 Philip A. Karlsson1*
Philip A. Karlsson1* Carolina Persson1
Carolina Persson1 James Akoko2,3
James Akoko2,3 Bernard Bett2Åke Lundkvist1
Bernard Bett2Åke Lundkvist1 Johanna F. Lindahl1,2,4
Johanna F. Lindahl1,2,4- 1Department of Medical Biochemistry and Microbiology, Uppsala University, Uppsala, Sweden
- 2Department of Biosciences, International Livestock Research Institute, Nairobi, Kenya
- 3Department of Biomedical Sciences and Technology, Maseno University, Maseno, Kenya
- 4Department of Clinical Sciences, Swedish University of Agricultural Sciences, Uppsala, Sweden
Brucella is a highly pathogenic bacteria endemic in Kenya, and in spite of its severity in humans, the highly inadequate Febrile Antigen Brucella Agglutination Test (FBAT) remains a primary tool for its diagnosis. Blood samples were collected from febrile patients in Kinna health center and screened by the local routine. Milk samples were purchased from local milk hawkers and analyzed for Brucella antibodies using the milk ring test (MRT). The MRT-positive milk was traced to farms, and lactating cattle were sampled for milk and blood. Milk was MRT-tested and the serum was analyzed using the Rose Bengal test (RBT) and iELISA. Available patient and farm samples were stored on FTA cards for qPCR analyses. Despite a limited sample size, our study, in line with previous reports, shows a low diagnostic sensitivity (67%) and specificity (40%) of FBAT when compared to qPCR. As many as 48% of the raw bulk cattle milk samples were MRT-positive for Brucella antibodies and 60% of cattle on three visited farms were IS711 qPCR-positive. This case-based One Health investigation confirms the suspected Brucella presence, suggesting a targeted vaccination at high-prevalence farms, urgent interventions on milk safety, and a re-evaluation of the diagnostic and treatment regimen.
Introduction
One of the most neglected diseases in Kenya is brucellosis, a zoonotic infection caused by the bacterial pathogen Brucella (1). Animals are the principal source of human infection, and human-to-human transmission rarely occurs (2, 3). Four Brucella species gave rise to disease in humans but the majority of cases are caused by B. abortus and B. melitensis (4). Brucella is concentrated and shed in the urine, placental, or fetal tissue where it can transmit through contact or aerosols, generating a contamination risk on close contact. It is additionally found in undercooked meat products or unpasteurized dairy, creating a food safety risk for downstream consumers (5). Brucella is listed as a category B risk organism for bioterrorism and ranked at the highest bacterial biosafety level (BSL3) (5, 6).
According to the World Health Organization (WHO), brucellosis is diagnostically confirmed with a positive cultivation or a several-fold rise in antibodies between the acute and convalescence phases, along with an epidemiological link and symptomatic picture. In pastoral settings where individuals live far from underequipped hospital dispensaries, such paired sera can be impossible to obtain. Cultivation can moreover require up to 30 days of incubation in high retainment facilities (BSL3), making true diagnoses of brucellosis extraordinarily challenging. Antibodies should additionally be measured by reliable standardized serological tools, such as the enzyme-linked immunosorbent assays (ELISA), Brucella microagglutination test (BMAT), or the Brucella Standard Agglutination Test (SAT), but the cost and laboratory requirements are currently unfeasible to implement at field sites. Rapid agglutination tests, such as the Rose-Bengal test (RBT) for serum or the milk ring test (MRT) for cattle milk, can provide cheap and easy alternatives for epidemiological screens, but only provide a little diagnostic value (7, 8). Brucellosis serology is prone to false positives due to a shared epitope between Brucella and multiple Gram-negative bacteria (9–11), and additional false positives can be found in milk towards the end of a lactation period, during mastitis, or in the presence of colostrum (8, 12).
The epidemiology of Brucella remains ill-understood. It is thought that brucellosis occurs endemically within pastoral communities keeping livestock, with prevalence estimates up to 12.5% in Kenya (13). A recent study in northeastern Kenya linked the seroprevalence of Brucella in cattle with humans, clearly showing the increased risk of living in pastoral settings as compared to living in a riverine environment (14). A recent report indicated that only 37% of health centers (n = 86) had the capacity to screen for brucellosis, and it remains elusive what proportion of these can give a true diagnosis (15). In the years 2014–2015, a study in the same region investigated the underreporting of brucellosis and found that 81.5% of Brucella-positive patients (n = 1,067) in Brucella-treating hospitals were misdiagnosed and instead prescribed treatment against diseases such as typhoid fever (43.2%) and malaria (20.5%) (16). Brucella requires a long treatment regimen, reaching 6 weeks with several antibiotics for uncomplicated brucellosis, which, along with the cost and treatment availability, lead to a low compliance (17, 18). Intracellular or dormant phases of brucellosis can escape inadequate treatment, followed by relapses in which new treatment options must be considered (17, 19–22).
Zoonotic transmission and the established correlation between the livestock prevalence of Brucella and human cases of brucellosis highlight the risk of exposure of Kenyan pastoralists, but how this transmission chain is facilitated remains poorly understood. Pastoral settings have fewer available diagnostic-treatment facilities, increasing the time and reducing the efficiency in brucellosis diagnostics. Few data are, however, available on how this isolated placement of pastoral health centers might jeopardize basic needs such as laboratory equipment and treatment availability. The many available tests for Brucella serology have moreover led to inconsistencies and confusion, allowing the introduction and distribution of highly unreliable tests, such as the Febrile Brucella Agglutination Test (FBAT) (23). Despite its proven inadequacy and cost-inefficiency due to misdiagnoses, FBAT is continuously being used in Kenya (24). This illustrates the challenge of evidential data reaching the destination of benefit, and additional scrutiny is needed to understand the distribution and establishment of these tests. Following diagnostic misconceptions, it moreover remains unknown if the updated treatment regimens from the 2006 Ioannina Recommendations are subject for a similar misinterpretation (19). The shear multitude of factors interfering with the prevention of brucellosis calls for new surveillance strategies and control policies.
Following reports of increasing cases of brucellosis in a pastoral town, Kinna (Figure 1), of Isiolo County, Northeastern Kenya, this smaller study investigated the local diagnostic tools available (proving to be FBAT) and the treatment options prescribed, and attempted to assess the functionality of the local test using qPCR from the Flinders Technology Associates (FTA) cards collected during a 2-month period. This study moreover investigated the claims of brucellosis (epidemiological link) by MRT-screening locally sold milk and traced positive bulk-samples back to three separate farms. A cluster-sampling was performed on the farms for downstream tests with MRT, RBT, iELISA, and qPCR. This case-based One Health investigation suggests a re-evaluation and implementation of the diagnostic and treatment routines, reinforces the presence of Brucella, and propose a directed vaccination for high-risk farms and critical interventions on milk safety.
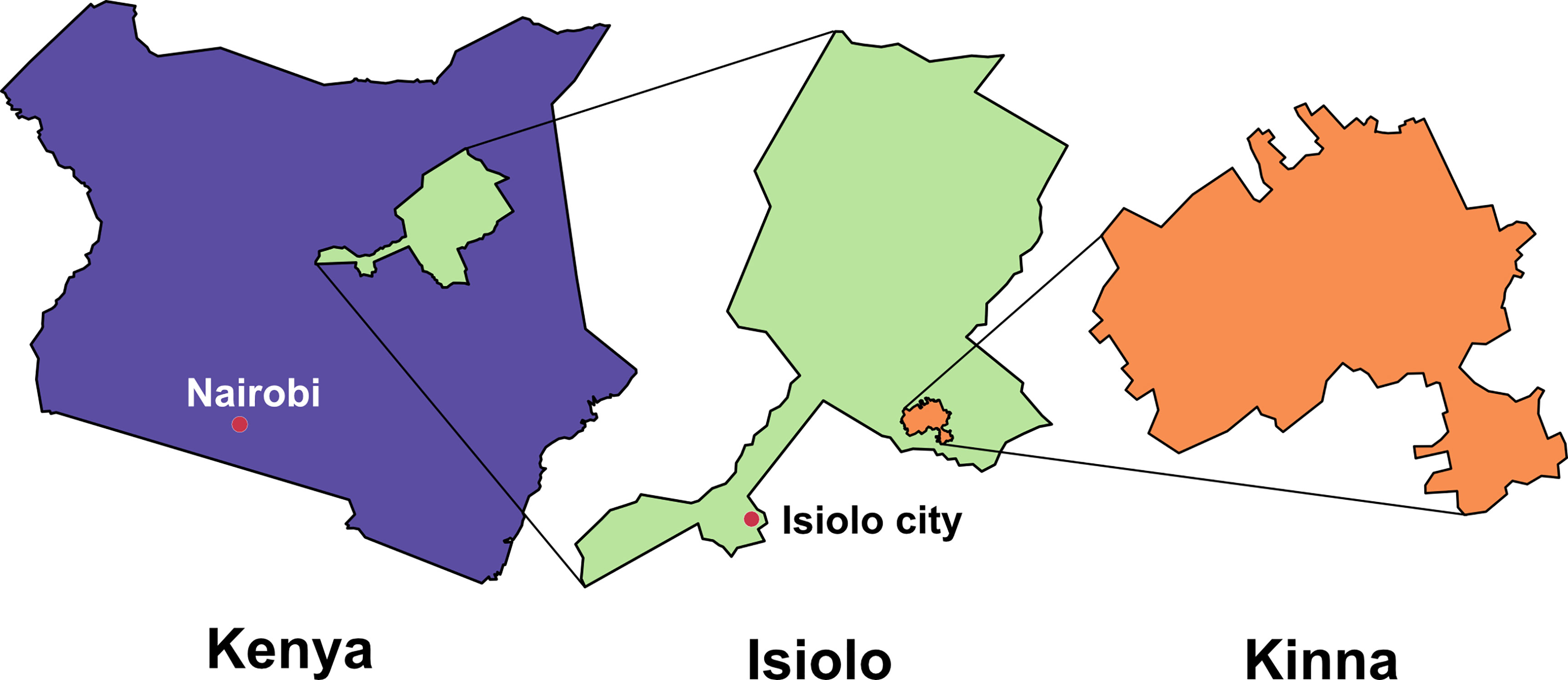
Figure 1 Overview of the study site. Illustration showing Kenya (purple), Isiolo county (green), and Kinna town (orange). Hallmark cities Nairobi and Isiolo are indicated (red).
Material and Methods
Study Scope and Design
This study focused on reported brucellosis cases in a pastoral region of Isiolo County, Kenya, in 2020. According to local reports, the health center had identified increasing numbers of cases, and co-infections with B. abortus and B. melitensis in numerous patients using FBAT (25). Local FBAT-testing and treatment operations were observed without interference by the researchers, entirely carried out by the dispensary staff according to their own protocols. For this study, blood samples were collected from suspected Brucella cases based on general symptoms of febrile disease, and patients were questioned about owning or working with animals and milk consumption habits. A questionnaire was subsequently designed for milk vendors. During 2 consecutive weeks, available local milk hawkers were asked about milk-pooling sizes, milk origin, and potential milk interventions, such as boiling or fermenting. Milk was tested for Brucella antibodies using the MRT for screening to identify the origin of infected milk. Three farms were visited, and milk and blood were collected from lactating cows. Extracted animal sera were serologically tested using RBT and iELISA. Blood and serum from all sources, along with farm animal milk samples, were applied on FTA cards and brought to laboratory for qPCR analysis. A detailed description of the used methods can be found in the supplementary materials.
Case Recruitment
A primary health care dispensary (lat:0.321256, long:38.210139) in the village of Kinna, a pastoral area in the county of Isiolo, Kenya, was visited during normal opening hours (Mon–Fri) from the end of January to the beginning of March 2020. Kinna has a total population of 11,175 people (08/2019), 48.6% female and 51.4% male [Kinna (Isiolo, Eastern Kenya, Kenya) - Population Statistics]. Patients presently, or in the last few weeks, fulfilling at least two criteria of (1) headache, (2) exhaustion, (3) muscle pain, (4) joint pain, (5) backpain, (6) discomfort in the eyes when exposed to light, (7) nausea, (8) vomiting, or (9) fever, were sent for FBAT testing as per the local routine. Tests against both Brucella abortus (Omega Diagnostics UK, Micropath®, OD095) and Brucella melitensis (Omega Diagnostics UK, Micropath®, OD105) were used and carried out on reusable glass slides at room temperature (RT) on a shaker (KJ-201BS Orbital Shaker) and assessed both by eye and in microscope for agglutination. All diagnostic routines using FBAT was carried out by the local technician as per regular practice. According to Omega Diagnostics, their FBATs have a 70% sensitivity and 70% specificity, and positive rapid slide tests should always be confirmed by a tube agglutination test (Omega Diagnostics Ltd., 8025A Issue 4A, 2013). Due to limitations in the dispensary equipment and reagent supplies, test-slides had to be washed and reused, tube agglutination tests had never been available, reagents were occasionally exposed for power outage (breaking cold-chain), and diagnosis was based on the rapid test alone. As the study was based on identifying cases under a restricted period, no sample size calculation was done, but all cases presented at the clinic were invited to participate.
Sample Collection and Processing
A total of 5 ml blood was drawn by the local hospital technician from patients above the age of 12 with two or more of the above symptoms, separated into both coagulation negative and positive vacutainers for a full blood and serum analysis. Serum samples were standing in RT for 20–30 minutes prior to centrifugation at 3,000–4,000 rpm RT for 5–10 min and transferred into cryovials using sterile plastic Pasteur pipettes. A total of 125 µl of serum and blood were moreover loaded onto FTA cards (GE Healthcare, FTA™ Classic Card) in a circular motion, starting from the center. FTA cards were dried at RT for a minimum of 3–6 hours before being packaged into light-protected bags with de-moisturizing silica gel packages. Extracted serum and EDTA samples were stored at -20°C prior to transportation.
During two consecutive weeks in February to March, the village of Kinna was scanned to identify all milk vendors daily. Vendors were verbally asked questions by a local interpreter about the milk origin, milk-pooling size, and milk treatments. GPS coordinates were denoted, and 15 ml of milk was purchased once per vendor from identified brokers in Kinna. Samples were transported in sterile Falcon tubes to the local veterinary lab in cool boxes every hour following the collection of the first sample. In this study, milk vendors were classified as individuals selling milk to the inhabitants of Kinna, and included unofficial but stationary milk stands, mobile motorbike sellers, and local distributing households. Available milk was bought but excluded from analysis if; (1) it had been fermented or (2) it contained milk derived from a seller with milk that was already analyzed. One part of each sample was subjected to MRT. The rest was centrifuged at 3,000 rpm RT for 15 min, after which, the fatty section of the milk was pierced, and the underlying skimmed milk was extracted for storage.
Milk vendors with MRT positive batches were approached the day after the analysis and asked for the farm of origin. The identified farmers were then approached at the same day and briefed on the MRT positive bulk milk from their farm. Milk and blood samples were collected from five lactating cattle per herd (“boma”), representing approx. one fourth to one eighth of the herd sizes. Milk was collected from all udder quarters in a sterile 15-ml Falcon tube by the herd owner. Blood was collected in EDTA and serum vacutainers by a veterinarian. Milk and EDTA tubes were stored in a cool box on ice until arrival at the veterinary lab in Kinna. Milk was treated in the same manner as vendor milk and blood was treated the same way as patient samples. Additionally, an amount of 125 µl of skimmed milk/blood/serum was applied to FTA cards before the tubes were frozen in -20°C. A total of 25 µl of serum was used to perform RBT and another 10 µl for iELISA testing.
Data Analysis
Derived values were entered into Microsoft Excel and 95% confidence intervals were calculated using ± Z [s ÷ √(n)] where Z = 1.96. For comparing local FBAT results, the number of positive cases per month were divided by the total number tested, generating three data-points per year (Jan–Mar). Significance estimations were obtained by comparing two separate years using a two-tailed t-test, analyzed and presented using GraphPad Prism 9 (GraphPad Software, San Diego, California USA).
Ethical Considerations
Sampling was approved by the Zoonotic Disease Unit at the Kenyan Ministry of Health and the Kenya Medical Research Institute (KEMRI/RES/7/3/1). Three different written informed consent forms for ages 5–12, 13–17, and above 18 had to be understood and approved by the patient and guardian before sampling. In events where signatures were not applicable, a fingerprint acted as a valid enactment of consent. The medical officer could sign in place of the guardian when no such was present for children above the age of 13, given that the child had understood, and on the premises that the parents were informed. Animal samples were collected after oral consent by the corresponding farmer.
Recruited patients were not provided compensation for participation in the study. Local routine antibiotic was provided free of charge by Isiolo County. A newly crafted infographic (Supplementary Figure 2) for the prevention of brucellosis was provided to all participants (patients and farmers). During this study, farmers were invited to a local community meeting and informed about the situation of brucellosis in the village.
Results
Health Center Patients – Febrile Brucella Agglutination Test
Local laboratory reports were assessed for counting the admitted febrile patients and FBAT-positive cases from the years 2018, 2019, and 2020, to evaluate if the locally suggested brucellosis increase had been observed. Despite the inadequacy of FBAT as a diagnostic tool, and regardless of more testing being performed in 2020, the perceived proportional increase of FBAT-positive cases/total number tested was significantly higher in 2020 when compared to both 2018 [p < 0.05, 95% Confidence Interval (CI95): 0.01–0.30] and 2019 (p < 0.05, CI95: 0.06–0.31) (Figure 2). No significant difference could be identified between the years 2018 and 2019.
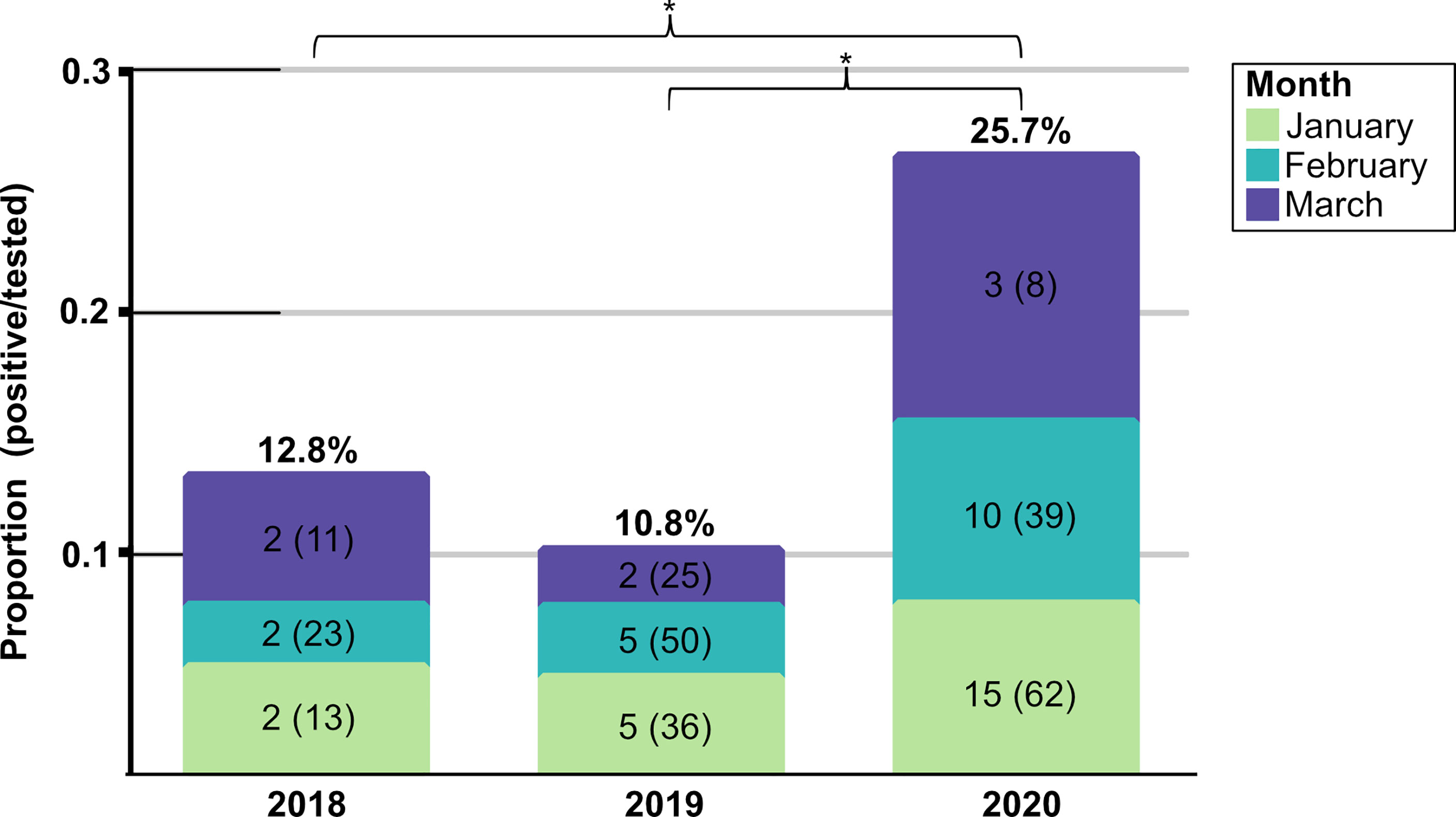
Figure 2 Number of cases registered in Kinna health center. Illustration for the number of FBAT-positive cases registered in Kinna Health Center, Garbatula, Isiolo, Kenya, during the years 2018, 2019, and 2020, showing the months January (green), February (turquoise), and March (purple). The number of positive cases is indicated for each month along with the total number tested (brackets). Only the first three days of March are included for 2020. Significance was calculated with an unpaired two-tailed t-test, assuming a normal distribution. *P < 0.05 for t-test.
During the 32 days of screening in Feb–March, there were 47 suspected cases of brucellosis, of which, 28% (13/47) tested positive by FBAT. Due to the high burden on the hospital staff and electricity outage with inadequate storage temperatures, only 12 samples were obtained for further analysis. Out of these 12 samples, 7 were FBAT positive and 4 were FBAT negative, representing 54% (7/13) and 12% (4/34) of the total number screened, respectively. Two FBAT-positive serum samples broke during centrifugation, leaving only the EDTA samples for qPCR. All patients answered that they consumed local milk.
If tested positive with FBAT, patients were prescribed a local routine treatment of doxycycline or ciprofloxacin and, occasionally, levofloxacin or streptomycin by the medical officer. For patients requiring admission at the daytime care unit, gentamicin was administered intravenously. Pregnant women were provided with augmentin (amoxicillin with clavulanic acid) or streptomycin. Most patients were prescribed monotreatment. Several patients were reportedly relapse patients from the previous year, but the records separating acute from relapse were not accessible in our study.
Determining Seroprevalence in Vendor Milk – Milk Ring Test
In total, 58 milk brokers were identified and 53 agreed to participate, one was excluded. Several of the milk vendors were children ages 8–15. The most common way to sell milk was through unofficial milk stands by hawkers selling in group, 79% (41/52); followed by distributing motorbikes, 10% (5/52); walking vendors, 8% (4/52); and distributing households, 6% (3/52). The type of milk sold included cow (64%, 33/52), camel (33%, 17/52), and goat (4%, 2/52). None of the goat milk had been boiled while 18% (6/33) and 35% (6/17) had been boiled for cow and camel, respectively. Milk was popularly sold from five village locations by stationary vendors selling in group: 8% A (4/52), 10% B (5/52), 31% C (16/52), 8% F (4/52), and 15% H (8/52) (Figure 3). The majority of the sold cow milk originated from the region Machesa (58%, 19/33). Several vendors selling in group measured milk for consumers in a jug or tray which was shared between the vendors of the same location.
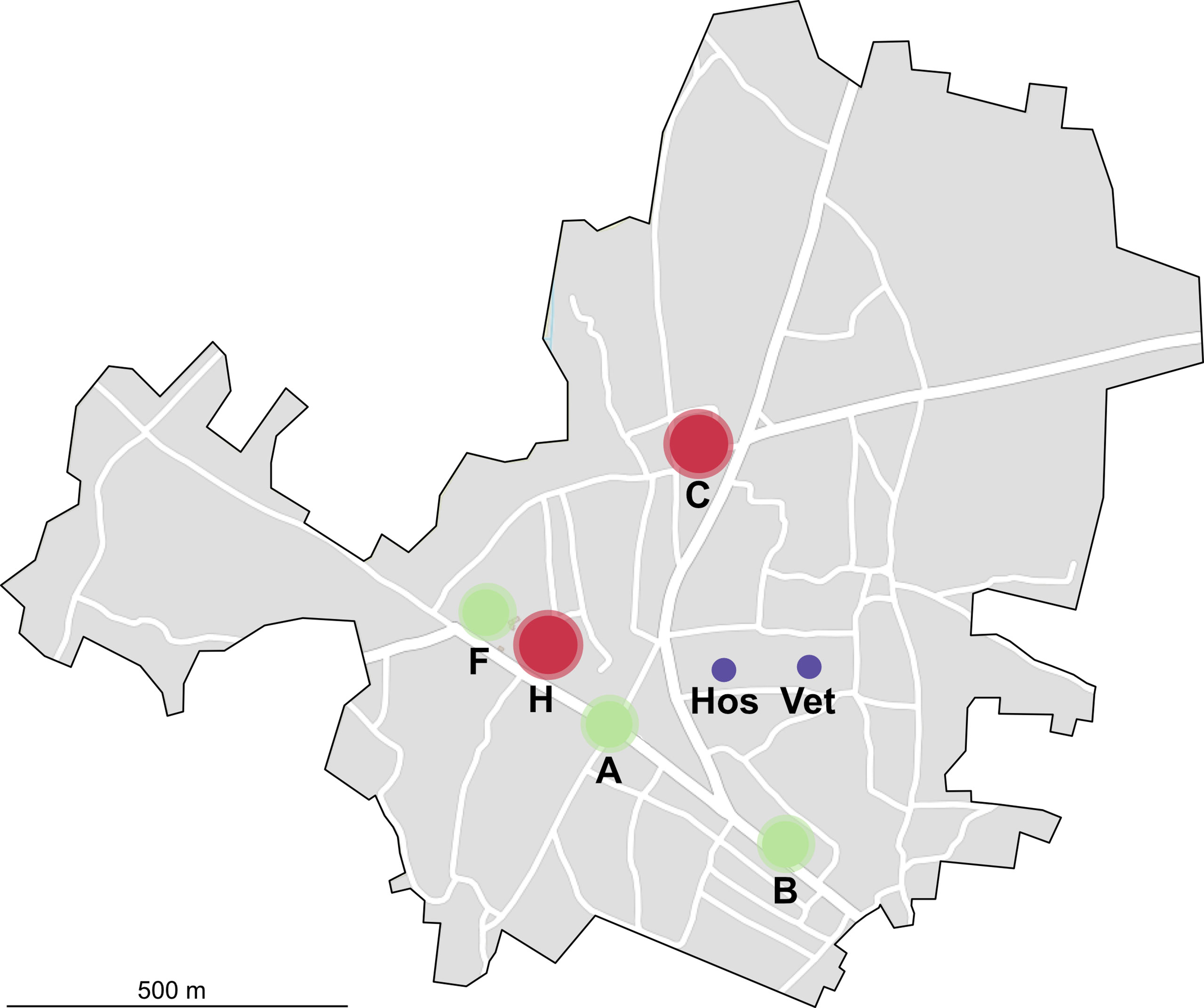
Figure 3 Map of Kinna, Isiolo. A map over Kinna illustrating the distribution of the five largest groups of stationary vendors (A, B, F, H). The hospital (Hos) and veterinary station (Vet) are indicated with purple color. Vendor groups (A, B, F) sold no MRT-positive milk, indicated by green color. Vendor groups (C, H) sold MRT-positive milk, indicated by red color.
A total of 52 collected samples were tested (Table 1). In total, 29% (15/52, CI95: 18%–42%) of the analyzed milk was MRT positive. Twelve of the samples had reportedly been boiled, 23% (12/52), and none of these tested positive. Disregarding the boiled samples, the overall seroprevalence of MRT-positive raw milk accumulated to 38% (15/40, CI95: 24%–53%). On a species level, only one camel (9%, 1/11, CI95: 2%–38%) and one goat (50%, 1/2, CI95: 10%–91%) accounted for positive cases, while 87% of the MRT positive raw milk came from cow, suggesting that nearly half of MRT-tested non-boiled cattle milk was positive (48%, 13/27, CI95: 31%–66%).
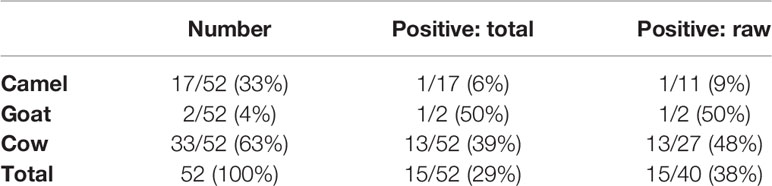
Table 1 Seroprevalence in local milk.
All the hawkers selling on foot or motorbike traded raw milk, correlating with the highest proportion of MRT-positive samples being found among walking (100%, 4/4, CI95: 51%–100%) and motorbike (40%, 2/5, CI95: 12%–77%) distributors. While only 22% (9/41, CI95: 12%–37%) of the milk from stationary vendors were positive, all the MRT-positive milk in this group could be charted to two unofficial stands having the highest number of hawkers (Figure 3). In the distribution area C, 25% (4/16, CI95: 11%–50%) of milk samples were positive while area H had 63% (5/8, CI95: 315–86%) seroprevalence.
Screening Antibodies in Farm Milk and Serum – Milk Ring Test, Rose Bengal Test and iELISA
Farm A (letters for farms not related to milk stands) in region Machesa contained a total of 207 cows divided into 11 herds with approx. 20 animals in each. Farm B in region Machesa contained a total of 76 cows divided into four herds with up to 20 cows in each. Farm C in region Rapsu contained a total of 60 animals divided into three herds with 20 animals in each where one herd had been separated and could not be sampled. Blood and milk were collected from five animals per available herd.
In total, 37 milk and 36 serum samples were serologically tested. The overall seroprevalence across the farms with the different serological techniques were MRT: 30% (11/37, CI95: 18%–46%), RBT: 22% (8/36, CI95: 12%–38%), and iELISA: 25% (9/36, CI95: 14%–41%). The highest seroprevalence was observed in farm C (MRT/RBT/iELISA: 60%, CI95: 31%–83%), followed by farm B (MRT: 24%, CI95: 10%–47%, iELISA: 18%, CI95: 6%–41%, RBT: 12%, CI95: 3%–34%). Farm A had only one seropositive sample (MRT: 10%, CI95: 2%–40%), and for that single sample, the blood samples had been lost.
RBT shared a general agreement (negatives and positives) of 97% (35/36, CI95: 86%–100%) with iELISA. MRT shared a 78% (28/36, CI95: 62%–88%) overall agreement with iELISA, dropping to a mere 46% (6/13, CI95: 23%–71%) if comparing the agreement for iELISA-positives. The differences observed in the serum and milk serology derived from RBT/iELISA included two specimens positive from farm C which was negative by MRT, and three weak (grade: 1+) and one strong (grade: 4+) MRT-positive specimens from farms B and C, respectively, which were negative by RBT/iELISA. That Brucella antibodies would be present in milk while absent in serum is a rather unlikely event, suggesting a potential contact with known MRT-pitfalls.
Screening of Serum, Blood, and Milk – qPCR
Pilots from the different FTA extraction protocols suggested that different protocols may be suitable for different matrices. Serum and blood samples were boiled while milk samples were extracted using the Qiagen DNase Blood and Tissue kit, as these had the highest reproducibility across positive replicates and gave lower CT values (data not shown). Although optimization work was performed, samples were rarely positive more than once across triplicates.
In patients, 50% (6/12, CI95: 25%–75%) were qPCR positive, four were positive only in serum, one positive only in blood, and one positive in both matrices. Two patient serum samples were lost in the field, the corresponding EDTA blood samples were negative. Out of the six qPCR positive samples, four were also positive on the hospital FBAT. Three samples that were reported as FBAT positive were qPCR negative. Although great care should be acted when comparing serological and qPCR data, we deem it important to highlight that hospital diagnosis was carried out using only serology. Despite our study being of a very small scale, as indicated by the large 95% confidence intervals, the qPCR results are indicative of a diagnostic sensitivity and specificity of the FBAT test of 67% (CI95: 22%–96%) and 40% (CI95: 5%–85%), respectively. This would give FBAT a diagnostic accuracy of 55% (CI95: 23%–83%).
In farm animals, 56% (20/36, CI95: 40%–71%) tested qPCR positive in serum/blood and 19% (7/37, CI95: 10%–34%) tested positive in milk. Out of 20 serum/blood positives, 13 were discovered in only serum, 2 were discovered in only blood, and 5 were discovered in both matrices. Five of the seven (71%) positive milk samples were also positive in serum/blood, two being found only in milk. Taken together, the prevalence based on all sources reached 60% (22/37, CI95: 44%–74%). The highest number qPCR-positives were found in farms A (70%, 7/10, CI95: 40%–89%), followed by farm C (60%, 6/10, CI95: 31%–83%) and farm B (53%, 9/17, CI95 31%–74%). Two serum/blood samples were lost, these turned out negative in the milk samples. One milk sample was lost after MRT testing, this turned out negative in the serum/blood samples.
Discussion
This study investigated a suggested increase of brucellosis in a pastoral area in Kenya and explored the diagnostic tools and treatment options related to it. The perceived increase proved to be significant. The local diagnosis was performed using the highly inadequate Febrile Brucella Antigen Test (FBAT). In 2017, FBATs were first shown to have a low and unreliable performance with a low specificity, leading to substantial misdiagnoses (23). The same paper highlighted that FBATs claim to distinguish between B. melitensis and B. abortus, when, in fact, no such separation is possible by serological rapid tests. As presented on numerous occasions, the antigen used for Brucella rapid tests is the species-shared C-epitope which is not species specific (26, 27). The 2017 paper moreover emphasized that the laboratory technicians and clinicians in health dispensaries have strong beliefs that such a separation is possible, which was also the case in our study, a belief enforced by the inconsistencies in the FBAT results (23). Our study merely obtained 12 patient samples in which 7 had been deemed FBAT-positive. All involved patients answered that they consumed unpasteurized milk, suggesting an epidemiological risk, but undermining the possibilities of odds ratio estimations. Raw milk consumed to this extent did not come as a surprise as the previous study in the same village in 2017 found that 88% of the inhabitants consumed unboiled milk (28).
Serological and qPCR data should only carefully be compared in sensitivity and specificity evaluations (29, 30). The lag-phase between infection and antibody response, as well as lingering antibody responses, imply that serology and qPCR will only occasionally agree (31). Despite this, the health center in Kinna diagnosed Brucella solely on FBAT serology, and we deemed it warranted to compare the diagnostic sensitivity and specificity between FBAT and qPCR, something which was similarly performed in a recent study (32). The authors estimated a diagnostic sensitivity for FBAT against qPCR of 36.6% and a diagnostic specificity of 69.3%, results of a similar character to our own smaller sample size showing 67% sensitivity (CI95: 22%–96%) and 40% specificity (CI95: 5%–85%).
According to the medical officer, patients diagnosed with Brucella using FBAT requiring daycare admission were prescribed gentamicin. Pregnant women were given a combination treatment of amoxicillin and clavulanic acid or streptomycin. During interviews, it became apparent that no consistent treatment schedule for brucellosis had been implemented in the dispensary. Since the 80s, the WHO has recommended the combination of doxycycline and streptomycin against Brucella, and only recently were these updated for the option to exchange streptomycin with rifampicin or gentamicin. Fluroquinolones such as ciprofloxacin should only be used as a third supplement or second-line treatment along with doxycycline for difficult cases (19). Some benefit has been shown when administering doxycycline in combination with trimethoprim-sulfamethoxazole during pregnancy, but never a β-lactam antibiotic like amoxicillin (33). Due to the high relapse rate and treatment failure in brucellosis, monotreatment should never be provided, and especially not with streptomycin which constitutes the first-line treatment of resistant-prone tuberculosis. Both diagnostic and treatment standards used in the dispensary were hence regarded inadequate by the researchers.
We found that cattle and camel milk were the two most popularly sold local milk types in Kinna, where camel milk was boiled to a larger degree than cattle milk. The most common way to sell milk was in groups of unofficial milk hawkers, even though mobile vendors and distributing households were identified too. A total of 13 out of 27 raw milk samples derived from cattle were positive, setting the raw milk seroprevalence for Brucella in cows to a startling 48% (CI95: 31%–66%). All MRT-positive milk from stationary stands derived from two main distribution areas, with the remaining MRT-positive samples coming from sporadic mobile vendors. The 2017 study showed that 88% of Kinna inhabitants consumed untreated milk (28), which matches our present results, finding that 77% (40/52, CI95: 64%–86%) of local milk was sold raw. Whether the milk market matches the local need and desire of unpasteurized dairy, or whether the inhabitants do not regard the state of the milk prior to consumption, is something that should be further investigated. Local hawkers were, in general, not difficult to interconnect with for the local communicator, and in two of the instances during farm-tracing, the vendor followed along to the corresponding farmer. Farmers were similarly cooperative and helped in providing information, restraining cattle, and offering milk.
When collecting fresh milk samples from cattle for MRT testing, it is desirable to take milk from all udder quarters with clean hands in animals with no mastitis and a controlled lactation cycle, to reduce the risk of false positives (8, 12). However, using a case-based study design like ours made it unfeasible to estimate what farms to visit in advance, and lactation patterns could not be resolved. Furthermore, it was not uncommon for herds to contain aggressive cattle, especially so for farm C, which made it impossible to keep hands sterile. Although the seroprevalence at the farms were not exceedingly different when comparing milk with the serum data, the overall agreement on positive results was no more than 46%. To our knowledge, only one previous study has similarly reported a low agreement between milk and serum (30). While MRT is a highly valued and functional screening technique in controlled settings, it remains challenging to account for the pitfalls leading to false positives in pastoral field settings. The qPCR data revealed that up to 60% (22/37, CI95: 44%–74%) of the visited cattle were positive against Brucella in either milk, blood, or serum, with a minimum of 50% positive in each farm. Serology and qPCR taken together, our data suggests that the longest lasting, and still ongoing, infection occurred in Rapsu (farm C), and that Brucella only recently reached Machesa (farms A/B). This conclusion was derived from the overall high level of qPCR positives with only farm C showing a more established antibody response. Additionally, farms A and B shared a common water point with several thousand animals, including sheep, goat, camel, and wildlife.
Regarding our methodological approach for sample transport, FTA cards constituted a useful but limiting setup for downstream qPCR analysis. All samples were run in triplicates, but rarely did any sample turn positive in all replicates, and when so, with high CT-values. The generally low CFU/ml blood of Brucella along with the dilution factor generated through extraction from the FTA cards may have contributed to these results (9, 34). The results might imply that triplicates were not enough to detect all cases, and firmly imply that more studies on the optimization of FTA-extracted DNA for qPCRs are valued. In line with previous reports, Brucella DNA was more frequently found in serum than in blood; however, why DNA occasionally was discovered in blood but not in serum remains elusive (35, 36). It might be that intracellularly located bacteria not always rupture to the extent required for serum DNA detection, but this has not yet been studied. Why boiling was sufficient for serum and blood but not for milk is unclear, but as previously stated, the milk matrix is more complex than the relatively clean serum (37, 38). The IS711 qPCR setup used in this study, including the AmpliTaq Gold polymerase and probe, was particularly used to reduce the background noise of undesirable DNA. The qPCR setup in combination with the commercial milk extraction and triplicate-runs accumulated to an expense not feasible for routine diagnostics. The main benefactor with FTA cards, with regard to Brucella, is the specimen inactivation at the field site, abstaining the need of a BSL3 facility.
Study Limitations
Using a case-based investigation for tracing zoonotic diseases in pastoral settings does come at a cost, and the authors of this paper do acknowledge some limitations associated to the study design and sample handling. The healthcare dispensary was manned by one medical officer and one technician, while continuously receiving numerous patients with a large variety of gravity. In addition, the dispensary was exposed for power-outages on multiple occasions, leading to the discarding of already collected samples. Although this resulted in a smaller sample size, the analyzed samples retained a high quality and the authors urge similar studies to bear the power-related aspect in mind. With regard to both the dispensary and the communication with hawkers, we highly encourage working together with a community local, as both cultural and linguistic barriers do exist between the country regions. The authors do promote the use of pamphlets without text and encourage the creation of these in consultation with the community local. As previously mentioned, the MRT does have known pitfalls which are more difficult to control for in case-based pastoral settings. Although we could not beforehand control for lactating cycles, the farmers generally had a good insight in the health of their animals, reducing the risks for mastitis. Even though milk from all udder quarters was collected, hands could not always be kept sterile. These factors might have caused false positive results, which is why we similarly encourage the use of serum tests, such as RBT, when available. The authors do hope that these insights will not discourage but rather aid future studies in the field, so that functional implementation strategies for disease prevention can be built.
Conclusion - Implementation Strategies
We undertook a One Health case-based investigation to investigate a suggested increase of brucellosis in a pastoral area of Kenya and evaluated the local diagnostic and treatment standards. The local hospital dispensary diagnosed brucellosis cases using the inadequate serological rapid test, FBAT, and provided treatment options other than that recommended by the 2006 Ioannina Recommendations. Further investigation revealed a high serological prevalence of Brucella antibodies in the locally distributed cattle milk, derived from local farms. In this study, three farms were shown to have a minimum 50% qPCR-prevalence of Brucella. Although we present suggestions for an improved control of brucellosiss, based on our study, the larger aspects of farm-to-consumer chain, the use of FBAT, and treatment insufficiencies are global issues. We suggest the following implementation strategies:
1. Routine screening for Brucella in farms distributing milk to local consumers, suggestively using the more reliable and easier-to-use Rose Bengal test (RBT).
2. Targeted vaccination for high-prevalence cattle farms, or milk-producing cattle farms sharing watering points with high-prevalence farms.
3. Urgent interventions on milk safety, preferably on milk distributed from high-prevalence cattle farms to maximize safety down the marketing chain. Secondly, aimed at hawkers that would have the option to boil milk prior to sales (although a financial benefactor must be identified). It is also desirable that this communication is done by a community local.
4. Local updates for big-scale farmers by a local expert (medical officer and chief veterinarian) on the status and progression of the disease in the community, preferably during community gatherings.
5. A top-down updated treatment regimen for brucellosis, provided by the County and based on the principles supported by the WHO, founded in the 2006 Ioannina Recommendations. The dispensaries are also dependent on the County for the provision of diagnostic tests, urging the need for a reevaluation on the proven financial and diagnostic losses using FBAT. Instead, RBT would provide a more reliable screen for animals and humans alike.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Zoonosis Disease Unit at the Kenyan Ministry of Health and the Kenya Medical Research Institute (KEMRI/RES/7/3/1). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. The animal study was reviewed and approved by Zoonosis Disease Unit at the Kenyan Ministry of Health and the Kenya Medical Research Institute (KEMRI/RES/7/3/1). Written informed consent for participation was not obtained from the owners because high degree of illiteracy meant farmers preferred oral consent.
Author Contributions
Conceptualization: PK, CP, BB, JL, and JA. Data curation: PK, CP, and JA. Formal analysis: PK and JL. Funding acquisition: BB. Investigation: PK, JA, CP, BB, and JL. Methodology: PK, CP, BB, JL, and JA. Project administration: BB. Validation: BB and JL. Writing – original draft: PK. Writing – review and editing: CP, BB, JL, JA, and ÅL. All authors contributed to the article and approved the submitted version.
Funding
Field work was supported by the project: Co-infection with Rift Valley fever virus, Brucella spp., and Coxiella burnetii in humans and animals in Kenya: Disease burden and ecological factors (Co-infection project) funded by the Defense Threat Reduction Agency, contract number HDTRA 11910031. Additional support for staff time was supported by the Agriculture for Nutrition and Health CGIAR program led by IFPRI. The project was also supported by the Minor Field Study program of the Swedish International Development Cooperation Agency. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the Minor Field Study program of the Swedish International Development Cooperation Agency, as well as the ILRI animal and human health research program. We would like to express our greatest appreciation to all the involved staff at ILRI, and the field veterinarians and clinical personnel at the field hospital who provided their irreplaceable assistance. Special thanks are extended to Tove Hoffman and Grace Watene for their help and input on the molecular methods.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2021.711425/full#supplementary-material
References
1. Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The New Global Map of Human Brucellosis. Lancet Infect Dis (2006) 6:91–9. doi: 10.1016/s1473-3099(06)70382-6
2. O’Callaghan D, Whatmore A. Brucella Genomics as We Enter the Multi-Genome Era. Brief. Funct Genomics (2011) 10:334–41. doi: 10.1093/bfgp/elr026
3. Wattam AR, Foster JT, Mane SP, Beckstrom-Sternberg SM, Beckstrom-Sternberg JM, Dickerman AW, et al. Comparative Phylogenomics and Evolution of the Brucellae Reveal a Path to Virulence. J Bacteriol (2014) 196:920–30. doi: 10.1128/JB.01091-13
4. Alton GG, Forsyth JRL. Brucella. In: Baron S, editor. Molecular Medical Microbiology, 2nd ed. Texas: Elsevier Ltd (2014). p. 1781–8. doi: 10.1016/B978-0-12-397169-2.00101-3
5. He Y. Analyses of Brucella Pathogenesis, Host Immunity, and Vaccine Targets Using Systems Biology and Bioinformatics. Front Cell Infect Microbiol (2012) 2:2. doi: 10.3389/fcimb.2012.00002
6. de Figueiredo P, Ficht TA, Rice-Ficht A, Rossetti CA, Adams LG. Pathogenesis and Immunobiology of Brucellosis: Review of Brucella-Host Interactions. Am J Pathol (2015) 185:1505–17. doi: 10.1016/j.ajpath.2015.03.003
7. Salman AMA. Evaluation of Four Serological Tests to Detect Prevalence of Bovine Brucellosis in Khartoum State. J Cell Anim. Biol (2012) 6:140–3. doi: 10.5897/jcab11.072
8. Mohamand N, Gunaseelan L, Sukumar B, Porteen K. Milk Ring Test for Spot Identification of Brucella Abortus Infection in Single Cow Herds. J Adv Vet Anim. Res (2014) 1:70–2. doi: 10.5455/javar.2014.a8
9. Kittelberger R, Bundesen PG, Cloeckaert A, Greiser-Wilke I, Letesson JJ. Serological Cross-Reactivity Between Brucella Abortus and Yersinia Enterocolitica 0:9: IV. Evaluation of the M- and C-Epitope Antibody Response for the Specific Detection of B. Abortus Infections. Vet Microbiol (1998) 60:45–57. doi: 10.1016/S0378-1135(97)00202-2
10. Hinić V, Brodard I, Thomann A, Holub M, Miserez R, Abril C. IS711-Based Real-Time PCR Assay as a Tool for Detection of Brucella Spp. In Wild Boars and Comparison With Bacterial Isolation and Serology. BMC Vet Res (2009) 5:22. doi: 10.1186/1746-6148-5-22
11. Bonfini B, Chiarenza G, Paci V, Sacchini F, Salini R, Vesco G, et al. Cross−Reactivity in Serological Tests for Brucellosis: A Comparison of Immune Response of Escherichia Coli O157:H7 and Yersinia Enterocolitica O:9 vs Brucella Spp. Vet Ital (2018) 54:107–14. doi: 10.12834/VetIt.1176.6539.2
12. Tallman KL, Herman HA. Adaptations and Limitations of Ring Test for Bovine Brucellosis. Agric Exp Stn. (1954) 546:44.
13. Enström S, Nthiwa D, Bett B, Karlsson A, Alonso S, Lindahl JF. Brucella Seroprevalence in Cattle Near a Wildlife Reserve in Kenya. BMC Res Notes (2017) 10:615. doi: 10.1186/s13104-017-2941-x
14. Lindahl J, Ontiri E, Bukachi S, Njeru I, Karanja J, Sang R, et al. Positive Association Between Brucella Spp. Seroprevalences in Livestock and Humans From a Cross-Sectional Study in Garissa and Tana River Counties, Kenya. PloS Negl Trop Dis (2019) 13:e0007506. doi: 10.1371/journal.pntd.0007506
15. Slotved HC, Yatich KK, Sam SO, Ndhine EO. The Capacity of Diagnostic Laboratories in Kenya for Detecting Infectious Diseases. Trop Med Health (2017) 45. doi: 10.1186/s41182-017-0049-6
16. Njeru J, Melzer F, Wareth G, El-Adawy H, Henning K, Pletz MW, et al. Human Brucellosis in Febrile Patients Seeking Treatment at Remote Hospitals, Northeastern Kenya 2014–2015. Emerg Infect Dis (2016) 22:2160–4. doi: 10.3201/eid2212.160285
17. Corbel M. Brucellosis in Humans and Animals. Geneva: WHO in Collaboration with the Food and Agriculture Organization of the UN and World Organization for Animal Health (2006).
18. Alavi SM, Alavi L. Treatment of Brucellosis: A Systematic Review of Studies in Recent Twenty Years. Casp. J Intern Med (2013) 4:636–41.
19. Ariza J, Bosilkovski M, Cascio A, Colmenero JD, Corbel MJ, Falagas ME, et al. Perspectives for the Treatment of Brucellosis in the 21st Century: The Ioannina Recommendations. PloS Med (2007) 4:e317. doi: 10.1371/journal.pmed.0040317
20. Godfroid J, Nielsen K, Saegerman C. Diagnosis of Brucellosis in Livestock and Wildlife. Croat. Med J (2010) 51:296–305. doi: 10.3325/cmj.2010.51.296
21. Lee SIL, Islam MA, Khatun MM, Choi GY, Jung JM, Baek BK, et al. Immunoglobulin Profiles in Acute Brucellosis Experimentally Induced by Brucella Canis in BALB/C Mice. Vector-Borne Zoonotic Dis (2010) 10:927–30. doi: 10.1089/vbz.2009.0125
22. Avijgan M, Rostamnezhad M, Jahanbani-Ardakani H. Clinical and Serological Approach to Patients With Brucellosis: A Common Diagnostic Dilemma and a Worldwide Perspective. Microb Pathog (2019) 129:125–30. doi: 10.1016/j.micpath.2019.02.011
23. de Glanville WA, Conde-Álvarez R, Moriyón I, Njeru J, Díaz R, Cook EAJ, et al. Poor Performance of the Rapid Test for Human Brucellosis in Health Facilities in Kenya. PloS Negl Trop Dis (2017) 11:e0005508. doi: 10.1371/journal.pntd.0005508
24. Alumasa L, Thomas LF, Amanya F, Njoroge SM, Moriyón I, Makhandia J, et al. Hospital-Based Evidence on Cost-Effectiveness of Brucellosis Diagnostic Tests and Treatment in Kenyan Hospitals. PloS Negl Trop Dis (2021) 15:e0008977. doi: 10.1371/journal.pntd.0008977
26. Ducrotoy MJ, Bertu WJ, Ocholi RA, Gusi AM, Bryssinckx W, Welburn S, et al. Brucellosis as an Emerging Threat in Developing Economies: Lessons From Nigeria. PloS Negl Trop Dis (2014) 8:e3008. doi: 10.1371/journal.pntd.0003008
27. Ducrotoy MJ, Conde-Álvarez R, Blasco JM, Moriyón I. A Review of the Basis of the Immunological Diagnosis of Ruminant Brucellosis. Vet Immunol Immunopathol (2016) 171:81–102. doi: 10.1016/j.vetimm.2016.02.002
28. Affognon H, Mburu P, Hassan OA, Kingori S, Ahlm C, Sang R, et al. Ethnic Groups’ Knowledge, Attitude and Practices and Rift Valley Fever Exposure in Isiolo County of Kenya. PloS Negl Trop Dis (2017) 11. doi: 10.1371/journal.pntd.0005405
29. Chang HY, Chang LY, Shao PL, Lee PI, Chen JM, Lee CY, et al. Comparison of Real-Time Polymerase Chain Reaction and Serological Tests for the Confirmation of Mycoplasma Pneumoniae Infection in Children With Clinical Diagnosis of Atypical Pneumonia. J Microbiol Immunol Infect (2014) 47:137–44. doi: 10.1016/j.jmii.2013.03.015
30. Shome R, Nagalinfam M, Shome BR, Misri J, Adamshree BS, Kamal A, et al. Milk Ring Test From Lab to Field: A Surveillance Strategy for States Under Brucellosis Control Program. Indian J Anim. Sci (2015) 85:1077–80.
31. Gilbert GL, Hawes LA. The Antibody Response to Brucella: Immunoglobulin Response Measured by Enzyme-Linked Lmmunosorbent Assay and Conventional Tests. Aust N Z. J Med (1981) 11:40–7. doi: 10.1111/j.1445-5994.1981.tb03734.x
32. Kiambi SG, Fèvre EM, Omolo J, Oundo J, de Glanville WA. Risk Factors for Acute Human Brucellosis in Ijara, North-Eastern Kenya. PloS Negl Trop Dis (2020) 14:e0008108. doi: 10.1371/journal.pntd.0008108
33. Bosilkovski M, Arapović J, Keramat F. Human Brucellosis in Pregnancy – an Overview. Bosn. J Basic Med Sci (2020) 20:415–22. doi: 10.17305/bjbms.2019.4499
34. Yagupsky P, Peled N, Press J, Abramson O, Abu-Rashid M. Comparison of BACTEC 9240 Peds Plus Medium and Isolator 1.5 Microbial Tube for Detection of Brucella Melitensis From Blood Cultures. J Clin Microbiol (1997) 35:1382. doi: 10.1128/jcm.35.6.1382-1384.1997
35. Zerva L, Bourantas K, Mitka S, Kansouzidou A, Legakis NJ. Serum is the Preferred Clinical Specimen for Diagnosis of Human Brucellosis by PCR. J Clin Microbiol (2001) 39:1661–4. doi: 10.1128/JCM.39.4.1661-1664.2001
36. Wang Y, Wang Z, Zhang Y, Bai L, Zhao Y, Liu C, et al. Polymerase Chain Reaction-Based Assays for the Diagnosis of Human Brucellosis. Ann Clin Microbiol Antimicrob (2014) 13:31. doi: 10.1186/s12941-014-0031-7
37. Mantur BG, Mangalgi SS. Evaluation of Conventional Castaneda and Lysis Centrifugation Blood Culture Techniques for Diagnosis of Human Brucellosis. J Clin Microbiol (2004) 42:4327–8. doi: 10.1128/JCM.42.9.4327-4328.2004
Keywords: Brucella, Neglected tropical diseases, milk, serology, FBAT, zoonosis, pastoralism, brucellosis in animals and humans
Citation: Karlsson PA, Persson C, Akoko J, Bett B, Lundkvist Å and Lindahl JF (2021) Using a One Health Case-Based Investigation for Improved Control of Brucellosis in Isiolo, Kenya. Front. Trop. Dis 2:711425. doi: 10.3389/fitd.2021.711425
Received: 18 May 2021; Accepted: 31 August 2021;
Published: 21 September 2021.
Edited by:
Suraj Bhattarai, Global Institute for Interdisciplinary Studies (GIIS), NepalReviewed by:
Olushayo Oluseun Olu, World Health Organization, South SudanI Wayan Gede Artawan Eka Putra, Udayana University, Indonesia
Copyright © 2021 Karlsson, Persson, Akoko, Bett, Lundkvist and Lindahl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philip A. Karlsson, cGhpbGlwLmthcmxzc29uQGltYmltLnV1LnNl