
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Trop. Dis. , 23 March 2022
Sec. Neglected Tropical Diseases
Volume 3 - 2022 | https://doi.org/10.3389/fitd.2022.850886
This article is part of the Research Topic Advances in the Molecular Epidemiology and Diagnostics of Leprosy and other Mycobacterial Diseases View all 6 articles
 Angélica Rita Gobbo1
Angélica Rita Gobbo1 Raquel Carvalho Bouth1Tania Mara Pires Moraes1
Raquel Carvalho Bouth1Tania Mara Pires Moraes1 Pablo Pinto2Patricia Fagundes da Costa1,3,4
Pablo Pinto2Patricia Fagundes da Costa1,3,4 Josafá Gonçalves Barreto1,3,5
Josafá Gonçalves Barreto1,3,5 Marco Andrey Cipriani Frade6Ândrea Kely Ribeiro-dos-Santos2,4,7Guilherme Augusto de Barros Conde8Malcolm S. Duthie9
Marco Andrey Cipriani Frade6Ândrea Kely Ribeiro-dos-Santos2,4,7Guilherme Augusto de Barros Conde8Malcolm S. Duthie9 Moises Batista da Silva1,3,4
Moises Batista da Silva1,3,4 John Stewart Spencer10
John Stewart Spencer10 Claudio Guedes Salgado1,3,4*
Claudio Guedes Salgado1,3,4*Diagnostic tests for leprosy are limited, especially to identify early leprosy cases. We performed active case findings of leprosy to validate three potential antigen candidates and one molecular target. Cases were diagnosed by characteristic skin lesions, nerve enlargement, or skin sensation loss. Serum samples obtained from all subjects were tested by ELISA to assess antibody titers to three Mycobacterium leprae specific antigens: NDO-BSA, LID-1, and NDO-LID. Most of the field cases on Mosqueiro Island, northern Brazil, also collected slit skin smear for qPCR. Active case finding diagnosed 105 new cases of leprosy out of 894 subjects (11.7%), revealing a high prevalence of M. leprae in the region. With the use of amplification of the M. leprae-specific RLEP by qPCR, 68/79 (86.07%) of these cases were positive, confirming leprosy in subjects diagnosed in the field. Patients diagnosed at the leprosy reference center showed much higher antibody titers to all three antigens, while titers of patients from the field were significantly lower. Our results support previous findings that active surveillance by experienced leprologists can diagnose additional cases based on clinical findings, that many would not be identified using ELISA assay with the available biomarkers, and that RLEP qPCR may be used to confirm the majority of the field cases.
The lack of diagnostic tools to detect early oligosymptomatic or even late well-defined cases contributes to the hidden endemic of leprosy, maintaining active foci of the disease in mostly tropical and developing countries (1). Pará state, located in the Brazilian Amazon region, is classified as hyperendemic for leprosy (29.82 new cases per 100,000 population in 2019). Considering the rate among children less than 15 years old, Pará is also classified as hyperendemic (9.60 new cases per 100,000 population), which is 3.1 times higher than Brazil’s national rate according to the National Notifiable Diseases Information System (SINAN) in 2019. Children diagnosed with leprosy are robust epidemiological indicators since the disease in people under 15 years old indicates recent disease spread and the existence of multiple active foci within communities (2). Untreated multibacillary (MB) cases are thought to be the main source of Mycobacterium leprae transmission in households (3); therefore, treatment of all diagnosed index cases and surveillance and follow-up of household contacts (HCs) are essential strategies for the early detection of leprosy cases to block transmission and to prevent irreversible nerve damage, disabilities, and deformities (4, 5).
Leprosy diagnosis is based mainly on well-accepted clinical signs/symptoms of loss of sensation on hypochromic or infiltrated skin lesions that can be accompanied by muscle weakness, nerve damage, pain, or loss of function. Since there is no laboratory diagnostic test, and detection of acid-fast bacilli is not very sensitive, molecular methods to detect M. leprae DNA in an earlobe slit skin smear (SSS) or a biopsy (6) using the repetitive element RLEP by PCR have shown promise as an early diagnostic tool (7).
The use of a simple ELISA to detect antibodies to the M. leprae-specific phenolic glycolipid I (PGL-I/NDO-BSA) antigen (8) has been in use for over 30 years. Antibody titers correlate well with the bacillary load and are almost universally positive in patients at the lepromatous end of the spectrum (borderline-lepromatous [BL] and lepromatous-lepromatous [LL]), although positive responses in paucibacillary (PB) patients are not frequent (9). Additional antigens used in serological tests include the fusion protein LID-1 (leprosy immune diagnostic 1, a combination of ML0405 and ML2331) (10), which, similar to PGL-I, detects positive responses in virtually all MB patients, and the glycoprotein NDO-LID, a combination of LID-1 and a disaccharide mimetic of PGL-I, which aim to be more sensitive than NDO-BSA (11).
Research with point-of-care (POC) tests have an increasing trend since it is an easy-to-perform method, which may allow diagnoses in the field without expert technical skills and support (12). PGL-I/NDO-BSA (12–14), LID-1 (15, 16), and NDO-LID (17–19) lateral flow assays showed feasibility to detect classic MB cases of leprosy, similar as ELISA method; however, its use for PB and, consequently, also for early leprosy cases is limited, impacting on its applicability.
Based on these findings, we decided to evaluate the antibody titers to these three antigens (NDO-BSA, LID-1, and NDO-LID) along with the molecular detection of RLEP by qPCR in leprosy patients, schoolchildren (SC), and HCs from the hyperendemic Mosqueiro Island in Pará state, Brazilian Amazon.
The present cross-sectional study was conducted on Mosqueiro Island, a district belonging to Belém, the capital of Pará state, Brazilian Amazon, which has a total population of approximately 30,000 inhabitants. The field studies were performed during a 1-week period from May 12 to 16, 2014. SC was randomly selected from four public schools (three elementary and one middle school). Newly diagnosed cases in children were followed up by visits to the households to examine HC. Blood was obtained from all SC and HC to assess antibody titers to the three different antigens. Earlobe SSSs were obtained from 79/105 new cases from the field to perform RLEP qPCR. As a control group, leprosy patients newly diagnosed at Dr. Marcello Candia Reference Unit in Sanitary Dermatology of the State of Pará (URE) located in Marituba, Pará, and their corresponding HC were examined, and blood samples were obtained.
This study conforms to the Declaration of Helsinki and was approved by the Institute of Health Sciences Research Ethics Committee from Pará Federal University (CAAE 26765414.0.0000.0018 CEP-ICS/UFPA). All individuals involved agreed voluntarily to participate and signed an informed consent form after receiving information about the study. Parents of minors or responsible adults signed their consent, allowing them to participate. All data analyzed were anonymized to protect the privacy of participants.
All subjects were examined and evaluated by experienced leprologists. The diagnosis of leprosy was based solely on well-accepted clinical signs and symptoms, including the detection of hypopigmented or infiltrated skin lesions with loss of sensation assessed with standard graded Semmes–Weinstein monofilaments (20) and the palpation of peripheral nerves to identify characteristic pain associated with inflammation or swelling. Each newly diagnosed patient was classified into one of the five clinical forms defined by Ridley–Jopling, except in cases where there was only a single hypopigmented macule without nerve involvement, indicating an early indeterminate form of leprosy. Indeterminate (I) and tuberculoid-tuberculoid (TT) forms were operationally categorized as PB, while all other forms (borderline-tuberculoid [BT], borderline-borderline [BB], BL, and LL) were grouped together as MB. Primary neural leprosy (PNL) was diagnosed if there was nerve enlargement associated with functional or sensory loss without any skin lesions. If only one nerve was affected, the case was classified as PB, whereas two or more enlarged nerves indicated MB. The DG was ranked from 0 to 2 (DG0, no disability; DG1, loss of sensation in the hand or foot; DG2, visible damage, deformity or disability) as determined during a clinical examination of sensory-motor functions based on a WHO standardized neurological evaluation (21).
All participants had blood samples collected in EDTA tubes after clinical evaluation. For antibodies titration, high-affinity polystyrene Immulon IV 96-well ELISA plates (Dynex Technologies, Chantilly, VA, USA) were coated overnight with 50 ng/50 µl of carbonate/bicarbonate sodium buffer with NDO-BSA, LID-1, or NDO-LID. The plates were blocked with blocking solution (phosphate-buffered saline [PBS], pH 7.2 with 1% bovine serum albumin [BSA], and 0.05% Tween-20 [T]) for 1 h. Serum samples were diluted 1:300 with a blocking solution and tested in duplicate for 2 h of incubation. The secondary anti-human IgM (Sigma-Aldrich, St. Louis, MO, USA, A0420) antibodies were used for NDO-BSA (dilution 1:10,000), while secondary anti-human IgG (Rockland, Gilbertsville, PA, USA, #609-1316 2 mg) were used for LID-1 (dilution 1:20,000), and both antibodies were used for NDO-LID. The reaction was developed by the insertion of an antibody conjugated with peroxidase in PBS/T for 1.5 h, and then the peroxidase color substrate o-phenylenediamine dihydrochloride (SIGMAFAST™ OPD, Sigma-Aldrich P9187, USA) was added to each well for 15 min. To stop the reaction, 50 µl/well of H2SO4 at 4 N was added and immediately read at 490 nm using an MRX Revelation 4.25 microplate reader (Dynex Technologies, Chantilly, VA, USA).
To control intra- and inter-test variations, positive (LL patient) and negative (non-endemic control [NEC]) controls were added to each plate. All samples were tested in duplicate plus a blank control well coated only with BSA.
Cutoff values were established using the mean of results plus 3 times SD of optical density (OD) of health endemic and non-endemic subjects. Results were considered from the mean of the duplicates less the blank value. Cutoff for anti-NDO-BSA and anti-LID-1 was 0.295 and for anti-NDO-LID was 0.475.
A wide range of molecular targets were evaluated for the detection of M. leprae (7); one of them is an RLEP family, which, despite a variable structure and unknown function, has 29 repetitions scattered on the M. leprae chromosome; for this reason, the RLEP region is easier to amplify, expanding the possibility of detection even with small amounts of sample (22). SSS samples of both earlobes were collected, immediately fixed in 1 ml of 70% ethanol, and stored for up to 30 days at room temperature before extraction.
DNA extraction was performed following the manufacturer’s recommendations (Qiagen DNeasy Blood and Tissue Kit, Germantown, MD, USA). RLEP detection was established with 10 ng of total DNA using 5′-GTGAGGGTAGTTGTT-3′ (LP1) and 5′-GGTGCGAATAGTT-3′ (LP2) primers (IDT, Integrated DNA Technologies, IA, USA) amplifying a 129-bp fragment detected by SYBR Green fluorescent DNA-binding dye using Applied Biosystems 7500 Real-Time PCR Systems. Each reaction was conducted in a total of 20 µl (4 μl of DNA template, 5 μl of water, 10 μl of SYBR, and 1 μl of primers). The reaction occurred with the following specifications: Uracil-DNA glycosylase (UDG) at 50°C for 2 min, prior 95°C for 2 min for initial denaturation followed by 45 cycles, each cycle consisting of denaturation at 95°C for 15 s, annealing at 58°C for 15 s and extension at 72°C for 1 min, and melting curve running in each experiment. To determine qPCR positivity, a standard curve was prepared from purified M. leprae DNA extracted from nude mouse footpads, and then five points of standard dilution (1:50, 1:100, 1:1,000, 1:2,000, and 1:5,000) of this DNA were included in each plate, plus three negative points as a template control (see Supplementary Figure 1 and Supplementary Table 1).
A melt curve was used to analyze the specificity of the amplified products. Samples were considered positive when the fluorescent signal intersected the automatically calculated threshold line. Amplifications with a cycle threshold (Ct) ≤ 45 were considered positive for RLEP. Pearson’s coefficient (r2) is calculated for each plate, and the plate results only were accepted if r2 ≥ 0.95. We perform qPCR experiments according to the MIQE checklist (see Supplementary Table 2).
A two-tailed Mann–Whitney U test was used for the comparison of antibody titers between two groups. All results were considered statistically significant when p < 0.05. To verify the antigen diagnostic performances, we calculated the area under the curve (AUC) by receiver operating characteristic (ROC) curve. The results above 0.7 were considered able to discriminate HC from patients.
This study was performed in accordance with the recommendations of the Brazilian National Ethics Committee (CONEP) guidelines approved by Pará Federal University Ethics Committee number CAAE 26765414.0.0000.0018 with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Pará Federal University Ethics Committee.
A total of 894 individuals from Mosqueiro Island were surveyed, 706 SC were examined for clinical signs/symptoms of leprosy (Figure 1), and 65 (9.2%) were SC diagnosed as a new case of leprosy (SCNC), presenting mainly hypochromic skin lesions with loss of sensation, with the number of lesions ranging from 0 to 9 (median 2). Subsequently, 188 HC of SCNC were evaluated at their homes during follow-up visits (range 1–9 and median of 2 HC per household), and 40 (21.2%) HCs were diagnosed as a new case of leprosy (HCNC). HCNC showed a median of three (range 0–21) skin lesions, and nine (22.5%) presented with disability grade 1 (DG1) (Table 1). In summary, active case finding diagnosed leprosy in 105 subjects (105/894, 11.7%), with 65 SC and 40 HC. Although 19 (18.1%) presented with DG1, there was no case with disability grade 2 (DG2).
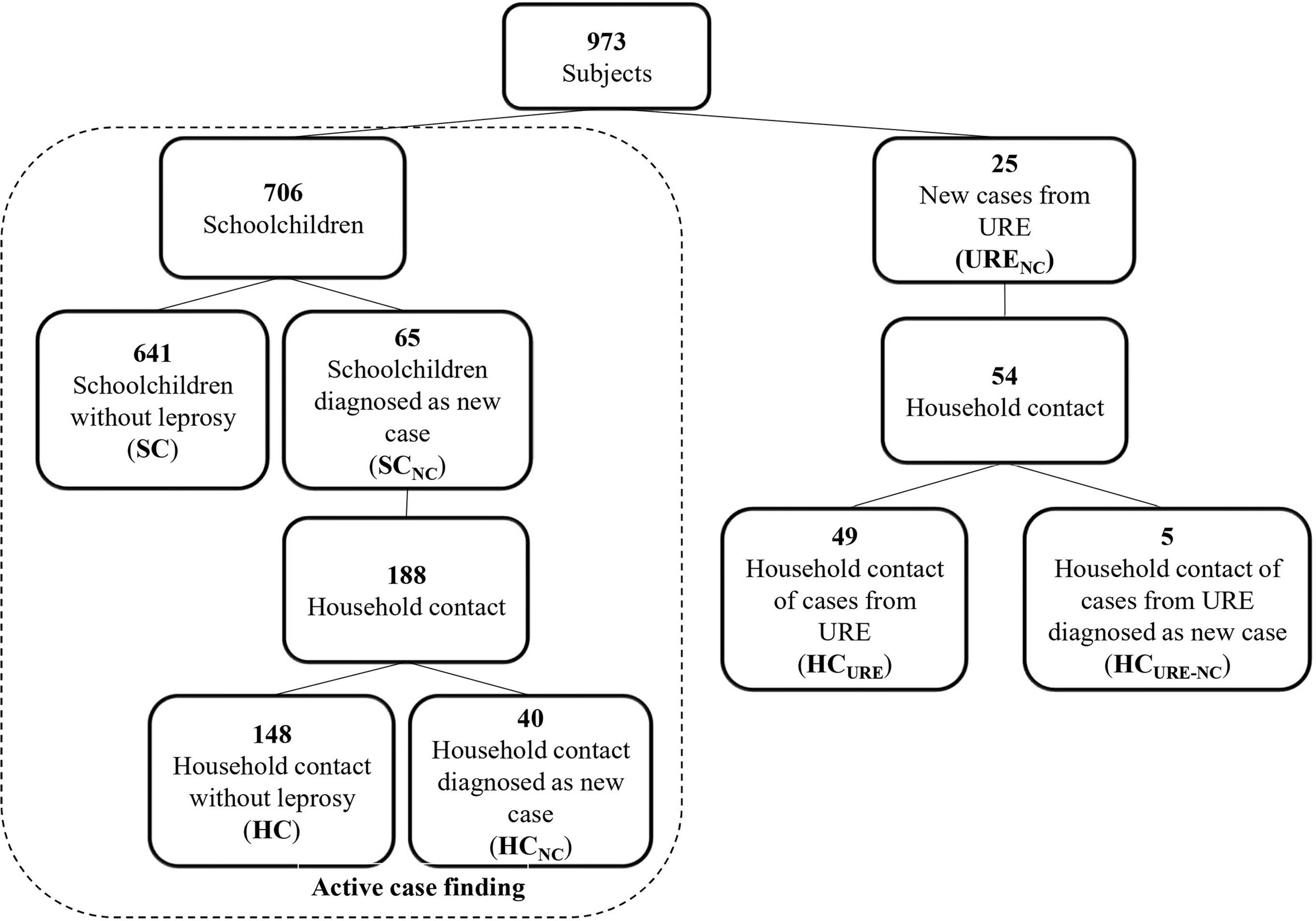
Figure 1 Diagram of study design. A total of 973 subjects were examined, including 706 SC and 188 HC of SCNC, resulting in 894 subjects. Furthermore, 25 URENC and 54 HC were also examined. URE, Dr. Marcello Candia Reference Unit in Sanitary Dermatology of the State of Pará. SC, schoolchildren; SCNC, schoolchildren diagnosed as new case; HC, household contacts; HCNC, household contacts diagnosed as new case; URENC, new cases from URE; HCURE, household contact of cases from URE; HCURE-NC, household contact of cases from URE diagnosed as new case.
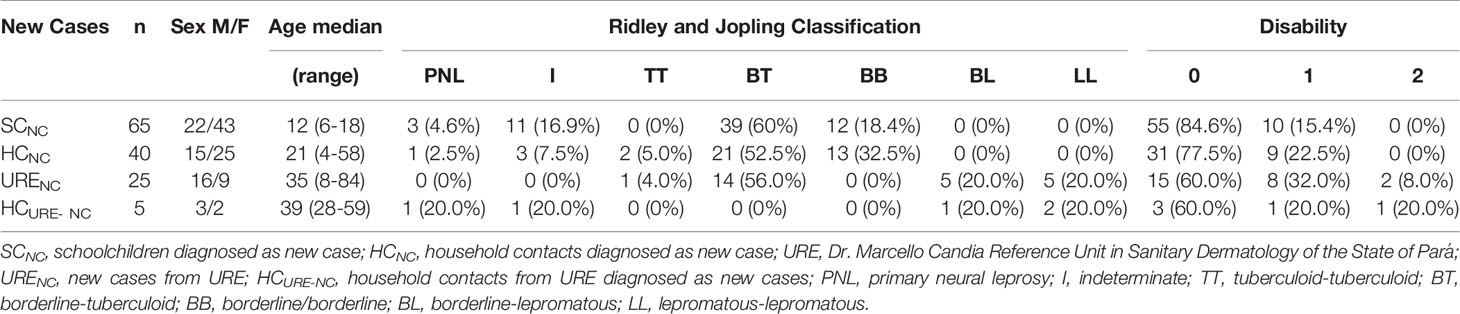
Table 1 Epidemiological characteristic of cases.
NDO-BSA, LID-1, and NDO-LID were quantified by ELISA for each group (SC, SCNC, HC, and HCNC), and seropositivity was characterized based on the cutoff defined for each antigen. There was no significant difference between the SC median versus the SCNC median for any of the antigens (p-value: 0.254, 0.955, and 0.282 for NDO-BSA, LID-1, and NDO-LID, respectively), with an equivalent OD range within each group. HC and HCNC also did not show differences for the three antigens tested (p-value: 0.968, 0.480, and 0.262 for NDO-BSA, LID-1, and NDO-LID, respectively). The seropositive percentages were slightly higher for HC than SC for NDO-BSA (70.9% and 68.8%, respectively) and NDO-LID (29.5% and 20.3%, respectively). Similarly, the seropositivity profile of newly diagnosed cases was the highest for NDO-BSA (73.3%), followed by NDO-LID (33.3%) and LID-1 (5.7%).
To ratify the clinical diagnosis, amplification of the RLEP region using qPCR was performed on 79/105 new cases diagnosed in the field. Out of the 49 SCNC, 43 (87.7%) were found to be positive, while of the 30 HCNC, 25 (83.3%) were positive. In total, 68/79 (86.07%) new cases were found to be positive, with a Ct median of 41.1 cycles (Figure 2A).
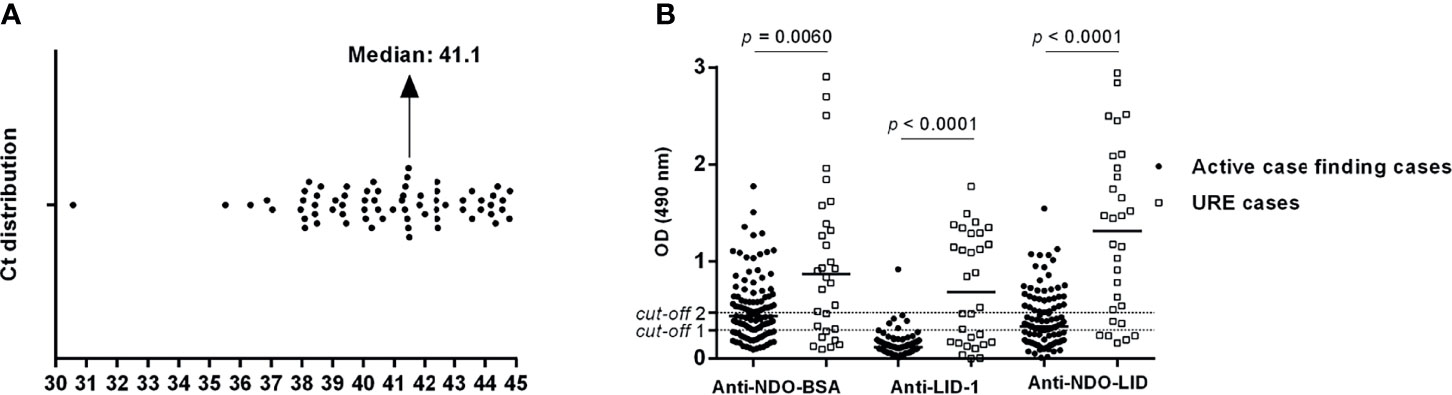
Figure 2 qPCR RLEP and ELISA analyses for leprosy cases diagnosed in the field. (A) Cycle threshold (Ct) distribution of 68/105 new cases diagnosed in the field (43 SCNC and 25 HCNC marked with circle dots). (B) Titers of anti-NDO-BSA, anti-LID-1, and anti-NDO-LID antibodies for 105 cases from active case finding (65 SCNC and 40 HCNC marked with circle dots) in comparison to 30 URE cases (25 URENC and 5 HCURE-NC marked with square dots) of leprosy. URE, Dr. Marcello Candia Reference Unit in Sanitary Dermatology of the State of Pará; SCNC, schoolchildren diagnosed as new case; HCNC, household contacts diagnosed as new case; URENC, new cases from URE; HCURE-NC, household contact of cases from URE diagnosed as new case. Statistical differences were calculated using a two-tailed Mann–Whitney U test using GraphPad Prism 6.
In comparison to the field diagnosis from Mosqueiro, we randomly selected 25 patients (24 MB and 1 PB) who were diagnosed at Dr. Marcello Candia Reference Unit in Sanitary Dermatology of the State of Pará (URE). These patients, new cases from URE (URENC), come from the surrounding region, referred by other basic health units or physicians for confirmation of suspected leprosy. Often, these individuals exhibit more advanced disease due to delays in diagnosis or misdiagnosis (23), which can manifest itself with an increased bacillary index, additional nerve damage, and increased levels of disability. Along with these 25 patients from URE, 54 of their HCs (HCURE) were also enrolled. Upon examination, five of these (9.2%) were found to have clinical symptoms of leprosy, and these HCs of cases from URE were diagnosed as a new case (HCURE-NC).
The antibody titers against the three antigens were determined for all PB (n = 17) and MB (n = 88) cases from Mosqueiro (SCNC and HCNC) versus PB (n = 1) and MB (n = 24) cases from URE. All cases from Mosqueiro demonstrated antibody titers significantly lower than those from URE cases, especially for anti-LID-1 and anti-NDO-LID antibodies (Figure 2B). When the titers were analyzed based on clinical form, there was a clear increase in the mean OD as subjects progressed from TT to LL, with 100% of BL (n = 5) and LL (n = 5) patients being positive against all three antigens (Figure 3).
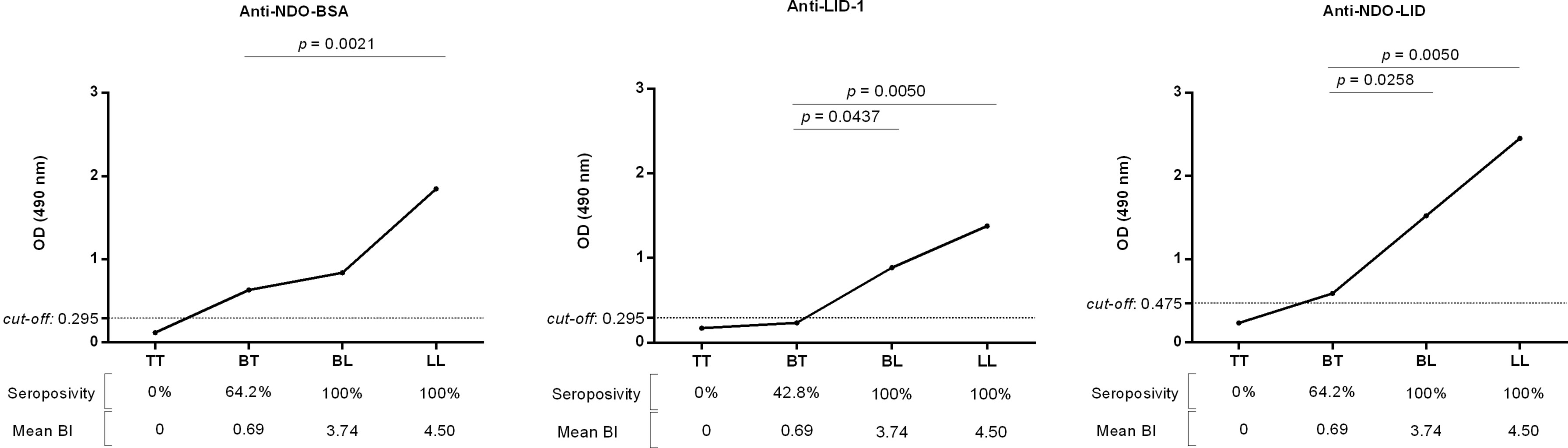
Figure 3 Antibody titer profile of well-defined leprosy cases. TT, tuberculoid-tuberculoid (n = 1); BT, borderline-tuberculoid (n = 14); BL, borderline lepromatous (n = 5); LL, lepromatous-lepromatous (n = 5). Graph dots represent the median of optical density (OD) for each clinical form. Statistical differences were calculated using a two-tailed Mann–Whitney U test using GraphPad Prism 6.
Comparing exclusively subjects without leprosy from Mosqueiro and URE (SC, HC, and HCURE), we observed that only anti-NDO-BSA demonstrated different levels of antibody titers between groups, with a high median on HC from Mosqueiro, followed by SC and HCURE from URE (Figure 4).
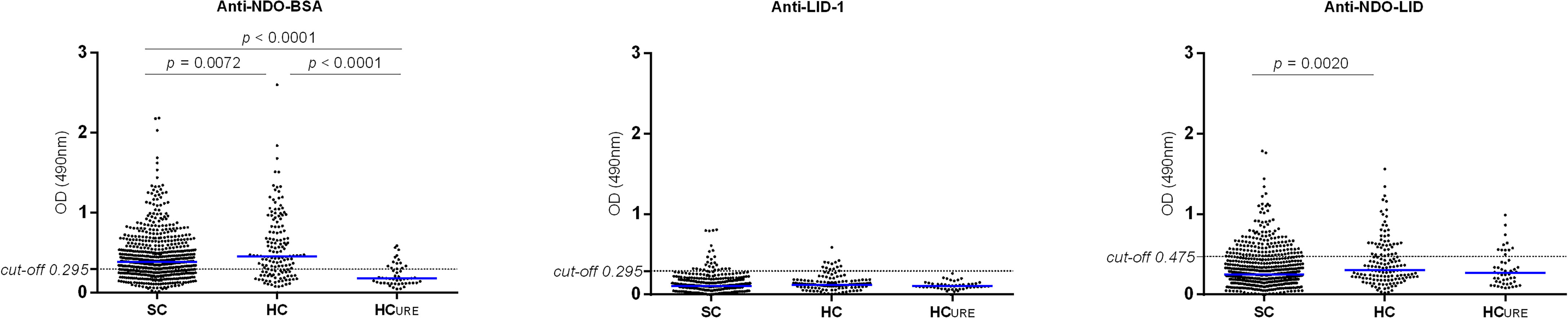
Figure 4 Anti-NDO-BSA, anti-LID-1, and anti-NDO-LID titers in subjects without leprosy. SC, schoolchildren (n = 641); HC, household contacts (n = 148); HCURE, household contact of cases from URE (n = 49). Statistical differences were calculated using a two-tailed Mann–Whitney U test using GraphPad Prism 6.
To evaluate the validity of NDO-BSA, LID-1, and NDO-LID as diagnostic tools, parameters of sensitivity, specificity, and accuracy were calculated for both classes of leprosy patients. No biomarker detected all cases of leprosy, independent of the disease progression at the time of diagnosis. The ability to identify leprosy cases through serology (sensitivity) was higher for NDO-BSA, followed by NDO-LID and LID-1. Anti-NDO-BSA antibodies presented the highest sensitivity either in the field or at URE; however, specificity and accuracy significantly decreased for early leprosy cases diagnosed in the field, limiting anti-NDO-BSA applicability as a diagnostic biomarker for cases in the initial stages. Anti-NDO-LID displayed equivalence to anti-NDO-BSA in all percentages for well-defined patients, while for field subjects, the sensitivity was notably lower. On the other hand, anti-LID-1 was the most effective for differentiating subjects with or without leprosy (specificity), even for cases diagnosed with initial clinical manifestations, showing 100% specificity for URE cases and 95% specificity for Mosqueiro cases. Unfortunately, anti-LID-1 antibodies showed very limited sensitivity, particularly for early diagnosis (Table 2).
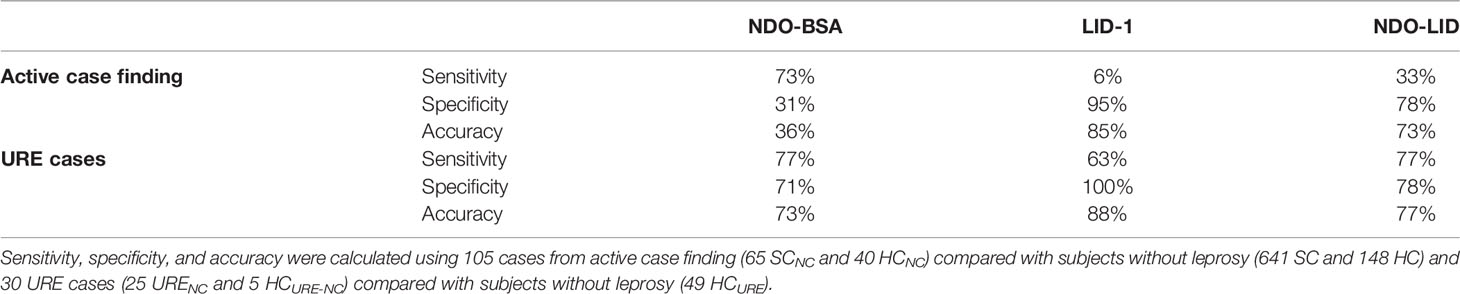
Table 2 Parameters of diagnostic validation of biomarkers tested.
Analyzing the correlation of laboratory test parameters by ROC curve, we verified a large difference in ROC curve power comparing well-defined URE cases or oligosymptomatic field cases. URE subjects presented a high AUC for all biomarkers, indicating the applicability of the use of these biomarkers for well-defined leprosy patients. In contrast, anti-NDO-BSA, anti-LID-1, or anti-NDO-LID antibodies did not discriminate serological cases and non-cases based on the AUC test (Figure 5).

Figure 5 Area under the curve (AUC) for NDO-BSA, LID-1, and NDO-LID. Correlation between cases diagnosed at URE (A) and cases from active case finding—Mosqueiro (B). (C) Non-differentiation line; analysis was performed using GraphPad Prism 6. URE, Dr. Marcello Candia Reference Unit in Sanitary Dermatology of the State of Pará. Area under the receiver operating characteristic (ROC) curve and statistical differences were calculated using GraphPad Prism 6.
Active case finding in schools is not a recent strategy (24); however, it became an important approach to find leprosy cases after inclusion in the WHO global leprosy strategy 2016–2020 (25). In our work, 706 students from Mosqueiro Island were clinically examined, resulting in 65 (9.2%) new cases being diagnosed. This percentage is even superior to our previous studies (5, 23), corroborating the fact that leprosy in Pará has a high number of hidden cases. Mosqueiro is one of the 33 poor islands on the periphery of the capital, with less than 20% coverage by the family health strategy.
Among the examined HC at the island, 40/188 subjects (21.2%) were diagnosed with leprosy, while at URE, only 5/49 (9.2%) were diagnosed with leprosy, corroborating that the field approach is more effective in finding new cases (5, 23, 26). Furthermore, no DG2 cases were found during active case finding on 105 new cases, while for the 5 new cases diagnosed at the URE, 2 had disabilities, 1 DG1 and 1 DG2, indicating that spontaneous demand may diagnose people with higher disability rates, also confirming previous findings (26).
Studies demonstrating the applicability of NDO-BSA (8, 27), LID-1 (18, 28), and NDO-LID (18, 29) to identify and differentiate PB and MB leprosy cases diagnosed at health centers have been published. Although there are divergent concepts of subclinical infection in relation to serology for the determination of infection rate in a community (30), our data ratify the hypothesis that antibody quantification can be an indicator of endemicity (5, 23). High levels of anti-NDO-BSA were observed in HC from Mosqueiro, indicating an increased risk of developing leprosy. HCs positive to PGL-I/ND-O-BSA have 3- to 8.6-fold more chance to progress to disease in relation to seronegative subjects (30–32). HCURE who presented initially high OD for anti-NDO-BSA were followed up and diagnosed (HCURE-NC, n = 5).
Previous works showed that HC anti-LID-1 positivity resulted in diagnosis with leprosy after 6–15 months (28, 33) of follow-up, indicating a very high predictive value. However, although all BL/LL from URE were positive for anti-LID-1 antibodies, only 6/105 (5.71%) of cases from active case finding were positive, indicating that this biomarker was not positively correlated with oligosymptomatic leprosy cases diagnosed in the field. Moreover, 26/641 healthy SC (4.05%) were seropositive with no clinical signs of leprosy and need follow-up to identify possible development of leprosy in the future.
No serological biomarker presented enough sensitivity to identify all cases of leprosy, either well-defined or oligosymptomatic; although anti-NDO-BSA antibodies presented a sensitivity closer to 75%, they showed low specificity, especially in early cases. Diagnostic validation parameters display a large range of sensitivity (2% to 63.8%) and specificity (66% to 98%) when comparing healthy subjects and patients (30, 34). Despite the strong correlation of anti-NDO-BSA titers with MB patients at URE with well-defined late diagnosed cases, this effect is lost in the field, even with MB patients, probably because M. leprae is highly circulating in the community, resulting in infection, not disease. This hypothesis is supported by the increased probability of detecting new cases in people living in houses where at least one seropositive dweller lives in comparison to people living in houses where nobody is positive for anti-PGL-I antibodies (35).
LID-1 and NDO-LID performance described in the literature generally refers to them as useful biomarkers for leprosy diagnosis. However, most of the data include well-defined cases, and relevant sensitivity, specificity, or AUC is observed mostly for classic MB patients (11, 18). Our findings for LID-1 presented 100% and 95% specificity for well-defined and oligosymptomatic cases. The main drawback for LID-1 is the poor sensitivity, with no more than 6% for oligosymptomatic early cases.
Another useful tool extensively applied for the detection of various bacterial diseases is qPCR, which was tested for diagnoses of patients or for monitoring HCs of leprosy cases (36). We observed 86.07% qPCR positivity in cases diagnosed in the field, similar to previous data using well-defined leprosy cases, corroborating the use of RLEP qPCR as a complementary tool to confirm the disease, even in early oligosymptomatic cases (37). These data are just confirming our previous work showing 83.9% positivity of RLEP PCR on new cases, in fact very near of the 86.07% that we had now, against 27.4% of contacts positive for RLEP PCR (38).
Taken together, our data indicate that 1) NDO-BSA, LID-1, and NDO-LID, for specificity or sensitivity reasons, are not reliable for use as POC diagnostic tools, especially for oligosymptomatic cases that are the main targets for leprosy control in the remaining endemic regions, and that 2) qPCR using RLEP is a reliable tool to use as a complementary laboratory exam for leprosy diagnosis, even in patients diagnosed early in the field.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Institute of Health Sciences Research Ethics Committee from Pará Federal University (CAAE 26765414.0.0000.0018 CEP-ICS/UFPA). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
The study concept was designed by AG, JB, MS, and CS. Active case-finding strategy was designed and supervised by JB. Clinical examination of sensory-motor functions was performed by MF and CS. The database software with all clinical and epidemiological information was created and managed by GC. Serological experiments were performed and analyzed by AG, TM, PC, and JS. Antigens used in serological experiments were generously provided by MD and JS. Molecular experiments were designed, managed, and performed by ÂR-d-S, RB, PP, and MS. The manuscript was primarily written by AG with substantial critical revision by JB, ÂR-d-S, MD, MS, JS, and CS. The final manuscript was read and approved by all co-authors.
This work was supported by CNPq (486183/2013-0 CNPq grant for MS; 448741/2014-8 grant for JB; 428964/2016-8 grant and 313633/2018-5 fellowship for CS; and 306815/2018-4 grant for ÂR-d-S), CAPES PROAMAZONIA 3288/2013, CAPES Biocomputacional – RPGPH (3381/2013), Brazil Ministry of Health 035527/2017, PROPESP/UFPA, VALE S.A. 27756/2019, Fulbright Scholar to Brazil 2019-2020 (JS), and the Heiser Program of the New York Community Trust for Research in Leprosy (JB, MS, CS, and JS) grants P15-000827, P16-000796, and P18-000250. The funders had no role in study design, data collection, analysis, interpretation, or writing of the report.
Author MD is employed by HDT Biocorp. He has provided antigens to commercial companies for the manufacture of diagnostic tests.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2022.850886/full#supplementary-material
1. Barreto JG, Guimarães LDS, Leão MRN, Ferreira DVG, Lima RADA, Salgado CG. Anti-PGL-I Seroepidemiology in Leprosy Cases: Household Contacts and School Children From a Hyperendemic Municipality of the Brazilian Amazon. Leprosy Rev (2011) 82:358–70. doi: 10.47276/lr.82.4.358
2. Boletim Epidemiológico - Hanseníase. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Brasília, Ministério da Saúde. (2021).
3. Job CK, Jayakumar J, Kearney M, Gillis TP. Transmission of Leprosy: A Study of Skin and Nasal Secretions of Household Contacts of Leprosy Patients Using PCR. Am J Trop Med Hygiene (2008) 78:518–21. doi: 10.4269/ajtmh.2008.78.518
4. Dogra S, Narang T, Khullar G, Kumar R, Saikia UN. Childhood Leprosy Through the Post-Leprosy- Elimination Era: A Retrospective Analysis of Epidemiological and Clinical Characteristics of Disease Over Eleven Years From a Tertiary Care Hospital in North India. Leprosy Rev (2014) 85:296–310. doi: 10.47276/lr.85.4.296
5. Barreto JG, Bisanzio D, Guimarães LS, Spencer JS, Vazquez-Prokopec GM, Kitron U, et al. Spatial Analysis Spotlighting Early Childhood Leprosy Transmission in a Hyperendemic Municipality of the Brazilian Amazon Region. PloS Neglected Trop Dis (2014) 8:1–10. doi: 10.1371/journal.pntd.0002665
6. Tatipally S, Srikantam A, Kasetty S. Polymerase Chain Reaction (PCR) as a Potential Point of Care Laboratory Test for Leprosy Diagnosis—a Systematic Review. Trop Med Infect Dis (2018) 3:1–14. doi: 10.3390/tropicalmed3040107
7. Turankar RP, Pandey S, Lavania M, Singh I, Nigam A, Darlong J, et al. Comparative Evaluation of PCR Amplification of RLEP, 16s rRNA, rpoT and Sod A Gene Targets for Detection of M. Leprae DNA From Clinical and Environmental Samples. Int J Mycobacteriology (2015) 4:54–9. doi: 10.1016/j.ijmyco.2014.11.062
8. Spencer JS, Brennan PJ. The Role of Mycobacterium Leprae Phenolic Glycolipid I (PGL-I) in Serodiagnosis and in the Pathogenesis of Leprosy. Leprosy Rev (2011) 82:344–57. doi: 10.47276/lr.82.4.344
9. Oskam L, Slim E, Bührer-Sékula S. Serology: Recent Developments, Strengths, Limitations and Prospects: A State of the Art Overview. Leprosy Rev (2003) 74:196–205.
10. Reece ST, Ireton G, Mohamath R, Guderian J, Goto W, Gelber R, et al. ML0405 and ML2331 are Antigens of Mycobacterium Leprae With Potential for Diagnosis of Leprosy. Clin Vaccine Immunol (2006) 13:333–40. doi: 10.1128/CVI.13.3.333-340.2006
11. Cardoso LPV, Dias RF, Freitas AA, Hungria EM, Oliveira RM, Collovati M, et al. Development of a Quantitative Rapid Diagnostic Test for Multibacillary Leprosy Using Smart Phone Technology. BMC Infect Dis (2013) 13:1–10. doi: 10.1186/1471-2334-13-497
12. Corstjens PLAM, van Hooij A, Tjon Kon Fat EM, Alam K, Vrolijk LB, Dlamini S, et al. Fingerstick Test Quantifying Humoral and Cellular Biomarkers Indicative for M. Leprae Infection. Clin Biochem (2019) 66:76–82. doi: 10.1016/j.clinbiochem.2019.01.007
13. Buhrer SS, Smits HL, Gussenhoven GC, Van Ingen CW, Klatser PR. A Simple Dipstick Assay for the Detection of Antibodies to Phenolic Glycolipid-I of Mycobacterium Leprae. Am J Trop Med Hygiene (1998) 58:133–6. doi: 10.4269/ajtmh.1998.58.133
14. Bobosha K, Tjon Kon Fat EM, van den Eeden SJF, Bekele Y, van der Ploeg-van Schip JJ, de Dood CJ, et al. Field-Evaluation of a New Lateral Flow Assay for Detection of Cellular and Humoral Immunity Against Mycobacterium Leprae. PloS Neglected Trop Dis (2014) 8:1–12. doi: 10.1371/journal.pntd.0002845
15. Duthie MS, Ireton GC, Kanaujia GV, Goto W, Liang H, Bhatia A, et al. Selection of Antigens and Development of Prototype Tests for Point-of-Care Leprosy Diagnosis. Clin Vaccine Immunol (2008) 15:1590–7. doi: 10.1128/CVI.00168-08
16. Souza MM, Netto EM, Nakatani M, Duthie MS. Utility of Recombinant Proteins LID-1 and PADL in Screening for Mycobacterium Leprae Infection and Leprosy. Trans R Soc Trop Med Hygiene (2014) 108:495–501. doi: 10.1093/trstmh/tru093
17. Duthie MS, Balagon MVF, Maghanoy A, Orcullo FM, Cang M, Dias RF, et al. Rapid Quantitative Serological Test for Detection of Infection With Mycobacterium Leprae , the Causative Agent of Leprosy. J Clin Microbiol (2014) 52:613–9. doi: 10.1128/JCM.02085-13
18. Amorim FM, Nobre ML, Ferreira LC, Nascimento LS, Miranda AM, Monteiro GRG, et al. Identifying Leprosy and Those at Risk of Developing Leprosy by Detection of Antibodies Against LID-1 and LID-NDO. PloS Neglected Trop Dis (2016) 10:1–17. doi: 10.1371/journal.pntd.0004934
19. Wen Y, You YG, Yuan L, Yuan YH, Zhang Y, Duthie MS, et al. Evaluation of Novel Tools to Facilitate the Detection and Characterization of Leprosy Patients in China. BioMed Res Int (2014) 2014:1–7. doi: 10.1155/2014/371828
20. Villarroel MF, Orsini MBP, Lima RC, Antunes CMF. Comparative Study of the Cutaneous Sensation of Leprosy-Suspected Lesions Using Semmes-Weinstein Monofilaments and Quantitative Thermal Testing. Leprosy Rev (2007) 78:102–9. doi: 10.47276/lr.78.2.102
21. WHO. Enhanced Global Strategy for Further Reducing the Disease Burden Due to Leprosy: Operational Guidelines (2011-2015). New Delhi: World Health Organization, Regional Office for South-East Asia. (2009).
22. Donoghue HD, Holton J, Spigelman M. PCR Primers That can Detect Low Levels of Mycobacterium Leprae DNA. J Med Microbiol (2001) 50:177–82. doi: 10.1099/0022-1317-50-2-177
23. Barreto JG, Guimarães LdeS, Frade MAC, Rosa PS, Salgado CG. High Rates of Undiagnosed Leprosy and Subclinical Infection Amongst School Children in the Amazon Region. Memórias do Instituto Oswaldo Cruz (2012) 107:60–7. doi: 10.1590/S0074-02762012000900011
24. Wharton LH. Leprosy Survey of School Children in British Guiana. Leprosy Rev (1947) 18:30–3. doi: 10.5935/0305-7518.19470006
25. WHO. Global Leprosy Strategy 2016–2020. Accelerating Towards a Leprosy-Free World. Monitoring and Evaluation Guide. New Delhi: World Health Organization, Regional Office for South-East Asia. (2017).
26. Tiendrebéogo A, Sow SO, Traore M, Sissoko K, Coulibaly B. Comparison of Two Methods of Leprosy Case Finding in the Circle of Kita in Mali. Int J leprosy other mycobacterial Dis (1999) 67:237–42.
27. Douglas JT, Cellona RV, Fajardo TT, Abalos RM, Balagon MVF, Klatser PR. Prospective Study of Serological Conversion as a Risk Factor for Development of Leprosy Among Household Contacts. Clin Diagn Lab Immunol (2004) 11:897–900. doi: 10.1128/CDLI.11.5.897
28. Duthie MS, Goto W, Ireton GC, Reece ST, Cardoso LPV, Martelli CMT, et al. Use of Protein Antigens for Early Serological Diagnosis of Leprosy. Clin Vaccine Immunol (2007) 14:1400–8. doi: 10.1128/CVI.00299-07
29. Duthie MS, Raychaudhuri R, Tutterrow YL, Misquith A, Bowman J, Casey A, et al. A Rapid ELISA for the Diagnosis of MB Leprosy Based on Complementary Detection of Antibodies Against a Novel Protein-Glycolipid Conjugate. Diagn Microbiol Infect Dis (2014) 79:233–9. doi: 10.1016/j.diagmicrobio.2014.02.006
30. Penna MLF, Penna GO, Iglesias PC, Natal S, Rodrigues LC. Anti-PGL-1 Positivity as a Risk Marker for the Development of Leprosy Among Contacts of Leprosy Cases: Systematic Review and Meta- Analysis. PloS neglected Trop Dis (2016) 10:1–11. doi: 10.1371/journal.pntd.0004703
31. Brasil MTLRF, de Oliveira LR, Rímoli NS, Cavallari S, Gonçalves OS, Lessa ZL, et al. Sorologia Anti PGL-1 E Risco De Ocorrência De Hanseníase Em Área De Alta Endemicidade do Estado De São Paulo: Quatro Anos De Seguimento. Rev Bras Epidemiologia (2003) 6:262–71. doi: 10.1590/S1415-790X2003000300010
32. Goulart IMB, Souza DOB, Marques CR, Pimenta VL, Gonçalves MA, Goulart LR. Risk and Protective Factors for Leprosy Development Determined by Epidemiological Surveillance of Household Contacts. Clin Vaccine Immunol (2008) 15:101–5. doi: 10.1128/CVI.00372-07
33. Spencer JS, Duthie MS, Geluk A, Balagon MF, Kim HJ, Wheat WH, et al. Identification of Serological Biomarkers of Infection, Disease Progression and Treatment Efficacy for Leprosy. Memorias do Instituto Oswaldo Cruz (2012) 107:79–89. doi: 10.1590/S0074-02762012000900014
34. Gurung P, Gomes CM, Vernal S, Leeflang MMG. Diagnostic Accuracy of Tests for Leprosy: A Systematic Review and Meta-Analysis. Clin Microbiol Infection (2019) 25:1315–27. doi: 10.1016/j.cmi.2019.05.020
35. Salgado CG, Ferreira DVG, Frade MAC, de Souza Guimarães L, da Silva MB, Barreto JG. High Anti-Phenolic Glycolipid-I IgM Titers and Hidden Leprosy Cases, Amazon Region. Emerging Infect Dis (2012) 18:889–90. doi: 10.3201/eid1805.111018
36. Gama RS, Gomides TAR, Gama CFM, Moreira SJM, de Neves Manta FS, de Oliveira LBP, et al. High Frequency of M. Leprae DNA Detection in Asymptomatic Household Contacts. BMC Infect Dis (2018) 18:1–6. doi: 10.1186/s12879-018-3056-2
37. Azevedo MdeCS, Ramuno NM, Fachin LRV, Tassa M, Rosa PS, Belone AdeFF, et al. qPCR Detection of Mycobacterium Leprae in Biopsies and Slit Skin Smear of Different Leprosy Clinical Forms. Braz J Infect Dis (2017) 21:71–8. doi: 10.1016/j.bjid.2016.09.017
Keywords: leprosy, active case finding, schoolchildren, serology, RLEP, qPCR
Citation: Gobbo AR, Bouth RC, Moraes TMP, Pinto P, da Costa PF, Barreto JG, Frade MAC, Ribeiro-dos-Santos AK, Conde GAB, Duthie MS, da Silva MB, Spencer JS and Salgado CG (2022) NDO-BSA, LID-1, and NDO-LID Antibody Responses for Infection and RLEP by Quantitative PCR as a Confirmatory Test for Early Leprosy Diagnosis. Front. Trop. Dis 3:850886. doi: 10.3389/fitd.2022.850886
Received: 08 January 2022; Accepted: 15 February 2022;
Published: 23 March 2022.
Edited by:
Pushpendra Singh, National Institute for Research in Tribal Health (ICMR), IndiaReviewed by:
Tarun Narang, Postgraduate Institute of Medical Education and Research, IndiaCopyright © 2022 Gobbo, Bouth, Moraes, Pinto, da Costa, Barreto, Frade, Ribeiro-dos-Santos, Conde, Duthie, da Silva, Spencer and Salgado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudio Guedes Salgado, Y2xhdWRpb2d1ZWRlc3NhbGdhZG9AZ21haWwuY29t; Y3NhbGdhZG9AdWZwYS5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.