 Leandro Junqueira Moragas1†Laíza Vianna Arruda1,2†Lucca de Lima Siqueira Oliveira1
Leandro Junqueira Moragas1†Laíza Vianna Arruda1,2†Lucca de Lima Siqueira Oliveira1 Felipe de Andrade Vieira Alves1,2
Felipe de Andrade Vieira Alves1,2 Natália Gedeão Salomão1,3Jemima Fuentes Ribeiro da Silva2Carlos Alberto Basílio-de-Oliveira4
Natália Gedeão Salomão1,3Jemima Fuentes Ribeiro da Silva2Carlos Alberto Basílio-de-Oliveira4 Rodrigo Panno Basílio-de-Oliveira4
Rodrigo Panno Basílio-de-Oliveira4 Ronaldo Mohana-Borges5Caio Gonçalves Azevedo2Gabriela Xavier de Oliveira2
Ronaldo Mohana-Borges5Caio Gonçalves Azevedo2Gabriela Xavier de Oliveira2 Jorge José de Carvalho2
Jorge José de Carvalho2 Fernando Colonna Rosman4,6Marciano Viana Paes1‡
Fernando Colonna Rosman4,6Marciano Viana Paes1‡ Kíssila Rabelo1,2*
Kíssila Rabelo1,2*- 1Laboratório Interdisciplinar de Pesquisas Médicas, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz, Rio de Janeiro, Brazil
- 2Laboratório de Ultraestrutura e Biologia Tecidual, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil
- 3Laboratório das Interações Vírus-Hospedeiros, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz, Rio de Janeiro, Brazil
- 4Departamento de Patologia, Faculdade de Medicina, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
- 5Laboratório de Genômica Estrutural, Instituto de Biofísica Carlos Chagas Filho, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
- 6Serviço de Anatomia Patológica, Hospital Municipal Jesus, Rio de Janeiro, Brazil
Introduction: The dengue virus (DENV) is the etiological agent that causes dengue fever illness, an arbovirus with a major endemic potential that has become increasingly prevalent in Brazil and has already been associated with fatal cases in children. DENV has tropism for several organs, including lungs causing pulmonary complications. The aim of this article was to evaluate the inflammatory and histopathological profile of the lung tissue of three fatal cases of children infected with DENV, which represents a group more susceptible to fatality due to its incomplete development.
Methods: Histopathological analysis was carried out using Hematoxylin and Eosin staining and special stains. While the characterization of the inflammatory response and cellular expression was done by marking the viral protein, macrophages, lymphocytes and pro-inflammatory cytokines.
Results and discussion: The results confirm that vascular dysfunctions such as hemorrhage, vascular congestion and edema associated with a mononuclear infiltrate were observed in all three cases. In addition, the presence of viral replication and increased expression of inflammatory markers were also observed. Such findings contribute to the study and description of dengue, especially its effects on lung tissue.
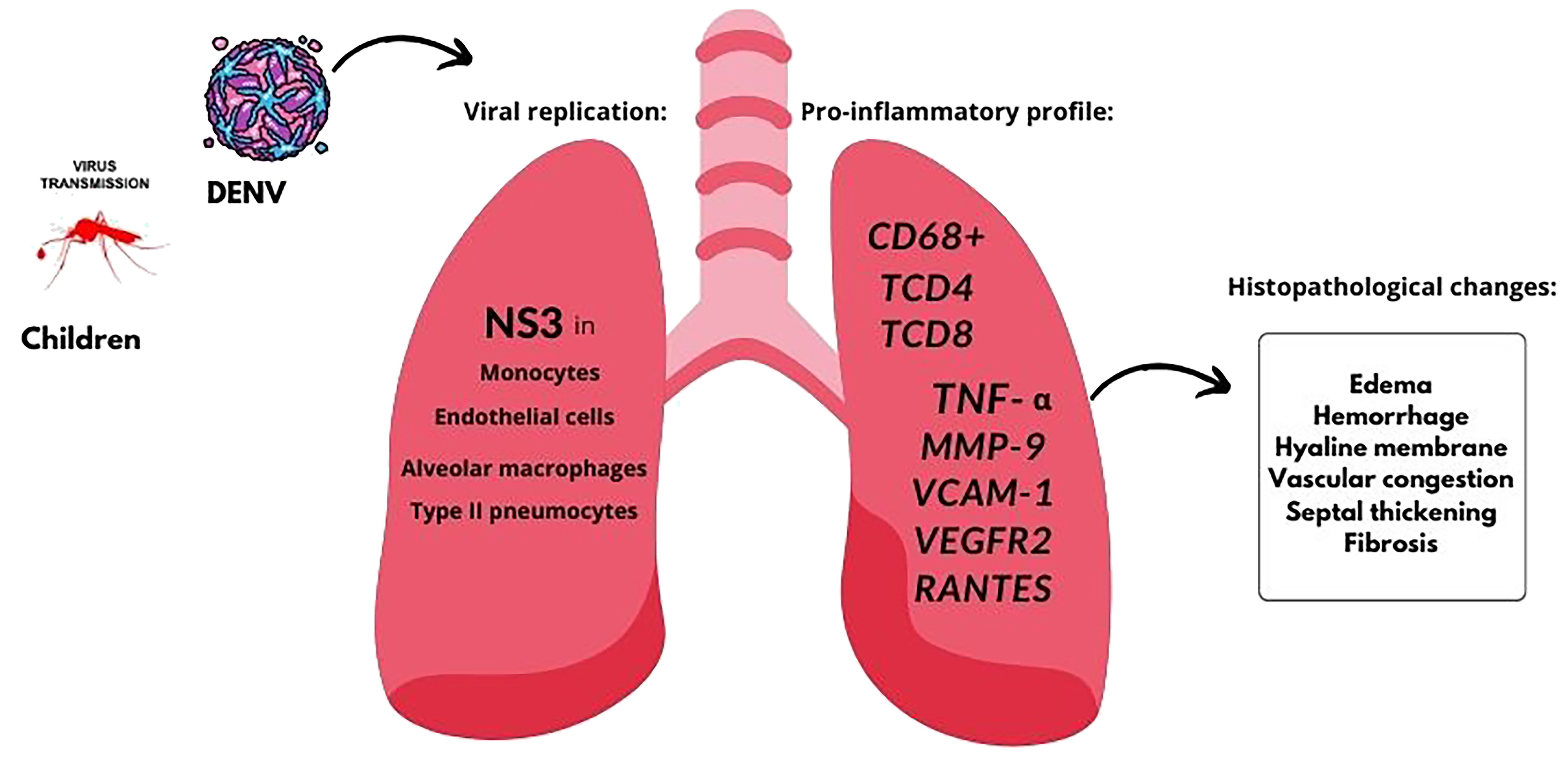
Graphical Abstract.
1 Introduction
Dengue fever (DF) is an arboviral disease that represents a global public health concern, especially in tropical and subtropical regions. Dengue virus (DENV) belongs to the Flaviviridae family transmitted mainly by mosquitoes of the Aedes genus (1). DF is endemic in several countries in Africa, Southeast Asia, the Western Pacific, and America (2, 3) and, during the last year, more than 5 million cases were reported globally (4). Brazil is one of the most affected countries, with a significant increase in the incidence of DF, reporting the highest number of cases (over 2.9 million) in America during the year of 2023 (4, 5). By June 2024, more than 6 million cases (6,121,980 cases) and around 4 thousand deaths from dengue fever had been registered in Brazil, indicating an increase in cases that constitutes a hyperendemic and emphasizes the importance of studying this disease in the country (6).
DENV comprises four distinct serotypes (DENV-1, DENV-2, DENV-3 and DENV-4), which are genetically related (7) and present similar clinical results – except in cases of secondary infection with a different serotype (8, 9). DENV infection commonly consists of a mild form, including symptoms such as arthralgia, headache, vomiting, myalgia, and skin rash (10). However, DF can progress to severe forms including dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) (11). Some studies have pointed out that the most serious conditions of DENV infection present hemorrhagic symptoms, severe plasma leakage and severe involvement of multiple organs (12–14), which is usually present in children aged less than 15 years (15, 16). Therefore, mortality is directly associated with the complications of the disease, which leads to the impairment of several organs (7, 17).
Multiple organs can be affected by DENV infection, and several studies have already identified impairment of the central nervous system, skeletal muscle, liver, heart, and lungs (18–26). Furthermore, histopathological changes have been also observed in the spleen, kidney, pancreas and placenta (22, 24, 27–30). Lung involvement during DENV infection has been documented in several studies and is generally correlated with severe forms of the disease (26, 31–34). Thus, extensive lung involvement, especially associated with pulmonary hemorrhage, is a terminal event and is closely associated with uncontrolled infection and DSS (34).
Due to their immature hemodynamic system, children and specifically infants tend to develop severe dengue fever (35, 36) – with vascular leakage and shock being more frequent and severe in children than in adults (37, 38). Systemic vascular leak syndrome typically manifests itself at the time of defervescence and is characterized by progressive leukopenia associated with thrombocytopenia, hemorrhagic manifestations, pleural effusion, and ascites (36). To detect a serious change in the disease, the identification of different plasma extravasation markers, such as RANTES, VEGFR-2 and VCAM-1, is often used (27, 39, 40). This is important, because a few years ago there was an increase in the number of serious cases in the younger age group, highlighting the importance of investigating the pathophysiology of dengue, especially in this group (16, 36).
In this context, the present work aimed to investigate the histopathological aspects of lung tissues from three fatal cases of dengue in children that occurred between 2008 and 2012, as well as covering the inflammatory immune profile. It is known that the combination of inflammatory markers and vascular permeability in the febrile phase of dengue is associated with the development of more severe outcomes (40). Therefore, we focused on investigating the presence of immune cells with a chronic profile, pro-inflammatory cytokines such as TNF-a and vascular permeability markers in lung. These patients developed severe dengue fever, which critically affected other organs, besides the lungs, including the liver, as previously described by our group (41). Therefore, histopathological, and immunohistochemical analysis of lung tissue damage can help to elucidate the immunological mechanisms involved in the pathogenesis of dengue in the lung and how this contributed to the outcome of these patients.
2 Methods
2.1 Ethical considerations
All procedures performed during this study were approved by the Ethics Committee of the Oswaldo Cruz Foundation/FIOCRUZ (CAEE: 47525115.3.0000.5248).
2.2 Clinical history of fatal cases and controls
Lung tissue samples came from three children who died from DENV infection, during the outbreak that occurred in Rio de Janeiro, between 2008 and 2012. The diagnosis of dengue fever was confirmed in all patients, due to the presence of anti-DENV IgM antibodies or detection of NS1 antigen by immunochromatography. The clinical history of all patients and the respective conditions of each case are described in Moragas, L. J. et al., 2023 (41). The negative controls of lung samples were obtained from three fatalities ranging from 8 to 13 years old presenting no signs of infectious diseases or lung disorder.
2.3 Histopathological analysis
The lung tissue fragments from necropsies were fixed in 10% formaldehyde, pH 7.2, processed and blocked-in paraffin resin. 5 µm thick sections were made using a microtome (Leica, Germany) and mounted on glass slides. Before staining, slides were deparaffinized in three xylene baths and rehydrated with decreasing concentrations of ethanol (100 to 70%) and water. Then, the sections were subjected to standard and special staining with Hematoxylin and Eosin (H.E.), Periodic Acid-Schiff (PAS), PicroSirius Red and Masson’s trichrome, prepared for viewing under a light microscope (Olympus, Tokyo, Japan). Photomicrographs were captured using Image-Pro Plus version 7 software (Media Cybernetics).
2.4 Immunohistochemistry procedures
For detection of NS3 protein as well as characterization of cell populations, cytokines and inflammatory mediators by immunohistochemistry, sections were treated as described in a previous work (33). Sections were then incubated overnight at 4˚C with the following primary antibodies: anti-NS3 (produced in house, expressed in Escherichia coli, purified and inoculated in BALB/c mice; dilution 1:100), rabbit anti-human CD4 monoclonal antibody clone SP35 (Spring Bioscience, CA, USA; dilution 1:100), mouse anti-human CD8 monoclonal antibody clone C8/144B (Dako, CA, USA; dilution 1:200), mouse anti-human CD68 monoclonal antibody clone EBM11 (Dako, CA, USA; dilution 1:200), rabbit anti-human TNF-α polyclonal antibody clone ab6671 (Abcam, MA, USA; dilution 1:200), rabbit anti-human RANTES monoclonal antibody clone ab189841 (Abcam, MA, USA; dilution 1:200), rabbit anti-human VEGFR-2 monoclonal antibody clone SP123 (Spring Bioscience, CA, USA; dilution 1:100), rabbit anti-human VCAM-1 monoclonal antibody clone ab134047 (Abcam, MA, USA; dilution 1:100), mouse anti-human MMP-9 monoclonal antibody clone sc-21733 (Santa Cruz Biotechnology, TX, USA; dilution 1:100). On the second day, sections were washed three times and incubated with secondary antibody (REVEAL complement, Spring Bioscience, CA, USA) for 10 min and with rabbit anti-mouse IgG-HRP conjugate (REVEAL polyvalent HRP, Spring Bioscience, CA, USA) for 15 min at room temperature; followed by reveal of the reaction with the substrate for peroxidase diaminobenzidine (Dako, CA, USA). Counterstaining was performed with Harry’s hematoxylin (Sigma, MO, USA) and then, sections were prepared for visualization under a light microscope (Olympus, Tokyo, Japan).
2.5 Damage quantification and statistical analysis
Quantification of lung lesions were performed by a semi quantitative analysis in sections stained with H.E. For each of the parameters used in the quantification of damages (septal thickening, hyaline membrane formation, degree of edema and hemorrhage, in addition to the presence of inflammatory infiltrate), a numerical scale ranging from 0 to 4 according to the severity and the extent of damage was assigned (0 = none, 1 = mild, 2 = moderate, 3 = severe and focally, 4 = severe and diffuse).The values were measured covering 20 randomly acquired fields at 1000x magnification, visualized by light microscopy.
Data were analyzed with GraphPad Prism software version 8.0 (La Jolla, CA, USA) using non-parametric statistical tests. Significant statistical differences between the analyzed groups (controls and cases) were determined using Mann-Whitney test with a threshold of p < 0.05.
3 Results
3.1 Histopathological analysis
The control tissue samples presented a regular structure, with no sign of rupture, edema, hemorrhage or other morphological disorder (Figure 1A). On the other hand, the three cases presented similar histopathological changes: areas of septal thickening and edema associated with a significant mononuclear inflammatory infiltrate (Figures 1B-D) which suggests vascular permeability alteration. Furthermore, it was possible to observe alveolar macrophage hyperplasia (Figures 1B, C). Also, the presence of positive PAS staining revealed the formation of hyaline membrane in areas of the alveolar septum (Figures 1F-H), compared to the control, which showed discrete PAS staining (Figure 1E). Intense staining in alveolar macrophages together with hyperplasia, suggests activation of these cells (Figures 1F-H).
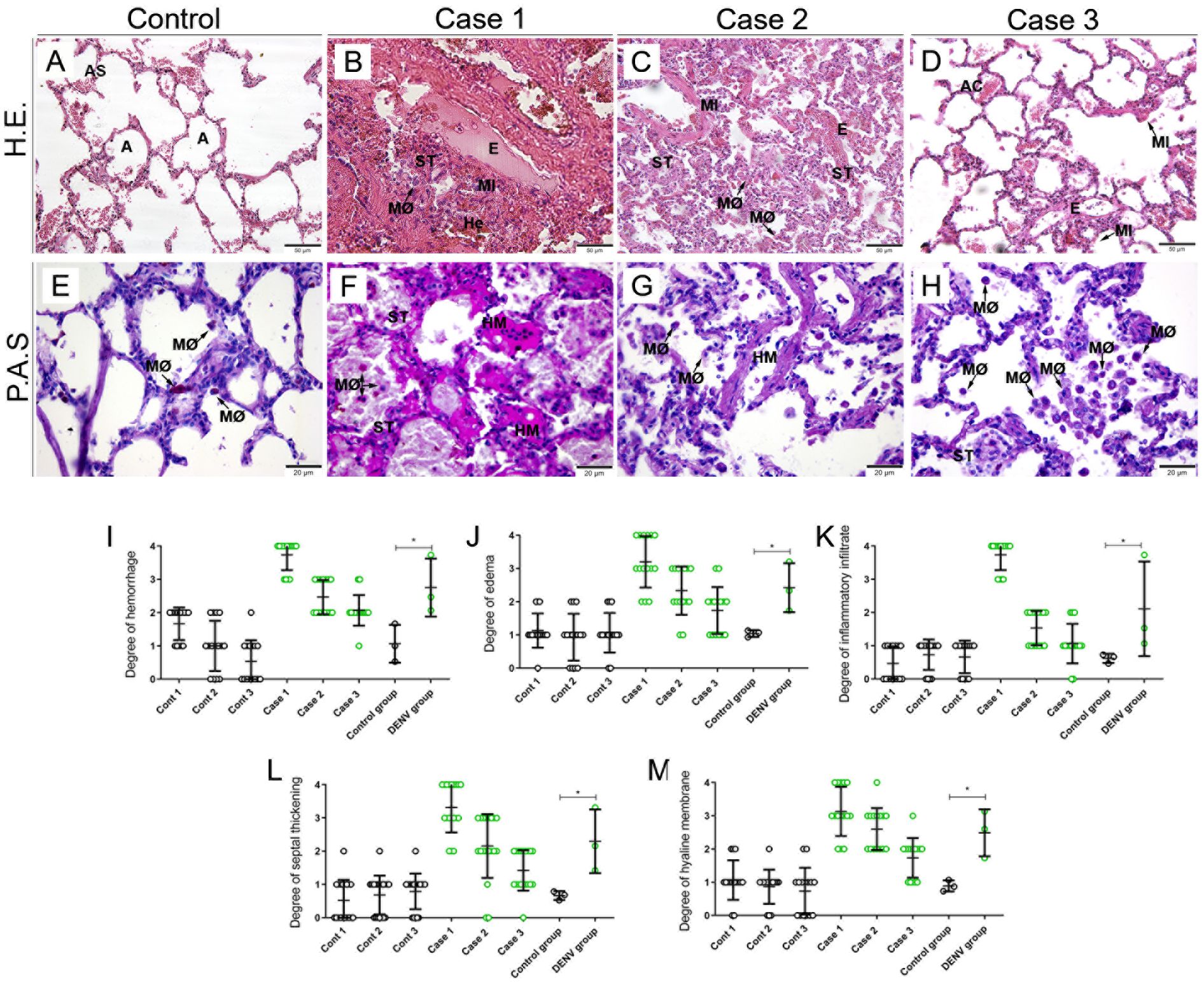
Figure 1. Histopathological aspects of lung tissues from fatal cases of DENV in children and respective controls. (A, E) Lung from non-dengue cases stained with H.E. and PAS, respectively showing preserved alveoli and normal appearance. Lung sections from fatal dengue cases showing alveolar macrophage hyperplasia (B, C), as well as areas of hemorrhage (B), septal thickening (B, C) and edema associated with inflammatory infiltrate (B-D). (F-H). Special PAS staining reveals glycogen deposits in alveolar septa associated with the formation of hyaline membrane, in addition to intense positive staining in alveolar macrophages. (AS) Alveolar Septum; (A) Alveolus; (MØ) Macrophage; (He) Hemorrhage; (E) Edema; (MI) Mononuclear Infiltrate; (ST) Alveolar Thickening; (AC) Alveolar Capillary; (HM) Hyaline Membrane. (I-M) Semiquantitative analysis of changes in the lung tissue of infected and control children. Asterisks indicate significant differences by the statistical test (*p < 0.05). (A-D) Magnification 20x, (E-H) magnification 40x.
Semi quantitative damage analysis was conducted using five distinct parameters: hemorrhage, edema, inflammatory infiltrate, septum thickening and hyaline membrane formation. Unlike the control, which showed no or low impairment, in all cases we observed septum thickening, formation of a hyaline membrane, presence of edema, hemorrhage and inflammatory infiltrate in different degrees (Figures 1I-M). Cases 2 and 3 presented a moderate degree in the five criteria used, while in case 1 we observed a high degree of inflammatory infiltrate and severe tissue involvement in relation to septum thickening, formation of hyaline membrane, presence of edema and hemorrhage (Figure 1I-M).
3.2 Evaluation of fibrosis by collagen deposition and matrix metalloproteinase-9 expression and in lung tissues
To evaluate the presence of fibrosis, we analyzed the deposition of collagen in areas of the lung by staining with Masson’s Trichrome and Picro Sirius Red. Furthermore, we detected metalloproteinase-9 (MMP-9), an enzyme that degrades type IV collagen and is a key modulator of the extracellular matrix and basement membrane. As expected, the control samples showed regular collagen deposition with an absence of MMP9 labeling (Figures 2A, E, I). In infected tissue, staining with Masson’s trichrome and Picro Sirius Red showed an increase in the deposition of collagen fibers around the pulmonary vein and, in regions of the parenchyma of some cases - coinciding with the alveolar septa and bronchi, suggesting areas of pulmonary fibrosis (Figures 2B, C, D, F-H). Furthermore, we detected the presence of MMP-9 in thickened alveolar septa (Figures 2J-L) inside alveolar macrophages, and type II pneumocytes.
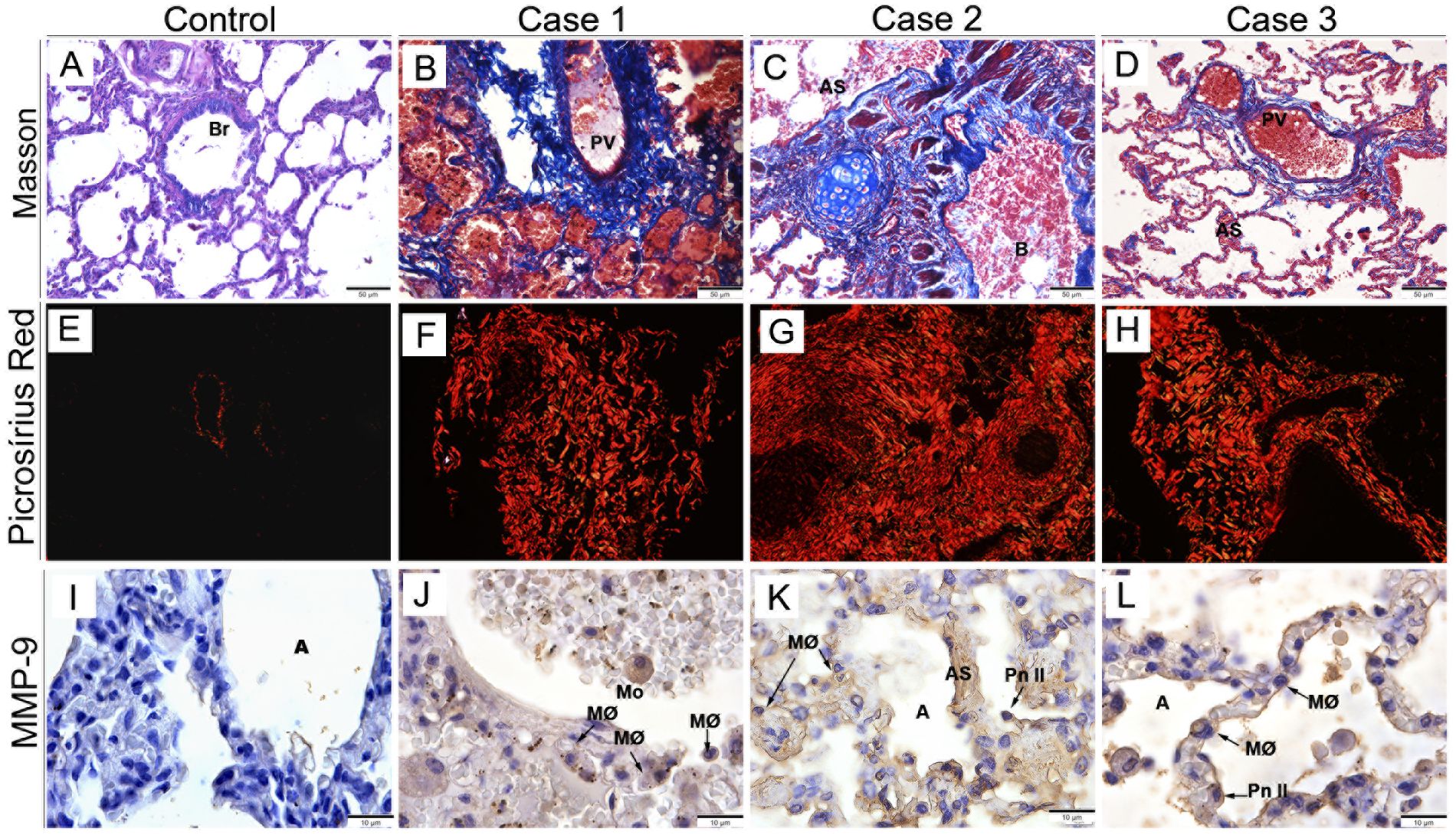
Figure 2. Analysis of collagen deposition in lung tissue and MMP-9 expression. Control case, stained with Masson’s trichrome (A) and Picrosirius red (E), showing a regular distribution of collagen fibers around the bronchiole and pulmonary vein. Infected lung tissue stained with Masson’s trichrome, demonstrating deposition of collagen fibers disseminated throughout the alveolar septa (B, C), around the pulmonary vein (B, D), and bronchiole (C). (F-H) Picro Sirius Red staining showing intense collagen deposition around the pulmonary vein and disseminated throughout the parenchyma. (I) Control lung tissues without MMP-9 expression. Detection of MMP-9 in alveolar macrophages (J-L), type II pneumocytes, and inside alveolar septa (K). (B) Bronchus; (Br) Bronchiole; (Pv) Pulmonary vein; (A) Alveolus; (MØ) Macrophage; (Mo) Monocyte; (AS) Alveolar Septum; (Pn II) Type II Pneumocyte. (A-D) Magnification 20x, (E-H) magnification 40x, (I-L) magnification 10x.
3.3 Detection of viral antigen
To investigate sites of viral replication in the lung tissues of the studied cases, it was performed the detection of the dengue nonstructural 3 (NS3) protein by immunohistochemistry assay. Controls (non-dengue cases) did not react with antibodies targeting NS3 antigen, revealing absence of viral replication in these tissues (Figure 3A). Positive reaction for NS3 antigen was indeed observed in all three dengue cases, mainly in type II pneumocytes (Figures 3B-E) and alveolar macrophages (Figures 3B-D), evidencing viral replication in these cells. The viral antigen was also detected in alveolar capillaries.
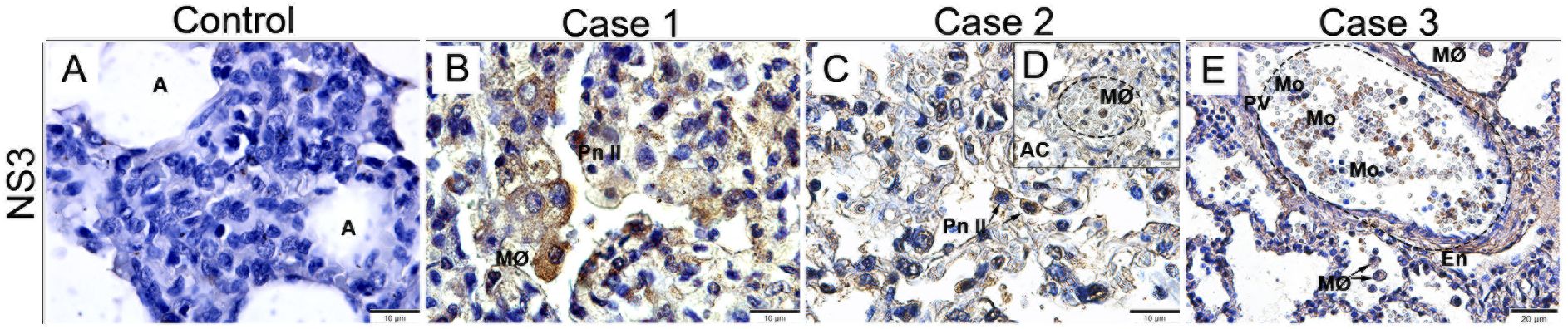
Figure 3. Detection of the NS3 protein antigen in lung tissues from DENV fatal cases of children. (A) Control lung tissue showing no presence of NS3 protein antigen. Detection of NS3 antigen in type II pneumocytes (B, C), macrophages inside the alveolar capillaries (D), and monocytes inside the pulmonary vein (E). (A) Alveolus; (MØ) Macrophages; (Pn II) Type II Pneumocyte; (AC) Alveolar Capillary; (Mo) Monocyte; (PV) Pulmonary vein. (A-D) Magnification 100x, (E) magnification 40.
3.4 Analysis of the lymphocyte profile in infected lung tissues
Areas with infiltrate observed in the lung tissue were characterized by the expression of CD4+ and CD8+ T cells. In both control samples, staining was observed as expected: few or none CD4+ T cells and CD8+ T cells homogeneously dispersed in the lung parenchyma (Figures 4A, E). In general, in all three cases we observe the presence of CD4+ T cells inside the pulmonary vein (Figure 4B) and associated with areas of hemorrhage in the alveoli (Figures 4C, D). Furthermore, we observed an increase in the number of CD8+ T cells, cytotoxic T lymphocytes, in the regions of septal thickening and spread throughout the parenchyma (Figures 4F-H) compared to the control.
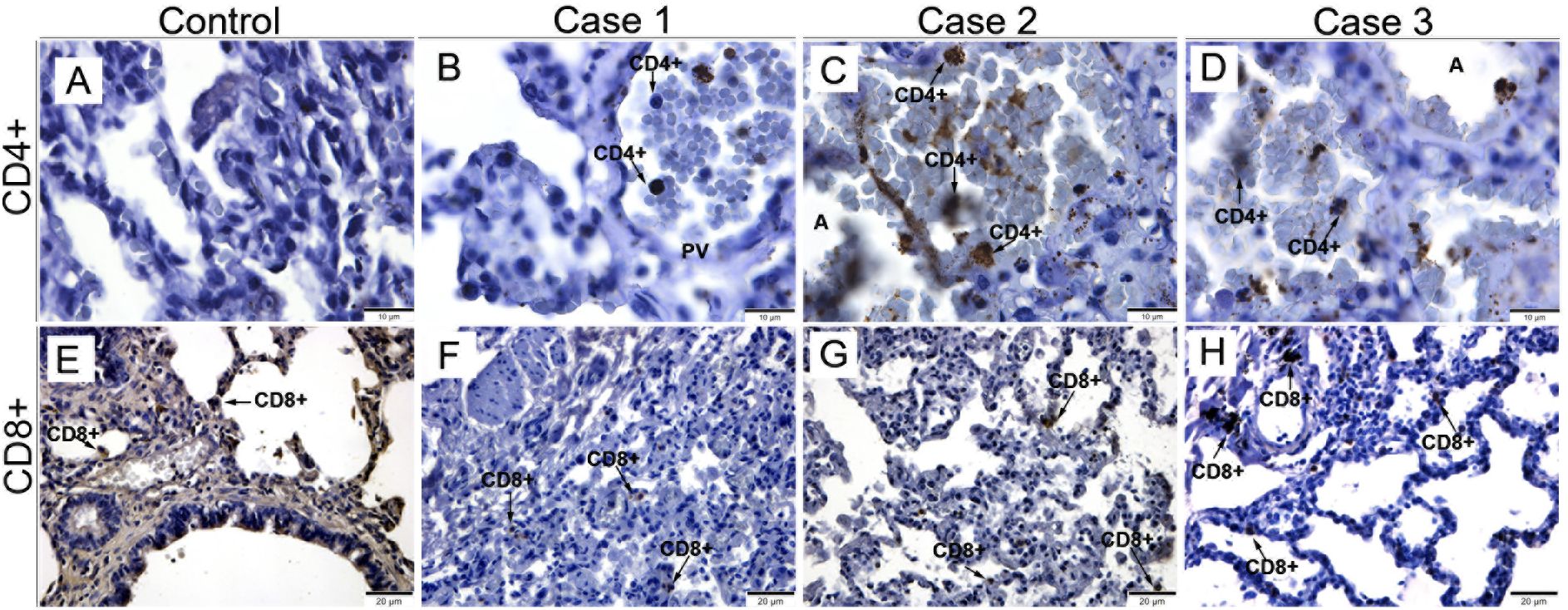
Figure 4. Profile of T lymphocytes in lung tissues from fatal cases of DENV in children. (A, E) Control cases with reduced expression of CD4+ and CD8+ T cells. Infected lung tissues, showing CD4+ T lymphocytes inside the pulmonary vein (B) and in the alveoli (C, D). (F-H) CD8+ cytotoxic T lymphocytes detected in areas of septal thickening. (CD4+) CD4+ T Lymphocytes; (PV) Pulmonary vein; (CD8+) CD8+ T Lymphocytes. (A-D) Magnification 100x, (E-H) magnification 40x.
3.5 Detection of macrophages and pro-inflammatory cytokine
To identify the profile of macrophages and cytokines present in the tissue of infected cases, we detected CD68+ cells and the pro-inflammatory cytokine TNF-α. In the control tissue, we observed the expected labeling of CD68+ cells in discrete areas in the lung alveoli and the absence of TNF-α labeling (Figures 5A, E). In infected tissues, we observed positive staining of CD68+ cells in regions of septal thickening, around the pulmonary vein (Figure 5B), in scattered throughout the lung parenchyma (Figure 5C) and in focal areas of the alveoli (Figure 5D). In addition, we detected the expression of TNF-α in the endothelial cells around the pulmonary vein (Figure 5F), inside monocytes and alveolar macrophages (Figure 5G), as well as in the peribronchiolar mononuclear infiltrate (Figure 5H).
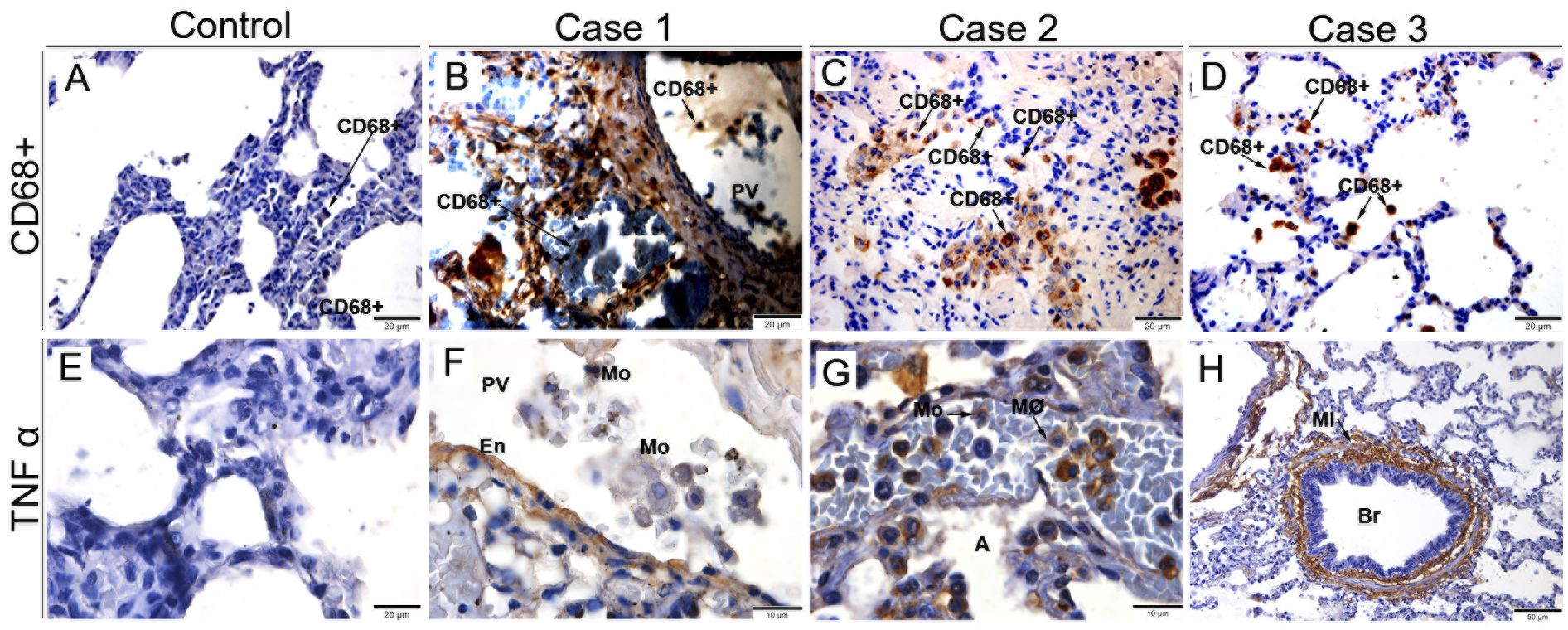
Figure 5. Characterization of macrophages and expression of TNF-α in fatal cases of DENV in children. (A) Control lung tissue with little expression of CD68+ macrophages. (B-D) Infected tissues expressing CD68+ macrophages throughout the lung parenchyma. (E) Control tissue presenting no expression of TNF-α. Expression of TNF-α in pulmonary vein endothelial cells (F), in Monocytes (G), and in the peribronchiolar Mononuclear infiltrate (H). (CD68+) CD68+ Macrophages; (PV) Pulmonary vein; (En) Endothelium; (Mo) Monocyte; (MØ) Macrophages; (MI) Mononuclear infiltrate; (Br) Bronchiole. (A-E) Magnification 40x, (F, G) magnification 100X, (H) magnification 20x.
3.6 Analysis of mediators involved in vascular permeability in lung tissues
The profile of mediators involved in vascular permeability and pro-inflammatory response was characterized mainly by the expression of RANTES, VEGFR-2 and VCAM-1, well-known markers implicated in the pathogenesis and progression of DENV disease. There was little or no detection of any of the mediators in control tissues (Figures 6A, F, J). On the other hand, in the patients’ tissues, we detected positive staining for RANTES inside macrophages, in the endothelial cells of the pulmonary veins (Figures 6B-E). Similarly, VEGFR-2 was detected in alveolar monocytes and macrophages and in pulmonary vein endothelial cells and alveolar capillaries (Figures 6G-I). Furthermore, we observed positive staining for VCAM-1 in circulating macrophages and monocytes, as well as in pulmonary vein endothelial cells (Figures 6K-M).
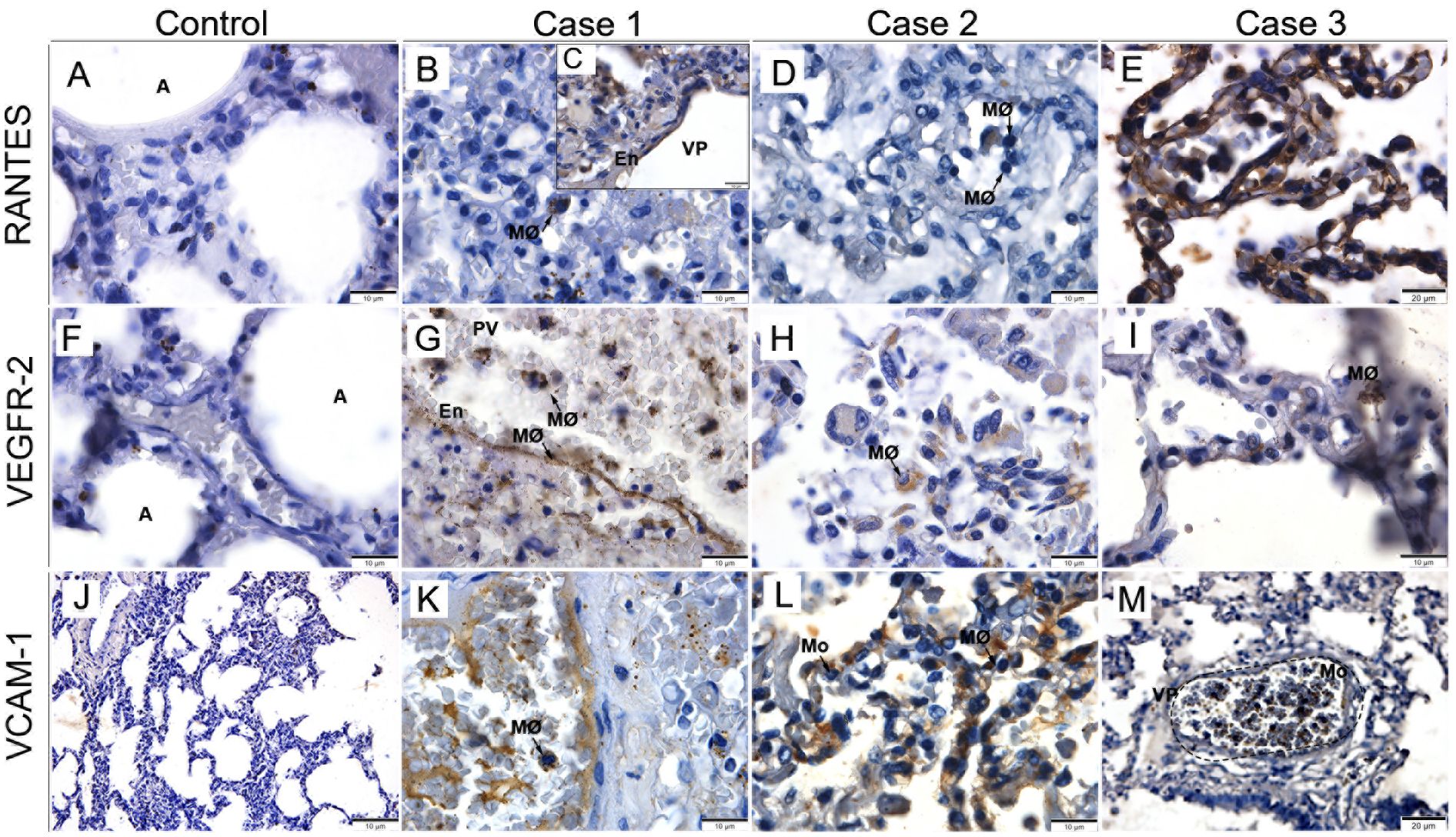
Figure 6. Characterization of vascular permeability in lung tissues from fatal cases of DENV in children. (A, F, J) Control tissues presenting little or no expression of RANTES, VEGFR-2 and VCAM-1. (B-E) Expression of RANTES in macrophages and endothelial cells of the pulmonary vein. (G-I) VEGFR-2 expressed in alveolar macrophages. (K-M) VCAM-1 expressed in circulating macrophages and monocytes. (A) Alveolus; (MØ) Macrophages; (PV) Pulmonary vein; (En) Endothelium; (Mo) Monocyte. (A-D, F-L) Magnification 100x, (E, M) magnification 40x.
4 Discussion
In studies involving human cases of dengue, the involvement of various organs during the course of the disease has been increasingly observed, especially in fatal cases (29, 42–52). However, few studies have targeted children, who have recently shown a high rate of conversion from classical dengue to severe dengue. Therefore, this study focused on this age group.
Regarding lung findings, we observed that areas of hemorrhage, edema, septal thickening and hyaline membrane formation are characteristics of dengue shock, which adds to the severity of fatal outcomes. Previous studies conducted in our group had similar results (29, 49). Additionally, in the present study, we observed hyperplasia of alveolar macrophages and areas with mononuclear infiltrate. Increase in cellularity, presence of mononuclear infiltrate and hyperplasia of alveolar macrophages have been previously reported in adult patients as complications resulting from DENV infection (29, 49).
The NS3 viral antigen was detected inside type II pneumocytes, alveolar macrophages and within the alveolar capillaries. These findings demonstrate that DENV was able to infect these cells and replicate, once NS3 protein participates actively in viral replication. Similar results were found by our group in previous studies with the lungs of adult patients, where NS3 antigen was detected inside alveolar macrophages, type II pneumocytes and endothelial cells (49). NS3 is a common target for observing viral replication, since it is a protease that remains only in the cytosol. It has been studied as a therapeutic target to prevent viral replication and disease progression (50, 51).
Masson’s Trichrome and Picro Sirius Red staining were used for better evidence of collagen fiber and we observed an increase in the expression of these fibers, particularly around the pulmonary vein. We also noted increased expression of these fibers disseminated throughout the parenchyma in some cases, coinciding with the alveolar septa and some bronchi. Previous studies have also observed an increase in collagen fiber expression in the region of the alveolar septa, promoting septal thickening (53). Through PAS staining, we observed positive marking, indicating a high concentration of carbohydrates (glycoproteins), which are normally found in connective tissues, mucus and the basement membrane. It was more evident in the alveolar septa, indicating the presence of a hyaline membrane. High concentrations of hyaline membrane were already reported in patients with severe dengue, suggesting DENV shock (29, 49, 54).
We also identify a greater presence of inflammatory cells (CD8+ T and CD4+ lymphocytes and CD68+ macrophages), mainly in regions of septal thickening, diffuse in the parenchyma and around the pulmonary vein. It is known that increased presence of CD4+ and CD8+ T lymphocytes in the lung is associated with Chronic Obstructive Pulmonary Disease (COPD), as it is believed that CD8+ T lymphocytes cause modifications in the elastic fibers and musculature of the bronchi. The bronchioles can become obstructed by fibrosis and infiltration of macrophages (CD68+) and CD8+ T lymphocytes. It is believed that macrophages and CD8+ T lymphocytes have important role in apoptosis and destruction of epithelial cells in the alveolar wall, releasing TNF-α, perforins and granzymes, in addition to stimulating the production of collagen fibers which induces fibrosis (55).
TNF-α expression was observed in the endothelial cells of the pulmonary vein, in monocytes and alveolar macrophages. Additionally, there was significant marking in a peribronchiolar mononuclear infiltrate. It is known that TNF-α is a cytokine involved in various inflammatory and fibrotic dysfunctions, playing an important role in the impairment of lung function. Anti-TNF-α therapies have shown good effects in controlling chronic pulmonary inflammatory response (56). As one of the main cytokines in the cytokine storm, TNF-a is a marker of disease severity and may be associated with severe infection. Studies with large numbers of patients confirm this association with outcomes in shock syndrome and dengue hemorrhagic fever (57). In addition, TNF-a was observes as one of the most prominent cytokines in the evaluation of immunoclusters in severe dengue in children (58).
There was an increase in the expression of other inflammatory mediators related to increased vascular permeability and cause of shock and deaths in dengue: RANTES, VEGF-R2, and VCAM-1. In our study, we observed higher expression of RANTES inside macrophages and endothelial cells of the pulmonary vein and pulmonary capillaries. RANTES has been described as responsible for the recruitment of T lymphocytes and blood monocytes, leading to an increase in alveolar macrophages and CD8+ T lymphocytes in the pulmonary parenchyma, contributing to the COPD condition (59). VEGFR-2 was detected in the endothelial cells of the pulmonary vein and alveolar capillaries, as well as in monocytes and alveolar macrophages. When bound to VEGF, it promotes the division, proliferation, and migration of endothelial cells, increasing vascular permeability and, consequently, plasma leakage (30, 60). Increased expressions of VCAM-1 were observed in macrophages, circulating monocytes, and endothelial cells of the pulmonary vein. This cytokine promotes the adhesion of lymphocytes, monocytes, eosinophils, and basophils to the vascular endothelium. Studies have found high concentrations of VCAM-1 in fibroblasts, collagen synthesizers (61), which may favor the formation of the hyaline membrane.
This study is one of the few focused on the immunopathogenesis of dengue in children. The most worrying aspect is that dengue cases in children tend to progress to severe dengue. It is not known for certain why children are more susceptible to severe dengue. We believe it may be due to the immaturity of the immune system and an inability to fight DENV, in which the side effects of cytokines and inflammatory mediators are more damaging than the disease itself. The increased presence of CD4+ T cells, CD8+ T cells and CD68+ macrophages indicate an exaggerated inflammatory response, which can culminate in dengue shock syndrome through the triggering of cytokines and inflammatory mediators. Investigating the main cells and inflammatory mediators involved in the pathogenesis of dengue contributes to clarifying the main mechanisms involved during an infection. In this way, we will be able to modulate the immune response, avoiding the deleterious effects of its activation and thus preventing progression to severe dengue and death. With this study, we have further clarified the immunopathogenesis of the disease, evaluating the possible biomarkers of severe dengue in order to identify them in the early stages of the disease and establish the best protocol for treatment.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
All procedures performed during this study were approved by the Ethics Committee of the Oswaldo Cruz Foundation/FIOCRUZ (CAEE: 47525115.3.0000.5248). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
LJ: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. LA: Methodology, Writing – original draft. LS: Investigation, Methodology, Writing – review & editing. FA: Investigation, Methodology, Writing – review & editing. NS: Investigation, Methodology, Writing – review & editing. JS: Investigation, Methodology, Writing – review & editing. CB-D-O: Investigation, Methodology, Writing – review & editing. RB-D-O: Investigation, Methodology, Writing – review & editing. RM-B: Methodology, Writing – review & editing. CA: Methodology, Writing – original draft. GO: Methodology, Writing – original draft. JC: Formal analysis, Investigation, Methodology, Writing – review & editing. FR: Formal analysis, Investigation, Methodology, Writing – review & editing. MP: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – review & editing. KR: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Fundação Carlos Chagas Filho de Support for Research in the State of Rio de Janeiro, grant number E-26/210.4001/2019, UERJ and Fiocruz.
Acknowledgments
The authors thank the Electronic and Confocal Microscopy Laboratory (LABMEL) in Rio de Janeiro State University (UERJ).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Murugesan A, Manoharan M. Dengue virus. In: Emerging and Reemerging Viral Pathogens. Elsevier (2020). p. 281–359 (Casablanca, Morocco). doi: 10.1016/B978-0-12-819400-3.00016-8
2. Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, et al. The global distribution and burden of dengue. Nature. (2013) 496:504–7. doi: 10.1038/nature12060
3. Chaturvedi UC, Shrivastava R. Dengue haemorrhagic fever: a global challenge. Indian J Med Microbiol. (2004) 22:5–6. doi: 10.1016/S0255-0857(21)02943-1
4. European Centre for Disease Prevention and Control. Dengue worldwide overview. Stockholm. ECDC (2023) (European Centre for Disease Prevention and Control site). Available at: https://www.ecdc.europa.eu/en/dengue-monthly (Acessed June, 3, 2024).
5. Fujita DM, Salvador FS, Nali LHDS, Andrade Júnior HF. Dengue and climate changes: Increase of DENV-1 in São Paulo/Brazil - 2023. Travel Med Infect Dis. (2023) 56:102668. doi: 10.1016/j.tmaid.2023.102668
6. Ministério da Saúde. Monitoramento das Arboviroses. Brasília: Ministério da Saúde (2024). Available at: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/a/aedes-aEgypti/monitoramento-das-arboviroses (Acessed August, 20, 2024).
7. Guzman MG, Gubler DJ, Izquierdo A, Martinez E, Halstead SB. Dengue infection. Nat Rev Dis Primers. (2016) 2:16055. doi: 10.1038/nrdp.2016.55
8. Khanam A, Gutiérrez-Barbosa H, Lyke KE, Chua JV. Immune-mediated pathogenesis in dengue virus infection. Viruses. (2022) 14:2575. doi: 10.3390/v14112575
9. Kok BH, Lim HT, Lim CP, Lai NS, Leow CY, Leow CH. Dengue virus infection - a review of pathogenesis, vaccines, diagnosis and therapy. Virus Res. (2023) 324:199018. doi: 10.1016/j.virusres.2022.199018
10. de Andrade Vieira Alves F, Nunes PCG, Arruda LV, Salomão NG, Rabelo K. The innate immune response in DENV- and CHIKV-infected placentas and the consequences for the fetuses: A minireview. Viruses. (2023) 15:1885. doi: 10.3390/v15091885
11. Htun TP, Xiong Z, Pang J. Clinical signs and symptoms associated with WHO severe dengue classification: a systematic review and meta-analysis. Emerging Microbes Infections. (2021) 10:1116–28. doi: 10.1080/22221751.2021.1935327
12. World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. Geneva: World Health Organization (2009).
13. Dhanoa A, Hassan SS, Ngim CF, Lau CF, Chan TS, Adnan NAA, et al. Impact of dengue virus (DENV) co-infection on clinical manifestations, disease severity and laboratory parameters. BMC Infect Dis. (2016) 16:406. doi: 10.1186/s12879-016-1731-8
14. Verdeal JCR, Costa Filho R, Vanzillotta C, de Macedo GL, Bozza FA, Toscano L, et al. Recomendações Para O Manejo de Pacientes com Formas Graves de Dengue. Rev Bras Ter Intensiv. (2011) 23:125–33. doi: 10.1590/S0103-507X2011000200004
15. Beltz LA. Dengue virus. In: Beltz LA, editor. Zika and other neglected and emerging flaviviruses. Elsevier B.V, Amsterdam (2021). p. 19–39. doi: 10.1016/B978-0-323-82501-6.00002-5
16. Rodriguez-Barraquer I, Cordeiro MT, Braga C, Souza WV, Marques ET, Cummings DA. From re-emergence to hyperendemicity: the natural history of the dengue epidemic in Brazil. PloS Negl Trop Dis. (2011) 5:1–7. doi: 10.1371/journal.pntd.0000935
17. Hentzy Moraes G, de Fátima Duarte E, Carmen Duarte E. Determinants of mortality from severe dengue in Brazil: a population-based case-control study. Am J Trop Med Hygiene. (2013) 88:670–6. doi: 10.4269/ajtmh.11-0774
18. Leowattana W, Laowattana T. Dengue hemorrhagic fever and the liver. World J Hepatol. (2021) 13:1968–76. doi: 10.4254/wjh.v13.i12.1968
19. Nimmagadda SS, Mahabala C, Boloor A, Manibettu Raghuram P, Akshatha Nayak U. Atypical manifestations of dengue fever – where do we stand today? J Clin Diagn Res. (2014) 8:71–3. doi: 10.7860/jcdr/2014/6885.3960
20. Mendez A, Gonzalez G. Abnormal clinical manifestations of dengue hemorrhagic fever in children. Biomedica. (2006) 26:61–70.
21. Jessie K, Fong M, Devi S, Lam S, Wong K. Thong localization of dengue virus in naturally infected human tissues, by immunohistochemistry and in situ hybridization. J Infect Dis. (2004) 189:1411–8. doi: 10.1086/383043
22. Basílio-de-Oliveira CA, Aguiar GR, Baldanza MS, Barth OM, Eyer-Silva WA, Paes MV. Pathologic study of a fatal case of dengue-3 virus infection in Rio de Janeiro, Brazil. Braz J Infect Dis. (2005) 9:341–7. doi: 10.1590/S1413-86702005000400012
23. Salgado DM, Eltit JM, Mansfield K, Panqueba C, Castro D, Vega MR, et al. Heart and skeletal muscle are targets of dengue virus infection. Pediatr Infect Dis J. (2010) 29:238–42. doi: 10.1097/INF.0b013e3181bc3c5b
24. Póvoa TF, Alves AMB, Oliveira CAB, Nuovo GJ, Chagas VLA, Paes MV. The pathology of severe dengue in multiple organs of human fatal cases: histopathology, ultrastructure, and virus replication. PloS One. (2014) 9:1–16. doi: 10.1371/journal.pone.0083386
25. Shivanthan MC, Navinan MR, Constantine GR, Rajapakse S. Cardiac involvement in dengue infection. J Infect Dev Ctries. (2015) 9:338–46. doi: 10.3855/jidc.6200
26. Marchiori E, Ferreira JLN, Bittencourt CN, Neto CA, Zanetti G, Mano CM, et al. Pulmonary hemorrhage syndrome associated with dengue fever, high-resolution computed tomography findings: a case report. Orphanet J Rare Dis. (2009) 4:8. doi: 10.1186/1750-1172-4-8
27. Oliveira LLS, Alves FAV, Rabelo K, Moragas LJ, Mohana-Borges R, de Carvalho JJ, et al. Immunopathology of renal tissue in fatal cases of dengue in children. Pathogens. (2022) 11:1543. doi: 10.3390/pathogens11121543
28. Alves FAV, Oliveira LLS, Salomão NG, Provance DW, Basílio-de-Oliveira CA, Basílio-de-Oliveira RP, et al. Cytokines and inflammatory mediators: markers involved in interstitial damage to the pancreas in two dengue fever cases associated with acute pancreatitis. PloS One. (2022) 17:1–16. doi: 10.1371/journal.pone.0262785
29. Póvoa TF, Oliveira ERA, Basílio-de-Oliveira CA, Nuovo GJ, Chagas VLA, Salomão NG, et al. Peripheral organs of dengue fatal cases present strong proinflammatory response with participation of IFN-gamma-, TNF-alpha- and RANTES-producing cells. PloS One. (2016) 11:1–19. doi: 10.1371/journal.pone.0168973
30. Nunes P, Nogueira R, Coelho J, Rodrigues F, Salomão N, José C, et al. A stillborn multiple organs' Investigation from a maternal DENV-4 infection: histopathological and inflammatory mediators characterization. Viruses. (2019) 11:319. doi: 10.3390/v11040319
31. Chen YC, Wang SY. Activation of terminally differentiated human monocytes/macrophages by dengue virus: productive infection, hierarchical production of innate cytokines and chemokines, and the synergistic effect of lipopolysaccharide. J Virol. (2002) 76:9877–87. doi: 10.1128/jvi.76.19.9877-9887.2002
32. von Ranke FM, Zanetti G, Hochhegger B, Marchiori E. Infectious diseases causing diffuse alveolar hemorrhage in immunocompetent patients: a state-of-the-art review. Lung. (2013) 191:9–18. doi: 10.1007/s00408-012-9431-7
33. Setlik RF, Ouellette D, Morgan J, McAllister CK, Dorsey D, Agan BK, et al. Pulmonary hemorrhage syndrome associated with an autochthonous case of dengue hemorrhagic fever. South Med J. (2004) 97:688–91. doi: 10.1097/00007611-200407000-00015
34. Wang CC, Liu SF, Liao SC, Lee IK, Liu JW, Lin AS, et al. Acute respiratory failure in adult patients with dengue virus infection. Am J Trop Med Hyg. (2007) 77:151–8. doi: 10.4269/ajtmh.2007.77.151
35. Elling R, Henneke P, Hatz C, Hufnagel M. Dengue fever in children: where are we now? Pediatr Infect Dis J. (2013) 32:1020–2. doi: 10.1097/INF.0b013e31829fd0e9
36. Verhagen LM, de Groot R. Dengue in children. J Infect. (2014) 69:S77–S86. doi: 10.1016/j.jinf.2014.07.020
37. Hammond SN, Balmaseda A, Pérez L, Tellez Y, Saborío SI, Mercado JC, et al. Differences in dengue severity in infants, children, and adults in a 3-year hospital-based study in Nicaragua. Am J Trop Med Hyg. (2005) 73:1063–70. doi: 10.4269/ajtmh.2005.73.1063
38. Trung DT, Thao le TT, Dung NM, Ngoc TV, Hien TT, Chau NV, et al. Clinical features of dengue in a large Vietnamese cohort: intrinsically lower platelet counts and greater risk for bleeding in adults than children. PloS Negl Trop Dis. (2012) 6:1–11. doi: 10.1371/journal.pntd.0001679
39. Vitoria WO, Thomé LS, Kanashiro-Galo L, Carvalho LV, Penny R, Santos WLC, et al. Upregulation of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 in renal tissue in severe dengue in humans: Effects on endothelial activation/dysfunction. Rev Soc Bras Med Trop. (2019) 52:e20180353. doi: 10.1590/0037-8682-0353-2018
40. Vuong NL, Lam PK, Ming DKY, Duyen HTL, Nguyen NM, Tam DTH, et al. Combination of inflammatory and vascular markers in the febrile phase of dengue is associated with more severe outcomes. Elife. (2021) 10:e67460. doi: 10.7554/eLife.67460
41. Moragas LJ, Alves F, Oliveira L, Salomão NG, Azevedo CG, da Silva JFR, et al. Liver immunopathogenesis in fatal cases of dengue in children: detection of viral antigen, cytokine profile and inflammatory mediators. Front Immunol. (2023) 14:1215730. doi: 10.3389/fimmu.2023.1215730
42. Bhamarapravati N, Tuchinda P, Boonyapaknavik V. Pathology of Thailand haemorrhagic fever: a study of 100 autopsy cases. Ann Trop Med Parasitol. (1967) 61:500–10. doi: 10.1080/00034983.1967.11686519
43. Nogueira RM, Schatzmayr HG, de Filippis AM, dos Santos FB, da Cunha RV, Coelho JO, et al. Dengue virus type 3, Brazil, 2002. Emerging Infect Dis. (2005) 11:1376–81. doi: 10.3201/eid1109.041043
44. Bosco Siqueira J, Martelli CMT, Coelho GE, Da Rocha Simplício AC, Hatch DL. Dengue and dengue hemorrhagic fever, Brazil, 1981-2002. Emerging Infect Dis. (2005) 11:48–53. doi: 10.3201/eid1101.031091
45. Ling LM, Wilder –Smith A, Leo YS. Fulminant hepatitis in dengue haemorrhagic fever. J Clin Virol. (2007) 38:265–8. doi: 10.1016/j.jcv.2006.12.011
46. Gupta A, Srinivasan R, Setia S, Soundravally R, Pandian DG. Uveitis following dengue fever. Eye. (2009) 23:873–6. doi: 10.1038/eye.2008.124
47. Sundaram C, Shantveer G, Uppin SG, Dakshinamurthy KV, Borgahain R. Acute disseminated encephalomyelitis following dengue hemorrhagic fever. Neurol India. (2010) 58:599–601. doi: 10.4103/0028-3886.68666
48. Miranda SLM, Caprara A, Rocha Peixoto AC, Monteiro CVM, Pessoa RS. Percepção de atores sociais responsáveis pela gestão de resíduos sólidos no contexto do dengue. In: Revista Brasileira de Promoção de Saúde, vol. 26. Fortaleza (2013). p. 233–41 (Fortaleza, Ceara, Brazil).
49. Rodrigues RS, Brum ALG, Paes MV, Póvoa TF, Basilio-de-Oliveira CA, Marchiori E, et al. Lung in dengue: Computed tomography findings. PloS One. (2014) 9:1–7. doi: 10.1371/journal.pone.0096313
50. Celegato M, Sturlese M, Vasconcelos Costa V, Trevisan M, Lallo Dias AS, Souza Passos IB, et al. Small-molecule inhibitor of flaviviral NS3-NS5 interaction with broad-spectrum activity and efficacy in vivo. mBio. (2023) 14:e0309722. doi: 10.1128/mbio.03097-22
51. Akram M, Hameed S, Hassan A, Khan KM. Development in the inhibition of dengue proteases as drug targets. Curr Med Chem. (2024) 31:2195–233. doi: 10.2174/0929867331666230918110144
52. Nunes PCG, Paes MV, de Oliveira CAB, Soares ACG, de Filippis AMB, Lima M, et al. Detection of dengue NS1 and NS3 proteins in placenta and umbilical cord in fetal and maternal death. J Med Virol. (2016) 88:1448–1452. doi: 10.1002/jmv.24479
53. Stanaway JD, Shepard DS, Undurraga EA, Halasa YA, Coffeng LE, Brady OJ, et al. The global burden of dengue: an analysis from the Global Burden of Disease Study 2013. Lancet Infect Dis. (2016) 16:712–23. doi: 10.1016/S1473-3099(16)00026-8
54. Pedrosa M, de Paiva M, Oliveira L, Pereira S, da Silva C, Pompeu J. Oral manifestations related to dengue fever: a systematic review of the literature. Aust Dental J. (2017) 62:404–11. doi: 10.1111/adj.12516
56. Ciambarella BT. Role of TNF–α in inflammatory response caused by silica particles in mice. Rio de Janeiro (2009). p. 60 (ARCa fiocruz). Available at: https://www.arca.fiocruz.br/bitstream/icict/8059/2/69443.pdf (Acessed June 5, 2024).
57. Masyeni S, Wardhana IMW, Nainu F. Cytokine profiles in dengue fever and dengue hemorrhagic fever: A study from Indonesia. Narra J. (2024) 4:e309. doi: 10.52225/narra.v4i1.309
58. Henrique Ferreira Sucupira P, Silveira Ferreira M, Santos Coutinho-da-Silva M, Alves Bicalho K, Carolina Campi-Azevedo A, Pedro Brito-de-Sousa J, et al. Serotype-associated immune response and network immunoclusters in children and adults during acute Dengue virus infection. Cytokine. (2023) 169:156306. doi: 10.1016/j.cyto.2023.156306
59. Costa CH, Rufino R, Lapa e Silva JR. Células inflamatórias e seus mediadores na patogênese da DPOC. Rev Assoc Med Bras. (2009) 55:347–54. doi: 10.1590/S0104-42302009000300031
60. Ding M, Liu L, Hu C, Liu Y, Qiao Y, Jiang X. Expression of VEGFR2 and NRP-1 in non-small cell lung cancer and their clinical significance. Chin J Cancer Res. (2014) 26:669–77. doi: 10.3978/j.issn.1000-9604.2014.12.04
Keywords: dengue virus, children, histopathology, lung, inflammation
Citation: Moragas LJ, Arruda LV, Oliveira LdLS, Alves FdAV, Salomão NG, da Silva JFR, Basílio-de-Oliveira CA, Basílio-de-Oliveira RP, Mohana-Borges R, Azevedo CG, Oliveira GXd, Carvalho JJd, Rosman FC, Paes MV and Rabelo K (2025) Detection of viral antigen and inflammatory mediators in fatal pediatric dengue: a study on lung immunopathogenesis. Front. Immunol. 16:1487284. doi: 10.3389/fimmu.2025.1487284
Received: 27 August 2024; Accepted: 13 January 2025;
Published: 04 February 2025.
Edited by:
Lei Tan, Chinese Academy of Agricultural Sciences, ChinaReviewed by:
Vivian Vasconcelos Costa, Federal University of Minas Gerais, BrazilMarcos Jessé Abrahão Silva, Evandro Chagas Institute, Brazil
Copyright © 2025 Moragas, Arruda, Oliveira, Alves, Salomão, da Silva, Basílio-de-Oliveira, Basílio-de-Oliveira, Mohana-Borges, Azevedo, Oliveira, Carvalho, Rosman, Paes and Rabelo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kíssila Rabelo, a2lzc2lsYXJhYmVsbzkxQGdtYWlsLmNvbQ==
†These authors share first authorship
‡Deceased