
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 22 January 2025
Sec. Primary Immunodeficiencies
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1492000
 Huifeng Fan1†
Huifeng Fan1† Zhiyong Yang2†
Zhiyong Yang2† Yuhui Wu3
Yuhui Wu3 Xiulan Lu4Tian Li5Xuyang Lu2
Xiulan Lu4Tian Li5Xuyang Lu2 Gen Lu1
Gen Lu1 Liming He6
Liming He6 Guoping Lu6*
Guoping Lu6* Li Huang7*
Li Huang7*Introduction: Talaromyces marneffei (T. marneffei) infections in children can occur secondary to inborn errors of immunity (IEIs). We aimed to investigate the clinical and genetic features of T. marneffei infection in Chinese pediatric patients.
Materials and methods: We retrospectively reviewed 18 pediatric patients with IEIs who were diagnosed with T. marneffei infections at five public hospitals in China from January 2015 to January 2023.
Results: The common clinical features among the patients were fever, cough, and hepatomegaly. The most common severe complications included septic shock, hemophagocytic lymphohistiocytosis (HLH), and acute respiratory distress syndrome (ARDS). Three cases presented with pan-hypogammaglobulinemia, while three other cases showed heightened levels of IgM. Elevated levels of IgE were detected in five cases, and six cases exhibited decreased T lymphocyte absolute counts. Four children were diagnosed with hyperimmunoglobulin M syndrome (HIGM) due to CD40LG mutations, three cases had severe combined immunodeficiency (SCID), and five were diagnosed with hyper-IgE syndrome (HIES). Gain-of-function (GOF) mutations in STAT1 led to STAT1 GOF in four cases. One patient was diagnosed with caspase-recruitment domain (CARD9) deficiency due to a compound mutation in the CARD9 gene, while another patient was confirmed with adenosine deaminase (ADA) deficiency.
Conclusion: T. marneffei infections in children with IEIs induced severe systemic complications. These children commonly exhibited abnormal immunoglobulin levels in peripheral blood, and underlying IEIs associated with T. marneffei infections have enhanced our understanding of the disease.
Talaromyces (formerly Penicillium) marneffei (T. marneffei) is a thermally dimorphic fungus endemic to Southeast Asia that causes systemic infections in humans (1). This fungus can grow in a filamentous form at 25°C–30°C or in a yeast-like form at 37°C (2), and it exists as yeast inside the host body (3). T. marneffei infection was first observed in bamboo rats in 1956 (4), and the first reported case of natural human infection occurred in 1973 (5). In adults, T. marneffei infection has been exclusively associated with acquired immunodeficiency syndrome (AIDS) caused by human immunodeficiency virus (HIV) infection (6). Notably, T. marneffei was ranked second among the world’s 10 most feared fungi in 2018 (7). In addition to the increasing T. marneffei infection rates among individuals with HIV, a rise in infections has also been observed in HIV-uninfected but immunocompromised patients (10.1%) since the mid-1990s (8). T. marneffei infection in HIV-uninfected children should be taken seriously, as it can lead to high mortality rates exceeding 50% in previous reports (9, 10), yet the symptoms and signs are often atypical (11). Therefore, identifying the underlying disease is a key link in the diagnosis and treatment of these patients.
In contrast to adults, pediatric patients with human inborn errors of immunity (IEIs) are more susceptible to T. marneffei infections (9, 12). The prevalence of T. marneffei infection is particularly high in HIV-uninfected pediatric patients with severe combined immunodeficiencies (SCID), hyperimmunoglobulin (hyper-IgE) syndrome (HIES), CD40LG deficiency, and others (13–15). We review the IEIs known to predispose individuals to T. marneffei infections. Understanding the pathogenesis of T. marneffei infections in HIV-uninfected patients is crucial. Additionally, it is also timely to decipher the cellular and molecular mechanisms of antifungal immunity while developing new approaches for treating T. marneffei infections.
A retrospective cohort study was conducted from January 2015 to January 2023 at five public hospitals in China. The inclusion criteria for the study were as follows (1): 28 days < age ≤ 18 years; (2) culture or histopathologically proven infections caused by T. marneffei; and (3) diagnosed IEIs. Exclusion criteria were HIV infection, cancer therapy, and organ transplantation.
The diagnosis of T. marneffei infections included a positive culture of T. marneffei from blood, bone marrow, and other clinical specimens on Sabouraud dextrose agar, following standard culture techniques. Identification was based on the morphology of the colonies. T. marneffei grew as a mold form at 25℃ and a yeast form at 37℃. At 25℃, it produced a soluble red pigment that diffused into the agar. Under the microscope, a typical broomstick shape with septal hyphae can be observed.
The diagnosis of IEIs was based on clinical characteristics and genetic tests, according to the updated classification by the Human Inborn Errors of Immunity Committee of the International Union of Immunological Societies (IUIS) (16). The predicted pathogenicity of novel variants was evaluated based on the American College of Medical Genetics and Genomics (ACMG) and the Association for Molecular Pathology (AMP) criteria (17). As noted, the National Institutes of Health (NIH) developed a clinical hyperimmunoglobulin E syndrome (HIES) scoring system (18), which can serve as a valuable reference for the diagnosis of HIES. For novel missense variants, minor allele frequency (MAF), combined annotation dependent depletion (CADD) score, and rare exome variant ensemble learner (REVEL) were used to evaluate pathogenicity.
All data were collected using a standardized form based entirely on the medical reports of each patient. The data included demographic information, domiciles, medical history, clinical manifestations, immunologic detection, genetic tests, complications, and prognosis. For patients with multiple admissions, data from the first admission were collected.
Ethical approval has been obtained from the National Key Research and Development Program of China (2021YFC2701801, 2021YFC2701803, 2021YFC2701805). All patients provided written informed consent for the use of their clinical and laboratory data from their medical reports.
A total of 18 children were enrolled in this study. The clinical features of the children are summarized in Table 1; Supplementary Table S1. There were 15 boys and 3 girls, with diagnostic ages ranging from 3 to 200 months (median age: 18.5 months). The median interval between onset and diagnosis was 0.7 months (interquartile range [IQR]: 0.33–2.0 months). The most common clinical presentations of T. marniffei infections were fever, cough, and hepatomegaly. Life-threatening complications during hospitalization included septic shock, acute respiratory distress syndrome (ARDS), hemophagocytic lymph histiocytosis (HLH), multiple organ dysfunction syndrome (MODS), and disseminated intravascular coagulation (DIC). Most patients (10/18, 55.56%) were confirmed by blood culture, with eight of them also confirmed by bone marrow specimens. In addition, two cases underwent airway mucosal biopsy. Antifungal therapy was administered in all cases, with a treatment course of 23 weeks (IQR: 12–26 weeks). Voriconazole was the most frequently used antifungal agent (10/18, 55.56%). The median length of stay was 25.5 days. However, three children (3/18, 16.67%) eventually died from T. marniffei infections (P8, P13, and P16), with recorded ages at death of 3 months, 4 months, and 17 months, respectively.

Table 1. Clinical characteristics of children with IEI with T. marneffei.
The immunologic detection and genetic tests at the time of diagnosis are shown in Table 2; Supplementary Table S2. All patients were HIV-negative, as determined by a serum-specific antibody test. The lymphocyte count, immunoglobulin and complement levels, and nitroblue tetrazolium (NBT) test results in peripheral blood were detected in all cases. Among them, three cases presented with pan-hypogammaglobulinemia (3/18, 16.67%) (P5, P12, and P13), three cases had heightened levels of IgM (3/18, 16.67%) (P6, P9, and P15), and five cases showed higher levels of IgE (5/18, 27.78%) (P1, P4, P9, P10, and P15). Low complement C3 levels were found in three cases (P8, P11, and P12). Six cases presented decreasing T lymphocyte counts, including CD 4+ and CD 8+ subsets in the results (P3, P8, P12, P13, P16, and P17). More than half of all cases (P3, P8, P9, P10, P12, P13, P14, P16, P17, and P18) had markedly decreased NK cell counts (10/18, 55.56%). The inverted CD4/CD8 ratio was observed in four patients (P4, P10, P12, and P13).
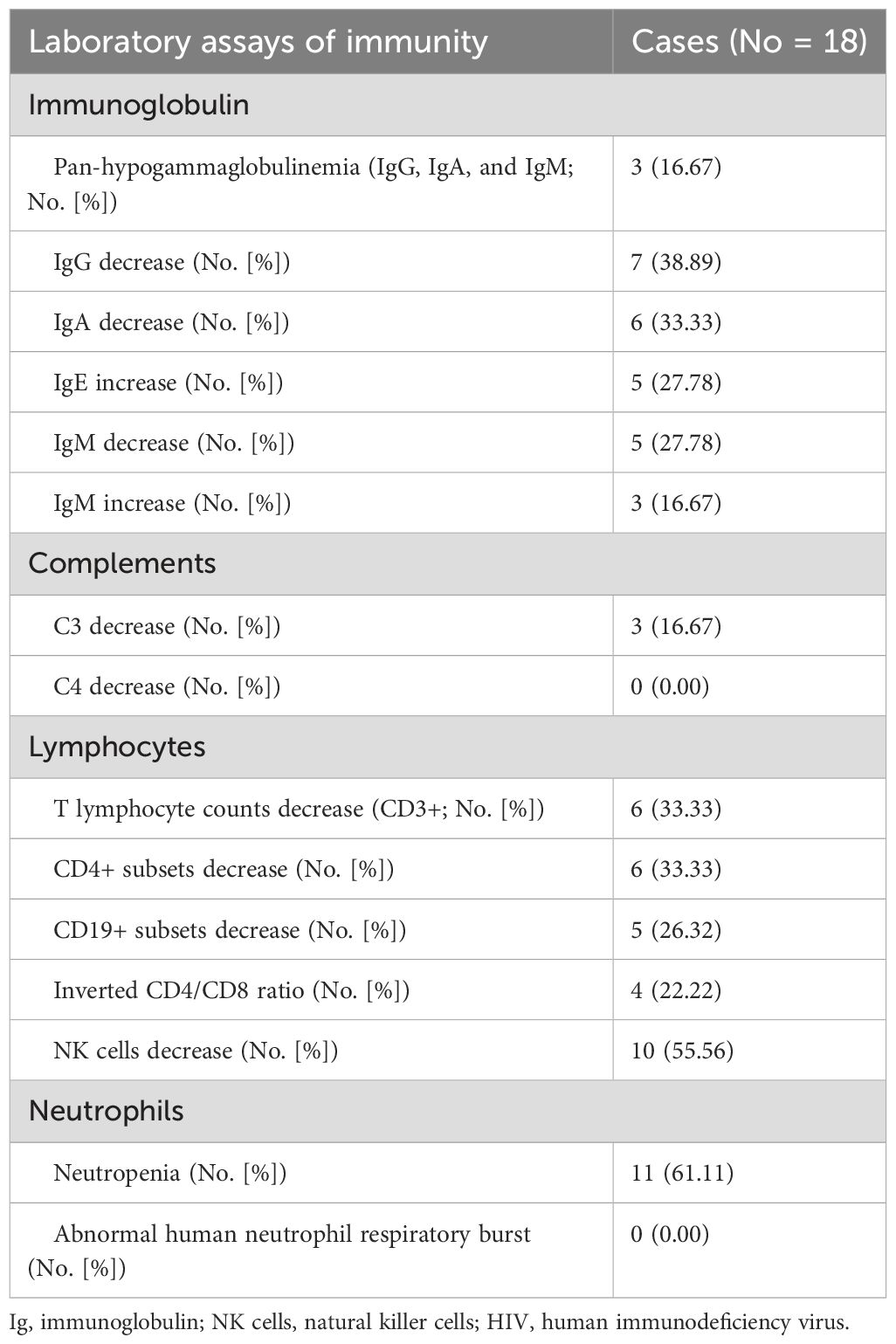
Table 2. Peripheral immunological evaluation of children with IEIs infected by T. marneffei.
In this cohort, eleven patients underwent gene panel sequencing, and whole exome sequencing (WES) was performed in seven patients. A total of 11 novel variants were identified in nine patients. According to the ACMG/AMP criteria, three novel variants were classified as likely pathogenic, and the rest were classified as pathogenic (Table 3). MAF, CADD score, and REVEL analyses were performed for four novel missense variants, and three variants were found to be harmful (P10, P15, and P16) (Supplementary Table S3). Four children (P5, P6, P7, and P14) were confirmed to have CD40 ligand deficiency due to mutations or microdeletion in the CD40LG gene. Three patients (P8, P12, and P13) were diagnosed with SCID caused by IL2RG mutations. Five cases were diagnosed with autosomal dominant-hyper immunoglobulin E syndrome (AD-HIES) due to mutations in STAT3, with a NIH score greater than 40 points for the novel STAT3 variants (Supplementary Table S4). Gain-of-function (GOF) mutations in STAT1 resulted in STAT1 GOF in four cases (P2, P3, P17 and P18). P11 was diagnosed with caspase-recruitment domain 9 (CARD9) deficiency due to compound mutations in the CARD9 gene, while P16 was confirmed to have adenosine deaminase (ADA) deficiency resulting from compound mutations in the ADA gene.
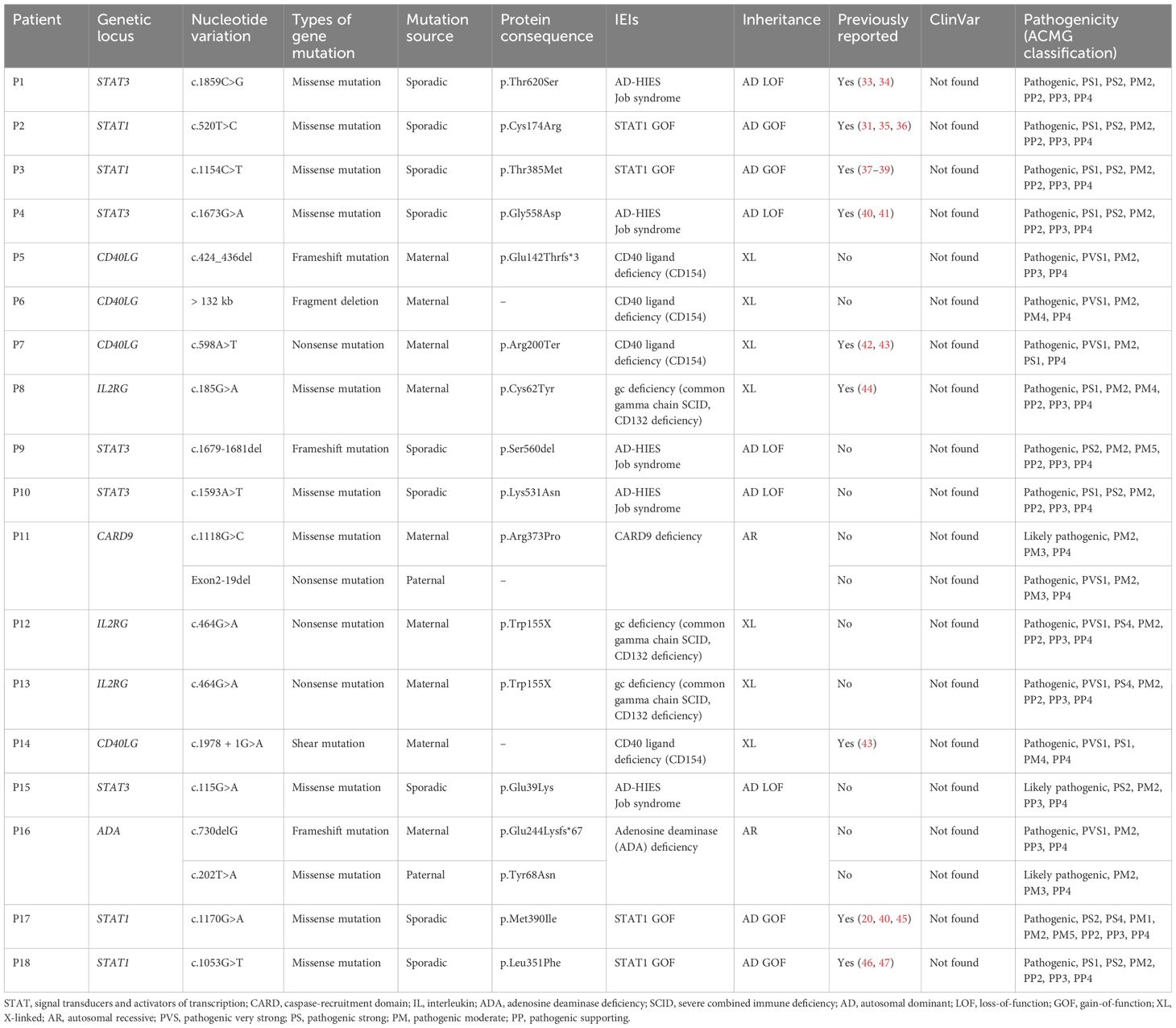
Table 3. Genetic mutations and human inborn errors of immunity in children with T. marneffei.
T. marneffei is a saprophytic pathogenic fungus capable of causing fatal systemic mycosis in immunocompromised hosts, mostly in tropical and subtropical Asia (19). In adults, T. marneffei infection predominantly affects AIDS patients, where it manifests as a severe deep mycosis with high mortality (6). With advancements in clinical immunological diagnostics, children with IEIs have been documented as vulnerable to T. marneffei infection (9, 12). Conditions such as CD40L deficiency, autosomal dominant (AD) hyper-IgE syndrome, IL-12/IFN-γ axis deficiency, and other unknown specific immune defects are increasingly associated with pediatric talaromycosis in HIV-uninfected patients (20). Furthermore, recognizing IEIs underlying T. marneffei infections is important to reduce mortality in children and facilitate the investigation of the pathogenic mechanism of T. marneffei infections. We retrospectively analyzed pediatric patients with T. marneffei infections between January 2015 and January 2023 at five public hospitals in China, all of them had diagnosed cases of IEIs through genetic testing. We summarized the clinical characteristics and peripheral immunity status of 18 children with T. marneffei infections over this decade. Meanwhile, we demonstrated diverse IEIs involving T. marneffei infections, which provides valuable insights into the pathogenic mechanisms of T. marneffei infections.
In pediatric patients with IEIs, the clinical manifestations of T. marneffei infections are more complex and severe than in HIV-infected patients (21). In this cohort, most cases presented with fever, cough, hepatosplenomegaly, lymphadenopathy, and weight loss simultaneously. Nonspecific clinical manifestations can potentially lead to the misdiagnosis of T. marneffei infection in HIV-uninfected children. However, serious complications such as HLH, septic shock, MODS, DIC, and ARDS were observed in some cases, as previously reported (22). In the present study, three fatalities were observed in children under the age of 2 years, with two cases involving infants aged 3 and 4 months, respectively. Despite rapid diagnosis, these infants developed serious complications and eventually died. Prior research indicated that 36.0% of pediatric patients experienced severe complications (23); however, in our study, the incidence was notably higher at 66.67%. It is important to highlight that systematic complications associated with IEIs in pediatric patients are prevalent and multifaceted. Pediatricians are made aware of this concern to facilitate the identification of T. marneffei infections and to prevent mortality.
In the present study, all these children were diagnosed with IEIs, and as a result, they exhibited abnormal immune parameters at the time of diagnosis, to varying degrees, including decreased levels of IgG and increased levels of IgE in peripheral blood. However, only in five cases did the number of peripheral blood lymphocytes significantly decreased. Previous studies have suggested that a reduction in the number of T lymphocytes or cellular immunity is probably the most important predisposing factor for T. marneffei infection in HIV-infected patients (9, 21, 24). Unlike HIV-infected patients, the common immunological findings in IEI children with T. marneffei infections are abnormal immunoglobulin changes. Meanwhile, reduced NK cell counts were identified in most patients. NK cells are the prototype innate lymphoid cells endowed with potent cytolytic functions that provide host defense against microbial infections (25). Previous research has indicated that NK cells are frequently found in HIV-negative T. marneffei-infected patients (20, 26). NK cells might play an important role in defense against T. marneffei. Further research is required to explore the mechanisms by which NK cells respond to T. marneffei infections.
After encountering T. marneffei, the host depends on both innate and acquired immune responses to eradicate the microorganism and combat infection. Multiple studies have shown that depletions of CD4 T lymphocytes is closely associated with an increased risk of T. marneffei infections (9, 27). Immune deficiencies involving cellular-mediated immune responses and CD4 lymphopenia have been documented to be associated with T. marneffei infection, thus increasing susceptibility to the infection (14, 27, 28). CD4 T-cell-mediated immunity, mainly Th1 and Th17 responses, is essential for protection against dimorphic fungi. In the gene interaction network of the cohort, IL2RG was the capital gene for typical X-SCID. ADA, a purine salvage pathway deficiency, results in a buildup of toxic metabolites, causing death in rapidly dividing cells, especially lymphocytes. The most complete form of ADA also leads to SCID (29). In this cohort, four patients were diagnosed with SCID, including three cases of X-SCID and one case of ADA deficiency. Among them, two infants of the three recorded fatalities were attributed to X-SCID resulting from mutations in the IL2RG gene, while the remaining case was associated with ADA deficiency, which is also classified as SCID. Only one X-SCID patient survived after antifungal therapy. Therefore, T. marneffei infections can be lethal in individuals with SCID.
The low proportions of circulating Th17 cells result from impaired pro-Th17 cytokine signaling or production (e.g., STAT3-HIES, which impairs signaling downstream from IL-6, IL-23, and IL-21, in particular) (30); an increase in signaling downstream from cytokines that inhibit Th17 cell differentiation (e.g., STAT1 GOF, which increases cellular responses to IFNs and IL-27, both of which inhibit Th17 cell differentiation) (31); and the impaired production of pro-Th17 cytokines by phagocytes upon fungal recognition (e.g., CARD9 deficiency) (32). Therefore, STAT3-HIES, STAT1 GOF, and CARD9 deficiency had varying degrees of impact on the induction of Th17. It was indeed found that patients with these IEIs, leading to increased susceptibility to T. marneffei infections in the cohort, exhibited such an effect. An analysis of the molecular and cellular basis of T. marneffei infections in these IEIs has suggested a possible role of Th17-mediated immunity in protection against T. marneffei infections.
The study still has some limitations that should be considered. This is a multicenter retrospective analysis, and 18 cases of IEIs were confirmed by gene sequencing from five hospitals over the past 8 years. Some HIV-negative children with T. marneffei did not receive genetic tests, and hence the proportion of such cases with underlying IEIs is unknown. In the retrospective study, a total of 11 novel variants were identified in nine patients. Relevant functional testing will be performed in the future to verify the potential mechanisms of these novel variants. Nevertheless, this study may provide a valuable reference for underlying IEIs of T. marneffei infection in HIV-negative children. Additionally, we will continue to focus on T. marneffei infections in pediatric populations and pursue investigations into the pathogenic mechanisms associated with T. marneffei infection.
T. marneffei infections in children with IEIs often involve severe systemic complications, necessitating thorough and careful observation by clinicians for early identification. Significant immunoglobulin abnormalities were observed in the peripheral blood of these children with severe T. marneffei infections. The study of IEIs underlying T. marneffei infections has deepened our understanding of the condition.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethical approval has been obtained from the National Key Research and Development Program of China (2021YFC2701801, 2021YFC2701803, 2021YFC2701805). All patients provided written informed consent for the use of their clinical and laboratory data from their medical reports.
HF: Formal analysis, Investigation, Writing – original draft, Methodology, Resources. ZY: Formal analysis, Methodology, Resources, Writing – original draft. YW: Data curation, Funding acquisition, Investigation, Resources, Writing – review & editing. XLL: Methodology, Resources, Writing – review & editing. TL: Data curation, Supervision, Writing – review & editing. XYL: Data curation, Supervision, Writing – review & editing. GL: Data curation, Funding acquisition, Supervision, Writing – review & editing. LMH: Investigation, Methodology, Resources, Writing – review & editing. GPL: Conceptualization, Funding acquisition, Project administration, Validation, Writing – review & editing. LH: Conceptualization, Project administration, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Key Research and Development Program of China (No. 2021YFC2701801, 2021YFC2701803, and 2021YFC2701805), the National Natural Science Foundation of China (No. 82370015), and the Sanming Project of Medicine in Shenzhen (No. SZSM202211034).
We would like to thank all the staff and patients for their contributions to our study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1492000/full#supplementary-material
1. Fang J, Chen R, Liu D. Talaromyces marneffei can capture CD86 proteins of macrophages. vitro Infect Drug Resist. (2022) 15:6801–10. doi: 10.2147/IDR.S389612
2. Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. (2011) 24:247–80. doi: 10.1128/CMR.00053-10
3. Chan YF, Chow TC. Ultrastructural observations on Penicillium marneffei in natural human infection. Ultrastruct Pathol. (1990) 14:439–52. doi: 10.3109/01913129009007223
4. Capponi M, Segretain G, Sureau P. Penicillosis from rhizomys sinensis. Bull Soc Pathol Exot Filiales. (1956) 49:418–21.
5. DiSalvo AF, Fickling AM, Ajello L. Infection caused by Penicillium marneffei: description of first natural infection in man. Am J Clin Pathol. (1973) 60:259–63. doi: 10.1093/ajcp/60.2.259
6. Limper AH, Adenis A, Le T, Harrison TS. Fungal infections in HIV/AIDS. Lancet Infect Dis. (2017) 17:e334–e43. doi: 10.1016/S1473-3099(17)30303-1
7. Wang F, Han R, Chen S. An overlooked and underrated endemic mycosis-talaromycosis and the pathogenic fungus talaromyces marneffei. Clin Microbiol Rev. (2023) 36:e0005122. doi: 10.1128/cmr.00051-22
8. Chan JF, Lau SK, Yuen KY, Woo PC. Talaromyces (Penicillium) marneffei infection in non-HIV-infected patients. Emerg Microbes Infect. (2016) 5:e19. doi: 10.1038/emi.2016.18
9. Guo J, Li BK, Li TM, Wei FL, Fu YJ, Zheng YQ, et al. Characteristics and prognosis of talaromyces marneffei infection in non-HIV-infected children in southern China. Mycopathologia. (2019) 184:735–45. doi: 10.1007/s11046-019-00373-4
10. He L, Mei X, Lu S, Ma J, Hu Y, Mo D, et al. Talaromyces marneffei infection in non-HIV-infected patients in mainland China. Mycoses. (2021) 64:1170–6. doi: 10.1111/myc.13295
11. Pongpom M, Vanittanakom P, Nimmanee P, Cooper CR Jr., Vanittanakom N. Adaptation to macrophage killing by Talaromyces marneffei. Future Sci OA. (2017) 3:FSO215. doi: 10.4155/fsoa-2017-0032
12. Fan H, Huang L, Jin Y, Chen C, Lu G, Zhang D, et al. Study ofPenicillium marneffeiInfection in Pediatric Patients Without Human Immunodeficiency Virus Infection in China. Pediatr Allergy Immunology Pulmonology. (2017) 30:53–9. doi: 10.1089/ped.2016.0722
13. Wang L, Luo Y, Li X, Li Y, Xia Y, He T, et al. Talaromyces marneffei infections in 8 chinese children with inborn errors of immunity. Mycopathologia. (2022) 187:455–67. doi: 10.1007/s11046-022-00659-0
14. Zeng Q, Jin Y, Yin G, Yang D, Li W, Shi T, et al. Peripheral immune profile of children with Talaromyces marneffei infections: a retrospective analysis of 21 cases. BMC Infect Dis. (2021) 21:287. doi: 10.1186/s12879-021-05978-z
15. Li Z, Yang J, Qiu Y, Yang F, Tang M, Li S, et al. Disseminated talaromyces marneffei infection with STAT3-hyper-igE syndrome: A case series and literature review. Open Forum Infect Dis. (2023) 10:ofac614. doi: 10.1093/ofid/ofac614
16. Tangye SG, Al-Herz W, Bousfiha A, Cunningham-Rundles C, Franco JL, Holland SM, et al. Human inborn errors of immunity: 2022 update on the classification from the international union of immunological societies expert committee. J Clin Immunol. (2022) 42:1473–507. doi: 10.1007/s10875-022-01289-3
17. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. (2015) 17:405–24. doi: 10.1038/gim.2015.30
18. Grimbacher B, Schaffer AA, Holland SM, Davis J, Gallin JI, Malech HL, et al. Genetic linkage of hyper-IgE syndrome to chromosome 4. Am J Hum Genet. (1999) 65:735–44. doi: 10.1086/302547
19. Hu Y, Zhang J, Li X, Yang Y, Zhang Y, Ma J, et al. Penicillium marneffei infection: an emerging disease in mainland China. Mycopathologia. (2013) 175:57–67. doi: 10.1007/s11046-012-9577-0
20. Lee PP, Lao-Araya M, Yang J, Chan KW, Ma H, Pei LC, et al. Application of flow cytometry in the diagnostics pipeline of primary immunodeficiencies underlying disseminated talaromyces marneffei infection in HIV-negative children. Front Immunol. (2019) 10:2189. doi: 10.3389/fimmu.2019.02189
21. Xue X, Zou J, Fang W, Liu X, Chen M, Arastehfar A, et al. Characteristics and prognosis of talaromyces marneffei infection in HIV-positive children in southern China. Mycopathologia. (2022) 187:169–80. doi: 10.1007/s11046-021-00614-5
22. Yang Q, Wu Y, Li X, Bao Y, Wang W, Zheng Y. Talaromyces marneffei infection and complicate manifestation of respiratory system in HIV-negative children. BMC Pulm Med. (2023) 23:100. doi: 10.1186/s12890-023-02390-y
23. Xing S, Zhang Z, Liu C, Zhang W, Zhang Z, Tang X, et al. Characteristics of endemic mycoses talaromyces marneffei infection associated with inborn errors of immunity. J Clin Immunol. (2024) 45:17. doi: 10.1007/s10875-024-01798-3
24. Ying RS, Le T, Cai WP, Li YR, Luo CB, Cao Y, et al. Clinical epidemiology and outcome of HIV-associated talaromycosis in Guangdong, China, during 2011-2017. HIV Med. (2020) 21:729–38. doi: 10.1111/hiv.13024
25. Morvan MG, Lanier LL. NK cells and cancer: you can teach innate cells new tricks. Nat Rev Cancer. (2016) 16:7–19. doi: 10.1038/nrc.2015.5
26. Hu F, Liu S, Liu Y, Li X, Pang R, Wang F. The decreased number and function of lymphocytes is associated with Penicillium marneffei infection in HIV-negative patients. J Microbiol Immunol Infect. (2021) 54:457–65. doi: 10.1016/j.jmii.2020.02.007
27. Lee PP, Chan KW, Lee TL, Ho MH, Chen XY, Li CH, et al. Penicilliosis in children without HIV infection–are they immunodeficient? Clin Infect Dis. (2012) 54:e8–e19. doi: 10.1093/cid/cir754
28. Han XJ, Su DH, Yi JY, Zou YW, Shi YL. A literature review of blood-disseminated P. marneffei infection and a case study of this infection in an HIV-negative child with comorbid eosinophilia. Mycopathologia. (2019) 184:129–39. doi: 10.1007/s11046-018-0255-8
29. Secord E, Hartog NL. Review of treatment for adenosine deaminase deficiency (ADA) severe combined immunodeficiency (SCID). Ther Clin Risk Manage. (2022) 18:939–44. doi: 10.2147/TCRM.S350762
30. de Beaucoudrey L, Puel A, Filipe-Santos O, Cobat A, Ghandil P, Chrabieh M, et al. Mutations in STAT3 and IL12RB1 impair the development of human IL-17-producing T cells. J Exp Med. (2008) 205:1543–50. doi: 10.1084/jem.20080321
31. Liu L, Okada S, Kong X-F, Kreins AY, Cypowyj S, Abhyankar A, et al. Gain-of-function human STAT1 mutations impair IL-17 immunity and underlie chronic mucocutaneous candidiasis. J Exp Med. (2011) 208:1635–48. doi: 10.1084/jem.20110958
32. Glocker E-O, Hennigs A, Nabavi M, Schäffer AA, Woellner C, Salzer U, et al. A homozygous CARD9 mutation in a family with susceptibility to fungal infections. New Engl J Med. (2009) 361:1727–35. doi: 10.1056/NEJMoa0810719
33. Xiang Q, Zhang L, Liu X, Wang S, Wang T, Xiao M, et al. Autosomal dominant hyper IgE syndrome from a single centre in Chongqing, China (2009-2018). Scand J Immunol. (2020) 91:e12885. doi: 10.1111/sji.12885
34. Zhang LY, Tian W, Shu L, Jiang LP, Zhan YZ, Liu W, et al. Clinical features, STAT3 gene mutations and Th17 cell analysis in nine children with hyper-IgE syndrome in mainland China. Scand J Immunol. (2013) 78:258–65. doi: 10.1111/sji.12063
35. Solimando AG, Desantis V, Palumbo C, Marasco C, Pappagallo F, Montagnani M, et al. STAT1 overexpression triggers aplastic anemia: a pilot study unravelling novel pathogenetic insights in bone marrow failure. Clin Exp Med. (2023) 23:2687–94. doi: 10.1007/s10238-023-01017-0
36. Sharfe N, Nahum A, Newell A, Dadi H, Ngan B, Pereira SL, et al. Fatal combined immunodeficiency associated with heterozygous mutation in STAT1. J Allergy Clin Immunol. (2014) 133:807–17. doi: 10.1016/j.jaci.2013.09.032
37. Ripen AM, Chear CT, Baharin MF, Nallusamy R, Chan KC, Kassim A, et al. A single-center pilot study in Malaysia on the clinical utility of whole-exome sequencing for inborn errors of immunity. Clin Exp Immunol. (2021) 206:119–28. doi: 10.1111/cei.13626
38. Scott O, Lindsay K, Erwood S, Mollica A, Roifman CM, Cohn RD, et al. STAT1 gain-of-function heterozygous cell models reveal diverse interferon-signature gene transcriptional responses. NPJ Genom Med. (2021) 6:34. doi: 10.1038/s41525-021-00196-7
39. Leiding JW, Okada S, Hagin D, Abinun M, Shcherbina A, Balashov DN, et al. Hematopoietic stem cell transplantation in patients with gain-of-function signal transducer and activator of transcription 1 mutations. J Allergy Clin Immunol. (2018) 141:704–17 e5. doi: 10.1016/j.jaci.2017.03.049
40. Liu L, Sun B, Ying W, Liu D, Wang Y, Sun J, et al. Rapid diagnosis of Talaromyces marneffei infection by metagenomic next-generation sequencing technology in a Chinese cohort of inborn errors of immunity. Front Cell Infect Microbiol. (2022) 12:987692. doi: 10.3389/fcimb.2022.987692
41. Pan M, Qiu Y, Zeng W, Tang S, Wei X, Zhang J. Disseminated Talaromyces marneffei infection presenting as multiple intestinal perforations and diffuse hepatic granulomatous inflammation in an infant with STAT3 mutation: a case report. BMC Infect Dis. (2020) 20:394. doi: 10.1186/s12879-020-05113-4
42. Hirbod-Mobarakeh A, Aghamohammadi A, Rezaei N. Immunoglobulin class switch recombination deficiency type 1 or CD40 ligand deficiency: from bedside to bench and back again. Expert Rev Clin Immunol. (2014) 10:91–105. doi: 10.1586/1744666X.2014.864554
43. Lee WI, Torgerson TR, Schumacher MJ, Yel L, Zhu Q, Ochs HD. Molecular analysis of a large cohort of patients with the hyper immunoglobulin M (IgM) syndrome. Blood. (2005) 105:1881–90. doi: 10.1182/blood-2003-12-4420
44. Khanolkar A, Wilks JD, Jennings LJ, Davies JL, Zollett JA, Lott LL, et al. Signaling impairments in maternal T cells engrafted in an infant with a novel IL-2 receptor gamma mutation. J Allergy Clin Immunol. (2015) 135:1093–6 e8. doi: 10.1016/j.jaci.2015.02.012
45. Bazan-Socha S, Gradzikiewicz A, Celinska-Lowenhoff M, Matyja-Bednarczyk A, Maciolek A, Babol-Pokora K. Chronic mucocutaneous candidiasis, pancytopenia, and systemic mycosis in a patient with STAT1 gene mutation ineffectively treated with ruxolitinib. Cent Eur J Immunol. (2022) 47:92–4. doi: 10.5114/ceji.2022.114884
46. Guisado Hernandez P, Blanco Lobo P, VilLaoslada I, de Felipe B, Lucena JM, Martin Gutierrez G, et al. SARS-CoV-2 infection in a pediatrics STAT1 GOF patient under Ruxolitinib therapy-a matter of balance? J Clin Immunol. (2021) 41:1502–6. doi: 10.1007/s10875-021-01081-9
Keywords: Talaromyces marneffei, inborn errors of immunity, immune status, gene mutation, children
Citation: Fan H, Yang Z, Wu Y, Lu X, Li T, Lu X, Lu G, He L, Lu G and Huang L (2025) Human inborn errors of immunity underlying Talaromyces marneffei infections: a multicenter, retrospective cohort study. Front. Immunol. 16:1492000. doi: 10.3389/fimmu.2025.1492000
Received: 06 September 2024; Accepted: 07 January 2025;
Published: 22 January 2025.
Edited by:
Qiao Liu, Children’s Hospital of Chongqing Medical University, ChinaReviewed by:
Saul Oswaldo Lugo Reyes, National Institute of Pediatrics, MexicoCopyright © 2025 Fan, Yang, Wu, Lu, Li, Lu, Lu, He, Lu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guoping Lu, MTM3ODg5MDQxNTBAMTYzLmNvbQ==; Li Huang, aHVhbmdsaTc1MjVAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.