 Louise Thomsen Schmidt Arenholt1,2,3*
Louise Thomsen Schmidt Arenholt1,2,3* Bodo Sahondra Randrianasolo4
Bodo Sahondra Randrianasolo4 Tiana Onintsoa Oliva Rabozakandraina4
Tiana Onintsoa Oliva Rabozakandraina4 Charles Emile Ramarokoto4
Charles Emile Ramarokoto4 Karoline Jøker1
Karoline Jøker1 Katrina Kæstel Aarøe1
Katrina Kæstel Aarøe1 Dorthe Brønnum1
Dorthe Brønnum1 Caspar Bundgaard Nielsen1
Caspar Bundgaard Nielsen1 Suzette Sørensen1,2,3
Suzette Sørensen1,2,3 Mads Lumholdt1
Mads Lumholdt1 Martin Jensen5
Martin Jensen5 Søren Lundbye-Christensen5
Søren Lundbye-Christensen5 Jørgen Skov Jensen6
Jørgen Skov Jensen6 Paul Corstjens7
Paul Corstjens7 Pytsje Hoekstra8
Pytsje Hoekstra8 Govert J van Dam8
Govert J van Dam8 Noriko Kobayashi9,10
Noriko Kobayashi9,10 Shinjiro Hamano9,10
Shinjiro Hamano9,10 Peter Derek Christian Leutscher1,3
Peter Derek Christian Leutscher1,3- 1Centre for Clinical Research, North Denmark Regional Hospital, Hjoerring, Denmark
- 2Department of Gynecology and Obstetrics, North Denmark Regional Hospital, Hjoerring, Denmark
- 3Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
- 4Association K’OLO VANONA, Antananarivo, Madagascar
- 5Research Data and Biostatistics, Aalborg University, Aalborg, Denmark
- 6Research Unit for Reproductive Microbiology, Bacteria, Parasites and Fungi, Statens Serum Institut, Copenhagen, Denmark
- 7Department of Cell and Chemical Biology, Leiden University Medical Centre, Leiden, Netherlands
- 8Department of Parasitology, Leiden University Medical Centre, Leiden, Netherlands
- 9Department of Parasitology, Institute of Tropical Medicine (NEKKEN), Nagasaki University, Nagasaki, Japan
- 10Graduate School of Biomedical Sciences, Nagasaki University, Nagasaki, Japan
Background: Single-dose praziquantel (PZQ) for treating urogenital schistosomiasis has been reported as inadequate for achieving significant resolution of female genital schistosomiasis (FGS)-associated cervicovaginal lesions. This randomised controlled trial aimed to assess the efficacy and safety of a repeated PZQ-dosing regimen.
Methods: The trial was conducted among women aged 15 to 34 with FGS-associated cervical lesions living in a Schistosoma haematobium-endemic area of northern Madagascar. A total of 116 women were randomly allocated to either repeated PZQ-dosing (n=58) or a single PZQ dose (n=58). All received an initial PZQ dose of 40mg/kg at baseline. In the repeated-dosing arm, additional doses were given 12 and 24 hours later and again at 5 and 10 weeks. Primary outcome was FGS-related cervical lesions at baseline compared to Week 15 follow-up. Secondary outcomes encompassed pelvic exam abnormalities, urogenital complaints, and biomarkers, including cervicovaginal S. haematobium DNA and circulating anodic antigens (CAA) in serum.
Results: Excluding 21 women who were pregnant or failed to attend follow-up visits, 95 women were eligible for per-protocol treatment effect analysis. A minor and insignificant reduction in cervical lesions was observed in both of the two treatment arms at Week 15 follow-up. A clear tendency towards decline in pelvic exam abnormalities and urogenital complaints in both treatment arm groups was observed. The reduction in number of women testing positive for CAA and mean CAA values was significant in both arms but less so in the single-dose arm. Mild to moderate adverse events of equal proportions were reported in both treatment arm groups.
Conclusion: FGS-associated cervical lesions appear refractory to PZQ treatment even when this is administered in a repeated-dosing regimen. In contrast, the repeated regimen seems more effective at eliminating the dwelling worm population than the single-dose regimen, as demonstrated by the CAA findings. Irrespective of dosing regimen, pelvic exam abnormalities and urogenital complaints saw equal reductions at follow-up. However, the outcome of our primary study emphasises the need for initiation early in life and a persistently maintained PZQ treatment strategy throughout childhood and adolescence to prevent lesions from establishing in the first place.
Clinical trial registration: https://clinicaltrials.gov/, dentifier NCT04115072.
Introduction
Female genital schistosomiasis (FGS) refers to the overall gynaecological manifestation of Schistosoma-parasitic flatworm infection, predominantly transmitted by the Schistosoma haematobium species (1). FGS has a high prevalence across sub-Saharan Africa, affecting an estimated 80 million African girls and women (1).
Females are infected with S. haematobium through contact with parasite-infested freshwater. In their free-swimming stage, the cercariae penetrate the skin and transform into schistosomula, subsequently maturing into schistosomes in the liver. Male and female schistosomes form pairs and migrate to the bladder and the genital organs, where egg excretion commences (2). The pathogenesis of FGS is assumed to be the result of a complex inflammatory immune response driven by antigens released from viable eggs secreted by the adult female worms and subsequently entrapped in urogenital tissue (3). Inflammation occurs in all strata of the genital tissue, including the small blood vessels (4–7). The inflammation extends beyond the site where eggs are deposited (7–10). FGS manifests through persistent long-term effects arising from the entrapment of eggs in the genital tissues leading to chronic inflammation and subsequent fibrotic calcified lesions (11, 12).
Women with FGS commonly report urogenital symptoms such as lower abdominal pain, vaginal discharge, and postcoital bleeding (13, 14). Using a colposcope, FGS is identifiable during pelvic exam by noting distinctive cervicovaginal lesions such as grainy sandy patches, homogenous yellow sandy patches, rubbery papules, and abnormal blood vessels (14, 15). The diagnosis is further supported by friable mucosal surfaces, spontaneous bleeding, and bleeding upon instrumental contact, in addition to tenderness reported by the women undergoing pelvic exam. Various Schistosoma biomarkers in serum, urine, and cervicovaginal samples likewise support FGS diagnosis. Unfortunately, these biomarkers are challenged by low sensitivity and specificity in relation to FGS and moreover by high resource and cost prerequisites (16). However, they have proven valuable in assessing overall Schistosoma disease comprehensively, encompassing bladder and gut conditions.
Praziquantel (PZQ), a widely used anthelmintic drug, has shown remarkable effectiveness in decreasing gross pathology related to urinary and intestinal schistosomiasis in major control programmes (17). However, its efficacy in treating FGS-associated cervicovaginal lesions appears to be somewhat limited (15). Its mode of action primarily targets the muscles of the worm, causing paralysis and detachment from blood vessels (18). The lesions appear refractory to treatment despite a relatively successful anti-helminthic treatment with PZQ to eliminate the majority of the dwelling adult worm population (11). This points to a compelling need to optimise PZQ treatment regimens specifically for women with FGS. A repeated treatment schedule may thus offer a means of optimising the effect of PZQ by killing a higher proportion of the adult worm population, leading to significant decreased deposition of eggs to the genital tissue. Such a deceleration of the inflammatory process may create a conducive environment for a gradual healing of the genital pathology. Based on this rationale, a randomised controlled trial (RCT) was conducted to assess the efficacy and safety of a repeated PZQ treatment regimen compared to the standardised single-dose PZQ regimen in women with FGS.
Methods
Primary and secondary study outcomes
The primary efficacy outcome of the RCT was changes in FGS-associated cervical lesions at the end of the trial. The secondary outcomes were effects on pelvic exam abnormalities and urogenital complaints, in addition to changes in Schistosoma biomarkers.
Study area and participants
The RCT was conducted in the Ambanja district of northwestern Madagascar, known as a hyper-endemic region for S. haematobium but with low endemicity for S. mansoni (19). The dominant ethnic group and the primary spoken dialect of the Malagasy language in this district is Sakalava. Women living in the Antsakoamanondro and Antranokarany village areas were invited to attend the local health clinic for screening and inclusion in the RCT.
The calculation of the participant sample size assumed a 33% difference at Week 15-follow-up in comparison to baseline of cervical lesions in women receiving a single PZQ dose for treatment of FGS (Arm A) versus women receiving a repeated PZQ dosing regimen (Arm B). Hence, 47 women per arm were needed to identify a significant difference between the repeated treatment group and the standard treatment (significance 0.05; power of the test 0.90). Taking into consideration a loss of 20% during follow-up, 58 women were planned for enrolment in each arm.
The inclusion criteria for participation in the RCT were age 15 to 35, current urogenital complaints, and the presence of at least one of the four cervical lesion types considered pathognomonic for the detection of FGS during pelvic exam: grainy sandy patches, homogenous yellow sandy patches, rubbery papules, or abnormal blood vessels (20–23). The exclusion criteria comprised virginity, pregnancy, a history of vulva, vagina, or uterus tumours, hysterectomy, HIV-positive status, medical conditions necessitating hospitalisation, PZQ treatment in the preceding three months, or presented contraindications to PZQ. The evaluation of exclusion criteria was conducted through a meticulous interview on medical history. Participation in the screening procedure and the RCT required signed consent following comprehensive oral information concerning the study. The RCT protocol comprised a medical interview, a gynaecological exam, and the collection of various specimens of bacteria, etc. followed by PZQ treatment at baseline. The clinical assessments were repeated at Week 5-, Week 10-, and Week 15-follow-ups for both treatment arms, as documented Table 1.

Table 1. Time plan for the assessment of the study variables.
Rationale for repeated treatment with praziquantel
The immunology of schistosomiasis is characterised by an imbalance of T-cell subpopulations combined with strong polyclonal activation of B-cells, eventually leading to an altered immune response to TH1- and TH2-dependent cytokines (24–26). The evidence shows that the clinical pathology seen at the cervix in women with FGS is a result of chronic inflammation caused by antigens released by adult worms and viable eggs. Treatment with PZQ of patients with intestinal or hepatosplenic schistosomiasis has shown normalisation in the pattern of TH1- and TH2-dependent cytokines before regression of morbidity (25, 26). This indicates that the elimination of all worms by treatment with praziquantel can re-establish normal immune responsiveness.
We therefore decided to evaluate a repeated treatment with PZQ administered at well-defined time intervals, with the first dose given at baseline, the second and third doses with an interval of 12 hours, the fourth dose at Week 5, followed by the fifth dose at Week 10.
This dosage regimen was based on the following assumptions:
— A single dose of 40 mg/kg eliminates approximately 90% of adult worms; three doses of 40mg/kg were thus considered necessary to eradicate all worms at baseline (12, 27–29).
— Schistosomulae exhibit resistance to PZQ. The fourth dose is consequently administered five weeks (Week 5) after the first to eliminate any adult worms developed from schistosomulae during this time, typically taking four to six weeks (30–32).
— Anticipating reinfection a few weeks following baseline treatment, given that women continue to be exposed to infested water (33). To eradicate remaining adult worms (32), a fifth dose was administered at Week 10.
Praziquantel treatment regimens and randomisation
A single-dose weight-based (40 mg/kg) PZQ regimen at baseline (Arm A) was compared with a regimen offering an initial single dose of PZQ and repeated at 12 hours, 24 hours, at Week 5, and at Week 10 (Arm B). The design of the two treatment arms was otherwise identical, with equal numbers of participants. The R software program (Version 3.6.0) generated a randomisation list of 120 distinct participant IDs without blocking. Sealed envelopes with a participant’s unique ID and their assigned treatment arm were subsequently prepared. The IDs were consecutively allocated to the participants, after which the corresponding envelope was opened to reveal their designated treatment arm. Neither the research team nor the participants were blinded regarding the allocated treatment.
After completion of the clinical assessment protocol at baseline and follow-up, the participants were treated with PZQ according to their randomisation status. Each woman received a meal one hour before PZQ administration. In both treatment arms the women remained at the clinic where they were closely observed for 30 hours following the administration of the initial dosages at baseline. This vigilance aimed to ensure their safety and to monitor adverse events, particularly considering the repeated doses in Arm B. If pregnancy or breastfeeding occurred in any follow-up visits, PZQ was not administrated to the woman. Nonattendance likewise led to exclusion. At each visit, the women underwent pregnancy testing through a urine-based pregnancy test. At the final visit, participants from both study arms were treated with a standard PZQ dosage of 40mg/kg, administered if signs of FGS persisted, including positive findings of S. haematobium eggs in urine.
Medical interviewing
Questionnaires were developed and tested in Sakalava, the dialect spoken in the study area. Questions regarding health concerns were carefully worded to ensure comprehension and relevance for the women. Detailed medical histories were obtained, specifically focusing on reproductive and sexual health. In identifying potential conditions associated with FGS, we thoroughly reviewed the existing literature, considering only clearly defined complaints directly linked to FGS and reported in at least two studies with representative samples of women affected by FGS. For publication purposes, the terms used in Sakalavan for the complaints were transcribed into French using layman’s terms and then translated literally into English.
Pelvic exam
A pelvic exam, including inspection and bimanual palpation, was conducted at baseline and at each of the three follow-up visits. The women were instructed not to clean their vulva and vagina on the day of the pelvic exam. If menstruating, participants were advised to reschedule the exam for a later date when bleeding had ceased.
During the pelvic exam, the woman was positioned in a dorsal lithotomy position with leg support. An exam of the vulva was performed by the naked eye. An appropriately sized vaginal speculum was gently introduced and cautiously opened to ensure minimum instrumental contact to the cervicovaginal epithelium, which was examined by the naked eye for cervicovaginal abnormalities, including bleeding and epithelial disruption defined as erosions, ulcerations, and friable cervical surface. Closer inspection in search of FGS-associated lesions was subsequently performed using a high-resolution Canon EOS M50 camera (Canon EOS M50; Canon, Tokyo, Japan) equipped with a 100mm macro-lens mounted with a circular LED light. Images of present cervical lesions were captured with the camera in autofocus mode and positioned approximately 30cm from the cervix. The best-quality images from baseline and from each follow-up visit were chosen from the portfolio of cervical images to evaluate FGS-associated cervical lesions. The digital images were stored in the Research Electronic Data Capture Version REDCap 9.5.6 data management system (REDCap) hosted by the North Denmark Regional Hospital.
Digital gridded imaging technique
The cervical images were assessed using the digital gridded image technique for quantifying FGS-associated cervical lesions with the application of the QubiFier software program, as previously reported (34). A semi-transparent circular grid composed of 424 equally sized squares, positioned to cover the cervical surface, was applied to each image. Squares that exhibited any of the four FGS-associated lesion types were marked manually. The number of marked squares was subsequently counted automatically by the QubiFier instrument and divided by 424, the number of affected squares. This quotient was multiplied by 100, resulting in a proportion range from 0 to 100 per cent. To derive the total quantum of lesions on the cervix, a cervical lesion proportion (CLP) was measured, representing all four lesion types. The proportion of each of the specific lesions [homogeneous yellow sandy patches proportion (HSP), grainy sandy patches proportion (GSP), and abnormal blood vessel proportion (BVP)] was calculated as a percentage between 0 and 100, in addition to a rubbery papules count (RPC) presented as an n-value. To assess the specific lesion types, an extended version of the original digital gridded image technique (34) has been developed, tested, and validated (35). A good to excellent interrater agreement has been found between observers for each of the specific lesion types and the total cervical lesion proportion.
The evaluation of the cervical images was conducted by an observer team comprising four medical students trained and supervised by a consultant gynaecologist with comprehensive experience in evaluating FGS-associated lesions. Hence, all five observers were considered proficient in this evaluation methodology. Each lesion type was assessed by the same observer, ensuring consistency in the scoring process among all images and visits. To guarantee consistent placement of the grid across images of the same woman, accounting for potential variations in image capture distance between visits, simultaneous assessment of all the selected images across baseline and the three follow-up visits was performed. Observers were blinded to the participant’s treatment group and the specific visit during which the image was captured.
Laboratory work
Several types of laboratory analyses were performed, including serum circulating anodic antigen (CAA), cervicovaginal S. haematobium DNA, urinary egg count, faecal parasites, sexually transmitted infections (STIs), and bacterial vaginosis as described in the sections below. A comprehensive panel of blood and urine samples were collected from each participant at baseline and each follow-up. Stool samples were examined only at baseline. Samples from the cervix and posterior vaginal fornix using cytobrush and swabs were also collected at each of the four scheduled visits. In addition, a cervicovaginal lavage was performed as described: 10 mL of sterile 0.9% NaCl were sprayed on the surface of the cervix and the inner half of the vaginal surfaces with a syringe which was immediately pulled back. The procedure was repeated four times.
Schistosoma haematobium DNA
DNA originating from S. haematobium eggs was measured in cervicovaginal specimens collected from the participants at baseline and follow-up at Weeks 5 and 15. Vaginal lavage and cervical swab tests for S. haematobium DNA were stored in liquid nitrogen and shipped to the Department of Parasitology, Institute of Tropical Medicine at Nagasaki University, Japan. Using the QIAamp DNA Mini Kit (QIAGEN, Germany), genomic DNA was extracted from 200 µL with both cervical swabs and vaginal lavage fluid. For identification of S. haematobium, the Schistosoma-specific internal transcribed spacer 2 (ITS2) (GenBank accession DQ677661) region was amplified by real-time PCR, using a primer set consisting of forward Sh63F (5’-GGTCTAGATGACTTGATCGAGATGCT-3’) and reverse Sh139R (5’-TCCCGAGCG CGTATAATGTCATTA-3’) (36). Negative and positive control samples were included in each amplification run. Thermocycling conditions were as follows: incubation at 95°C for 3 min, followed by 45 cycles of 95°C for 15 sec and 60°C for 30 sec. Amplification, detection, and analysis were performed with QuantStudio™ 7 Flex Real-Time PCR System (Singapore, Singapore) (37). The cycle threshold (Ct) cut-off value was set at 42 to categorise the samples into infection-positive or -negative.
Circulating anodic antigens
Circulating anodic antigens (CAA) were measured in serum samples collected at baseline and at Week 5-, Week 10-, and Week 15-follow-ups. Schistosome gut antigens are continuously excreted into the host circulation by metabolically active worms, the concentration of CAA reflecting the number of adult worms present in the circulation, independent of the anatomic location. The Up-Converting reporter Particle Lateral Flow test for the detection of schistosome CAA was used to detect Schistosoma infections (38). All serum samples were tested using the SCAA20 format using 20 µl of serum, while for the most sensitive concentration format we used 500 µl of serum (SCAA500) (39). In short, 20/500 μL aliquots were mixed with equal volumes of 4% (w/v) trichloro-acetic acid (TCA) and centrifuged to remove interfering proteins and to dissociate potential immune complexes. Supernatants (for the 500 µl aliquots after 25-fold concentration to 20 μL over a 10 kDa Amicon Ultra-0·5 mL Centrifugal Filter, Millipore Corporation) were incubated with the UCP-antibody conjugate solution and run on LF strips, which were scanned for UCP reporter signals with a Packard FluoroCount strip reader adapted for UCP detection. A standard dilution curve of the TCA-soluble fraction of adult worm antigen (AWA-TCA) with known CAA concentrations was used as reference to validate the cut-off (39). Results are expressed as pg CAA/mL serum; a CAA concentration above 1 pg/mL was considered positive (38).
Urine and stool examination
Morning urine samples were collected and subjected to filtration through a 14 µm polycarbonate membrane, with a volume of 50 mL, to ascertain the presence of S. haematobium eggs (40). Results are expressed as the number of eggs per 50 mL and evaluated at baseline and Week 15-follow-up. Using the Merthiolate Iode Formol (MIF) concentration technique, eggs in stool were identified at baseline only (41).
Eosinophilia
To assess the immunologic response to S. haematobium, blood samples were analysed for eosinophilia at baseline and 15-week follow-up. A differential white blood cell count was performed to assess the percentage of eosinophils present in the blood sample.
Sexually transmitted infections and bacterial vaginosis
Serum specimens were tested for Treponema pallidum at baseline by a rapid plasma reagin test (RPR) (Linear Cromatest, Montgat, Barcelona, Spain) and a hemagglutination assay (TPHA) (Linear Cromatest, Montgat, Barcelona, Spain) performed at the healthcare clinic in Ambanja. Direct microscopy was available at the local laboratory for detecting Trichomonas vaginalis in the vaginal fluid and enabled immediate diagnosis-guided treatment of trichomonas. Moreover, T. vaginalis was also assessed using PCR, as described below; data from the direct microscopy are not reported.
Testing for Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium infection, as well as bacterial vaginosis, was conducted at baseline and Week 15. For this purpose, cervicovaginal swabs were collected in 2 mL of Copan eNat using a regular flocked swab (Copan, Brescia, Italy). Specimens were stored at ambient temperature for no more than 12 hours until storage at minus 80°C was secured, subsequently to be shipped on dry ice to the Statens Serum Institute in Copenhagen, Denmark, for analysis. DNA extraction was performed using 200 µL of the collected swab specimens on a MagNAPure instrument (Roche Molecular Systems Inc., CA, USA) with the Pathogen Universal 200 MagNA Pure protocol and eluted in 100 µL elution buffer. All real-time PCRs were performed with 5 µl of extracted DNA, each assay undergoing internal control for inhibition. For C. trachomatis, primers targeted the 16S rRNA gene (42), and the N. gonorrhoeae assay targeted the porA pseudogene (43) using a modified TaqMan® probe. Positive samples were confirmed by an assay targeting the opa gene (44). The T. vaginalis assay targeted a specific repeat sequence using primers as previously described (45) and a modified TaqMan MGB® probe. Positive results were confirmed by repeating the PCR. M. genitalium was detected using primers and probes targeting the major MgPa adhesin (46).
Bacterial vaginosis (BV) was also diagnosed at baseline and at follow-up 15 weeks later in a combined assay detecting the presence of abnormal vaginal microbiota, including Fannyhessea vaginae, also known as Atopopium vaginae, and Gardnerella species as previously described (47) using cut-off at 10,000 geq/µl template for F. vaginae and 100,000 geq/µl template for Gardnerella spp.
For detection of human papillomavirus (HPV) and herpes simplex virus (HSV) at baseline, a cervical swab specimen was collected using a cytobrush, which was subsequently stored in a dry tube at minus 80°C until further processing at the Centre for Clinical Research at the North Denmark Regional Hospital. DNA was purified from the cytobrushes using the QIAamp MinElute Media kit (QIAGEN). HPV detection was performed as previously described (48). HSV-1 and HSV-2 analyses were performed using the GeneProof Herpes Simplex virus (HSV-1/2) PCR kit according to the manufacturer´s recommendations. HPV and HSV analyses were performed in duplicates; samples were considered positive only if viral DNA was detected twice.
The results of the analyses conducted at the reference laboratories in Denmark were not promptly accessible during the baseline study period or at any of the subsequent visits. The treatment of STIs and other gynaecological disease manifestations, including BV and yeast infection, therefore had to be based on the syndromic approach recommended by the Ministry of Health of Madagascar (49). The study participants were moreover treated in accordance with the results of T. pallidum and T. vaginalis testing as part of the local study set-up. When results from the reference laboratory became available, the women and their partners were offered treatment.
Adverse events
For a period of 30 hours after the initial dosages of PZQ were administered at baseline, women in both treatment groups were thoroughly monitored by a physician from the research team. Any potential adverse events were documented and categorised by severity as mild, moderate, or major. Alanine aminotransferase (ALT) and bilirubin levels were evaluated at baseline and 24 hours after the first dosage. Elevated values were defined as ALT levels ≥25 U/L and bilirubin levels exceeding 1 mg/dl.
Data management and analysis
A unique identifier (ID code) was assigned to each participant. The local team entered all data obtained at the investigation site in Madagascar into the Research Electronic Data Capture (REDCap) database on the virtual server at North Denmark Regional Hospital. The Danish research team entered other data obtained from the reference laboratory sites in the database, access to which required a personal username and password; all changes were automatically logged. Only authorised members of the team had access to the stored data. All data were handled to ensure data safety and observance of privacy rules according to the General Data Protection Regulation (GDPR) and the Danish Data Protection Act. The ID code list and hard copies of all records were securely stored in a designated room at the local investigator’s site, with access restricted and safeguarded by using a locked cabinet accessible solely by the main investigator in Madagascar.
Statistics
Continuous data were summarised as mean (95% CI), and comparisons between Arm A and Arm B were conducted using an unpaired t-test; for comparison between time points a paired t-test was performed. Comparison between arms of difference from baseline to follow-up was made using an unpaired t-test. Data that failed to meet normal distribution underwent bootstrap analysis (5,000–8,000 replications) to calculate CI and p-values. Categorical data were described as number of patients (n,%) and compared between arms using Fisher’s exact test; McNemar’s test was used for comparison between time points. Comparison between arms of changes over time was performed using generalised linear models. Analyses were conducted using SPSS (IBM SPSS Statistics 29.0.0.0 (Version 241)). P-values <0.05 were considered significant.
The clearance rate for cervicovaginal S. haematobium DNA was defined as the proportion of S. haematobium PCR-positive women before treatment compared with the proportion of S. haematobium PCR-negative at follow-up. The clearance rate for S. haematobium eggs in urine was calculated similarly.
Results
Of the 381 women assessed for eligibility by questionnaire and pelvic exam, 116 (88.5%) were enrolled in the RCT, with 58 randomly assigned to each treatment arm (A and B) (Figure 1). The participants’ mean age was 25.5 years (95% CI 24.3–26.7). No statistically significant differences were found between the two treatment arms regarding socio-demographic and reproductive health history characteristics (Table 2).
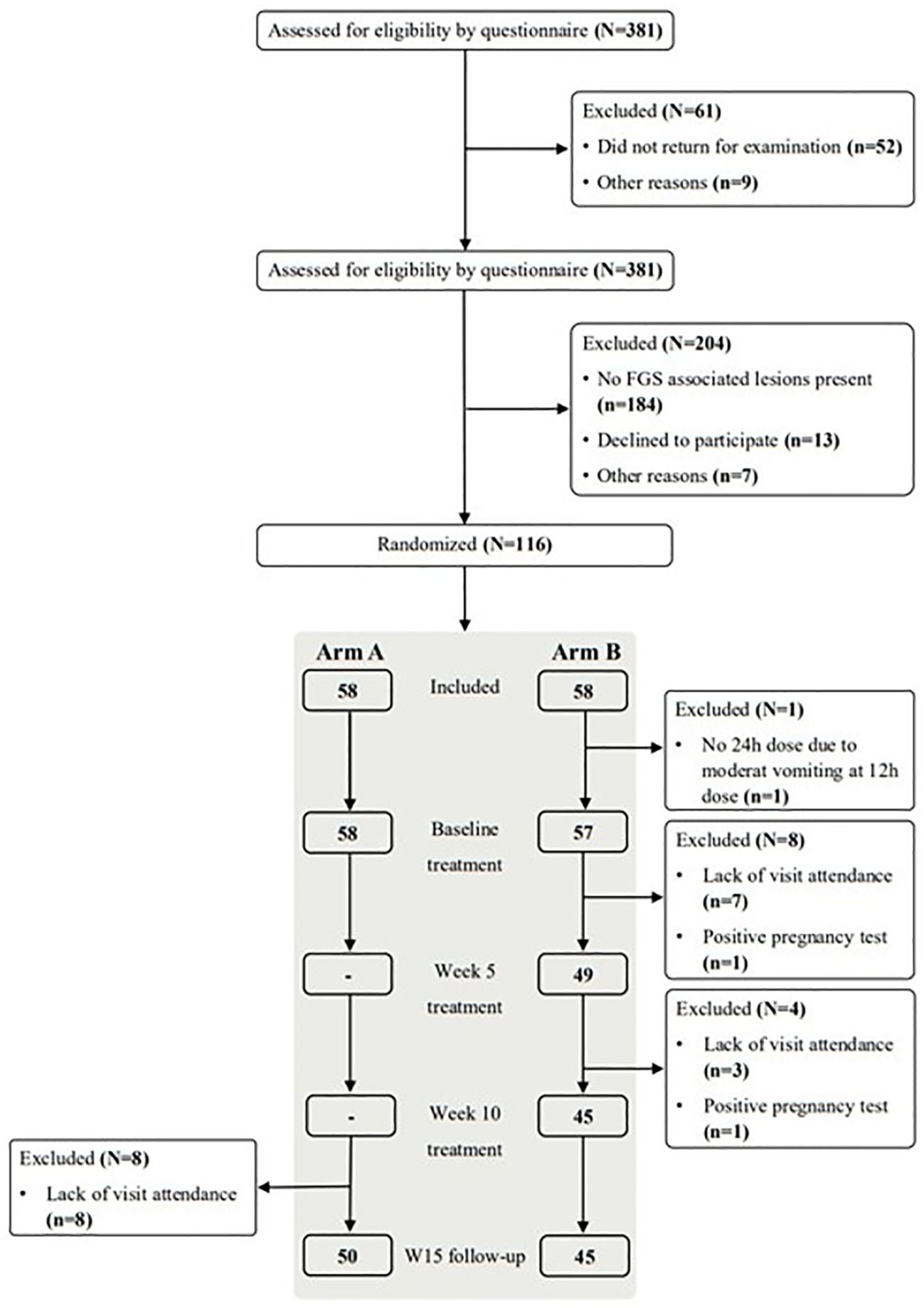
Figure 1. Patient flow during the study period. FGS: female genital schistosomiasis, W15: week 15, Number stated for week 15 are women eligible for final assessment pro-protocol.
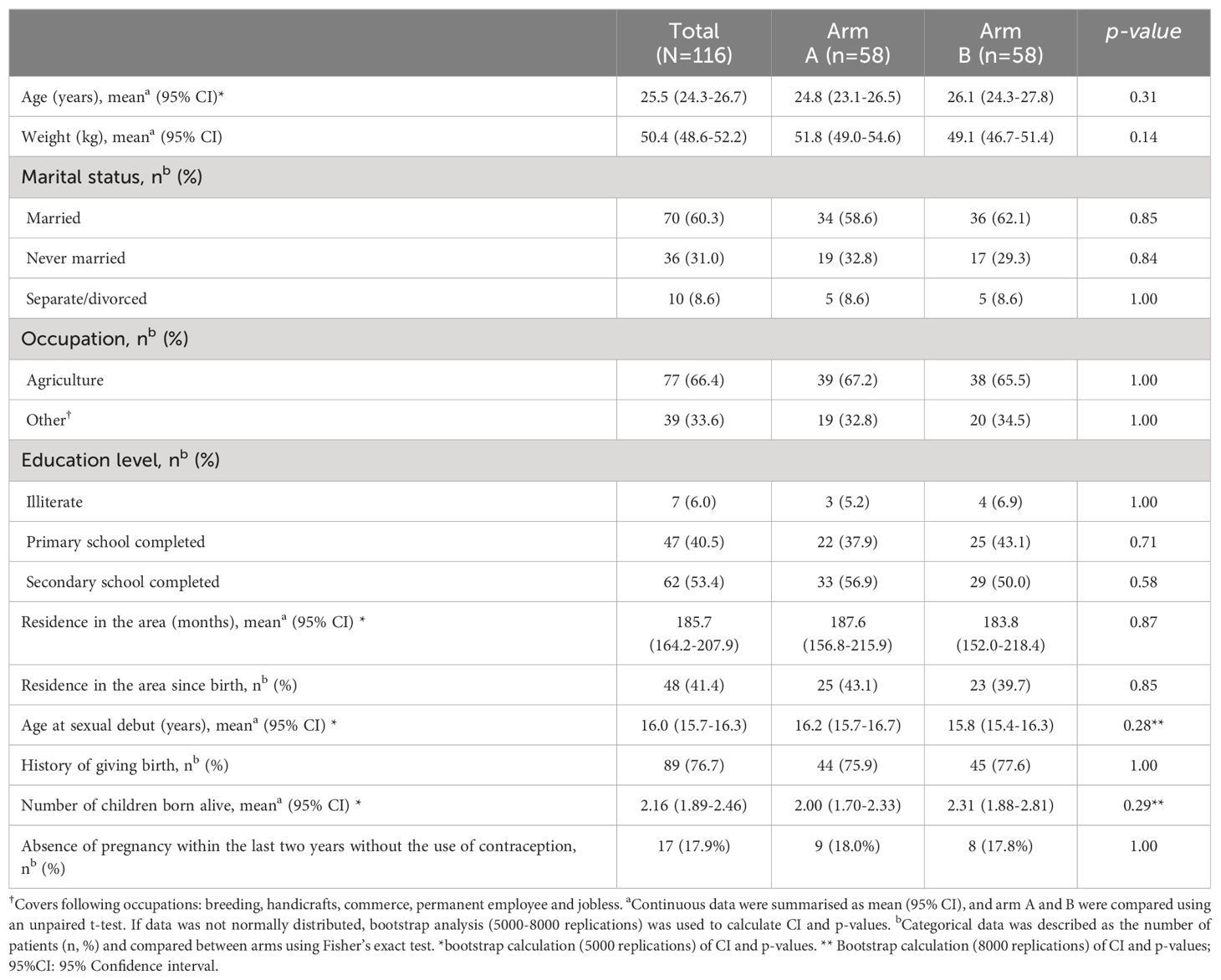
Table 2. Socio-demographic and reproductive health history characteristics of the study participants at baseline.
Participants eligible for final assessment of study outcomes
At the completion of clinical assessments at baseline, a single dose of PZQ was administered to all 58 women in Arm A (Supplementary Table 1). Eight participants failed to appear for follow-up at Week 15, leaving 50 women available for the final data analysis in Arm A (Figure 1). Dosing of PZQ three times within 24 hours was administered to the 58 women in Arm B at the end of the completed clinical assessment at baseline. As the third dose was not administered to one participant due to moderate vomiting after the second dose (12 hours after the initial dose), she was excluded from the final analysis. Hence, 57 women in Arm B received the complete PZQ dosage regimen at baseline as per the study protocol (Supplementary Table 1). Seven women failed to meet for the Week 5 session, and one woman was excluded from the study due to pregnancy. At Week 10, three women failed to appear for the treatment session; and with one further woman excluded from the study due to pregnancy, 45 women were available for the final data analysis in Arm B (Figure 1). Hence, a total of 95 women were included in the final per-protocol data analysis.
Cervical lesions
Due to suboptimal image quality in some instances, our assessment for the baseline evaluation was limited to 91 images (47 in Arm A, 44 in Arm B). At baseline, grainy sandy patches were found in 100% of the RCT population of 91 women, abnormal blood vessels in 95.6%, homogenous yellow sandy patches in 83.5%, and rubbery papules in 91.2%.
Comparison of lesion scores and counts showed no statistically significant differences between arms at baseline and at follow-ups at Weeks 5, 10, and 15 (Figure 2). Evaluating changes in CLP scores from baseline to the three follow-up visits, we observed a significant reduction in Arm B at Week 10 (p=0.001) (Figure 2). For both treatment arms, significant reductions in RPC were observed between baseline and all three time points, except between Arm A at baseline and Week 10 (p=0.10) and between Arm B at baseline and Week 15 (p=0.21). Regarding HSP, we noticed a significant reduction from baseline to Week 5 (p=0.010) in Arm B; a reduction which did not meet statistical significance at Week 10 (p=0.10) and Week 15 (p=0.15). There were no significant differences in HSP from baseline to any of the three follow-up visits for Arm A. In the same arm, we observed a significant reduction in GSP between baseline and Week 5 (p=0.005), while no significant changes were noted at Weeks 10 or 15. Similarly, no significant changes were observed in Arm B during any of the follow-up assessments. BVP showed no significant changes in either Arm A or B.
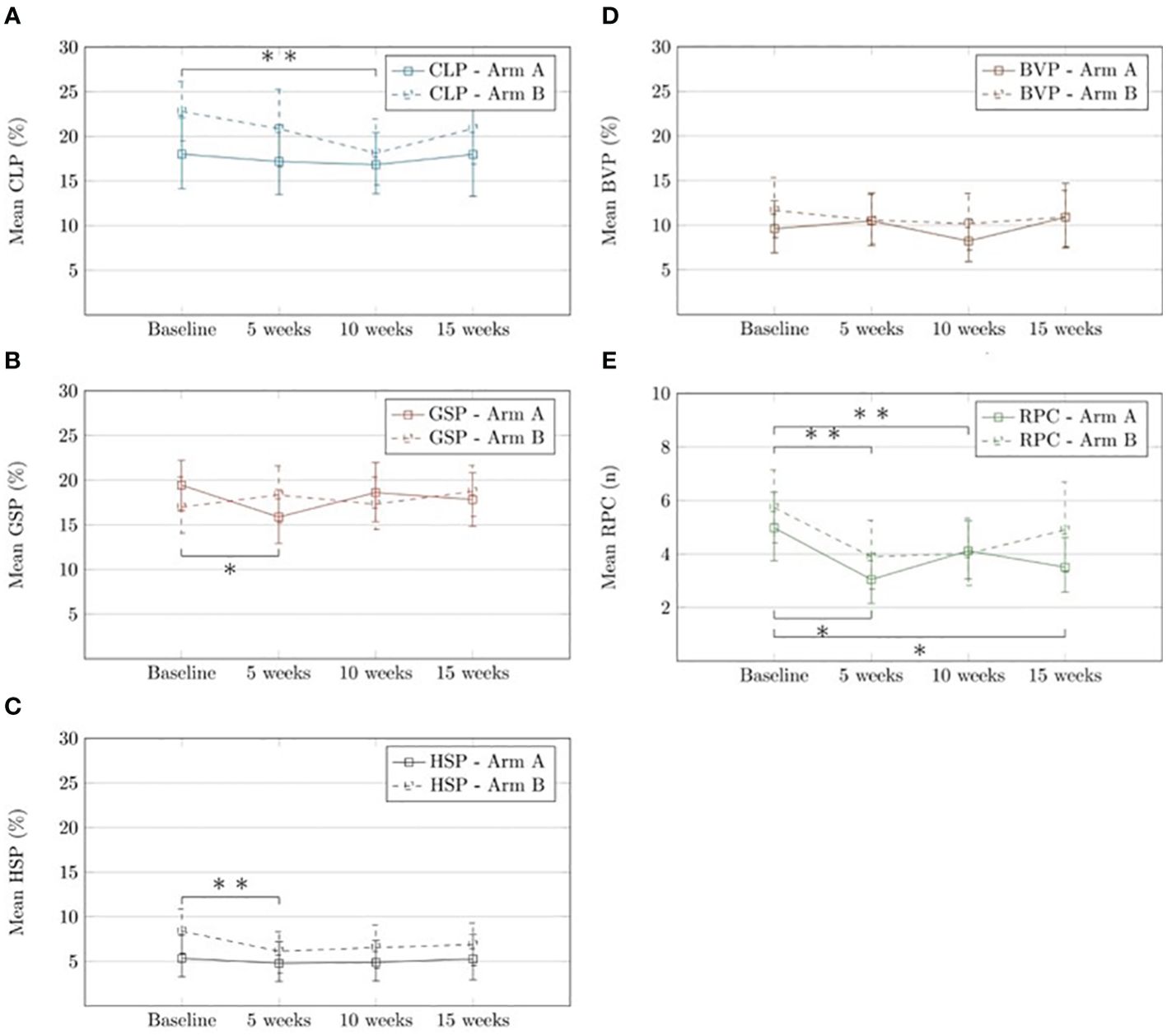
Figure 2. Mean values of cervical lesion parameters for baseline, week 5, week 10 and week 15 in arm (A) and arm (B) study groups A: Mean CLP (%). B: Mean GSP (%). C: Mean HSP (%). D: Mean BVP (%). E: Mean RPC (n). Data were summarised as mean (95% CI), and comparisons between arm A and arm B were conducted using unpaired t-test. Since data were not normally distributed, the bootstrap calculation (5000 replications) of Cl and p-values was used. For comparison between each time point, a paired t-test was used. Since data was not normally distributed the bootstrap calculation (3000 replications) of Cl and p-values was used. *Significant difference in mean value between baseline and follow-up timepoint for arm (A). **Sigificant difference in mean value between baseline and follow-up timeport for arm (B). Number of images applicable for assessment. Arm (A) baseline, n = 47 week 5, n = 43 week 10, n = 42 week 15, n = 45 Arm (B): baseline, n = 44, week 5, n=44, week 10, n = 43 week 15, n = 42. CLP, Cervical lesion proportion; GSP, Grainy sundy patches proportion; HSP, Homogeneous yellow sandy patches proportion; BVP, Abnormal blood vessel proportion; RPC, Rubbery papules count; 95% CI, 95% Confidence interval.
Pelvic exam abnormalities
Bleeding (upon instrumental contact or spontaneous) and epithelial disruption were the two main categories of abnormality observed in the women during the pelvic exam at baseline (Table 3). Both abnormalities had declined at Week 15 follow-up. However, in neither of the two treatment arms nor in the overall RCT population did the data reach statistical significance. Tenderness during the pelvic exam was reported by 39.6% of the women, either in relation to cervical motion (n=24), the uterus (n=18), or the adnexa (n=16). Cervical motion tenderness declined significantly in both treatment arms (p<0.01). A similar decline was observed in relation to uterine tenderness in Arm A (p=0.07) and in Arm B (p<0.01), and adnexal tenderness in Arm A (p=0.04).
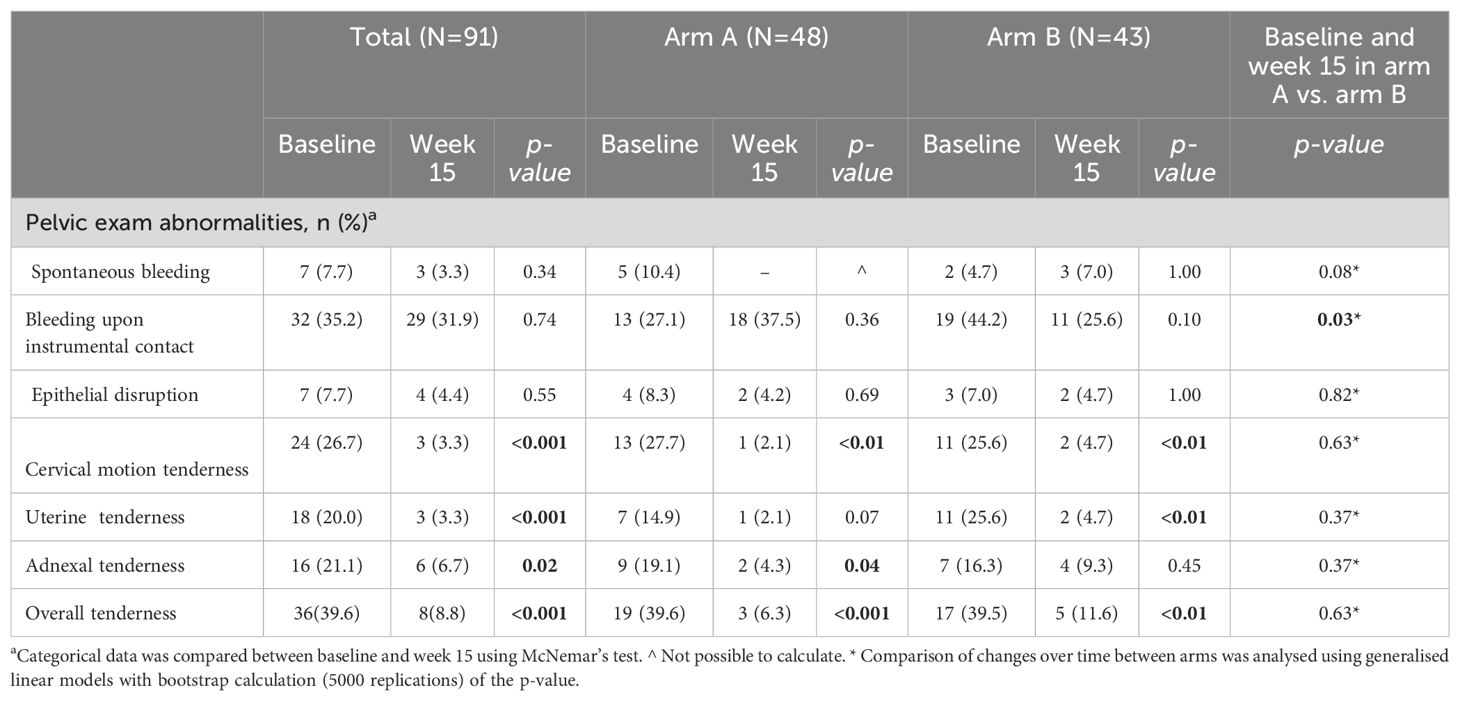
Table 3. Pelvic exam abnormalities at baseline in comparison to week 15 follow-up.
Urogenital complaints
Lower abdominal pain emerged as the most prevalent complaint reported by 53.7% of the women at baseline, followed by smelly vaginal discharge (48.4%), vulvovaginal itching (47.4%), sexual intercourse pain/abnormal sensation (47.4%), irregular menstruation (37.8%), abnormal colour of vaginal discharge (37.8%), painful micturition (30.5%), abnormal vulvovaginal sensation (23.3%), spontaneous bleeding episodes (15.8%), and bleeding after sexual intercourse (7.4%). A clear pattern of decline in urogenital complaints was observed from baseline to Week 15-follow-up in both treatment arms (Table 4). It is noteworthy that only Arm B, in contrast to Arm A (p=0.30), saw a statistically significant decline in reported irregular menstruation (p<0.001).
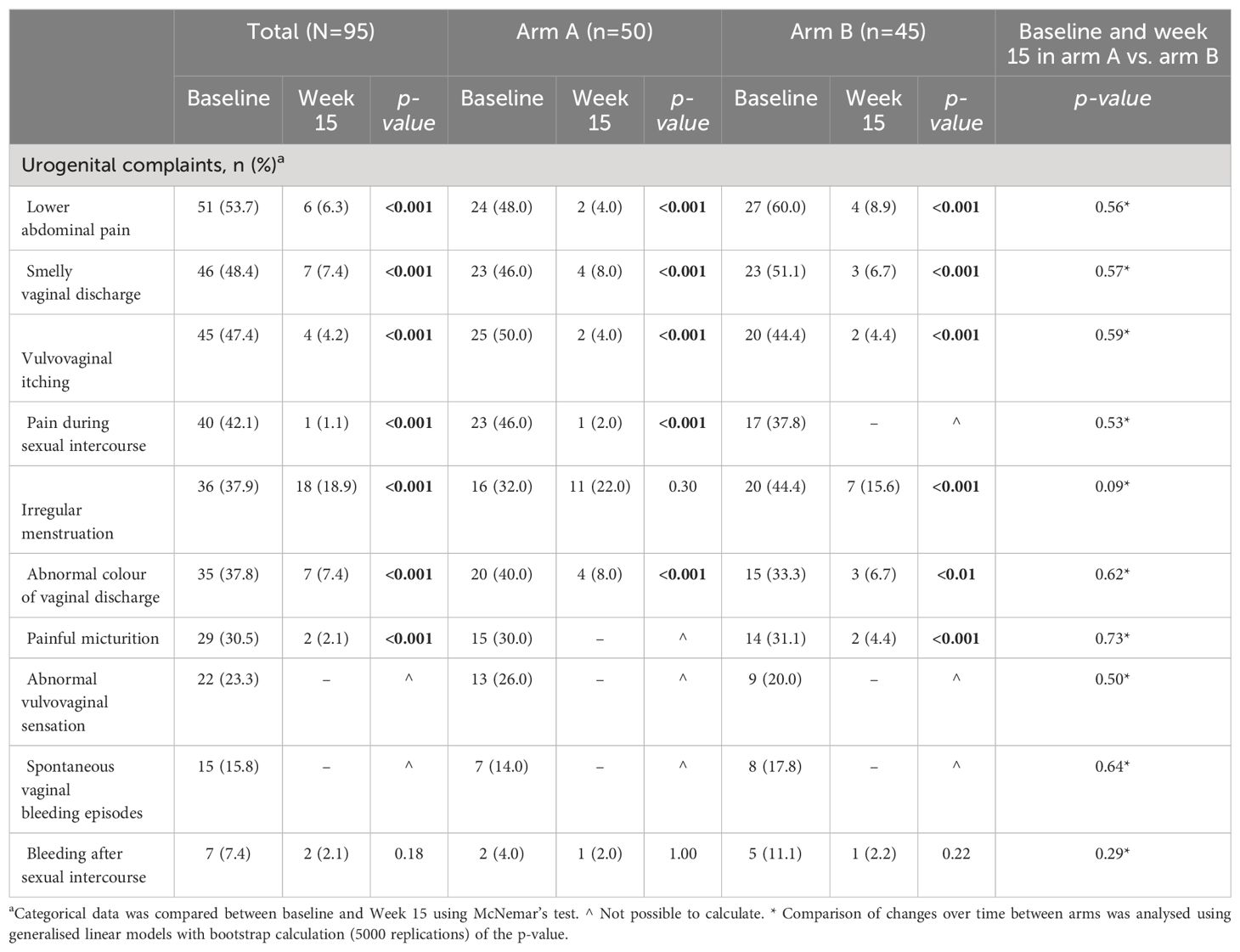
Table 4. Urogenital complaints at baseline in comparison to week 15 follow-up.
Schistosoma biomarkers
Nine women (18.8%) in Arm A and five women (11.6%) in Arm B were positive for cervicovaginal S. haematobium DNA at baseline. By Week 5, two women in Arm A remained positive for S. haematobium DNA (clearance rate 77.8%). Although no women in Arm B were positive (clearance rate 100%), the clearance rate between the two treatment arms failed to reach statistically significant difference (p=0.396). None of the initially DNA-positive women were positive at Week 15 (100% cure rate). Two women in Arm A (4.2%) and one woman in Arm B (2.3%) had positive findings of cervicovaginal S. haematobium DNA by Week 15 despite having tested negative at the previous two visits.
Overall, 74.7% of the women tested positive for CAA in serum at baseline. The proportion of women testing positive for CAA in serum showed a statistical significant decrease in Arm B compared to Arm A at all follow-up visits (Figure 3). Both arms exhibited a reduction in mean CAA levels, with Arm B showing a notably statistical significant decrease compared to Arm A at Week 10 (p=0.02) and a nearly significant reduction at Week 15 (p=0.08) (Figure 3).
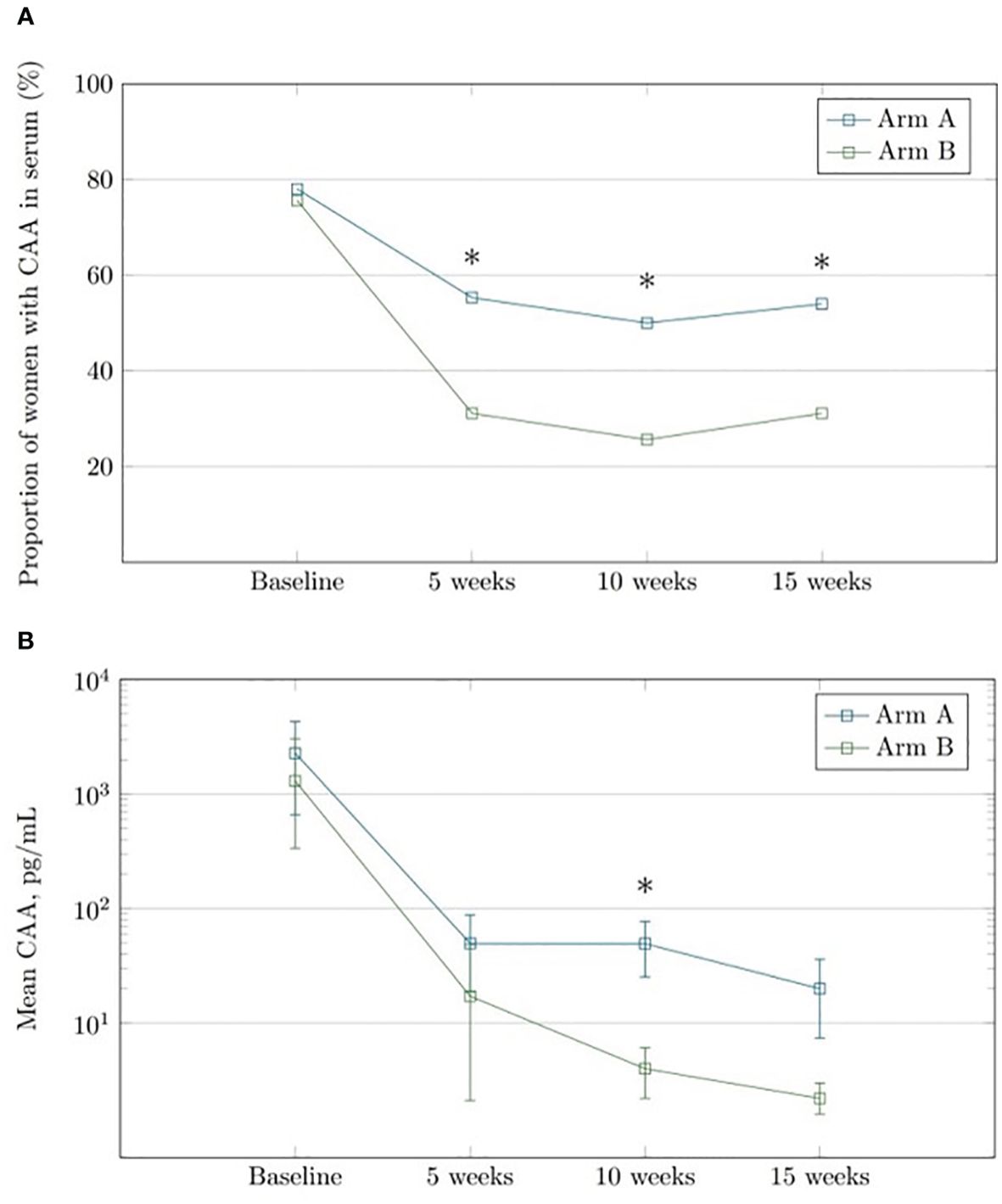
Figure 3. The changes from the baseline to the follow-up in circulating anodic cationic antigens (CAA) among the women in the two treatment arms. (A) Changes in the proportion of women positive for CAA in serum at baseline, Week 5, Week 10 and Week 15, respectively. Comparison between Arm A and Arm B using Fisher's exact test (B). Mean CAA values (pg/ml) in women positive for CAA in serum at baseline, week 5, week 10 and week 15. Comparison between arm A and arm B using unpaired t-test with bootstrap calculation (5000 replications) of Cl and p-values. *Significant difference between arm A and armB.
In Arm A, 38 women (76.0%) were found to have S. haematobium eggs in their baseline urine samples; three women remained positive at Week 15 (6.0%) with a clearance rate of 92.1%. In Arm B, the baseline urine samples from 31 women (68.9%) contained eggs; none were positive at Week 15 (100% clearance rate), with no significant difference between treatment arms (p=0.161). The mean egg count decreased from an initial range of 38.7 (18.7–66.1) to 4.0 (1.0–7.0) in Arm A (p=0.08), in Arm B from 42.5 (15.6–76.0) to 0 (p-values not computable). There was no significant difference in egg count reduction between the two treatment arms (p=1.00).
Stool findings
While none of the women were positive for Schistosoma mansoni eggs in the stool, our findings revealed the presence of other intestinal parasites. Three women (2.6%) were infected with Ankylostoma duodenale, and single cases (each accounting for 0.9%) of Ascaris lumbricoides, Trichuris trichiura, Entamoeba hystolytica, and Hymenolepis nana were identified. Anti-helminthic treatment was administered to women with positive stool findings.
Eosinophilia
In Arm A, we noticed an increase in the blood eosinophil percentage from 6.98 at baseline to 7.38 at Week 15. In contrast, Arm B showed a decrease in the eosinophil percentage from 7.24 at baseline to 5.82 at Week 15. However, it should be highlighted that none of the changes were statistically significant when comparing the two time points within each group (Arm A: p=0.706, Arm B: p=0.181) and the two treatment arms (p=0.225).
Sexually transmitted infections and bacterial vaginosis
Five women were diagnosed with T. pallidum infection at baseline (Table 5). Moreover, 45.2% and 4.3% of the women were diagnosed with HPV and HSV, respectively, while 39.3% were diagnosed with either N. gonorrhoea, C. trachomatis, M. genitalium, or T. vaginalis. At Week 15-follow-up, the overall percentage of the four latter pathogens had risen to 46.1%. The number of women diagnosed with BV likewise increased from baseline to follow-up at Week 15, from 16 (18.2%) to 35 women (39.8%) (Table 5). At no time was a statistically significant difference observed between the arms. For an overview of the medications administered to the women due to STI symptoms or positive field laboratory test results, see Supplementary Table 2.
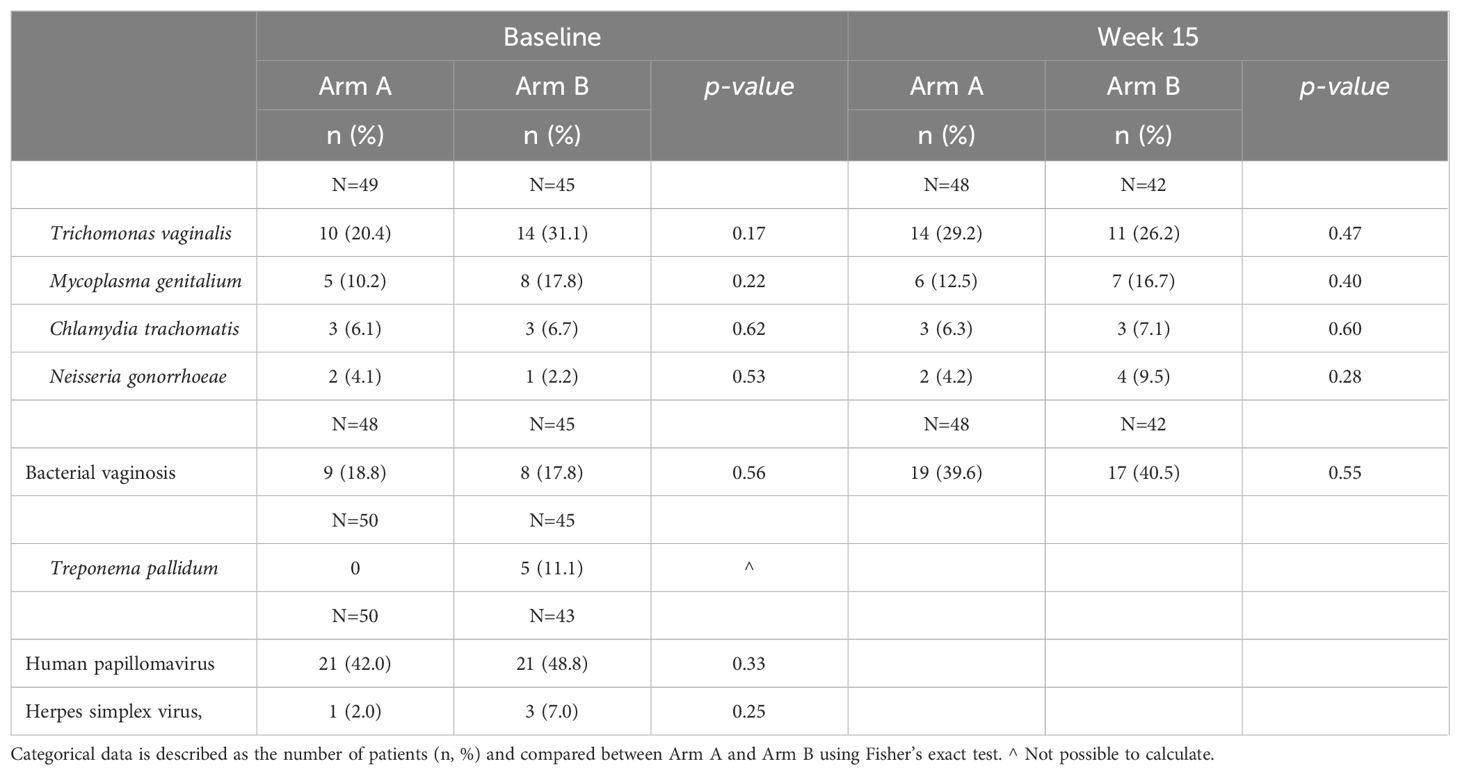
Table 5. Sexually transmitted infections and bacterial vaginosis in the study participants at the baseline and the week 15 follow-up.
Outcomes in women with no sexually transmitted infection or bacterial vaginosis
Since STIs and bacterial vaginosis BV can mimic the symptoms and signs of FGS, it is important to assess the outcome measures in women without these conditions. Among 16 women (8 in each treatment arm), no STI or BV was detected during any visit from baseline to Week 15. There was no significant difference between the two treatment arms regarding cervical lesions, urogenital complaints, or pelvic exam abnormalities (Supplementary Tables 3, 4).
Safety
Overall, no major adverse events were observed in either of the two treatment arms, all events being registered as potentially related to the PZQ treatment (Supplementary Table 5). In Arm A, mild to moderate events were registered in 22 women (37.9%) after baseline treatment. The most frequent symptom was elevated ALT levels, 17 women testing above the upper normal limit (29.3%). Five of the 17 women with elevated post-treatment ALT levels had already exhibited elevated ALT levels before administration of the PZQ treatment. In Arm B, the majority of adverse events were recorded after administration of the 12-hour dose. Vomiting was the predominant symptom reported (12.1%) for all women. In Arm B, seven women (12.1%) displayed elevated levels of ALT 24 hours after the first treatment administration. Elevated ALT levels had also been detected prior to PZQ treatment in five individuals. We found no significant changes in mean levels of ALT and bilirubin between the two arms at baseline; neither was this the case from baseline to Week 15-follow-up in any of the treatment arms.
Discussion
To our knowledge, this is the first RCT to evaluate a repeated PZQ regimen for the treatment of FGS in comparison to the standard PZQ single-dose regimen as currently recommended by the World Health Organization (50). Having clinical implications in particular for reproductive health, FGS may require a different therapeutic approach than is normally practiced for urinary schistosomiasis in large-scale morbidity control programmes.
Only a few observational studies have evaluated post-treatment outcomes in women with FGS using a PZQ standard regimen of 40mg/kg (3, 51). Kjetland et al. found no association between PZQ treatment and significant reduction in genital lesions at 12-month follow-up (11). A similar finding was made in this RCT. Neither CLP nor the three specific lesion-type proportions had declined significantly at 15- week follow-up in any of the two treatment arms. However, RPC did show a significant decline but only in the group of women who received the PZQ standard regimen. We moreover found significantly lower proportions for most of the specific lesion types and CLP when comparing findings at Week 5 and/or at Week 10 with baseline findings. However, the significant reduction seemed to have diminished by Week 15, a tendency that may be attributed to potential reinfection with S. haematobium during the study period and the maturing of the early parasitic stages into adult worms, causing new lesions to develop.
Rubbery papules probably represent a cervical lesion type of more recent pathogenetic origin than the other three lesion types. In contrast, grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels are characterised by long-term chronicity spanning years or decades since early childhood (10). As a result, it may be anticipated that the three lesion types tend to become refractory to PZQ treatment. PZQ having killed the adult Schistosoma worms dwelling in the pelvic region, the influx and disposition of new eggs in the urogenital organs are reduced. As a result of this immediate treatment outcome, the egg-induced inflammatory processes in the affected tissue may diminish, thus allowing a certain extent of spontaneous healing. However, the common occurrence of reinfection in endemic areas means that the treated women experience only temporary benefits. While PZQ treatment may cause some resolution of rubbery papules at Week 15, even when the drug is administered in a single-dose regime, no major clinical impact should necessarily be expected due to the relatively insignificant contribution of rubbery papules to the overall burden of FGS-associated vaginocervical pathology and morbidity.
We note that the follow-up evaluation in the RCT was performed 15 weeks after baseline, leaving relatively little time for the healing of grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels. It cannot be ruled out that the final evaluation of the effect of the repetitive PZQ treatment regimen on the resolution of the three lesion types, some of which may endure for years, requires more than 15 weeks to follow-up. However, even in a best-case scenario, this would probably evidence only partial resolution of the lesions. Such marginal improvement is to be expected in view of the findings reported by Kjetland et al. from their 12-month follow-up study (11). The findings of our RCT provide a relevant supplement to the findings of the previous study as our digital gridded image technique assessment of lesions was purely quantitative. While this tool provides opportunities for more detailed insights into the resolution of the different cervical lesions, it likewise contributes to our understanding of the natural history of FGS.
Concerning pelvic exam abnormalities, no significant improvement of the two vaginal bleeding parameters (bleeding upon instrumental contact and spontaneous bleeding) was observed in this RCT, neither in the overall trial population nor in the two treatment arms. However, the women who received the repeated PZQ-dosing treatment (Arm B) experienced a near-significant improvement relating to bleeding upon instrumental contact. Moreover, for all three categories (cervical motion, uterine, and adnexal tenderness) the entire trial population reported fewer tenderness complaints during the pelvic exam, thus giving evidence of a significant decline from baseline to follow-up. In general, we found a significant decline in urogenital complaints by the women at Week 15-follow-up. Even though FGS-associated cervical lesions appear refractory to PZQ treatment, we believe that the observed improvements for both pelvic exam abnormalities and for urogenital complaints promise potential benefits for women’s reproductive health. The observed pattern of decline in pelvic exam abnormalities and urogenital complaints in conjunction with PZQ treatment suggests causality between FGS and the gynaecological manifestations. This observation supports the therapeutic effect of PZQ as part of the overall FGS morbidity control strategy, even if only partial resolution of the chronic cervicovaginal was achieved.
We note that the pattern of clinical improvements occurred despite the fact that the prevalence of STI and BV at Week 15-follow-up remained high, and was at an even higher level compared to baseline. STI and BV may, along with S. haematobium infection, also have contributed to the observed gynaecological manifestations. Uncertainty thus remains in relation to the apparent discrepancy between the significant decline in vaginal discharge complaints in the women at follow-up, even though vaginal discharge is strongly associated with STI and BV, both of which were even more prevalent in Week 15 compared to baseline.
Given the substantial overlap of symptoms and clinical findings between STI and FGS, it may have been advantageous to exclude women with STI and/or BV. However, because of the high prevalence of STI among women with FGS, we opted to test the repeated-dosing regimen in the general population rather than excluding those with STI and/or BV. To address the symptom and sign overlap between FGS and STIs/BV, all clinical outcome analyses were conducted in the subset of women without STIs or BV (eight in each treatment arm). These analyses did not provide stronger evidence for the efficacy of the repeated dose regimen.
During the study period, the frequency and mean values of the three Schistosoma biomarkers saw a significant decline, verifying the effect of PZQ treatment on S. haematobium infection in general, and FGS specifically, as demonstrated by the reduction in the proportion of women detected positive for cervicovaginal S. haematobium DNA. We also note our observation in Arm B of a significantly lower percentage of women with CAA in serum compared to Arm A and likewise a significantly lower CAA mean value at Week 10 in Arm B. These findings suggest that the repeated PZQ dosing regimen is more effective in reducing the Schistosoma worm burden compared with the standard single-dose regimen.
Neither the cervical lesions nor the pelvic exam abnormalities nor the Schistosoma biomarker findings in this RCT provides convincing support for replacing the standard PZQ single-dose regimen with a repeated PZQ-dose regimen. The implementation of repeated dosing across sub-Saharan Africa would prove difficult when considered in the larger context of FGS morbidity control and separated from the existing and well-integrated single-dose PZQ strategy directed at all those infected with S. haematobium, irrespective of age and sex. Rather, we believe that by commencing treatment of girls and boys very early in life with regular intervals and maintaining the strategy continuously into adulthood, this egg-induced pathology may be prevented from establishing a level of severity and chronicity by which adequate resolution of pathology is no longer achievable by PZQ as observed in our trial.
This RCT has some limitations. Firstly, the effect of treatment was evaluated only by assessment of FGS-associated lesions of the cervix. A more complete investigation of pathology resolution in the cervicovaginal mucosa lining after PZQ treatment may have been obtained by simultaneously procuring data for similar lesion types in the vagina. Using the cervical lesion approach as a proxy for a broader spectrum of FGS-associated pathology in the lower genital tract means that interpretation of the conclusions of the RCT should bear this limitation in mind.
Secondly, as the study population was selected to comprise only women with FGS-associated lesions, the secondary-effect outcomes of PZQ treatment do not allow a comprehensive interpretation in relation to pelvic exam abnormalities and urogenital complaints because women with FGS, not being detected with FGS-associated cervical lesions, were not included in the study.
Thirdly, our failure to convince the participants to refrain from vulvovaginal cleaning before the pelvic exam means that their urogenital complaints concerning abnormal vaginal discharge could not be compared with the objective findings of the pelvic exam.
Fourthly, rather than the chosen three-month exclusion criterion of women treated with PZQ prior to baseline, a six-to-twelve-month interval would have been more appropriate. However, constraints on availability and economy and the absence of a mass drug program targeting adults mean that few of the women in the study area receive treatment for schistosomiasis. Moreover, randomising the women have further alleviated this concern, and as evidenced by the baseline data demonstrating comparability among women in the two treatment arms.
The trial further carries a risk of bias since neither the participants nor the research team in Madagascar were blinded to arm allocation or visit. While a double-blinded study would have been advantageous, logistical constraints in the field made this unfeasible, primarily due to the limited number of investigators in the remote rural setting of the study, where medication and examination were conducted by the same physician. However, blinding in the evaluation of cervical lesions, our primary study outcome, was secured by a setup ensuring that assessors had no knowledge of group allocation or visit number.
The discrepancy in follow-up durations between the two treatment arms should also be noted. Women in the single-treatment Arm A had a 15-week interval from baseline treatment to final assessment. In contrast, the repeated-treatment Arm B had only a 5-week gap from the last dose of PZQ to the final assessment at Week 15, allowing a longer period for potential reinfection with S. haematobium. This may have contributed to a higher incidence of reinfection and subsequent positive biomarker results among women in Arm A.
Conclusions
The findings of this RCT yield inadequate support for replacing the PZQ single-dose regimen with a repeated-dosing regimen for treating gynaecological manifestations associated with FGS. Neither the pelvic exam abnormalities nor specific cervicovaginal lesions nor the urogenital complaints as observed at the Week 15-follow-up support a repeated-dosing regimen. Overall, as the cervical lesions in women with FGS appear refractory to PZQ treatment, this constitutes an imperative call for regular mass-retreatment strategy starting early in life for girls and boys living in Schistosoma-endemic areas to prevent chronic pathology and establish a level at which resolution by PZQ treatment is no longer an option. Finally, the RCT has confirmed the frequent co-existence of STI and BV in women with FGS. This finding is essential when developing syndromic treatment strategies for the healthcare management of women with urogenital complaints living in Schistosoma-endemic areas.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was carried out in accordance with the Declaration of Helsinki and the Guideline for Good Clinical Practice. The studies involving humans were approved by Committee of Ethics at the Ministry of Health in Antananarivo (Comité d’Ethique de la Recherche Bio-Médicale auprès du Ministère de la Santé Publique); (Authorization Number: 098-MSANP/CERBM; Number: 059-MSANP/CERBM; Number: 065 MSANP/SG/-AGMED/CNPV/CERBM). The study was registered at clinicaltrials.gov (NCT04115072). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was required from all the participants. Girls can be affected by FGS since pre-puberty, and life-threatening sequels of FGS may already occur at an adolescent age, therefore we considered it unethical to exclude women 15-17-years old from the study. To respect confidentiality of these adolescent participants, the informed consent of a third party (parent or legal guardian) was not asked for. The Ethics committee approved this procedure.
Author contributions
LA: Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing, Investigation, Data curation. BR: Conceptualization, Investigation, Writing – review & editing. TR: Conceptualization, Writing – review & editing, Investigation. CR: Investigation, Writing – review & editing, Conceptualization. KJ: Investigation, Writing – review & editing, Formal analysis, Methodology, Data curation, Validation. KK: Investigation, Methodology, Writing – review & editing. DB: Writing – review & editing, Formal analysis, Project administration, Validation. CB: Writing – review & editing, Investigation. SS: Investigation, Writing – review & editing. ML: Writing – review & editing, Data curation, Formal analysis. MJ: Data curation, Formal analysis, Writing – review & editing. SL: Data curation, Formal analysis, Writing – review & editing. JJ: Formal analysis, Writing – review & editing, Investigation, Methodology. PC: Formal analysis, Investigation, Writing – review & editing, Methodology. PH: Formal analysis, Writing – review & editing, Investigation, Methodology. GJ: Formal analysis, Investigation, Methodology, Writing – review & editing. NK: Formal analysis, Investigation, Methodology, Writing – review & editing. SH: Formal analysis, Investigation, Writing – review & editing. PL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declare that this study received funding from Merck KGaA, 250 Frankfurters Strasse, 64293, Darmstadt, Germany (Funder's Study ID Number: MS200157-0021). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors wish to express their sincere gratitude to the following individuals and Organizations for their invaluable contributions and support of the research study: Prof. Dr. Hermann Feldmeier, Institute of Microbiology and Infection Immunology, Charité-Universitätsmedizin Berlin, corporate member of Freie Universtät Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany, Clara Fabienne Rasoamanamihaja, Paulin Ramasy Manjary, and Bemarivo Jeannoé Assany, Ministry of Health, Antananarivo, Madagascar, Kristine Brøndbjerg Øby and Maria Jensen, Centre for Clinical Research, North Denmark Regional Hospital, Denmark.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1322652/full#supplementary-material
References
1. Lai YS, Biedermann P, Ekpo UF, Garba A, Mathieu E, Midzi N, et al. Spatial distribution of schistosomiasis and treatment needs in sub-Saharan Africa: a systematic review and geostatistical analysis. Lancet Infect Dis. (2015) 15:927–40. doi: 10.1016/S1473-3099(15)00066-3
2. Orish VN, Morhe EKS, Azanu W, Alhassan RK, Gyapong M. The parasitology of female genital schistosomiasis. Curr Res Parasitol Vector Borne Dis. (2022) 2:100093. doi: 10.1016/j.crpvbd.2022.100093
3. Odegaard JI, Hsieh MH. Immune responses to Schistosoma haematobium infection. Parasite Immunol. (2014) 36:428–38. doi: 10.1111/pim.12087
4. Helling-Giese G, Kjetland E, Gundersen S, Poggensee G, Krantz I, Feldmeier H. Schistosomiasis in women: manifestations in the upper reproductive tract. Acta Tropica. (1996) 62:225–38. doi: 10.1016/s0001-706x(96)00025-3
5. Jourdan PM, Holmen SD, Gundersen SG, Roald B, Kjetland EF. HIV target cells in schistosoma haematobium-infected female genital mucosa. Am J Trop Med Hyg. (2011) 85:1060–4. doi: 10.4269/ajtmh.2011.11-0135
6. Jourdan PM, Randrianasolo BS, Feldmeier H, Chitsulo L, Ravoniarimbinina P, Roald B, et al. Pathologic mucosal blood vessels in active female genital schistosomiasis: new aspects of a neglected tropical disease. Int J Gynec Pathol. (2012) 32:137–40. doi: 10.1097/PGP.0b013e31824fe327
7. Swai B, Poggensee G, Mtweve S, Krantz I. Female genital schistosomiasis as evidence of a neglected cause for reproductive ill-health: a retrospective histopathological study from Tanzania. BMC Infect Diseases. (2006) 6:134. doi: 10.1186/1471-2334-6-134
8. Schanz A, Richter J, Beyer I, Baldus SE, Hess AP, Kruessel JS. Genital schistosomiasis is a cause of female sterility and acute abdomen. Fertil Steril. (2010) 93:2075.e7–9. doi: 10.1016/j.fertnstert.2009.05.043
9. Ramarokoto CE, Kildemoes AO, Randrianasolo B, Ravoniarimbinina P, Ravaoalimalala VE, Leutscher P, et al. Eosinophil granule proteins ECP and EPX as markers for a potential early-stage inflammatory lesion in female genital schistomiasis (FGS). PloS Negl Trop Dis. (2014) 8:e2974.
10. Gelfand M, Ross MD, Blair DM, Weber MC. Distribution and extent of schistosomiasis in female pelvic organs, with special reference to the genital tract, as determined at autopsy. Am J Trop Med Hyg. (1971) 20:846–9. doi: 10.4269/ajtmh.1971.20.846
11. Kjetland EF, Mduluza T, Ndhlovu PD, Gomo E, Gwanzura L, Midzi N, et al. Genital schistosomiasis in women: a clinical 12-month in vivo study following treatment with praziquantel. Trans R Soc Trop Med Hyg. (2006) 100:740–52. doi: 10.1016/j.crpvbd.2022.100093
12. Downs JA, Kabangila R, Verweij JJ, Jaka H, Peck RN, Kalluvya SE, et al. Detectable urogenital schistosome DNA and cervical abnormalities 6 months after single-dose praziquantel in women with Schistosoma haematobium infection. Trop Med Int Health. (2013) 18:1090–6. doi: 10.1111/tmi.12154
13. Nour NM. Schistosomiasis: health effects on women. Rev Obstet Gynecol. (2010) 3(1):28–32. doi: 10.1371/journal.pntd.0002974
14. Kjetland EF, Poggensee G, Helling-Giese G, Richter J, Sjaastad A, Chitsulo L, et al. Female genital schistosomiasis due to Schistosoma haematobium. Clinical and parasitological findings in women in rural Malawi. Acta Trop. (1996) 62:239–55. doi: 10.1016/S0001-706X(96)00026-5
15. Kjetland EF, Ndhlovu PD, Mduluza T, Gomo E, Gwanzura L, Mason PR, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hyg. (2005) 72:311–9. doi: 10.4269/ajtmh.2005.72.311
16. Le L, Hsieh MH. Diagnosing urogenital schistosomiasis: dealing with diminishing returns. Trends Parasitol. (2017) 33:378–87. doi: 10.1016/j.pt.2016.12.009
17. Liu R, Dong HF, Guo Y, Zhao QP, Jiang MS. Efficacy of praziquantel and artemisinin derivatives for the treatment and prevention of human schistosomiasis: a systematic review and meta-analysis. Parasit Vectors. (2011) 4:201. doi: 10.1186/1756-3305-4-201
18. McManus DP, Dunne DW, Sacko M, Utzinger J, Vennervald BJ, Zhou XN. Schistosomiasis. Nat Rev Dis Primers. (2018) 4:13. doi: 10.1038/s41572-018-0013-8
19. Deka MA. Predictive risk mapping of schistosomiasis in Madagascar using ecological niche modeling and precision mapping. Trop Med Infect Dis. (2022) 7:15. doi: 10.3390/tropicalmed7020015
20. Randrianasolo BS, Jourdan PM, Ravoniarimbinina P, Ramarokoto CE, Rakotomanana F, Ravaoalimalala VE, et al. Gynecological manifestations, histopathological findings, and schistosoma-specific polymerase chain reaction results among women with Schistosoma haematobium infection: a crosssectional study in Madagascar. J Infect Dis. (2015) 212:275–84. doi: 10.1093/infdis/jiv035
21. Kjetland EF, Norseth HN, Taylor M, Lillebo K, Kleppa E, Holmen SD, et al. Classification of the lesions observed in female genital schistosomiasis. Int J Gynecology Obstetrics. (2014) 127:227–8. doi: 10.1016/j.ijgo.2014.07.014
22. World Health Organization. Female genital schistosomiasis. A pocket atlas for clinical health-care professionals. Geneva: World Health Organization (2015).
23. Holmen S, Galappaththi-Arachchige HN, Kleppa E, Pillay P, Naicker T, Taylor M, et al. Characteristics of blood vessels in female genital schistosomiasis: Paving the way for objective diagnostics at the point of care. PloS Negl Trop Dis. (2016) 10:e0004628. doi: 10.1371/journal.pntd.0004628
24. Zwingenberger K, Irschick E, Vergetti Siqueira JG, Correia Dacal AR, Feldmeier H. Tumour necrosis factor in hepatosplenic schistosomiasis. Scand J Immunol. (1990) 31:205–11. doi: 10.1111/j.1365-3083.1990.tb02761.x
25. Zwingenberger K, Irschick E, Siqueira Vergetti JG, Correia Dacal AR, Janssen-Rosseck R, Bienzle U, et al. Release of interleukin 2 and gamma interferon by peripheral mononuclear cells in human Schistosoma mansoni infection normalises after chemotherapy. Scand J Immunol. (1989) 30:463–71. doi: 10.1111/j.1365-3083.1989.tb02451.x
26. Feldmeier H, Gastl GA, Poggensee U, Daffalla AA, Nogueira-Queiroz JA, Capron A, et al. Immune response in chronic Schistosomiasis haematobium and mansoni. Reversibility of alterations after anti-parasitic treatment with praziquantel. Scand J Immunol. (1988) 28:147–55. doi: 10.1111/j.1365-3083.1988.tb02426.x
27. Hailegebriel T, Nibret E, Munshea A. Efficacy of praziquantel for the treatment of human schistosomiasis in Ethiopia: A systematic review and meta-analysis. J Trop Med. (2021) 2021:2625255. doi: 10.1155/2021/2625255
28. Bustinduy AL, Waterhouse D, de Sousa-Figueiredo JC, Roberts SA, Atuhaire A, Van Dam GJ, et al. Population pharmacokinetics and pharmacodynamics of praziquantel in Ugandan children with intestinal schistosomiasis: higher dosages are required for maximal efficacy. mBio. (2016) 7(4):e00227-16. doi: 10.1128/mBio.00227-16
29. Xiao SH, Sun J, Chen MG. Pharmacological and immunological effects of praziquantel against Schistosoma japonicum: a scoping review of experimental studies. Infect Dis Poverty. (2018) 7:9. doi: 10.1186/s40249-018-0391-x
30. Xiao SH, Catto BA, Webster LT Jr. Effects of praziquantel on different developmental stages of Schistosoma mansoni in vitro and in vivo. J Infect Dis. (1985) 151:1130–7. doi: 10.1093/infdis/151.6.1130
31. Cioli D, Pica-Mattoccia L. Praziquantel. Parasitol Res. (2003) 90 Supp 1:S3–9. doi: 10.1007/s00436-002-0751-z
32. Costain AH, MacDonald AS, Smits HH. Schistosome egg migration: mechanisms, pathogenesis and host immune responses. Front Immunol. (2018) 9:3042. doi: 10.3389/fimmu.2018.03042
33. Schuster A, Randrianasolo BS, Rabozakandraina OO, Ramarokoto CE, Brønnum D, Feldmeier H. Knowledge, experiences, and practices of women affected by female genital schistosomiasis in rural Madagascar: A qualitative study on disease perception, health impairment and social impact. PloS Negl Trop Dis. (2022) 16:e0010901. doi: 10.1371/journal.pntd.0010901
34. Arenholt LTS, Aaroe KK, Norderud K, Lumholdt M, Randrianasolo BS, Ramarokoto CE, et al. Cervical lesion proportion measure using a digital gridded imaging technique to assess cervical pathology in women with genital schistosomiasis. PloS Negl Trop Dis. (2022) 16:e0009995. doi: 10.1371/journal.pntd.0009995
35. Dragsbæk SJ, Carstens SK, Østergaard IS, Jøker K, Randrianasolo BS, Leutscher P, et al. Measurement of cervical grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels proportions in women with female genital schistosomiasis – a clinical validation study of the digital gridded imaging technique. Front Trop Dis. (2024). under submission. doi: 10.3389/fitd.2024.1322696
36. Obeng BB, Aryeetey YA, de Dood CJ, Amoah AS, Larbi IA, Deelder AM, et al. Application of a circulating-cathodic-antigen (CCA) strip test and real-time PCR, in comparison with microscopy, for the detection of Schistosoma haematobium in urine samples from Ghana. Ann Trop Med Parasitol. (2008) 102:625–33. doi: 10.1179/136485908X337490
37. Tanaka M, Kildemoes AO, Chadeka EA, Cheruiyot BN, Sassa M, Moriyasu T, et al. Potential of antibody test using Schistosoma mansoni recombinant serpin and RP26 to detect light-intensity infections in endemic areas. Parasitol Int. (2021) 83:102346. doi: 10.1016/j.parint.2021.102346
38. Corstjens PLAM, de Dood CJ, Knopp S, Clements MN, Ortu G, Umulisa I, et al. Circulating anodic antigen (CAA): A highly sensitive diagnostic biomarker to detect active Schistosoma infections-improvement and use during SCORE. Am J Trop Med Hyg. (2020) 103:50–7. doi: 10.4269/ajtmh.19-0819
39. Corstjens PL, De Dood CJ, Kornelis D, Fat EM, Wilson RA, Kariuki TM, et al. Tools for diagnosis, monitoring and screening of Schistosoma infections utilising lateral-flow based assays and upconverting phosphor labels. Parasitology. (2014) 141:1841–55. doi: 10.1017/S0031182014000626
40. Feldmeier H, Bienzle U, Dietrich M, Sievertsen HJ. Combination of a viability test and a quantification method for Schistosoma haematobium eggs (filtration–trypan blue-stainingtechnique). Tropenmed Parasitol. (1979) 30:417–22.
41. Wang LC. Improvement in the identification of intestinal parasites by a concentrated Merthiolate-iodine-formaldehyde technique. J Parasitol. (1998) 84:457–8. doi: 10.2307/3284514
42. Westh H, Jensen JS. Low prevalence of the new variant of Chlamydia trachomatis in Denmark. Sex Transm Infect. (2008) 84:546–7. doi: 10.1136/sti.2008.031906
43. Hjelmevoll SO, Olsen ME, Sollid JU, Haaheim H, Unemo M, Skogen V. A fast real-time polymerase chain reaction method for sensitive and specific detection of the Neisseria gonorrhoeae porA pseudogene. J Mol Diagn. (2006) 8:574–81. doi: 10.2353/jmoldx.2006.060024
44. Tabrizi SN, Chen S, Tapsall J, Garland SM. Evaluation of opa-based real-time PCR for detection of Neisseria gonorrhoeae. Sex Transm Dis. (2005) 32:199–202. doi: 10.1097/01.olq.0000154495.24519.bf
45. Pillay A, Radebe F, Fehler G, Htun Y, Ballard RC. Comparison of a TaqMan-based real-time polymerase chain reaction with conventional tests for the detection of Trichomonas vaginalis. Sex Transm Infect. (2007) 83:126–9. doi: 10.1136/sti.2006.022376
46. Jensen JS, Björnelius E, Dohn B, Lidbrink P. Use of TaqMan 5’ nuclease real-time PCR for quantitative detection of Mycoplasma genitalium DNA in males with and without urethritis who were attendees at a sexually transmitted disease clinic. J Clin Microbiol. (2004) 42:683–92. doi: 10.1128/JCM.42.2.683-692.2004
47. Haahr T, Humaidan P, Elbaek HO, Alsbjerg B, Laursen RJ, Rygaard K, et al. Vaginal microbiota and in vitro fertilisation outcomes: Development of a simple diagnostic tool to predict patients at risk of a poor reproductive outcome. J Infect Dis. (2019) 219:1809–17. doi: 10.1093/infdis/jiy744
48. Brusen Villadsen A, Bundgaard-Nielsen C, Ambühl L, Tang Svendsen M, Søkilde Pedersen I, Stæhr Hansen E, et al. Prevalence and type distribution of human papillomavirus infections in Danish patients diagnosed with vulvar squamous cell tumors and precursors. Gynecol Oncol Rep. (2021) 37:100828. doi: 10.1016/j.gore.2021.100828
49. Guidelines for the management of symptomatic sexually transmitted infections (2021) (Geneva: World Health Organization). Licence: CC BY-NC-SA 3.0 IGO.
50. World Health Organization. Schistosomiasis. Available online at: https://www.who.int/news-room/factsheets/detail/schistosomiasis.
51. Richter J, Poggensee G, Kjetland EF, Helling-Giese G, Chitsulo L, Kumwenda N, et al. Reversibility of lower reproductive tract abnormalities in women with Schistosoma haematobium infection after treatment with praziquantel-an interim report. Acta Trop. (1996) 62:289–301. doi: 10.1016/s0001-706x(96)00030In
Keywords: Schistosoma haematobium, female genital schistosomiasis, praziquantel, urogenital complaints, gynaecological manifestations
Citation: Arenholt LTS, Randrianasolo BS, Rabozakandraina TOO, Ramarokoto CE, Jøker K, Kæstel Aarøe K, Brønnum D, Bundgaard Nielsen C, Sørensen S, Lumholdt M, Jensen M, Lundbye-Christensen S, Jensen JS, Corstjens P, Hoekstra P, J van Dam G, Kobayashi N, Hamano S and Leutscher PDC (2024) Repeated versus single praziquantel dosing regimen in treatment of female genital schistosomiasis: a phase 2 randomised controlled trial showing no difference in efficacy. Front. Trop. Dis 5:1322652. doi: 10.3389/fitd.2024.1322652
Received: 16 October 2023; Accepted: 18 July 2024;
Published: 29 August 2024.
Edited by:
Margaret Gyapong, University of Health and Allied Sciences, GhanaReviewed by:
Evaristus Mbanefo, National Institutes of Health (NIH), United StatesValentina Marchese, Bernhard Nocht Institute for Tropical Medicine (BNITM), Germany
Copyright © 2024 Arenholt, Randrianasolo, Rabozakandraina, Ramarokoto, Jøker, Kæstel Aarøe, Brønnum, Bundgaard Nielsen, Sørensen, Lumholdt, Jensen, Lundbye-Christensen, Jensen, Corstjens, Hoekstra, J van Dam, Kobayashi, Hamano and Leutscher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louise Thomsen Schmidt Arenholt, bHRzYUBybi5kaw==