
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 14 February 2025
Sec. Primary Immunodeficiencies
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1532367
 Sandra Martínez Mercader1
Sandra Martínez Mercader1 Victor Garcia-Bustos1,2*Pedro Moral Moral1,3*Carmen Martínez Buenaventura1Elisa Escudero Vergara1María Carmen Montaner Bosch1Héctor Balastegui-Martín1,3Sonia Galindo Maycas4Berta Palací Mur4Marian Escobar Palazón5María Moreno Mulet5Ignacio Campanero Carrasco6Alicia López7Carlos Daniel Hernández Ruiz8Laura Ruiz-López9
Victor Garcia-Bustos1,2*Pedro Moral Moral1,3*Carmen Martínez Buenaventura1Elisa Escudero Vergara1María Carmen Montaner Bosch1Héctor Balastegui-Martín1,3Sonia Galindo Maycas4Berta Palací Mur4Marian Escobar Palazón5María Moreno Mulet5Ignacio Campanero Carrasco6Alicia López7Carlos Daniel Hernández Ruiz8Laura Ruiz-López9 Rocío Guzmán Guzmán9,10Marta Dafne Cabañero-Navalon1,3
Rocío Guzmán Guzmán9,10Marta Dafne Cabañero-Navalon1,3Background and aim: Subcutaneous immunoglobulin (SCIg) has emerged as an alternative to intravenous administration for patients with primary (PID) and secondary immunodeficiencies (SID), offering benefits such as fewer systemic adverse reactions and greater patient autonomy. However, comprehensive real-world data on SCIg use, including clinical and patient-centered outcomes, remain scarce. This study, conducted by expert immunodeficiency nursing teams, assesses the clinical characteristics, reported adverse effects, and quality-of-life outcomes associated with SCIg therapy with different formulations in patients with PID and SID across Spain.
Methods: A multicenter, cross-sectional study was conducted across 8 immunodeficiency nursing units in Spain, involving 223 adult patients treated with SCIg from 2004 to 2024. Data on demographics, comorbidities, SCIg treatment characteristics, reported adverse events, and quality-of-life metrics (EuroQol-5D-3L, Gijón Scale) were collected and analyzed.
Results: The cohort (61.4% female, mean age: 47.1 years) included 65% PID patients, with common variable immunodeficiency being the most frequent diagnosis (39.8%). SCIg demonstrated good tolerability overall, with no significant differences in global adverse event rates between facilitated 10% (fSCIg) and 20% formulations. However, 10% fSCIg was associated with higher reported frequencies of mild local rash (58.7% vs. 36.9%, p=0.002) and fever (10.6% vs. 1.7%, p=0.01). Quality-of-life scores indicated minimal limitations in mobility and self-care, with a mean subjective health rating of 72.7/100. Patients using 20% SCIg required fewer educational sessions for self-administration compared to the 10% group.
Conclusion: The different SCIg formulations in this large, multicenter cohort was effective and generally well-tolerated, supporting its use for maintaining adequate IgG levels and promoting patient independence in PID and SID. The study’s findings advocate for tailored approaches that optimize patient satisfaction and address individual needs, emphasizing the critical role of dedicated immunodeficiency nursing teams in ensuring safe, effective, and patient-centered SCIg administration.
Immunoglobulin replacement therapy (IgRT) is an essential intervention for patients with primary (PID) and secondary immunodeficiencies (SID) who experience impaired antibody production. IgRT has demonstrated efficacy in reducing infection rates and severity, preventing organ damage, and lowering mortality (1, 2). Initially introduced in the 1950s as intramuscular preparations for humoral PID, immunoglobulin therapy evolved significantly with advancements in plasma fractionation, leading to the development of intravenous immunoglobulin (IVIg) in the 1980s. In Spain, subcutaneous immunoglobulin (SCIg) became available in 2004, with facilitated 10% SCIg (fSCIg) formulations introduced in 2017 (3, 4) (AEMPS, Hizentra; AEMPS, Hyqvia).
Although IVIg and SCIg have comparable efficacy, SCIg is associated with several advantages, including fewer systemic side effects, improved quality of life, and reduced healthcare costs (5, 6). A meta-analysis of 24 studies involving 946 PID patients found that transitioning from IVIg to SCIg resulted in higher serum IgG levels and fewer adverse events, with no increase in infection rates (7). Furthermore, home-based SCIg administration has been shown to yield economic benefits compared to hospital-based IVIg treatment (8). SCIg therapy also enhances patient autonomy and flexibility, as it can be self-administered at home following comprehensive training from expert immunodeficiency nurses. This specialized training is critical for safe and effective self-management, addressing infusion procedures, adverse event mitigation, and preventive measures.
Despite these advantages, SCIg remains underutilized in Spain and Europe, even within specialized centers (9). Inconsistencies persist across national guidelines regarding SCIg indications for SID, and discrepancies remain between recommendations and clinical practice (10, 11). Furthermore, even after three decades since SCIg’s introduction, there remains a significant lack of international real-world data on its use, particularly in SID populations, insights that are crucial for optimizing and expanding its application in this group (12). Comprehensive epidemiological and clinical insights into SCIg therapy for both PID and SID are notably limited.
This study aims to provide a comprehensive cross-sectional assessment of the use of both 20% and 10% fSCIg preparations in specialized PID nursing units across Spain, evaluating clinical and sociodemographic characteristics, administration practices, therapeutic outcomes, adverse effects, and the impact on quality of life, including social, economic, and psychological dimensions for both PID and SID patients.
A multicenter, retrospective study was conducted in Spain between November 2023 and August 2024, involving patients aged 14 years and older with PID and SID who had received or were receiving SCIg since its introduction in Spain in 2004. Patients were prescribed SCIg based on clinical severity and infection burden, as determined by their reference clinical practitioners and clinical guidelines. Eight immunodeficiency units from different hospitals participated in the development of the GEIE Spanish Registry, an initiative led by the Immunodeficiency Nursing Group of the Spanish Society of Immunology (Figure 1). Patients with a diagnosis of PID or SID who had received SCIg (including facilitated SCIg) for at least one month during their clinical course, were considered eligible for inclusion.
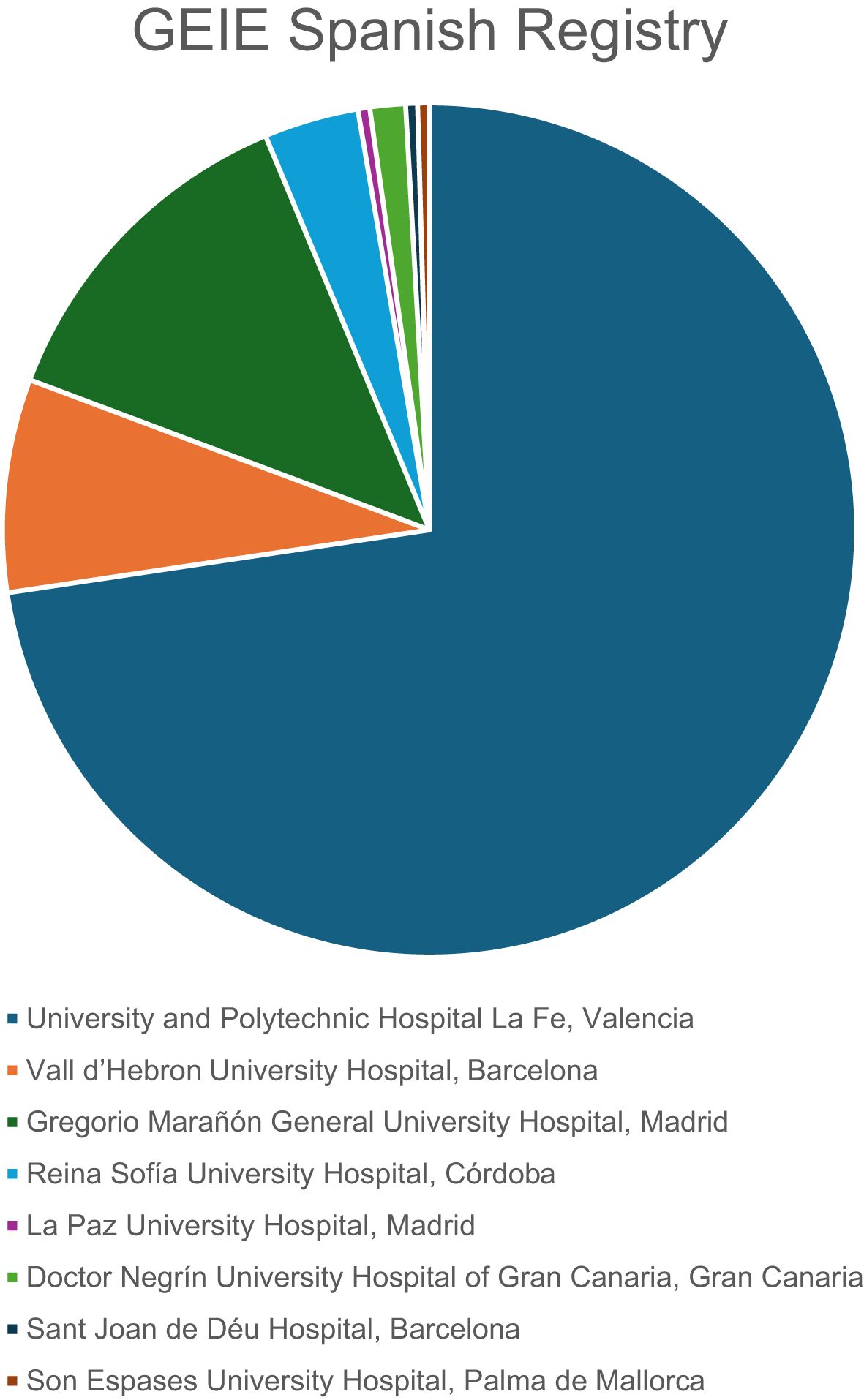
Figure 1. Distribution of patients contributed by each hospital in the GEIE Spanish Registry study.
The protocol of the GEIE Spanish Registry was independently approved by all institutional Ethical Committees of each participating hospital under their corresponding registry codes. Anonymity and data confidentiality of all included patients were ensured in accordance with the Spanish regulation of observational studies. The work was performed according to the Declaration of Helsinki and followed the STROBE guidelines.
The GEIE Spanish Registry systematically compiles sociodemographic, epidemiological, and clinical data, including patient comorbidities, characteristics of SCIg therapy, technical aspects of SCIg administration, reported adverse effects, and a comprehensive evaluation of the patients’ social, economic, and psychological status. Data were collected retrospectively from medical records and supplemented with information from patient interviews using predefined questionnaires, especially regarding to adverse events and quality of life impacts. All data were obtained by expert nurses specialized in immunodeficiency care.
Demographic data collected included sex, current age, date of birth, age at treatment initiation, diagnosis (PID or SID), and, in the case of PID, the specific diagnosis. Comorbidities were also documented, including immune dysregulation-related conditions such as autoimmune cytopenias, organ-specific autoimmunity, and a history of benign lymphoproliferation affecting the spleen or lymph nodes. The presence of bronchiectasis or parenchymal lung disorders was recorded, as well as any history of chronic liver disease, enteropathy, or dermatological conditions. Additionally, a history of solid or hematologic malignancies, solid organ transplantation, or hematopoietic stem cell transplantation (HSCT) was registered, along with any drug allergies or other allergic conditions.
The use of oral or subcutaneous anticoagulants and antiplatelet therapies was documented. Baseline total IgG levels prior to SCIg initiation and trough IgG levels during treatment were recorded. Information was collected on whether patients were actively receiving SCIg at the time of inclusion, or if they had switched to IVIg or discontinued IgRT, including reasons for these changes. Local adverse reactions to SCIg (erythema, pain, pruritus, swelling, fluid leakage, hematoma, ulceration, necrosis), as well as systemic adverse reactions to SCIg (headache, asthenia, fever, arthralgia, myalgia, generalized rash, wear-off effect), were recorded according to cumulative patient experience.
Details of SCIg administration were captured, including the type of SCIg product, the site of administration (outpatient clinic, external consultation, or home), dosage in grams per week, frequency of administration, infusion volume (for both 20% and 10% concentrations), infusion time, number of infusion sites, and needle gauge and length. The patient’s abdominal circumference and the number of training sessions required for self-administration were also documented.
Socioeconomic data collected included the distance from the patient’s home to the hospital and their employment status. The Gijón Scale (13) was applied to assess family situation, including living arrangements, monthly income, housing conditions, social relationships, and social network support. Additionally, patients completed the EuroQol-5D-3L questionnaire (14), which evaluates mobility, self-care ability, daily activities, presence of pain, anxiety and depression, and includes a self-rated health score ranging from 0 to 100. Both scales are available in the Supplementary Material (Supplementary Tables S1, S2).
Due to the epidemiological and cross-sectional design of the study, variables were primarily analyzed using descriptive statistics. Analyses were conducted using R statistical software (version 4.2.1, R Development Core Team, 2022). Quantitative data were reported as mean ± standard deviation (SD), while qualitative data were presented as absolute counts and percentages, excluding missing values. Subanalyses of key variables used the χ² or Fisher’s exact test for categorical data and the Student’s t-test for continuous data, following verification of statistical assumptions. A two-tailed p-value <0.05 was considered statistically significant.
A total of 223 participants were included in the study, with a higher proportion of women (61.4%, n=137) than men (38.6%, n=86). The mean age at inclusion was 47.1 years (SD: 18.6). Of the participants, 65.0% (n=145) had PID, while the remaining 35.0% (n=78) were diagnosed with SID. Among those with PID, the most common diagnosis was common variable immunodeficiency (CVID) (39.8%, n=88), followed by IgG subclass deficiency (6.3%, n=14), combined IgA and IgG subclass deficiency (5.9%, n=13), and syndromic immunodeficiencies (5.4%, n=12). Among the participants with SID, the most frequent causes included immunosuppressive therapy and chemotherapy due to lymphoma (33.3%, n=26), myeloma (24.4%, n=19), autoimmune diseases (12.8%, n=10), and leukemia (6.4%, n=5).
Patients with PID included 54 men (42.5%) and 73 women (57.5%). Their mean age was 41.05 (SD 17.52) years old. Autoimmune cytopenia was present in 14.2% of participants. Regarding organ-specific autoimmune disease, 12 patients (9.45%) had hypothyroidism and 11 patients (7.8%) had arthritis. There were no patients with type 1 diabetes mellitus. Among systemic autoimmune diseases, 2.4% had Sjögren syndrome. Notably, lymph node or spleen affectation was documented in 15.75% (n=20). Liver disease was present in 21 patients (16.54%). Bronchiectasis and non-infectious lung involvement was present in 42 (33.07%) and 31 (24.41%) patients, respectively. Enteropathy was noted in 25.2% (n=32). Skin disease was present in 24.41% (n=31).
Among patients with SID, 27 were men (34.6%) and 51 were women (65.4%). They were significantly older than those with PID, with a mean age of 58.72 (SD 15.26) years old (p<0.0001). Hematologic neoplasias were present in 61.90% (n=39) and solid tumor was documented in 11.11% patients (n=7). Four patients (6.35%) had received a solid organ transplantation and other 15 patients (23.81%) had received HSCT.
One hundred and fourteen patients (52.05%) of the cohort were receiving SCIg 20%, and 105 (47.95%) were receiving fSCIg 10%. When examining the Ig preparations, Hyqvia® (n=105, 47.95%) was the most commonly used (n=102, 46.57%), followed by Hizentra® (n=102, 46.57%) and Xembify® (n=12, 5.48%). There were no patients receiving push-SCIg therapy. Previous treatment with IVIg was documented in 148 (66.67%) patients.
Serum IgG levels prior treatment initiation were 563.01 mg/dL (SD 348.14), while the mean IgG trough levels during treatment was 1,041.16 mg/dL (SD 361.63). The average SCIg total week dose administered was 8.04 g (SD: 2.87). The dosing frequency for SCIg varied, with 40.19% (n=86) receiving weekly infusions, 11.21% every two weeks (n=25), 28.97% (n=62) every three weeks, and 18.69% (n=40) monthly. Patients typically used an average of 1.86 injection points (SD: 0.38) per infusion. The most common injection site for SCIg was the abdomen, used by 61.26% (n=136) of participants, followed by alternating between the abdomen and thighs (22.07%, n=49). Injection exclusively in the thighs was reported by 13.51% (n=30), while 1.35% (n=3) alternated injection sites between the arms, abdomen, and thighs.
Two patients alternated arms and thighs (0.90%) and another two patients used only the arms (0.90%).The mean abdominal perimeter in our cohort was 89.49cm (SD: 14.85). Regarding needle length, the majority (78.83%, n=175) used 9 mm needles, followed by 12 mm needles (9.01%, n=20), 8 mm needles (6.31%, n=14), 10 mm needles (3.15%, n=7) and 6 mm needles (2.70%, n=6). The majority of the needles used were 26 G (58.37%, n=129) and 27 G (41.63%, n=92). A summary of the results is represented in Figure 2.
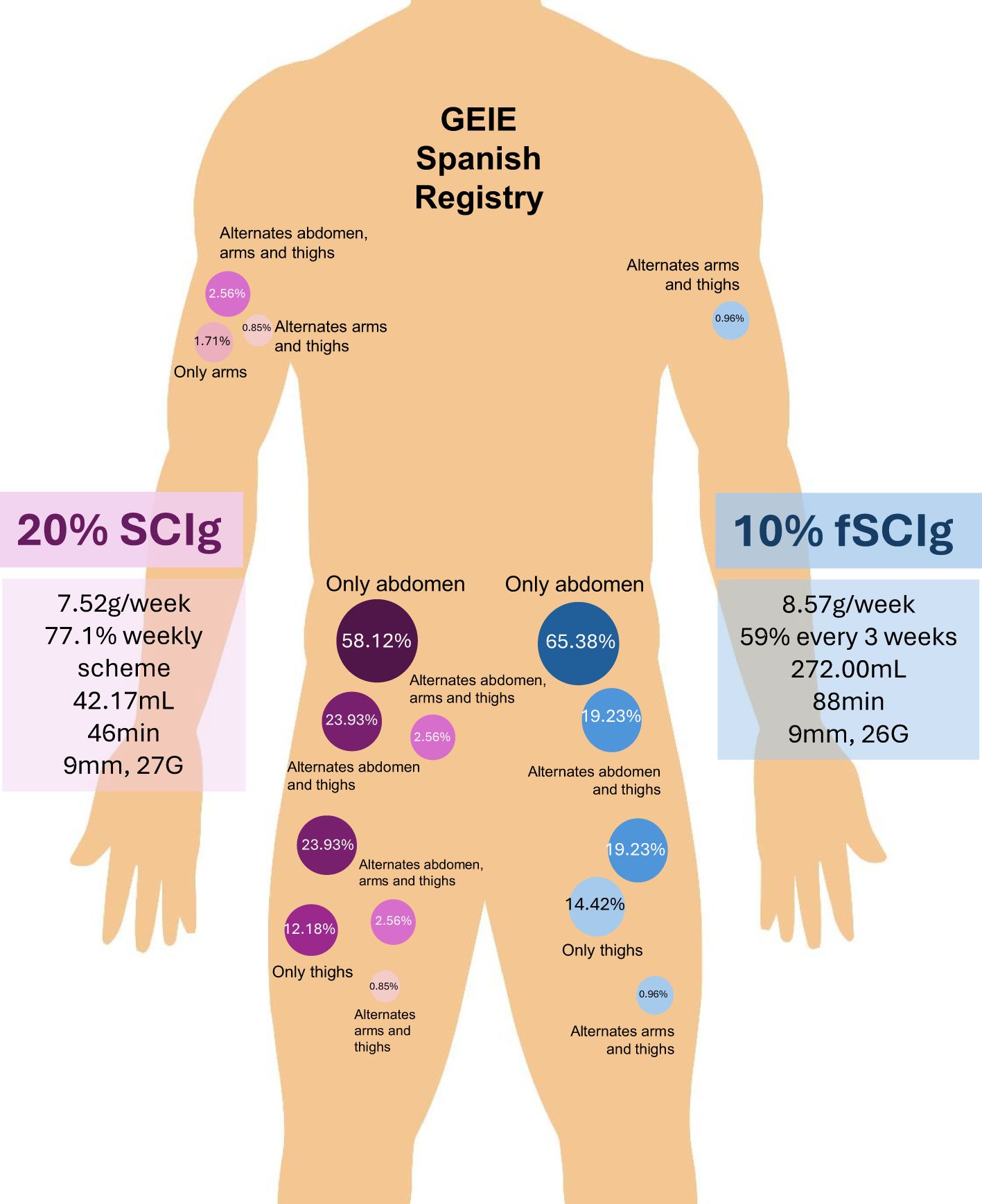
Figure 2. Injection site distribution and administration characteristics of subcutaneous immunoglobulin (SCIg) therapy in GEIE Spanish Registry.
Patients attended an average of 3 educational sessions (SD: 1.14) for training on SCIg self-administration. Only one patient of the whole cohort administered SCIg in the hospital, while the rest, administered them at home. The average distance from the patient’s residence to the hospital was 31.14 km (SD: 40.13).
When comparing 20% SCIg versus 10% fSCIg characteristics (Table 1), age did not differ significantly between groups nor did the sex distribution. The average weekly SCIg dose was significantly lower in the 20% SCIg group (7.52 g/week, SD: 2.21) compared to the 10% fSCIg group (8.57 g/week, SD: 3.34; p = 0.007). Although these differences were uniformly distributed across PID and SID, the mean weekly dose did not significantly differ between PID and SID for either formulation (Table 2). No significant differences were found when comparing IgG trough levels for both types of SCIg. Mean infusion volume for 20% SCIg was 42.17 mL (SD: 15.54) and 272mL (SD: 83.65) for 10% fSCIg (p < 0.0001). Conversely, average infusion time was significantly longer for 10% fSCIg (88.31 minutes, SD: 56.85) than for 20% SCIg (46.08 minutes, SD 17.07; p < 0.0001). Most patients receiving SCIg 20% (77.1%) were on a weekly dosing schedule, with 22.9% receiving infusions biweekly. In contrast, the majority of 10% fSCIg recipients followed less frequent regimens, with 59.0% on a three-week cycle and 38.1% on a monthly schedule. However, isolated cases of 10% fSCIg users required weekly or biweekly administration. No significant difference was observed in the number of injection points per infusion.
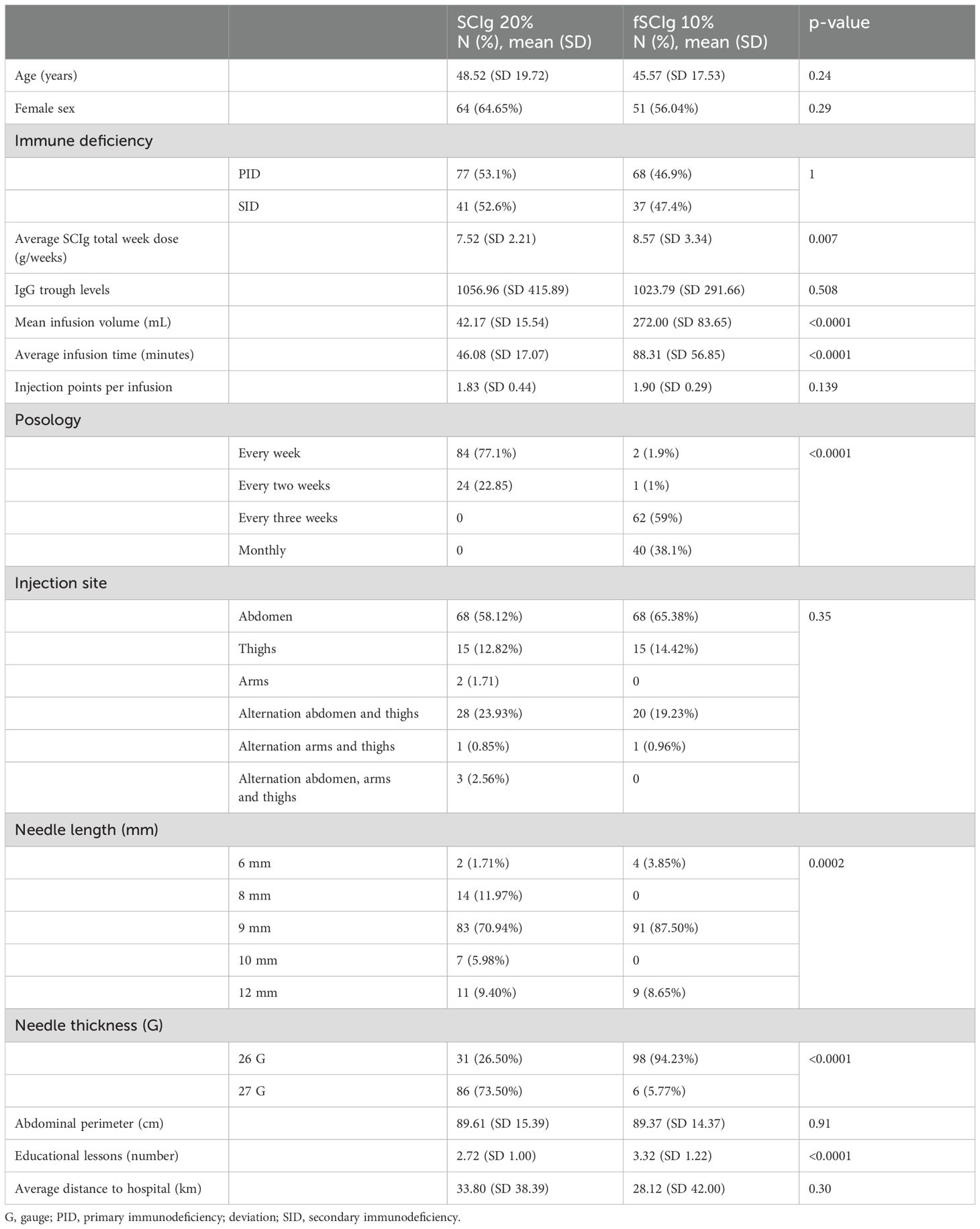
Table 1. Demographic, clinical, and administration characteristics of patients treated with 20% vs. 10% facilitated subcutaneous immunoglobulin (fSCIg).
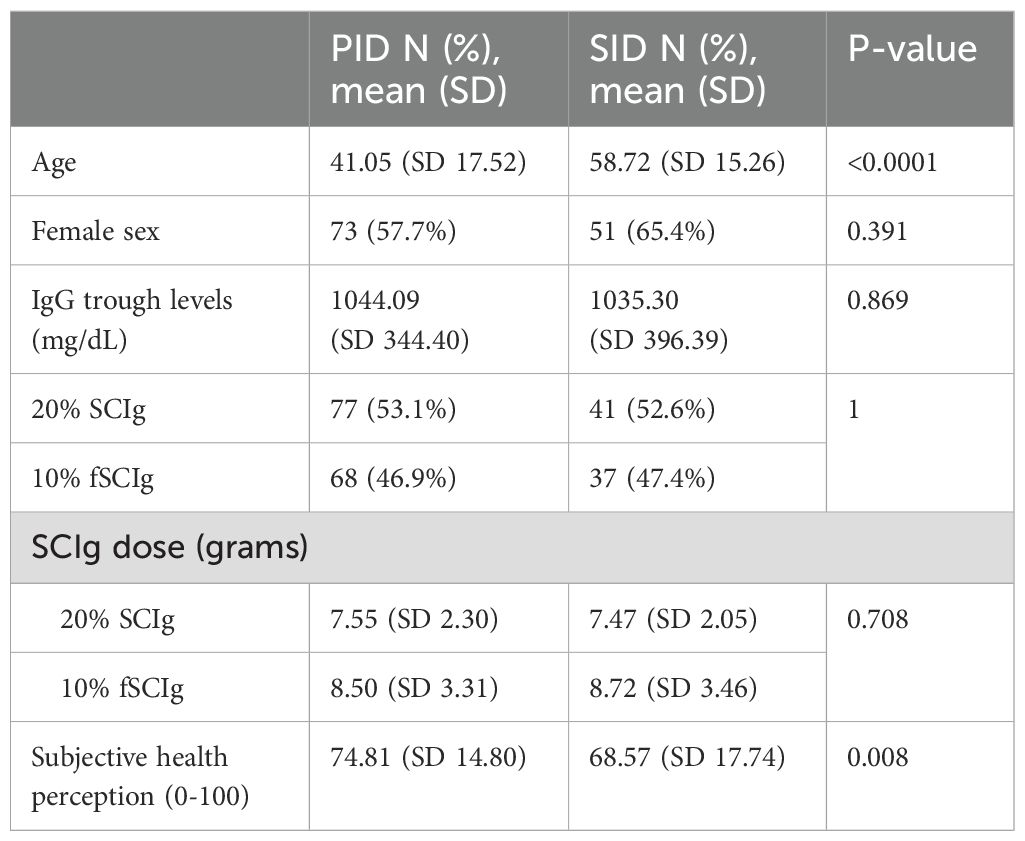
Table 2. Comparison of demographic, clinical, and treatment characteristics between primary immunodeficiency (PID) and secondary immunodeficiency (SID) patients across different subcutaneous immunoglobulin (SCIg) formulations.
Regarding injection sites, similar proportions of patients used the abdomen as the primary site. Needle characteristics varied, with 20% SCIg patients predominantly using 9 mm length (70.94%), while a greater variety of needle lengths were observed in the 10% fSCIg group. Needle thickness differed notably, with 26G needles predominantly used in 10% fSCIg (94.23%), whereas SCIg 20% patients primarily used 27G (73.50%; p < 0.0001). There was no significant difference in abdominal perimeter or distance to hospital. However, 10% fSCIg patients required a significantly higher number of educational lessons (3.32, SD 1.22) compared to those receiving 20% SCIg (2.72, SD 1.00; p < 0.0001).
Adverse reactions, both local and systemic, were assessed in patients receiving 20% versus 10% fSCIg, with no overall differences observed (p=0.16 and p=0.08, respectively). However, detailed analysis revealed that certain local adverse reactions, such as local rash (58.65% vs. 36.94%, p=0.002) and pruritus (59.62% vs. 38.74%, p=0.004), were significantly more frequent in the 10% fSCIg group. Systemic reactions, including headache (25.96% vs. 13.68%, p=0.03) and fever (10.58% vs. 1.71%, p=0.01), were also notably higher in patients receiving 10% fSCIg. Additional details on adverse reactions are presented in Table 3.
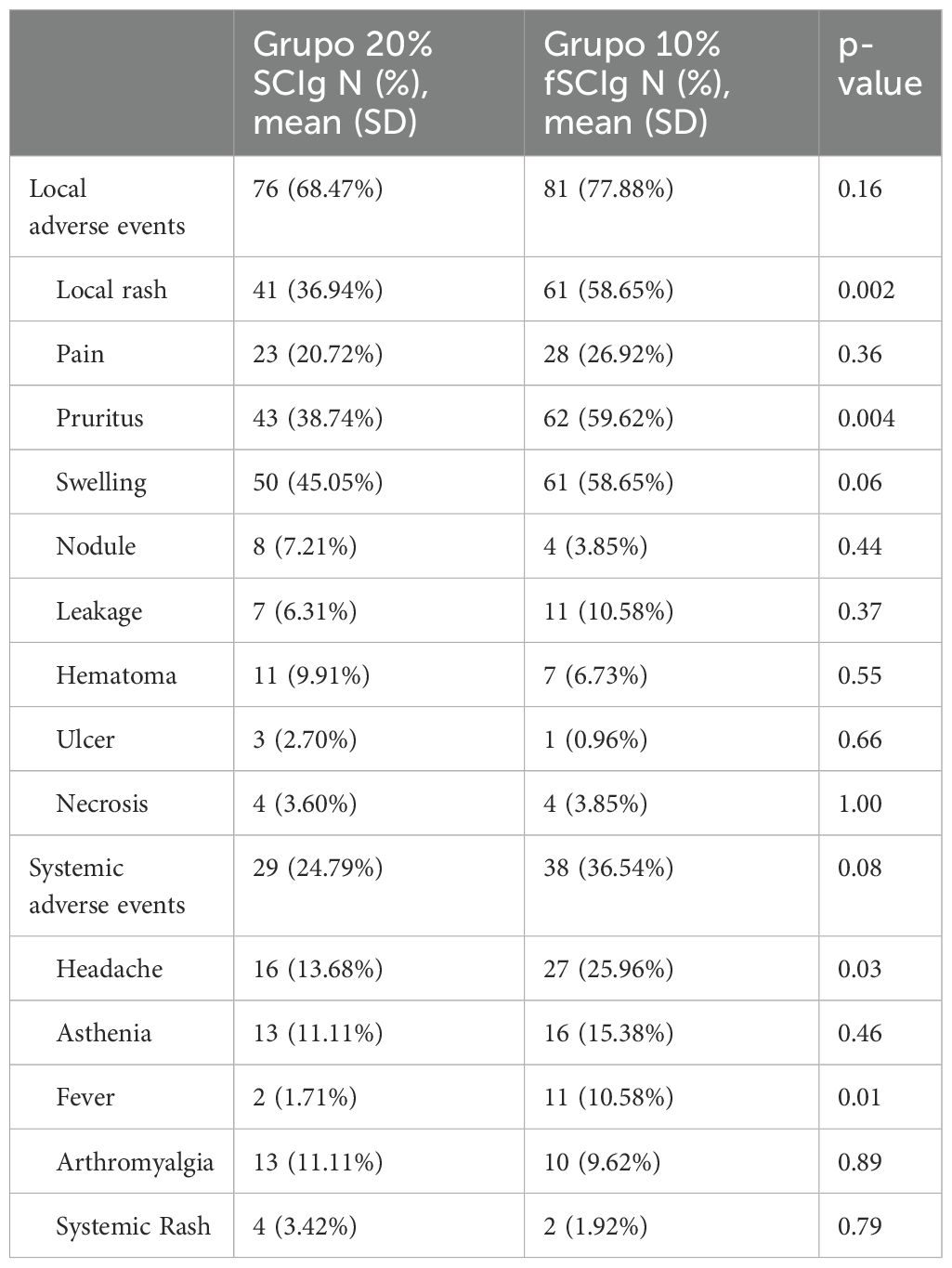
Table 3. Local and systemic adverse events in patients treated with 20% vs. 10% fSCIg.
Local adverse events were investigated concerning the simultaneous use of antiplatelet agents or oral and subcutaneous anticoagulants. No significant differences were observed in the incidence of local adverse effects between patients receiving SCIg who were also undergoing antiplatelet or anticoagulant therapy and those who were not. The occurrence of local reactions, including swelling, rash, and pain, was comparable across all groups. Further details are represented in Tables 4, 5.
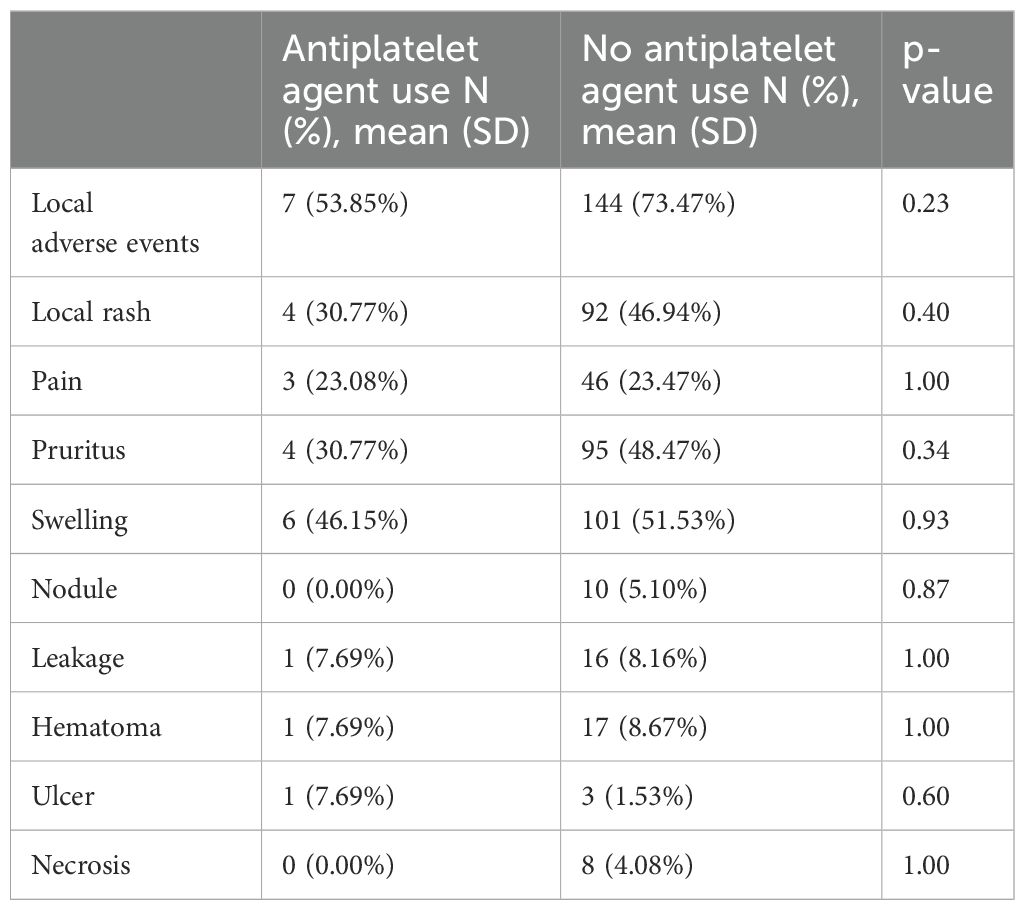
Table 4. Local adverse events in relation to antiplatelet agent use.
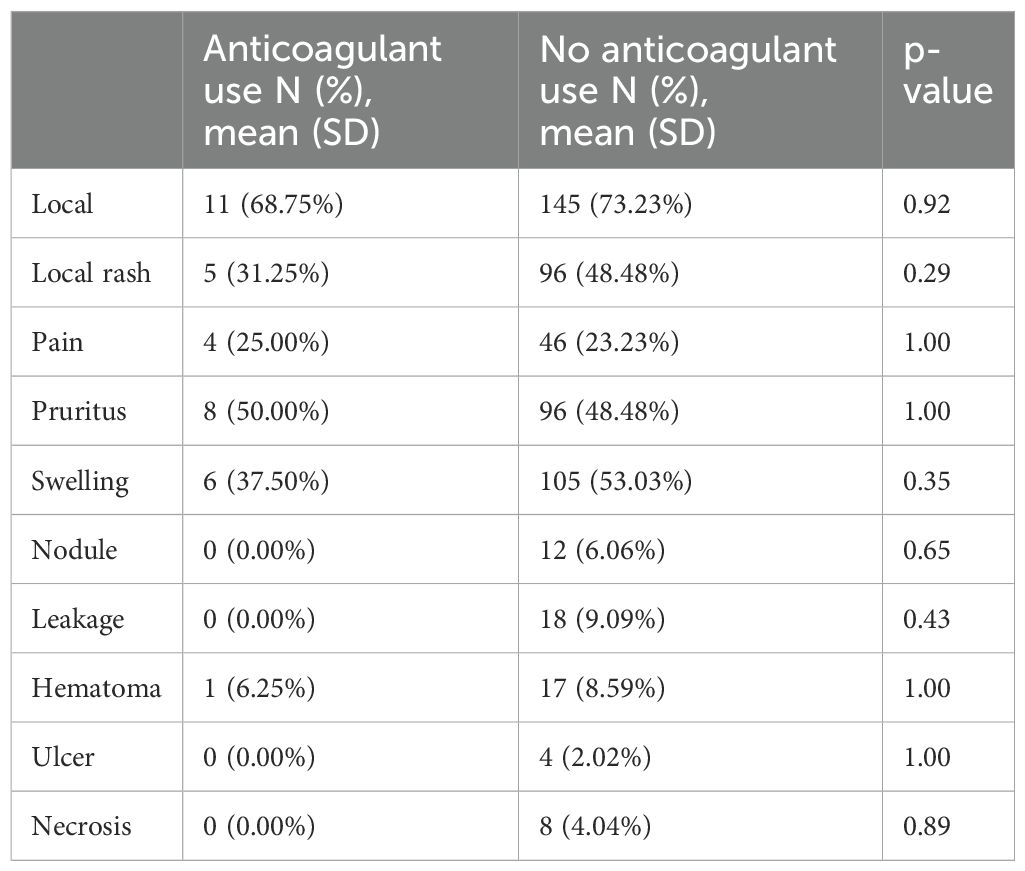
Table 5. Local adverse events in relation to anticoagulant use.
In terms of employment, 40% (n=88) were employed, 14.55% (n=32) were students, and 16.82% (n=37) had a disability allowance. The remaining participants were either retired (24.09%, n=53) or unemployed (4.55%, n=10).
The Gijón Scale (13) was applied to assess family situation, monthly income, housing conditions, social relationships, and social network support (Table 6). Nearly half (47.06%) of patients live independently with family, and 31.67% reside with a spouse of similar age. Economically, most patients (51.64%) report incomes above 1.5 times the minimum wage, while 15.49% earn below the minimum contributory pension. All patients have adequate housing, and a substantial majority (94.42%) maintain active social relationships, with 99.54% reporting support from family or neighbors.
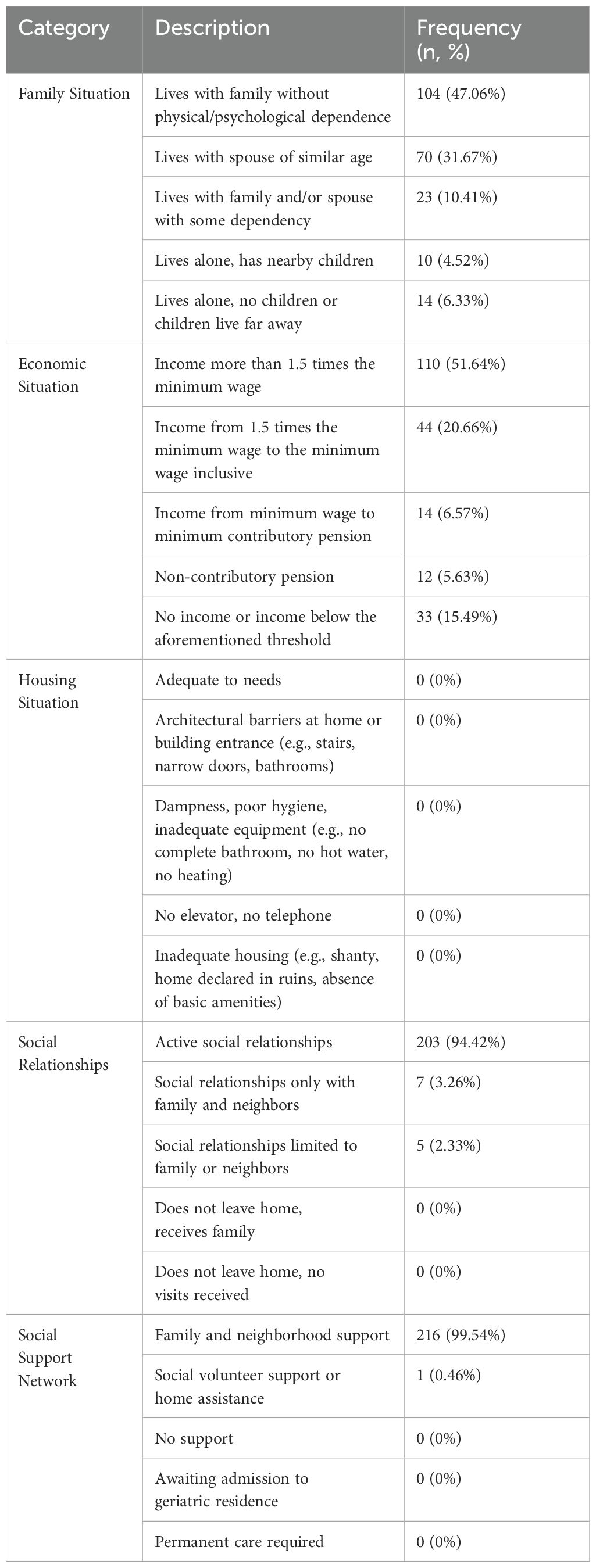
Table 6. Gijón scale categories: family situation, economic situation, housing situation, social relationships, and social support network.
Additionally, EuroQol-5D-3L questionnaire (14) was also applied for the evaluation of mobility, self-care ability, daily activities, presence of pain, anxiety and depression. Patients generally experience few limitations. Most report no issues with mobility (79.72%) and personal care (89.86%), with a large proportion (77.42%) able to perform daily activities independently. Pain is minimal for 66.82%, and anxiety affects only 21.40% at moderate levels, with severe cases being rare (1.40%). The average subjective health rating stands at 72.69/100. Significant differences were found in this subjective health perception between PID and SID, with SID patients having significantly lower scores (68.57/100) than PID patients (74.81/100) (p=0.008) (Table 2). Further details are represented in Table 7.
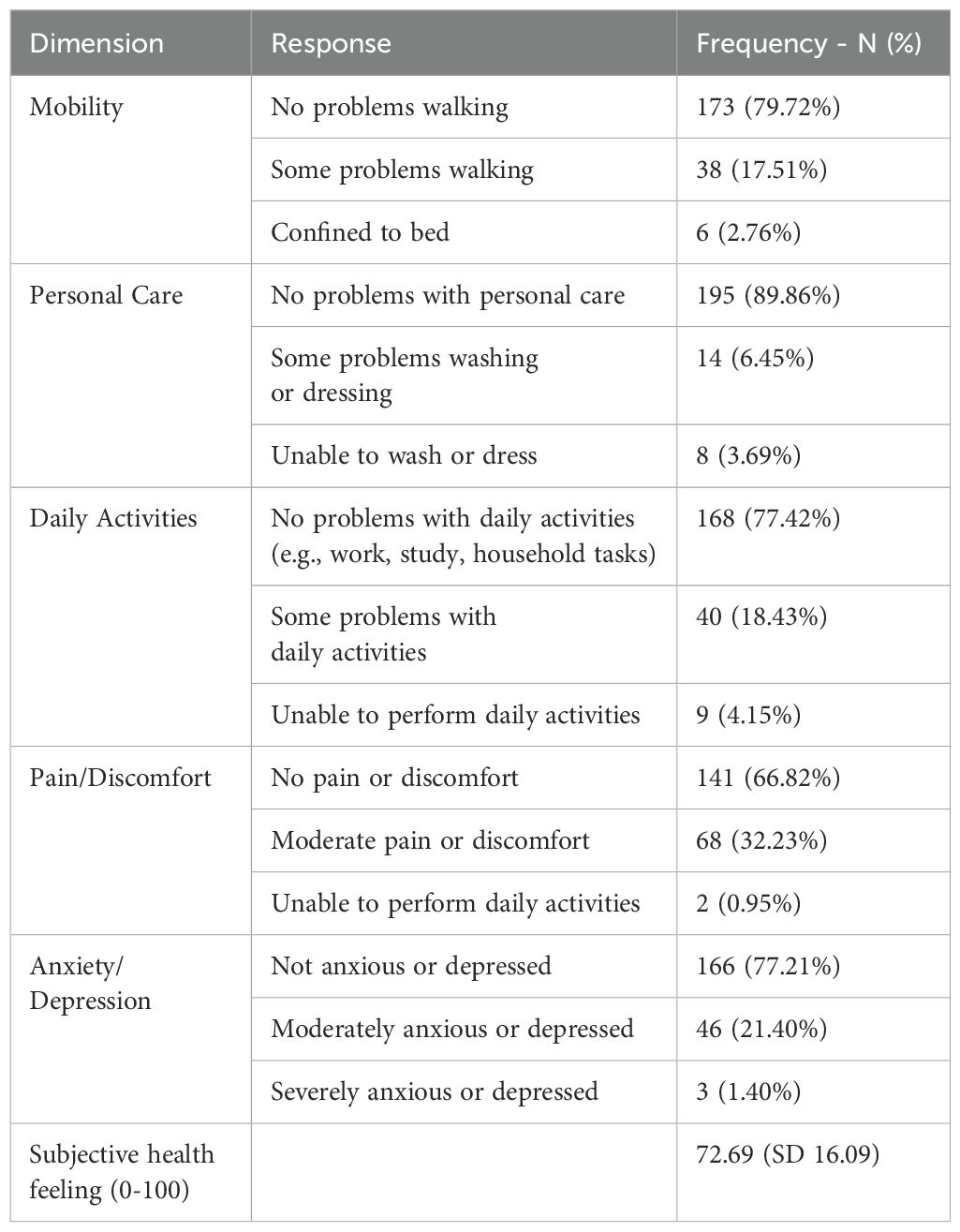
Table 7. EuroQol-5D-3L scale dimensions: mobility, personal care, daily activities, pain/discomfort, anxiety/depression, and subjective health perception.
This study provides important real-world data on the use of different SCIg formulations in patients with PID and SID across multiple centers in Spain. Our findings confirm the overall effectiveness of SCIg in maintaining adequate IgG levels and demonstrate a favorable safety profile, with no significant differences in overall adverse event rates between the 10% and 20% formulations. Ten percent SCIg was linked to higher frequencies of certain mild local and systemic adverse events, such as local rash and fever, yet its dosing schedule resulted in less disruption to daily life. Quality-of-life assessments revealed minimal limitations in daily activities, underscoring SCIg potential to enhance patient autonomy and satisfaction. These results highlight the need for individualized treatment strategies and underscore the vital role of expert immunodeficiency nursing teams in ensuring safe and effective SCIg administration.
Most real-world studies on SCIg focus on small, highly homogeneous subgroups of patients, either with PID or SID, or those receiving a specific type of Ig, either 10% or 20% formulations (15–22). This approach does not accurately reflect everyday practice in specialized nursing units or outpatient immunodeficiency clinics, where both types of immunodeficiencies and different Ig formulations are commonly managed. By including all four patient subgroups, our study extends the applicability of SCIg recommendations to both younger and older patients, as demonstrated by the significantly higher mean age for SID in our cohort compared to PID, and to patients with diverse and complex comorbidities. These include immune dysregulation inherent to certain PIDs, patients who have undergone chemotherapy regimens, those who have received hematologic or solid organ transplants, and individuals on anticoagulant or antiplatelet therapy. Our findings provide consistent evidence on the tolerability, efficacy, and quality-of-life impact of SCIg across different formulations for a broader patient population.
Comparing these findings to prior studies, this study reinforces previous evidence that SCIg therapy, independently of its formulation, is an effective alternative to IVIg for achieving adequate IgG levels in patients with immunodeficiency (5, 6). Our findings align with previous real-world data, showing that 10% fSCIg is typically administered every three weeks or monthly, resulting in a lower treatment burden and minimal interference with daily activities, while 20% SCIg is administered on a weekly to biweekly schedule (18, 21). No significant differences in IgG trough levels were observed between the 20% and 10% SCIg groups, despite the significantly lower average weekly dose in the 20% SCIg group, regardless of PID or SID status. This outcome may be explained by pharmacokinetic differences between the formulations and suggests potential cost-effectiveness in specific contexts, even though more frequent monthly injections and infusion sessions are required.
Most patients also used a mean of 2 sites per infusion in our cohort (21). However, needle length and caliber was relatively lower in our report than in previous experiences for both presentations (15, 18–20). Patients in our cohort treated with 10% fSCIg formulations required more educational sessions for self-administration, consistent with previous findings (16). Consequently, 20% SCIg may be a more suitable and simpler option for patients who have relatively more difficulty with self-administration. These results underscore the importance of a dedicated nursing team in educating and supporting patients using SCIg.
In recent years, the transition from IVIg to SCIg has been promoted, as SCIg administration offers significant advantages, including reduced systemic adverse reactions and the convenience of home-based treatment, both of which have been shown to improve patient satisfaction and autonomy (23–25). Despite its benefits, the use of SCIg in Spain remains suboptimal. This is largely due to the long-standing preference for IVIg, limited training among healthcare professionals in SCIG administration, established IVIg-specific infrastructure, and a general lack of familiarity with SCIG protocols. Data from the Spanish GTEM-SEMI-CVID registry reveal that the majority of CVID patients in Spain continue to receive IVIg, underscoring the need for sustained efforts to facilitate the transition to SCIg (9). In our cohort, 66% of patients were previously treated with IVIg and have continued this regimen, while the remaining patients initiated SCIg directly following the identification of the need for IgRT.
It is essential to recognize that SCIg administration can be associated with both local and systemic adverse effects. The variation in adverse reactions observed between different SCIg formulations in our study aligns with international findings, suggesting that formulation concentration may significantly influence patient tolerance and comfort (6). Our study reports one of the highest rates of local adverse events compared to other cohorts (12, 18, 22, 26), likely due to the inclusion of typically expected local infusion reactions associated with subcutaneous administration. Moreover, we observed a notably high rate of systemic adverse events, potentially due to the large proportion of patients using 10% fSCIg in our cohort, compared to other studies where the sample size for 10% fSCIg users was limited (12). Additionally, this information was collected through patient-reported questionnaires as part of our patient-experience-centered approach, capturing cumulative experiences over time rather than measured data from a specific observational period. Consequently, direct comparisons with other studies may be limited.
We have reported that facilitated 10% fSCIg has been related to the development of more local adverse events than 20% SCIg, as previously described (15, 16); in our case, specifically, pruritus and rash. When exploring the relationship between the development of local complications and the concomitant use of antiplatelet or anticoagulant therapies, no significant differences were found. This concurs with previous evidence and supports the safety of SCIg in these groups of patients (27, 28). Additionally, 10% fSCIg was significantly associated with the development of systemic adverse events when compared to 20% SCIg in our cohort. In this regard, we have noted that fever and headache have been significantly more frequently observed in the 10% fSCIg group, as documented by other studies (17, 18, 29). In fact, in the FIGARO study with 156 patients, systemic adverse reactions were reported in 7.4% of all visits, with flu-like symptoms, fatigue, fever, and headache being the most commonly reported reactions (18). However, some reports have not documented this difference, possible related to very low sample size (16). Interestingly, in a study including 327 patients with CVID receiving IGRT under several administration routes reported similar degrees of concern regarding IgRT related adverse events independently of the administration route (30). This highlights the need for thoroughly informing patients about these differences in adverse reactions so they can collaboratively select the preferred route of administration, ensuring their choice aligns with their tolerance and comfort preferences.
The analysis of socioeconomic status and health perception offers valuable insights into the well-being and characteristics of the patient population receiving SCIg, as previously reported in studies devoted to the quality of life in patients undergoing this therapy (23–25). Employment data show a diverse mix of active workers, students, individuals on disability allowances, and retirees, reflecting varying levels of economic independence within this cohort. Despite these differences, the Gijón Scale demonstrates overall socioeconomic stability, with the majority of patients living in adequate housing, maintaining active social connections, and benefiting from strong family and neighborhood support. Additionally, caregiver involvement is minimal due to the high degree of patient autonomy achieved through home-based SCIg administration, which is facilitated by comprehensive educational programs provided by expert nursing teams.
Health perception, evaluated using the EuroQol-5D-3L, shows generally positive outcomes, with few limitations in mobility, personal care, or daily activities, and a low incidence of severe pain or discomfort, irrespective of socioeconomic status. This stability is likely supported by Spain’s comprehensive public healthcare system, which ensures free access to nursing and medical care, as well as to all necessary consumables, SCIg, and infusion pumps. These findings underscore the economic, social, and educational characteristics of this patient population and the crucial role of structured support systems in promoting long-term adherence and well-being.
While anxiety and depression are present, they are generally moderate. These findings suggest that patients demonstrate resilience in daily functioning, though ongoing psychological and social support remains essential to address the needs of those experiencing significant discomfort or mental health challenges. The average subjective health rating of 72.69 out of 100 further reflects a positive but improvable perception of well-being. However, significant differences in subjective health perception were observed between PID and SID patients, with SID patients reporting lower scores. This underscores the need to address not only social and economic factors but also the impact of comorbidities and the type of immunodeficiency to enhance patient adherence and satisfaction with SCIg. Multidisciplinary support—particularly from expert nursing teams—plays a critical role in tailoring care and optimizing long-term outcomes for this diverse patient population.
The study has several strengths. Its multicentric approach, involving diverse immunodeficiency units across Spain, enhances the generalizability of findings and captures a comprehensive patient population with varied backgrounds and health status. The large sample size and standardized data collection through the GEIE Spanish Registry provide robust evidence of SCIg’s real-world effectiveness and tolerance in patients with PID and SID. Additionally, the focus on both clinical outcomes and socio-economic impact is unique, offering a holistic view of SCIg’s benefits and challenges in this population.
However, this study has limitations that should be noted. The retrospective design may introduce biases, as certain patient details and adverse reactions may have been overreported or inconsistently documented, and also affected by memory bias. Additionally, the absence of a control group treated with IVIg limits the ability to directly compare the efficacy and safety of SCIg versus IVIg within this cohort. In this regard, the study did not investigate the reasons for transitioning from IVIg to SCIg, which remains an important area for future exploration. Moreover, a prospective record of the number of mild and severe or recurrent infections was not performed, and we only assessed effectiveness in maintaining IgG trough levels. The absence of a pediatric population also limits the evidence of this study to patients over 14 years old. Lastly, although the multicentric design strengthens generalizability, variations in training and administration practices across centers could influence patient outcomes and perceptions of SCIg therapy.
This multicenter study provides valuable real-world insights into the use of SCIg therapy in patients with PID and SID across Spain. Our findings confirm SCIg effectiveness in maintaining adequate IgG levels and its adequate safety profile, along with the associated benefits of increased patient autonomy and quality of life. The study emphasizes the need for tailored treatment strategies that consider not only the formulation and potential adverse effects but also factors such as dosing schedules, patient preferences, and the specific clinical and socioeconomic profile of each individual. The socioeconomic assessment highlights that most patients benefit from stable housing and robust social support networks, which, together with Spain’s comprehensive public health system, may contribute to the generally positive health perceptions observed. Understanding the factors influencing the transition from IVIg to SCIg, including social, demographic, and patient preferences, represents a valuable area of research for future studies and for establishing switching protocols. Overall, our results underscore the importance of personalized care and the role of dedicated nursing teams in supporting optimal outcomes and patient satisfaction with SCIg therapy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
SM: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. VG-B: Formal analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing. PM: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. CM: Investigation, Writing – original draft, Writing – review & editing. EE: Conceptualization, Writing – original draft, Writing – review & editing. MCMB: Investigation, Writing – original draft, Writing – review & editing. HB-M: Investigation, Writing – original draft, Writing – review & editing. SG: Investigation, Writing – original draft, Writing – review & editing. BP: Investigation, Writing – original draft, Writing – review & editing. ME: Investigation, Writing – original draft, Writing – review & editing. MMM: Investigation, Writing – original draft, Writing – review & editing. IC: Investigation, Writing – original draft, Writing – review & editing. AL: Investigation, Writing – original draft, Writing – review & editing. CH: Investigation, Writing – original draft, Writing – review & editing. LR-L: Investigation, Writing – original draft, Writing – review & editing. RG: Investigation, Writing – original draft, Writing – review & editing. MC-N: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was partially funded by the Ayudas a la Investigación 2024 program, granted by the Official College of Nursing of Valencia (Colegio Oficial de Enfermería de Valencia).
We would like to express our gratitude to the Official College of Nursing of Valencia (Colegio Oficial de Enfermería de Valencia) for their support through the Ayudas a la Investigación 2024 program. We also thank all members of the GEIE Spanish Registry for their invaluable contributions to this study. Additionally, we acknowledge the European Society for Immunodeficiencies (ESID) for their support to the last author, which greatly enhanced the development of this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1532367/full#supplementary-material
1. Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol. (2006) 117:S525–53. doi: 10.1016/j.jaci.2006.01.015
2. Wood P, Stanworth S, Burton J, Jones A, Peckham DG, Green T, et al. Recognition, clinical diagnosis and management of patients with primary antibody deficiencies: a systematic review. Clin Exp Immunol. (2007) 149:410–23. doi: 10.1111/j.1365-2249.2007.03432.x
3. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Hizentra, INN-human normal immunoglobulin: Summary of Product Characteristics . Available online at: https://cima.aemps.es/cima/pdfs/es/ft/11687006/FT_11687006.html.pdf (Accessed October 31, 2024).
4. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). HyQvia, INN-human normal immunoglobulin (SCIg): Summary of Product Characteristics .Available online at: https://cima.aemps.es/cima/pdfs/es/ft/113840001/FT_113840001.html.pdf (Accessed October 31, 2024).
5. Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol. (2012) 32:1180–92. doi: 10.1007/s10875-012-9720-1
6. Wasserman RL, Melamed I, Stein MR, Gupta S, Puck J, Engl W, et al. Recombinant human hyaluronidase-facilitated subcutaneous infusion of human immunoglobulins for primary immunodeficiency. J Allergy Clin Immunol. (2012) 130:951–7.e11. doi: 10.1016/j.jaci.2012.06.021
7. Shabaninejad H, Asgharzadeh A, Rezaei N, Rezapoor A. A comparative study of intravenous immunoglobulin and subcutaneous immunoglobulin in adult patients with primary immunodeficiency diseases: A systematic review and meta-analysis. Expert Rev Clin Immunol. (2016) 12:595–602. doi: 10.1586/1744666X.2016.1155452
8. Fu LW, Song C, Isaranuwatchai W, Betschel S. Home-based subcutaneous immunoglobulin therapy vs hospital-based intravenous immunoglobulin therapy: A prospective economic analysis. Ann Allergy Asthma Immunol. (2018) 120:195–9. doi: 10.1016/j.anai.2017.11.002
9. Cabañero-Navalon MD, Garcia-Bustos V, Nuñez-Beltran M, Císcar Fernández P, Mateu L, Solanich X, et al. Current clinical spectrum of common variable immunodeficiency in Spain: The multicentric nationwide GTEM-SEMI-CVID registry. Front Immunol. (2022) 13:1033666. doi: 10.3389/fimmu.2022.1033666
10. Legendre P, Chahwan D, Marjanovic Z, Vignon M, Hermine O, Lortholary O, et al. Utilization of intravenous or subcutaneous immunoglobulins in secondary immune deficiency (ULTIMATE): A retrospective multicenter study. Clin Immunol. (2020) 215:108419. doi: 10.1016/j.clim.2020.108419
11. Benbrahim O, Viallard JF, Choquet S, Royer B, Bauduer F, Decaux O, et al. A French observational study describing the use of human polyvalent immunoglobulins in hematological Malignancy-associated secondary immunodeficiency. Eur J Haematol. (2018) 101:48–56. doi: 10.1111/ejh.13078
12. Cinetto F, Neri R, Vianello F, Visentin A, Barilà G, Gianese S, et al. Subcutaneous immunoglobulins replacement therapy in secondary antibody deficiencies: Real life evidence as compared to primary antibody deficiencies. PloS One. (2021) 16:e0247717. doi: 10.1371/journal.pone.0247717
13. García-González JV, Díaz-Palacios E, Salamea A, Cabrera D, Menéndez A, Fernández-Sánchez A, et al. Evaluación de la fiabilidad y validez de una escala de valoración social en el anciano. Aten Primaria. (1999) 23:434–40.
14. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. (2001) 33:337–43. doi: 10.3109/07853890109002087
15. Yalcin Gungoren E, Yorgun Altunbas M, Dikici U, Meric Z, Eser Simsek I, Kiykim A, et al. Insights into patient experiences with facilitated subcutaneous immunoglobulin therapy in primary immune deficiency: A prospective observational cohort. J Clin Immunol. (2024) 44:169. doi: 10.1007/s10875-024-01771-0
16. Hustad NB, Degerud HM, Hjelmerud I, Fraz MSA, Nordøy I, Trøseid M, et al. Real-world experiences with facilitated subcutaneous immunoglobulin substitution in patients with hypogammaglobulinemia, using a three-step ramp-up schedule. Front Immunol. (2021) 12:670547. doi: 10.3389/fimmu.2021.670547
17. Wiesik-Szewczyk E, Sołdacki D, Paczek L, Jahnz-Różyk K. Facilitated subcutaneous immunoglobulin replacement therapy in clinical practice: A two center, long-term retrospective observation in adults with primary immunodeficiencies. Front Immunol. (2020) 11:981. doi: 10.3389/fimmu.2020.00981
18. Borte M, Hanitsch LG, Mahlaoui N, Fasshauer M, Huscher D, Speletas M, et al. Facilitated subcutaneous immunoglobulin treatment in patients with immunodeficiencies: the FIGARO study. J Clin Immunol. (2023) 43:1259–71. doi: 10.1007/s10875-023-01470-2
19. Dimou M, Speletas M, Milito C, Pyzik A, Huscher D, Kamieniak M, et al. Insights into facilitated subcutaneous immunoglobulin use in patients with secondary immunodeficiency diseases: A FIGARO subgroup analysis. Cancers (Basel). (2023) 15:4524. doi: 10.3390/cancers15184524
20. Fasshauer M, Borte M, Bitzenhofer M, Pausch C, Pittrow D, Park M, et al. Real-world use, safety, and patient experience of 20% Subcutaneous immunoglobulin for primary immunodeficiency diseases. Adv Ther. (2023) 40:5168–87. doi: 10.1007/s12325-023-02649-0
21. Rosenbach K, Park M, Sanchirico M, Nwose O, Paris K. Real-world evidence of tolerability of 20% Subcutaneous immunoglobulin treatment. J Clin Immunol. (2023) 43:912–20. doi: 10.1007/s10875-023-01436-4
22. Viallard JF, Agape P, Barlogis V, Cozon G, Faure C, Fouyssac F, et al. Treatment with Hizentra in patients with primary and secondary immunodeficiencies: a real-life, non-interventional trial. BMC Immunol. (2016) 17:34. doi: 10.1186/s12865-016-0169-5
23. Anterasian C, Duong R, Gruenemeier P, Ernst C, Kitsen J, Geng B. Quality of life differences for primary immunodeficiency patients on home SCIG versus IVIG. J Clin Immunol. (2019) 39:814–22. doi: 10.1007/s10875-019-00705-5
24. Mallick R, Jolles S, Kanegane H, Agbor-Tarh D, Rojavin M. Treatment satisfaction with subcutaneous immunoglobulin replacement therapy in patients with primary immunodeficiency: a pooled analysis of six hizentra® Studies. J Clin Immunol. (2018) 38:886–97. doi: 10.1007/s10875-018-0562-3
25. Vultaggio A, Azzari C, Milito C, Finocchi A, Toppino C, Spadaro G, et al. Subcutaneous immunoglobulin replacement therapy in patients with primary immunodeficiency in routine clinical practice: the VISPO prospective multicenter study. Clin Drug Investig. (2015) 35:179–85. doi: 10.1007/s40261-015-0270-1
26. Rubinstein A, Mabudian M, McNeil D, Patel NC, Wasserman RL, Gupta S, et al. Long-term safety of facilitated subcutaneous immunoglobulin 10% treatment in us clinical practice in patients with primary immunodeficiency diseases: results from a post-authorization safety study. J Clin Immunol. (2024) 44(8):181. doi: 10.1007/s10875-024-01769-8
27. Stein MR, Koterba A, Rodden L, Berger M. Safety and efficacy of home-based subcutaneous immunoglobulin G in elderly patients with primary immunodeficiency diseases. Postgrad Med. (2011) 123:186–93. doi: 10.3810/pgm.2011.09.2474
28. Kuryan J, Galowitz S, Kaplan B. Tolerability of subcutaneous immunoglobulin (SCIG) in patients receiving antiplatelet (AP) and anticoagulant (AC) therapy. J Clin Immunol. (2012) 129(2 Suppl):AB247.
29. Dimou M, Iliakis T, Maltezas D, Bitsani A, Kalyva S, Koudouna A, et al. Efficacy-safety of facilitated subcutaneous immunoglobulin in immunodeficiency due to hematological Malignancies. A Single-Center Retrospective Analysis Anticancer Res. (2018) 38:4187–91. doi: 10.21873/anticanres.12712
Keywords: subcutaneous immunoglobulin (SCIg), primary immunodeficiency (PID), secondary immunodeficiency (SID), patient-centered outcomes, quality of life
Citation: Martínez Mercader S, Garcia-Bustos V, Moral Moral P, Martínez Buenaventura C, Escudero Vergara E, Montaner Bosch MC, Balastegui-Martín H, Galindo Maycas S, Palací Mur B, Escobar Palazón M, Moreno Mulet M, Campanero Carrasco I, López A, Hernández Ruiz CD, Ruiz-López L, Guzmán Guzmán R and Cabañero-Navalon MD (2025) Patient-centered outcomes with subcutaneous immunoglobulin use for infection control in primary and secondary immunodeficiencies: data of a GEIE Spanish Registry. Front. Immunol. 16:1532367. doi: 10.3389/fimmu.2025.1532367
Received: 21 November 2024; Accepted: 22 January 2025;
Published: 14 February 2025.
Edited by:
Hirokazu Kanegane, Tokyo Medical and Dental University, JapanReviewed by:
Chrysoula Perdikogianni, University of Crete, GreeceCopyright © 2025 Martínez Mercader, Garcia-Bustos, Moral Moral, Martínez Buenaventura, Escudero Vergara, Montaner Bosch, Balastegui-Martín, Galindo Maycas, Palací Mur, Escobar Palazón, Moreno Mulet, Campanero Carrasco, López, Hernández Ruiz, Ruiz-López, Guzmán Guzmán and Cabañero-Navalon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victor Garcia-Bustos, dmljdG9yZ2FyY2lhYnVzdG9zQGdtYWlsLmNvbQ==; Pedro Moral Moral, bW9yYWxfcGVkQGd2YS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.