 Fernando Rodríguez-Jorge1†
Fernando Rodríguez-Jorge1† José Ignacio Fernández-Velasco2*†‡
José Ignacio Fernández-Velasco2*†‡ Noelia Villarrubia2
Noelia Villarrubia2 Julia Gracia-Gil3Eva Fernández3
Julia Gracia-Gil3Eva Fernández3 Virginia Meca-Lallana4Carolina Díaz-Pérez4
Virginia Meca-Lallana4Carolina Díaz-Pérez4 Susana Sainz de la Maza2Eva María Pacheco5Ana Quiroga6Lluis Ramió-Torrentà6Sergio Martínez-Yélamos7Laura Bau7
Susana Sainz de la Maza2Eva María Pacheco5Ana Quiroga6Lluis Ramió-Torrentà6Sergio Martínez-Yélamos7Laura Bau7 Enric Monreal1Ana López-Real8
Enric Monreal1Ana López-Real8 Alexander Rodero-Romero2Laura Borrega9Santiago Díaz10Pablo Eguía10
Alexander Rodero-Romero2Laura Borrega9Santiago Díaz10Pablo Eguía10 Mercedes Espiño2
Mercedes Espiño2 Juan Luis Chico-García1
Juan Luis Chico-García1 Francisco Javier Barrero11
Francisco Javier Barrero11 María Luisa Martínez-Ginés12
María Luisa Martínez-Ginés12 José Manuel García-Domínguez12Soraya De la Fuente13
José Manuel García-Domínguez12Soraya De la Fuente13 Irene Moreno14
Irene Moreno14 Raquel Sainz-Amo1,2M. Alba Mañé-Martínez15
Raquel Sainz-Amo1,2M. Alba Mañé-Martínez15 Ana Caminero16
Ana Caminero16 Fernando Castellanos-Pinedo17Ana Gómez López13
Fernando Castellanos-Pinedo17Ana Gómez López13 Andrés Labiano-Fontcuberta13Lucía Ayuso18Rossana Abreu19Miguel Ángel Hernández19
Andrés Labiano-Fontcuberta13Lucía Ayuso18Rossana Abreu19Miguel Ángel Hernández19 José Meca-Lallana20Lorena Martín-Aguilar21
José Meca-Lallana20Lorena Martín-Aguilar21 Alfonso Muriel García22
Alfonso Muriel García22 Jaime Masjuan1
Jaime Masjuan1 Lucienne Costa-Frossard1
Lucienne Costa-Frossard1 Luisa María Villar2
Luisa María Villar2- 1Neurology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 2Immunology Department, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 3Neurology Department, Complejo Hospitalario Universitario de Albacete, Albacete, Spain
- 4Neurology Department, Hospital Universitario La Princesa, Madrid, Spain
- 5Neurology Department, Hospital Universitario Juan Ramon Jimenez, Huelva, Spain
- 6Neurology Department, Hospital Universitario de Gerona Doctor Josep Trueta, Gerona, Spain
- 7Neurology Department, Hospital Universitario de Bellvitge, Barcelona, Spain
- 8Neurology Department, Complejo Hospitalario Universitario La Coruña, La Coruña, Spain
- 9Neurology Department, Hospital Universitario Fundación Alcorcón, Madrid, Spain
- 10Neurology Department, Hospital Universitario Gran Canaria Doctor Negrín, Gran Canaria, Spain
- 11Neurology Department, Hospital Universitario Clínico San Cecilio Granada, Granada, Spain
- 12Neurology Department, Hospital General Universitario Gregorio Marañon, Madrid, Spain
- 13Neurology Department, Hospital Universitario Doce de Octubre, Madrid, Spain
- 14Neurology Department, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
- 15Neurology Department, Hospital Universitario Joan XXII, Tarragona, Spain
- 16Neurology Department, Complejo Asistencial de Ávila, Ávila, Spain
- 17Neurology Department, Hospital Virgen del Puerto, Cáceres, Spain
- 18Neurology Department, Hospital Universitario Principe de Asturias, Madrid, Spain
- 19Neurology Department, Hospital Universitario Nuestra Señora Candelaria, Tenerife, Spain
- 20Neurology Department, Hospital Clínico Universitario Virgen de la Arrixaca, Murcia, Spain
- 21Neurology Department, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 22Biostatistics Department, Hospital Universitario Ramón y Cajal, Madrid, Spain
Objective: To ascertain the changes of serum neurofilament light chain (sNfL) and glial fibrillary acidic protein (sGFAP) values in relapsing–remitting multiple sclerosis (RRMS) patients treated with ocrelizumab and their association with treatment response.
Methods: Multicenter prospective study including 115 RRMS patients initiating ocrelizumab treatment between February 2020 and March 2022 followed during a year. Serum samples were collected at baseline and every 3 months to measure sNfL and sGFAP levels using single-molecule array (SIMOA) technology. Based on age and body mass index, sNfL values were standardized using z-score. NEDA (non-evidence of disease activity)-3 status was defined for patients free of disease activity after a year of follow-up. Inflammation (INFL) was considered when new relapses occurred during follow-up or new MRI lesions were found at 1-year exploration. PIRA (progression independent of relapse activity) was defined as disability progression occurring in the absence of relapses or new MRI activity.
Results: After a year on ocrelizumab, 85 patients (73.9%) achieved NEDA-3. Thirty patients did not achieve NEDA: 20 (17.4%) because of INFL and 10 (8.7%) because of PIRA. Of INFL patients, 6 (30.0%) had relapses, and 17 (85.0%) had at least one new MRI lesion at the 12-month examination. At baseline, INFL patients had higher sNfL (p = 0.0003) and sGFAP (p = 0.03) than the NEDA-3 group. PIRA patients mostly exhibited low sNfL and heterogeneous sGFAP levels. After a year, NEDA-3 and INFL patients showed similar decreases in sNfL (p < 0.0001) and sGFAP (p < 0.0001 for NEDA-3 and p = 0.001 for INFL ones). However, the decrease occurred earlier in NEDA-3 patients. Accordingly, sNfL > 1.5 z-score 3 months after ocrelizumab initiation indicated a higher risk of inflammation (OR = 13.6; p < 0.0001). Decrease in sGFAP values occurred later in both groups, with significant reductions observed at 12 months for INFL and 6 and 12 months for NEDA-3. No significant changes in sNfL or sGFAP were observed in PIRA patients.
Conclusion: Ocrelizumab induced normalization of sNfL and sGFAP in the majority of NEDA-3 and inflammatory patients but did not cause changes in the PIRA group. Our data suggest that normalization of sNfL and sGFAP is associated with the lack of inflammatory-associated disease progression but it may not affect non-inflammatory PIRA.
1 Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease of the central nervous system (CNS), characterized by inflammation, demyelination, and axonal damage, which leads to the deterioration of neurological function. The accumulation of irreversible disability can result from either relapse-associated worsening (RAW) or progression independent of relapse activity (PIRA) (1). High-efficacy disease-modifying therapies (heDMTs), which include anti-CD20 drugs, have demonstrated near-complete suppression of new relapses and new MRI activity. However, a significant percentage of patients experience silent disability progression (2).
Serum neurofilament light chain (sNfL) levels, obtained within the first year of the disease, have emerged as a useful prognostic biomarker capable of identifying MS patients at high risk of disability progression (3). Early administration of heDMTs in this patient group may prevent such outcomes (4). Conversely, elevated serum glial fibrillary acidic protein (sGFAP) levels appear to be associated with PIRA (5, 6). The impact of heDMTs on patients with high sGFAP values remains to be ascertained.
Ocrelizumab is a humanized monoclonal antibody that specifically targets CD20+ B cells. It has demonstrated a high level of efficacy in preventing new relapses and T2 MRI lesions, with an overall favorable safety profile in clinical trials (7). Furthermore, ocrelizumab has shown a lower progression rate than interferon beta-1a suggesting its potential role in preventing PIRA, particularly in patients with higher exposure to the drug. Ocrelizumab also seems to have a role in decreasing disability progression in older patients than recruited in clinical trials in selected cases under the age of 65 years (8). It has been suggested that higher levels of ocrelizumab in the serum may have a greater impact on disability progression (9). However, there is a lack of predictive factors for clinical response to ocrelizumab in relapsing–remitting MS.
Several studies and authors have explored other biomarkers of response to ocrelizumab in relapsing MS patients, such as switching to a low inflammatory profile increasing T CD8 regulatory cell percentage (10). Kinetics of B-cell repopulation has also shown an influence in radiological activity, being higher in patients with a faster repopulation rate, suggesting a potential benefit of tailoring ocrelizumab dosage in this group (11). In addition, one study has demonstrated that relapsing MS patients switching from fingolimod to ocrelizumab had a suboptimal response compared with those switching from other disease-modifying treatments or naïve patients (12).
Assessing both sNfL and GFAP may be useful for identifying different stages of MS and for predicting prognosis and treatment response (5). Our study aims to evaluate variations of sNfL and sGFAP levels in relapsing–remitting multiple sclerosis (RRMS) patients treated with ocrelizumab and to ascertain the value of both serum biomarkers in predicting response to treatment.
2 Materials and methods
2.1 Patients
This multicenter prospective longitudinal study was conducted at Ramón y Cajal University Hospital following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. The study involved 115 patients, diagnosed with RRMS according to the revised McDonald criteria (13), who consecutively began ocrelizumab treatment in 20 Spanish university hospitals. Recruitment comprised from February 2020 to March 2022. We collected demographic, clinical, and radiological variables at baseline.
This study received approval from the Ramón y Cajal University Hospital Clinical Research Ethics Committee. Prior to participation, written informed consent was obtained from every patient. Anonymized data supporting the findings of this study will be made available to qualified investigators upon reasonable request for 3 years following the study’s publication.
We followed patients prospectively for a year with clinical assessments every 6 months. Increases of the Expanded Disability Status Scale (EDSS) score were considered based on difference between baseline and 1-year scores. If baseline EDSS was 0, increases were defined for more than 1.5 points. If baseline EDSS was 1 to 5, increases were defined for at least 1 point. If baseline EDSS was >5.5 or greater, increases were defined for 0.5 points. Baseline MRI examination was performed within a month before treatment initiation following clinical protocols established in each center. A second MRI study was performed after a year of follow-up.
We classified patients in three groups according to their response to ocrelizumab treatment after 1 year of follow-up. The NEDA-3 group for patients with no evidence of disease activity: no clinical relapses, no disability progression measured by increases in EDSS score, and no new MRI lesions during the year of follow up. The Inflammatory activity group (INFL) for patients with relapses and/or radiological activity after a year of follow-up, and the PIRA group for patients with disability progression independent of relapses and of new T2 or contrast-enhancing lesions at the 12 month of MRI study. Disability progression was considered when EDSS progression was confirmed 6 months after the first EDSS increase was documented. An additional EDSS evaluation was performed at 18 months from baseline in patients showing disability worsening at 1 year.
2.2 Sample collection
Patient blood specimens were obtained just before initiating ocrelizumab treatment and 3, 6, 9, and 12 months thereafter. Serum samples were sent to the Immunology Department of Hospital Ramón y Cajal (Madrid) and stored at −80°C until processed.
2.3 Serum NfL and GFAP quantification
sNfL and sGFAP levels were quantified in an SR-X instrument (Quanterix, Lexington, MA) using the single molecule array (SIMOA) technique (Quanterix, Billerica, MA). We used NF-light Advantage Kit (Quanterix, Billerica, MA) and Serum GFAP Discovery Kit (Quanterix, Billerica, MA), respectively, according to the manufacturer’s instructions. A standardized score (z-score), reflecting the age and body mass index-adjusted standard deviations of sNfL levels from a normative data set of healthy controls, was also considered. A value of 1.5 z-score was considered as cut-off based on previous data (3).
2.4 Statistical analysis
We performed statistical analyses with GraphPad Prism 9.5 software (GraphPad Prism Inc., San Diego, CA) and Stata v17 (StataCorp LLC). Categorical variables were analyzed with a χ2 or Fisher´s exact test. We used Friedman test adjusted for Dunn multiple comparison test to asses differences between baseline and after 3, 6, 9, and 12 months from the same patients. To evaluate the interaction between times and each patient group, a linear mixed-effects model, multilevel models were used to evaluate time, group, and their interaction, subject as random factor. Kruskal–Wallis was used for inter-group comparisons. Spearman test was used to study correlations between sNfL and sGFAP values. To analyze risks of having a relapse since ocrelizumab initiation, we employed multivariable Cox proportional hazard regressions. These regressions provided hazard ratios (HRs) with corresponding 95% confidence intervals (CIs). The multivariable model was adjusted for age, sex, disease duration, relapses in previous year, baseline EDSS, and T2 lesion load. We considered p-values lower than 0.05 as statistically significant.
2.5 Ethical considerations
Written informed consent was obtained from every patient prior to their inclusion in the present study, which was approved by the Ethics Committee of each center participating in this study.
3 Results
This multicenter prospective longitudinal study enrolled 115 MS patients [76 women (66.1%), diagnosed at the age of 41.6 ± 10.1 (mean ± SD) years] who initiated ocrelizumab in 20 Spanish hospitals. Twenty-six patients (22.6%) were naïve, and 89 (77.4%) switched from other disease-modifying treatment due to lack of efficacy or safety reasons. Baseline patient data are depicted in Table 1.
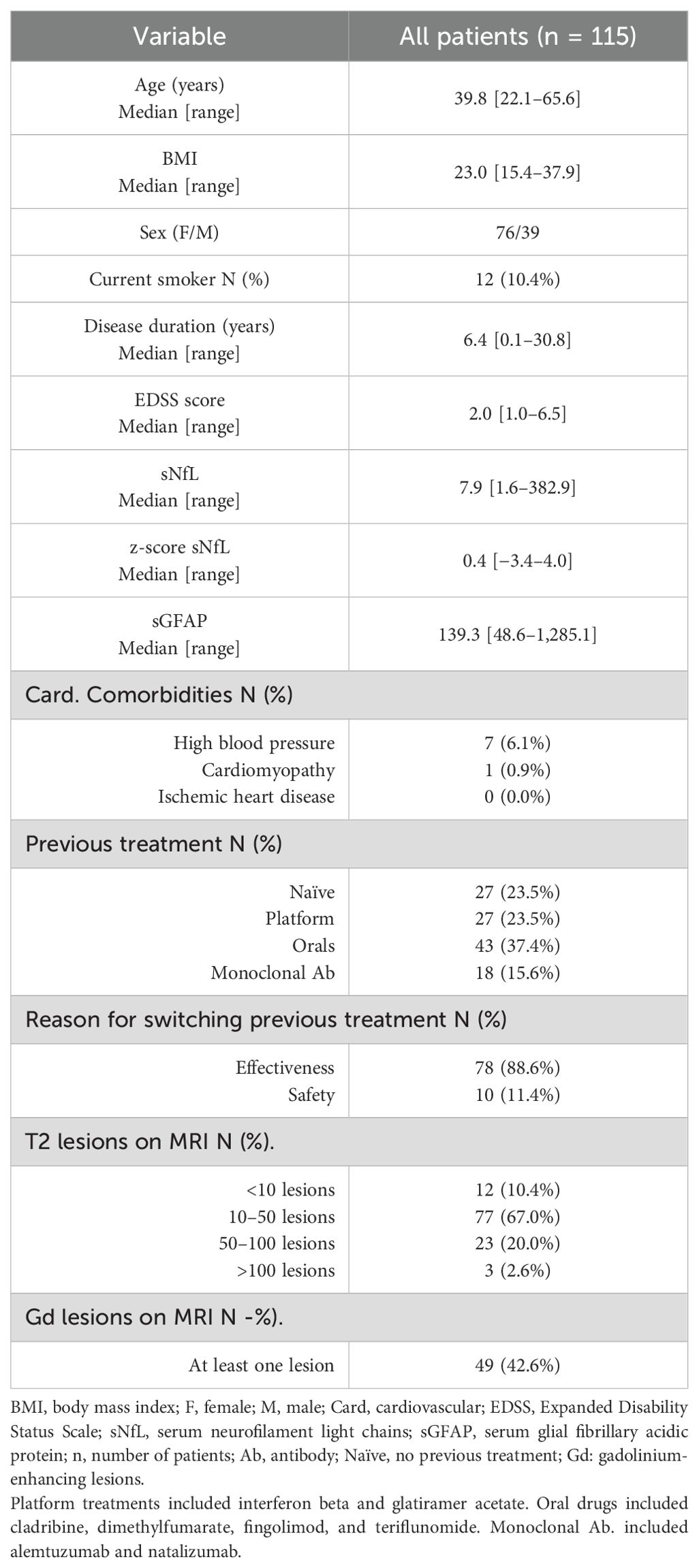
Table 1. Baseline data and patient characteristics.
After a year on ocrelizumab, 85 patients (73.9%) achieved NEDA-3 status (NEDA-3), 20 (17.4%) had inflammatory activity (INFL), and 10 (8.7%) had disease progression independent of relapses (PIRA). Of the INFL patients, 17 (85.0%) had at least one new T2 lesion at 12-month MRI examination, with 3 (15.0%) of them having new gadolinium-enhancing lesions, and 6 (30.0%) had a relapse during treatment follow-up with a median [range] time of 4.94 [0.10–11.80] months. To analyze the risk of suffering this first relapse since starting ocrelizumab, we performed a multivariable regression analysis incorporating both sNfL z-score and sGFAP levels as predictors (Table 2). Patients with elevated sNfL z-scores at baseline exhibit a higher risk of experiencing a relapse (HR of 2.12; 95% CI 1.12–3.99; p = 0.02). sGFAP levels was not associated with heightened risk of relapses.
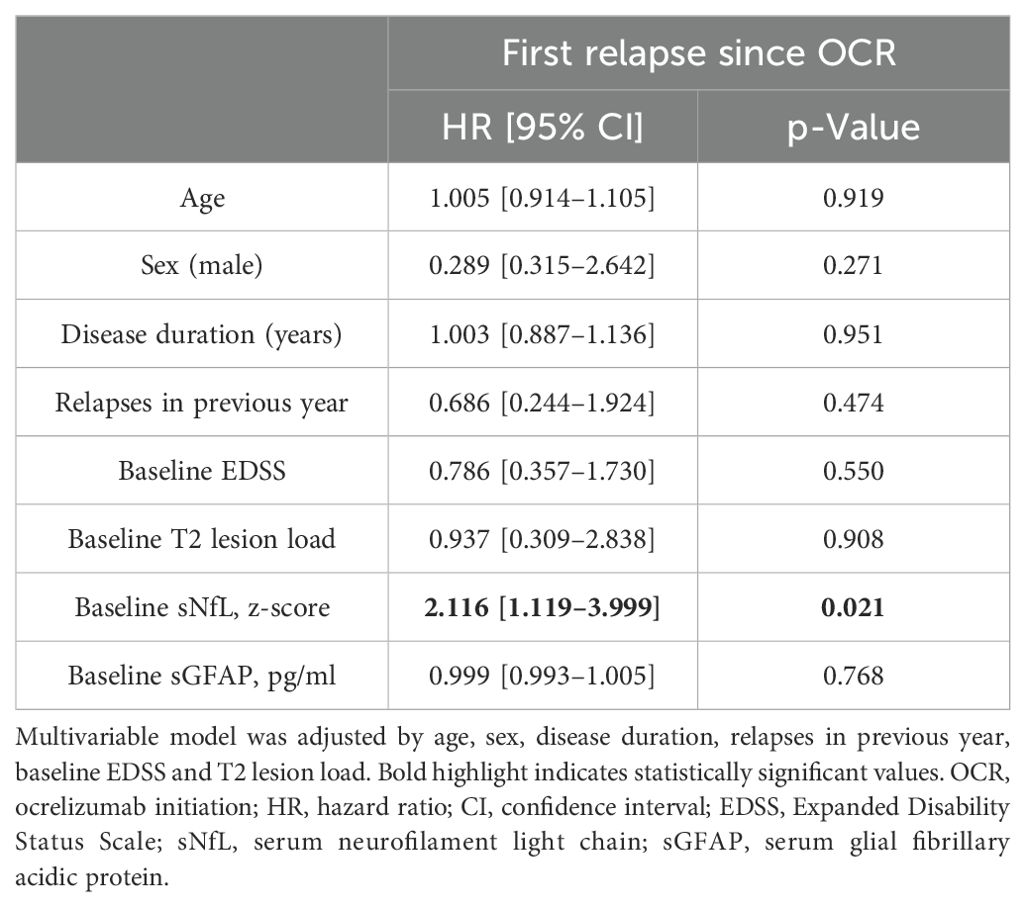
Table 2. Multivariable Cox regression model testing the associations between baseline sNfL z-score and sGFAP levels and the risk of first relapse appearance since o initiation.
No baseline differences were found between the three groups in terms of patient age, body mass index, smoking status, cardiovascular comorbidities, disease duration, EDSS score, or number of MRI lesions. However, the percentage of women was higher in the INFL group than that in the NEDA-3 group (87.0% vs. 59.8%, p = 0.02, Table 3). Additionally, of no naïve-treatment patients, 78 (88.6%) switched from previous treatment due to lack of effectiveness (appearance of clinical and/or radiological activity) and 10 (11.4%) due to safety reasons, with no significant differences between groups. Interestingly, patients with PIRA received more frequently an oral drug as previous treatment than those in the INFL (p = 0.009, Table 3) and NEDA-3 (p = 0.0004, Table 3) groups.

Table 3. Differences among groups in baseline characteristics.
At baseline, the INFL patients exhibited higher sNfL z-score than the NEDA-3 (p = 0.0003) and PIRA (p = 0.01) ones (Figure 1A). The INFL group also showed higher sGFAP values than the NEDA-3 group (p = 0.03, Figure 1B). By contrast, PIRA patients showed no differences in sGFAP values compared with the other two groups.
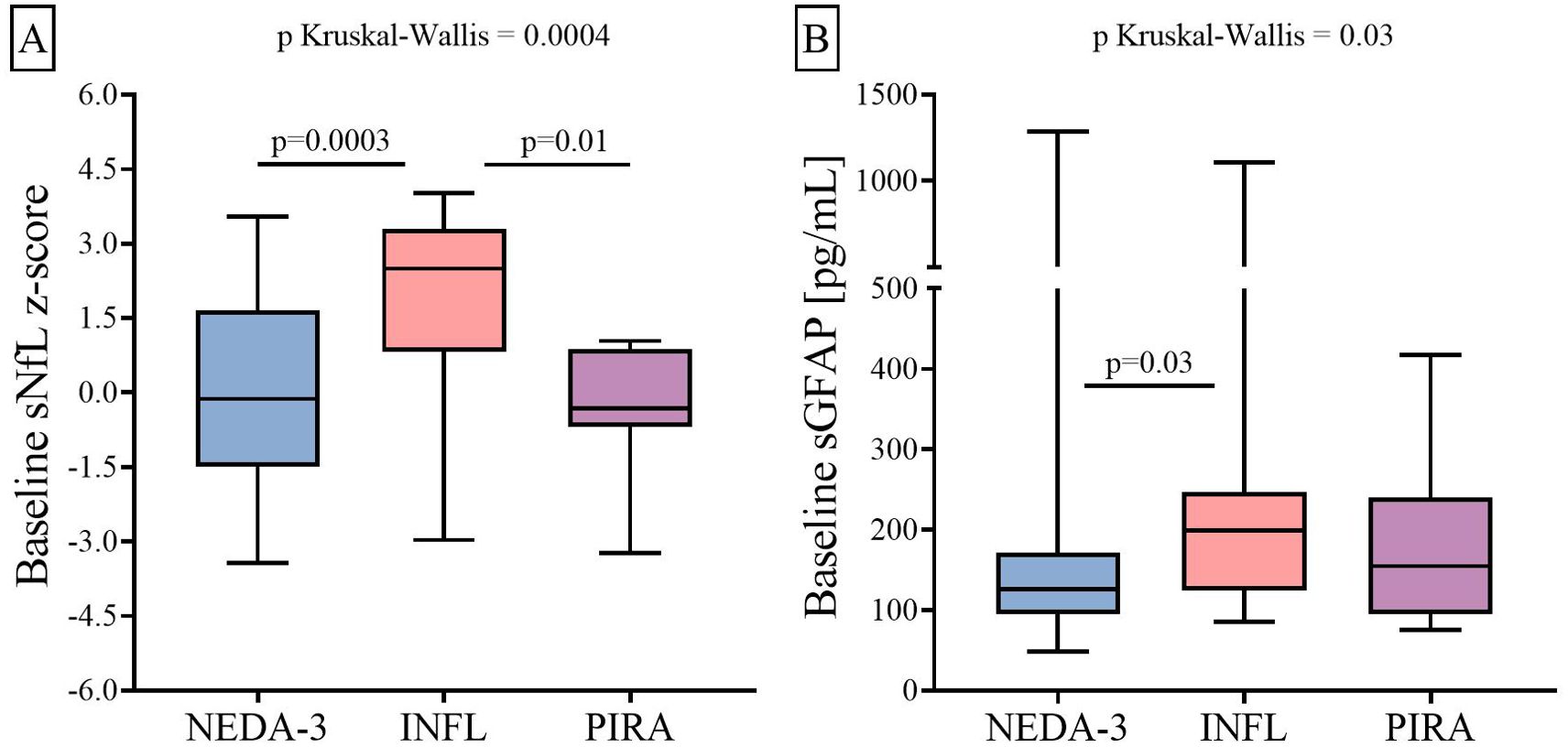
Figure 1. Differences between three groups of RRMS patients in baseline sNfL (A) and sGFAP (B) levels. RRMS, relapsing–remitting multiple sclerosis; sNfL, serum neurofilament light chains; sGFAP, serum glial fibrillary acidic protein; KW, Kruskal–Wallis test; NEDA-3, patients free of disease activity at 12 months of ocrelizumab initiation (n = 85); INFL, patients with new relapses and/or radiological activity during follow-up (n = 20); PIRA, patients who had confirmed disability progression in the absence of relapses or new MRI activity at 12 months of ocrelizumab initiation (n = 10).
After a year of treatment, sNfL z-score and sGFAP values decreased in the NEDA-3 (p = 0.000001 and p = 0.0004, respectively) and INFL groups (p = 0.00004 and p = 0.001, respectively). However, we did not appreciate significant changes in any of both variables in the PIRA patients (Figures 2A, B).
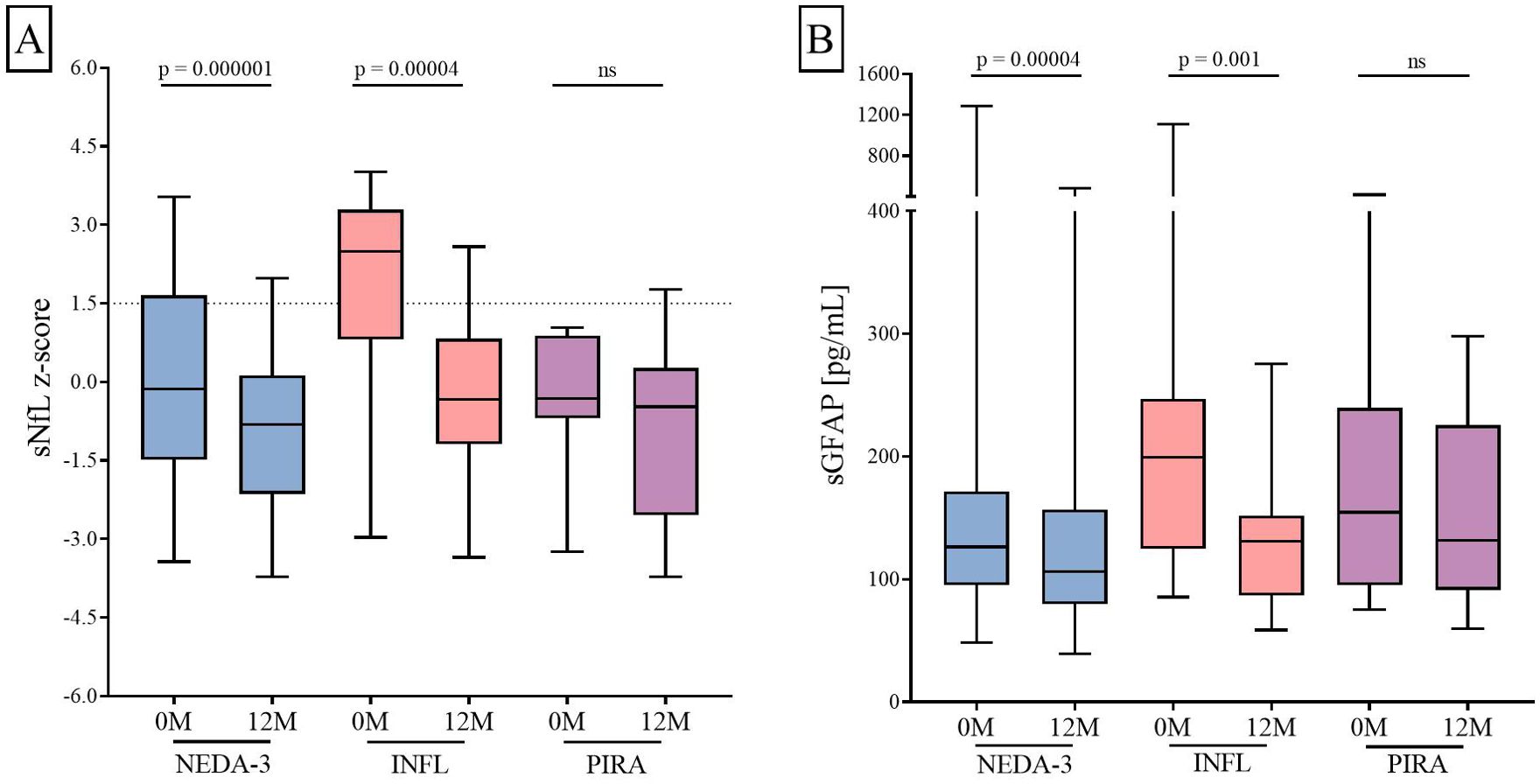
Figure 2. Changes in sNfL (A) and sGFAP (B) levels induced by ocrelizumab. sNfL and sGFAP levels measured before (0M) and at 12 months (12M) of ocrelizumab initiation. Abbreviations: sNfL, serum neurofilament light chains; sGFAP, serum glial fibrillary acidic protein. ns: non-significant; NEDA-3, patients free of disease activity at 12 months of ocrelizumab initiation (n = 85); INFL, patients with new relapses and/or radiological activity during follow-up (n = 20); PIRA, patients who had confirmed disability progression in the absence of relapses or new MRI activity at 12 months of ocrelizumab initiation (n = 10).
We next explored the kinetics of sNfL and sGFAP changes at 3, 6, 9, and 12 months of follow-up (Figure 3) where reductions only occurred in both the NEDA (p = 0.0000004 for sNfL z-score and p = 0.000001 for sGFAP) and INFL (p = 0.0000006 for sNfL z-score and p = 0.002 for sGFAP) groups.
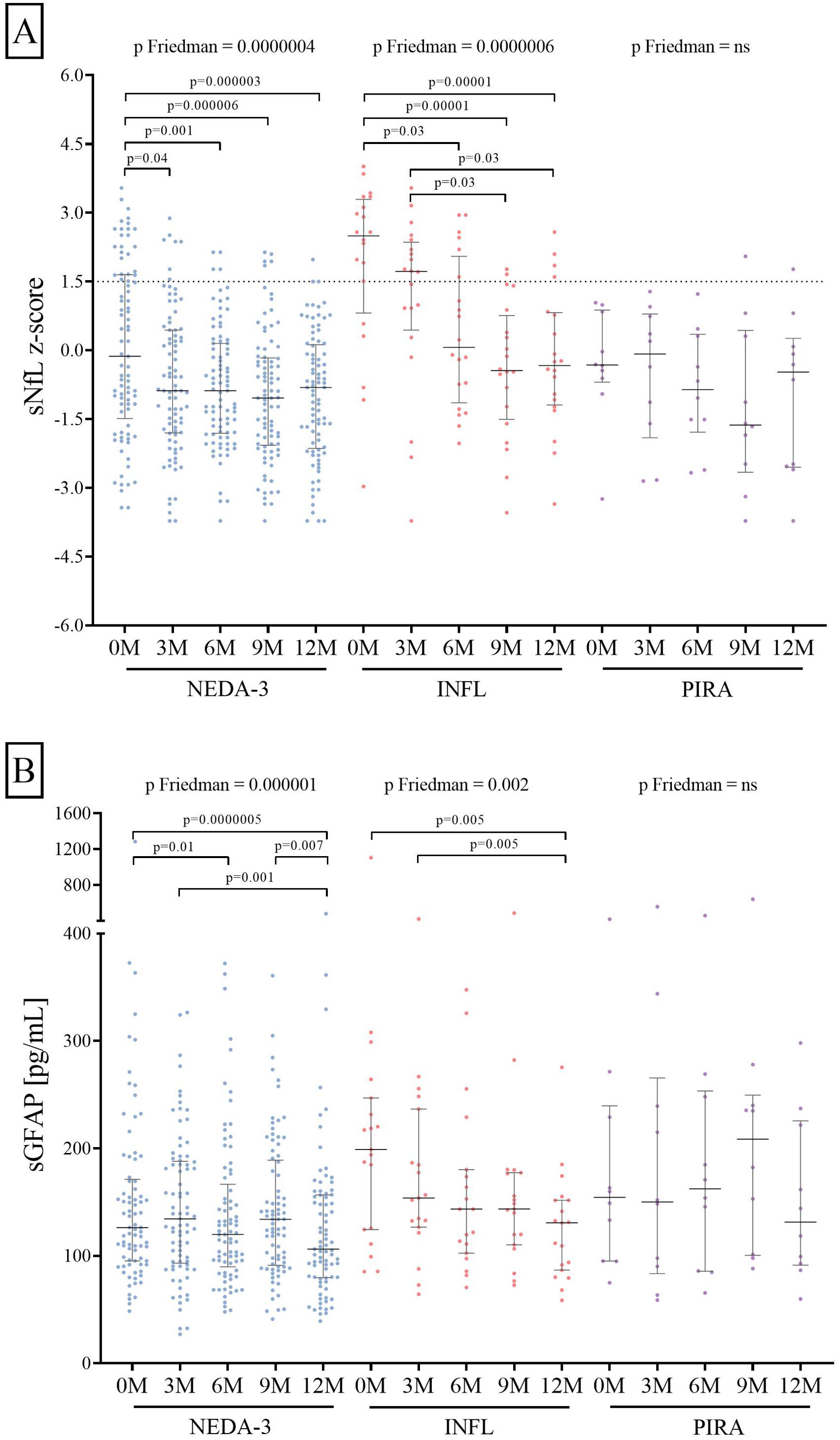
Figure 3. Three-month variations in sNfL (A) and sGFAP (B) levels induced by ocrelizumab treatment. sNfL and sGFAP levels measured before (0M) and at 3 (3M), 6 (6M), 9 (9M), and 12 (12M) months of ocrelizumab initiation. Abbreviations: sNfL, serum neurofilament light chains; sGFAP, serum glial fibrillary acidic protein; NEDA-3, patients free of disease activity at 12 months of ocrelizumab initiation (n = 85); INFL, patients with new relapses and/or radiological activity during follow-up (n = 20); PIRA, patients who had confirmed disability progression in the absence of relapses or new MRI activity at 12 months of ocrelizumab initiation (n = 10).
While a drop in the sNfL z-score was already observed at 3 months after ocrelizumab initiation in the NEDA-3 group (p = 0.04) and at 6 months in the INFL group (p = 0.03, Figure 3A), significant decreases in sGFAP values occurred after 12 months of follow-up. In the NEDA-3 patients, it was observed at 6 months after treatment initiation (p = 0.01) and remained consistent after 1 year (p = 0.0000005, Figure 3B). In the inflammatory ones, the reduction became significant at 12 months (p = 0.005, Figure 3B). No changes in the sNfL and sGFAP values were observed in the PIRA group.
Based on sNfL, we assessed the risk of developing inflammatory activity during the follow-up period (Figure 4). A 1.5 sNfL z-score cut-off value was applied, and we analyzed the results obtained from baseline, 3-month, and 6-month samples (Figures 4A–C, respectively). At baseline, 70.6% of the NEDA-3 patients had an sNfL z-score below 1.5, whereas only 25.0% of the INFL patients had sNfL at these levels (p = 0.0003). After 3 months of ocrelizumab treatment, 91.8% of NEDA-3 patients achieved an sNfL z-score below 1.5, whereas only 45.0% of INFL patients did (p = 0.00001). The differences remained significant at 6 months (p = 0.006). By 9 months, no significant differences were observed between the two groups. These findings were consistent with the clinical data, as 71.4% of patients who experienced a relapse during treatment did so within the first 6 months following ocrelizumab administration. We selected values obtained at 3 months after initiating ocrelizumab as the most effective predictor (sensitivity 61.1%, specificity 89.7%, negative predictive value 87.4%, Supplementary Table 1) of inflammatory status. An sNfL value higher than a 1.5 z-score at this point clearly increased the risk of experiencing inflammatory activity during the first year of treatment [p = 0.00001, odds ratio (OR) = 13.6; 95% confidence interval (CI): 4.2–45.2].

Figure 4. Risk of achieving inflammatory activity at baseline (A), 3 months (B), and 6 months (C) of ocrelizumab follow-up. Number (N) of patients with sNFL values above (orange) or below (green) 10 pg/ml. OCR, ocrelizumab treatment; sNfL, serum neurofilament light chains; NEDA-3, patients free of disease activity at 12 months of ocrelizumab initiation (n = 85); INFL, patients with new relapses and/or radiological activity during follow-up (n = 20); OR, odds ratio; CI, confidence interval.
4 Discussion
Ocrelizumab is a high-efficacy monoclonal antibody that selectively depletes CD20+ cells while maintaining B-cell reconstitution and pre-existing humoral immunity (14). Different works demonstrated the high efficacy of this drug in RRMS patients (15–17). Different data demonstrated its ability in prevention relapse-associated disability worsening (RAW) as it was observed that most cases of disability progression in patients treated with ocrelizumab were associated with PIRA (18, 19). We aimed to explore the association of sNfL or sGFAP values with RAW and PIRA in a multicenter prospective cohort of 115 RRMS patients treated with ocrelizumab and followed for a year. sNfL levels can serve as a biomarker for monitoring inflammation (3, 20–22) and can predict disease progression (4). Additionally, sGFAP, a marker of astroglial activation, has been associated with MS progression in combination with high sNfL values or as an independent factor (6). High values of sNfL and sGFAP may indicate disease progression associated with acute inflammation, while high sGFAP levels with low sNfL values seem to be more associated with non-inflammatory PIRA (23). However, these biomarkers present some problems for their clinical use. They are not specific for MS and can be increased in other neurological diseases (24) or some other conditions as renal impairment (25). This should be ruled out when evaluating the association of sNfL with MS activity. In addition, sNfL normal values increase with age (3), so it may be difficult to establish the best cut-off values. This was partially solved for sNfL using 10 pg/ml, as the cut off, especially for young individuals, or z-score values (3, 4, 23). For sGFAP, this has been more complicated, but a cut-off value of 140 pg/ml was recently established for individuals younger than 55 years (26).
After follow-up, we classified patients as NEDA-3, INFL, or PIRA according to their response to treatment. sNfL levels reflect acute axonal damage and are strongly associated with acute inflammatory activity manifested as relapses or new MRI lesions (3, 21). Accordingly, we defined inflammatory activity as the presence of new relapses or new T2 or contrast-enhancing MRI lesions. NEDA-3 was described as no inflammatory activity and no disability progression. Different options are being considered to define NEDA-4, with brain atrophy as a widely considered candidate. However, technical issues limit its usefulness, and the use of soluble biomarkers is gaining attention (27). We used sNfL that also reflects axonal damage and is highly reproducible. Additionally, atrophy clearly associates with higher sNfL values (28).
NEDA-3 patients constituted 73.9% of our cohort, the other 17.4% of the patients had inflammatory activity, and the remaining 8.7% experienced PIRA. The NEDA-3 group was characterized by a rapid and maintained decrease in sNfL z-score and a significant decrease in sGFAP values after follow-up. By contrast, inflammatory patients had higher sNfL and sGFAP values at disease onset and showed a more prolonged time to normalize sNfL. In fact, a high sNfL at baseline was associated with a higher risk of relapses during follow-up. By contrast, GFAP levels was not associated with the risk of new relapses. However, after a year, both biomarkers clearly decreased in both groups. This is interesting, since most relapses in the inflammatory group occurred in the first 6 months of treatment, thus corroborating the association of sNfL with acute inflammation (21) and the effect of ocrelizumab in patients with highly inflammatory disease (7, 9, 15). In this line, only a patient with inflammatory activity experienced disability progression showing the effect of ocrelizumab in preventing RAW or inflammatory PIRA (18). Finally, PIRA patients showed low levels of sNfL at treatment onset, but 70% of these patients had high sGFAP values. Ocrelizumab treatment did not change significantly sNfL or sGFAP values in these patients.
Our results can be useful in clinical practice. High sNfL and sGFAP at treatment onset indicate patients at high risk of RAW and inflammatory PIRA, who can respond to treatment with ocrelizumab. Control of the acute inflammatory response seems to precede the normalization of the innate immune response, which has been closely linked to neurodegeneration (29). Conversely, elevated values of sGFAP with normal sNfL may indicate a higher risk of non-inflammatory PIRA. This distinction should aid in fine-tuning treatment selection for MS. In our study, patients with non-inflammatory PIRA had longer disease duration and higher baseline EDSS scores. All of them were previously on oral drugs, and only one had high sNfL levels, compared to the 70% who had elevated sGFAP values unaffected by ocrelizumab treatment. A more inflammatory phase could precede PIRA in these patients, and allowing suboptimal response to treatment for prolonged periods could result in a highly disabling disease with fewer therapeutic options (30). The biomarkers described here could help to prevent therapeutic inertia, which affects up to 25% of daily treatment decisions in MS (31). In fact, early use of ocrelizumab resulted in an optimal response to treatment in naïve-treatment (16) and highly active MS patients (32). Future research is needed to determine the effects of other disease-modifying drugs in preventing both types of disease progression.
Additionally, a high sNfL z-score at the 3-month sample could serve as a reliable biomarker for identifying patients at a high risk of inflammation. This information could be valuable in determining which patients would get profit from a higher dose of ocrelizumab, since the precise characteristics of the patients who would benefit from larger doses are not clearly defined (9).
This study has some limitations such as the relatively limited number of patients and time of follow-up. An independent multicenter study with a higher number of patients followed for a more prolonged period of time would be needed to confirm our data.
In summary, our data demonstrate that sNfL and sGFAP are an important tool to identify patients at risk of inflammatory PIRA, who will benefit from early ocrelizumab treatment. In addition, these biomarkers will contribute, in junction with clinical and MRI data, to avoid therapeutic inertia. It can lead to non-inflammatory PIRA, which reduces the probability of an effective response to treatment in MS patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ramón y Cajal University Hospital Clinical Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FR-J: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. JF-V: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. NV: Conceptualization, Investigation, Methodology, Writing – review & editing. JG-G: Conceptualization, Investigation, Writing – review & editing. EF: Conceptualization, Investigation, Writing – review & editing. VM-L: Conceptualization, Investigation, Writing – review & editing. CD-P: Conceptualization, Investigation, Writing – review & editing. SS: Conceptualization, Investigation, Writing – review & editing. EP: Conceptualization, Investigation, Writing – review & editing. AQ: Conceptualization, Investigation, Writing – review & editing. LR-T: Conceptualization, Investigation, Writing – review & editing. SM-Y: Conceptualization, Investigation, Writing – review & editing. LBa: Conceptualization, Investigation, Writing – review & editing. EM: Conceptualization, Investigation, Writing – review & editing. AL-R: Conceptualization, Investigation, Writing – review & editing. AR-R: Conceptualization, Investigation, Methodology, Writing – review & editing. LBo: Conceptualization, Investigation, Writing – review & editing. SDS: Conceptualization, Investigation, Writing – review & editing. PE: Conceptualization, Investigation, Writing – review & editing. ME: Conceptualization, Investigation, Methodology, Writing – review & editing. JC-G: Conceptualization, Investigation, Writing – review & editing. FB: Conceptualization, Investigation, Writing – review & editing. MM-G: Conceptualization, Investigation, Writing – review & editing. JG-D: Conceptualization, Investigation, Writing – review & editing. IM: Conceptualization, Investigation, Writing – review & editing. RS-A: Conceptualization, Investigation, Writing – review & editing, Methodology. MM-M: Conceptualization, Investigation, Writing – review & editing. AC: Conceptualization, Investigation, Writing – review & editing. FC-P: Conceptualization, Investigation, Writing – review & editing. AL-F: Conceptualization, Investigation, Writing – review & editing. LA: Conceptualization, Investigation, Writing – review & editing. RA: Conceptualization, Investigation, Writing – review & editing. MH: Conceptualization, Investigation, Writing – review & editing. JM-L: Conceptualization, Investigation, Writing – review & editing. LM-A: Conceptualization, Investigation, Writing – review & editing. JM: Conceptualization, Investigation, Writing – review & editing. LC-F: Conceptualization, Investigation, Writing – review & editing. LV: Conceptualization, Investigation, Writing – review & editing, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft. AG-L: Supervision, Validation, Investigation, Writing – review & editing. AM-G: Methodology, Supervision, Formal analysis, Writing – review & editing. SD: Supervision, Validation, Investigation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Red Española de Esclerosis Múltiple (REEM) (RD16/0015/0001), Red Española de Enfermedades Inflamatorias (REI) (RD21/0002/0053), and by the grant PI21/00828, integrated in the Plan Estatal I+D+I and co-funded by ISCIII-Subdirección General de Evaluación and Fondo Europeo de Desarrollo Regional (FEDER, “Otra manera de hacer Europa”).
Acknowledgments
We would like to acknowledge Clara Aguirre Hernández, Gary Álvarez Bravo, and Marta Domı́nguez Gallego for their work in collecting clinical data of MS patients as neurologists, Ana Marı́a Pérez Macias for their labor in collecting blood samples and daily care of patients with MS as nurse specialists, and to David Garcı́a Zamorano, Sonia Ortega Sánchez, and Tamara Villanueva Blanco for their technical assistance with the sample analyses.
Conflict of interest
FR-J received research grants and travel support for speaking engagements from Janssen, Biogen, Novartis, Roche, Sanofi-Genzyme, Bristol-Myers-Squibb and Merck. JG-G received research support, compensation for participating on advisory boards, lecture fees, and/or travel support from Almirall, Bayer, Biogen, Genzyme‐Sanofi, Novartis, Roche, and Teva. EF received research support, compensation for participating on advisory boards, speaking fees, and/or funding for travel from Almirall, Bayer, Biogen, Genzyme‐Sanofi, Merck, Novartis, and Roche. VM-L received consulting and speaking fees from Almirall, Biogen, Genzyme, Janssen, Merck, Novartis, Roche, Terumo, Sanofi, Teva, and Bristol Myers Squibb. CD-P received funding for training and scientific meetings from Sanofi, Merck, Novartis and Roche. SS received research grants, travel support or honoraria for speaking engagements from Almirall, Biogen, Bristol Myers Squibb, Janssen, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. AQ is funded by a grant from the Fundación Francisco Soria y Melguizo and has received funding from Merck, Novartis, and Horizon Therapeutics to attend conferences. LR-T received compensation for consulting services and speaking fees from Biogen, Novartis, Bayer, Merck, Sanofi, Genzyme, Roche, Bristol-Myers-Squibb, TEVA, and Horizon. SM-Y received honoraria for participating on advisory boards and for collaborations as consultant and scientific communications and also received research support as well as funding for travel and congress expenses from Roche, Biogen Idec, Novartis, TEVA, Merck, Genzyme, Sanofi, Bayer, Almirall, and Bristol Myers Squibb. EM received research grants, travel support, or honoraria for speaking engagements from Almirall, Merck, Roche, Sanofi, Bristol Myers Squibbb, Biogen, Janssen, and Novartis. AL-R received speaker and consultation fees from Biogen, Janssen, Novartis, Roche and Sanofi, and congress travel support from Roche. LBo received research grants and travel support from Merck, Roche, Novartis, Sanofi, Horizon and Bristol Myer Squibb. JC-G received speaker fees, travel support, and/or served on advisory boards by Biogen, Sanofi, Bayer, Janssen, BMS, and Bial. FB received compensation for consulting services and speaking honoraria from Almirall, Biogen, Bristol Myer Squibb, Genzyme, Johnson & Johnson, Merck, Novartis, Roche, Sanofi, Teva. MM-G received compensation for consulting services and speaking fees from Merck, Biogen, Novartis, Sanofi-Genzyme, Almirall, BMS, Janssen, Roche, Horizon, and Viatris. JG-D received honoraria as speaker, advisor and researcher from Almirall, Bristol Myers Squibb, Biogen, Janssen, Merck, Novartis, Roche, Teva, and Sanofi. MM-M received research support, funding for travel and congress expenses from Biogen Idec, Teva Pharmaceutical Industries Ltd., Sanofi-Aventis, Merck Serono, Novartis, Bayer Schering Pharma, Bristol Myers Squibb and Roche. JM-L received honoraria as a consultant, lecturer in meetings and has participated in clinical trials and other research projects promoted by Alexion, Almirall, Biogen, Bristol-Meyers-Squibb, Horizon, Johnson & Johnson, Merck, Neuraxpharm, Novartis, Roche, Sandoz, Sanofi and UCB. LC-F received speaker fees, travel support, and/or served on advisory boards by Biogen, Sanofi, Merck, Bayer, Novartis, Roche, Teva, Celgene, Ipsen, Biopas, Almirall. LV received research grants and personal fees from Merck, Roche, Sanofi, Bristol Myers Squibb, Biogen, and Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1480676/full#supplementary-material
Supplementary Table 1 | Predictive values of sNFL z-scores in determining inflammation. PPV, positive predictive value; NPV, negative predictive value; M, months; sNfL, sNfL, serum neurofilament light chains.
References
1. Lublin FD, Häring DA, Ganjgahi H, Ocampo A, Hatami F, Čuklina J, et al. How patients with multiple sclerosis acquire disability. Brain. (2022) 145:3147–61. doi: 10.1093/brain/awac016
2. University of California, San Francisco MS-EPIC Team, Cree BAC, Hollenbach JA, Bove R, Kirkish G, Sacco S, et al. Silent progression in disease activity-free relapsing multiple sclerosis. Ann Neurol. (2019) 85:653–66. doi: 10.1002/ana.25463
3. Benkert P, Meier S, Schaedelin S, Manouchehrinia A, Yaldizli Ö, Maceski A, et al. Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurol. (2022) 21:246–57. doi: 10.1016/S1474-4422(22)00009-6
4. Monreal E, Fernández-Velasco JI, García-Sánchez MI, Sainz de la Maza S, Llufriu S, Álvarez-Lafuente R, et al. Association of serum neurofilament light chain levels at disease onset with disability worsening in patients with a first demyelinating multiple sclerosis event not treated with high-efficacy drugs. JAMA Neurol. (2023) 80:397–403. doi: 10.1001/jamaneurol.2023.0010
5. Barro C, Healy BC, Liu Y, Saxena S, Paul A, Polgar-Turcsanyi M, et al. Serum GFAP and NfL levels differentiate subsequent progression and disease activity in patients with progressive multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2022) 10:e200052. doi: 10.1212/NXI.0000000000200052
6. Meier S, Willemse EAJ, Schaedelin S, Oechtering J, Lorscheider J, Melie-Garcia L, et al. Serum glial fibrillary acidic protein compared with neurofilament light chain as a biomarker for disease progression in multiple sclerosis. JAMA Neurol. (2023) 80:287–97. doi: 10.1001/jamaneurol.2022.5250
7. Hauser SL, Bar-Or A, Comi G, Giovannoni G, Hartung HP, Hemmer B, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. (2017) 376:221–34. doi: 10.1056/NEJMoa1601277
8. Chisari CG, Bianco A, Brescia Morra V, Calabrese M, Capone F, Cavalla P, et al. Effectiveness of ocrelizumab in primary progressive multiple sclerosis: a multicenter, retrospective, real-world study (OPPORTUNITY). Neurotherapeutics. (2023) 20:1696–706. doi: 10.1007/s13311-023-01415-y
9. Hauser SL, Bar-Or A, Weber MS, Kletzl H, Günther A, Manfrini M, et al. Association of Higher Ocrelizumab Exposure With Reduced Disability Progression in Multiple Sclerosis [published correction appears in Neurol Neuroimmunol Neuroinflamm. 2023 Mar 27;10(3). Neurol Neuroimmunol Neuroinflamm. (2023) 10:e200094. doi: 10.1212/NXI.0000000000200094
10. Abbadessa G, Miele G, Maida E, Vanore E, Cipriano L, Coppola C, et al. Immunomodulatory effects of ocrelizumab and candidate biomarkers for monitoring treatment response in multiple sclerosis. Mult Scler. (2023) 29:779–88. doi: 10.1177/13524585221147635
11. Abbadessa G, Miele G, Cavalla P, Valentino P, Marfia GA, Signoriello E, et al. CD19 Cell Count at Baseline Predicts B Cell Repopulation at 6 and 12 Months in Multiple Sclerosis Patients Treated with Ocrelizumab. Int J Environ Res Public Health. (2021) 18:8163. doi: 10.3390/ijerph18158163
12. Pfeuffer S, Rolfes L, Ingwersen J, Pul R, Kleinschnitz K, Korsen M, et al. Effect of previous disease-modifying therapy on treatment effectiveness for patients treated with ocrelizumab. Neurol Neuroimmunol Neuroinflamm. (2023) 10:e200104. doi: 10.1212/NXI.0000000000200104
13. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
14. Greenfield AL, Hauser SL. B-cell Therapy for Multiple Sclerosis: Entering an era. Ann Neurol. (2018) 83:13–26. doi: 10.1002/ana.25119
15. Hauser SL, Kappos L, Arnold DL, Bar-Or A, Brochet B, Naismith RT, et al. Five years of ocrelizumab in relapsing multiple sclerosis: OPERA studies open-label extension. Neurology. (2020) 95:e1854–67. doi: 10.1212/WNL.0000000000010376
16. Cellerino M, Boffa G, Lapucci C, Tazza F, Sbragia E, Mancuso E, et al. Predictors of ocrelizumab effectiveness in patients with multiple sclerosis. Neurotherapeutics. (2021) 18:2579–88. doi: 10.1007/s13311-021-01104-8
17. Lanzillo R, Carotenuto A, Moccia M, Capasso N, Petracca M, Spiezia A, et al. Ocrelizumab treatment in multiple sclerosis: Prospective real world observational multi-center study in Campania, Italy. J Neurol Sci. (2021) 429:118129. doi: 10.1016/j.jns.2021.118129
18. Kappos L, Wolinsky JS, Giovannoni G, Arnold DL, Wang Q, Bernasconi C, et al. Contribution of relapse-independent progression vs relapse-associated worsening to overall confirmed disability accumulation in typical relapsing multiple sclerosis in a pooled analysis of 2 randomized clinical trials. JAMA Neurol. (2020) 77:1132–40. doi: 10.1001/jamaneurol.2020.1568
19. Ingwersen J, Masanneck L, Pawlitzki M, Samadzadeh S, Weise M, Aktas O, et al. Real-world evidence of ocrelizumab-treated relapsing multiple sclerosis cohort shows changes in progression independent of relapse activity mirroring phase 3 trials. Sci Rep. (2023) 13:15003. doi: 10.1038/s41598-023-40940-w
20. Thebault S, Bose G, Booth R, Freedman MS. Serum neurofilament light in MS: The first true blood-based biomarker? Mult Scler. (2022) 28:1491–7. doi: 10.1177/1352458521993066
21. Novakova L, Zetterberg H, Sundström P, Axelsson M, Khademi M, Gunnarsson M, et al. Monitoring disease activity in multiple sclerosis using serum neurofilament light protein. Neurology. (2017) 89:2230–7. doi: 10.1212/WNL.0000000000004683
22. Fernández-Velasco JI, Monreal E, Kuhle J, Meca-Lallana V, Meca-Lallana J, Izquierdo G, et al. Baseline inflammatory status reveals dichotomic immune mechanisms involved in primary-progressive multiple sclerosis pathology. Front Immunol. (2022) 13:842354. doi: 10.3389/fimmu.2022.842354
23. Monreal E, Fernández-Velasco JI, Álvarez-Lafuente R, Sainz de la Maza S, García-Sánchez MI, Llufriu S, et al. Serum biomarkers at disease onset for personalized therapy in multiple sclerosis. Brain. (2024), awae260. doi: 10.1093/brain/awae260. Online ahead of print
24. Khalil M, Teunissen CE, Lehmann S, Otto M, Piehl F, Ziemssen T, et al. Neurofilaments as biomarkers in neurological disorders—Towards clinical application. Nat Rev Neurol. (2024) 20:269–87. doi: 10.1038/s41582-024-00955-x
25. Akamine S, Marutani N, Kanayama D, Gotoh S, Maruyama R, Yanagida K, et al. Renal function is associated with blood neurofilament light chain level in older adults. Sci Rep. (2020) 10:20350. doi: 10.1038/s41598-020-76990-7
26. Rodero-Romero A, Monreal E, Sainz-Amo R, García Domínguez JM, Villarrubia N, Veiga-González JL, et al. Establishing normal serum values of neurofilament light chains and glial fibrillary acidic protein considering the effects of age and other demographic factors in healthy adults. Int J Mol Sci. (2024) 25:7808. doi: 10.3390/ijms25147808
27. Marastoni D, Turano E, Tamanti A, Colato E, Pisani AI, Scartezzini A, et al. Association of levels of CSF osteopontin with cortical atrophy and disability in early multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2024) 11:e200265. doi: 10.1212/NXI.0000000000200265
28. Sotirchos ES, Fitzgerald KC, Singh CM, Smith MD, Reyes-Mantilla M, Hersh CM, et al. Associations of sNfL with clinico-radiological measures in a large MS population. Ann Clin Transl Neurol. (2023) 10:84–97. doi: 10.1002/acn3.51704
29. Absinta M, Maric D, Gharagozloo M, Garton T, Smith MD, Jin J, et al. A lymphocyte-microglia-astrocyte axis in chronic active multiple sclerosis. Nature. (2021) 597:709–14. doi: 10.1038/s41586-021-03892-7
30. Tur C, Carbonell-Mirabent P, Cobo-Calvo Á, Otero-Romero S, Arrambide G, Midaglia L, et al. Association of early progression independent of relapse activity with long-term disability after a first demyelinating event in multiple sclerosis. JAMA Neurol. (2023) 80:151–60. doi: 10.1001/jamaneurol.2022.4655
31. Saposnik G, Andhavarapu S, Fernández Ó, Kim HJ, Wiendl H, Foss M, et al. Factors associated with treatment escalation among MS specialists and general neurologists: Results from an International cojoint study. Mult Scler Relat Disord. (2022) 58:103404. doi: 10.1016/j.msard.2021.103404
Keywords: multiple sclerosis, ocrelizumab, neurofilament light chain, glial fibrillary acidic protein, serum biomarkers
Citation: Rodríguez-Jorge F, Fernández-Velasco JI, Villarrubia N, Gracia-Gil J, Fernández E, Meca-Lallana V, Díaz-Pérez C, Sainz de la Maza S, Pacheco EM, Quiroga A, Ramió-Torrentà L, Martínez-Yélamos S, Bau L, Monreal E, López-Real A, Rodero-Romero A, Borrega L, Díaz S, Eguía P, Espiño M, Chico-García JL, Barrero FJ, Martínez-Ginés ML, García-Domínguez JM, De la Fuente S, Moreno I, Sainz-Amo R, Mañé-Martínez MA, Caminero A, Castellanos F, Gómez López A, Labiano-Fontcuberta A, Ayuso L, Abreu R, Hernández MÁ, Meca-Lallana J, Martín-Aguilar L, Muriel García A, Masjuan J, Costa-Frossard L and Villar LM (2024) Biomarkers of response to ocrelizumab in relapsing–remitting multiple sclerosis. Front. Immunol. 15:1480676. doi: 10.3389/fimmu.2024.1480676
Received: 14 August 2024; Accepted: 19 September 2024;
Published: 12 November 2024.
Edited by:
Simona Bonavita, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Gianmarco Abbadessa, University of Campania Luigi Vanvitelli, ItalyAntonio Carotenuto, University of Naples Federico II, Italy
Copyright © 2024 Rodríguez-Jorge, Fernández-Velasco, Villarrubia, Gracia-Gil, Fernández, Meca-Lallana, Díaz-Pérez, Sainz de la Maza, Pacheco, Quiroga, Ramió-Torrentà, Martínez-Yélamos, Bau, Monreal, López-Real, Rodero-Romero, Borrega, Díaz, Eguía, Espiño, Chico-García, Barrero, Martínez-Ginés, García-Domínguez, De la Fuente, Moreno, Sainz-Amo, Mañé-Martínez, Caminero, Castellanos, Gómez López, Labiano-Fontcuberta, Ayuso, Abreu, Hernández, Meca-Lallana, Martín-Aguilar, Muriel García, Masjuan, Costa-Frossard and Villar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Ignacio Fernández-Velasco, amZ2ZWxhc2NvQHNhbHVkLm1hZHJpZC5vcmc=
†These authors have contributed equally to this work and share first authorship
‡ORCID: José Ignacio Fernández-Velasco, orcid.org/0000-0001-9148-671X