Inf Dis. (2008) 47:775–82. doi: 10.1086/591127
Keywords: Schistosoma haematobium, female genital schistosomiasis, gynecological manifestations, Schistosoma DNA, circulating anodic antigens, sexually transmitted infections, bacterial vaginosis
Citation: Randrianasolo BS, Jøker K, Arenholt LTS, Rabozakandraina TOO, Ramarokoto CE, Brønnum D, Jensen M, Christensen SL, Jensen JS, Corstjens P, van Dam GJ, Kobayashi N, Hamano S and Leutscher PDC (2024) An assessment of gynecological manifestations in women with female genital schistosomiasis with reference to Schistosoma biomarkers, sexually transmitted infections and bacterial vaginosis. Front. Trop. Dis 5:1322667. doi: 10.3389/fitd.2024.1322667
Received: 16 October 2023; Accepted: 25 July 2024;
Published: 27 August 2024.
Edited by:
Thiago Almeida Pereira, Stanford University, United StatesReviewed by:
G. Takop Nchanji, TroDDIVaT Initiative, CameroonChiaka Anumudu, University of Ibadan, Nigeria
Copyright © 2024 Randrianasolo, Jøker, Arenholt, Rabozakandraina, Ramarokoto, Brønnum, Jensen, Christensen, Jensen, Corstjens, van Dam, Kobayashi, Hamano and Leutscher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Derek Christian Leutscher, cC5sZXV0c2NoZXJAcm4uZGs=
†These authors share first authorship